performing electrophysiological measurements in humans inside magnetic resonance imaging scanners;...
TRANSCRIPT

Performing electrophysiological measurements in humans inside Magnetic
Resonance Imaging scanners; applications in Epilepsy research and other areas
Louis Lemieux
Department of Clinical and Experimental EpilepsyUCL Institute of Neurology, Queen Square, London
&MRI Unit, Epilepsy Society
Chalfont St Peter, BuckinghamshireUK

Lemieux – ACES / Europe Dublin 2015
Outline
• Epilepsy
• Multimodal neuroimaging in humans
– EEG and functional MRI (fMRI)
– Mapping epileptic events using scalp EEG-fMRI
• Going deeper: intracranial EEG-fMRI
– Technique implementation
– An epileptic seizure
• Conclusions

Lemieux – ACES / Europe Dublin 2015
Rely on accurate anatomical targeting
Epilepsy• Epilepsy is the most common serious chronic neurological
condition affecting all ages– 50 million people affected in the world– Economic costs (~€20 billion/year for Europe).
• 30% of all people with epilepsy have seizures that do not respond to medical treatment, leading to:– Cognitive decline– Poor quality of life– Significantly increased mortality– High societal costs
• Need for improved treatment– Surgery– Drug delivery
• Need for improved localisation of the epileptogenic areas

Lemieux – ACES / Europe Dublin 2015
• fMRI
– Allows tomographic visualisation of haemodynamic changes associated with
brain activity
– Has better temporal resolution than PET (…for epileptic spikes)
– Is non-invasive (BOLD)
• EEG
– Important observable of brain activity in humans
– Reflects neuronal signal generation and synchronisation
– Important clinical tool in epilepsy (epileptic spikes, seizures, etc)
– Non-invasive (scalp) & cheap
Basic principles: EEG & fMRI
Lemieux – ACES / Europe Dublin 2015
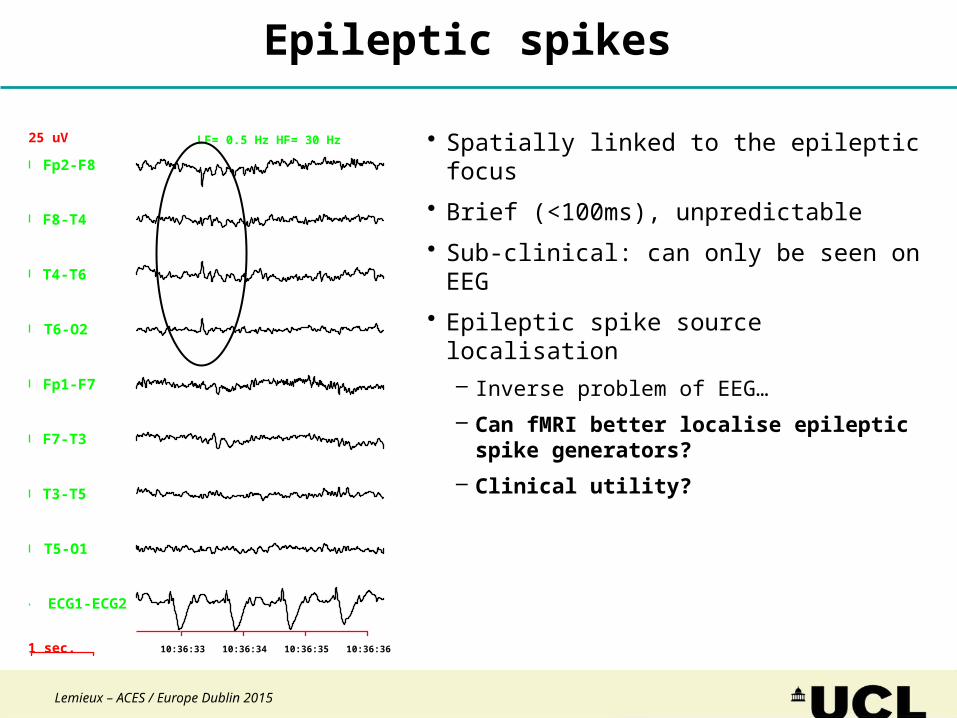
LF= 0.5 Hz HF= 30 Hz
1 sec.
25 uV
10:36:33 10:36:34 10:36:35 10:36:36
Fp2-F8
F8-T4
T4-T6
T6-O2
Fp1-F7
F7-T3
T3-T5
T5-O1
ECG1-ECG2
Epileptic spikes
• Spatially linked to the epileptic focus
• Brief (<100ms), unpredictable
• Sub-clinical: can only be seen on EEG
• Epileptic spike source localisation– Inverse problem of EEG…
– Can fMRI better localise epileptic spike generators?
– Clinical utility?

Lemieux – ACES / Europe Dublin 2015
EEG-fMRI in epilepsyData acquisition strategy
Subject at restSimultaneous EEG-MRI
• fMRI:− Echo-planar imaging (EPI) fMRI
scanning sequences
− Whole-brain coverage
• EEG:− 64-channel cap on scalp
− MR-compatible amplifier and digitiser
− Digital signal transmitted to recording laptop outside the scanner room

Lemieux – ACES / Europe Dublin 2015
EEG-fMRI of epileptic spikes
Continuous EEG and fMRI:
EEG-based GLM
Spike-related BOLD
[Krakow et al, 1999; Lemieux et al, 2001]
1 sec.
25 uV
10:36:33 10:36:34 10:36:35 10:36:36
Fp2-F8
F8-T4
T4-T6
T6-O2
Fp1-F7
F7-T3
T3-T5
T5-O1
ECG1-ECG2

Lemieux – ACES / Europe Dublin 2015
Fp1-Pz
F7 – Pz
T3 – Pz
T5 – Pz
O1 – Pz
Fp2 – Pz
F8 – Pz
T4 – Pz
T6 – Pz
O2 – Pz
Fp1 – F7
F7 – T3
T3 – T5
T5 – O1
Fp2 – F8
F8 – T4
T4 – T6
T6 – O2
ECG
OSC
1 Second LF = 0.5 Hz HF = 45 Hz50uV
The intra-MRI EEG artefact problem

Lemieux – ACES / Europe Dublin 2015
Fp1-Pz
F7 – Pz
T3 – Pz
T5 – Pz
O1 – Pz
Fp2 – Pz
F8 – Pz
T4 – Pz
T6 – Pz
O2 – Pz
Fp1 – F7
F7 – T3
T3 – T5
T5 – O1
Fp2 – F8
F8 – T4
T4 – T6
T6 – O2
ECG
OSC
1 Second LF = 0.5 Hz HF = 45 Hz50uV
[Allen et al, 2000]
The intra-MRI EEG artefact problem

Lemieux – ACES / Europe Dublin 2015
Fp1-Pz
F7 – Pz
T3 – Pz
T5 – Pz
O1 – Pz
Fp2 – Pz
F8 – Pz
T4 – Pz
T6 – Pz
O2 – Pz
Fp1 – F7
F7 – T3
T3 – T5
T5 – O1
Fp2 – F8
F8 – T4
T4 – T6
T6 – O2
ECG
OSC
1 Second LF = 0.5 Hz HF = 45 Hz50uV
[Allen et al, 1999]
The intra-MRI EEG artefact problem
Lemieux – ACES / Europe Dublin 2015
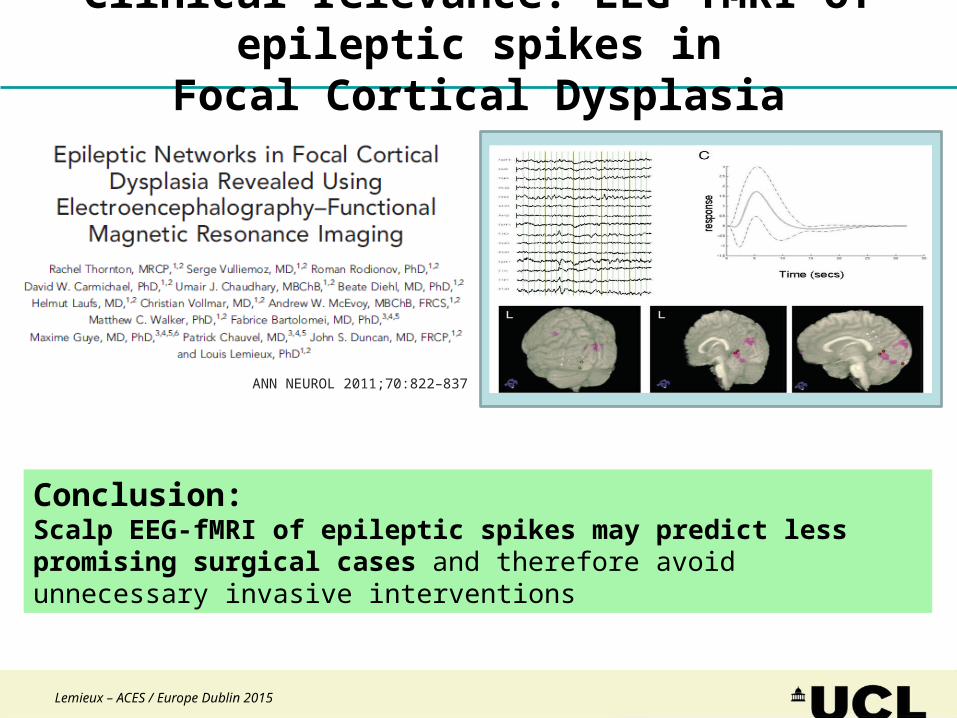
Clinical relevance: EEG-fMRI of epileptic spikes inFocal Cortical Dysplasia
ANN NEUROL 2011;70:822–837
Conclusion:Scalp EEG-fMRI of epileptic spikes may predict less promising surgical cases and therefore avoid unnecessary invasive interventions

Lemieux – ACES / Europe Dublin 2015
icEEG: Subdural grids and depth electrodes• Surgically placed on cortex• Sampling similar to high-density scalp EEG• Used to map epileptogenic tissue in relation to eloquent
cortex• 6x8 array of 3mm diameter Pt-Ir disk contacts
[Fried et al, 1999]
• Surgically inserted within brain• Used to detect epileptogenicity and propagation in deep
cortex/lesions• Sensitivity profile very different from scalp EEG and grids:
‘tunnel vision’ [see Cosandier et al 2007; Church et al, 1985]
• ‘Spencer probe’ commercial design• Pt-Ir cylindrical contacts & Ni-Cr terminations and wires
contained in polyurethane

Lemieux – ACES / Europe Dublin 2015
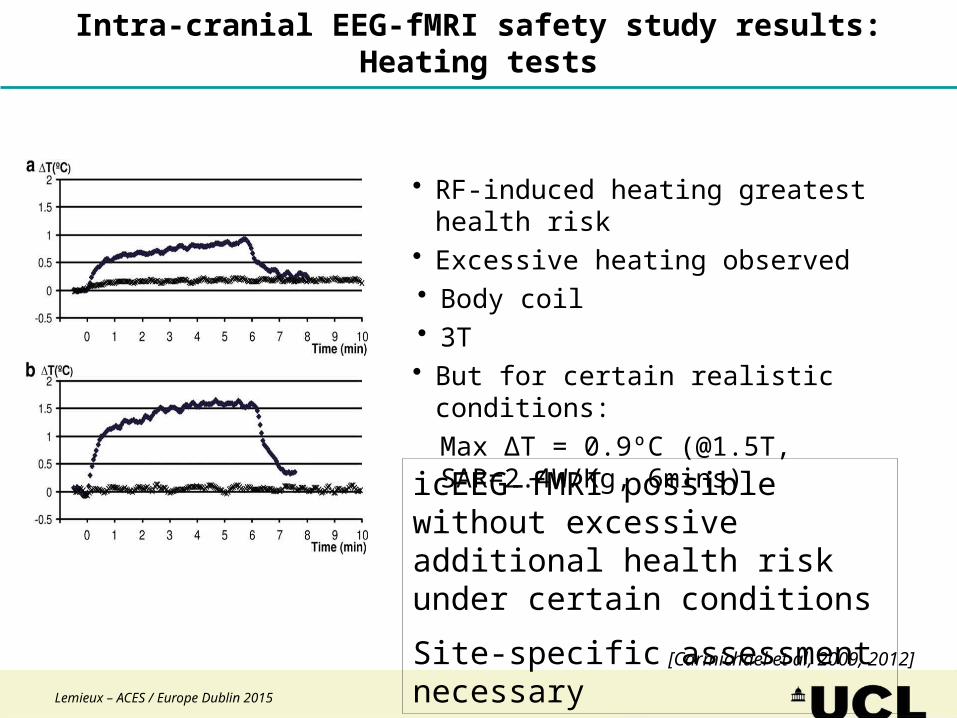
[Carmichael et al, 2009; 2012]
• Health hazards• RF-induced heating• Induced voltages (stimulation)• Factors considered:• Field strength: 1.5T and 3T• RF transmit coil type: head and body• Electrodes: depths and grids • EEG wires
• Geometry and placement• Length• Termination
Simultaneous icEEG-fMRI:Safety tests in phantoms
Lemieux – ACES / Europe Dublin 2015
[Carmichael et al, 2009, 2012]
• RF-induced heating greatest health risk• Excessive heating observed• Body coil• 3T• But for certain realistic conditions:
Max ∆T = 0.9ºC (@1.5T, SAR=2.4W/Kg, 6mins)
icEEG-fMRI possible without excessive additional health risk under certain conditions
Site-specific assessment necessary
Intra-cranial EEG-fMRI safety study results:Heating tests

Lemieux – ACES / Europe Dublin 2015
1) Use likely safest regime2) Strict protocol:
- 1.5T Siemens Avanto / head (quad.) Tx/Rx coil- 90cm cables with 10cm fold along scanner central Z xis- Foam insert designed for exact positioning
- Position EEG system and cables reproducibly- Low SAR sequences:
- T1 volume, gradient echo EPI [TE=40ms], B0 map- 3-4% of 3.2 W/Kg- max duration 10 minutes
3) Close monitoring and documenting of patient responses, images, appearance of brain surface, histology
icEEG-fMRI: Implementation

Lemieux – ACES / Europe Dublin 2015
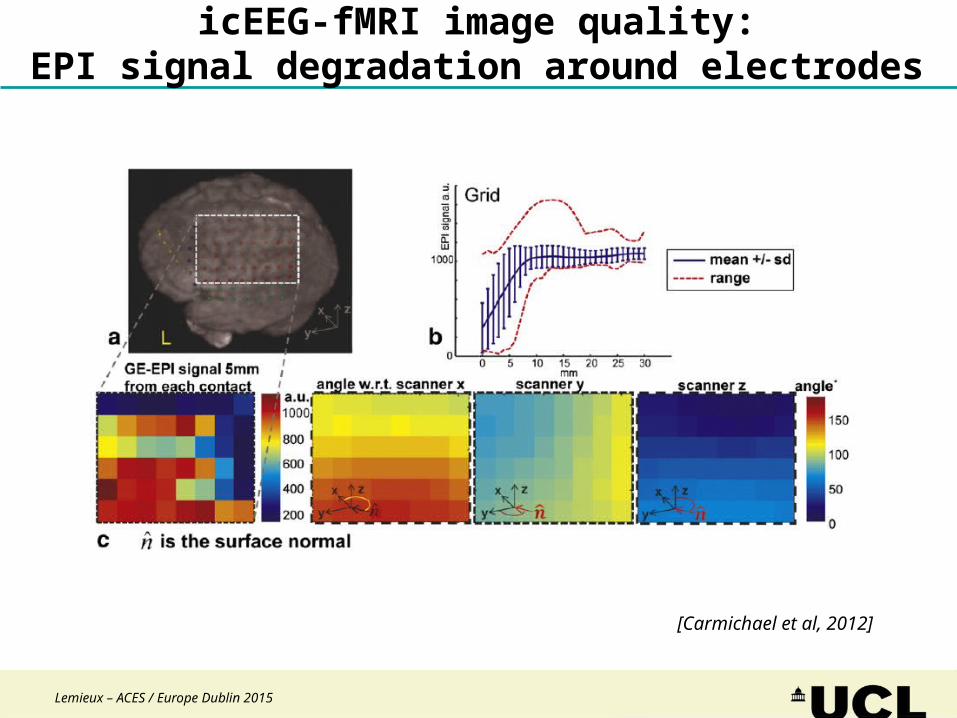
icEEG-fMRI image quality:EPI signal degradation around electrodes
[Carmichael et al, 2012]
Lemieux – ACES / Europe Dublin 2015
icEEG-fMRI image quality:EPI signal degradation around electrodes
[Carmichael et al, 2012]
Lemieux – ACES / Europe Dublin 2015
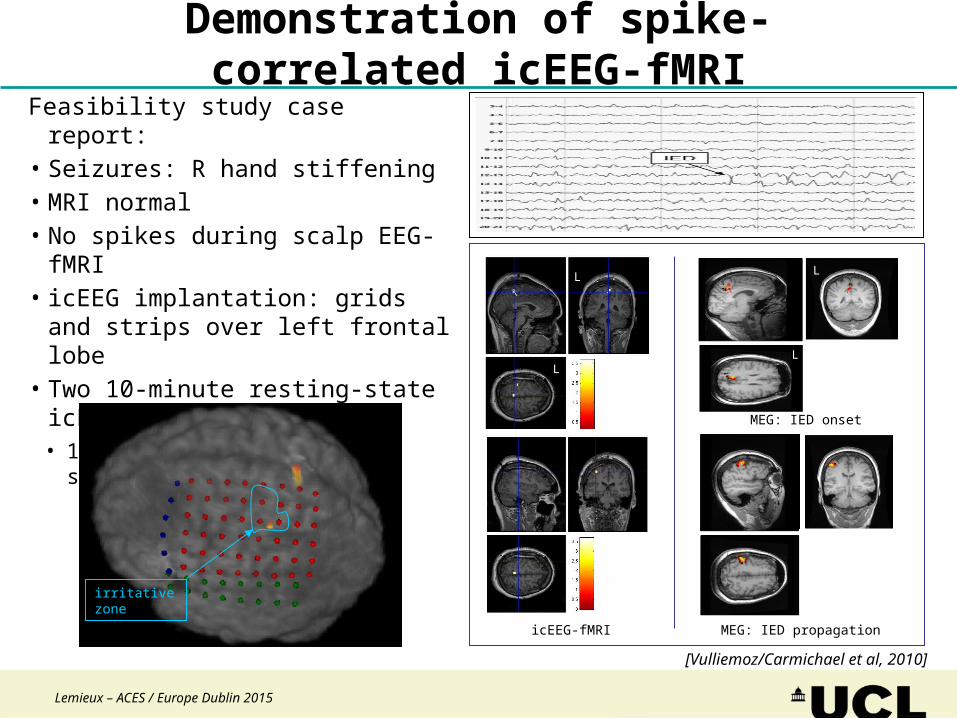
Feasibility study case report:• Seizures: R hand stiffening• MRI normal• No spikes during scalp EEG-fMRI• icEEG implantation: grids and strips over
left frontal lobe• Two 10-minute resting-state icEEG-fMRI
sessions:• 100’s of L fronto-central spikes
L
icEEG-fMRI
MEG: IED onset
L
L
MEG: IED propagation
L
L
irritative zone
Demonstration of spike-correlated icEEG-fMRI
[Vulliemoz/Carmichael et al, 2010]

Lemieux – ACES / Europe Dublin 2015
Conclusions
EEG-fMRI allows:• Haemodynamic mapping of events with specific EEG features• ‘Extends’ EEG: whole-brain coverage, source complexity-independent
Intracranial EEG-fMRI:• Fascinating, complex data• Exquisite electrophysiological sensitivity• Image data quality is an issue:
− Electrode composition is suboptimal for MR imaging− Clinical impact: Limits ability to locate the electrodes in relation to the
anatomy− Research impact: Reduces the amount of fMRI signal available for
analysis
Lemieux – ACES / Europe Dublin 2015
Team / collaborators / funding
David W. CarmichaelUmair ChaudharyAna-Carolina Coan (Campinas)Alessio De Ciantis (Firenze)Beate DiehlJohn S. DuncanMadeline GradeMarco LeiteAndrew McEvoyTeresa MurtaIrene PappalardoSuejen Perani (King’s)Sofia Markoula (Ioannina)Roman RodionovCatherine ScottNiraj SharmaRachel C. ThorntonAndré van GraanAnna Vaudano (Modena)Matthew C. WalkerBritta Wandschneider+ The Clinical Neurophysiology and
Neuroradiology teams at the National Hospital for Neurology and Neurosurgery, Queen Square
K Friston (UCL)M Guye / F Bartolomei / P Chauvel / JP Ranjeva (Marseille)S Vulliemoz / C Michel (Geneva)P Figueiredo (Lisbon)M Papadopoulou / D Marinazzo (Ghent)Radhakrishnan A / Chandrasekharan K / Sreedharan S (Trivandrum)R Quian Quiroga / C Pedreira (Leicester)V Kokkinos (Thessaloniki)S Meletti (Modena)F Cendes (Campinas)K Mullinger / R Bowtell (Nottingham)KR Muller / V Samek / D Blythe (Berlin)H Laufs (Frankfurt)J Daunizeau (Paris)K Whittingstall (Sherbrooke)E Formisano / F De Martino (Maastricht)M Torkmani Azar (Konya)
Funding:Action Medical ResearchBrain Research Trust / James Tudor FoundationNIHR (UK Department of Health)Medical Research CouncilSupport in kind:Brain Products
Thank you

Lemieux – ACES / Europe Dublin 2015
The problem of presurgical test validation• Validation of localisation tests in epilepsy is fundamentally limited• Gold standard is not golden:
• Surgical resection localisation and outcome data
• Ictiogenic ‘source’ must be considered a network in most patients a priori
• Elements of a possible solution• Improved characterisation / Modelling
• Functional connectivity networks
• Effective connectivity (“DCM”)
• Validation / Interventions:• Surgical: connection disruptions (functional connectivity sufficient?)
• More sophisticated: stimulation (effective connectivity necessary?)

Lemieux – ACES / Europe Dublin 2015
What else the EEG-fMRI can tell us?
Psychophysiologial interaction (PPI)
-0.8 -0.6 -0.4 -0.2 0 0.2 0.4 0.6 0.8-1.5
-1
-0.5
0
0.5
1
1.5
LFdl activity
LFp
resp
onse
Psychophysiologic Interaction
IED
seed ROI
Vaudano et al., 2013-Frontiers in Neurology
2. Connectivity analysis2. Connectivity analysis

Lemieux – ACES / Europe Dublin 2015
Interictal EEG
Intracranial EEG-fMRI:Incidental Studies of Other Brain
Phenomena in Humans

Lemieux – ACES / Europe Dublin 2015
EEG oscillations: their functional roles and brain state correlates
Classical EEG oscillation bands• Delta (0.5-3.5Hz):
– deep sleep, learning, motivational processes and reward system• Theta (4-7 Hz):
– working memory, emotional arousal and fear conditioning• Alpha (8-12 Hz):
– cortical operations during the awake resting-state in the absence of sensory inputs, disengagement of task-irrelevant brain areas, working memory and short-term-memory retention
– Rolandic Alpha / ‘Mu rhythm’ (9-11 Hz)• Suppressed during task
• Beta (13-30 Hz):– Vigilence and attention– Rolandic Beta
• Linked to motor functions• Inhibited by motor imagery
• Gamma (> 30 Hz):– feature integration, attention, etc
Lemieux – ACES / Europe Dublin 2015
Rolandic Alpha (‘Mu’) and Beta on Scalp EEG
• What are their respective roles?
• They fluctuate similarly but are not perfectly correlated
• Based on MEG, their spatial distributions seem to differ:
• Rolandic Alpha: post-central (primary somatosensory)
• Rolandic Beta: pre-central (primary motor)
• fMRI-based localisation?...

Lemieux – ACES / Europe Dublin 2015
fMRI of Rolandic Alpha and Beta on scalp EEG: Ritter et al, 2009
• Bilateral hand motor task• 15 healthy subjects• Two main fMRI models:
• Band/channel• Blind source separation
Beta – BOLD correlation:
Conclusions
Complex data quality correction and modelling methodology
BOLD of Rolandic alpha and beta rhythms differ: postcentral gyrus (SI) for alpha and precentral gyrus (MI) for beta;
Negative Rolandic alpha and beta rhythms - BOLD correlation in the pericentral cortex

Lemieux – ACES / Europe Dublin 2015
BOLD Mapping of Rolandic Alpha and Beta oscillations on ECoG
Tim
e
HRF
Band Averaging
(around peak)
0.5mV
M1
S1
8,9…
30Hz
M1
S1
Identification of patient-specific
band peak
Spatial PCA:1st PC
[Perani et al, in preparation]
Grid placed over left motor cortexicEEG-fMRI:
• Rest (epileptic activity mapping)• Alternating finger tapping task (no rest)
For each band: Alpha and Beta

Lemieux – ACES / Europe Dublin 2015
L
L
L
L
[Perani et al, in preparation]
BOLD Mapping of Rolandic Alpha and Beta on ECoG:Task data
BOLD increases
BOLD decreases BOLD decreases
BOLD increases
Alpha (Mu) Beta

Lemieux – ACES / Europe Dublin 2015
Intra-cranial EEG-fMRI of interictal spikesSummary BOLD maps across all IZ1 IED
[Chaudhary - submitted]
7 cases had concordant maps: better outcome (ILAE 1 & 3)
5 cases had discordant maps:worse outcome (ILAE 4 & 5; 5 cases)
Case # 3 (ILAE class 1)
Case # 13 (ILAE class 4)
SPM{F} contrast across all IZ1 IED-related effects
Summary measure for comparison:Relationship of BOLD clusters with the presumed, icEEG-derived EZ

Lemieux – ACES / Europe Dublin 2015
Conclusions (2)
• EEG-fMRI (+video) to have increased importance in neuroscience• Intracranial EEG-fMRI
• Analysis is complex: additional layer on top of icEEG analysis & interpretation• Abundance of activity -> more reliable maps than scalp EEG-fMRI• Interpretation: compare it against what?
• How precious is our ‘gold’ standard?• Surgical outcome + localisation of resected tissue: what about disruption of
wider networks?
• Effective connectivity: ‘the full multimodal generator model’ (DCM)• Improved biophysical models of epileptogenic networks being developed• Applicable to icEEG, then fMRI

Lemieux – ACES / Europe Dublin 2015
Seizure propagation in hypothalamic hamartomas (HH)
• Seizures originate in HH, and control of seizures can be achieved by surgically removing the HH.
• Possible surgical alternative: disconnection of the underlying pathway.
• Different seizure propagation pathways have been described in HH [Leal et al. Epilepsia 2003; Kahane et al. Epileptic Disord. 2003]:
• Aim: identify the correct seizure propagation pathway in individual patients using DCM.
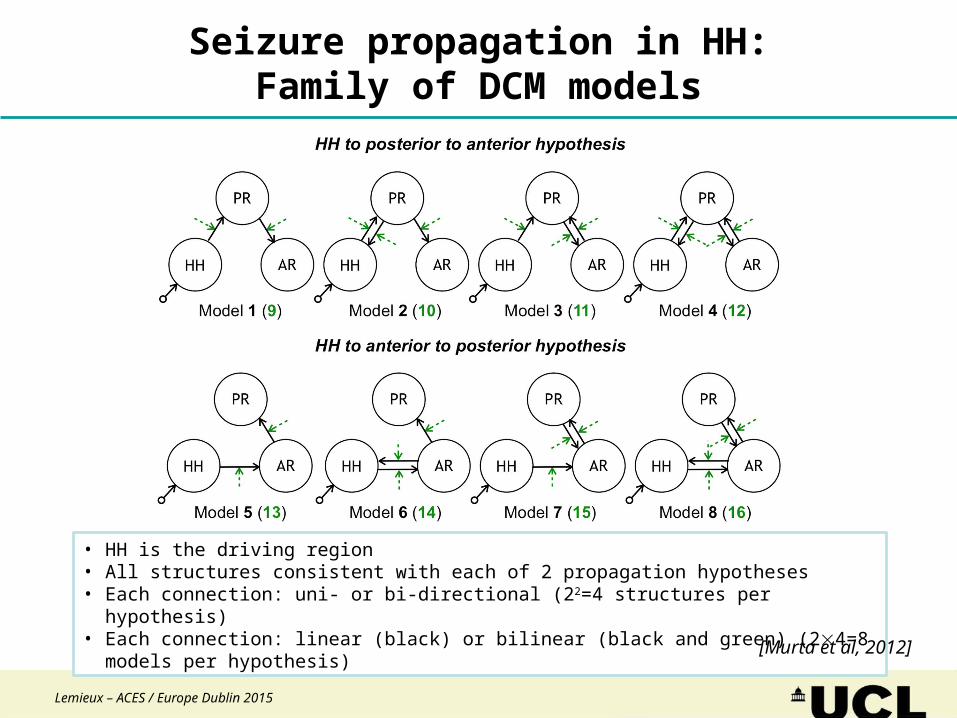
1.HH to temporal-occipital (posterior, PR) to frontal lobe (anterior, AR)
(through the fornix)
2.HH to frontal (anterior, AR) to temporal-occipital (posterior, PR) lobe
(through the mammillo-thalamo-cingulate pathway)
[Murta et al, 2012]
Lemieux – ACES / Europe Dublin 2015
Seizure propagation in HH:Family of DCM models
• HH is the driving region• All structures consistent with each of 2 propagation hypotheses• Each connection: uni- or bi-directional (22=4 structures per hypothesis)• Each connection: linear (black) or bilinear (black and green) (24=8 models per hypothesis)
[Murta et al, 2012]

Lemieux – ACES / Europe Dublin 2015
Seizure propagation in HH: Bayesian model comparison
[Murta et al, 2012]
Most likely model
Model 1:
HH → temp-occ. → frontal

Beyond mapping:Networks and causality(and a detour via IGE)

Lemieux – ACES / Europe Dublin 2015
• Multi-modal imaging = Combinations of images or maps– from different sources (instruments)
or– that show different aspects (e.g. MR contrasts)
• Fundamental assumption: measurements relate to the same phenomenon– Location– Time
Multi-modal imaging: basics
Lemieux – ACES / Europe Dublin 2015
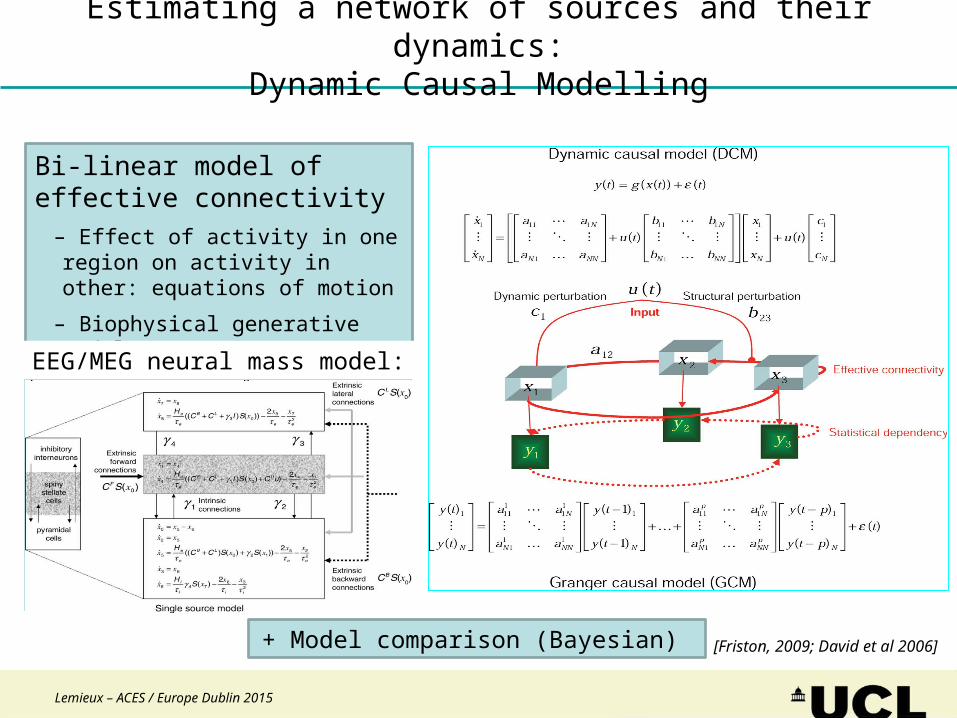
Estimating a network of sources and their dynamics:Dynamic Causal Modelling
[Friston, 2009; David et al 2006]
Bi-linear model of effective connectivity
– Effect of activity in one region on activity in other: equations of motion
– Biophysical generative model
fMRI:EEG/MEG neural mass model:
+ Model comparison (Bayesian)

Lemieux – ACES / Europe Dublin 2015
EEG fMRI of GSW - QS 1.5T seriesGroup analysis
IGE
N=18
Sup Post Par ↓
Front ↓
Post Cing ↓
Thalam ↑
[Hamandi et al., 2006]
Th
Th
Lemieux – ACES / Europe Dublin 2015
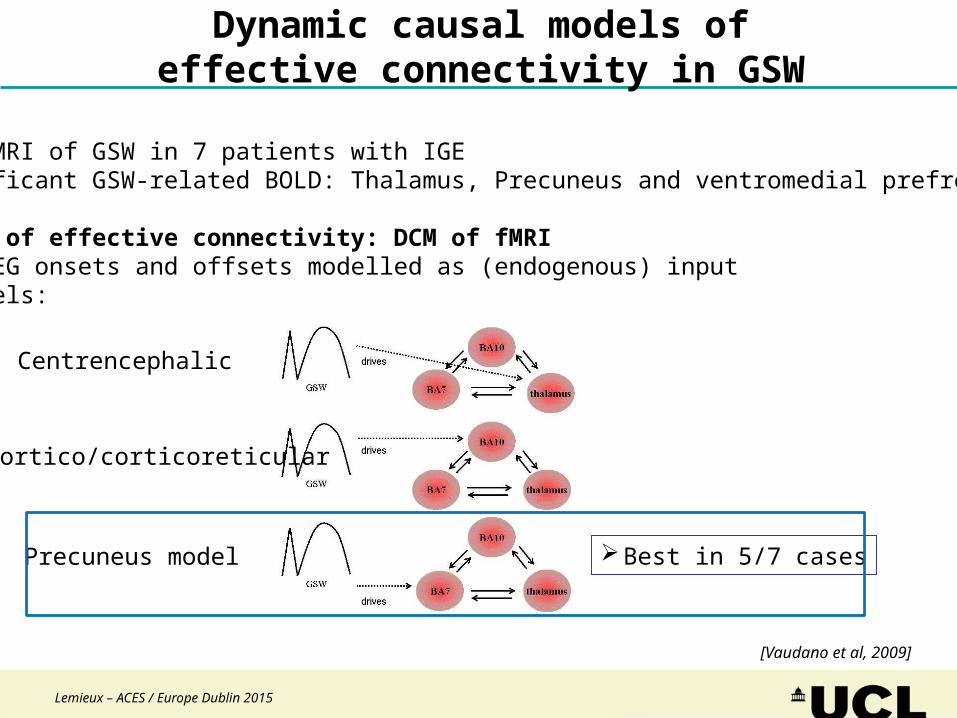
Dynamic causal models ofeffective connectivity in GSW
Centrencephalic
Cortico/corticoreticular
Precuneus model
[Vaudano et al, 2009]
Data:EEG-fMRI of GSW in 7 patients with IGESignificant GSW-related BOLD: Thalamus, Precuneus and ventromedial prefrontal
Model of effective connectivity: DCM of fMRIGSW EEG onsets and offsets modelled as (endogenous) input3 models:
Best in 5/7 cases

Lemieux – ACES / Europe Dublin 2015
Integrate and Fire Neurons
Mean Field Population Dynamics
DCM of focal seizuresA more realistic biophysical model of (fast) ictal activity
Time (s)
Freq
uenc
y (H
z)
5 10 15 20 25 30
8
16
32
64
128
Model: Coupled neural population dynamics
[M Leite, unpublished]

Lemieux – ACES / Europe Dublin 2015
+10mV
-70mV
E vs. I
Pyr Int
Cur
rent
(pA
)
Phase (%) Phase (%)
Phase (%) Phase (%)
Cur
rent
(pA
)C
urre
nt (
pA)
Current (pA) Current (pA)
Pyr Int
U
[M Leite; unpublished - In collaboration with D Kullmann and D Kuzmin]
A more realistic biophysical modelof (fast) ictal activity: Validation initial results

Lemieux – ACES / Europe Dublin 2015
Resting-state BOLD
BOLD increases
BOLD decreases BOLD decreases
BOLD increases
L
L
L
L
[Perani et al, in preparation]
Alpha (Mu) Beta