performances based financing scheme in rwanda investing more strategically 1
TRANSCRIPT
Performances Based Financing scheme in Rwanda
INVESTING MORE STRATEGICALLY
1
Outline of Presentation
Rwandan Context PBF scheme in Rwanda
PBF approach Implementation model and funds flows PBF funding in Rwanda
Some Achievements and Challenges
3
Background The performance-based funding (PBF) is one of the
pillars of health financing and strengthening the health system in Rwanda. This approach was introduced in order to strengthen the motivation of care providers and results (output) than traditional financing (for input) had not previously yielded

Historical
Started in 2002 as pilote by two NGOs in former Butare and Cyangugu provinces.
The MoH integreted the PBF in 2005 HSSPI and decided to implement PBF in the whole country’ health facilities.
The scaling up started in early 2006 with the second phase of decentralisation.
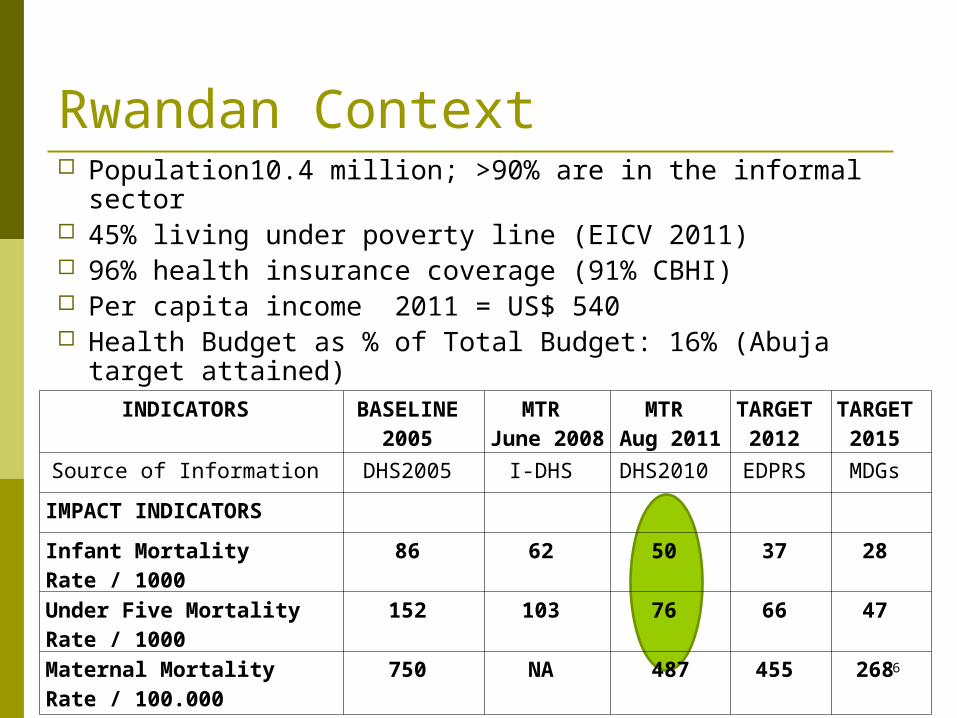
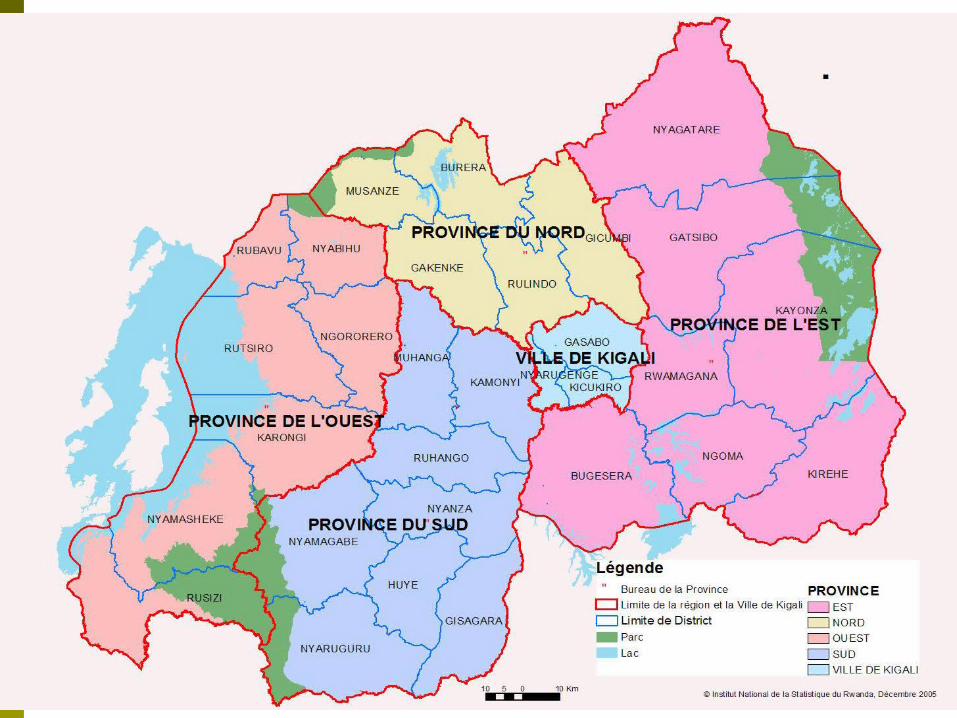
Rwandan Context Population10.4 million; >90% are in the informal sector 45% living under poverty line (EICV 2011) 96% health insurance coverage (91% CBHI) Per capita income 2011 = US$ 540 Health Budget as % of Total Budget: 16% (Abuja target
attained)
INDICATORS BASELINE 2005
MTR June 2008
MTR Aug 2011
TARGET 2012
TARGET 2015
Source of Information DHS2005 I-DHS DHS2010 EDPRS MDGs
IMPACT INDICATORS
Infant Mortality Rate / 1000 86 62 50 37 28
Under Five Mortality Rate / 1000 152 103 76 66 47
Maternal Mortality Rate / 100.000 750 NA 487 455 268 6
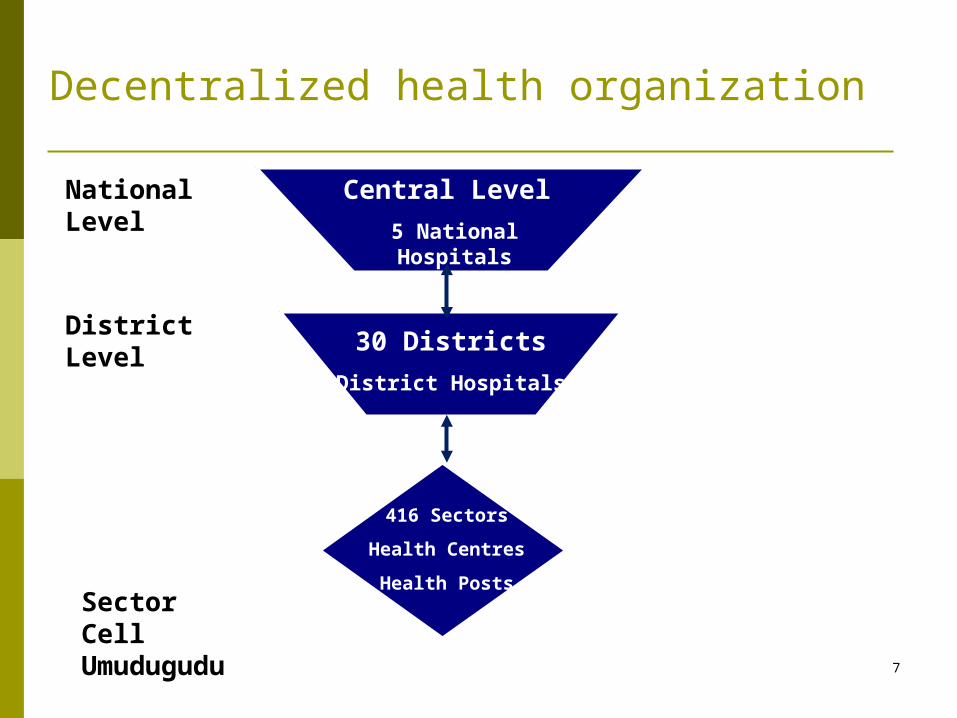
416 Sectors
Health Centres
Health Posts
30 Districts
District Hospitals
Central Level
5 National Hospitals
SectorCellUmudugudu
District Level
National Level
Decentralized health organization
7
Performance-Based FinancingValue for Money approach
Objectives:• Improve efficiency & rational use of health resources• Coverage of high impact interventions• Increase utilization of qualitative services care• Improve equity in resource allocation• Increase health worker motivation• Empower users of HF by giving them voice• Strengthen autonomy of health structures and build
capacity of managers
The national PBF model is composed of the following components: (1) PBF model for health centers; (2) PBF for district hospitals; and (3) Community PBF
8
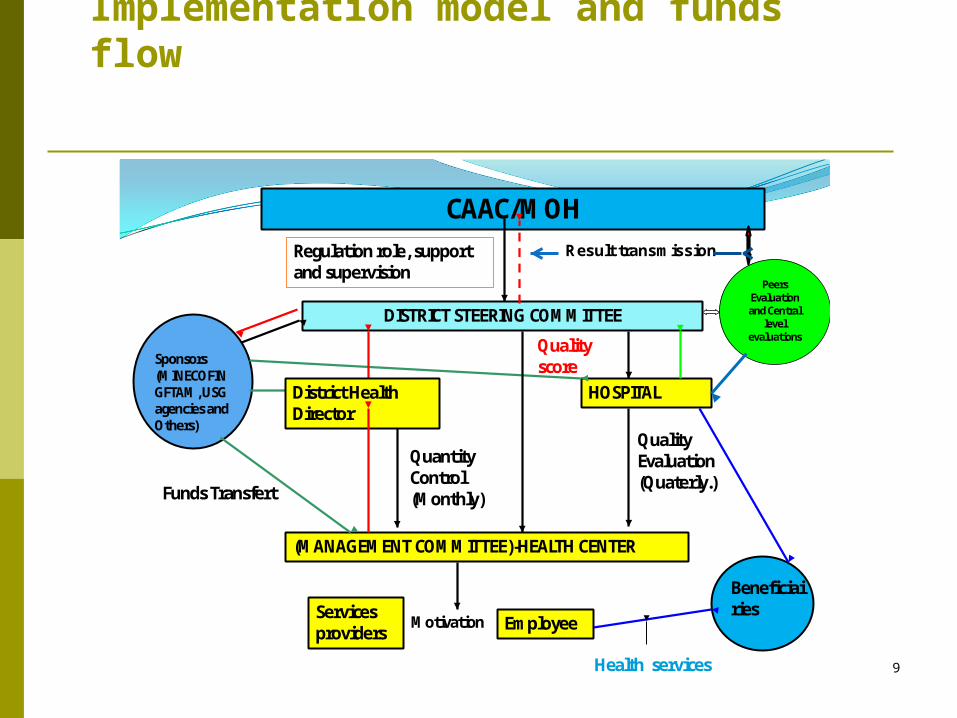
Implementation model and funds flow
CAAC/MOHRegulation role, support and supervision
DISTRICT STEERING COMMITTEE
HOSPITAL
Sponsors (MINECOFIN GFTAM, USG agencies and Others)
(MANAGEMENT COMMITTEE)-HEALTH CENTER
Services providers Employee
Quantity Control (Monthly)
Quality Evaluation (Quaterly.)
Motivation
Funds Transfert
Beneficiairies
Quality score
Health services
District Health Director
Result transmission
PeersEvaluation and Central
levelevaluations
9
INDICATORS ON MERGER DESEASES
1. HIV The SSF/HIV Grant is currently providing PBF funds to
Health Facilities (DHs and HCs) 18 indicators are paid (HIV/AIDS, TB/HIV, Reproductive
Health/HIV)
2. TB The PBF TB program has been scaled up at the national
level within 498 health facilities including 42 Districts Hospitals, 147 Health Center – Center of Diagnosis and Treatment “CDT”, 296 Health Center – Center of Treatment “CT”, 8 Prisons – CDT and 6 Prisons – CT
26 indicators are paid 10
Progress of implementation
CAAC submit the quarterly progress report Data verification and counter verification mechanism in
place Payment verification mechanism in place Integration with other health financing initiatives (CBHI) Payment made
11
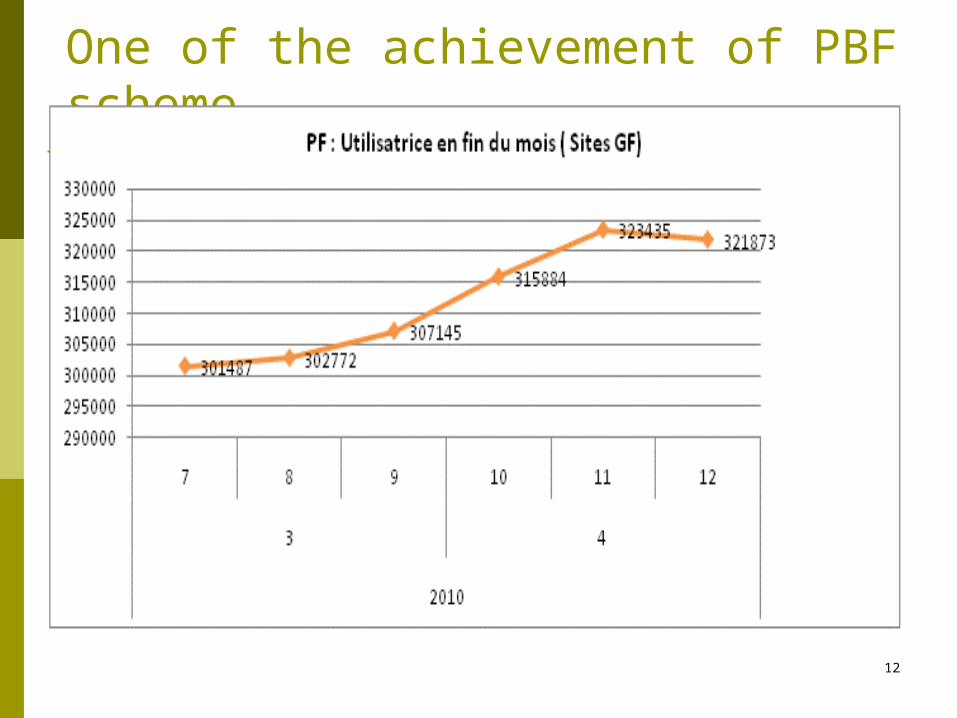
One of the achievement of PBF scheme
12

ONE OF THE RESULT: Trend of prenatal care quality between treatment and control facilities (2006-2008).
-0.10
0
-0.13
0.15
-0.15
-0.10
-0.05
0.00
0.05
0.10
0.15
0.20
Baseline (2006) Follow up (2008)
Stan
dard
ized
Pre
nata
l eff
ort s
core
Control facilities Treatment (PBF facilities)
15 % Standard deviation increase due to PBF
13
Impact of PBF
Two years into the national roll-out, the over-all performance of health facilities showed significant increase. As of 3rd quarter 2010, quality score of district hospitals in the country is 72.2% (range 33%-96%) (MSH, 2011).
A rigorous impact evaluation of the health centre PBF found positive effect on HIV, MCH and TB outcomes. Institutional delivery increased over-all but 7% more in PBF facilities between 2006-2008. PBF has increased prenatal care quality significantly (SPH/WB, 2010)
Individual VCT for HIV has significantly increased but more so for married couple VCT
14
Successful role-out of performance based financing (PBF) Careful phased approach Purchase of verified quality services Increased discretionary resources for health facilities Improved motivation of staff (financial incentives and equalization
of revenues) Strengthened quality assurance mechanisms (supervision and
verification) Clarified supervision, evaluation and "coaching" (peer-review)
The Rwandan example shows foremost the synergies of a number of reforms, i.e. difficult to attribute the percentages of success to each and every one of these reforms 15
Challenges for PBF Clarify role in long term vision and strengthen links with
demand side financing mechanisms Maintain momentum and improve assessment process Sustainability of PBF from Partners in this global
financial crisis and economic downtown Need to continuously revise indicators and increase the
PBF award to buy results Need to promote equity in PBF awarding
16
Thank you for your attention
17