perforated peptic ulcers - department of surgery at · pdf fileng ek, lam yh, sung jj, et al....
TRANSCRIPT
Perforated peptic ulcers
Dr V. Roudnitsky
KCH
downstatesurgery.org
Peptic ulcer disease
• Peptic ulcers are focal defects in the gastric or duodenal mucosa that extend into the submucosa or deeper
• Caused by an imbalance between mucosal defenses and acid/peptic injury
• The costs of PUD, including lost work time and productivity, are estimated to be above $8 billion per year in the United States
• In the United States with a prevalence of about 2%, and a lifetime cumulative prevalence of about 10%, peaking around age 70 years
downstatesurgery.org

downstatesurgery.org
Helicobacter Pylori
• 50% of the world's population is infected with H. pylori• Only 10 to 15% of patients colonized with H. pylori will
develop PUD over their lifetime• HP possesses the enzyme urease:
– converts urea into ammonia and bicarbonate• The Bicarbonate buffers the acid secreted by the stomach. • The ammonia is damaging to the SECs
• Inhibitory effect on antral D cells that secrete somatostatin– No inhibition of antral G-cell gastrin production
• Local alkalinization of the antrum (antral acidification is the most potent antagonist to antral gastrin secretion)
• The end result is hypergastrinemia and acid hypersecretion
downstatesurgery.org

downstatesurgery.org
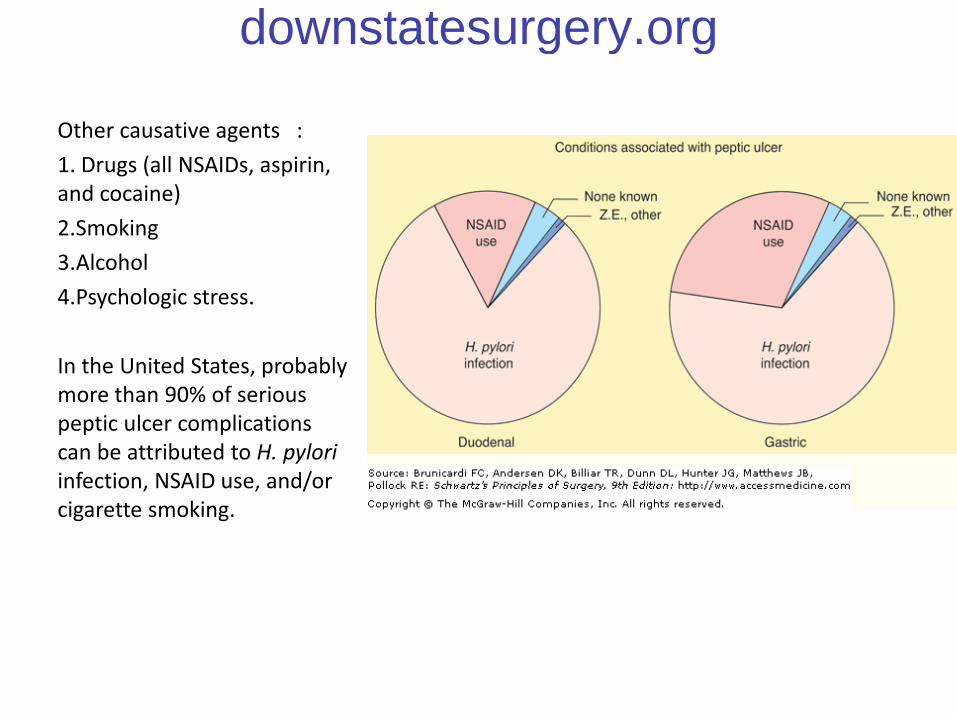
Other causative agents :
1. Drugs (all NSAIDs, aspirin, and cocaine)
2.Smoking
3.Alcohol
4.Psychologic stress.
In the United States, probably more than 90% of serious peptic ulcer complications can be attributed to H. pyloriinfection, NSAID use, and/or cigarette smoking.
downstatesurgery.org
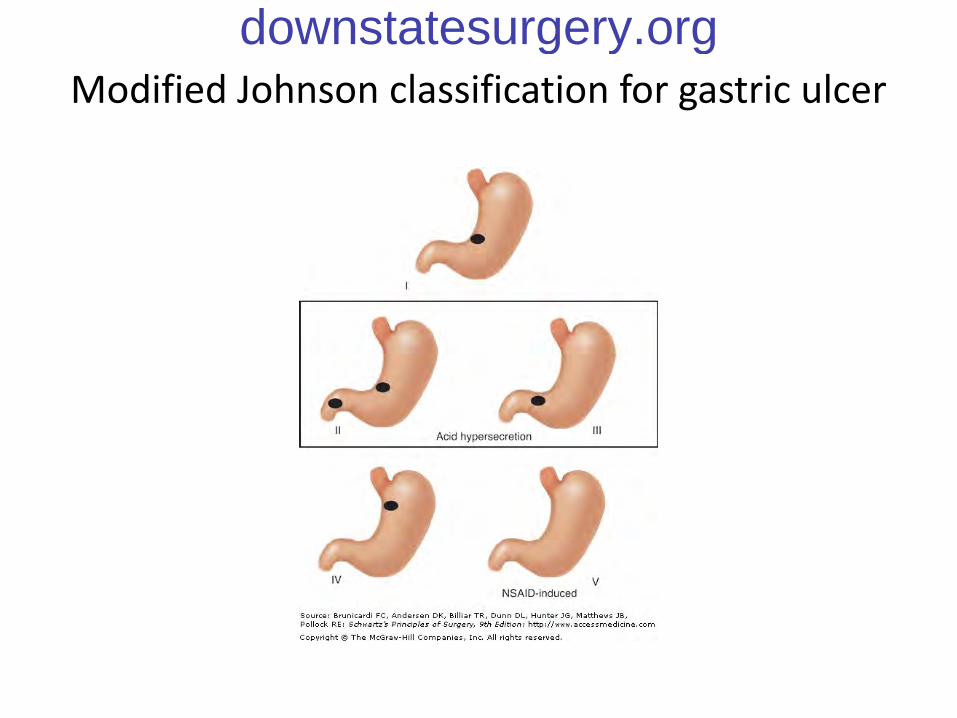
Modified Johnson classification for gastric ulcerdownstatesurgery.org
The incidence of emergency surgery and the death rate associated with
peptic ulcers has not changed significantly for last few decades
downstatesurgery.org
SURGICAL COMPLICATIONS OF PEPTICULCER DISEASE
• Perforation
• Bleeding
• Gastric Outlet Obstruction
• Intractable disease
downstatesurgery.org
SURGICAL COMPLICATIONS OF PEPTICULCER DISEASE : PERFORATION
• Acute perforations of the duodenum are estimated to occur in 2% to 10% of patients with ulcers
• Surgery almost always indicated
• Conservative management should considered in patients who do not have :
– generalized peritonitis
– hemodynamic instability
– free peritoneal perforation on a Gastrografin upper gastrointestinal study
downstatesurgery.org

SURGICAL COMPLICATIONS OF PEPTICULCER DISEASE : PERFORATION
• Conservative management– serial physical and laboratory examinations – nasogastric suction– intravenous acid secretion suppression– intravenous broad-spectrum antibiotics
• In any time during conservative management the patient deteriorates, an operation is indicated
• Retrospective and prospective, randomized studies suggest that conservative management is effective in properly selected patients
downstatesurgery.org

Crofts TJ, Park KG, Steele RJ, et al. A randomized trial of nonoperative treatment for perforated peptic ulcer. New Eng J Med 1989;320:970–973
Berne TV, Donovan AJ. Nonoperative treatment of perforated duodenal ulcer. Arch Surg 1989;124:830–832
Keane TE, Dillon B, Afdhal HH, et al. Conservative management of peforatedduodenal ulcer. Br J Surg 1988;75:583–584
Donovan AJ, Berne TV, Donovan JA. Perforated duodenal ulcer: An alternative therapeutic plan. Arch Surg 1998;133:1166–1171
Marshall C, Ramaswamy P, Bergin FG, et al. Evaluation of a protocol for the nonoperative management of perforated peptic ulcer. Br J Surg 1999;86:131–134
downstatesurgery.org

SURGICAL COMPLICATIONS OF PEPTICULCER DISEASE : PERFORATION
• Appropriate surgical management of perforated ulcers remained controversial :– Simple patch ( laparoscopic or open) vs antiulcer
operation???
downstatesurgery.org

Cellan-Jones(1929) /Graham Patch(1937)
downstatesurgery.org
Comparison Between Open and Laparoscopic Repairof Perforated Peptic Ulcer Disease
World J Surg (2008) 32:2371–2374
• Prospective , non randomized study• August 2006-2007, 33 patient included, single institution• Laparoscopic patch 19, open Patch 14• The primary end points :
– total operative time– nasogastric tube utilisation– intravenous fluid requirement– total time of urinary catheter and abdominal drainage usage– return to normal diet– intravenous/intramuscular opiate– time to full mobilization– total in-patient hospital– stay.
downstatesurgery.org
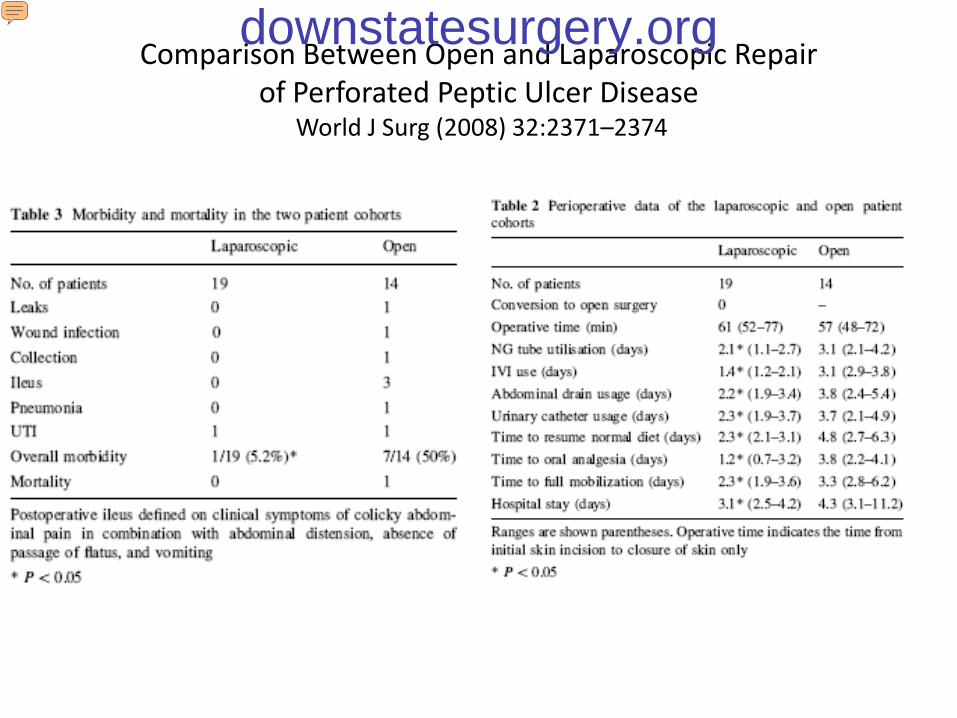
Comparison Between Open and Laparoscopic Repairof Perforated Peptic Ulcer Disease
World J Surg (2008) 32:2371–2374
downstatesurgery.org
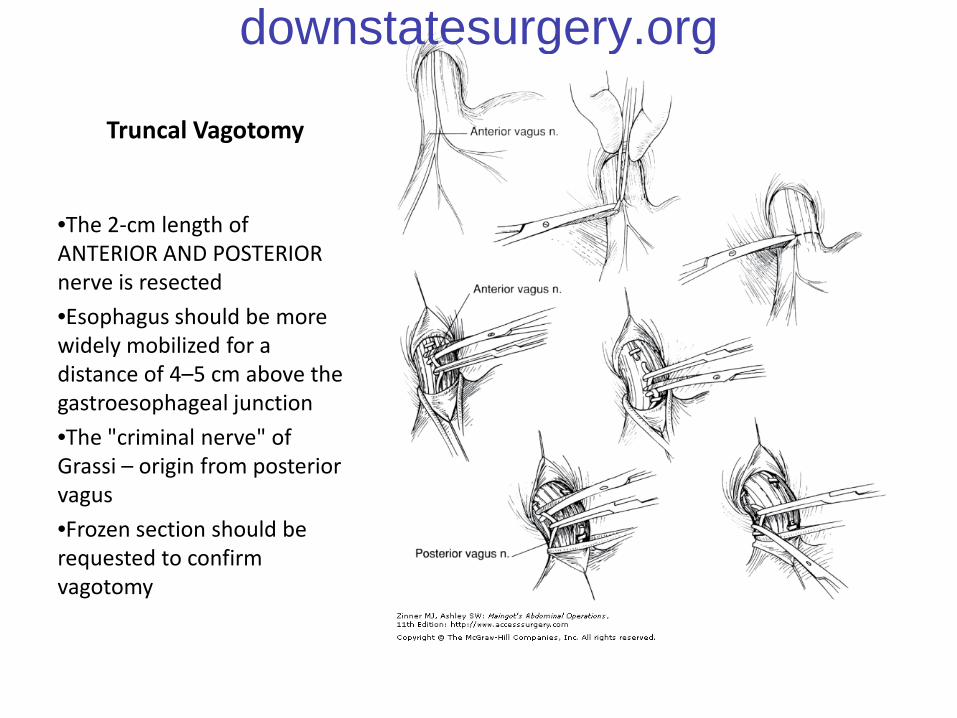
Truncal Vagotomy
•The 2-cm length of ANTERIOR AND POSTERIOR nerve is resected
•Esophagus should be more widely mobilized for a distance of 4–5 cm above the gastroesophageal junction
•The "criminal nerve" of Grassi – origin from posterior vagus
•Frozen section should be requested to confirm vagotomy
downstatesurgery.org

Selective Vagotomy
Preserve:
•posteriorly derived vagalbranch that innervates the small intestine and pancreas
•anteriorly derived vagalbranch that supplies the gallbladder and liver
•involves interruption of both nerves of Latarget and therefore does not avoid the need for a drainage procedure
downstatesurgery.org
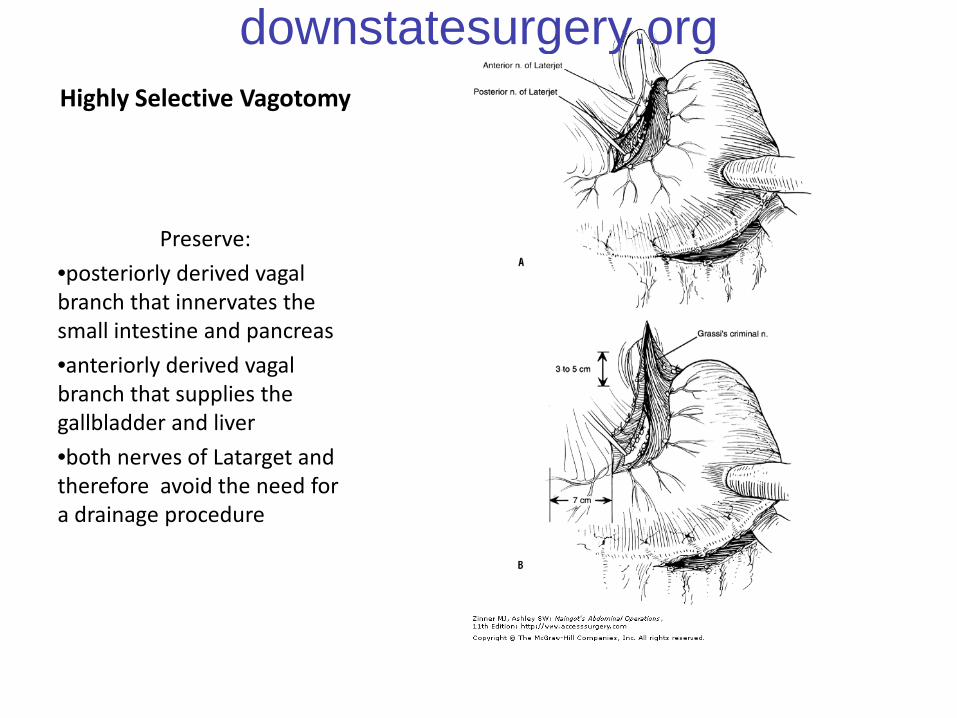
Highly Selective Vagotomy
Preserve:
•posteriorly derived vagalbranch that innervates the small intestine and pancreas
•anteriorly derived vagalbranch that supplies the gallbladder and liver
•both nerves of Latarget and therefore avoid the need for a drainage procedure
downstatesurgery.org
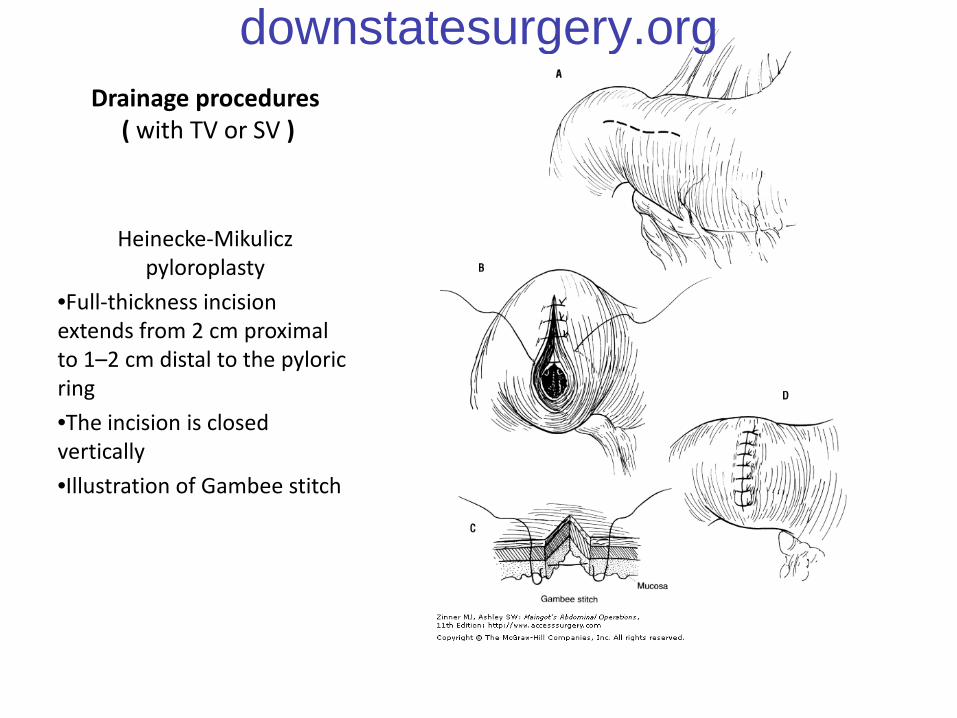
Drainage procedures( with TV or SV )
Heinecke-Mikuliczpyloroplasty
•Full-thickness incision extends from 2 cm proximal to 1–2 cm distal to the pyloric ring
•The incision is closed vertically
•Illustration of Gambee stitch
downstatesurgery.org

Drainage procedures
Finney U-shaped pyloroplasty
•The inverted U-shaped incision into the lumens of the stomach and duodenum
•Suture of the posterior septum of the stomach and duodenum
•The first anterior tier of sutures (Connell) is placed
downstatesurgery.org
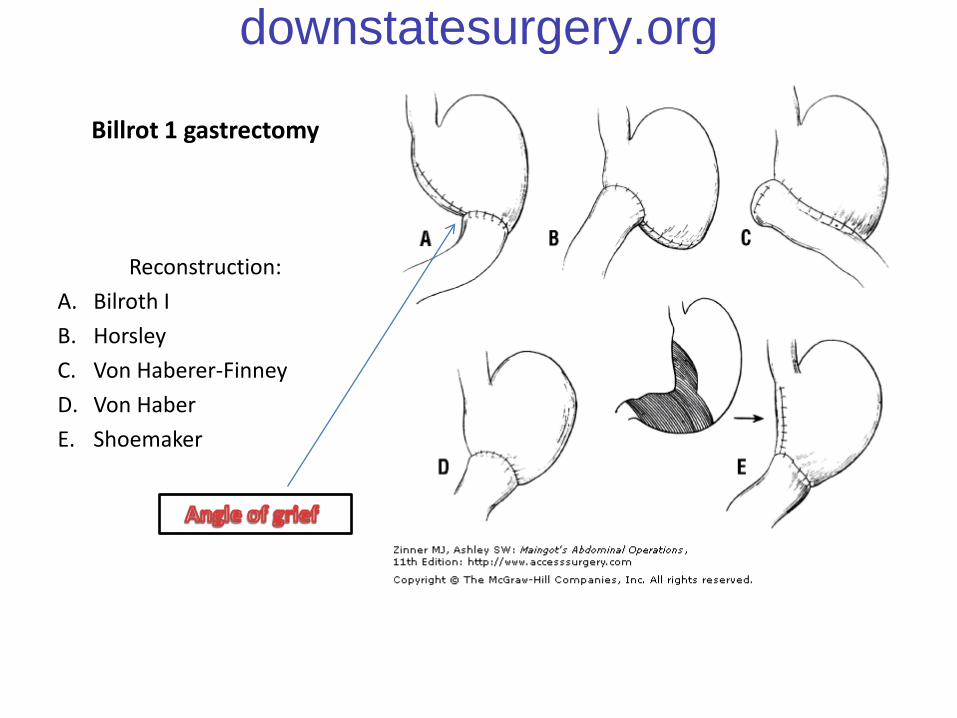
Billrot 1 gastrectomy
Reconstruction:
A. Bilroth I
B. Horsley
C. Von Haberer-Finney
D. Von Haber
E. Shoemaker
downstatesurgery.org
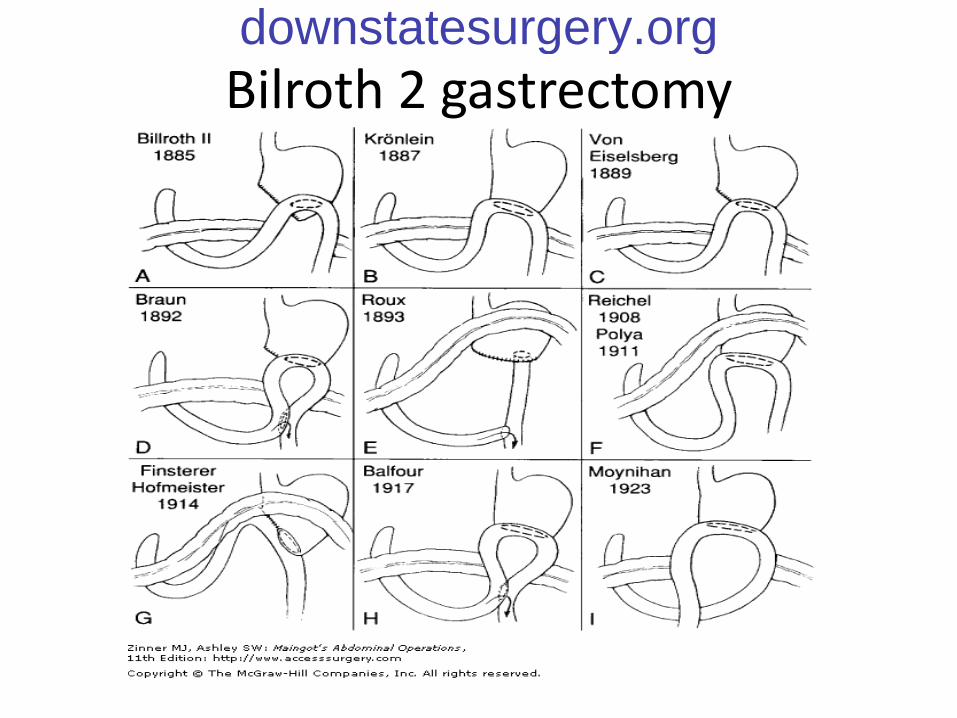
Bilroth 2 gastrectomydownstatesurgery.org
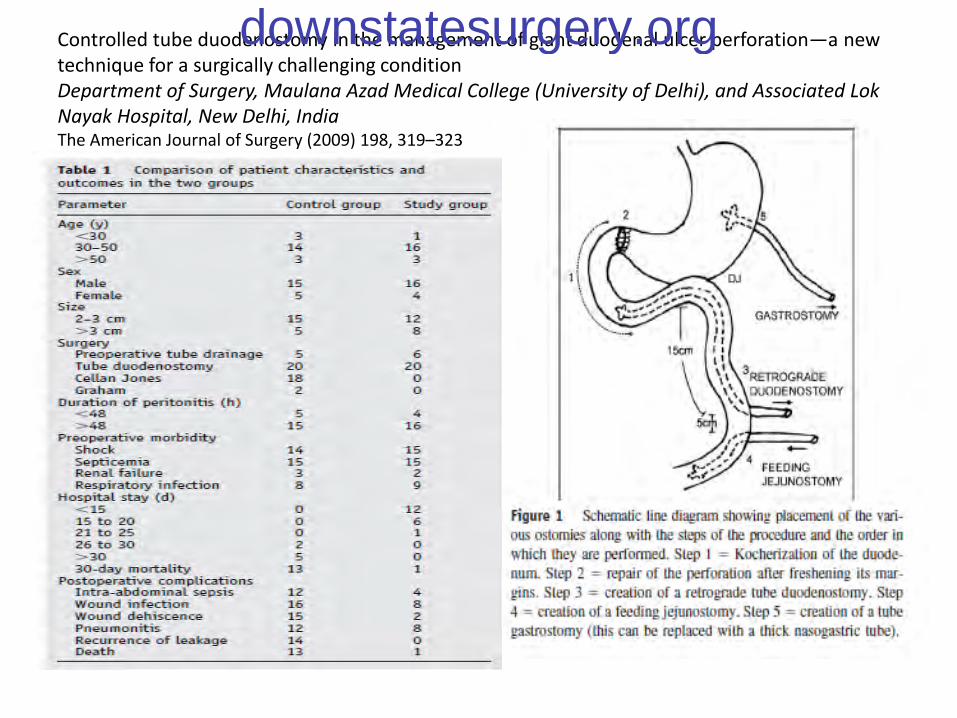
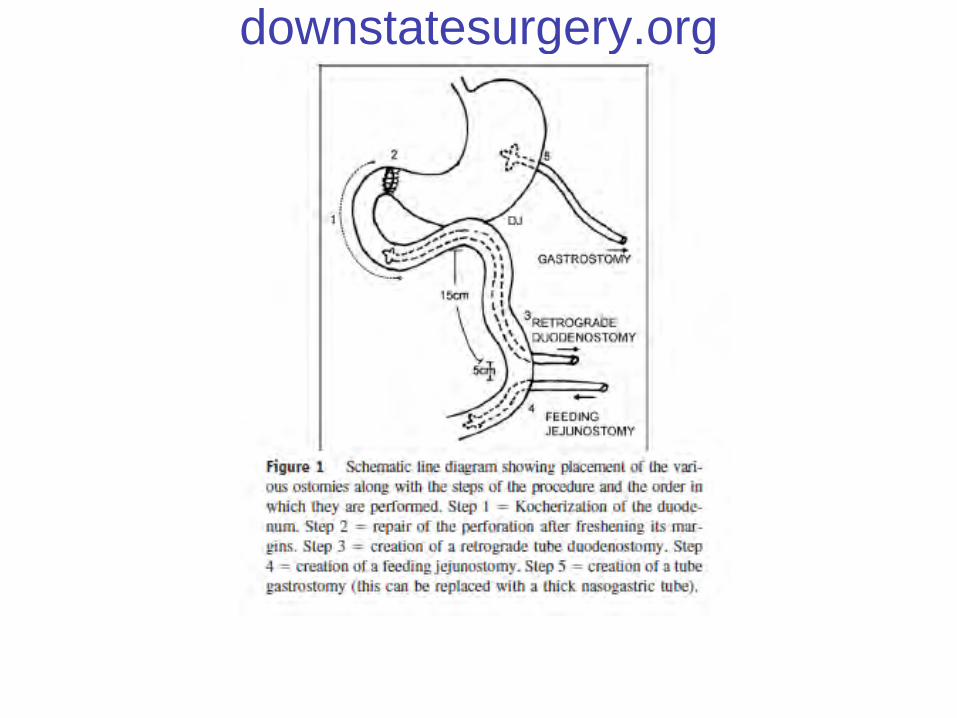
Controlled tube duodenostomy in the management of giant duodenal ulcer perforation—a new technique for a surgically challenging conditionDepartment of Surgery, Maulana Azad Medical College (University of Delhi), and Associated LokNayak Hospital, New Delhi, IndiaThe American Journal of Surgery (2009) 198, 319–323
downstatesurgery.org
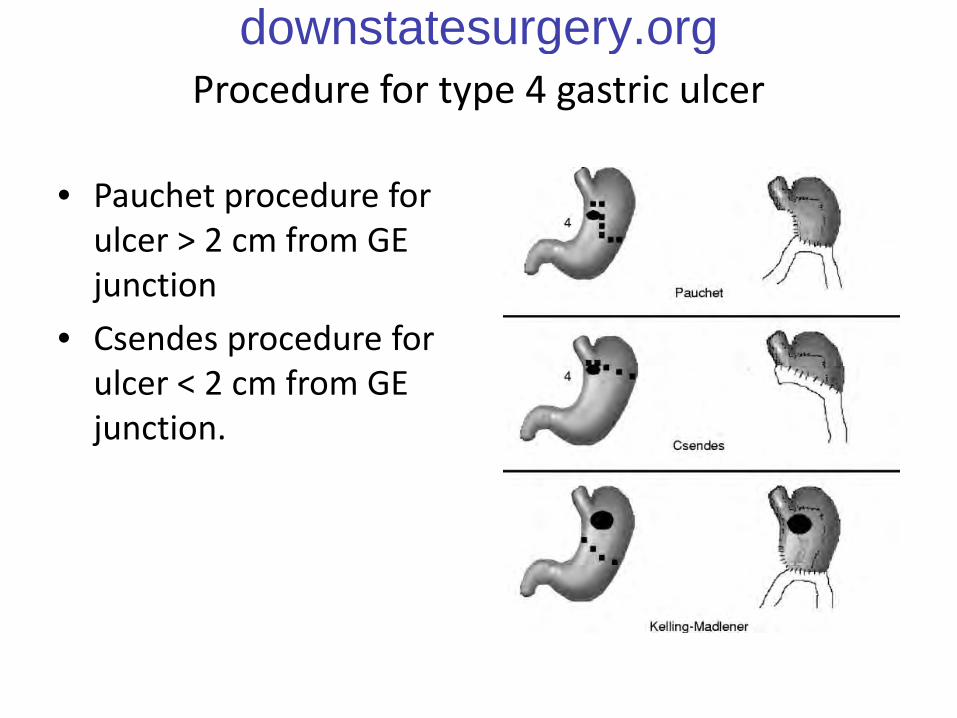
Procedure for type 4 gastric ulcer
• Pauchet procedure for ulcer > 2 cm from GE junction
• Csendes procedure for ulcer < 2 cm from GE junction.
downstatesurgery.org

downstatesurgery.org
downstatesurgery.org
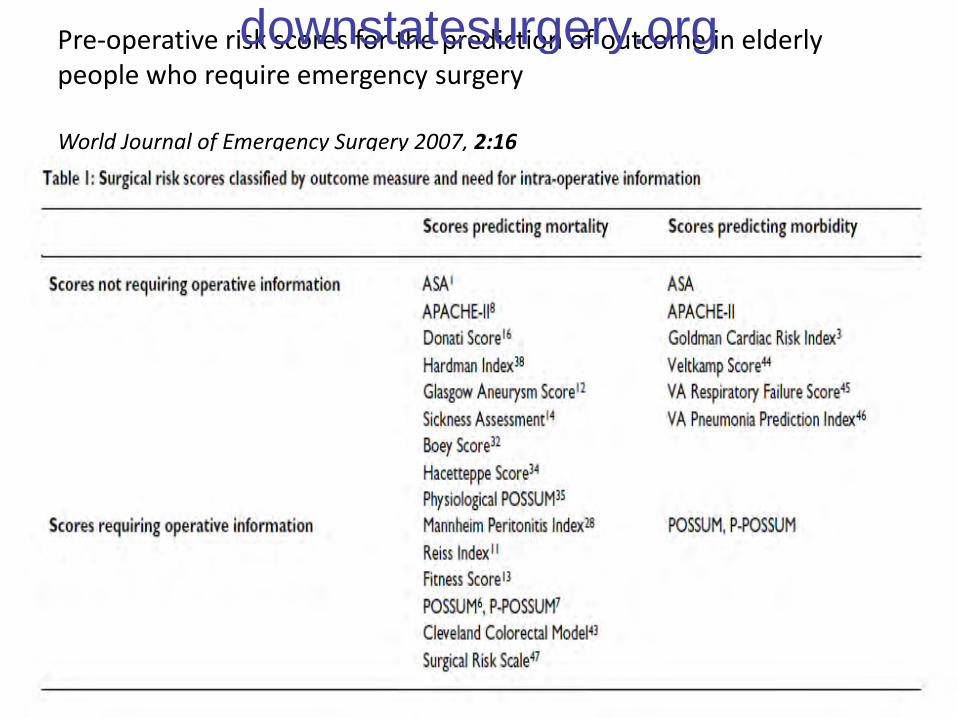
Pre-operative risk scores for the prediction of outcome in elderlypeople who require emergency surgery
World Journal of Emergency Surgery 2007, 2:16
downstatesurgery.org
downstatesurgery.org

Ng EK, Lam YH, Sung JJ, et al. Eradication of Helicobacter pylori prevents recurrenceof ulcer after simple closure of duodenal ulcer perforation. Ann Surg.
2000;231:153-158.
• 129 patients with perforated DU• 104(81%) with positive HP• Surgery – simple patch• Randomization:
– HP therapy + PPI– PPI therapy alone
• 1 Year endoscopic evaluation for recurrent ulcer:– HP therapy group – 5% of recurrent ulcer– PPI group – 38%
downstatesurgery.org

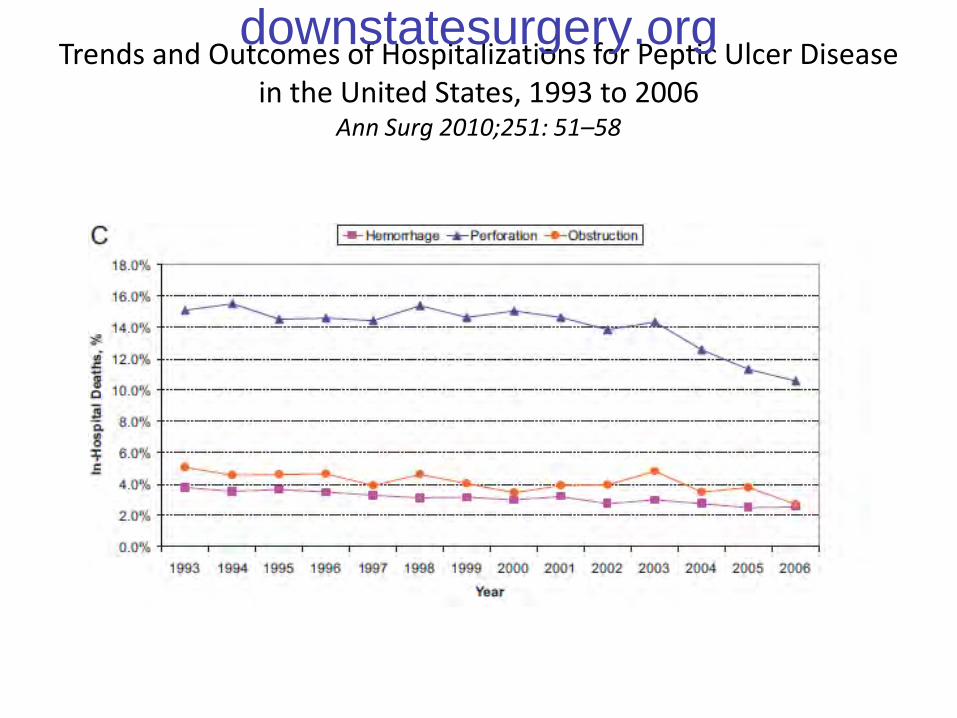
Trends and Outcomes of Hospitalizations for Peptic Ulcer Diseasein the United States, 1993 to 2006
Ann Surg 2010;251: 51–58
downstatesurgery.org
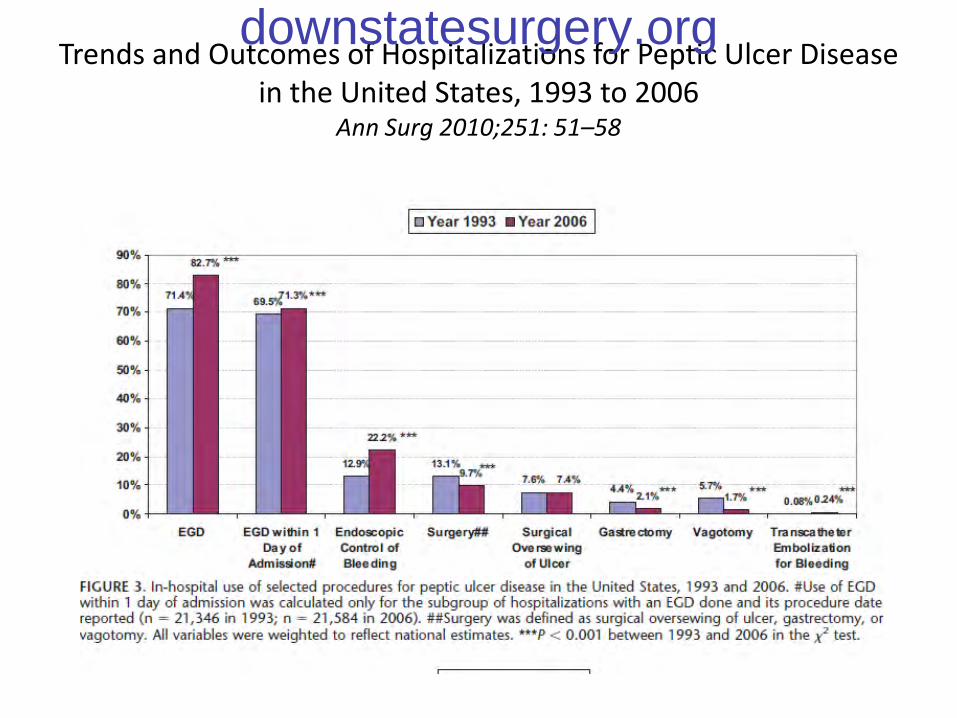
Trends and Outcomes of Hospitalizations for Peptic Ulcer Diseasein the United States, 1993 to 2006
Ann Surg 2010;251: 51–58
downstatesurgery.org
Trends and Outcomes of Hospitalizations for Peptic Ulcer Diseasein the United States, 1993 to 2006
Ann Surg 2010;251: 51–58
downstatesurgery.org

Emerging Trends in Peptic Ulcer Disease andDamage Control Surgery in the H. pylori Era
From the Department of Surgery, Harbor-UCLA Medical Center, Torrance, CaliforniaTHE AMERICAN SURGEON September 2005
downstatesurgery.org
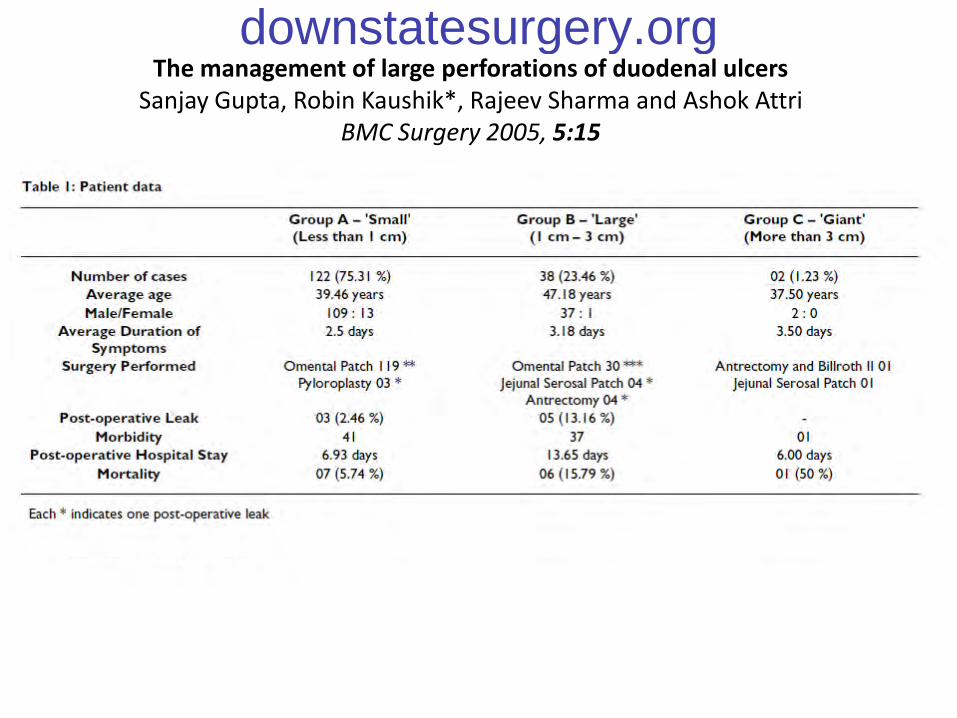
The management of large perforations of duodenal ulcersSanjay Gupta, Robin Kaushik*, Rajeev Sharma and Ashok Attri
BMC Surgery 2005, 5:15
downstatesurgery.org
downstatesurgery.org

Who is the Patient with PUD perforation who needs antiulcer surgery in 21 century?
• Failure of medical treatment ?
• Need for long term steroids or NSAIDs?
• Smokers /EtOH?
• Non compliant patients?
• Prepyloric and pyloric channel perforation?
downstatesurgery.org
Did HP treatment +PPI have been replaced antiulcer surgery???
downstatesurgery.org