pediatrics in the red rocks 2015 - azaap · ... t 4 (free)(free) high ( ) low ( ) ... adapted...
TRANSCRIPT

Endocrine cases
Cindy Chin, MD
Pediatrics in the Red Rocks 2015

Objectives
1. Interpret thyroid function tests.
2. Identify growth curves worrisome for endocrine causes of short stature.
3. Define what constitutes precocious and delayed puberty.
4. Discuss endocrine workup for obesity

Outline
• Thyroid
• Growth
• Puberty
• Obesity

Thyroid
• Hypothalamic-pituitary-thyroid axis
• Thyroid labs
• Thyroid lab interpretation
• Treatment
• Summary
• Cases

https://embryology.med.unsw.edu.au/embryology/images/1/1f/HPT_axis.jpg

• TSH: Marker of thyroid function
https://embryology.med.unsw.edu.au/embryology/images/1/1f/HPT_axis.jpg

http://fce-study.netdna-ssl.com/images/upload-flashcards/914084/572135_m.jpg
Various metabolic effects
Protein synthesis
mRNA
DNA
T4
I
T3
T4 T3
TBG
Blood Tissue Target cell
Total T4 versus Free T4

http://us.bestpractice.bmj.com/best-practice/monograph/1121.html
Factors that affect TBG affect Total T4, Total T3

T4 metabolism T3 + reverse T3
T4
T3 reverse T3
T2
(active) (inactive)

Thyroid lab interpretation
http://www.thyroid.org/blood-test-for-thyroid/
(free) T4 (free) High () Low () Low ()
Hyperthyroidism () Hypothyroidism () Primary
Hypothyroidism () Secondary
Low () / nL
Normal
Normal
TSH
CONDITION: Normal
Low () High ()

Adapted from http://www.thyroid.org/blood-test-for-thyroid/
T4 (free) Normal Normal
Hypothyroidism () Subclinical
Normal
Hyperthyroidism () Subclinical
Normal
TSH
CONDITION: Normal
Low () High ()
Thyroid lab interpretation
Treatment: Hypothyroidism
• Levothyroxine (LT4)
– Administration
• Tablet only – Crushed, mixed with a little milk/water
– Take from spoon (± syringe)
• Avoid calcium, iron, soy, and fiber
• Time of day: ? (Some think it is stimulating)
Hypothyroidism: Treatment
• Levothyroxine (LT4) – Dosing
• Newborn: 10-15 μg/kg/day
• 6-12 mo: 6-8 μg/kg/day
• 1-5 yo: 4-6 μg/kg/day
• 6-12 yo: 3-5 μg/kg/day
• 12 yo-adult: 2-4 μg/kg/day
• adult: average 1.75 μg/kg/day
Adjust dose based on biochemical and clinical response.
Too much, too quickly can adversely affect final adult height. • Hypothyroidism: Delayed bone age
• Excessive treatment Bone age advancement > Height catch-up

Hypothyroidism: Treatment
T4 T3
Human production ~ 10 1
Levothyroxine 100%
Liothyronine (Cytomel) 100%
Liotrix (Thyrolar) 4 1
Desiccated thyroid extract - Beef, pork (Armour, Westhroid, Nature-throid)
~ 4 1
Hyperthyroidism: Treatment
• Anti-thyroid drug (ATD)
– Methimazole: 0.5-1 mg/kg/day (daily or BID)
• MOA: Inhibit thyroid hormone synthesis (mainly on TPO)
– Propylthiouracil: 5-10 mg/kg/day (TID)
• Black box warning: Liver toxicity
• MOA: Inhibit thyroid hormone synthesis (mainly on TPO), Inhibit peripheral T4 T3

Hyperthyroidism: Treatment
• β blocker
– For CV, neuromuscular overactivity
– Stop when euthyroid
– Atenolol: 25-50 mg po daily
– Propanolol: 20 mg BID-QID
• Inhibit peripheral T4 T3
• Do not use in asthma patients

Thyroid: Summary
• Primary method to evaluate thyroid function – TSH, free T4 (± T3 in hyperthyroidism)
• Interpretation of lab results – Free T4 Normal, subclinical, hypo-/hyper-thyroid
– TSH The cause (1° vs. 2°)
• 1st line therapy – Hypothyroidism: Levothyroxine
– Hyperthyroidism: Methimazole

Thyroid: Case 1
TSH (0.5-5.4)
Free T4
(0.9-1.6) Total T4
(4.5-12.5)
44.63 0.7 4.7
Decide if labs are:
– Normal
– Hypothyroidism: 1° versus 2°
– Hyperthyroidism
– Subclinical: Hypothyroidism versus Hyperthyroidism

Thyroid: Case 2
TSH (0.45-4.5)
Free T4
(0.93-1.6) Total T4
(4.5-12)
Initial 0.4 0.84 6.1
6 mo later 0.271 0.92 6.7
7 mo later 0.478 0.9 5.9
Decide if labs are:
– Normal
– Hypothyroidism: 1° versus 2°
– Hyperthyroidism
– Subclinical: Hypothyroidism versus Hyperthyroidism

Thyroid: Case 3
TSH (0.72-11)
Free T4
(0.83-3.09)
4 weeks old 11.59 1.5
6 weeks old 18.71 1.58
8 weeks old 20.16 1.34
Decide if labs are:
– Normal
– Hypothyroidism: 1° versus 2°
– Hyperthyroidism
– Subclinical: Hypothyroidism versus Hyperthyroidism

Thyroid: Case 4
TSH (0.45-4.5)
Total T4
(4.5-12) Total T3
(71-180)
< 0.006 19.8 619
Decide if labs are:
– Normal
– Hypothyroidism: 1° versus 2°
– Hyperthyroidism
– Subclinical: Hypothyroidism versus Hyperthyroidism

Thyroid: Case 5
TSH (0.45-4.5)
Free T4
(0.8-1.7)
1.11 1.2
Decide if labs are:
– Normal
– Hypothyroidism: 1° versus 2°
– Hyperthyroidism
– Subclinical: Hypothyroidism versus Hyperthyroidism

Growth: Case 1
• 11 yo M: Concern for short stature

Short stature
• Birth history
• Skeletal maturation/potential
• Habits/other history
• Growth pattern
• Suspected endocrinopathy

Short stature
• Birth history
– Pregnancy complications
– Birth
• Anthropometrics: Length, weight
• Prematurity
• Abnormalities – Midline defects
– Hypoglycemia/jitteriness
– Significant jaundice
– Male: Microphallus
– Female: Puffiness of hands/feet, neck webbing
SGA without catch-up growth by 2-4 yo GH indication
Raise concern for hypopituitarism - GH deficiency - TSH deficiency - ACTH deficiency
Turner syndrome

Short stature
• Skeletal maturation/potential
– 1st tooth eruption
– 1st tooth shedding
– Genetic height potential
• Parental heights (if possible measure yourself)
Mid-parental height
– Familial puberty timing
• Maternal/sister’s menarche
• When father/brother stopped growing

http://exceptionalsmiles.org/oral-hygiene-basics/tooth-chart/

Mid-parental height
• If not enough time to calculate, here is a calculator:
http://medcalc3000.com/HeightPotential.htm

Rose SR et al. Peds in Review, 2005, 26: 414

Rose SR et al. Peds in Review, 2005, 26: 414

Short stature
• Habits
– Nutrition
– Sleep
• Other history
– Head trauma (e.g., meningitis, loss of consciousness)
– Co-morbidities (e.g., asthma, ADHD, CV/renal/other)
Rose SR et al. Peds in Review, 2005, 26: 414

Normal growth
Age Weight velocity Height velocity
0-1 yo - 0-3 months - 3-6 months - 6-12 months
30 g/day 20 g/day 10 g/day
25 cm/yr (10 inch/yr)
1-2 years 2 kg/yr 10 cm/yr (4 inch/yr)
2-4 years 2 kg/yr 7.5 cm/yr (3 inch/yr)
4 years - puberty 2 kg/yr 5 cm/yr (2 inch/yr)
Puberty 10 cm/yr (4 inch/yr)

Boy (similar one exists for girls)
http://sph.sagepub.com/content/3/1/32/F2.large.jpg
Growth velocity

Supine length: Until 2 years old
http://www.boysgirlsbabygrowth.com/how-to-measure-baby-length/

Standing height: Average of 3 measurements (within 0.3 cm of each other)
Look straight ahead
Shoulders relaxed
Arms at sides
Legs straight, knees together
Feet flat, heels almost together,
feet pointed outward at 60° angle
Shoulder blades, buttocks, and heels
touching measurement surface

Growth: Case 1 • 11 yo M: Concern for short stature
MPH

Growth: Case 1 • 11 yo M: Concern for short stature
x x
x
MPH

Growth: Case 1 • 11 yo M: Concern for short stature
x x
x
MPH
MPH
If referring to pediatric endocrinology, please send growth charts/measurements.

Upper:lower segment ratio
http://www.childhealth-explanation.com/growth-assessment.html
Feet together
Standing height – lower segment _______________
Distance from pubic symphysis to floor
Lower segment
Upper segment
Pubic symphysis

Arm span
http://www.childhealth-explanation.com/growth-assessment.html
Fingertip to fingertip

Rose SR et al. Peds in Review, 2005, 26: 414

Rose SR et al. Peds in Review, 2005, 26: 414

Rose SR et al. Peds in Review, 2005, 26: 414
Endocrinopathy Short stature
Treatment initiation

GH deficiency

GH deficiency: Treated

Physical exam • General
– Features of specific syndromes – Upper:lower segment calculation, arm span
• Face/ENT – Midline defects – Teeth development – Tonsillar hypertrophy
• Neck – Webbing – Thyromegaly
• Chest – Nipple placement/shield chest
• CV – Edema in hands/feet – Murmur
• MSK – Hands: Shortening of metacarpals, clinodactyly, palmar crease – Pectus carinatum/excavatum
• Pubertal staging • Neuro (for potential CNS cause)
http://www.atitesting.com/ati_next_gen/skillsmodules/content/physical-assessment-child/images/PA-Child-HFN_t2.jpg
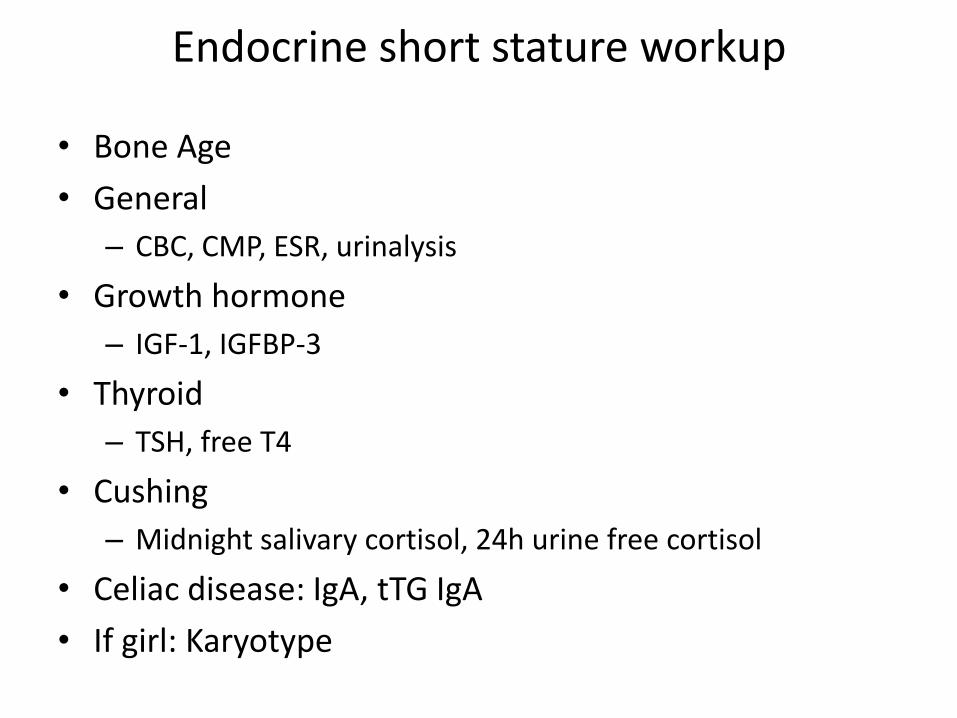
Endocrine short stature workup
• Bone Age
• General
– CBC, CMP, ESR, urinalysis
• Growth hormone
– IGF-1, IGFBP-3
• Thyroid
– TSH, free T4
• Cushing
– Midnight salivary cortisol, 24h urine free cortisol
• Celiac disease: IgA, tTG IgA
• If girl: Karyotype

Summary • Birth history
– Birth parameters SGA?
– Concerns for hypopituitarism?
– Syndromic features?
• Skeletal maturation/potential
– Teeth development
– Parental heights Mid-parental height
– Parental puberty pattern
• Habits: Diet, sleep
• Co-morbidities & medications
• Growth pattern
• Referral necessary? To whom?

Rose SR et al. Peds in Review, 2005, 26: 414
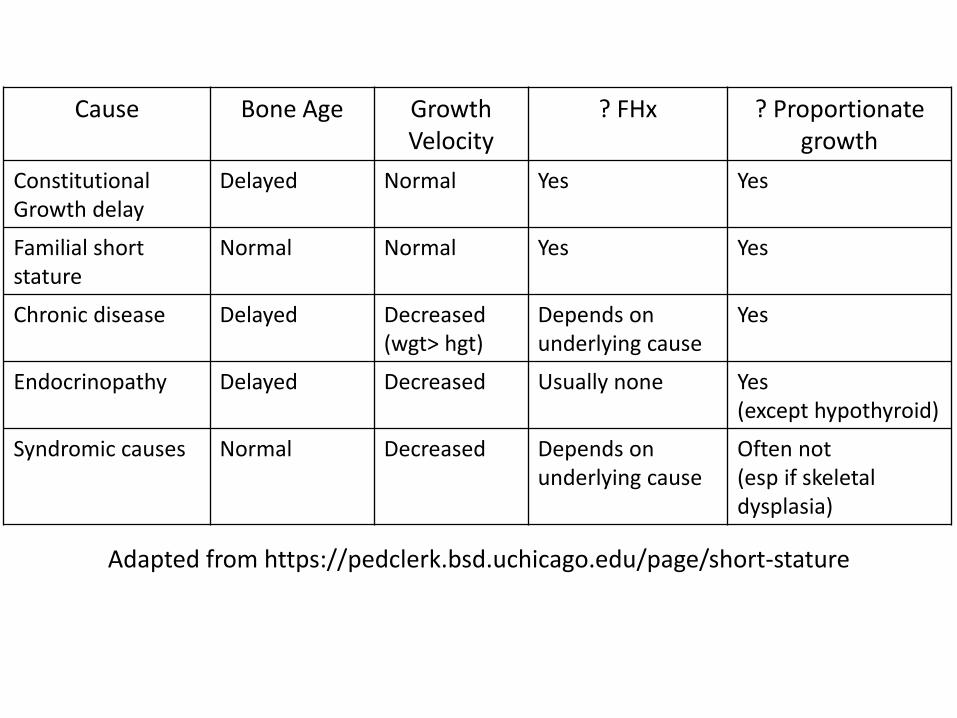
Cause Bone Age Growth Velocity
? FHx ? Proportionate growth
Constitutional Growth delay
Delayed Normal Yes Yes
Familial short stature
Normal Normal Yes Yes
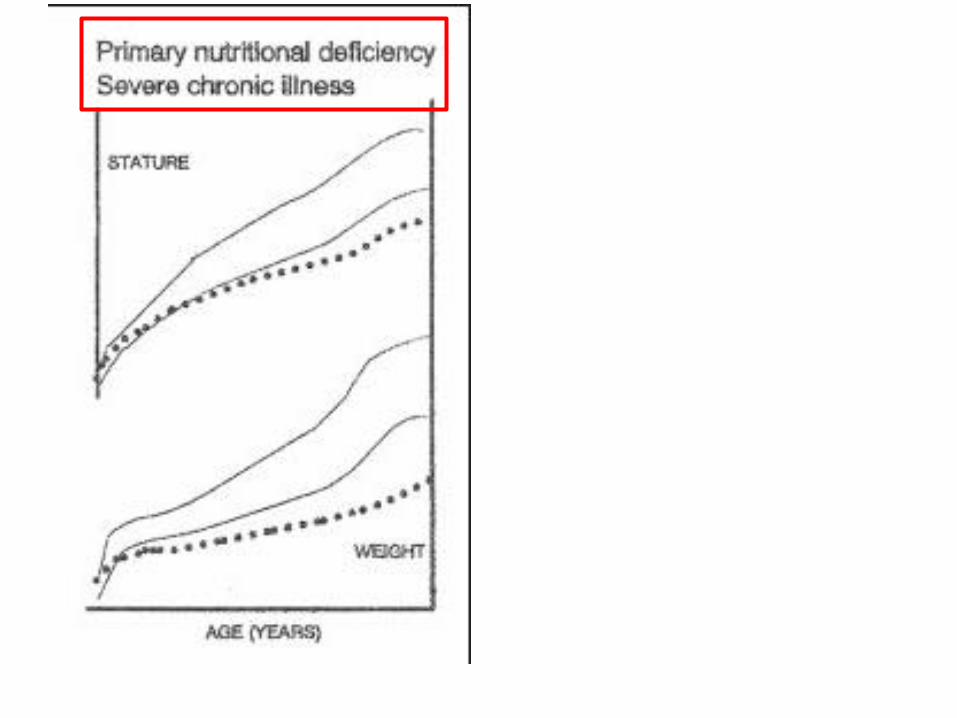
Chronic disease Delayed Decreased (wgt> hgt)
Depends on underlying cause
Yes
Endocrinopathy Delayed Decreased Usually none Yes (except hypothyroid)
Syndromic causes Normal Decreased Depends on underlying cause
Often not (esp if skeletal dysplasia)
Adapted from https://pedclerk.bsd.uchicago.edu/page/short-stature
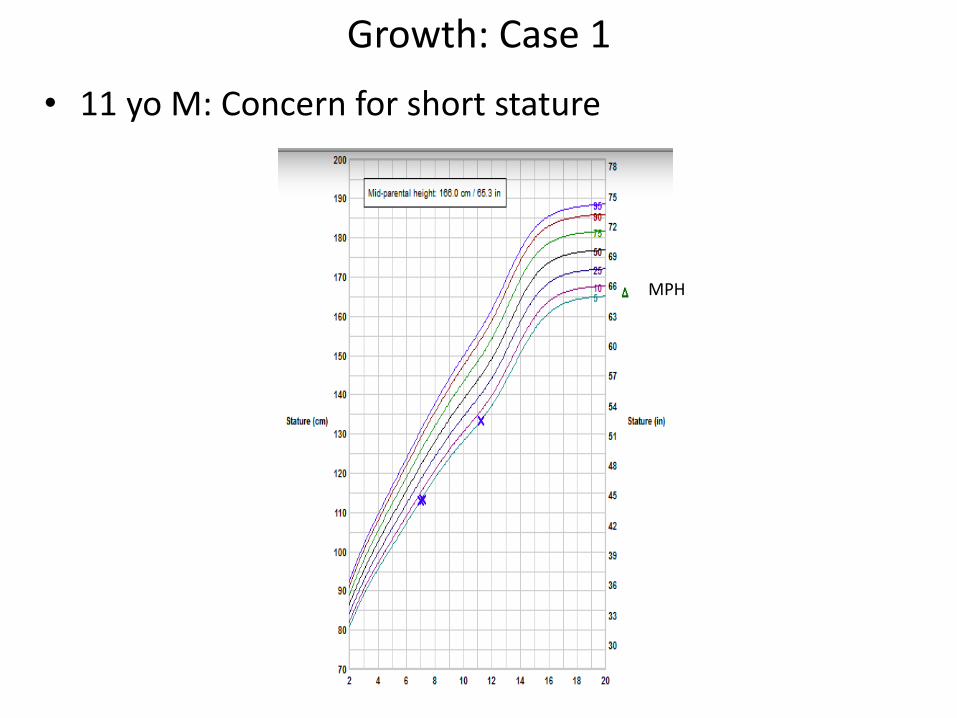
Growth: Case 1
• 11 yo M: Concern for short stature
MPH MPH

For each of the following cases:
• Does the growth fit a pattern?
– Constitutional growth delay
– Familial short stature
– Chronic disease
– Endocrinopathy
– Syndrome
• Refer?
– To whom?

Growth: Case 1
• 11 yo M: Concern for short stature
MPH

For each of the following cases:
• Does the growth fit a pattern?
– Constitutional growth delay
– Familial short stature
– Chronic disease
– Endocrinopathy
– Syndrome
• Refer?
– To whom?
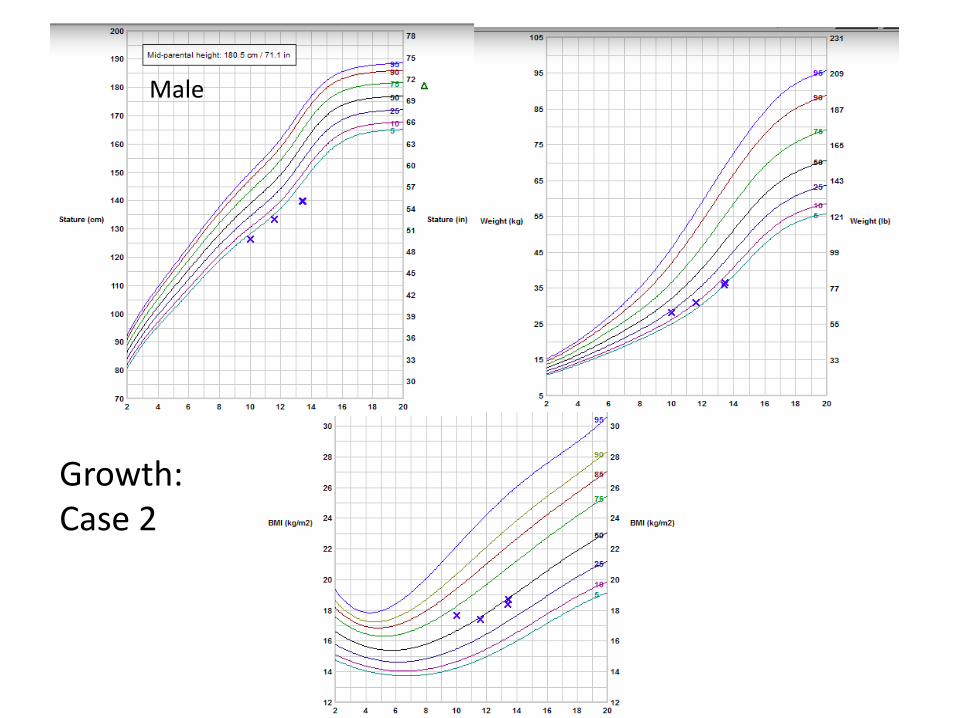
Male
Growth: Case 2

For each of the following cases:
• Does the growth fit a pattern?
– Constitutional growth delay
– Familial short stature
– Chronic disease
– Endocrinopathy
– Syndrome
• Refer?
– To whom?

Female
Growth: Case 3

For each of the following cases:
• Does the growth fit a pattern?
– Constitutional growth delay
– Familial short stature
– Chronic disease
– Endocrinopathy
– Syndrome
• Refer?
– To whom?
Male
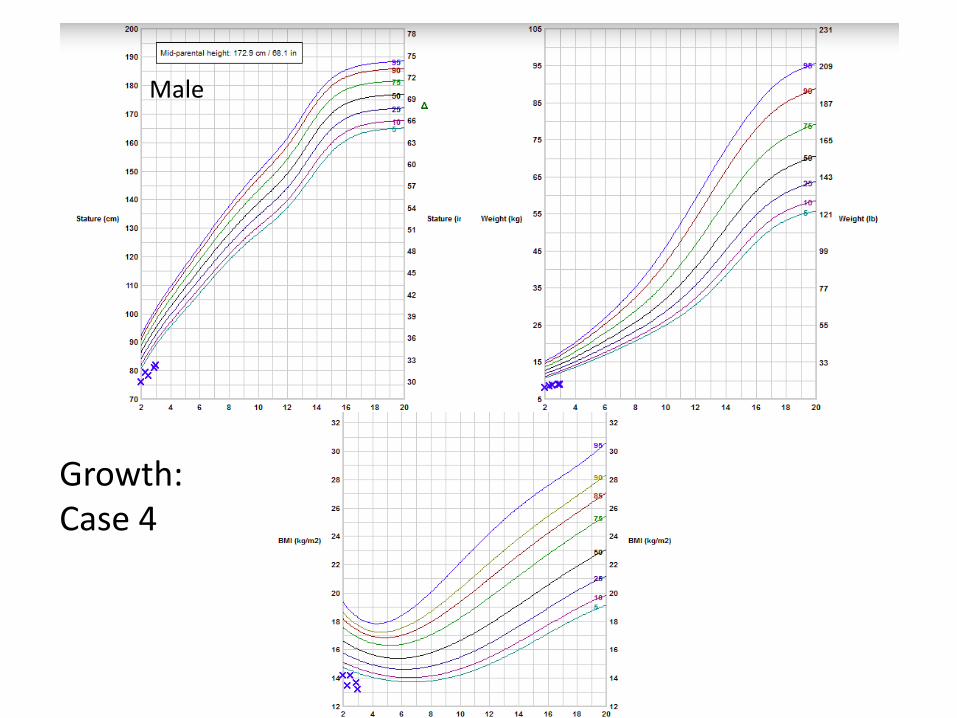
Growth: Case 4

For each of the following cases:
• Does the growth fit a pattern?
– Constitutional growth delay
– Familial short stature
– Chronic disease
– Endocrinopathy
– Syndrome
• Refer?
– To whom?

Growth: Case 4
Male

Growth: Case 5
Female

For each of the following cases:
• Does the growth fit a pattern?
– Constitutional growth delay
– Familial short stature
– Chronic disease
– Endocrinopathy
– Syndrome
• Refer?
– To whom?

Puberty
• Normal puberty
• Precocious puberty
• Delayed puberty
• Cases

Hypothalamic-pituitary-gonadal axis

Timing of puberty

Gonadotropin (LH and FSH) production
2 weeks 2 months 9-10 years
Time after birth
“Mini-puberty of infancy”

Timing of puberty: Mediating factors
• Family patterns: “Early/late bloomers”
– Father: When stopped growing
– Mother: Age at menarche
• Skeletal maturation
– Hormone deficiencies or chronic illness
Delayed bone age
Delayed onset of puberty
• Nutritional status
– Higher BMI Earlier puberty

Puberty: Normal Range for Onset
• Girls
– Youngest • 6 years in African Americans
• 7 years in Caucasians
• Classic teaching: 8 years
– Mean: 9-10 years
– Oldest: 13 years

1st visible
sign
Signs of Puberty: Female

Tanner stages: Female

1st visible
sign
Signs of Puberty: Male

Tanner stages: Male

Testicular Volume
Tanner stage 1 2 3 4 5
Volume (mL) <2 2-4 4-9
9-16 16-25
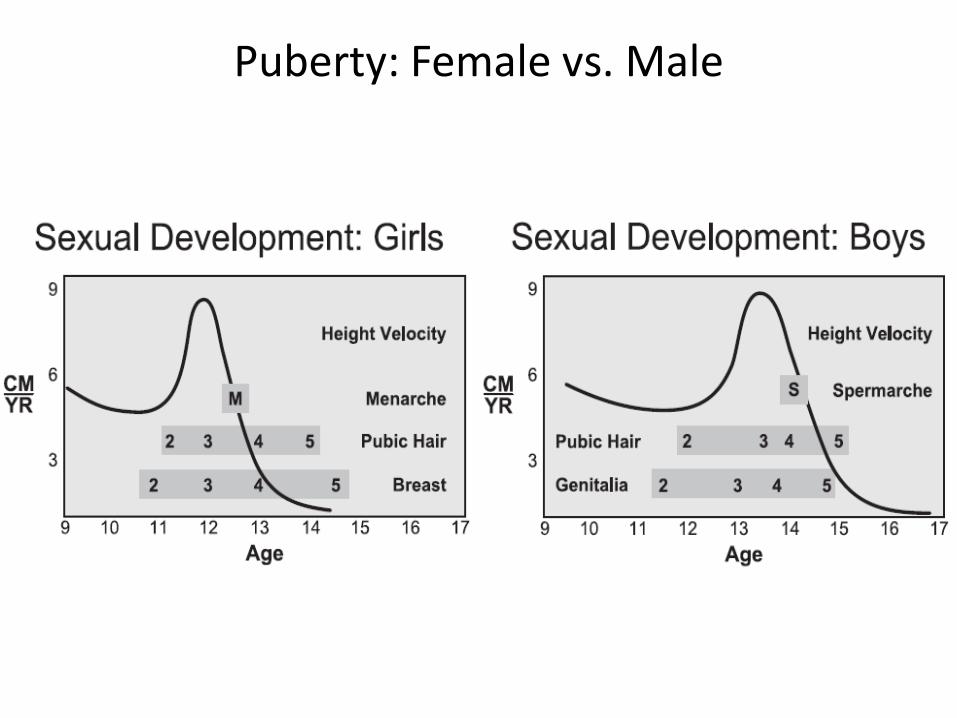
Puberty: Female vs. Male

Precocious puberty
• Signs of sexual maturation (androgen and estrogen activity) at an earlier than normal age.

Precocious puberty
• Girls:
– Any breast/pubic hair: <7 yo (Caucasian), <6 yo (AA)
– ≥ 7 yo (Caucasian) ≥ 6 yo (AA)
• Rapid progression of puberty
• Rapid bone age advancement
• New CNS findings
• Emotional state adversely affected
• Boys: <9 yo

Precocious puberty
• Differential diagnosis
– Normal variant
– Premature thelarche
– Premature adrenarche
– Hypothyroidism
– True precocious puberty


Precocious puberty: Central vs. peripheral

True precocious puberty: Differential diagnoses
• Idiopathic (girls)
• CNS tumor
• Other CNS disorder
• hCG producing tumor (boys)
Central Peripheral
• Genetic – Congenital adrenal hyperplasia
– McCune-Albright syndrome
– Testotoxicosis
• Gonadal tumor
• Adrenal tumor

Precocious puberty
• Potential workup
– Bone age
– FSH, LH, estradiol/testosterone (on pediatric assays)
– 17-OH progesterone, androstenedione, DHEA-S
– TSH, free T4

Delayed puberty
• No secondary sexual characteristics
– Girls (no thelarche): > 13 years
– Boys (testes < 4 mL): > 14 years
• Primary amenorrhea (No menarche: )
– By 16 years
– Within 3 years of thelarche

Delayed puberty
• Differential diagnosis
– Normal variant/constitutional growth delay
– Secondary to chronic illness
– Hypergonadotropic hypogonadism
– Hypogonadotropic hypogonadism
– Hypothyroidism
– Prolactinoma
– Turner syndrome

Delayed puberty: 1° vs. 2° hypogonadism

Delayed puberty
• Potential workup
– Bone age
– FSH, LH, estradiol/testosterone (on pediatric assays)
– TSH, free T4
– Prolactin

Case 1
• CC: Breast development
• HPI: 3 yo girl
– Mother noticed breast development in the newborn period which regressed.
– Left breast enlarged again at 18 months
– At 20 months the right enlarged as well
– 35-36 months for one month, nipple prominent
• ROS: No vaginal bleeding, body odor, acne
• FHx: No one with early puberty – Dad: 5’9”
– Mom: 5’4”

Physical Exam: - Healthy appearing - Breast: Tanner 3, 5cm, nipples small - GU: Tanner 1
Case 1
Puberty case: Framework
• Age: Early, normal, late
• Growth velocity: Fast, normal, slow
• Family history
– Mid-parental height
– Puberty
• Sex hormone activity: Androgen/estrogen/both/neither
• Proposed workup
• Refer?
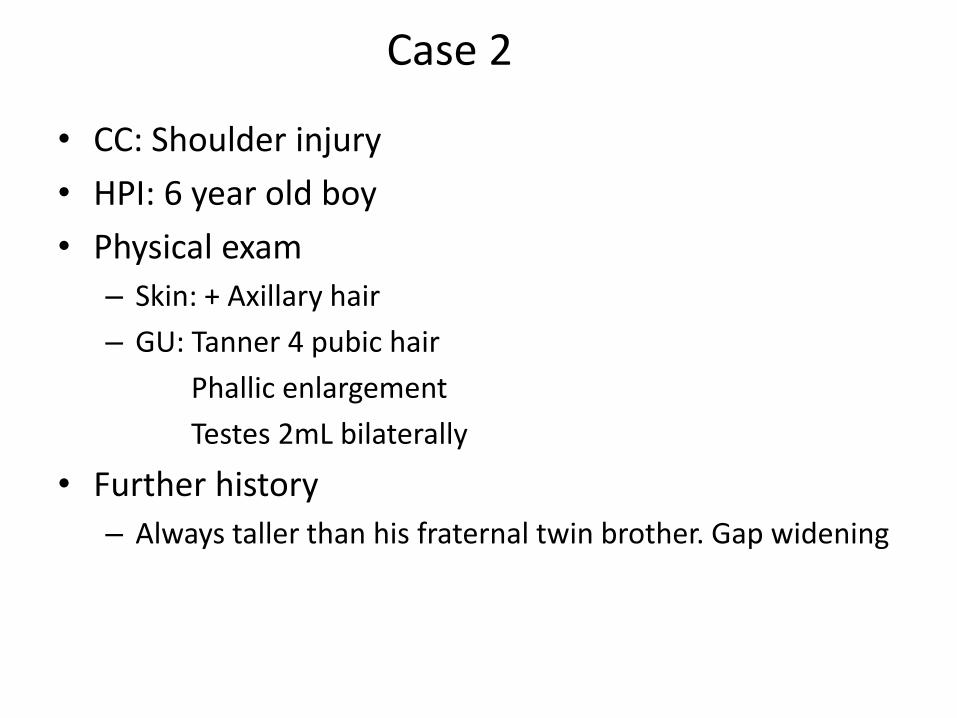
Case 2
• CC: Shoulder injury
• HPI: 6 year old boy
• Physical exam
– Skin: + Axillary hair
– GU: Tanner 4 pubic hair
Phallic enlargement
Testes 2mL bilaterally
• Further history
– Always taller than his fraternal twin brother. Gap widening

Case 2

Puberty case: Framework
• Age: Early, normal, late
• Growth velocity: Fast, normal, slow
• Family history
– Mid-parental height
– Puberty
• Sex hormone activity: Androgen/estrogen/both/neither
• Proposed workup
• Refer?

Case 3
• CC: Well child visit
• HPI: 14 year old girl
• Physical exam
– Breast: Tanner 1
– GU: Tanner 1
– Extremities: Edema of hands and feet
• Family history
– Father: 5’11”
– Mother: 5’3”, menarche 12 years old

Puberty case: Framework
• Age: Early, normal, late
• Growth velocity: Fast, normal, slow
• Family history
– Mid-parental height
– Puberty
• Sex hormone activity: Androgen/estrogen/both/neither
• Proposed workup
• Refer?

Case 4
• CC: Lack of menses
• HPI: 17 year old girl
• History: – Breast development in 3rd grade
– Increased body odor in 4th grade
– Axillary/pubic hair in 5th grade
• ROS: No abdominal cramping, no acne or excess/coarse hair
• Physical exam – BMI: 65th %ile
– Breast: Tanner 5
– GU: Tanner 5
• Family history – Father: 6’0”
– Mother: 5’4”, menarche at 10 years old

Obesity
• Genetic causes
• Co-morbidities
• Lab evaluation
• Participant questions

Genetic causes of obesity
• Dysmorphic syndromes
– Albright hereditary osteodystrophy
– Alström
– Bardet-Biedl
– Carpenter
– Cohen
– Prader-Willi
Wit JM et al. Hormone Researche, 2007, 68 (Suppl 2): 101-106

Albright hereditary osteodystrophy
http://medlibes.com/entry/albright-hereditary-osteodystrophy

Alström Bardet-Biedl Laurence-Moon
Type 2 diabetes mellitus x x
Hypogonadism x x
Mental retardation x x
Obesity x x
Post-axial polydactyly x
Renal dysfunction x x
Retinitis pigmentosa x x x
Sensorineural hearing loss
x
Spastic paraplegia x
Forsythe E & Beales PL. Eur J Hum Genetics, 2013, 21: 8-13 Marshall JD et al. Curr Genomics, 2011, 12: 225-235
Wit JM et al. Hormone Research, 2007, 68 (Suppl 2): 101-106

Bardet-Biedl syndrome
A-D: Typical facial features (subtle, not always present). Features include deep-set eyes, hypertelorism, downward slanting palpebral fissures, a flat nasal bridge, small mouth, malar hypoplasia and retrognathia. (e) Brachydactyly and scars from excision of accessory digits. (f) Dental crowding. (g) High-arched palate. (h) Fundoscopy demonstrating rod-cone dystrophy.
Forsythe E & Beales PL. Eur J Hum Genetics, 2013, 21: 8-13

Carpenter syndrome
http://openi.nlm.nih.gov/detailedresult.php?img=3429868_humu0032-E2069-f2&req=4

Cohen syndrome
El Chehadeh-Dhebbar S et al. Eur J Hum Genetics, 2013, 21: 736-742

Prader Willi syndrome
(a) An 8-month-old female with hypotonia and G-tube. (b) A 19-year-old male typical body habitus with fat distributed primarily in abdomen, hips, and thighs. (BMI = 67; Z score = +3.49) (c) A 34-year-old man in relatively good dietary control. (BMI = 30; Z score = +1.66)
Cassidy SB et al. Genetics in Medicine, 2012, 14: 10-26

Genetic causes of obesity
Monogenic obesity – Leptin
– Leptin receptor
– POMC (Pro-opiomelanocortin)
– Prohormone convertase
– MC3R
– MC4R
Seely RJ & Woods SC. Nat Rev Neuroscience, 2003, 4: 901-909 Speiser PW et al. JCEM, 2005, 90: 1871-1887
Leptin
Leptin - R
POMC MC3R
MC4R

Genetic causes: Summary
• Genetic causes of obesity exist. However diagnosis does not yet change management of the obesity.

Potential co-morbidities
• Cholelithiasis
• Dyslipidemia
• Hypertension
• Musculoskeletal conditions
• Non-alcoholic fatty liver disease
• Obstructive sleep apnea
• Polycystic ovary syndrome
• Type 2 diabetes mellitus
August GP et al. JCEM, 2008, 93: 4576-4599

Endocrine causes of obesity: Lab evaluation
• Endocrine causes
– Growth hormone deficiency/Hypopituitarism
– Hypothyroidism
– Cushing syndrome
• Usually not recommended unless:
– Height velocity
– Growing at lower height %tile than predicted by mid-parental height
August GP et al. JCEM, 2008, 93: 4576-4599

Endocrine causes of obesity: Lab evaluation
• Endocrine causes – Growth hormone deficiency/Hypopituitarism
• GH deficiency: IGF-1, IGBP-3
• ACTH deficiency: 8 AM serum cortisol
– Hypothyroidism • TSH, free T4
– Cushing syndrome • Midnight salivary cortisol, 24h urine free cortisol
• Usually not recommended unless: – Height velocity
– Growing at lower height %tile than predicted by mid-parental height
August GP et al. JCEM, 2008, 93: 4576-4599

Potential co-morbidities: Lab evaluation
• Cholelithiasis • Dyslipidemia – Fasting lipid panel • Hypertension • Musculoskeletal conditions • Non-alcoholic fatty liver disease - CMP • Obstructive sleep apnea • Polycystic ovary syndrome
– 17-OHP, androstenedione, DHEA-S, free testosterone – TSH, free T4 – Prolactin
• Type 2 diabetes mellitus – Hemoglobin A1c, fasting glucose, (not usually 1st test: 2h OGTT)
Vitamin D: Screening • AAP
– No universal screening for children who are:
• Healthy
• Dark skinned
• Obese
• Endocrine Society – Not the general population
– Pediatrics: Screen those at risk
• Obese
• Black, Hispanic
• Malabsorption
• Medications: Glucocorticoid, anticonvulsant, antifungal, antiretroviral
• IOM: No specific screening recommendations
Golden NH et al. Pediatrics, 2014, 134: e1229-e1243 Holick MF et al. JCEM, 2011, 96: 1911-1930
Institute of Medicine, Dietary Reference Intakes for Calcium and Vitamin D. 2010

Vitamin D: Screening
• AAP
– No universal screening for: • Healthy
• Dark skinned
• Obese
– Mention conditions at risk for reduced bone mass (table)
Conditions Associated with Reduced Bone Mass in Children and Adolescents ____________________________ Genetic conditions Osteogenesis imperfecta Idiopathic juvenile osteoporosis Turner syndrome Chronic illness Cystic fibrosis Connective tissue disorders (lupus, juvenile idiopathic arthritis, juvenile dermatomyositis) Inflammatory bowel disease, celiac disease Chronic renal failure Childhood cancer Cerebral palsy Chronic immobilization Eating disorders, including anorexia nervosa, bulimia nervosa, eating disorders NOS, and the female athlete triad Endocrine conditions Cushing syndrome Hypogonadism Hyperthyroidism Hyperparathyroidism Growth hormone deficiency Diabetes mellitus Medications Glucocorticoids Anticonvulsants Chemotherapy Leuprolide acetate Proton pump inhibitors SSRIs DMPA _____________________________________
Table adapted from Golden NH et al. Pediatrics, 2014, 134: e1229-e1243

Vitamin D
Holick MF et al. JCEM, 2011, 96: 1911-1930 Institute of Medicine, Dietary Reference Intakes for Calcium and Vitamin D. 2010
Misra M et al. Pediatrics, 2009: 122: 398-417
Vitamin D level ng/mL (nmol/L)
Endocrine Society
Institute of Medicine
Pediatric Endocrine
Society
Severe deficiency ≤ 5 (12.5)
Deficiency < 20 (50) < 12 (30) ≤ 15 (37.5)
Insufficiency 21-29 (52.5-72.5) 12-20 (30-50) 15-20 (37.5-50)
Sufficiency 30-100 (75-250) 20-50 (50-125) 20-100 (50-250)
Excess > 50 (125) > 100 (250)
Intoxication > 150 (375)

Vogiatzi MG et al. JCEM, 2014, 99: 1132-1141
Lab evaluation: Summary
• Do not routinely screen for endocrine causes of obesity unless concern for poor height velocity or growing at a lower than expected percentile.
• Co-morbidity screening
– CMP, fasting lipid panel, hemoglobin A1c
• Vitamin D:
– Screening and sufficiency levels are controversial