pediatrics 2013- sreening para has
TRANSCRIPT

Screening for Hypertension in Children and Adolescentsto Prevent Cardiovascular Disease
abstractBACKGROUND AND OBJECTIVE: The prevalence of hypertension is in-creasing in children, and may persist into adulthood. This systematicreview was conducted for the US Preventive Services Task Force rec-ommendation on the effectiveness of screening asymptomatic childrenand adolescents for hypertension in order to prevent cardiovasculardisease.
METHODS: Eligible studies were identified from Medline and theCochrane Library (through July 2012). We included trials and controlledobservational studies in asymptomatic children and adolescents on theeffectiveness and harms of screening and treatment, as well as accu-racy of blood pressure measurement. One author extracted study char-acteristics and results, which were checked for accuracy by a secondauthor.
RESULTS: No studies evaluated the effects of screening for hyperten-sion on health outcomes. Two studies of screening tests for elevatedblood pressure reported moderate sensitivities (0.65, 0.72) and speci-ficities (0.75, 0.92). Sensitivities and specificities of child hypertensionfor the later presence of adult hypertension (7 studies) were wideranging (0–0.63 and 0.77–1.0, respectively), and associations betweenchild hypertension and carotid intima media thickening and protein-uria in young adults (3 studies) were inconsistent. Seven studiesreported that drug interventions effectively lowered blood pressurein adolescents over short follow-up periods. No serious treatment-related adverse effects were reported.
CONCLUSIONS: There is no direct evidence that screening for hyper-tension in children and adolescents reduces adverse cardiovascularoutcomes in adults. Additional studies are needed to improve diagnosisand risk stratification of children with elevated blood pressure and toquantify risks and benefits of interventions. Pediatrics 2013;131:490–525
AUTHORS: Matthew Thompson, MD, MPH, DPhil,a,b TracyDana, MLS,a Christina Bougatsos, MPH,a Ian Blazina, MPH,a
and Susan L. Norris, MD, MPH, MSca
aOregon Evidence-Based Practice Center, Oregon Health andScience University, Portland, Oregon; and bDepartment ofPrimary Care Health Sciences, Oxford University, Oxford, UnitedKingdom
KEY WORDShypertension, children, adolescents, screening, treatment, drug,lifestyle
ABBREVIATIONSADAPT—Dietary/Exercise Alteration Program TrialCI—confidence intervalDBP—diastolic blood pressureOR—odds ratioRCT—randomized controlled trialSBP—systolic blood pressureUSPSTF—US Preventive Services Task Force
Dr Thompson made substantial contributions to conception anddesign, acquisition of data, analysis and interpretation of data,drafted the article and revised it critically for importantintellectual content, and gave final approval of the version to bepublished. He is guarantor for this article. Ms Dana andBougatsos, Mr Blazina, and Dr Norris made substantialcontributions to conception and design, acquisition of data,analysis and interpretation of data, revised the article criticallyfor important intellectual content, and gave final approval of theversion to be published.
The staff at the Agency for Healthcare Research Quality andmembers of the US Preventive Services Task Force developedthe scope of the work and reviewed draft manuscripts. Approvalfrom the Agency for Healthcare Research Quality was requiredbefore the manuscript was submitted for publication, but theauthors are solely responsible for the content and the decisionto submit it for publication.
www.pediatrics.org/cgi/doi/10.1542/peds.2012-3523
doi:10.1542/peds.2012-3523
Accepted for publication Dec 19, 2012
Address correspondence to Matthew Thompson, MD, MPH, DPhil,Department of Primary Care Health Sciences, Oxford University,New Radcliffe House, Woodstock Road, Oxford OX2 6GG, UK. E-mail:[email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: This review was supported by the Agency forHealthcare Research Quality for the US Preventive Services TaskForce under contract 290-2007-10057-I to support the work ofthe US Preventive Services Task Force.
490 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
Between 1% and 5% of children andadolescents have hypertension, and itsprevalence has risen in the UnitedStates by 1% to 2% over recent deca-des.1–4 Hypertension is usually asymp-tomatic, and a significant proportion ofchildren with hypertension are un-diagnosed.5,6 Screening children andadolescents for elevated blood pres-sure could identify hypertension at anearly stage where interventions couldbe initiated, potentially decreasing therate of progression of hypertensionfrom childhood to adulthood and re-ducing the clinical consequences ofhypertension in adulthood.7
The strongest risk factor for primaryhypertension in children of all ages andboth genders is elevated BMI8–14; chil-dren who are overweight or obese havea two- to threefold increased risk ofhypertension.8–10 This increased risk isparticularly concerning given that∼17% of children and adolescents inthe United States are now obese15 andhave higher risk of other cardiovascu-lar risk factors such as an adverselipid profile and insulin resistance.16
Other risk factors for primary hyper-tension include low birth weight, gen-der, ethnicity, and a positive familyhistory.2,3,9,10,17–19
Secondary hypertension is most com-monly related to underlying renal pa-renchymal or renovascular disease;less common causes include aorticcoarctation and endocrine disorders.20,21 Elevated blood pressure is usuallyonly 1 clinical manifestation of the un-derlying disorder, and treatment istypically directed at correcting theunderlying cause.
For the majority of children and ado-lescents, the rationale for identifyingelevated blood pressure lies in the po-tential to stratify risk of future cardio-vascular disease. There is convincingevidence that structural and functionalchanges in the cardiovascular system,which indicate early atherosclerosis,can be detected in adolescents andyoung adults. What is less clear are thenature and magnitude of the relation-ship between elevated blood pressureand other cardiovascular risk factors inchildren or adolescents and cardiovas-cular risk in adults. Cohort studies thathave followed children to young adult-hood suggest that adiposity, insulin re-sistance, and an adverse lipid profileprogress at an increased rate in pre-hypertensive and hypertensive childrenand adolescents compared with nor-motensive children.7,22,23
AIMS OF THIS REVIEW
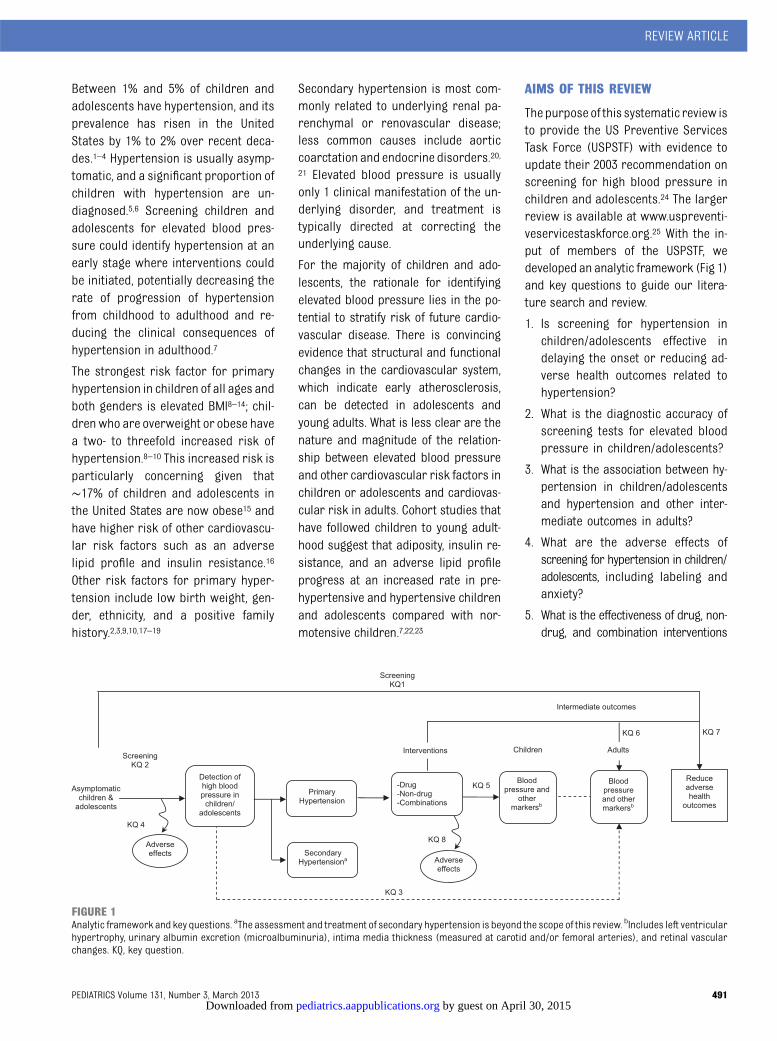
Thepurpose of this systematic review isto provide the US Preventive ServicesTask Force (USPSTF) with evidence toupdate their 2003 recommendation onscreening for high blood pressure inchildren and adolescents.24 The largerreview is available at www.uspreventi-veservicestaskforce.org.25 With the in-put of members of the USPSTF, wedeveloped an analytic framework (Fig 1)and key questions to guide our litera-ture search and review.
1. Is screening for hypertension inchildren/adolescents effective indelaying the onset or reducing ad-verse health outcomes related tohypertension?
2. What is the diagnostic accuracy ofscreening tests for elevated bloodpressure in children/adolescents?
3. What is the association between hy-pertension in children/adolescentsand hypertension and other inter-mediate outcomes in adults?
4. What are the adverse effects ofscreening for hypertension in children/adolescents, including labeling andanxiety?
5. What is the effectiveness of drug, non-drug, and combination interventions
FIGURE 1Analytic framework and key questions. aThe assessment and treatment of secondary hypertension is beyond the scope of this review. bIncludes left ventricularhypertrophy, urinary albumin excretion (microalbuminuria), intima media thickness (measured at carotid and/or femoral arteries), and retinal vascularchanges. KQ, key question.
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 491 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

for treating primary hypertensionin children/adolescents?
6. What is the effectiveness of drug,nondrug, and combination inter-ventions initiated for the treatmentof primary hypertension in children/adolescents for reducing blood pres-sure and other intermediate outcomesin adults?
7. What is the effectiveness of drug,nondrug, and combination inter-ventions initiated for the treatmentof primary hypertension in children/adolescents for reducing adversehealth outcomes in adults relatedto primary hypertension?
8. What are the adverse effects ofdrug, nondrug, and combinationinterventions for treating primaryhypertension in children/adoles-cents?
METHODS
ThisreviewwasdevelopedbytheOregonEvidence-Based Practice Center undercontract with the Agency for HealthcareResearch Quality (contract 290-2007-10057-I) and follows the systematic re-view methods of the USPSTF.26,27
Search Strategies
We searched the Cochrane CentralRegister of Controlled Trials and theCochrane Database of SystematicReviews (through July 2012) and Med-line (1946 to July 9, 2012) for relevantstudies and systematic reviews, andmanually reviewed reference lists forrelevant citations (Appendix 1).
Study Selection and Processes
Papers were selected for full review ifthey met predefined inclusion criteria(Appendix 2). Controlled studies ofscreening for hypertension in asymp-tomatic children and adolescents wereincluded. For studies of diagnostic ac-curacy, eligible studies included a refer-encestandardcomparisonandprovided
adequate data to reproduce contingencytables. Evidence from randomizedplacebo-controlled trials was used toassess the efficacy of treatments onmultiple outcomes, including bloodpressure, other intermediate healthoutcomes, and final health outcomes, inchildhood, adolescence, and adulthood.Studies with ,30 participants andstudies of interventions for the treat-ment of obesity and lipid disorders inchildren were excluded, because thesepopulations are considered in otherUSPSTF recommendations.28,29 To assessharms of treatment, studies withouta comparison or a placebo group wereincluded. Studies of secondary hyper-tension were excluded, although somestudies included proportions of partic-ipants with secondary hypertension.
All citations identified throughsearchesand other sources were independentlyreviewed by 2 authors for inclusion andexclusion. Discrepancies at the full-textlevelwere resolved through consensus.One author extracted data on the pa-tient population, study design, testingmethods, analysis, follow-up, and re-sults, andasecondauthorcheckeddataextraction for accuracy.
Quality Assessment and Synthesis
By using predefined criteria developedby the USPSTF,26 2 authors rated thequality of studies (good, fair, poor) andresolved discrepancies by consensus.Authors assessed the overall strengthof the body of evidence for each keyquestion as good, fair, or poor by usingmethods developed by the USPSTF onthe basis of the number, quality, andsample size of studies, as well as theconsistency of results among studiesand directness of the evidence.26 Thelimited number of studies and theheterogeneity of study designs, inter-ventions, and diagnostic tests pre-cluded meta-analyses; results aretherefore summarized qualitatively asmeans or as ranges, as appropriate.
RESULTS
Our literature search identified a totalof 6435 citations, of which we reviewed1059 full-text publications and included34 studies (Fig 2).
Key Question 1: Is Screening forHypertension in Children/Adolescents Effective in Delayingthe Onset or Reducing AdverseHealth Outcomes Related toHypertension?
No randomized trials compared healthoutcomes related to hypertension inscreened versus nonscreened child oradolescent populations.
Key Question 2: What Is theDiagnostic Accuracy of ScreeningTests for Elevated Blood Pressurein Children and Adolescents?
We identified 2 fair-quality studies thatprovided data on the diagnostic accu-racyof screening tests (Appendix 3).30,31
Compared with a reference standardof 24-hour ambulatory measurement,office-based blood pressure measure-ment (3 measurements at each of 2clinic visits) had a sensitivity of 0.65(95% confidence interval [CI], 0.45–0.80) and a specificity of 0.75 (95% CI,0.63–0.84).31 The positive predictivevalue was 0.37 (95% CI, 0.28–0.47) andthe negative predictive value was 0.63(95% CI, 0.53–0.72). All 105 participants(mean age, 13 years) had been re-ferred for evaluation at a specialtyclinic, so they may not have been rep-resentative of screened populations ofasymptomatic children. In addition,ambulatory measurement is not yetan internationally accepted referencestandard in children and adolescents.A second study examined a randomsample of 9017 eighth graders, ofwhom about 10% (900/9017) had bloodpressure .95th percentile on initialscreening, whereas the remainder(8117/9017) were normotensive.30 Atfollow-up in 10th grade, the sensitivity
492 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

and specificity of initial elevated bloodpressure for persistent elevation ofblood pressure were 0.72 (95% CI,0.65–0.78) and 0.92 (95% CI, 0.91–0.92),respectively; however, the positivepredictive value was low (0.17 [95% CI,0.15–0.20]). This study primarily fol-lowed only the sample of childrenwhose initial screening test was posi-tive rather than the entire population,which may have biased the diagnosticaccuracy in this study.
In addition, 12 studies compared $1measurement of blood pressure withsubsequent reference measurementsbut did not meet our inclusion criteriabecause either they failed to apply thereference tests to participants whoinitially screened negative or they didnot use an acceptable reference stan-dard.11,32–42 Positive predictive valuesamong these studies ranged from 0.04to 0.53. The reasons for this heteroge-neity were unclear but did not appear
to be related to varying prevalence ofhypertension, method or device usedfor testing, or thresholds used to de-fine positive tests.
Key Question 3: What Is theAssociation Between Hypertensionin Children/Adolescents andHypertension and OtherIntermediate Outcomes in Adults?
Ten longitudinal studies provided evi-dence on the association between ele-vated blood pressure or hypertensionin childhood and elevated blood pres-sure, hypertension, or intermediateoutcomes in adults (Appendix 4).7,43–51
These studies used different thresh-olds for defining elevated blood pres-sure and hypertension in childhoodand different definitions of hyperten-sion in adults. The sensitivities andspecificities of elevated blood pressureor hypertension in childhood for pre-dicting adult hypertension ranged from
0 to 0.63 and 0.77 to 1, respectively,depending on thresholds.45,47,51 Positivepredictive values (ie, the probability ofadult hypertension given the presenceof elevated blood pressure or hyper-tension in childhood) ranged from 0.19to 0.65.45,47 Five studies reported sig-nificant associations between elevatedblood pressure in childhood and hy-pertension in adults, with odds ratios(ORs) ranging from 1.1 to 4.57,47 andrelative risks ranging from 1.5 to 9.43,44,48
Two studies reported conflicting find-ings on the association between child-hood hypertension and carotid intimamedia thickness in young adults. Sys-tolic blood pressure (SBP) .80th per-centile in adolescence was mildlyassociated with carotid intima mediathickness in adulthood in 1 study (re-gression coefficient, 0.013; P, .001).50
A second study, however, found no in-creased risk of carotid intima mediathickness in adulthood related to
FIGURE 2Literature search flow diagram. aCochrane databases include the Cochrane Central Register of Controlled Trials and the Cochrane Database of SystematicReviews. bOther sources include reference lists, suggested by peer reviewers, etc. cSome articles are included for.1 key question. dTwelve of these studiesdid not provide enough data to recreate 2 3 2 tables or calculate sensitivity and specificity.
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 493 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

elevated systolic blood pressure inchildhood (highest quartile versuslower 3 quartiles: OR, 1; 95% CI, 0.80–1.25), although the level of SBP elevationis not defined in this study.49 Childhoodhypertension was significantly associ-ated with microalbuminuria in blackbut not white adults in a single study.46
We found no evidence for associationsbetween diagnosed hypertension inchildhood and other intermediate orfinal health outcomes.
Key Question 4: What Are theAdverse Effects of Screening forHypertension in Children andAdolescents, Including Labelingand Anxiety?
One small good-quality study compared85 children (10–18 years of age) withelevated blood pressure identified byscreening to children matched by ageand gender from the same commu-nity.52 The only outcome reported wasrates of school absenteeism, which didnot differ significantly between the 2groups.
Key Question 5: What Is theEffectiveness of Drug, Nondrug,and Combination Interventions forTreating Primary Hypertension inChildren and Adolescents?
Fourteen fair-quality randomized con-trolled trials (RCTs)33,53–66 (in 15 pub-lications) of treatment of hypertensionin children and adolescents met in-clusion criteria (Table 1; Appendix 5). Theproportion of children with primary hy-pertension ranged from 31%54 to 56%55;however, most studies did not report theproportion of participants with second-ary hypertension.53,57–60,62,64–66
Drug Interventions
All seven included trials of drug inter-ventions examined different drugs.53–59
Most compared active drug (in differ-ent doses) to placebo, with follow-up ofonly 4 weeks. The magnitude of effects
on SBP and diastolic blood pressure(DBP) varied and were not consis-tently different from changes inblood pressure in the placebo group(or these differences were not re-ported).
Five studies53,54,57–59 reported the per-centage of participants achieving tar-get blood pressure at the end of thefollow-up period, and all noted an in-crease in those who achieved targetlevels with the active drug (range 15–86% of subjects). However, 26% to 47%of children in the placebo groups alsoachieved normal blood pressure at theend of the study period.53–59 Moststudies reported significant reductionsinmean SBP (range, 1.9–10.2mm Hg) andDBP (range, 0.4–8.1 mm Hg). Eplerenone(50 mg/day) produced a small increasein mean SBP and no change in DBP.55
Most studies had limitations, most no-tably the failure to report the statisticalsignificance of differences between treat-ment groups in addition to within-grouptreatment differences. Also, comparisonamong studies was difficult because ofvarying drug dosages.
Drug Plus Lifestyle Interventions
The school-based A Dietary/ExerciseAlteration Program Trial (ADAPT) ex-amined the effectiveness of a multi-component, school-based intervention,including nutrition education for andpromotion of diet modification to chil-drenandparents; expandedcommunityavailability of low-sodium foods in gro-cery stores, restaurants, and schoollunches; a school-based exercise pro-gram; and propranolol and chlorthali-done compared with a no interventiongroup.60,61 This complex interventionresulted in a significant decrease inboth SBP and DBP at the 6-monthfollow-up (mean SBP change: 27.6mm Hg [P, .0001]; mean DBP change:26.9 mm Hg [P, .01]) compared withthe control group. At 30 months, how-ever, SBP increased from baseline in
both the intervention (1.4 mm Hg) andcontrol groups (3.5 mm Hg), althoughDBP remained below baseline levels(mean change: 24.2 mm Hg in the in-tervention group and 23.3 mm Hg inthe control group).
Lifestyle Interventions
Most of the six trials examining lifestyleinterventions included support relatedto the interventions (eg, regular check-ins) in addition to diet, exercise, ormeditation.33,62–66 Only 1 study demon-strated statistically significant reduc-tions in blood pressure comparedwith untreated controls.64 This small,school-based RCT compared the effectsof 5 versus 3 weekly physical educationclasses in hypertensive children andreported that blood pressure de-creased significantly more in partic-ipants receiving 5 weekly classes overthe 8-month follow-up period (meanbetween-group difference in SBP =24.9mm Hg and DBP =23.8 mm Hg; P, .05for both outcomes).64 In another trial,a low-sodium diet combined with per-sonalized support from a nutritionistand/or potassium chloride supplemen-tation was effective in reducing bloodpressure compared with usual careplus placebo at 36 months among girlsbut not among boys.66 Other studies ofmeditation,63 relaxation,33 and dietarychanges62,65 reported no significantdifferences between intervention andcontrol groups.
Key Question 6: What Is theEffectiveness of Drug, Nondrug,and Combination InterventionsInitiated for the Treatment ofPrimary Hypertension in Children/Adolescents for Reducing BloodPressure and Other IntermediateOutcomes in Adults?
No RCTs examined the effectiveness ofinterventions for hypertension in chil-dren or adolescents for reducing bloodpressure or other intermediate out-comes in adults.
494 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

TABLE 1 Effect of Interventions on Blood Pressure: Reported Mean Differences From Baseline and/or Placebo
Author, Year, Duration Interventions Baseline (mm Hg) Follow-up(mm Hg)
Mean Difference:Follow-up VersusBaseline (mm Hg)
MeanDifference atFollow-up:Intervention
VersusPlacebo(mm Hg)
SBP DBP SBP DBP SBP DBP SBP DBP
Drug interventionsBatisky et al 200776 (4 wk) Metoprolol 0.2 mg/kg 131.4 76.3 126.2 73.2 25.2 23.1 24.6 26.1
Metoprolol 1.0 mg/kg 135.0 81.0 127.3 76.1 27.7 24.9 23.5 23.2Metoprolol 2.0 mg/kg 130.60 76.7 124.3 69.2 26.3 27.5 20.2 210.1Placebo 132.7 81.4 130.8 79.3 21.9 22.1 — —
Flynn et al 200454 (4 wk) Amlodipine 2.5 mg 137.9a 74.2a Not reported 26.9 24.2 Not reportedAmlodipine 5 mg 28.7 24.4Placebo 23.6 20.4 — —
Li et al 201055 (4 wk) Eplerenone 25 mg 125.0 71.3 124.1 70.7 20.9 20.6 25.4 0.8Eplerenone 50 mg 125.7 70.9 126.2 70.9 0.5 0.0 23.3 1.0Eplerenone 100 mg 128.1 70.3 127.0 69.4 21.1 20.9 22.5 20.5Placebo (mean, all arms) 128.7 70.4 129.5 69.9 0.8 20.5 — —
Sorof et al 200256 (4 wk) Bisoprolol + hydrochlorothiazide(all doses)
133.8 83.0 124.0 76.0 29.8 27.0 24.5 23.5
Placebo 133.8 81.8 128.5 79.5 25.3 22.3 — —
Trachtman et al 200357 (3 wk) Felodipine 2.5 mg Not reported 20.7 22.1Felodipine 5 mg 20.1 24.6Felodipine 10 mg 21.1 1.3Placebo Not reported 83.1 Not reported 81.0 Not reported 22.1 — —
Trachtman et al 200858 (4 wk) Candesartan (all doses) Not reported 210.2 26.6 Not reportedPlacebo 23.7 21.8 — —
Wells et al 201059 (4 wk) Telmisartan, low-dose 132.0 79.0 123.0 71.3 29.7 28.1 23.6 24.2Telmisartan, high-dose 131.0 78.4 117.0 70.6 214 27.8 28.5 24.9Placebo 130.0 78.4 126.0 75.5 26 23.5 — —
Drug plus lifestyle interventionsBerenson et al 198360 (6 mo) ADAPT program 116.6 77.7 109.0 70.8 27.6 26.9 26.5 23.6
Control 118.5 78.3 115.5 74.4 23.0 23.9 — —
Berenson et al 199061 (30 mo)b ADAPT program 116.6 77.7 118.0 73.5 1.4 24.2 23.6 21.7Control 118.5 78.5 122.0 75.2 3.5 23.3 — —
Lifestyle interventionsCouch et al 200862 (6 mo) DASH diet 129.4 80.4 120.1 75.2 29.3 25.2 0.1 21.2
Routine care 124.3 81.7 120.0 76.4 24.3 25.3 — —
Ewart et al 198733 (9 mo) Relaxation training 127.0 79.1 118.6 72.9 28.4 26.2 22.3 23.1No intervention 126.5 80.4 120.9 76.0 25.6 24.4 — —
Gregoski et al 201163 (3 mo) Meditation 119.4 68.1 116.6 66.3 22.8 21.8 24.4 22.4LifeSkills training 119.6 68.0 119.8 68.2 0.2 0.2 21.2 20.5Regular health education 121.4 69.3 121.0 68.7 20.4 20.6 — —
Hansen et al 199164 (3 mo) Extra physical education classes Not reported 24.9 23.8No extra classes — —
Howe et al 199165 (4 wk) Low sodium diet 115.0a 60.1a 112.6 59.1 Not reported 21.2 20.9High sodium diet 113.8 60 — —
DASH, Dietary Approaches to Stop Hypertension; —, indicates that data is not available.a Values for total cohort; data not stratified according to treatment group.b Continuation of Berenson et al 1983 study.
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 495 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

Key Question 7: What Is theEffectiveness of Drug, Nondrug,and Combination InterventionsInitiated for the Treatment ofPrimary Hypertension in Children/Adolescents for Reducing AdverseHealth Outcomes in Adults Relatedto Primary Hypertension?
No RCTs examined the effectiveness ofinterventions for hypertension in chil-dren or adolescents for reducing clin-ical outcomes in adults.
Key Question 8: What Are theAdverse Effects of Drug, Nondrug,and Combination Interventions forTreating Primary Hypertension inChildren and Adolescents?
Drug Interventions
Twelve trials reported adverse eventswith drug therapy (Appendix 6).53–59,67–71
One study was rated good quality67; theremainderwereof fairquality.53–55,57–59,68–71
Four of the studies included childrenwithprimary hypertension,53,57–59 whereas theremainder included children with pri-mary or secondary hypertension.54,55,67–71
The number of children enrolled in thestudies ranged from 76 to 304, the meanage ranged from 12 to 14 years, and theduration of follow-up for reporting ad-verse events ranged from 4 weeks to 1year.
Serious adverse events were rarelyreported, and there were no deaths inany of the studies. One study of meto-prolol reported 1 case each of pneu-monia andmetometrorrhagia.53 Anotherstudy reported a case of near syncopeand an elevated creatinine in a patientwho received an incorrect dose of tel-misartan. A third study reported 8 seri-ous adverse events among 304 patients,although none were considered to betreatment related.55
Adverse event data were often poorlyreported, and most studies reportednoncomparative data from open-labelextensions of RCTs. Five studies ofmonotherapy reported similar rates of
adverse events in the intervention(range, 27–77%) and placebo groups(range, 25–66%).55,57,59,67,68 Childrentaking a combination of bisoprolol plushydrochlorothiazide had lower overallrates of adverse events compared withplacebo (53–75%, P = .05) after 12weeks of follow-up.56 Withdrawalscaused by adverse events ranged from0% to 7% in children receiving activetreatments53,54,56–59,67–71 and 0% to6.2% in placebo groups.53,56,58,59,67,68
Headache was the most common spe-cific adverse event in most studies:rates ranged from 2% to 33% in childrenreceiving active treatments,53,56,57,59,68,71
but only 2 studies reported rates forthe placebo group. One study reportedthat no headaches occurred in theplacebo group compared with 11%of active treatment patients,59 where-as in a second study, headache wasreported in 31% versus 26% (pla-cebo versus combination treatment,significance not reported).56 Othercommonly reported adverse eventsassociated with active treatmentswere cough, upper respiratory in-fections, and gastrointestinal events,including nausea and diarrhea, al-though specific rates were not alwaysreported.53,54,56–59,68–71
Two studies pooled adverse event datafrom selected drug trials submittedto the Food and Drug Administrationover a 7-year period; however, neitherstudyusedstandardsystematic reviewmethods.72,73 Pooled patient-level datafrom 1707 children from 10 placebo-controlled RCTs of 10 different activeagents72 revealed similar rates of ad-verse events between active treat-ment (0.83 events per patient) andplacebo groups (0.76 per patient) af-ter 2 to 4 weeks of follow-up (between-group P = .37). Pooled data from 8 RCTsof hypertensive children revealed nodifference in the incidence of coughbetween active treatment and placebogroups (3% in both groups; P = .86).73
Other Interventions
The fair-quality ADAPT of a propranololand chlorthalidone/lifestyle interventiondescribed inkeyquestion54reportednoadverse events.60,61 No studies of life-style modification alone reported ad-verse events.
DISCUSSION
Direct evidence linking screening ofchildren and adolescents for hyper-tension and delaying the onset orreducing the risk cardiovascular out-comes in adults is not available, andindirect evidence is sparse and of vari-able quality. We did not identify evidencefor the effectiveness of interventionsused to treat primary hypertension inchildren on lowering blood pressurelevels or reducing adverse health out-comes in adults. A summary of the evi-dence is provided in Table 2.
High-quality data on the diagnostic ac-curacy of blood pressuremeasurementto detect hypertension were alsosparse and suggest moderate sensi-tivities (0.65 and 0.72), with somewhathigher specificities (0.75 and 0.92).These data suggest that many childrenwho have elevated blood pressure onscreening will not have hypertension.There are also some data to suggestthat hypertension in childhood is as-sociated with hypertension in youngadults (OR range, 1.1–4.5; relative riskrange, 1.5–9) or has low to moderatesensitivities (0 and 0.63) and specific-ities (0.77 and 1) for predicting adulthypertension. Moreover, the associa-tion between childhood hypertensionand carotid intima media thicknessand microalbuminura in young adultswas also inconclusive, and direct evi-dence on other intermediate or finalhealth outcomes was lacking.
The effectiveness of antihypertensivemedications in children and adoles-cents has been examined in 7 trials, allof which were small and of short du-ration, and each examined a different
496 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

TABLE 2 Summary of Evidence
Number of Studies(Overall Quality)
Limitations Consistency Applicability toPrimary Care
Summary of Findings
Key question 1: Is screening for hypertension in children/adolescents effective in delaying the onset or reducing adverse health outcomes related to hypertension?No studies NA NA NA NA
Key question 2: What is the diagnostic accuracy of screening tests for elevated blood pressure in children/adolescents?2 trials (poor) Studies were flawed or not directly applicable
to an asymptomatic US population. Only 1included a comparisonwith a gold standardof ambulatory monitoring.
Consistent Low Sensitivity and specificity of office-basedscreening for hypertension was 0.65 and0.75 (positive predictive value, 0.37)compared with ambulatory screening in 1study of a referred population.
A second, school-based study comparing aninitial positive screen to subsequentdiagnosis of hypertension had sensitivity(0.72) and specificity (0.92), but the positivepredictive value was lower (0.17).
Key question 3: What is the association between hypertension in children/adolescents and hypertension and other intermediate outcomes in adults?10 cohort studies (poor) Studies used different thresholds for defining
elevated blood pressure and hypertensionin children and different definitions ofhypertension in adults. Studies hadmethodologic shortcomings.
Inconsistent Moderate Sensitivities and specificities of elevated bloodpressure or hypertension from childhood toadult hypertension ranged from0 to 0.66 andspecificities of 0.77 to 1. PPVs ranged from0.19 to 0.65. Five studies reported significantassociations between elevated bloodpressure in childhood and hypertension inadults, with ORs ranging from 1.1 to 4.5 andRRs of 1.5 to 9. Two studies reportedassociations between childhoodhypertension and carotid intima mediathickness in young adults, with conflictingfindings. One study reported a significantassociation between childhood hypertensionand microalbuminuria only in blackindividuals.
Key question 4: What are the adverse effects of screening for hypertension in children/adolescents, including labeling and anxiety?1 study (poor) Evidence limited to results from1, good-quality
studyNA (1 study) High Children labeled as hypertensive did not miss
more days of school in the year afterdiagnosis compared with prelabeling orcompared with nonhypertensive children.Other harms associated with screeningwere not reported.
Key question 5: What is the effectiveness of drug, nondrug, and combination therapies for treating primary hypertension in children/adolescents?14 RCTs (poor) Longest drug study duration was only 4 wk Consistent Moderate Children achieving normotensive status (on the
basis of varyingdefinitions) ranged from15%to86%inpatients takingdrugtreatmentsand11% to 48% in patients taking placebo.
For many studies, the proportion of childrenwith secondary hypertension was unclear
There were significant reductions ofmean SBP(range 2–10 mm Hg), and mean DBP (range0.4–8 mm Hg) with some drugs anddosages. The difference betweenintervention and placebo groups rangedfrom 0 to 9mm Hg for SBPand 0.5 to 10mmHg for DBP. However, reductions were oftenonly at higher doses of active treatments,and studies only lasted for 4 wk.
One school-based study of a drug plus lifestyleintervention reported a significant,sustained reduction in blood pressure in thecombination group versus the control group.
Studies of nondrug therapies were limited, andonly 1 study examining the effect ofadditional physical education classes inschool reported a sustainedmean reductionin blood pressure in for both boys and girls.
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 497 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

agent. Most importantly, their antihy-pertensive effects varied in magnitude,were not consistently present fora given agent for both SBP and DBP, andwere not consistently different fromplacebo or from baseline. Blood pres-sures inplacebogroupsoften improvedalong with those of the interventiongroup, suggesting regression to themean. From the limited data we iden-tified, medications appeared to be welltolerated, with no serious adverseeffects.
Interventions for treating elevatedblood pressure that involve lifestyleinterventions alone or in combinationwith an antihypertensive medicationfound inconsistent results. Of the 3studies that had positive results, in-creased physical education at schoolwas effective at reducing blood pres-sure in 1 study,64 whereas in a secondlonger-term school-based study, the
effects of an antihypertensive com-bined with a complex lifestyle program(the ADAPT program) were not sus-tained,60,61 and finally, a low sodiumdiet combined with personalized sup-port was only effective in girls.66
Themost important potential limitationof this review was the absence of anyevidence to address several of the keyquestions and the limited quantity andquality of evidence for others. This lackof evidence inevitably limits the con-clusions that can be drawn from thisreview. Second, our search strategy,although rigorous, may have failed toidentify relevant studies. We used ci-tation searching of included articlesand reviewed all articles identified bythe expert reviewers to augment oursearch strategy. We limited our searchto English language publications, whichcould have limited eligible studies.We cannot exclude the possibility of
publication and selective reportingbiases, but we were not able to formallytest for this. In addition, by includingonly studies where the interventionswere directed against treatment of hy-pertension (eg, rather than obesity),indirect evidence was excluded. Finally,identified studies had multiple defi-ciencies in reporting and methodology,which limited the data available foranalysis and interpretation. Limitationsincluded the lack of studies that exam-ined 1 intervention in .1 trial or obvi-ous clinical heterogeneity, precludingthe use of meta-analyses.
Future research in this area needs toaddress the followingmajor gaps in thecurrent state of evidence.
� Diagnostic accuracy of blood pres-sure measurement in primarycare and community settings forscreening children of varying agesand characteristics. This includes
TABLE 2 Continued
Number of Studies(Overall Quality)
Limitations Consistency Applicability toPrimary Care
Summary of Findings
Key question 6: What is the effectiveness of drug, nondrug, and combination therapies initiated for the treatment of primary hypertension in children/adolescents forreducing blood pressure and other intermediate outcomes in adults?No studies NA NA NA NA
Key question 7: What is the effectiveness of drug, nondrug, and combination therapies initiated for the treatment of primary hypertension in children/adolescents forreducing adverse health outcomes in adults related to primary hypertension?No studies NA NA NA NA
Key question 8: What are the adverse effects of drug, nondrug, and combination therapies for treating primary hypertension in children/adolescents?15 studies (13 RCTs, 2 FDA
analyses) (fair)Numerous trials from key question 5 did notreport comparative events rates betweenactive treatment and placebo arms, andadverse event rates overall ere not well-reported in most studies.
Consistent Moderate Studies of antihypertensive drugs in childrenand adolescents generally reported nosignificant difference between activetreatments and placebo in adverse eventrates or in withdrawals due to adverseevents. In one study, a combination ofbisoprolol and hydrochlorothiazide wasassociated with lower adverse event ratesthan placebo.
Four studies reported serious adverse events,although with the exception of 1 case ofsyncope due to a dosing error, seriousadverse events were generally not deemedtreatment related. Analysis of FDA datarevealed no significant difference betweendrug treatments and placebo in theincidence of specific adverse events,including headache (the most commonlyreported adverse event), cardiac events,gastrointestinal events, and cough.
No studies reported on harms associated withnondrug treatments.
FDA, Food and Drug Administration; NA, not applicable; PPV, positive predictive value; RR, relative risk.
498 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

identifying the number, frequency,and timing of readings neededto confirm or rule out hyperten-sion.74
� Adverse effects of screening, in-cluding health care utilization, bur-den on the family, and discomfortand anxiety for the child and fam-ily.
� Epidemiologic studies to describethe natural history of elevatedblood pressure and hypertensionin children and adolescents, id-entifying factors that predictpersistence into adulthood, andregression to normal based onbaseline characteristics such asage, BMI, and pattern of bloodpressure. Such studies need touse current definitions of hyper-tension and be of sufficient dura-tion to draw clinically usefulconclusions.74,75
� Epidemiologic studies to better de-fine thresholds used to definehypertension in children and ado-lescents and their association withboth structural (eg, carotid intimamedia thickening, left ventricularmass) and functional (eg, arterialstiffening) markers of target endorgan damage related to hyperten-sion.
� Longer-term trials of benefits andrisks of all antihypertensive agents(as monotherapy and in combina-tion) and evidence for both short-and long-term safety. Given theexpected duration of antihyperten-sive therapy, the absence of long-term safety data is a significantlimitation.
� Large, controlled, good-quality trialsof feasible nondrug interventionsfor children and adolescents usingmore sophisticated approaches tocomplex interventions to identifycomponents that provide the great-est benefit over prolonged periods.
CONCLUSIONS
The prevalence of hypertension inchildren and adolescents is increasingin the United States, largely driven byincreased BMI. Screening children forelevated blood pressure or hyperten-sion has the potential to shift themanagement of hypertension to youn-ger age groups and potentially reducefuture cardiovascular disease risk inadults. However, at present, the evi-denceneeded tosupport thesepracticesis limited. Although it would be logisti-cally (and ethically) very challengingto demonstrate the effects of inter-ventions in children and adolescents
with elevated blood pressure on car-diovascular outcomes occurring manydecades later in adults, there areclearly a number of outstanding re-search gaps that can be addressed byfeasible research designs in a muchshorter time frame. Increasingly, bloodpressure is being viewed within a par-adigm of overall cardiovascular riskstratification, along with other riskfactors, such as lipid profiles, insulinresistance, and BMI.16 We anticipatethat addressing these current gaps inthe evidence for blood pressure will becritical to add to clinicians’ ability toidentify children and adolescents withincreased cardiovascular risk and alsoto offer a balanced assessment of theoverall benefit of interventions to re-duce this risk and prevent future car-diovascular disease.
ACKNOWLEDGMENTSThe authors thank the responsibleMed-ical Officer at the Agency of HealthcareResearch and Quality, Iris Mabry-Hernandez, MD,MPH, and US PreventiveServices Task Force members KirstenBibbins-Domingo, PhD, MD, DavidGrossman, MD, MPH, BernadetteMelnyk, PhD, RN, CPNP/NPP, andWandaNicholson, MD, MPH. We also thankMatthew Gillman, MD, for providingclinical expertise.
REFERENCES
1. Lurbe E, Álvarez J, Redon J. Diagnosis andtreatment of hypertension in children. CurrHypertens Rep. 2010;12(6):480–486
2. Obarzanek E, Wu CO, Cutler JA, Kavey RE,Pearson GD, Daniels SR. Prevalence andincidence of hypertension in adolescentgirls. J Pediatr. 2010;157(3):461–467, 467,e1–e5
3. Din-Dzietham R, Liu Y, Bielo M-V, Shamsa F.High blood pressure trends in children andadolescents in national surveys, 1963 to2002. Circulation. 2007;116(13):1488–1496
4. Flynn JT, Falkner BE. The importance ofblood pressure screening in children.
J Pediatr. 2009;155(2):299–300, author re-ply 299–300
5. Brady TM, Solomon BS, Neu AM, Siberry GK,Parekh RS. Patient-, provider-, and clinic-level predictors of unrecognized elevatedblood pressure in children. Pediatrics.2010;125(6). Available at: www.pediatrics.org/cgi/content/full/125/6/e1286
6. Hansen ML, Gunn PW, Kaelber DC. Under-diagnosis of hypertension in children andadolescents. JAMA. 2007;298(8):874–879
7. Sun SS, Grave GD, Siervogel RM, Pickoff AA,Arslanian SS, Daniels SR. Systolic bloodpressure in childhood predicts hyperten-
sion and metabolic syndrome later in life.Pediatrics. 2007;119(2):237–246
8. Rosner B, Cook N, Portman R, Daniels S,Falkner B. Blood pressure differences byethnic group among United States childrenand adolescents. Hypertension. 2009;54(3):502–508
9. Falkner B, Gidding SS, Ramirez-Garnica G,Wiltrout SA, West D, Rappaport EB. The re-lationship of body mass index and bloodpressure in primary care pediatricpatients. J Pediatr. 2006;148(2):195–200
10. Sorof JM, Lai D, Turner J, Poffenbarger T,Portman RJ. Overweight, ethnicity, and the
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 499 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

prevalence of hypertension in school-agedchildren. Pediatrics. 2004;113(3 pt 1):475–482
11. Moore WE, Eichner JE, Cohn EM, ThompsonDM, Kobza CE, Abbott KE. Blood pressurescreening of school children in a multira-cial school district: the Healthy Kids Pro-ject. Am J Hypertens. 2009;22(4):351–356
12. Chiolero A, Cachat F, Burnier M, Paccaud F,Bovet P. Prevalence of hypertension inschoolchildren based on repeated meas-urements and association with overweight.J Hypertens. 2007;25(11):2209–2217
13. Liao CC, Su TC, Chien KL, et al. Elevatedblood pressure, obesity, and hyperlipid-emia. J Pediatr. 2009;155(1):79–83, 83, e1
14. Jago R, Harrell JS, McMurray RG, EdelsteinS, El Ghormli L, Bassin S. Prevalence ofabnormal lipid and blood pressure valuesamong an ethnically diverse population ofeighth-grade adolescents and screeningimplications. Pediatrics. 2006;117(6):2065–2073
15. Centers for Disease Control and Pre-vention. Overweight and obesity: data andstatistics. Available at: www.cdc.gov/obe-sity/childhood/data.html. Accessed Decem-ber 3, 2012
16. Friedemann C, Heneghan C, Mahtani K,Thompson M, Perera R, Ward AM. Cardio-vascular disease risk in healthy childrenand its association with body mass index:systematic review and meta-analysis. BMJ.2012;345:e4759
17. Muntner P, He J, Cutler JA, Wildman RP,Whelton PK. Trends in blood pressureamong children and adolescents. JAMA.2004;291(17):2107–2113
18. Jung FF, Ingelfinger JR. Hypertension inchildhood and adolescence. Pediatr Rev.1993;14(5):169–179
19. Hohn AR, Dwyer KM, Dwyer JH. Bloodpressure in youth from four ethnic groups:the Pasadena Prevention Project. J Pediatr.1994;125(3):368–373
20. Flynn JT. Evaluation and management ofhypertension in childhood. Prog PediatrCardiol. 2001;12(2):177–188
21. Viera AJ, Neutze DM. Diagnosis of sec-ondary hypertension: an age-based ap-proach. Am Fam Physician. 2010;82(12):1471–1478
22. Srinivasan SR, Myers L, Berenson GS.Changes in metabolic syndrome variablessince childhood in prehypertensive andhypertensive subjects: the Bogalusa HeartStudy. Hypertension. 2006;48(1):33–39
23. Rademacher ER, Jacobs DR Jr, Moran A,Steinberger J, Prineas RJ, Sinaiko A. Re-lation of blood pressure and body massindex during childhood to cardiovascular
risk factor levels in young adults. JHypertens. 2009;27(9):1766–1774
24. US Preventive Services Task Force. Guide toClinical Preventive Services: PeriodicUpdates. 3rd ed. Rockville, MD: Agency forHealthcare Research and Quality; 2003
25. Thompson M, Bougatsos C, Dana T, BlazinaI, Norris S. Screening for Hypertension inChildren and Adolescents to Prevent Car-diovascular Disease: Systematic Review forthe U.S. Preventive Services Task Force.Rockville, MD: Agency for Healthcare Re-search and Quality
26. Harris RP, Helfand M, Woolf SH, et al;Methods Work Group, Third US PreventiveServices Task Force. Current methods ofthe US Preventive Services Task Force:a review of the process. Am J Prev Med.2001;20(3 suppl):21–35
27. US Preventive Services Task Force. Proceduremanual: section 4 evidence report development.Available at: www.uspreventiveservicestaskforce.org/uspstf08/methods/procmanual4.htm.Accessed December 3, 2012
28. Whitlock EP, O’Connor EA, Williams SB, BeilTL, Lutz KW. Effectiveness of weight man-agement interventions in children: a tar-geted systematic review for the USPSTF.Pediatrics. 2010;125(2). Available at: www.pediatrics.org/cgi/content/full/125/2/e396
29. Haney EM, Huffman LH, Bougatsos C, FreemanM, Steiner RD, Nelson HD. Screening andtreatment for lipid disorders in childrenand adolescents: systematic evidence re-view for the US Preventive Services TaskForce. Pediatrics. 2007;120(1). Available at:www.pediatrics.org/cgi/content/full/120/1/e189
30. Fixler DE, Laird WP. Validity of mass bloodpressure screening in children. Pediatrics.1983;72(4):459–463
31. Stergiou GS, Nasothimiou E, Giovas P,Kapoyiannis A, Vazeou A. Diagnosis of hy-pertension in children and adolescentsbased on home versus ambulatory bloodpressure monitoring. J Hypertens. 2008;26(8):1556–1562
32. Berenson GS, Dalferes E Jr, Savage D,Webber LS, Bao W. Ambulatory bloodpressure measurements in children andyoung adults selected by high and lowcasual blood pressure levels and parentalhistory of hypertension: the BogalusaHeart Study. Am J Med Sci. 1993;305(6):374–382
33. Ewart CK, Harris WL, Iwata MM, Coates TJ,Bullock R, Simon B. Feasibility and effec-tiveness of school-based relaxation in low-ering blood pressure. Health Psychol. 1987;6(5):399–416
34. Fixler DE, Laird WP, Fitzgerald V, Stead S,Adams R. Hypertension screening inschools: results of the Dallas study. Pedi-atrics. 1979;63(1):32–36
35. Kelsall JE, Watson AR. Should school nursesmeasure blood pressure? Public Health.1990;104(3):191–194
36. Michaud PA. Adolescent hypertension:a follow-up study in the community. RevEpidemiol Sante Publique. 1989;37(1):23–28
37. Miller FS III, Record NB Jr. Hypertensioncontrol in rural Maine. Franklin County highblood pressure program. J Maine MedAssoc. 1976;67(9):280–283
38. Rames LK, Clarke WR, Connor WE, ReiterMA, Lauer RM. Normal blood pressure andthe evaluation of sustained blood pressureelevation in childhood: the Muscatine study.Pediatrics. 1978;61(2):245–251
39. Reichman LB, Cooper BM, Blumenthal S,et al. Hypertension testing among highschool students. I. Surveillance proceduresand results. J Chronic Dis. 1975;28(3):161–171
40. Sailors EL. Project “hypertension alert”.J Sch Health. 1983;53(6):374–376
41. Sinaiko AR, Gomez-Marin O, Prineas RJ.“Significant” diastolic hypertension in pre-high school black and white children. Thechildren and adolescent blood pressureprogram. Am J Hypertens. 1988;1(2):178–180
42. Stern B, Heyden S, Miller D, Latham G, Kli-mas A, Pilkington K. Intervention study inhigh school students with elevated bloodpressures. Dietary experiment with poly-unsaturated fatty acids. Nutr Metab. 1980;24(3):137–147
43. Bao W, Threefoot SA, Srinivasan SR,Berenson GS. Essential hypertension pre-dicted by tracking of elevated blood pres-sure from childhood to adulthood: theBogalusa Heart Study. Am J Hypertens.1995;8(7):657–665
44. Beckett LA, Rosner B, Roche AF, Guo S. Se-rial changes in blood pressure from ado-lescence into adulthood. Am J Epidemiol.1992;135(10):1166–1177
45. Gillman MW, Cook NR, Rosner B, et al.Identifying children at high risk for thedevelopment of essential hypertension. JPediatr. 1993;122(6):837–846
46. Hoq S, Chen W, Srinivasan SR, Berenson GS.Childhood blood pressure predicts adultmicroalbuminuria in African Americans,but not in whites: the Bogalusa Heart Study.Am J Hypertens. 2002;15(12):1036–1041
47. Juhola J, Magnussen CG, Viikari JSA, et al.Tracking of serum lipid levels, blood pres-sure, and body mass index from childhoodto adulthood: the Cardiovascular Risk in
500 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

Young Finns Study. J Pediatr. 2011;159(4):584–590
48. Lauer RM, Clarke WR, Mahoney LT, Witt J.Childhood predictors for high adult bloodpressure. The Muscatine Study. Pediatr ClinNorth Am. 1993;40(1):23–40
49. Li S, Chen W, Srinivasan SR, et al. Child-hood cardiovascular risk factors andcarotid vascular changes in adulthood:the Bogalusa Heart Study. JAMA. 2003;290(17):2271–2276
50. Raitakari OT, Juonala M, Kähönen M, et al.Cardiovascular risk factors in childhoodand carotid artery intima-media thicknessin adulthood: the Cardiovascular Risk inYoung Finns Study. JAMA. 2003;290(17):2277–2283
51. Shear CL, Burke GL, Freedman DS, WebberLS, Berenson GS. Designation of childrenwith high blood pressure—considerationson percentile cut points and subsequenthigh blood pressure: the Bogalusa HeartStudy. Am J Epidemiol. 1987;125(1):73–84
52. Stenn PG, Noce A, Buck C. A study of thelabelling phenomenon in school childrenwith elevated blood pressure. Clin InvestMed. 1981;4(3–4):179–181
53. Batisky DL, Sorof JM, Sugg J, et al; Toprol-XLPediatric Hypertension Investigators. Effi-cacy and safety of extended release meto-prolol succinate in hypertensive children 6to 16 years of age: a clinical trial experience.J Pediatr. 2007;150(2):134–139, 139, e1
54. Flynn JT, Newburger JW, Daniels SR, et al;PATH-1 Investigators. A randomized, placebo-controlled trial of amlodipine in childrenwith hypertension. J Pediatr. 2004;145(3):353–359
55. Li JS, Flynn JT, Portman R, et al. The efficacyand safety of the novel aldosterone antag-onist eplerenone in children with hyper-tension: a randomized, double-blind, dose-response study. J Pediatr. 2010;157(2):282–287
56. Sorof JM, Cargo P, Graepel J, et al. Beta-blocker/thiazide combination for treatmentof hypertensive children: a randomizeddouble-blind, placebo-controlled trial.Pediatr Nephrol. 2002;17(5):345–350
57. Trachtman H, Frank R, Mahan JD, et al.Clinical trial of extended-release felodipinein pediatric essential hypertension. PediatrNephrol. 2003;18(6):548–553
58. Trachtman H, Hainer JW, Sugg J, Teng R,Sorof JM, Radcliffe J; Candesartan inChildren with Hypertension (CINCH)Investigators. Efficacy, safety, and phar-
macokinetics of candesartan cilexetil inhypertensive children aged 6 to 17 years.J Clin Hypertens (Greenwich). 2008;10(10):743–750
59. Wells TG, Portman R, Norman P, HaertterS, Davidai G, Fei Wang . Safety, efficacy,and pharmacokinetics of telmisartan inpediatric patients with hypertension.Clin Pediatr (Phila). 2010;49(10):938–946
60. Berenson GS, Voors AW, Webber LS, et al. Amodel of intervention for prevention ofearly essential hypertension in the 1980s.Hypertension. 1983;5(1):41–54
61. Berenson GS, Shear CL, Chiang YK, WebberLS, Voors AW. Combined low-dose medica-tion and primary intervention over a 30-month period for sustained high bloodpressure in childhood. Am J Med Sci. 1990;299(2):79–86
62. Couch SC, Saelens BE, Levin L, Dart K, Fal-ciglia G, Daniels SR. The efficacy of a clinic-based behavioral nutrition interventionemphasizing a DASH-type diet for adoles-cents with elevated blood pressure.J Pediatr. 2008;152(4):494–501
63. Gregoski MJ, Barnes VA, Tingen MS,Harshfield GA, Treiber FA. Breathingawareness meditation and LifeSkills Train-ing programs influence upon ambulatoryblood pressure and sodium excretionamong African American adolescents.J Adolesc Health. 2011;48(1):59–64
64. Hansen HS, Froberg K, Hyldebrandt N,Nielsen JR. A controlled study of eightmonths of physical training and reductionof blood pressure in children: the Odenseschoolchild study. BMJ. 1991;303(6804):682–685
65. Howe PR, Cobiac L, Smith RM. Lack of effectof short-term changes in sodium intake onblood pressure in adolescent school-children. J Hypertens. 1991;9(2):181–186
66. Sinaiko AR, Gomez-Marin O, Prineas RJ.Effect of low sodium diet or potassiumsupplementation on adolescent blood pres-sure. Hypertension. 1993;21(6 pt 2):989–994
67. Hazan L, Hernández Rodriguez OA, BhoratAE, Miyazaki K, Tao B, Heyrman R; Assess-ment of Efficacy and Safety of Olmesartanin Pediatric Hypertension Study Group. Adouble-blind, dose-response study of theefficacy and safety of olmesartan medox-omil in children and adolescents with hy-pertension. Hypertension. 2010;55(6):1323–1330
68. Li JS, Berezny K, Kilaru R, et al. Is the ex-trapolated adult dose of fosinopril safe andeffective in treating hypertensive children?Hypertension. 2004;44(3):289–293
69. Shahinfar S, Cano F, Soffer BA, et al. Adouble-blind, dose-response study of los-artan in hypertensive children. Am JHypertens. 2005;18(2 pt 1):183–190
70. Soffer B, Zhang Z, Miller K, Vogt BA, Sha-hinfar S. A double-blind, placebo-controlled,dose-response study of the effectivenessand safety of lisinopril for children withhypertension. Am J Hypertens. 2003;16(10):795–800
71. Wells T, Frame V, Soffer B, et al; EnalaprilPediatric Hypertension Collaborative StudyGroup. A double-blind, placebo-controlled,dose-response study of the effectivenessand safety of enalapril for children withhypertension. J Clin Pharmacol. 2002;42(8):870–880
72. Smith PB, Li JS, Murphy MD, Califf RM,Benjamin DK Jr. Safety of placebo controlsin pediatric hypertension trials. Hyperten-sion. 2008;51(4):829–833
73. Baker-Smith CM, Benjamin DK Jr, Califf RM,Murphy MD, Li JS, Smith PB. Cough in pe-diatric patients receiving angiotensin-converting enzyme inhibitor therapy orangiotensin receptor blocker therapy inrandomized controlled trials. Clin Phar-macol Ther. 2010;87(6):668–671
74. Chen X, Wang Y, Appel LJ, Mi J. Impacts ofmeasurement protocols on blood pressuretracking from childhood into adulthood:a metaregression analysis. Hypertension.2008;51(3):642–649
75. Tirosh A, Afek A, Rudich A, et al. Pro-gression of normotensive adolescents tohypertensive adults: a study of 26,980teenagers. Hypertension. 2010;56(2):203–209
76. Batisky DL. Obesity and the role of lifestyleand dietary intervention in the manage-ment of pediatric hypertension. J MedLiban. 2010;58(3):171–174
77. Juonala M, Viikari JSA, Hutri-Kähönen N,et al. The 21-year follow-up of the Cardio-vascular Risk in Young Finns Study: riskfactor levels, secular trends and east-westdifference. J Intern Med. 2004;255(4):457–468
78. Frank GC, Farris RP, Ditmarsen P, Voors AW,Berenson GS. An approach to primarypreventive treatment for children with highblood pressure in a total community. J AmColl Nutr. 1982;1(4):357–374
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 501 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
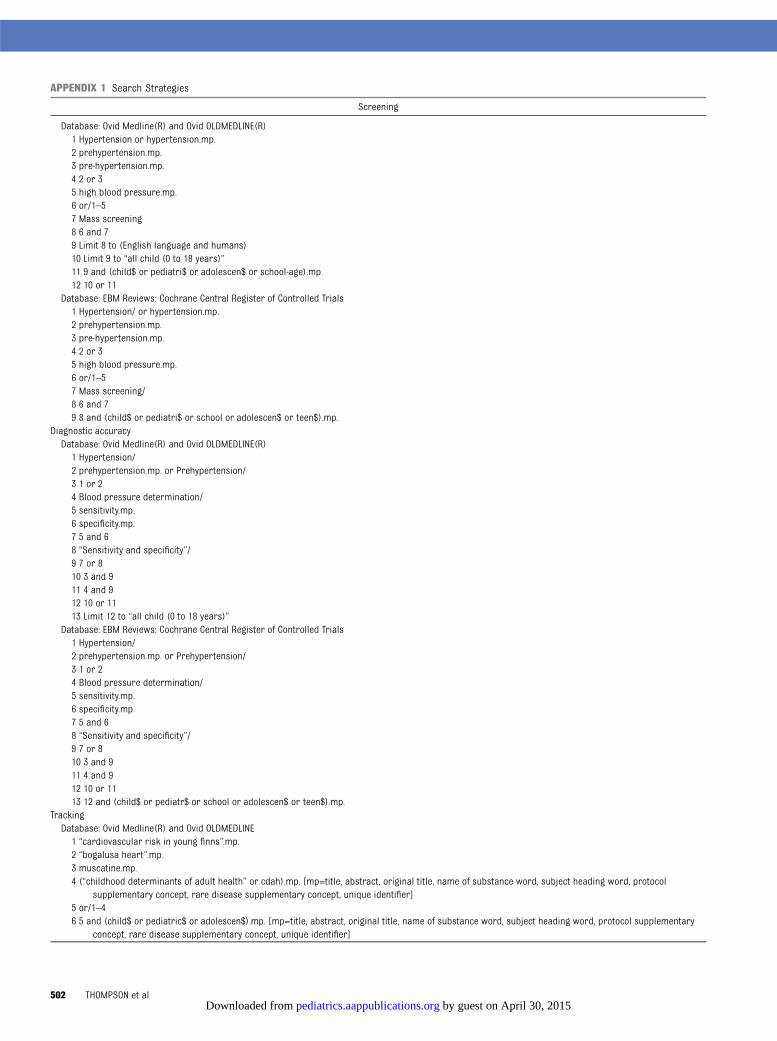
APPENDIX 1 Search Strategies
Screening
Database: Ovid Medline(R) and Ovid OLDMEDLINE(R)1 Hypertension or hypertension.mp.2 prehypertension.mp.3 pre-hypertension.mp.4 2 or 35 high blood pressure.mp.6 or/1–57 Mass screening8 6 and 79 Limit 8 to (English language and humans)10 Limit 9 to “all child (0 to 18 years)”11 9 and (child$ or pediatri$ or adolescen$ or school-age).mp.12 10 or 11
Database: EBM Reviews: Cochrane Central Register of Controlled Trials1 Hypertension/ or hypertension.mp.2 prehypertension.mp.3 pre-hypertension.mp.4 2 or 35 high blood pressure.mp.6 or/1–57 Mass screening/8 6 and 79 8 and (child$ or pediatri$ or school or adolescen$ or teen$).mp.
Diagnostic accuracyDatabase: Ovid Medline(R) and Ovid OLDMEDLINE(R)1 Hypertension/2 prehypertension.mp. or Prehypertension/3 1 or 24 Blood pressure determination/5 sensitivity.mp.6 specificity.mp.7 5 and 68 “Sensitivity and specificity”/9 7 or 810 3 and 911 4 and 912 10 or 1113 Limit 12 to “all child (0 to 18 years)”
Database: EBM Reviews: Cochrane Central Register of Controlled Trials1 Hypertension/2 prehypertension.mp. or Prehypertension/3 1 or 24 Blood pressure determination/5 sensitivity.mp.6 specificity.mp.7 5 and 68 “Sensitivity and specificity”/9 7 or 810 3 and 911 4 and 912 10 or 1113 12 and (child$ or pediatr$ or school or adolescen$ or teen$).mp.
TrackingDatabase: Ovid Medline(R) and Ovid OLDMEDLINE1 “cardiovascular risk in young finns”.mp.2 “bogalusa heart”.mp.3 muscatine.mp.4 (“childhood determinants of adult health” or cdah).mp. [mp=title, abstract, original title, name of substance word, subject heading word, protocol
supplementary concept, rare disease supplementary concept, unique identifier]5 or/1–46 5 and (child$ or pediatric$ or adolescen$).mp. [mp=title, abstract, original title, name of substance word, subject heading word, protocol supplementary
concept, rare disease supplementary concept, unique identifier]
502 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
APPENDIX 1 Continued
Screening
7 blood pressure.mp. or Blood Pressure/8 Hypertension/ or hypertension.mp.9 7 or 810 9 and (child$ or pediatric$ or adolescen$).mp.11 10 and adult$.mp. [mp=title, abstract, original title, name of substance word, subject heading word, protocol supplementary concept, rare disease
supplementary concept, unique identifier]12 Longitudinal studies/13 11 and 1214 6 or 1315 “Amsterdam Growth and Health Longitudinal Study”.mp.16 15 and (child$ or pediatric$ or adolescen$).mp.17 14 or 1618 17 not pregnancy.mp. [mp=title, abstract, original title, name of substance word, subject heading word, protocol supplementary concept, rare disease
supplementary concept, unique identifier]19 17 not infan$.mp. [mp=title, abstract, original title, name of substance word, subject heading word, protocol supplementary concept, rare disease
supplementary concept, unique identifier]20 18 or 1921 Limit 20 to (English language and humans)22 Atherosclerosis/23 Vascular diseases/24 Albuminuria/25 Cerebrovascular disorders/26 Hypertrophy, Left ventricular/27 Hypertension/28 or/22–2729 21 and 28
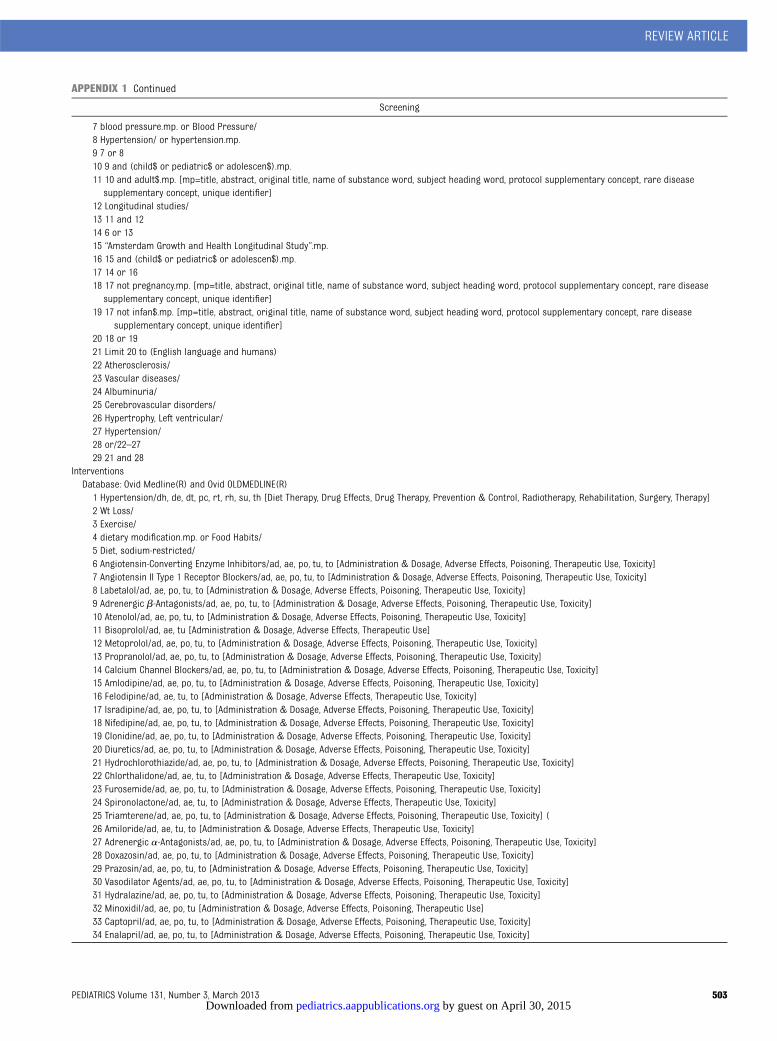
InterventionsDatabase: Ovid Medline(R) and Ovid OLDMEDLINE(R)1 Hypertension/dh, de, dt, pc, rt, rh, su, th [Diet Therapy, Drug Effects, Drug Therapy, Prevention & Control, Radiotherapy, Rehabilitation, Surgery, Therapy]2 Wt Loss/3 Exercise/4 dietary modification.mp. or Food Habits/5 Diet, sodium-restricted/6 Angiotensin-Converting Enzyme Inhibitors/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]7 Angiotensin II Type 1 Receptor Blockers/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]8 Labetalol/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]9 Adrenergic b-Antagonists/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]10 Atenolol/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]11 Bisoprolol/ad, ae, tu [Administration & Dosage, Adverse Effects, Therapeutic Use]12 Metoprolol/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]13 Propranolol/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]14 Calcium Channel Blockers/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]15 Amlodipine/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]16 Felodipine/ad, ae, tu, to [Administration & Dosage, Adverse Effects, Therapeutic Use, Toxicity]17 Isradipine/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]18 Nifedipine/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]19 Clonidine/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]20 Diuretics/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]21 Hydrochlorothiazide/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]22 Chlorthalidone/ad, ae, tu, to [Administration & Dosage, Adverse Effects, Therapeutic Use, Toxicity]23 Furosemide/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]24 Spironolactone/ad, ae, tu, to [Administration & Dosage, Adverse Effects, Therapeutic Use, Toxicity]25 Triamterene/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity] (26 Amiloride/ad, ae, tu, to [Administration & Dosage, Adverse Effects, Therapeutic Use, Toxicity]27 Adrenergic a-Antagonists/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]28 Doxazosin/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]29 Prazosin/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]30 Vasodilator Agents/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]31 Hydralazine/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]32 Minoxidil/ad, ae, po, tu [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use]33 Captopril/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]34 Enalapril/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 503 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX 1 Continued
Screening
35 Fosinopril/ad, ae, tu, to [Administration & Dosage, Adverse Effects, Therapeutic Use, Toxicity]36 Lisinopril/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]37 Losartan/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]38 (benazepril or quinapril or irbesartan or terazosin).mp.39 or/2–3840 Hypertension/41 39 and 4042 1 or 4143 Limit 42 to (English language and humans)44 Limit 43 to “all child (0 to 18 years)”
Database: EBM Reviews: Cochrane Central Register of Controlled Trials1 Wt Loss/2 Exercise/3 dietary modification.mp. or Food Habits/4 Diet, Sodium-Restricted/5 Angiotensin-Converting Enzyme Inhibitors/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]6 Angiotensin II Type 1 Receptor Blockers/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]7 Labetalol/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]8 Adrenergic b-Antagonists/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]9 Atenolol/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]10 Bisoprolol/ad, ae, tu [Administration & Dosage, Adverse Effects, Therapeutic Use]11 Metoprolol/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]12 Propranolol/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]13 Calcium Channel Blockers/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]14 Amlodipine/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]15 Felodipine/ad, ae, tu, to [Administration & Dosage, Adverse Effects, Therapeutic Use, Toxicity]16 Isradipine/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]17 Nifedipine/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]18 Clonidine/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]19 Diuretics/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]20 Hydrochlorothiazide/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]21 Chlorthalidone/ad, ae, tu, to [Administration & Dosage, Adverse Effects, Therapeutic Use, Toxicity]22 Furosemide/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]23 Spironolactone/ad, ae, tu, to [Administration & Dosage, Adverse Effects, Therapeutic Use, Toxicity]24 Triamterene/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]25 Amiloride/ad, ae, tu, to [Administration & Dosage, Adverse Effects, Therapeutic Use, Toxicity]26 Adrenergic a-Antagonists/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]27 Doxazosin/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]28 Prazosin/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]29 Vasodilator Agents/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]30 Hydralazine/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]31 Minoxidil/ad, ae, po, tu [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use]32 Captopril/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]33 Enalapril/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]34 Fosinopril/ad, ae, tu, to [Administration & Dosage, Adverse Effects, Therapeutic Use, Toxicity]35 Lisinopril/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]36 Losartan/ad, ae, po, tu, to [Administration & Dosage, Adverse Effects, Poisoning, Therapeutic Use, Toxicity]37 (benazepril or quinapril or irbesartan or terazosin).mp.38 or/1–3739 Blood Pressure/40 38 and 39
Systematic reviewsDatabase: EBM Reviews: Cochrane Database of Systematic Reviews1 hypertension.ti.2 blood pressure.ti.3 1 or 24 3 and (child$ or pediatri$ or school or adolescen$ or teen$).mp.5 4 not (neonat$ or newborn or infan$).ti.6 5 not (pregnan$ or postpartum).ti.
504 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX 2 Inclusion and Exclusion Criteria
Key Questions Inclusion Criteria Exclusion Criteria
Settings All Primary care clinics, well-child/adolescent visits, school orcommunity-based screening
Pediatric specialty/subspecialty clinics, inpatient, or long-termcare settings, emergency or urgent care facilities
Populations 1, 2, and 4 Asymptomatic, otherwise healthy children and adolescents, 0–18y of age, with no known diagnosis of hypertension
Pregnant adolescents
3 and 5–8: Primary hypertension defined as average blood pressurebetween 95th percentile and 5 mm Hg above the 99thpercentile
Majority of study population included secondary hypertension
Interventions 1–4: Blood pressure measurements using auscultatory oroscillometric devices that can be performed in a primary careclinic
24-h, ambulatory, or home-based blood pressuremeasurements.Diagnostic tests or investigations used to identify or confirmpossible causes of secondary hypertension
5–8: Drug: Antihypertensive medications which are currently FDA-approved for use in children/adolescents
Interventions for treatment of secondary hypertension
Lifestyle: Diet, exercise, etc. Interventions where reduction in blood pressure was nota primary objective of the study (eg, weight loss studies)
Outcomes 4, 5, and 6: Blood pressure Measures of cognitive functionLeft ventricular hypertrophy (defined using left ventricular mass
index and/or measures of left ventricular geometry)Bloodpressurevariability, suchasdiurnalvariationsornocturnalblood pressure dipping
Urinary albumin excretion (microalbuminuria) Arterialwall dysfunction, includingmeasuresofarterial stiffness,pulse wave velocity, or augmentation index
Intima-medial thickness (measured at carotid and/or femoralarteries)
Metabolicmeasures, eg,measuresof impairedglucose tolerance,levels of insulin, lipid profiles, homocysteine levels
Retinal vascular changes uric acid levelsInflammatory markers including C-reactive proteinBody changes in weight or BMI
1 and 7: Severe visual impairment Studies reporting intermediate outcomesStage IV or V chronic kidney diseaseCardiovascular events, including ischemic heart disease, heart
failureCerebrovascular events, including hemorrhagic and thrombotic
stroke, Hypertensive encephalopathyMortality (all-cause and disease-specific)
2 Measures of predictive validity of screening tests (eg, predictivevalue, likelihood ratios, sensitivity, specificity)
Studies that do not provide enough data to recreate 23 2 tablesor calculate sensitivity and specificity
Studies that do not use a true reference standard forcomparison
3 Measures of association (eg, odds ratio; risk ratio, sensitivity,specificity, correlation or regression coefficients)
Studies not reporting measures of association
8 Side effects of hypertension treatments or interventions —
Study designs 1 Randomized controlled trials, controlled clinical trials,observational studies with a comparison group (eg,comparative cohort and case-control studies), and systematicreviews
Study designs other than those specified
2 Studies of predictive validity that compare with a referencestandard (eg, ambulatory monitoring)
Study designs other than those specified
3 Longitudinal cohort and epidemiology studies Study designs other than those specified4 and 8 Randomized controlled trials, controlled clinical trials,
observational studies with a comparison group (eg, largecohort and case-control studies), and systematic reviews. Ifnone were identified, uncontrolled before-after studies wereexamined.
Study designs other than those specified
5–7 Randomized controlled trials, controlled clinical trials,observational studies with a comparison group (eg, largecohort and case-control studies), and systematic reviews
Study designs other than those specified
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 505 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
3DiagnosticAccuracy
ofScreeningforElevated
BloodPressure
inChildrenandAdolescents
Study,
Year
Screening
Test
ReferenceStandard
DefinitionofaPositive
ScreeningExam
ination
Population
Sensitivity
Specificity
PositivePredictive
Value
NegativePredictive
Value
Quality
Rating
Fixler and
Laird
1983
30
Threemeasureswith
mercury
manom
eter
measuredatleast4
wkapart
Initialscreeningresults
comparedwith
subsequent
measures
SBPor
DBP$95th
percentilebasedon
norm
ativelevelsfor
thestudy
population
n=9017;eighth
graderswith
follow-
upat10th
grade;
meanagenot
reported;allwerein
eighthgradeattim
eofinitialscreening:
53%male,44%
black,42%white,
14%Hispanic
Initialpositivescreen
versus
subsequent
screens:0.72
(95%
CI,0.65–0.78)
Initialpositivescreen
versus
subsequent
positivescreening
test:0.92(95%
CI,
0.91–0.92)
Initialpositivescreen
versus
subsequent
positivescreening
test:0.17(95%
CI,
0.15–0.2)
Initialpositivescreen
versus
subsequent
positivescreening
test:0.993
(95%
CI,
0.991–0.994)
Fair
Stergiou
etal
2008
31
Threeaveraged
measurementswith
mercury
sphygm
omanom
eter,
measuredin
nondom
inant
arminsittingposition
after
5minat
rest
24-ham
bulatory
bloodpressure
measurements
SBPor
DBP$95th
percentilebasedon
USnorm
ativeblood
pressure
tables
N=102;100%
referred
forscreening;mean
age13
y(SD,3;
range,6–18);63%
male;race
not
reported
Positiveam
bulatory
resultversus
positiveclinicresult:
0.65
(95%
CI,0.45–
0.80)
Positiveam
bulatory
resultversus
positiveclinicresult:
0.75
(95%
CI,0.63–
0.84)
Positiveam
bulatory
resultversus
positiveclinicresult:
0.37
(95%
CI,0.28–
0.47)
Positiveam
bulatory
resultversus
positiveclinicresult:
0.63
(95%
CI,0.53–
0.72)
Fair
506 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
4StudiesTracking
Hypertension
From
Childhood
toAdulthood
Author,Year,andStudyName
(Follow-up)
DefinitionofHTNin
Childhood
DefinitionofHTNin
Adulthood
Outcom
esQuality
Considerations
Recruitm
ent
Attrition:%
with
completedata,%
oforiginalNat
follow-up
Measurement
MethodStated
for
Both
TimePeriods?
StatisticalAnalysisand
Adjusted
Variables
Bloodpressure
outcom
esBaoetal1995
43;Bogalusa
HeartS
tudy
(15y)
.80th
percentile
SBP.140mmHg
orDB
P.90
mmHg
orever
treatedfor
hypertension
Hypertension
atfollow-up,
baselinehighestS
BPquintileversus
otherSBP
quintiles:
Unclear;datafrom
1505
subjectswho
completed
baseline
andfollow-upsurveys
(of3865atbaseline)
Noloss
(Cohortselected
basedon
availability
ofdata;39%
oforiginal
cohortcompleted
both
surveys)
Yes
Logisticregression;age,
race,sex,SBP,DBP,
BMI,change
inBM
I
18%(54/301)
vs.5%(60/
1204);risk
ratio
3.6;95%
CI,2.5–5.1
Hypertension
atfollow-up,
baselinehighestD
BPquintileversus
otherDB
Pquintiles:
15%(45/301)
vs.6%(72/
1204);risk
ratio
2.5;95%
CI,1.8–3.6
Beckettetal19924
4 ;Fels
Longitudinal
Study(20y)
SBPnotd
efined
DBP.90
mmHg
DBP80
vs.60mmHg
atage
15andpresence
ofhypertension
atage35:
Unclear;datafrom
523
subjectswho
completed
baseline
andfollow-upsurveys
(of976
atbaseline)
Noloss
(Cohortselected
basedon
availability
ofdata;54%
oforiginal
cohortcompleted
both
surveys)
Nonotapplicable
Males:riskratio
3.0;females:
risk
ratio
4.5
DBP85
vs.60mmHg
atage
15andpresence
ofhypertension
atage35:
Males:riskratio
3.9;
females:riskratio
6.6
DBP90
vs.60mmHg
atage
15andpresence
ofhypertension
atage35:
Males:riskratio
4.9;
females:riskratio
9.0
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 507 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
4Continued
Author,Year,andStudyName
(Follow-up)
DefinitionofHTNin
Childhood
DefinitionofHTNin
Adulthood
Outcom
esQuality
Considerations
Recruitm
ent
Attrition:%
with
completedata,%
oforiginalNatfollow-up
Measurement
MethodStated
for
Both
TimePeriods?
StatisticalAnalysisand
Adjusted
Variables
Gillm
anetal1993
45;Study
not
named
(12y)
.90th
percentile(SBP:
113mmHg,w
ithin
study)
.90th
percentile(SBP:
139mmHg,w
ithin
study)
Positivepredictivevalue,
sensitivity,and
specificity
ofBP
atage10
predicting
BP.
90th
percentileat
age20:
Childrenfrom
asingle
schoolinEastBoston,
MA;samplingmethod
unclear
6%(20/337)
attrition
Yes
notapplicable
SBP,males:
.75th
percentile(108
mmHg):0.26,0.59,0.80
.90th
percentile(113
mmHg):0.35,0.33,0.93
.95th
percentile(117
mmHg):0.44,0.17,0.97
.99thpercentile(123
mmHg):0.58,0.04,.0.99
SBP,females:
.75th
percentile(108
mmHg):0.27,0.66,0.79
.90th
percentile(114
mmHg):0.39,0.36,0.94
.95th
percentile(118
mmHg):0.48,0.20,0.98
.99thpercentile(125
mmHg):0.65,0.04,.0.99
DBP,males:
.75th
percentile(68
mmHg):0.21,0.34,0.82
.90th
percentile(71
mmHg):0.24,0.16,0.93
.95th
percentile(73
mmHg):0.27,0.08,0.97
.99thpercentile(77
mmHg):0.34,0.01,.0.99
DBP,females:
.75th
percentile(67
mmHg):0.19,0.49,0.77
.90th
percentile(71
mmHg):0.24,0.23,0.92
.95th
percentile(74
mmHg):0.30,0.10,0.98
.99thpercentile(78
mmHg):0.38,0.02,.0.99
508 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
4Continued
Author,Year,andStudyName
(Follow-up)
DefinitionofHTNin
Childhood
DefinitionofHTNin
Adulthood
Outcom
esQuality
Considerations
Recruitm
ent
Attrition:%
with
completedata,%
oforiginalNatfollow-up
Measurement
MethodStated
for
Both
TimePeriods?
StatisticalAnalysisand
Adjusted
Variables
Juholaetal2011
47;Cardio-
vascular
Risk
inYoungFinnsStudy(27y)
$95th
percentile
Unclear
Prehypertensionor
hypertension
inadulthoodandBP
$95th
percentileinchildhood:
Finnishchildrenand
adolescentsaged
3,6,
9,12,and
15y
random
lysampled
from
5cities
38.7%(1392/3596)lostto
follow-upat27
yYes
Logisticregression;age,
sex,race,study
year
Female,ages
6and9:OR
2.4
(95%
CI,1.1–5.2)
Female,ages
12,15,and18:
OR2.3(95%
CI,1.6–3.5)
Otherpublication:Juonalaetal
2004
77Males,ages6and9:OR
2.8
(95%
CI,1.5–5.1)
Males,ages12,15,and18:
OR2.1(95%
CI,1.5–3.1)
PPV,sensitivity,specificityof
BP.95%percentilein
childhood
and
hypertension
inadulthood
Allages6–18:0.44;0.1;0.97
Laueretal1993
48;M
uscatine
Study(unclear)
Unclear;results
reported
for.90th
percentile
SBPor
DBP.90th
percentile(cohort
specific)
24%ofchildrenwith
BP.90th
percentilehadBP
.90th
percentilein
adulthood;risk
ratio
2.4
(P,
.001)
Unclear;datafrom
2445
subjectswho
completed
baseline
andfollow-upsurveys
(num
beratbaseline
notreported)
Noloss
(Cohortselected
basedon
availability
ofdata)
Yes
notapplicable
39%ofchildrenwith
SBP
.90th
percentilehad
SBP.80th
percentilein
adulthood;risk
ratio
1.9
(P,
.001)
17%ofchildrenwith
DBP
.90th
percentilehad
DBP.90th
percentilein
adulthood;risk
ratio
1.7
(P,
.001)
32%ofchildrenwith
DBP
.90th
percentilehad
DBP.80th
percentilein
adulthood;risk
ratio
1.5
(P,
.001)
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 509 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
4Continued
Author,Year,andStudyName
(Follow-up)
DefinitionofHTNin
Childhood
DefinitionofHTNin
Adulthood
Outcom
esQuality
Considerations
Recruitm
ent
Attrition:%
with
completedata,%
oforiginalNatfollow-up
Measurement
MethodStated
for
Both
TimePeriods?
StatisticalAnalysisand
Adjusted
Variables
Shearetal1987
51;Bogalusa
HeartS
tudy
(8y)
Notreported
$140/90
mmHg
SBP$80th
percentileat
years1,4,and6and
hypertensive
atfollow-
up:
Datafrom
1501
subjects
who
completed
baselineandfollow-up
surveys(of4238
subjectsatbaseline)
Noloss
(cohortselected
basedon
availability
ofdata;35%
oforiginal
subjectscompleted
both
surveys)
Yes
notapplicable
Sensitivity:0.27;Specificity:
0.95
DBP$80th
percentileat
years1,4,and6and
hypertensive
atfollow-
up:
Sensitivity:0.33;Specificity:
0.96
SBP$90th
percentileat
years1,4,and6and
hypertensive
atfollow-
up:
Sensitivity:0.13;Specificity:
0.99
DBP$90th
percentileat
years1,4,and6and
hypertensive
atfollow-
up:
Sensitivity:0.07;Specificity:
0.99
SBP$95th
percentileat
years1,4,and6and
hypertensive
atfollow-
up:
Sensitivity:0.07;Specificity:
1.0
DBP$95th
percentileat
years1,4,and6and
hypertensive
atfollow-
up:
Sensitivity:0.0;Specificity:
1.0
510 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
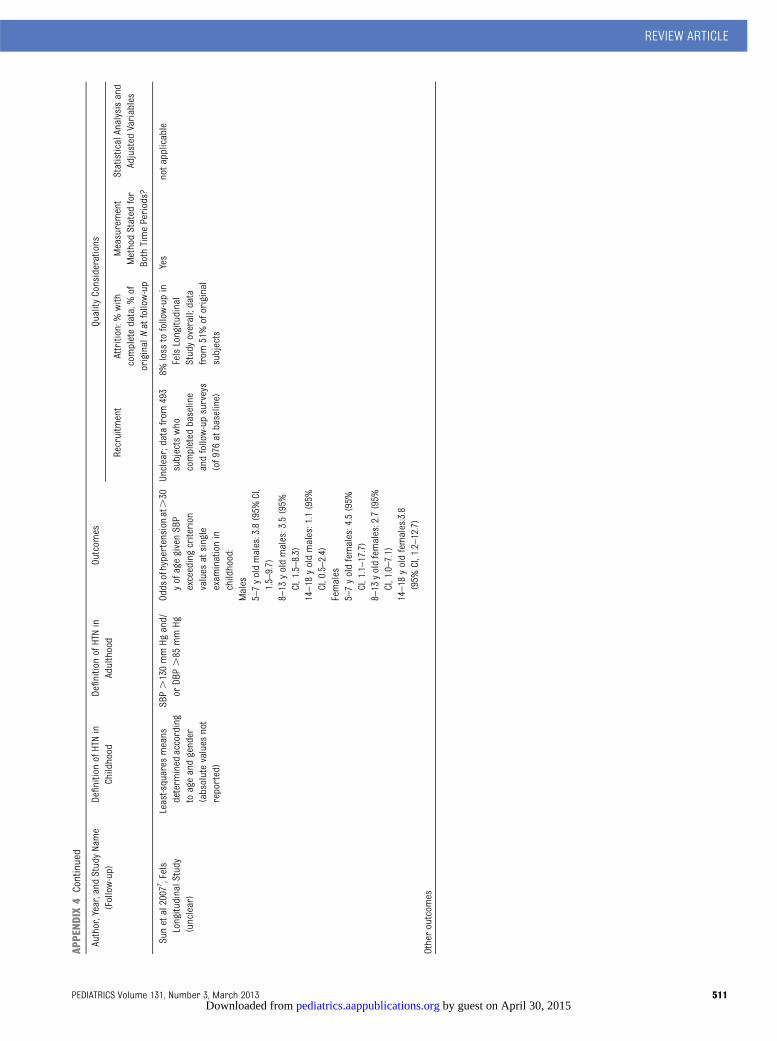
APPENDIX
4Continued
Author,Year,andStudyName
(Follow-up)
DefinitionofHTNin
Childhood
DefinitionofHTNin
Adulthood
Outcom
esQuality
Considerations
Recruitm
ent
Attrition:%
with
completedata,%
oforiginalNat
follow-up
Measurement
MethodStated
for
Both
TimePeriods?
StatisticalAnalysisand
Adjusted
Variables
Sunetal2007
7 ;Fels
LongitudinalStudy
(unclear)
Least-squares
means
determ
ined
according
toageandgender
(absolutevalues
not
reported)
SBP.130mmHg
and/
orDB
P.85
mmHg
Odds
ofhypertension
at.30
yofagegivenSBP
exceedingcriterion
values
atsingle
exam
inationin
childhood:
Unclear;datafrom
493
subjectswho
completed
baseline
andfollow-upsurveys
(of976
atbaseline)
8%loss
tofollow-upin
FelsLongitudinal
Studyoverall;data
from
51%oforiginal
subjects
Yes
notapplicable
Males
5–7yoldmales:3.8(95%
CI,
1.5–9.7)
8–13
yoldmales:3.5(95%
CI,1.5–8.3)
14–18
yoldmales:1.1(95%
CI,0.5–2.4)
Females
5–7yoldfemales:4.5(95%
CI,1.1–17.7)
8–13
yoldfemales:2.7(95%
CI,1.0–7.1)
14–18
yoldfemales:3.8
(95%
CI,1.2–12.7)
Otheroutcom
es
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 511 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
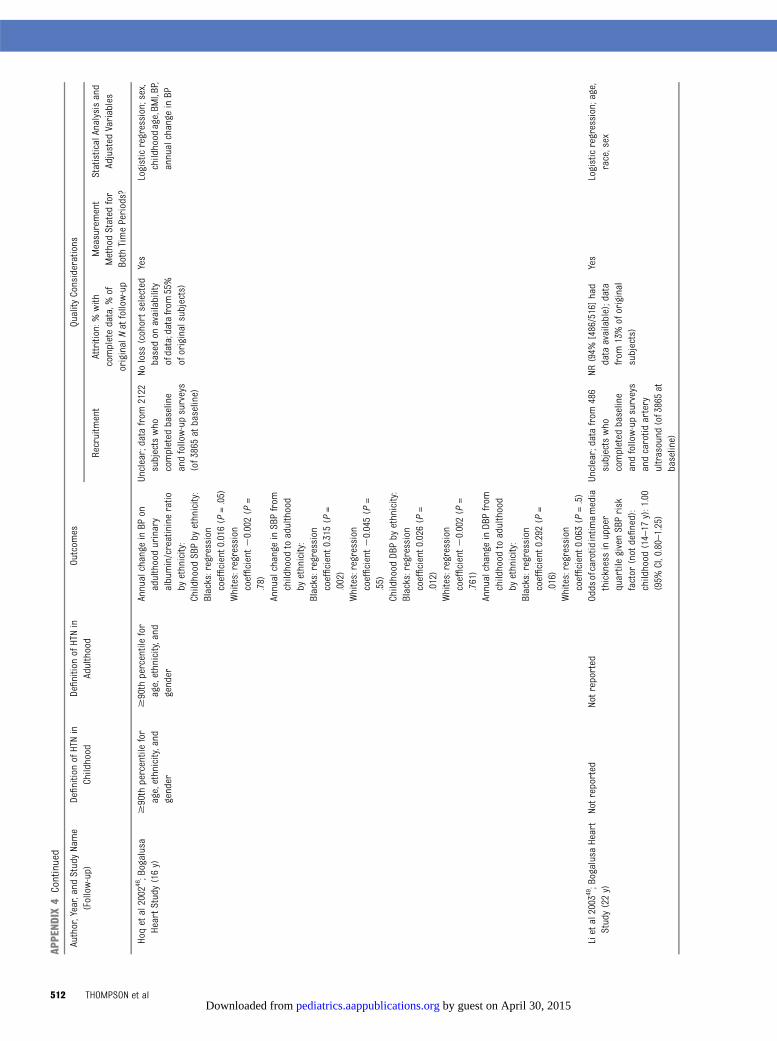
APPENDIX
4Continued
Author,Year,andStudyName
(Follow-up)
DefinitionofHTNin
Childhood
DefinitionofHTNin
Adulthood
Outcom
esQuality
Considerations
Recruitm
ent
Attrition:%
with
completedata,%
oforiginalNatfollow-up
Measurement
MethodStated
for
Both
TimePeriods?
StatisticalAnalysisand
Adjusted
Variables
Hoqetal2002
46;Bogalusa
HeartS
tudy
(16y)
$90th
percentilefor
age,ethnicity,and
gender
$90th
percentilefor
age,ethnicity,and
gender
Annualchange
inBP
onadulthoodurinary
albumin/creatinineratio
byethnicity:
Unclear;datafrom
2122
subjectswho
completed
baseline
andfollow-upsurveys
(of3865atbaseline)
Noloss
(cohortselected
basedon
availability
ofdata;datafrom
55%
oforiginalsubjects)
Yes
Logisticregression;sex,
childhood
age,BM
I,BP,
annualchange
inBP
Childhood
SBPby
ethnicity:
Blacks:regression
coefficient0.016
(P=.05)
Whites:regression
coefficient2
0.002(P
=.78)
Annualchange
inSBPfrom
childhood
toadulthood
byethnicity:
Blacks:regression
coefficient0.315
(P=
.002)
Whites:regression
coefficient2
0.045(P
=.55)
Childhood
DBPby
ethnicity:
Blacks:regression
coefficient0.026
(P=
.012)
Whites:regression
coefficient2
0.002(P
=.761)
Annualchange
inDB
Pfrom
childhood
toadulthood
byethnicity:
Blacks:regression
coefficient0.292
(P=
.016)
Whites:regression
coefficient0.063
(P=.5)
Lietal2003
49;BogalusaHeart
Study(22y)
Notreported
Notreported
Odds
ofcarotid
intim
amedia
thicknessinupper
quartilegivenSBPrisk
factor
(notdefined):
childhood
(14–17
y):1.00
(95%
CI,0.80–1.25)
Unclear;datafrom
486
subjectswho
completed
baseline
andfollow-upsurveys
andcarotid
artery
ultrasound
(of3865at
baseline)
NR(94%
[486/516]had
dataavailable);data
from
13%oforiginal
subjects)
Yes
Logisticregression;age,
race,sex
512 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
4Continued
Author,Year,andStudyName
(Follow-up)
DefinitionofHTNin
Childhood
DefinitionofHTNin
Adulthood
Outcom
esQuality
Considerations
Recruitm
ent
Attrition:%
with
completedata,%
oforiginalNatfollow-up
Measurement
MethodStated
for
Both
TimePeriods?
StatisticalAnalysisand
Adjusted
Variables
Raitakarietal2003
50;
Cardiovascular
Risk
inYoungFinnsStudy(21y)
$80th
percentile
$80th
percentile
RelationshipbetweenSBP
.80th
percentileatage
12–18
(meanage14.9y)
andcarotid
intim
amedia
thickness21
ylater:
regression
coefficient
0.013(SE0.003);P
,.001
Finnishchildrenand
adolescentsaged
3,6,
9,12,and
15y
random
lysampled
from
5cities
38%(1367/3596)lostto
follow-upat21
yYes
Logisticregression;age,
sex
BMI,body
massindex;BP,blood
pressure;DBP,diastolicbloodpressure;NR,notreported;PPV,positive
predictivevalue;SBP,systolicbloodpressure.
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 513 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
5Interventions
forHypertension
inChildrenandAdolescents
Author,Year(Quality
Rating)
StudyDesign
and
SettingDuration
NDemographicCharacteristics
Intervention
ProportionofPatientsAchieving
#95th
PercentileofBloodPressure
forAge,Gender,and
Height
BloodPressure
(mmHg)
Drug
interventions
Batisky
etal2007
53
(fair)
RCT
140
Meanage13
(SD2.8)
yGroupA:MetoprololER0.2mg/kg
Groups
A–Cpooled:46%
(95%
CI,37–
55)
Meanchange
from
baseline,SBP:
28sites
70%male
GroupB:MetoprololER1.0mg/kg
GroupB:26%(95%
CI,8–44)
GroupA:25.2(95%
CI,2
7.7to22.6)
UnitedStates
26%black
GroupC:MetoprololER2.0mg/kg
GroupB:27.7(95%
CI,2
11.3to24.0)
4wk
MeanSBP:132mmHg
GroupD:Placebo
GroupC:26.3(95%
CI,2
8.7to23.8)
MeanDB
P:78
mmHg
GroupD:21.9(95%
CI,2
5.5to
1.8)
74%BM
I$95%percentile
Meanchange
from
baseline,DB
P:GroupA:23.1(95%
CI,2
5.7to20.5)
GroupB:24.9(95%
CI,2
8.6to21.3)
GroupC:27.5(95%
CI,2
10.0to25.0)
GroupD:22.1(95%
CI,2
5.7to
1.5)
Flynnetal2004
54
(fair)
RCTcrossover
268
Meanage12
(SD3.3)
yStudyPhase2(includedplacebo
comparison)
SBP
Phase2results
49sitesinNorthandSouthAm
erica
MeanSBP:137.9(SD12.7)
mmHg
GroupA:Am
lodipine
2.5mg/day
GroupA:40%
Meanchange
from
baseline,SBP:
4wk
MeanDB
P:74.2(SD11.6)
mmHg
GroupB:Am
lodipine
5.0mg/day
GroupB:35%
GroupA:26.96
12.5(P=NS)(P=.05
versus
placebo)
31.3%(84/268)
primary
hypertension
GroupC:Placebo
GroupC:30%
GroupB:28.76
13.3(P
=NS)(2
3.6
612.7,P
=.01versus
placebo)
DBP
GroupC:23.66
12.7(P
=NS)
GroupA:42%
Meanchange
from
baseline,DB
P:GroupB:75%
GroupA:24.26
10.7(P
=NS)
GroupC:48%
GroupB:24.46
10.2(P
=NS)
GroupC:20.46
11.0(P
=NS)
Lietal2010
55(fair)
RCT
304
Meanagenotreported(53%
,12
y)StudyPhaseB(includedplacebo
comparison)
NRPhaseBresults
43sitesintheUS,India,South
Africa,
Russia,and
Dominican
Republic
63%male
GroupA:Eplerenone
25mgonce
daily
Least-squares
meanchange
from
baseline,SBP:
4wk
35%black
GroupB:Eplerenone
25mgtwicedaily
GroupA:P=NS
57%white
GroupC:Eplerenone
25mgbidfor2
wk
followed
by50
mgbidfor4wk
GroupB:2.76
(95%
CI,2
5.5to0;P=
.048
versus
placebo)
11%Hispanic
GroupD:Placebo
GroupC:P=NS
8%Asian
Least-squares
meanchange
from
baseline(any
group),DBP:P
=NS
56%primaryhypertension
514 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
5Continued
Author,Year(Quality
Rating)
StudyDesign
and
SettingDuration
NDemographicCharacteristics
Intervention
ProportionofPatientsAchieving
#95th
PercentileofBloodPressure
forAge,Gender,and
Height
BloodPressure
(mmHg)
Sorofetal20025
6
(fair)
RCT
94Meanage14
yGroupA:Bisoprololfumarate2.5+
hydrochlorothiazide6.25
NRLeastsquares
meanchange
from
baseline,SBP:
Clinicaltrialfrom22
sitesinUnited
States
andBrazil
57%male
GroupB:Bisoprolol5mg+
hydrochlorothiazide6.25
mg
Groups
A–Cpooled:2
9.3(P
,.05
versus
placebo)
4wk
43%white
GroupC::Bisoprololfum
arate10
mg+
hydrochlorothiazide6.25
mg
GroupD:24.9
41%black
GroupD:Placebo
Least-squares
meanchange
from
baseline,DB
P:14%Hispanic
Groups
A–Cpooled:2
7.2(P
,.05
versus
placebo)
1%Asian
GroupD:22.7
1%multiracial
MeanBM
I=28
Trachtman
etal
2003
57(fair)
RCT
133
Meanage12
y(SD3)
GroupA:2.5mgfelodipine
ERBP
#90th
percentile
MeandifferenceSBPat
follow-up
versus
placebo(95%
CI):
Clinicaltrialat30sitesintheUnited
States
60%male
GroupB:5mgfelodipine
ERGroupA:15%
GroupA:20.71
(24.8to3.38;P
=NS)
3wk
39%black
GroupC:10mgfelodipine
ER,titrated
totargetdose
GroupB:18%
GroupB:20.06
(24.6to3.3;P=NS)
GroupD:Placebo
GroupC:19%
GroupC:21.73
(26.58
to3.13;P
=NS)
GroupD:11%
MeandifferenceDB
Patfollow-up
versus
placebo(95%
CI):
GroupA:22.07
(26.82
to2.69;P
=NS)
GroupB:24.64
(29.18
to0.09;P
,.05)
GroupC:1.31
(23.56
to6.11;P
=NS)
Trachtman
etal
2008
58(fair)
RCT
240
Meanagenotreported(29%
,12
y;71%.12
y)GroupA:Candesartan2/4mg
GroupA:54%
Least-squares
meanchange
from
baseline,SBP:
Clinicaltrialat42sitesinUnited
States
andEurope
71%male
GroupB:62%
Groups
A–C:-10.22
(P,
.0001versus
placebo)
4wk
69%BM
I$95th
percentile
GroupB:Candesartan8/16
mg
GroupC:65%
GroupD:23.66
47%black
GroupC:Candesartan16/32mg
GroupD:31%
Leastsquares
meanchange
from
baseline,DB
P:45%white
GroupD:Placebo
Groups
A–C:26.56
(P=.0029versus
placebo)
GroupD:21.8
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 515 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
5Continued
Author,Year(Quality
Rating)
StudyDesign
and
SettingDuration
NDemographicCharacteristics
Intervention
ProportionofPatientsAchieving
#95th
PercentileofBloodPressure
forAge,Gender,and
Height
BloodPressure
(mmHg)
Wellsetal2010
59
(fair)
RCT
77Meanage:14
y(SD3y)
GroupA:Telmisartan1mg/kg/day
(low
-dosegroup)
GroupA:50%(6–,12
y);68%
(12–,18
y)Adjusted
meandifferenceSBPat
follow-upversus
placebo(95%
CI):
Clinicaltrialat16sitesinUnited
States,Brazil,andMexico
57%male
GroupB:Telmisartan1mg/kg/day,
titratedup
to2mg/k/dayafter1wk
(high-dose
group)
GroupB:86%(6–,12
y);79%
(12–,18
y)GroupA:23.6(2
9.2to1.9,P=NS)
4wk
51%white
GroupC:Placebo
GroupC:33%(6–,12
y);27%
(12–,18
y)GroupB28.5(2
14to23.0,P=.0027)
37%black
Adjusted
meandifferenceDB
Pat
follow-upversus
placebo:
GroupA:24.5(2
9.5to0.4,P=NS)
GroupB:24.8(2
9.7to0,P=.051)
Drug
plus
lifestyleinterventions
Berenson
etal1983
60
(fair)
RCT
150
NRADAPTProgram
NRMeanchange
from
baseline,SBP:
School-based
inUnitedSates
GroupA:Propranolol20–40
mg+
chlorthalidone6.25–12.5mg+
nutrition
educationandprom
otion
ofdietarymodification
GroupA:27.6
Otherpublication:
Franketal1982
786mo
GroupB:Hypertensive
controlgroup
with
notreatm
ent
GroupB:23.0
Meanchange
from
baseline,DB
P:GroupA:26.9
GroupB:23.9
Berenson
etal1990
61
(fair)
RCT
150
Meanage12
ySameas
above
NRAdjusted
meandifference,SBP:
School-based
inUnitedStates
55%male
GroupAversus
GroupB:23.6(SD1.12;
P,
.01)
Continuationof
Berenson
etal
1983
60
30mo
47%white
Adjusted
meandifferenceDB
P:MeanSBP117.7mmHg
GroupAversus
GroupB:21.7(SD0.82;
P,
.05)
MeanDB
P78.1mmHg
Lifestyleinterventions
Diet Co
uchetal2008
62
(fair)
RCT
57Meanage14
yGroupA:DASH-type
dietmodified
for
adolescentpopulation+counseling
NRMeandifferenceatfollow-up,SBP:
CincinnatiChildren’sHospitalM
edical
Center,UnitedStates
63%male
GroupB:Counselingalone
GroupAversus
GroupB:0.1
6mo
MeanSBP128.7mmHg
Meandifferenceatfollow-up,DB
P:MeanDB
P80.5mmHg
GroupAversus
GroupB:21.2
Proportionachievingnorm
otensive
status:
GroupA61%versus
GroupB44%;P
=NS
Howeetal1991
65
(fair)
RCTcrossover
103
Meanage13y(range11–14y)
GroupA:Low-sodiumdiet(,
75mmol/
day)+counseling
NRNo
significant
differences
inSBPor
DBPbetweendiets;baselinevalues
notreported
School-based
MeanSBP115.0mmHg
GroupB:High-sodiumdiet(.
150
mmol/day)diet+counseling
Adelaide,Australia
MeanDB
P60.1mmHg
2phases
of4wkeach
516 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
5Continued
Author,Year(Quality
Rating)
StudyDesign
and
SettingDuration
NDemographicCharacteristics
Intervention
ProportionofPatientsAchieving
#95th
PercentileofBloodPressure
forAge,Gender,and
Height
BloodPressure
(mmHg)
Sinaikoetal
1993
66(fair)
RCT
210
Meanage13
yGroupA:Lowsodium
diet(,
70mmol/
day)
NRChangesinSBP:
St.Pauland
Minneapolispublic
schools,UnitedStates
50%male
GroupB:Potassiumchloride
supplementation
Boys:Nosignificant
differences
inratesofincrease
inSBPbetween
lowsodium
,potassium
supplement,andplacebogroups.
3y
MeanSBP113.8mmHg
GroupC:Participant’s
usualdiet+
placebo
Girls:Significant
differenceinSBP
betweenlowsodium
group(slight
overalldecrease)
andtheplacebo
group(significant
increase
from
baseline).Nootherdifferences
betweengroups.
MeanDB
P65.1mmHg
ChangesinDB
P:Boys:Nosignificant
differences
inratesofincrease
inBP
betweenlow
sodium
,potassium
supplement,
andplacebogroups
Girls:Thelowsodium
groupwas
the
onlygroupthathadratesof
increase
inDB
Pcomparedwith
placebothatweresignificantly
greaterthan
zero
Exercise
Hansen
etal
1991
64(fair)
RCT
137
Agerange9–11
yGroupA:3extralessonsperw
eekofan
ordinaryschoolphysicaleducation
program
NRMeandifferenceatfollow-up,SBP:
Odense,Denmark
Otherdemographic
characteristics:NR
GroupB:No
extraphysicaleducation
lessons
GroupAversus
GroupB:24.9;P,
.05
School-based
Meandifferenceatfollow-up,DB
P:8mo
GroupAversus
GroupB:23.8;P,.05;
Meditation
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 517 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
5Continued
Author,Year(Quality
Rating)
StudyDesign
and
SettingDuration
NDemographicCharacteristics
Intervention
ProportionofPatientsAchieving
#95th
PercentileofBloodPressure
forAge,Gender,and
Height
BloodPressure
(mmHg)
Gregoskietal
2011
63(fair)
RCT
166
Meanage15
yGroupA:Breathingaw
areness
meditation
NRMean24-hSBPat3-mofollow-up:
School-based
inUnitedStates
59%female
GroupB:LifeSkillstraining
(weekly50-
minsessions
focusing
ontraining
inproblem-solving
skills,reflective
listening,conflictresolution,anger
managem
enttoenhancesocial
skillsandassertiveness)
GroupAversus
GroupBversus
GroupC:
3mo
100%
black
GroupC:Health
educationcontrol
116.6vs
119.8vs
121.0
MeanSBP118.9mmHg
GroupAversus
GroupB:P=NS
MeanDB
P63.6mmHg
GroupAversus
GroupC:P=.05
Mean24-hDB
Pat3-mofollow-up:
GroupAversus
GroupBversus
GroupC:
66.3vs
68.2vs
68.7;P
=NS
forall
comparisons
Progressivemusclerelaxation
Ewartetal19873
3
(fair)
RCT
159
BMIrange:19.0–31.2
GroupA:Progressivemuscle
relaxation(12wk,15–20
min,4
d/wk)
provided
inschool
NRNo
significant
differences
between
SBPandDB
Pbetweentreatm
ent
andcontrolgroups
2largeUS
BaltimoreCitypublichigh
schools
Meanage15y(range13–17y)
9mo
60%male
55%black
BP,blood
pressure;DASH,DietaryApproaches
toStop
Hypertension;ER,extended
release;NR
,not
reported;NS,notsignificant.
518 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
6Harm
sof
Interventions
forHypertension
inChildrenandAdolecents
Author,Year(Quality
Rating)
Relevance
Type
ofStudySettingand
Duration
MeanAge
(SD)
(y)
NumberRandom
ized
orAnalyzed
Intervention
AEs
Drug
interventions
Batisky
etal
2007
53(fair)
Allparticipantshadprimary
hypertension
RCT
12.5(2.8)
144random
ized
indosing
study
100analyzed
insafetystudy
4-wkdose
rangingstudy:
4-wkdose-ranging
study:
28centers
ERmetoprololsuccinate0.2–2.0
mg/kg
1withdraw
alduetoAEs
UnitesStates
Placebo
Heartratedecreasedby
6.5bpm
in1.0mg/kg
group(com
pared
with
increase
of5.4bpmin
placebogroup),
4-wkdose-ranging
study
52-wkopen-labelstudy:
Fatigue
notedby
1patienteach
inthe0.2,1.0,and2.0mg/kg
groups
52-wksafetystudy
25mgor
12.5mgonce
daily
atinvestigator
discretion;
increase
every2wkuntil
maximum
of200mgonce
daily
52-wksafetystudy:
5withdraw
alsduetoAEs(1each
offatigue,nightmares,
anxiety,dizziness,asthma)
SeriousAEs:2/100(2%;1
pneumoniaand1
menom
etrorrhagia)
OtherAEs:
Headache:30%
Upperrespiratorytract
infection:20%
Cough:19%
Nasopharyngitis:13%
Pharyngolaryngealpain:12%
Fatigue:9%
Diarrhea:7%
Dizziness:6%
Flynnetal2004
54
(fair)
31%with
primary
hypertension
RCTcrossover
12.1(3.3)
268random
ized;84with
primary
hypertension
Amlodipine
2.5–5.0mg/day
Withdraw
alsduetoAEs:
Clinicaltrialfrom49
centersin
NorthandSouthAm
erica
Placebo
12/268
(??%
),ofwhich
6considered
bystudy
investigatorstobe
studydrug
related(3
worsening
hypertension,1facialedem
a,1
finger
edem
aandrash,1
prem
atureventricular
contractions)
24-wkphases
SeriousAEs:
5/268(2%;1
each:urinary
tract
infection,gastroenteritis
and
hypovolemia,pulmonary
edem
a,pneumonia,
pancreatitis)
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 519 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
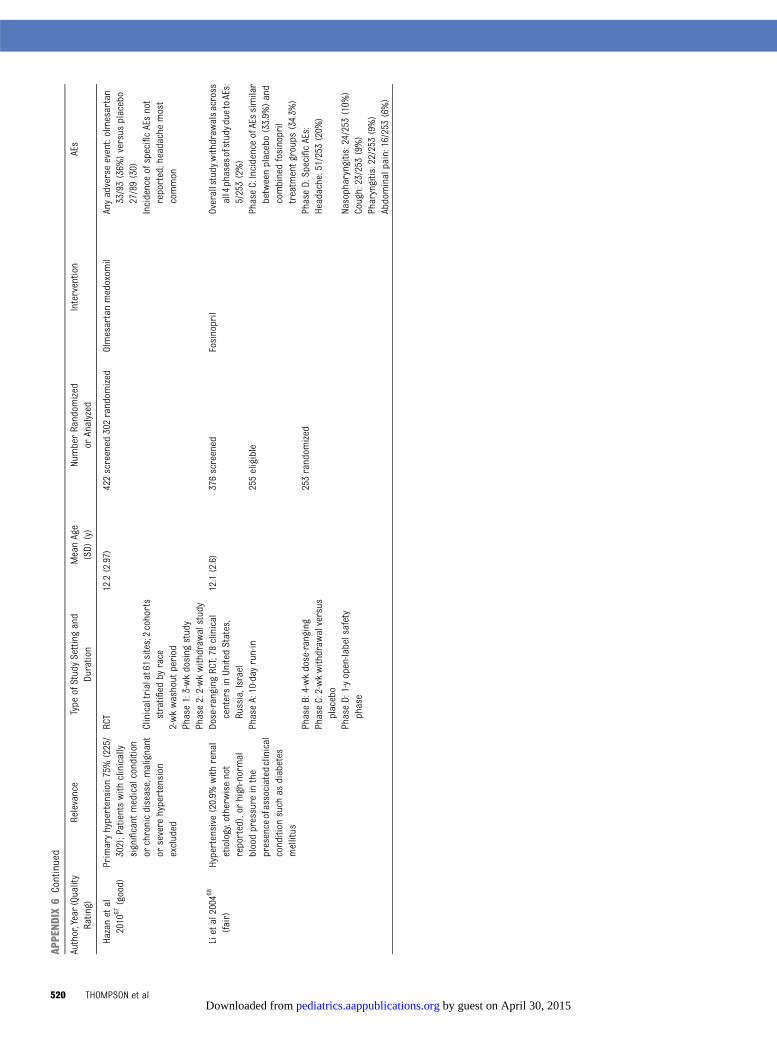
APPENDIX
6Continued
Author,Year(Quality
Rating)
Relevance
Type
ofStudySettingand
Duration
MeanAge
(SD)
(y)
NumberRandom
ized
orAnalyzed
Intervention
AEs
Hazanetal
2010
67(good)
Primaryhypertension
75%(225/
302);Patientswith
clinically
significant
medicalcondition
orchronicdisease,malignant
orsevere
hypertension
excluded
RCT
12.2(2.97)
422screened
302random
ized
Olmesartanmedoxom
ilAnyadverseevent:olmesartan
33/93(36%
)versus
placebo
27/89(30)
Clinicaltrialat61sites;2cohorts
stratified
byrace
IncidenceofspecificAEsnot
reported;headachemost
common
2-wkwashout
period
Phase1:3-wkdosing
study
Phase2:2-wkwithdraw
alstudy
Lietal2004
68
(fair)
Hypertensive
(20.9%
with
renal
etiology,otherwisenot
reported),or
high-normal
bloodpressure
inthe
presenceofassociated
clinical
condition
such
asdiabetes
mellitus
Dose-ranging
RCT;78
clinical
centersinUnitedStates,
Russia,Israel
12.1(2.6)
376screened
Fosinopril
Overallstudy
withdraw
alsacross
all4phasesofstudydue
toAEs:
5/253(2%)
PhaseA:10-day
run-in
255eligible
PhaseC:IncidenceofAEssimilar
betweenplacebo(33.9%
)and
combinedfosinopril
treatm
entgroups(34.3%
)PhaseB:4-wkdose-ranging
253random
ized
PhaseD:SpecificAEs:
PhaseC:2-wkwithdraw
alversus
placebo
Headache:51/253(20%
)
PhaseD:1-yopen-labelsafety
phase
Nasopharyngitis:24/253(10%
)Cough:23/253
(9%)
Pharyngitis:22/253(9%)
Abdominalpain:16/253(6%)
520 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
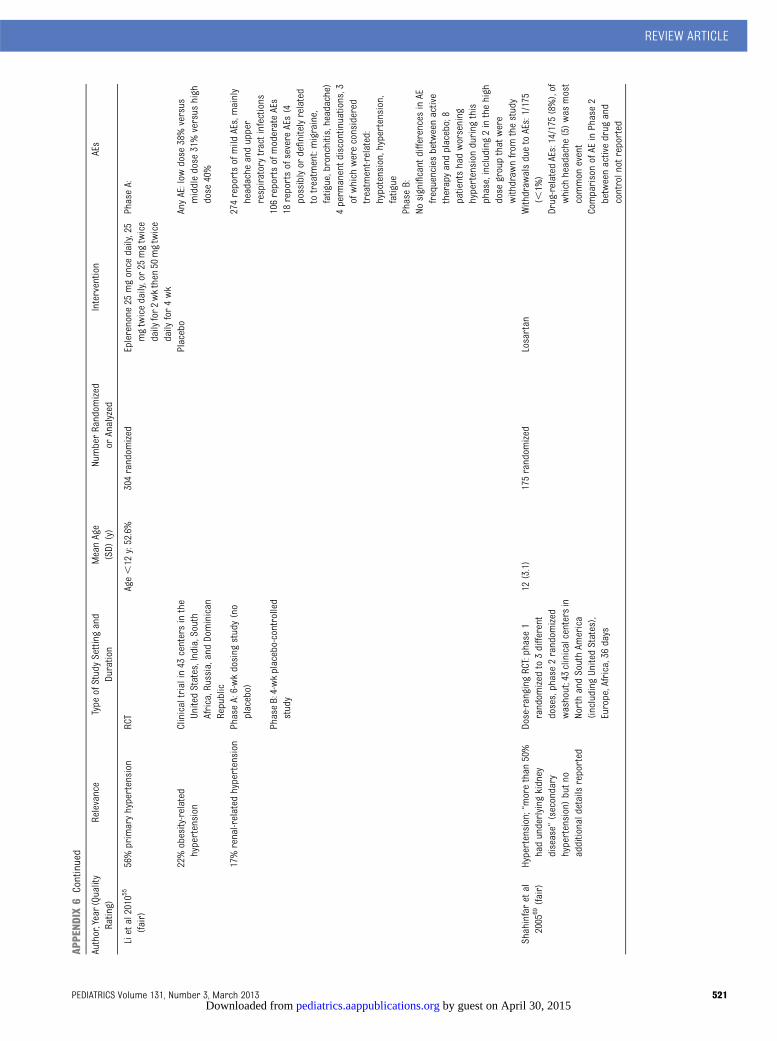
APPENDIX
6Continued
Author,Year(Quality
Rating)
Relevance
Type
ofStudySettingand
Duration
MeanAge
(SD)
(y)
NumberRandom
ized
orAnalyzed
Intervention
AEs
Lietal2010
55
(fair)
56%primaryhypertension
RCT
Age,12
y:52.6%
304random
ized
Eplerenone
25mgonce
daily,25
mgtwicedaily,or25
mgtwice
daily
for2wkthen
50mgtwice
daily
for4wk
PhaseA:
22%obesity-related
hypertension
Clinicaltrialin43
centersinthe
UnitedStates,India,South
Africa,Russia,andDominican
Republic
Placebo
AnyAE:low
dose
38%versus
middledose
31%versus
high
dose
40%
17%renal-related
hypertension
PhaseA:6-wkdosing
study(no
placebo)
274reportsofmild
AEs,mainly
headache
andupper
respiratorytractinfections
PhaseB:4-wkplacebo-controlled
study
106reportsofmoderateAEs
18reportsofsevere
AEs(4
possiblyor
definitelyrelated
totreatm
ent:migraine,
fatigue,bronchitis,headache)
4perm
anentd
iscontinuations,3
ofwhich
wereconsidered
treatm
ent-related:
hypotension,hypertension,
fatigue
PhaseB:
Nosignificant
differences
inAE
frequenciesbetweenactive
therapyandplacebo;8
patientshadworsening
hypertension
during
this
phase,including2inthehigh
dose
groupthatwere
withdraw
nfrom
thestudy
Shahinfaretal
2005
69(fair)
Hypertension;“morethan
50%
hadunderlying
kidney
disease”
(secondary
hypertension)butn
oadditionaldetailsreported
Dose-ranging
RCT:phase1
random
ized
to3different
doses,phase2random
ized
washout;43clinicalcentersin
NorthandSouthAm
erica
(including
UnitedStates),
Europe,Africa,36
days
12(3.1)
175random
ized
Losartan
Withdraw
alsduetoAEs:1/175
(,1%
)Drug-related
AEs:14/175
(8%),of
which
headache
(5)was
most
common
event
ComparisonofAE
inPhase2
betweenactivedrug
and
controlnot
reported
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 521 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
6Continued
Author,Year(Quality
Rating)
Relevance
Type
ofStudySettingand
Duration
MeanAge
(SD)
(y)
NumberRandom
ized
orAnalyzed
Intervention
AEs
Sofferetal
2003
70(fair)
Hypertension;unclear
severityof
underlying
kidney
disease
(study
entryrequired
glom
eruralfiltrationrate$30
mL/min/1.73m2 )
Dose-ranging
RCT
Meannotreported47%
,6–12
y,53%13–16
y
115random
ized
Lisinopril
Withdraw
alsduetoAEs:1/115
(,1%
)Phase1random
ized
to3
different
doses,phase2
random
ized
washout
Drug-related
AEs:14/115
(12%
)
Multisite
(num
berandlocation
notreported);29days
Headache:4/115
(4%)
Gastrointestinal(abdom
inal
pain,diarrhea,nausea
and/or
vomiting):2/115(2%)
Dizziness:2/115(2%)
Cough:1/115(,
1%)
Sorofetal20025
6
(fair)
Excluded
severe
hypertension
andcorrectablesecondary
hypertension
RCT
13.8(3.1)
94random
ized
(62treatm
ent+
32placebo)
B/HT
(n=62):
B/HT
grouphadfeweroverallAEs
than
placebogroup,33/62
(53%
)vs24/32(75%
)(P=.047)
andfewer
seriousAEs,1/62
(2%)vs
5/32
(16%
)(P
=.016)
Clinicaltrialfrom22
centersin
UnitedStates
andBrazil
B/HT
group:
2-wkrun-in,8-wktitration
period,-wkdose
maintenance
period,2-wktapering
period
B2.5mg/HT
6.25
mg
Mostcom
mon
AEwas
headache
(26%
)B5mg/HT
6.25
mg
1patient
hadsevere
hypertension,and
discontinuedthestudy.
B10
mg/HT
6.25
mg
Placebogroup:
Mostcom
mon
AEwas
headache
(31%
)Placebo(n
=32)
2patientshadsevere
hypertension,and
discontinuedthestudy
Trachtman
etal
2003
57(fair)
Excluded
secondary
hypertension
RCT
12.1(2.7)
133random
ized
ERfelodipine
1withdraw
aldueto
“heart
racing”;heartratewas
96bpmandECGnorm
al;and
1withdraw
alduetovomiting
thefirstdose
(5mg)
Clinicaltrialat30sitesinthe
UnitedStates
2.5mg(n
=33),5mg(n=340,or
10mg(n
=31),titratedto
targetdose
over
2–3wk,
dependingon
dosage
%reportingAEs:placebo66%and
64%,56%
,and
77%inthe
felodine
ER2.5mg,5.0mg,and
10mggroups,respectively
1-to3-wkscreeningperiod,2-to
3-wkdose
titrationperiod,3-
wkmaintenance
study
Placebo(n
=35)
Mostcom
mon
AEswere
headaches(33%
),respiratory
infections
(12%
),andnausea
(10%
)Pedaledemawas
notedin2(2%)
ofpatients
522 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
6Continued
Author,Year(Quality
Rating)
Relevance
Type
ofStudySettingand
Duration
MeanAge
(SD)
(y)
NumberRandom
ized
orAnalyzed
Intervention
AEs
Trachtman
etal
2008
58(fair)
Excluded
secondary
hypertension
RCT
%Age.12
y:70.8%
240random
ized
4wktrial:
3/240patientsinthe4wktrial
and5/233patientsinthe52
wk
studydiscontinuedduetoAEs,
specifically
hypotension,arm
fracture,dizziness,headache,
lowwhitebloodcellcount,and
progressionofunderlying
renaldisease
(2patients)
Otherhypertensives,except
for
otherangiotension
receptor
blockers,w
ereperm
itted
Clinicaltrialat42sitesinUnited
States
andEurope
Candesartandoses2,8,and16
mg/dayforthose,50
kg,and
4,16,and
32mg/dayforthose
$50
kg
Mostcom
mon
AEs:headache,
upperrespiratoryinfection,
dizziness,cough,andsore
throat
4-wktrialand
1-yopen-label
study
Placebo
Open
labelstudy:
Candesartanat4or
8mg/dayto
start,butlater
adjusted
tocontrolBP
Wellsetal2002
71
(fair)
Severe
orsymptom
atic
hypertension
excluded
Dose-ranging
RCT
Median12
y110enrolled
Enalapril
Drug-related
AEs:12/110
(11%
)2-wkdose
rangingphaseand2-
wkplacebocontrolled
washout
phase
Dizziness:4/110(4%)
Headache:2/110
(2%)
Cough:3/110(3%)
Noincidenceofrenalfailure,
angioedemaor
hyperkalem
ia5laboratory
AEspossibly,
probablyor
definitelyrelated
tostudydrug
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 523 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
6Continued
Author,Year(Quality
Rating)
Relevance
Type
ofStudySettingand
Duration
MeanAge
(SD)
(y)
NumberRandom
ized
orAnalyzed
Intervention
AEs
Wellsetal2010
59
(fair)
Excluded
secondary
hypertension
RCT
14(2.5)
115enrolled
Telmisartanlowdose
(1mg/kg/
day)(n
=30)and
high
dose
(1mg/kg/daytitratedup
to2mg/
k/dayafter1wk)
(n=31)
AnyAE:
Clinicaltrialat16
centersin
UnitedStates,Brazil,and
Mexico
77random
ized
Placebo(n
=16)
High-dosepatients:41.9%
4wk,after2-wkwashout
period
Lowdose
patients:41.7%
Placebopatients:31.3%
Significancenotreported
2patientsdiscontinueddueto
AEs,both
inthehigh
dose
group:1patient
who
experiencedaseriousAE
(nearsyncopeandmoderate
increase
inbloodurea
nitrogen
andserum
creatinine)
who
received
anexcessivedose
inerror;and1
patient
duetomoderate-
intensity
dizziness,weakness,
andheadache
Drug
plus
lifestyleinterventions
Berenson
etal
1983
60(fair)
BP.90th
percentileforheight,
controlgroup
with
blood
pressure
,80th
percentiles
andthe50–60thpercentilefor
comparison(based
oncentilesderivedfrom
study)
“Close
toclinicaltrial”
12150(50high
bloodpressure
treatm
entgroup,50high
blood
pressure
comparisongroup,
50mediumbloodpressure
comparisongroup)
GroupA:
AEsreported
asvery
low
incidencewith
nomajor
complications
Excluded
childrenwith
evidence
ofsecondaryhypertension
School-based
Propranolol
1temporary
withdraw
alfrom
activetreatm
entd
ueto
nightm
ares
6mo
20mg/dayforchildren,
40kg,
40mg/dayforthose.40
kg+
chlorthalidone
6.25
mgperdayforchildren
,40kg,12.5mg/dayforthose
.40
kg+nutrition
education
andprom
otionofdietary
modificationtochildrenand
parents
GroupB(highBP
elevationat
baseline):
Notreatm
ent
GroupC(m
ediumBP
elevationat
baseline):
Notreatm
ent
524 THOMPSON et al by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

APPENDIX
6Continued
Author,Year(Quality
Rating)
Relevance
Type
ofStudySettingand
Duration
MeanAge
(SD)
(y)
NumberRandom
ized
orAnalyzed
Intervention
AEs
Otherclinicalstudies(FDA
analyses)
Baker-Sm
ithetal
2010
73(not
rated)
Mild
tomoderatehypertension
Nonsystematicreview
andmeta-
analysisofdatafrom
8trials
subm
itted
toFDAbetween
1998
and2005
(original
studiesnotcited)
131299
analyzed
(42%
placebo+
58%activedrug)
ACEs
(6datasets)andARBs
(2datasets),includingbenazepril
(n=85),enalapril(n=101),
fosinopril(n
=222),lisinopril
(n=104),quinapril(n
=112),
ramipril(n=217),irbesartan
(n=293),losartan(n
=165)
Subjectswho
reported
coughin
thecohortreceivingactive
drugs(21/748,2.8%
)vs
placebo(14/551,2.5%
),P=.86
2wk(m
edian)
Dosagesnotreported
Subjectswho
reported
coughin
theACEgroup:(17/524,3.2%
);ARBgroup(4/224,1.8%),P=.34
Smith
etal2008
72
(notrated)
Unclear;severe
hypertension
andsignificant
renaldisease
excluded
Nonsystematicreview
andmeta-
analysisofdatafrom
10RCTs
subm
itted
toFDAbetween
1998
and2005
(original
studiesnotcited)
12.1
1707
analyzed
(685
placebo,1022
activetreatm
ents)
Activetreatm
ents(n
=1022;
meandosesnotreported):
amlodipine
(n=258),
benazepril(n
=85),enalapril
(n=101),felodipine(n
=133),
fosinopril(n
=235),
irbesartan
(n=295),lisinopril
(n=104),losartan(n
=165),
quinapril(n=112),ram
ilpril
(n=219)placebo(n
=685)
Placeboversus
activetreatm
ent:
2to4wk(variedby
trial)
Nosignificantdifferencebetween
groups
foranyAEs
AnyAE:235/685
(34%
)vs
382/
1022
(37%
)Hypertension:3/685
(4%)vs
1/1022
(.1%
)Hypotension:0/235(0%)vs
3/1022
(.1%
)Cardiac:8/685(1%)vs
16/1022
(2%)
Neuropsychological:13/685(2%)
vs26/1022(3%)
Headache:113/685
(17%
)vs179/
1022
(18%
)Syncope:15/685
(2%)vs
31/1022
(3%)
Gastrointestinal:54/685(8%)vs
90/1022(9%)
Asthma:11/685
(2%)vs
12/1022
(1%)
Elevated
LFT:7/685(1%)vs
7/1022
(.1%
)Muscleaches:11/685
(2%)vs17/
1022
(2%)
ACE,angiotensin-convertingenzymeinhibitors;AE,adverseevent;ARB,
angiotensinreceptor
blockers;bpm,beatsperminute;B/HT,bisoprolol
fumarate/hydrochlorothiazide;ECG,
electrocardiograph;ER,extended
release;FDA,
Food
andDrug
Administration;LFT,liver
functiontest.
REVIEW ARTICLE
PEDIATRICS Volume 131, Number 3, March 2013 525 by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2012-3523; originally published online February 25, 2013; 2013;131;490Pediatrics
NorrisMatthew Thompson, Tracy Dana, Christina Bougatsos, Ian Blazina and Susan L.
Cardiovascular DiseaseScreening for Hypertension in Children and Adolescents to Prevent
ServicesUpdated Information &
mlhttp://pediatrics.aappublications.org/content/131/3/490.full.htincluding high resolution figures, can be found at:
References
ml#ref-list-1http://pediatrics.aappublications.org/content/131/3/490.full.htat:This article cites 74 articles, 30 of which can be accessed free
Citations
ml#related-urlshttp://pediatrics.aappublications.org/content/131/3/490.full.htThis article has been cited by 4 HighWire-hosted articles:
Rs)3Peer Reviews (PPost-Publication
http://pediatrics.aappublications.org/cgi/eletters/131/3/490
R has been posted to this article: 3One P
Subspecialty Collections
ular_disorders_subhttp://pediatrics.aappublications.org/cgi/collection/cardiovascCardiovascular Disorders
_subhttp://pediatrics.aappublications.org/cgi/collection/cardiologyCardiologythe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from
DOI: 10.1542/peds.2012-3523; originally published online February 25, 2013; 2013;131;490Pediatrics
NorrisMatthew Thompson, Tracy Dana, Christina Bougatsos, Ian Blazina and Susan L.
Cardiovascular DiseaseScreening for Hypertension in Children and Adolescents to Prevent
http://pediatrics.aappublications.org/content/131/3/490.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 30, 2015pediatrics.aappublications.orgDownloaded from