pediatric orbital floor fractures
TRANSCRIPT

Review Article
Pediatric orbital floor fracturesLeslie A. Wei, MD, and Vikram D. Durairaj, MD
PURPOSE To summarize the unique aspects of orbital floor fractures in children with regard to clin-
Author affiliations: DepartmentMedicine, Denver ColoradoSubmitted July 12, 2010.Revision accepted February 5,Reprint requests: Vikram D.
University of Colorado Denver,Aurora, CO 80045 (email: vikrCopyright � 2011 by the Am
Strabismus.1091-8531/$36.00doi:10.1016/j.jaapos.2011.02
Journal of AAPOS
ical presentation, management, and outcomes.
METHODS MEDLINE was searched using PubMed for English-language articles on orbital floor
fractures in children. All 154 indexed articles pertaining to floor fractures in patients under18 years of age in PubMed were reviewed. Studies looking at primarily complex fracturesand case reports and studies that included pediatric patients but did not analyze them sep-arately were excluded. Overall, 25 studies were included for the review.RESULTS Inferior trapdoor fractures with muscle and soft tissue incarceration are the most common
type of orbital fracture in children (27.8%-93%). They often present uniquely withseverely restricted extraocular motility and diplopia (44%-100%), nausea and vomiting(14.7-55.6%), and minimal signs of external trauma. The majority of studies (83%) thatanalyzed time to surgery in relation to outcomes found that children who present early afterinitial injury and undergo prompt surgical repair appear to recover faster and have betterpostoperative motility than those receiving delayed treatment.CONCLUSIONS Our understanding of pediatric orbital floor fractures continues to evolve. For young
patients with symptomatic diplopia with positive forced ductions, soft tissue entrapmentconfirmed by computed axial tomography, and/or trapdoor fracture plus restricted ocularmovement, having surgery within 2-5 days has been shown to result in better postoperativeoutcomes. It is recommended that surgery be considered within 48 hours of diagnosis.Long-term prospective studies are still needed to further characterize orbital floor frac-tures in children. ( J AAPOS 2011;15:173-180)Isolated orbital floor fractures are usually the result ofblunt facial trauma. Orbital floor fractures, alsoknown as “blowout” fractures, were first described
by Smith and Regan1 in 1957 and describe an isolated frac-ture of the orbital floor with the orbital rim intact. Theexact means of orbital floor fracture are still debated.The 2 dominant theories are the “hydraulic” mechanism,according to which increased intraorbital pressure resultsin direct compression and fracture of the bony floor, andthe “buckling” mechanism, according to which force trans-mitted posteriorly through the orbital rim transientlybuckles and then fractures the thin orbital floor.1,2 Boththeories are supported by theoretical and experimentalmodels in the literature.2-5
Blowout fractures of the orbital floor have been well-described and studied in adults6,7; however, they have notbeen as well studied in children. Pediatric orbital floor
of Ophthalmology, University of Colorado, School of
2011.Durairaj MD, Rocky Mountain Lions Eye Institute,School of Medicine, 1675 N Aurora Ct., Mail Stop F731,[email protected]).erican Association for Pediatric Ophthalmology and
.005
fractures can present differently than adult orbital floorfractures and can have adverse long-term consequences ifnot recognized and dealt with appropriately. Clinically,low-velocity but high-force crush injuries are themost com-mon cause of orbital floor fractures in children.8 They areoften related to sports, accidents during play, motor vehicleaccidents, or assault.9-11 Among all pediatric orbital floorfractures, the subset of trapdoor fractures make up a largeproportion and have been reported to comprise from27.8% to 93% of cases.9,10,12-14 Conversely, adults aremore often found to have comminuted, or “open-door,”fractures, without tissue entrapment, that can be observedfor 2 weeks prior to repair.13 The difference between adultand pediatric injury is attributable to variations in the facialanatomy of children versus adults.
Children under the age of 7 have thicker sinus walls,greater bone elasticity, more cheek fat pad, and a propor-tionately smaller and flat midface, all of which are thoughtto be protective of the orbital floor.15 Orbital floor frac-tures in this age group are in fact uncommon. Orbitalroof fractures, however, are themost common pediatric or-bital fracture in very young children.15,16 Koltai andcolleagues15 found that after the age of 7 years (�1 year)the probability of lower orbital fractures surpasses theprobability of roof fractures. Thus as the face and sinusesdevelop, orbital floor fractures become increasingly com-mon as a result of blunt facial trauma.10-12
173

174 Wei and Durairaj Volume 15 Number 2 / April 2011
While young adults are by far the most common demo-graphic group presenting with fractures requiring surgery,children still make up a significant percentage of floor frac-tures.6,7 Pediatric cases make up approximately 22% of allorbital floor fractures requiring surgical repair.6 Floor frac-tures comprise 15% of pediatric facial fractures and makeup 70% of internal orbital fractures in small case series ofchildren of all ages.10,19,33 Young men in their twentieshave been found to be at the highest risk for orbital floorfractures, and in children, males with orbital floorfractures outnumber females 4:1.7,11
The purpose of this review is to summarize the uniqueaspects of orbital floor fractures in children with regardto clinical presentation, management, and outcomes.
Methods
MEDLINE database was searched using PubMed for English-
language articles containing the following key words: pediatric or-
bital floor fracture, pediatric orbital blow-out fracture, pediatric orbital
trapdoor fracture, orbital floor fractures in children, orbital blow-out
fractures in children, and orbital trapdoor fractures in children. All
154 articles indexed in PubMed pertaining to orbital floor frac-
tures in patients under the age of 18 were reviewed; studies look-
ing at primarily complex fractures (for example, combined orbital
floor and medial wall fractures), case studies, and studies that in-
cluded some pediatric patients but did not analyze them as a sep-
arate group were excluded. Overall, 25 studies were included for
review (Table 1).
Results
Presentation
Classic symptoms and signs of an orbital floor fracture in-clude severe pain, diplopia, infraorbital anesthesia, limitedextraocular motility (particularly supraduction and infra-duction in cases of entrapment), enophthalmos, subcon-junctival hemorrhage, and periorbital soft tissueecchymosis and edema. Less commonly seen are subcuta-neous/subconjunctival emphysema, hyphema, epistaxis,ptosis, and pupillary dilation from compression of para-sympathetic nerve fibers that travel with the inferior divi-sion of the third cranial nerve. Between 44% and 100%of children with entrapment had severely limited extraocu-lar motility (Figure 1).9-14,19-25,27-33 Diplopia can be causedby entrapment of extraocular muscles, direct damage to themuscles during the initial injury, swelling and hemorrhage,or injury to branches of motor nerves. Direct damage andinjury to the nerve may be irreversible and result inpersistent diplopia.34 Overall, diplopia and extraocularmotility limitations are more common in children than inadults, whereas periorbital swelling is relatively lesscommon.10,25
Because children have immature bones with greater elas-ticity, they are more likely to present with trapdoor frac-tures (Figure 2).9,12,25 A trapdoor fracture is a linear,
medially hinged but minimally displaced fracture thatclassically runs along the infraorbital nerve canal. Itopens transiently at the time of injury and then springsback into place, entrapping periorbital tissue. Smalltrapdoor orbital floor fractures such as those often seenin children are more likely to have high compartmentpressures around the inferior rectus muscle, resulting intissue ischemia. Two common presentations of trapdoorfractures in children are the oculocardiac reflex and thewhite-eyed blowout fracture.
The oculocardiac reflex is the triad of symptoms (nau-sea/vomiting, bradycardia, and syncope) that results fromcommunication between the ophthalmic division of the tri-geminal nerve and the visceral motor nucleus of the vagusnerve via the reticular formation. This symptomatologyhas been reported as highly suggestive of inferior rectusor orbital soft-tissue entrapment in the setting of knownperiocular trauma and can be considered an indicationfor immediate surgery.14,19,30 An average of 1 in 4children with serious entrapment requiring surgery willpresent with nausea and vomiting (range, 14.7% to55.6%) as well as restricted extraocular motility.9,10,12,14
The presence of nausea and vomiting has been reportedto have a positive predictive value of 75% for a trapdoorfracture.23 Furthermore, nausea and vomiting had a re-ported positive predictive value of 83.3% for inferior rectusentrapment in the presence of a documented trapdoorfracture.23
The other unique presentation is the white-eyed blow-out fracture, first coined by Jordan and colleages20 in1998, which describes patients who have orbital floor frac-tures and a history of periocular trauma and marked extra-ocular motility restriction but no enophthalmos, minimalperiorbital soft-tissue edema, and negative or equivocal im-aging findings. Pediatric patients who presented like thisand who were operated on within 24-48 hours had betterlong-term postoperative motility than those who under-went the standard 2-week waiting period.20
A thorough examination should be performed at presen-tation if possible. In comparison with adults, children usu-ally present with less periorbital edema and are able toundergo a full ophthalmologic examination.20,25 Visualacuity, extraocular motility, forced ductions, and pupillaryfunctions should be assessed for possible entrapment,muscle or nerve palsy, and optic neuropathy from orbitalcompartment syndrome. Complete ophthalmicexamination should be done if possible to look fortraumatic corneal injury, hyphema, lens dislocation,lacrimal injuries, vitreous hemorrhage, retinal detachment,commotio retinae, and ruptured globe. Although overtglobe injury is rare, it must be ruled out in all perioculartrauma patients.
Imaging
Imaging should be performed when there is a history of fa-cial trauma combined with clinical evidence of a fracture on
Journal of AAPOS
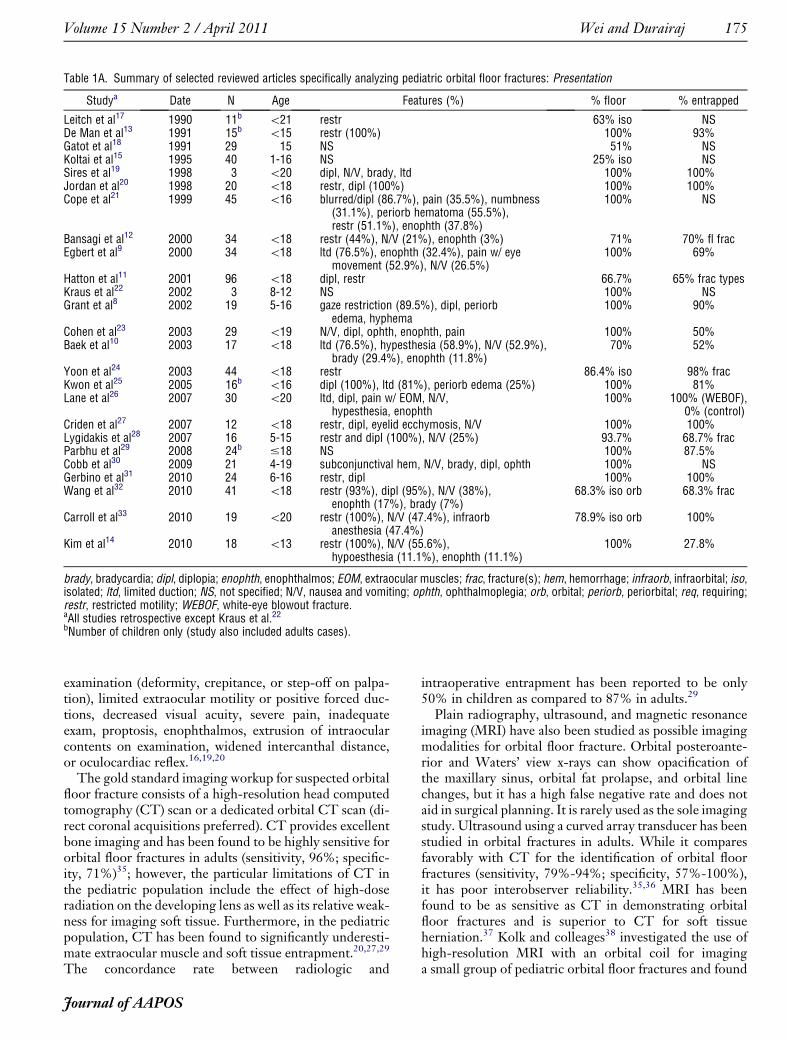
Table 1A. Summary of selected reviewed articles specifically analyzing pediatric orbital floor fractures: Presentation
Studya Date N Age Features (%) % floor % entrapped
Leitch et al17 1990 11b \21 restr 63% iso NSDe Man et al13 1991 15b \15 restr (100%) 100% 93%Gatot et al18 1991 29 15 NS 51% NSKoltai et al15 1995 40 1-16 NS 25% iso NSSires et al19 1998 3 \20 dipl, N/V, brady, ltd 100% 100%Jordan et al20 1998 20 \18 restr, dipl (100%) 100% 100%Cope et al21 1999 45 \16 blurred/dipl (86.7%), pain (35.5%), numbness
(31.1%), periorb hematoma (55.5%),restr (51.1%), enophth (37.8%)
100% NS
Bansagi et al12 2000 34 \18 restr (44%), N/V (21%), enophth (3%) 71% 70% fl fracEgbert et al9 2000 34 \18 ltd (76.5%), enophth (32.4%), pain w/ eye
movement (52.9%), N/V (26.5%)100% 69%
Hatton et al11 2001 96 \18 dipl, restr 66.7% 65% frac typesKraus et al22 2002 3 8-12 NS 100% NSGrant et al8 2002 19 5-16 gaze restriction (89.5%), dipl, periorb
edema, hyphema100% 90%
Cohen et al23 2003 29 \19 N/V, dipl, ophth, enophth, pain 100% 50%Baek et al10 2003 17 \18 ltd (76.5%), hypesthesia (58.9%), N/V (52.9%),
brady (29.4%), enophth (11.8%)70% 52%
Yoon et al24 2003 44 \18 restr 86.4% iso 98% fracKwon et al25 2005 16b \16 dipl (100%), ltd (81%), periorb edema (25%) 100% 81%Lane et al26 2007 30 \20 ltd, dipl, pain w/ EOM, N/V,
hypesthesia, enophth100% 100% (WEBOF),
0% (control)Criden et al27 2007 12 \18 restr, dipl, eyelid ecchymosis, N/V 100% 100%Lygidakis et al28 2007 16 5-15 restr and dipl (100%), N/V (25%) 93.7% 68.7% fracParbhu et al29 2008 24b #18 NS 100% 87.5%Cobb et al30 2009 21 4-19 subconjunctival hem, N/V, brady, dipl, ophth 100% NSGerbino et al31 2010 24 6-16 restr, dipl 100% 100%Wang et al32 2010 41 \18 restr (93%), dipl (95%), N/V (38%),
enophth (17%), brady (7%)68.3% iso orb 68.3% frac
Carroll et al33 2010 19 \20 restr (100%), N/V (47.4%), infraorbanesthesia (47.4%)
78.9% iso orb 100%
Kim et al14 2010 18 \13 restr (100%), N/V (55.6%),hypoesthesia (11.1%), enophth (11.1%)
100% 27.8%
brady, bradycardia; dipl, diplopia; enophth, enophthalmos; EOM, extraocular muscles; frac, fracture(s); hem, hemorrhage; infraorb, infraorbital; iso,isolated; ltd, limited duction; NS, not specified; N/V, nausea and vomiting; ophth, ophthalmoplegia; orb, orbital; periorb, periorbital; req, requiring;restr, restricted motility; WEBOF, white-eye blowout fracture.aAll studies retrospective except Kraus et al.22bNumber of children only (study also included adults cases).
Volume 15 Number 2 / April 2011 Wei and Durairaj 175
examination (deformity, crepitance, or step-off on palpa-tion), limited extraocular motility or positive forced duc-tions, decreased visual acuity, severe pain, inadequateexam, proptosis, enophthalmos, extrusion of intraocularcontents on examination, widened intercanthal distance,or oculocardiac reflex.16,19,20
The gold standard imaging workup for suspected orbitalfloor fracture consists of a high-resolution head computedtomography (CT) scan or a dedicated orbital CT scan (di-rect coronal acquisitions preferred). CT provides excellentbone imaging and has been found to be highly sensitive fororbital floor fractures in adults (sensitivity, 96%; specific-ity, 71%)35; however, the particular limitations of CT inthe pediatric population include the effect of high-doseradiation on the developing lens as well as its relative weak-ness for imaging soft tissue. Furthermore, in the pediatricpopulation, CT has been found to significantly underesti-mate extraocular muscle and soft tissue entrapment.20,27,29
The concordance rate between radiologic and
Journal of AAPOS
intraoperative entrapment has been reported to be only50% in children as compared to 87% in adults.29
Plain radiography, ultrasound, and magnetic resonanceimaging (MRI) have also been studied as possible imagingmodalities for orbital floor fracture. Orbital posteroante-rior and Waters’ view x-rays can show opacification ofthe maxillary sinus, orbital fat prolapse, and orbital linechanges, but it has a high false negative rate and does notaid in surgical planning. It is rarely used as the sole imagingstudy. Ultrasound using a curved array transducer has beenstudied in orbital fractures in adults. While it comparesfavorably with CT for the identification of orbital floorfractures (sensitivity, 79%-94%; specificity, 57%-100%),it has poor interobserver reliability.35,36 MRI has beenfound to be as sensitive as CT in demonstrating orbitalfloor fractures and is superior to CT for soft tissueherniation.37 Kolk and colleages38 investigated the use ofhigh-resolution MRI with an orbital coil for imaginga small group of pediatric orbital floor fractures and found

Table 1B. Summary of selected reviewed articles specifically analyzing pediatric orbital floor fractures: Surgery
Study
Surgery
Time to surg (av) Complications% Approach Implant
Leitch et al17 100% NS NS w/in 2 wks noneDe Man et al13 93% medial palpebral
incision � oroantrallyo w/in 2 wks restr + dipl req strab surg (36%)
Gatot et al18 100% transant none NS noneKoltai et al15 50% NS NS NS NSSires et al19 100% NS cranial bone, poly, sil 1 day diplJordan et al20 100% NS sil (55%), poly (5%) 2-40 days restr (60%) req 2nd surg (20%)Cope et al21 69% blepharoplasty (55%),
infraorb (26%),transconj (19%)
sil (90%),polydiaxonone (6.5%),cranium (3%)
4 days 75% overall early: persistentdipl (55%), infraorb dys (11%),infection (7%); 64% overall late:persistent dipl (36%),infraorb dys (13%), req 2ndsurg (16%), enophth (7%),epiphora (4%)
Bansagi et al12 32%a NS gel, poly 13.4 days (all frac) noneEgbert et al9 100% transcutaneous,
transconjTeflon (88%),
sil (6%),bone graft (3%), gel (3%)
NS early: duction deficits, dipl,residual enophth, cellulitis (3%),subperiosteal hem (13%); late:duction deficits (3%)
Hatton et al11 51%a NS NS NS noneKraus et al22 100% transconj nasoseptal cartilage NS enophth (33%)Grant et al8 90% transconj, subcil pericranial shave
bone graft3 days dipl (19%), scarring (6%)
Cohen et al23 48% transconj, subcil NS 1-9 days early: dipl, reduced motility (14%);late: continued entr req 2ndoperation and strab surg (7%)
Baek et al10 88% transconjb poly (100%) w/in 2 wks diplYoon et al24 82% transconj sil, poly 12.8 days early: hyper (28%), infraorb dys
(11%), optic neuropathy (6%),hypo (3%), cheek edema (2.7%);late: hyper and persistent diplreq strab surg (3%)
Kwon et al25 100% transorb (81.3%),transorb/transant (18.7%)
NS 1-5 days (56%),.5 days (43%)
NS
Lane et al26 100% N NS 6.4 days (WEBOF),15.6 days (control)
early: dipl (88% WEBOF, 50%control); late: dipl (75% WEBOF,21% control)
Criden et al27 100% transconj gel, nylon w/in 4 days restr and dipl (83%), infraorbhypesthesia (17%)
Lygidakis et al28 100% lower eyelid incision dura substitute (69%),poly (31%)
NS persistent restr (6%)
Parbhu et al29 100% NS NS 7.38 days NSCobb et al30 100% NS NS NS early: dipl (80%); late: dipl (62%)Gerbino et al31 100% subcil lyo (63%), resorbable plate
(21%), bone graft (17%)\4 days (83%),
.4 days (18%)restr (33%)
Wang et al32 100% subcil, transconj nylon, poly 23 days eso (5%), hyper (5%), enophth (5%),ptosis (3%), infraorb nervedysfunction (3%)
Carroll et al33 100% transconj poly (100%) �titanium plate
7 days dipl (37%), eso req surg (5%)
Kim et al14 100% transconjb poly (100%) w/in 2 wks temporary hyper (28%) [timing NS]
dipl, diplopia; dys, dysesthesia; enophth, enophthalmos; entr, entrapped/entrapment; eso, esotropia; fl, floor; freq, frequent(ly); frac, fracture(s);grp, group; hem, hemorrhage; hyper, hypertropia; hypo, hypotropia; infraorb, infraorbital; inj, injury; iso, isolated; ltd, limited duction; lyo, lyophilizeddura; NS, not specified; orb, orbital; poly, porous polyethylene; req, requiring; restr, restricted motility; sil, silicone; strab, strabismus; subcil, sub-ciliary; surg, surg; transant, transantral; transorb, transorbital; transconj, transconjunctival; WEBOF, white-eye blowout fracture.aFractures requiring surgery.bWith endoscopic guidance.
Journal of AAPOS
176 Wei and Durairaj Volume 15 Number 2 / April 2011

Table 1C. Summary of selected reviewed articles specifically analyzing pediatric orbital floor fractures: Results
Study Conclusions/Recommendations
Leitch et al17 Children are not more likely than adults to have symptomatic postoperative diplopia.De Man et al13 Immediate surgery is recommended for children with decreased motility, forced ductions,
and CT evidence of blowout floor fractures.Gatot et al18 A transantral approach with catheter balloon is viable.Koltai et al15 Orbital floor fractures are more likely in children .7 years old.Sires et al19 Immediate repair for patients with oculocardiac reflex and entrapment is recommended.Jordan et al20 Surgery in 2-4 days of WEBOF led to improved motility outcomes versus standard 2-week watch-and-wait.Cope et al21 Younger patients are more likely than adults to have persistent problems after blowout fractures.Bansagi et al12 More complete return of ocular motility is likely after surgery within 2 weeks versus later surgery.Egbert et al9 Ductions and diplopia improve faster (median, 4 days) after surg within 7 days
of injury versus later surgery (median, 10.5 days).Hatton et al11 The floor is the most frequent location of orbital fractures in children, often requiring surgery.Kraus et al22 Nasoseptal cartilage is safe for reconstruction.Grant et al8 Patients with trapdoor fractures and restricted motility with early intervention had better postoperative function.Cohen et al23 Patients with trapdoor fractures who present with nausea and vomiting are at high risk of entrapment.Baek et al10 Inferior trapdoor fractures are a common type in children.Yoon et al24 Surg within 5 days of injury leads to more rapid and better postoperative improvement in
patients with severely restricted motility.Kwon et al25 Diplopia, restricted motility, and trapdoor fractures are more common in children than adults;
recovery is faster in children repaired within 5 days of injury.Lane et al26 WEBOF is frequently misdiagnosed in the primary care setting.Criden et al27 Despite surgery, recovery of ocular motility may take months in children.Lygidakis et al28 Satisfactory resolution of symptoms after surgery on blowout fractures was noted.Parbhu et al29 There is poor concordance between radiologic and intraoperative evidence for entrapment in children.Cobb et al30 Oculovagal reflex is often unrecognized.Gerbino et al31 Return of full extraocular motility is better when fractures are treated w/in 24 hours.Wang et al32 More complete resolution of motility limitation and diplopia after surgery within 1 month versus late repairs.Carroll et al33 Recovery times tend to increase with increasing delays in surgery.Kim et al14 Prompt surgery is recommended for patients with marked restricted motility and experiencing nausea and vomiting.
CT, computed axial tomography; WEBOF, white-eye blowout fracture.
Volume 15 Number 2 / April 2011 Wei and Durairaj 177
that it provided excellent imaging with high intra- and in-terrater agreement.In clinical practice, CT remains the imaging study of
choice in children with a suspected orbital floor fracturebecause it is fast, sensitive for fracture, and less costlythan MRI. MRI may be considered if there is clinical evi-dence of soft tissue entrapment that is not seen on CT orif there is concern for radiation. At this time, plain x-raysand ultrasounds are insufficient primary imaging modali-ties for pediatric orbital floor fractures.
Indications for Surgery
Commonly accepted indications for surgery for orbitalfloor fracture are symptomatic nonresolving diplopia, mus-cle or soft tissue entrapment on CT, and positive forcedductions or other clinical evidence of entrapment, enoph-thalmos (.2 mm at presentation), oculocardiac reflex (bra-dycardia, nausea, and syncope), fractures comprisinggreater than 50% of the orbital floor, or no clinical im-provement over several weeks.19,20,39 Ideally, surgeryshould not be performed on the basis of imaging alonebut on the basis of both radiologic and clinical evidenceof entrapment. Strong clinical evidence of entrapmentwithout radiologic confirmation has been advocated asgrounds for surgery given the high rate of trapdoorfractures with incarcerated muscle in children.12,20
Journal of AAPOS
Management
The timing of surgical repair for orbital floor fracturescontinues to evolve. Over the last half a century, recom-mendations for floor fractures in adults have ranged fromimmediate surgery to conservative watching and waitingfor 4-6 months.19,20,31,40 No prospective randomizedtrials have been done in children to determine theoptimal timing. Accepted indications for immediaterepair include nonresolving oculocardiac reflex, white-eyed blowout fracture, and early enophthalmos or hypo-globus.19,20
Bansagi and Meyer12 found that surgical interventionless than 2 weeks after injury resulted in a more completereturn of ocularmotility than later intervention in children.Egbert and colleagues9 also noted that resolution of duc-tion deficits or diplopia was suboptimal in children whowere repaired more than 1 month from time of injury. Jor-dan and colleagues20 studied 20 children with white-eyedblowout fractures and found a better and faster improve-ment in ocular motility in those operated on within 2-4days in comparison to 2 weeks and therefore recommendedsurgery within 2 days. More recently, Gerbino and col-leagues31 found that the return of extraocular motilitywas better when fractures were surgically corrected within24 hours of the initial injury. Thus for patients with symp-tomatic diplopia with positive forced ductions, CT-confirmed soft-tissue entrapment, or trapdoor fracture

FIG 1. Right white-eyed blowout fracture in a 12-year-old girl with im-paired supraduction on attempted upgaze.
FIG 2. High-resolution coronal head computed axial tomographydemonstrating left orbital trapdoor fracture with incarceration of theinferior rectusmuscle. Periorbital fat and inferior rectus have herniatedthrough the narrow linear fracture into the maxillary sinus, and thesubsequent “spring back” of the trapdoor bone flap strangulates thetissues with subsequent muscle necrosis (arrow).
FIG 3. Intraoperative visualization of orbital floor fracture via thetransconjunctival approach. The edge of the fracture can be seen an-teriorly, with entrapped muscle and periorbita posteriorly.
178 Wei and Durairaj Volume 15 Number 2 / April 2011
plus restricted ocular movement, surgery within 1-5 dayshas been shown to result in better postoperative ocular mo-tility, and it is generally recommended that surgery be un-dertaken within 48 hours of diagnosis.8,9,12,13,19,20,24,25,31,32
Additional rationale for early intervention includes the factthat patients who present late for surgery are often found tohave significant scarring, fibrosis, and callus formation inthe fracture area, making adequate reduction of orbitalcontents difficult.8,25
Methods of Repair
Surgical approaches to repair orbital floor fracture in chil-dren are similar to those in adults. Repair can be under-taken through transconjunctival, transcutaneous, ortransantral approaches. The transconjunctival approach isgenerally preferred by ophthalmologists and affords excel-lent direct visualization of the fracture (Figure 3); however,inexperienced orbital surgeons can encounter difficultywith visualization of the posterior orbital floor for releaseof entrapped tissue and positioning of implants. Becausetranscutaneous approaches have a higher incidence of ec-tropion and eyelid retraction compared to other ap-proaches, they are now rarely used. The transantral
approach can offer the benefit of better visualization ofthe posterior orbital floor, minimal lower eyelid injury,and the flexibility to repair the fracture without having towait for resolution of periorbital edema. This approach israrely used by orbital surgeons. The adjunctive use of en-doscopic guidance for better visualization has been re-ported in several series of patients with comparableoutcomes.10,14
Either alloplastic or autogenous implants can be usedto repair orbital floor fractures in children. Autogenousdonor sites include calvarium, iliac, rib, or cartilage (ear,nasal septum, etc).8,22 Grafting from the immatureskeleton carries the risk of growth retardation at thedonor site. Additional concerns with autografts includeincreased operation time, a second operation site, anddifficulty shaping the graft to fit the defect; however,Grant and colleagues8 found minimal donor site morbid-ity and easy forming of pericranial shaved bone grafts inchildren. Numerous allografts have also been used inthe repair of orbital floor fractures including porous poly-ethylene, gelatin film, nylon foil, polydioxanone, porcinedermis, and dura substitute. Advantages of alloplastic im-plants include availability, durability, choice of absorbableor nonabsorbable implants, and increased tensile strength.All alloplastic implants carry the risk of infection, migra-tion, extrusion, and foreign body reaction with excessivefibrosis. While many different types of implants havebeen studied extensively in adults, they have not beenstudied specifically in children. The implants most em-ployed according to the literature include porous polyeth-ylene, autogenous bone, dura, silicone, fluorocarbonpolymers, and gelatin film.8-10,12-14,20,21,31-33 Ultimately,technique and choice of implant are at the discretionand comfort of the surgeon as each has advantages anddisadvantages.
Complications
Possible complications from surgical repair of orbital floorfractures in children include infection, hemorrhage,
Journal of AAPOS

Volume 15 Number 2 / April 2011 Wei and Durairaj 179
motility problems (restriction and persistent diplopia),implant-related complications (migration/extrusion, pal-pable hardware, autologous graft donor site pain), muscleor optic nerve incarceration or compression, fistula, cystandmucocele formation, cosmesis, infraorbital dysesthesia,and lacrimal system problems (dacrocystitis, obstruction).The most commonly reported complication in all studiesreviewed is persistent diplopia. Other infrequent complica-tions include infection, subperiosteal hemorrhage, infraor-bital dysesthesia, enophthalmos, ectropion, epiphora, andreduced visual acuity.8,9,14,21,24,27,32 Persistent diplopiamay be a more common complication in children asa result of the unique pediatric trapdoor fracture patternthat results in direct damage to the extraocular muscles orpotentially the nerves themselves.10,21,23 Tissue ischemiaand the subsequent inflammatory response have beenhypothesized to lead to fibrosis and long-term decreasedmotility.8,19,23 Furthermore, children have rapid boneregeneration and in 1 week can form a callus arounda fracture that makes accurate surgical reapproximation ofthe fracture edges challenging.25 Later intervention wasalso found to be associated with more motility complica-tions.8,9,12,19,20,24,25,31,32 The combination of pediatricpathophysiology and delayed repair may be responsiblefor the high rate of extraocular motility restriction andpersistent diplopia.
Discussion
Most studies have found that earlier surgical interventionfor children with entrapment results in better outcomesthan later intervention.8,9,12,19,20,24,25,31,32 Whencomparing children to adults, some studies suggest thatthe overall long-term outcomes of children after surgicalorbital floor fracture repair (regardless of timing) are worsethan those of adults.13,21 Cope and colleagues21 studied 45children with orbital floor blowout fractures and found thatthe youngest age group (\9 years) had the highest inci-dence of persistent diplopia (over 50%) and that the diplo-pia took twice as long to resolve compared to olderchildren. Resolution of diplopia in children \9 yearstook between 10 and 18 months, and they were more likelyto have small, linear trapdoor defects of the anterior orbitalfloor with resultant entrapment.21
The poorer outcomes in children may be contributing tothe reportedly high rate of misdiagnosis and underrecogni-tion of orbital floor fractures with entrapment. Review ofthe literature concerning initial evaluation and manage-ment of pediatric orbital floor fractures in the emergencydepartment has shown that white-eyed blowout fracturesand orbital floor fractures presenting with oculocardiac re-flex symptoms go unrecognized and uninvestigated in asmany as one third of pediatric facial trauma patients be-cause the symptoms are attributed to concussion.26,30
Consequently, ophthalmologic evaluation and orbital CTare delayed while the patients undergo observation forconcussion. This period of observation in children with
Journal of AAPOS
entrapped orbital floor fractures increases the risk of muscleischemia, permanent motility restriction, and diplopia.
Conversely, some authors have found no difference infinal outcome between children and adults. Leitch and col-leagues17 found that pediatric patients who underwentblowout fracture repair did not have more symptomaticpostoperative diplopia than adults. Others have foundthat while children often have a longer period of recoverythan adults, they have no difference in complications orlong-term outcome.25,33 In fact, Criden and Ellis27 foundthe recovery of extraocular motility to be prolonged inhis cohort of children despite an early surgical intervention.
In conclusion, nearly all studies done on pediatric orbitalfloor fractures have been retrospective case series or chartreviews, often with small numbers of patients. Direct com-parisons of different surgical methods and implant typeshave not been performed. As current studies have shown,orbital floor fractures in children have unique aspects interms of the type of fracture, clinical presentation, and con-siderations for management. Additionally, outcomes inchildren with orbital floor fractures differ from adults.The weight of the literature supports earlier surgical inter-vention in children given the higher likelihood of entrap-ment, potentially subtle presentation, and worseoutcomes with delayed treatment. Long-term prospectivestudies are certainly needed to further characterize orbitalfloor fractures in children.
References
1. Smith B, ReganWF. Blow-out fracture of the orbit. Am JOphthalmol1957;44:733-9.
2. Fujino T. Experimental “blow out” fracture of the orbit. PlastReconstr Surg 1974;54:81-2.
3. Rhee JS, Kilde J, Yoganadan N, Pintar F. Orbital blowout fractures:Experimental evidence for the pure hydraulic theory. Arch FacialPlast Surg 2002;4:98-101.
4. Gilliland GD, Gilliland G, Fincher T, Harrington J, Gilliland JM.Assessment of biomechanics of orbital fracture: A study in goats andimplications for oculoplastic surgery in humans. Am J Opthalmol2005;140:868-76.
5. Warwar R, Bullock J, Ballal DR, Ballal R.Mechanisms of orbital floorfractures: A clinical, experimental, and theoretical study. OphthalPlast Reconstr Surg 2000;16:188-200.
6. Tong L, Bauer RJ, Buchman SR. A current 10-year retrospective sur-vey of 199 surgically treated orbital floor fractures in a nonurbantertiary care center. Plast Reconstr Surg 2001;108:612-21.
7. Hwang K, You SH, Soh IA. Analysis of orbital bone fractures: A 12-year study of 391 patients. J Craniofac Surg 2009;20:1218-23.
8. Grant JH, Patrinely JR, Weiss AH, Kierney P, Gruss J. Trapdoorfracture of the orbit in the pediatric population. Plast Reconstr Surg2002;109:482-9.
9. Egbert JE, May K, Kersten RC, Kulwin DR. Pediatric orbital floorfractures: Direct extraocular muscle involvement. Ophthalmology2000;107:1875-9.
10. Baek SH, Lee EY. Clinical analysis of internal orbital fracture in chil-dren. Korean J Ophthalmol 2003;17:44-9.
11. Hatton MP, Watkins LM, Rubin PA. Orbital fractures in children.Ophthal Plast Reconstr Surg 2001;17:174-9.
12. Bansagi ZC, Meyer DR. Internal orbital fractures in the pediatric agegroup: Characterization andmanagement. Ophthalmology 2000;107:829-36.

180 Wei and Durairaj Volume 15 Number 2 / April 2011
13. DeMan K,Wijngaarde R, Hes J, de Jong PT. Influence of age on themanagement of blow-out fractures of the orbital floor. Int J OralMax-illofac Surg 1991;20:330-36.
14. Kim J, Lee H, Chi M, Park M, Lee J, Baek S. Endoscope-assistedrepair of pediatric trapdoor fractures of the orbital floor: Character-ization and management. J Craniofac Surg 2010;21:101-5.
15. Koltai PJ, Amjad I, Meyer D, Feustel PJ. Orbital fractures in children.Arch Otolaryngol Head Neck Surg 1995;121:1375-9.
16. Chapman VM, Fenton LZ, GaoD, Strain JD. Facial fractures in chil-dren: Unique patterns of injury observed by computed tomography.J Comput Assist Tomogr 2009;33:70-72.
17. Leitch RJ, Burke JP, Strachan IM. Orbital blowout fractures—Theinfluence of age on surgical outcome. Acta Ophthalmol (Copenh)1990;68:118-24.
18. GatotA,ToviF.Early treatment of orbital floor fractureswith catheterballoon in children. Int J Pediatr Otorhinolaryngol 1991;21:97-101.
19. Sires BS, Stanley RB, Levine LM. Oculocardiac reflex caused by or-bital floor trapdoor fracture: An indication for urgent repair. ArchOphthalmol 1998;116:955-6.
20. Jordan DR, Allen LH,White J, Harvey J, Pashby R, Esmaeli B. Inter-vention within days for some orbital floor fractures: the white-eyedblowout. Ophthal Plast Reconstr Surg 1998;14:379-90.
21. Cope MR, Moos KF, Speculand B. Does diplopia persist after blow-out fractures of the orbital floor in children? Br J OralMaxillofac Surg1999;37:46-51.
22. Kraus M, Gatot A, Kaplan DM, et al. Post-traumatic orbital floor re-construction with nasoseptal cartilage in children. Int J Pediatr Oto-rhinolaryngol 2002;64:187-92.
23. Cohen SM, Garrett CG. Pediatric orbital floor fractures: Nausea/vomiting as signs of entrapment. Otolaryngol Head Neck Surg2003;129:43-7.
24. Yoon KC, Seo MS, Park YG. Orbital trapdoor fracture in children.J Korean Med Sci 2003;18:881-5.
25. Kwon JH, Moon JH, Kwon MS, et al. The differences of blowoutfracture of the inferior orbital wall between children and adults.Arch Otolaryngol Head Neck Surg 2005;131:723-7.
26. Lane K, Penne RB, Bilyk JR. Evaluation andmanagement of pediatricorbital fractures in a primary care setting. Orbit 2007;26:183-91.
27. Criden MR, Ellis FJ. Linear nondisplaced orbital fractures with mus-cle entrapment. J AAPOS 2007;11:142-7.
28. Theologie-Lygidakis N, Iatrou I, Alexandridis C. Blow-out fracturesin children: Six years’ experience. Oral Surg Oral Med Oral PatholOral Radiol Endod 2007;103:757-63.
29. Parbhu KC, Galler KE, Li C, et al. Underestimation of soft tissue en-trapment by computed tomography in orbital floor fractures in thepediatric population. Ophthalmology 2008;115:1620-25.
30. Cobb A, Murthy R, Manisali M, et al. Oculovagal reflex in paediatricorbital floor fractures mimicking head injury. Emerg Med J 2009;26:351-3.
31. Gerbino G, Roccia F, Bianchi FA, et al. Surgical management of or-bital trapdoor fracture in a pediatric population. J Oral MaxillofacSurg 2010;68:1310-16.
32. Wang NC, Ma L, Wu SY, et al. Orbital blow-out fractures in chil-dren: Characterization and surgical outcome. Chang Gung Med J2010;33:313-20.
33. Carroll SC, Ng SGJ. Outcomes of orbital blowout fracture surgery inchildren and adolescents. Br J Ophthalmol 2010;94:736-9.
34. WojnoTH.The incidenceof extraocularmuscle and cranial nerve palsyin orbital floor blow-out fractures. Ophthalmology 1987;94:682-7.
35. Jank S, Emshoff R, Etzeldorfer M, et al. Ultrasound vs computed to-mography in the imaging of orbital floor fractures. J Oral MaxillofacSurg 2004;62:150-54.
36. Jank S, Deibl M, Strobl H, et al. Interrater reliability of sonographicexaminations of orbital floor fractures. Eur J Radiol 2005;54:344-51.
37. Freund M, Hahnel S, Sartor K. The value of magnetic resonance im-aging in the diagnosis of orbital floor fractures. Eur Radiol 2002;12:1127-33.
38. Kolk A, Stimmer H, Klopfer M, et al. High resolution magnetic res-onance imaging with an orbital coil as an alternative to computed to-mography scan as the primary imaging modality of pediatric orbitalfractures. J Oral Maxillofac Surg 2009;67:348-56.
39. BurnstineMA.Clinical recommendations for repair of isolated orbitalfloor fractures. Ophthalmology 2002;109:1207-13.
40. Putterman AM, Stevens TS, Urist MJ. Nonsurgical management ofblow-out fractures of the orbital floor. Am J Ophthalmol 1974;77:232-9.
Journal of AAPOS