pediatric neck masses - utmb home | utmb · pdf file1 y ± 14 y 6.0 y suppurative...
TRANSCRIPT

Pediatric Neck Masses
Mark Domanski, M.D. Michael Underbrink, M.D. Dept. of Otolaryngology University of Texas Medical Branch, Galveston October 31st, 2007
1

Total % of total
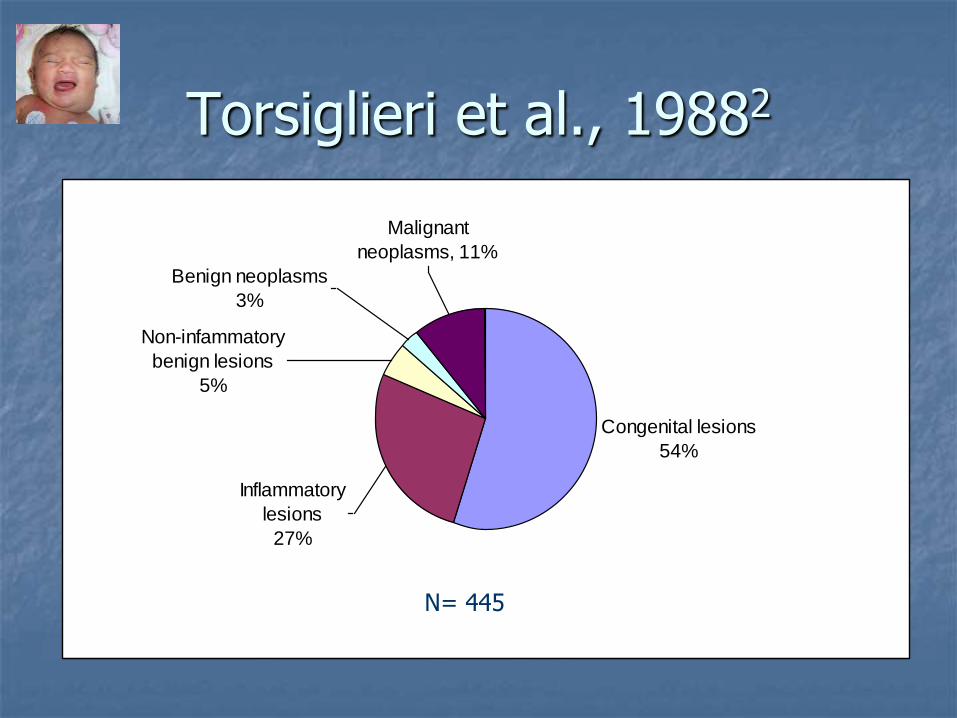
Congeital lesions 244 55% Branchial cleft cyst 78 18% Thyroglossal duct cyst 73 16% Dermoid cyst 43 10% Lymphangioma 34 8% Hemangioma 10 2% Teratoma 2 Bronchogenic cyst 2 Thymic cyst 1 Myelomeningocele 1 Inflammatory lesions 118 27% Reactive lympadenopathy 71 16% Undetermined etiology 66 15% Sinus histiocytosis 5 1% Granulomatous disease 32 7% Atypical mycobacteria 20 4% Cat scratch disease 6 1% Toxoplasmosis 2 Sarcoid 2 Suppurative lympadenitis 10 2% Sialadenitis 5 1%
Non-infammatory benign lesions
23 5%
Inclusion cyst 13 3% Fibromatosis 9 2% Keliod 1 Benign neoplasms 12 3% Neurofibroma 3 1% Lipoma 3 1% Lipoblastoma 2 Paraganglioma 1 Goiter 1 Benign mixed tumor 1 Osteoblastoma 1 Malignant neoplasms 48 11% Lymphoma 34 8% Hodgkin's 23 5% Non-Hodkin's 11 2% Thyroid Carcinoma 6 1% Rhabdomyosarcoma 2 Neuroblastoma 2 Fibrous histiocytoma 1 Acinic cell carcinoma 1 Histiocytosis X 1 Chloroma 1 Total 445
Torsiglieri et al., 19882
Torsiglieri et al., 19882
Inflammatory
lesions
27%
Malignant
neoplasms, 11%
Benign neoplasms
3%
Non-infammatory
benign lesions
5%
Congenital lesions
54%
N= 445

Initial Evaluation
H&P Age
Onset
Rapidity of growth
Fluctuation in size
Pain
Infection
Trauma
Travel
Exposure
PE Size
Multiplicity
Laterality
Consistency
Color
Mobility
Tenderness
Fluctuation
Congenital
Inflammatory
Benign
Malignant

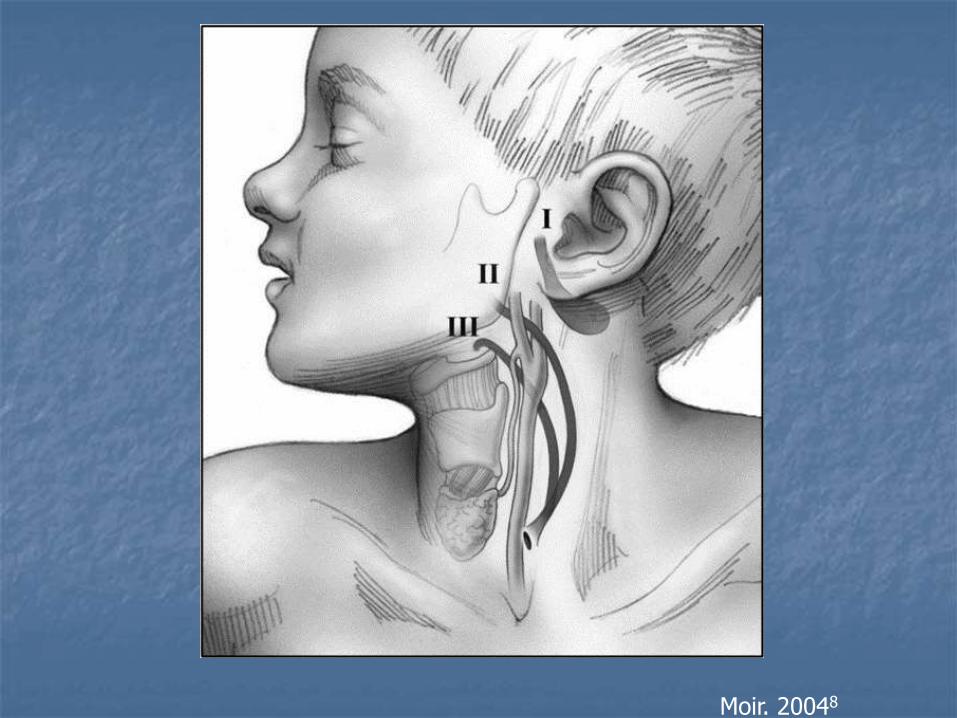
Location, Location, Location!
Moir. 20048

Age of Distrubtion Range Average (years)
Brachial cleft cyst 6m – 16 y 3.6 y Thyroglossal duct cyst 9 m – 17 y 6.1 y Dermoid cyst 9 m – 15 y 3.7 y Lymphangioma 9m – 15 y 3.6 y Hemangioma 1 day – 15 y 5.6 y Reactive lymphadenopathy
3 m – 18 y 8.0 y
Graunlomatous disease
1 y – 14 y 6.0 y
Suppurative lymphadenitis
4 m – 15 y 7.3 y
Sialadenitis 11 y – 13 y 11.2 y Inclusion cyst 3 y – 12 y 4.4 y Fibriomatosis 1 m – 10 y 3.1 y Lymphoma 4 y – 21 y 11.7 y Thyroid Carcinoma 8 y – 17 y 12.3 y Others 2 weeks – 18 y 4.6 y
Torsiglieri et al., 19882

Likely Etiology Determines Direction of Testing
X-ray
U/S
CT
MRI
FNA
Surgical Biopsy
Tissue Culture
CXR
Labs
PPD
Gram stain
Culture

Pediatric Neck Masses
1. Congenital lesions
2. Inflammatory lesions
3. Non-inflammatory benign lesions
4. Benign neoplasms
5. Malignant neoplasms

Pediatric Neck Masses
1. Congenital lesions
2. Inflammatory lesions
3. Non-inflammatory benign lesions
4. Benign neoplasms
5. Malignant neoplasms

1. Congenital Lesions
Branchial cleft cyst 78 18% Thyroglossal duct cyst 73 16% Dermoid cyst 43 10% Lymphangioma 34 8% Hemangioma 10 2% Teratoma 2 Bronchogenic cyst 2 Thymic cyst 1 Myelomeningocele 1
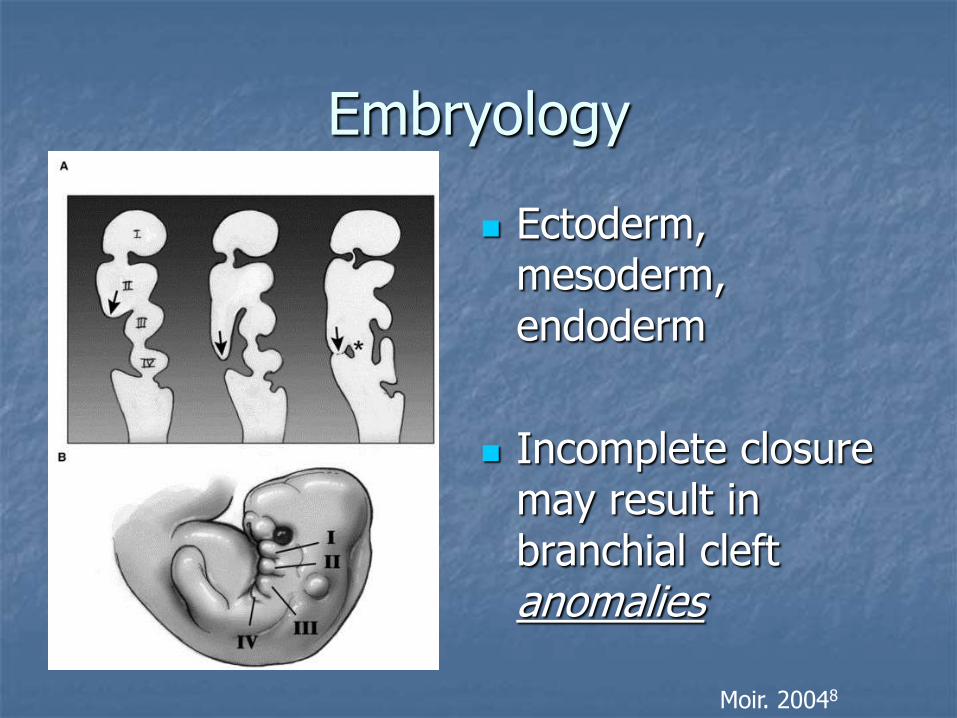
Embryology
Ectoderm, mesoderm, endoderm
Incomplete closure may result in branchial cleft anomalies
Moir. 20048

Development of First Four Arches
Nicollas. 20003
Each arch layer gives rise to:
•nerve (ectoderm)
•artery, muscle and cartilage (mesoderm)
•glands (endoderm).

Cyst Sinus Fistula
Schroeder. 20074
Branchial Cleft Anomalies

Distribution of neck malformations as cysts, fistulas, or sinuses
per Nicollas et. al. (n=191)
Nicollas. 20003
(Sinus)
Total 139 5 47 191
Moir. 20048

Imagining in Branchial Cleft Cysts
MRI
More reliably confirms cystic nature
More precisely defines lesion
Better to delineate glandular tissue
ie fat planes
CT
Adequate for most lesions
Cost, availability
U/S
cystic vs noncystic
does not evaluate extent
Both MRI and CT have difficulty distinguishing branchial cleft cyst from lymphangioma in children.
Branstetter, 20069

1st Branchial Cleft Cyst, Type II
Type I Ectodermal duplication of
EAC Near external auditory
canal Usually inferior and
posterior to tragus
Type II Associated with
submandibular gland
Branstetter, 20069
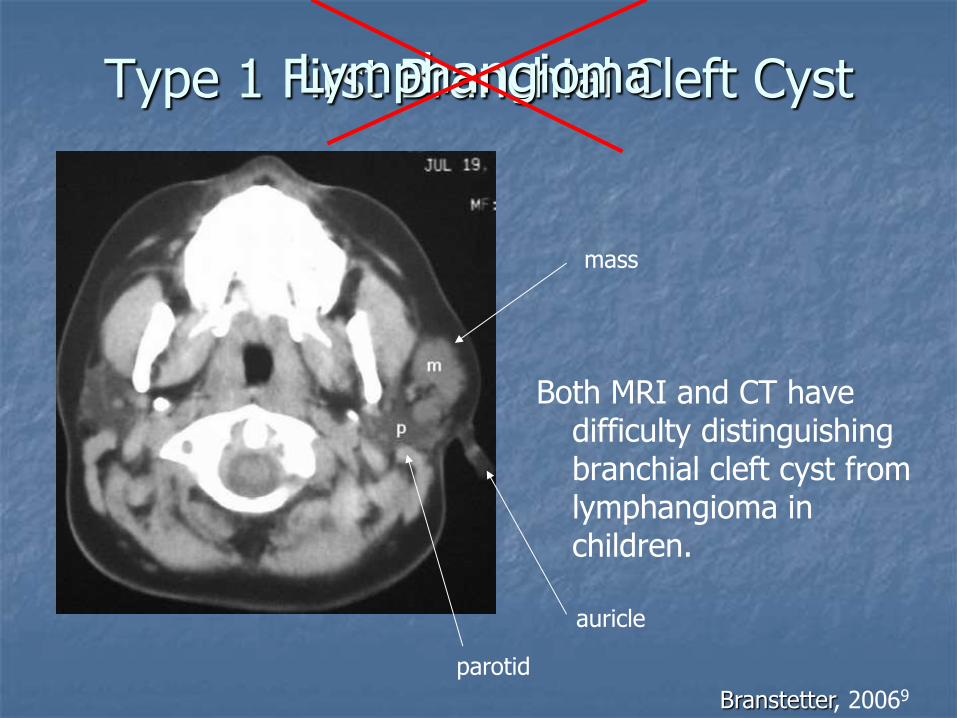
Type 1 First Branchial Cleft Cyst
Both MRI and CT have difficulty distinguishing branchial cleft cyst from lymphangioma in children.
Branstetter, 20069
Lymphangioma
mass
auricle
parotid

Branchial Cyst
Noncalcified mass
CT shows lesion under SCM
Malik et al, 20026

2nd Brachial Cleft Cyst T2 MRI
Posterior to R submandibular gland
Thickened walls suggest prior hemorrhage or infection
Gujar and Mukherji 20045

Anterior to carotid bifurcation
Schroeder et al, 20074

Under the anterior SCM
Schroeder et al, 20074
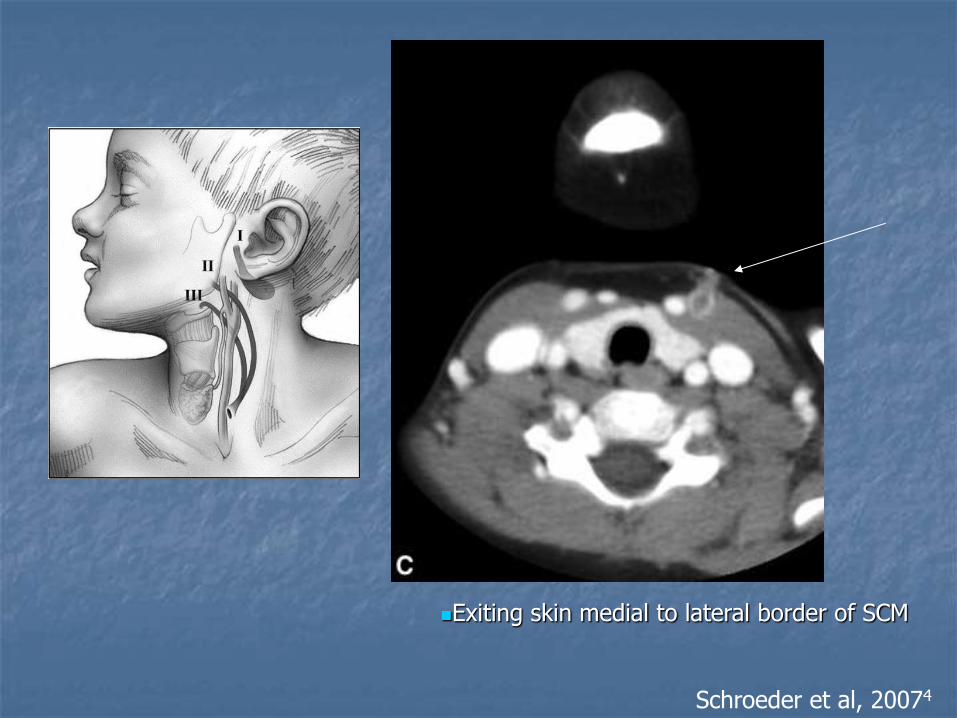
Exiting skin medial to lateral border of SCM
Schroeder et al, 20074

Left 2nd BA Fistula
Anterior to carotid bifurcation Under the anterior SCM Exiting skin medial to lateral border of SCM
Schroeder et al, 20074

Moir. 20048

Moir. 20048

Moir. 20048
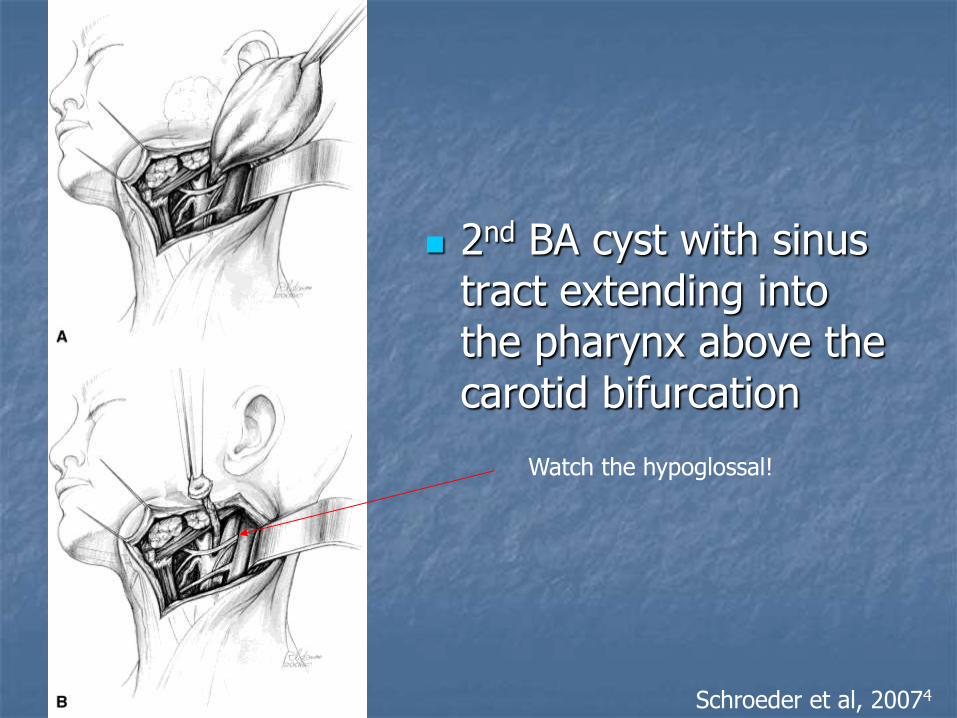
2nd BA cyst with sinus tract extending into the pharynx above the carotid bifurcation
Schroeder et al, 20074
Watch the hypoglossal!

Preauricular Sinus
Not related to 1st branchial cleft anomalies
Active infection during excision increases chance of recurrance
Moir. 20048

Thyroglossal Duct Cyst
persistent tract from the descent of the thyroid from the foramen cecum
epithelial lining composed of either squamous or respiratory epithelium
confirm normal thyroid tissue
Learning Radiology.com 200711
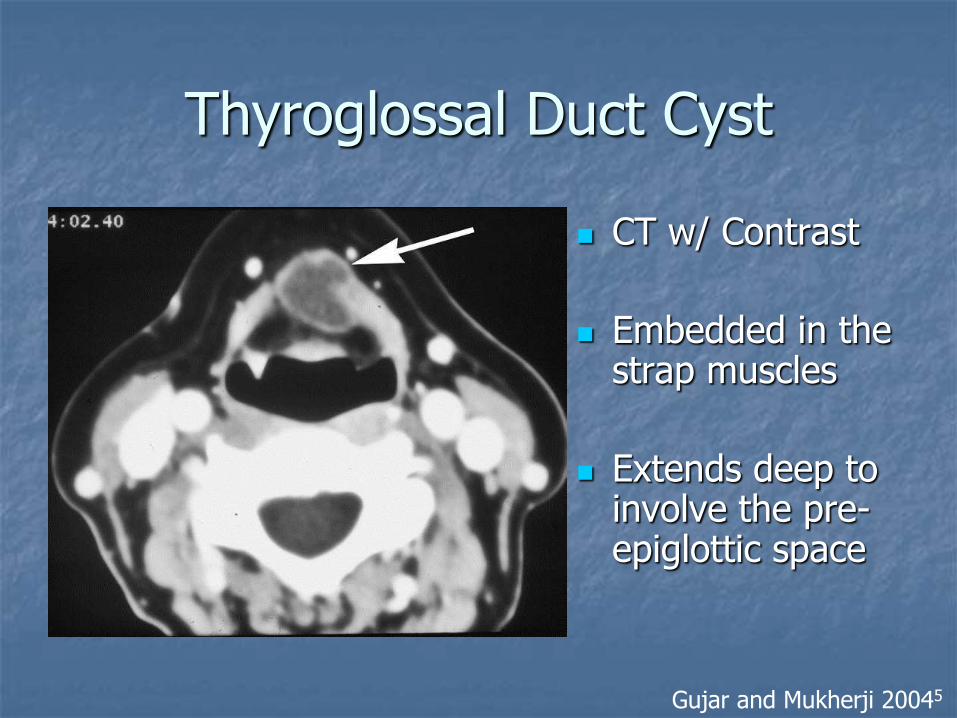
Thyroglossal Duct Cyst
CT w/ Contrast
Embedded in the strap muscles
Extends deep to involve the pre-epiglottic space
Gujar and Mukherji 20045
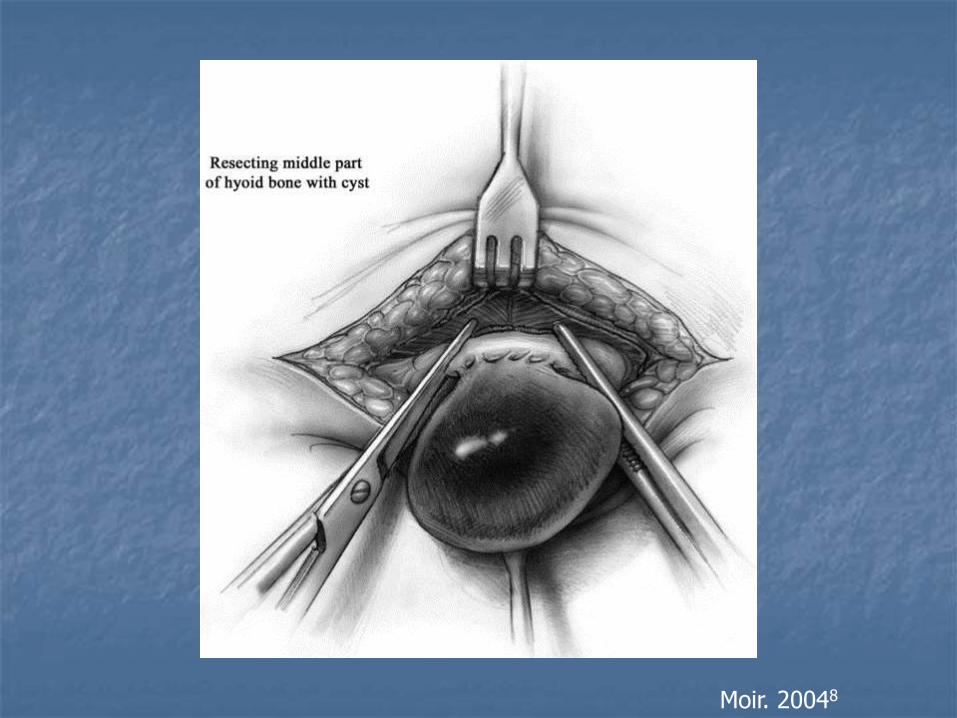
Moir. 20048

Moir. 20048

Dermoid Cysts
Ectoderm and mesoderm
7% of dermoid cysts occur in head and neck
Thought to be of congenital inclusion type
mean diameter = 1.2 cm (0.6-3.3)
Treatment: complete excision
Pryor et al 200512

Dermoid Cysts – Cranial Theory
Grunwald in 1910
As neuroectodermal tract recedes, demal attachements follow its course and can form a sinus or cyst
Beware of possible intracranial involvement
Pryor et al 200512

•Orbit is the most common site for dermoids in the head and neck (61%)
•Direct excision is sufficient for neck dermoids, more extensive approaches (craniotomy, mastoidectomy) are needed for other sites
Diff dx: in midline of neck: thyroglossal duct cyst
in head & neck, n = 59
Pryor et al 200512
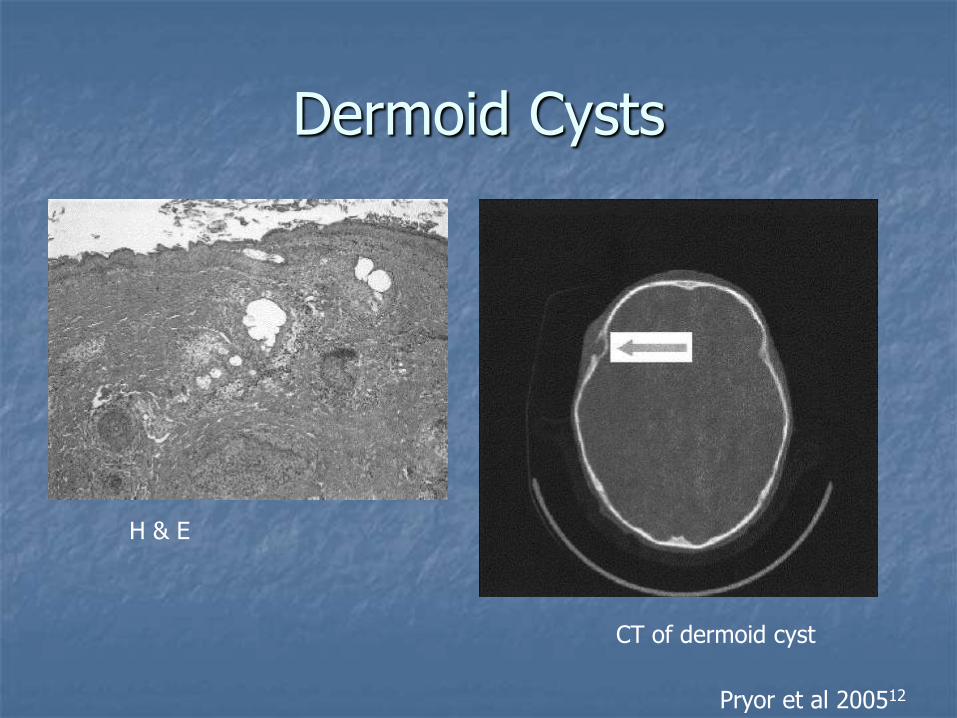
Dermoid Cysts
H & E
CT of dermoid cyst
Pryor et al 200512

Teratoma
H&N account for ~2% of teratomas
Newborn – 2.5 yr at presentation
All 3 germinal layers present
Mostly benign lesions amenable to curative excision
Wakhlu A et al 200013

Teratoma
• Prognosis good if no respiratory compromise
• Usually well differentiated and recurrence is uncommon
• Antenatal diagnosis is routine in developed world
Wakhlu A et al 200013
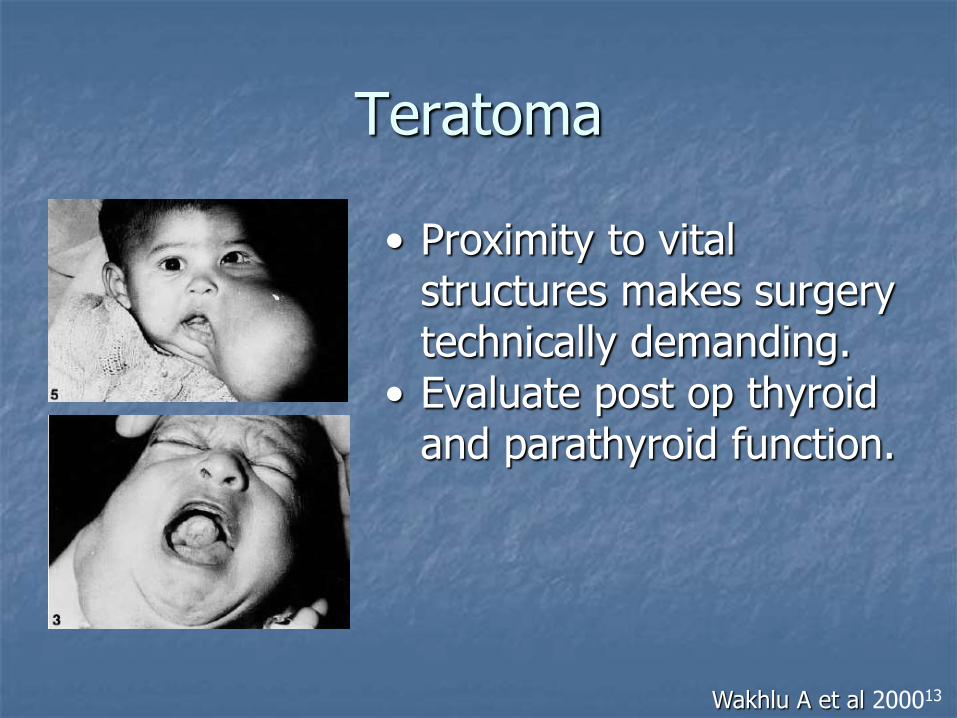
Teratoma
• Proximity to vital structures makes surgery technically demanding.
• Evaluate post op thyroid and parathyroid function.
Wakhlu A et al 200013

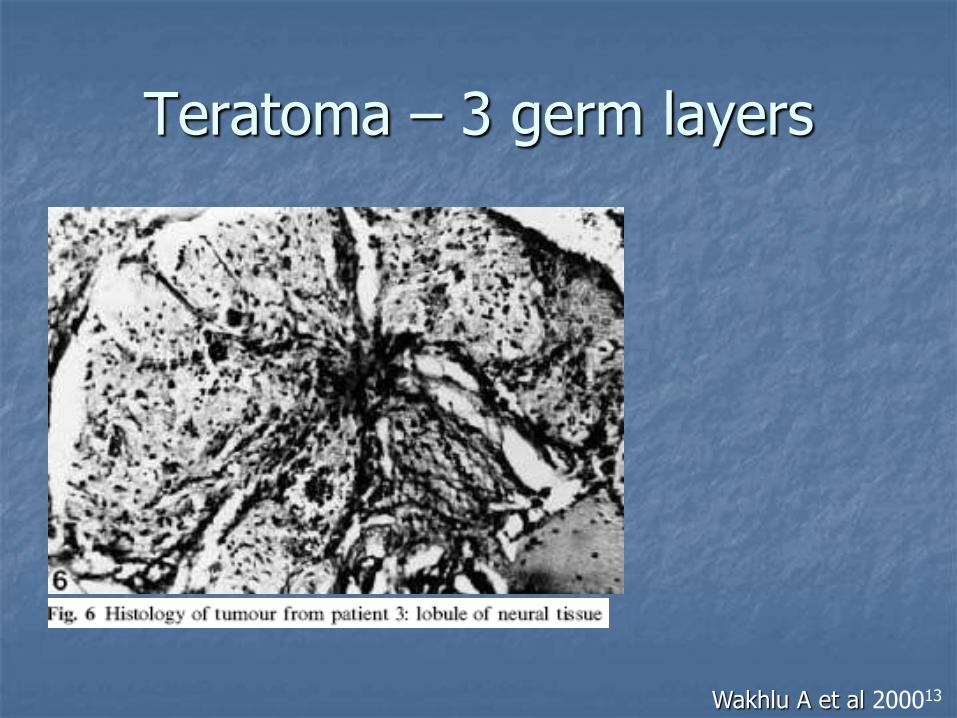
Teratoma – 3 germ layers
Arise from pluripotent cells and ectopic embryogenic non-germ cells
Wakhlu A et al 200013

Teratoma – 3 germ layers
Wakhlu A et al 200013
Teratoma – 3 germ layers
Wakhlu A et al 200013

Hypopharyngeal Teratoma
calcified calcification and fat
Malik et al, 20026

Teratoma T1 MRI
Fatty
Calcified
Gujar and Mukherji 20045

Lymphangioma
Benign, multiloculated, soft
Posterior neck triangle predominance
Multi-septated, insinuating lesions
Infiltrate and cross tissue planes
Most occur by 2 yrs of age
Incidence: 1 in 6,000 to 16,000 births
Burezq 200614 Head and and Neck Surgery, 200615

Lymphatic Vascular malformation
T1 MRI
High signal represents proteinaceous fluid
Crosses tissue planes
Gujar and Mukherji 20045

Centrifugal vs Centripetal
Centrifugal theory
the lymphatic system develops as mesenchymal spaces that later coalesce into a system of vessels that eventually join the venous system.
Centripetal theory
jugular and posterior lymphatics form as outgrowths of endothelium from veins into the surrounding mesenchyme.
Burezq 200614

Classification
Size:
Microcystic: capillary lymphangiomas lesions are less than 1 cm in diameter
Macrocystic: cystic hygromas cysts are larger than 1 cm
Cystic hygromas #1 type of lymphangioma
Gross et al, 200616

Cystic Hygroma
Noncalcified
Septated on U/S
Malik et al, 20026

Cystic Composition
5-year-old boy with lymphangioma
L parotid & parapharyngeal space
mixed macro- andmicrocystic type
Treated by surgical resection
Gross et al, 200616

Type 1 First Branchial Cleft Cyst
Both MRI and CT have difficulty distinguishing branchial cleft cyst from lymphangioma in children.
Branstetter, 20069
Lymphangioma
mass
auricle
parotid

Burezq et al, 2006 (expert opinion)
1. Error in establishing a communication between the lymphatic and venous system
Cystic hygroma
2. Error in morphogenesis of lymphatic system: this includes other types of lymphatic malformations
microcystic, macrocystic and mixed lymphatic lesions
Burezq 200614

Management - Controversial
Spontaneous resolution? Formation of new lymphatic channels?
Serial aspiration?
Sclerosant Agents? OK-432 (lyophilizied mixture of low-virulence group A Sterp
pyogens
Surgical Excision? Is the surgical risk out weigh the benefit in a benign lesion
Burezq 200614
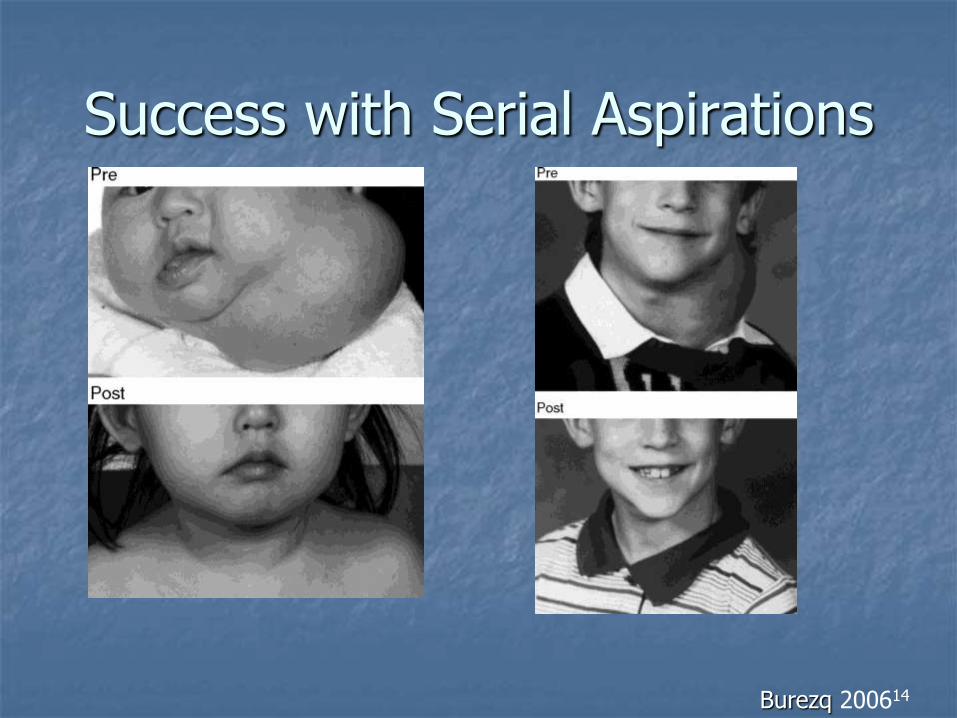
Success with Serial Aspirations
Burezq 200614

Success with OK-432
Supraclavicular macrocystic lymphangioma
Gross et al, 200616
Hemangioma
Less than 1/3 present at birth
Usually seen in 1st few months of life and enlarge progressively
90% cases involutes spontaneously
Sclerosing agents controversial

Glut-1
erythrocyte-type glucose transporter
found only in microvascular endothelia of blood–tissue barriers such as in the central nervous system, retina, placenta, ciliary muscle, and endoneurium of peripheral nerves
Hemangiomas stain consistently for Glut-1, in all stages of development and involution whereas vascular malformations did not
Mo et al, 200617
MacArther, 200618

Pediatric Neck Masses
1. Congenital lesions
2. Inflammatory lesions
3. Non-inflammatory benign lesions
4. Benign neoplasms
5. Malignant neoplasms

Pediatric Neck Masses
1. Congenital lesions
2. Inflammatory lesions
3. Non-inflammatory benign lesions
4. Benign neoplasms
5. Malignant neoplasms
2. Inflammatory Lesions
Reactive lympadenopathy 71 16% Undetermined etiology 66 15% Sinus histiocytosis 5 1% Granulomatous disease 32 7% Atypical mycobacteria 20 4% Cat scratch disease 6 1% Toxoplasmosis 2 Sarcoid 2 Suppurative lympadenitis 10 2% Sialadenitis 5 1%

When does cervical lymphadenopathy require FNA?
Benign reactive lymph node may persist for weeks to months
Lymphoma can present the same way
Rapkiewicz et al 200721
To FNA or not to FNA?
Reactive lymphadenopathy the most likely etiology of pediatric neck masses
Diagnostic dilema: a mass that does not resolve after initial treatment
Rapkiewicz et al 200721

FNA ancillary studies
Gram stain, culture
Acid fast stain
Imunocytochemistry
Cytogenetics
Rapkiewicz et al 200721

Limitations to FNA
A lesion may not be homogenous
FNA samples only part of the mass
May miss the true lesion
Unable to appreciate histological architecture
Rapkiewicz et al 200721

Time to contemplate open biopsy
Enlarging mass
Poor response to medical treatment
Suspicious clinical course
Unusual image findings
Systemic symptoms
Rapkiewicz et al 200721

Case – F.R.
8 y/o female, hx + PPD several yrs prior
Presents with R cervical adenopathy
FNA suggests granuloma
Repeat FNA -> same result
AFB stain and cultures negative
Clarithromycin and ethambutol started
Rapkiewicz et al 200721

Case – F.R.
Adenopathy and pain increased
Third FNA non-diagnostic
CT shows bulky homogenous lymphadenopathy of R upper spinal accessory and upper jugular chains.
Open biopsy displayed Hodgkin's lymphoma.
Rapkiewicz et al 200721

Reactive Lymphadenopathy
3-year-old child
Multiple hypoechoic lesions
variable shape and sizes
consistent with reactive lymph nodes
Malik et al, 20026

Enlarged Lymph Node
Nonspecific
Cause:
cryptococcal adenitis
Yeastlike fungus
Gujar and Mukherji 20045

Atypical mycobacteria: ex: cryptococcus
Saprobe in nature
worldwide distribution
Found in soil
Portal of entry is lung
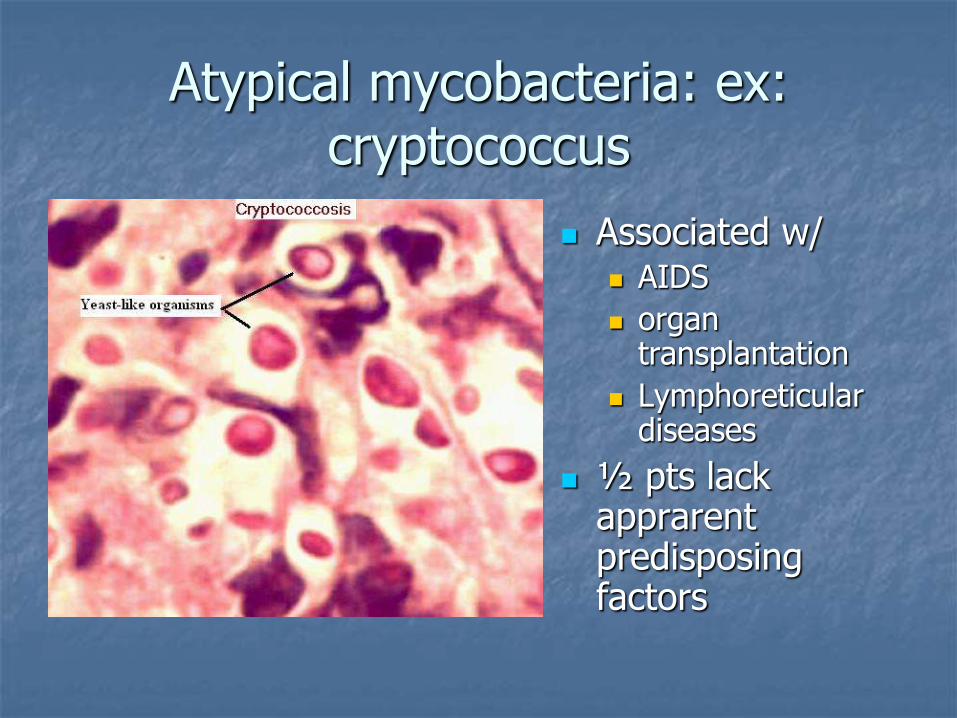
Atypical mycobacteria: ex: cryptococcus
Associated w/ AIDS
organ transplantation
Lymphoreticular diseases
½ pts lack apprarent predisposing factors

Bartonella henselae
Hypoechoic masses with irregular rim of isoechoic tissue
Biopsy: Cat Scratch Disease
Malik et al, 20026

Bartonella henselae
Gram – coccobacillus
2- 14 day incubation
Dx: requires prolonged incubation (2 + weeks)
Rx: erythromycin 1-4 m (unclear efficacy)
Normally benign course
Malik et al, 20026
In heart valve

Peritonsillar Abcess
Soft tissue density in submental space
Malik et al, 20026

Retropharyngeal Abscess
Widening of prevertebral space
Malik et al, 20026

Retropharyngeal Space Abscess
Gujar and Mukherji 20045

Retropharyngeal Peritonsillar
Malik et al, 20026

Sppurative Cervical Adenitis
hypoechoic
Malik et al, 20026

Thyroid Abscess
Malik et al, 20026

Pediatric Neck Masses
1. Congenital lesions
2. Inflammatory lesions
3. Non-inflammatory benign lesions
4. Benign neoplasms
5. Malignant neoplasms

Pediatric Neck Masses
1. Congenital lesions
2. Inflammatory lesions
3. Non-inflammatory benign lesions
4. Benign neoplasms
5. Malignant neoplasms

3. Non-inflammatory Benign Lesions
Inclusion cyst 13 3% Fibromatosis 9 2% Keloid 1

Inclusion Cyst
Acquired dermoid cysts result from a part of the skin being traumatically
implanted in the deeper layers after ectopic formation of a dermal cyst lined with squamous epithelium.
Congenital inclusion dermoid cysts form along the lines of embryologic fusion and contain both dermal and epidermal derivatives. Dermoid cysts of the head and neck are thought to be
the congenital inclusion type.
Pryor et al 200512

Inclusion Cyst
many cysts originate from the infundibular portion of the hair follicle, and the more general term, epidermoid cyst, is favored
Becker et a, 200519

Epidermal Inclusion Cyst
Cyst containing keratinous material true epidermis with a granular layer and adjacent laminated keratinous material
Becker et al, 200519
Torticollis

Fibromatosis Colli
SCM
Isoechoic mass
CT shows isodense mass R side
Note normal SCM on L side
Malik et al, 20026

Fibromatosis Colli - FNA
Paucicellular specimen
Bland spindle cell cytology
r/o nodular fascitis and fibrosarcoma
Rapkiewicz et al 200721

Fibromatosis Colli
r/o nodular fascitis and fibrosarcoma
Roy, 200720
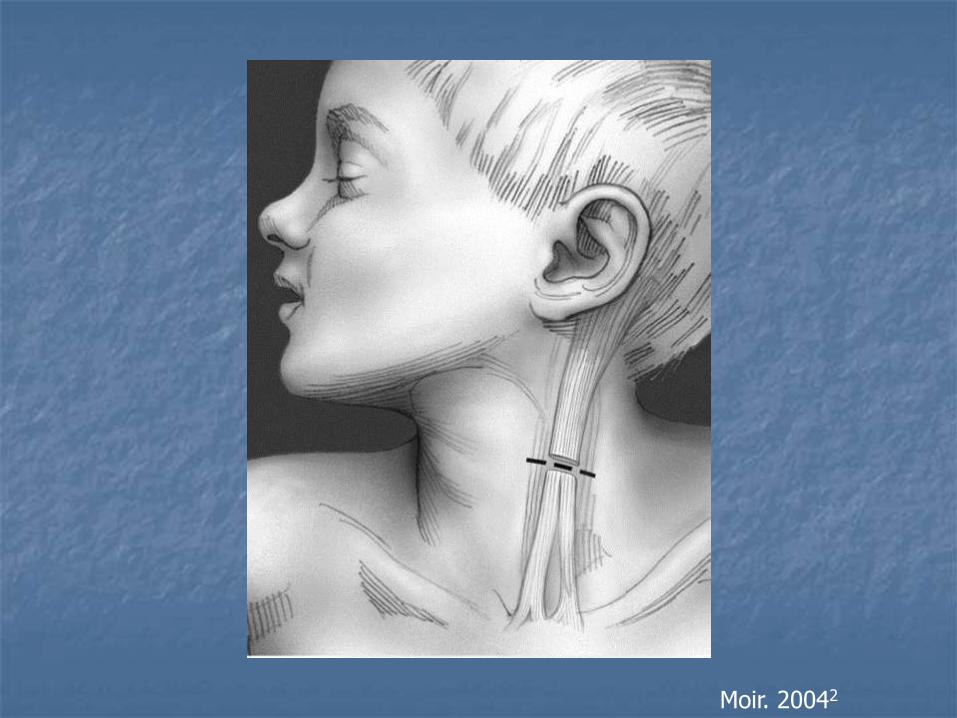
Moir. 20042

Pediatric Neck Masses
1. Congenital lesions
2. Inflammatory lesions
3. Non-inflammatory benign lesions
4. Benign neoplasms
5. Malignant neoplasms

Pediatric Neck Masses
1. Congenital lesions
2. Inflammatory lesions
3. Non-inflammatory benign lesions
4. Benign neoplasms
5. Malignant neoplasms

4. Benign Neoplasms
Neurofibroma 3 1% Lipoma 3 1% Lipoblastoma 2 Paraganglioma 1 Goiter 1 Benign mixed tumor 1 Osteoblastoma 1

Neurofibroma
solitary lesion
vs
part of the generalized syndrome of neurofibromatosis NF-1, aka von Recklinghausen disease
NF-2
Believed to arise from Schwann cell but origin uncertain

Neurofibroma
solitary lesion
vs
part of the generalized syndrome of neurofibromatosis NF-1, aka von Recklinghausen disease
NF-2
Believed to arise from Schwann cell but origin uncertain

Neurofibroma
T2 MRI
Central low T2 signal is characteristic of neurofibromas
Gujar and Mukherji 20045

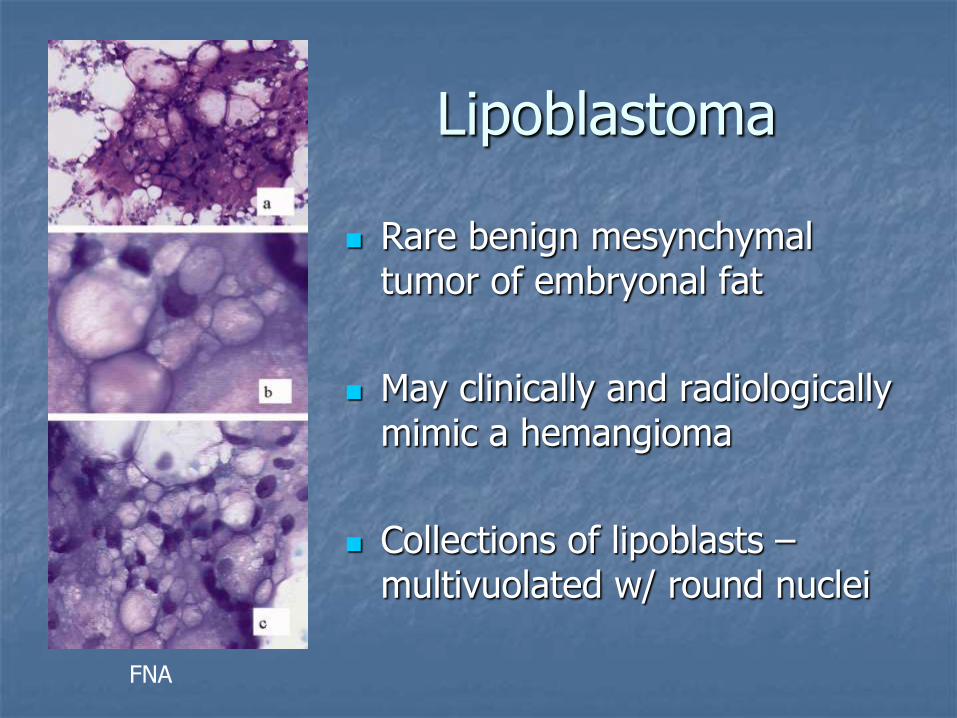
Lipoblastoma
Rare benign mesynchymal tumor of embryonal fat
May clinically and radiologically mimic a hemangioma
Collections of lipoblasts – multivuolated w/ round nuclei
FNA
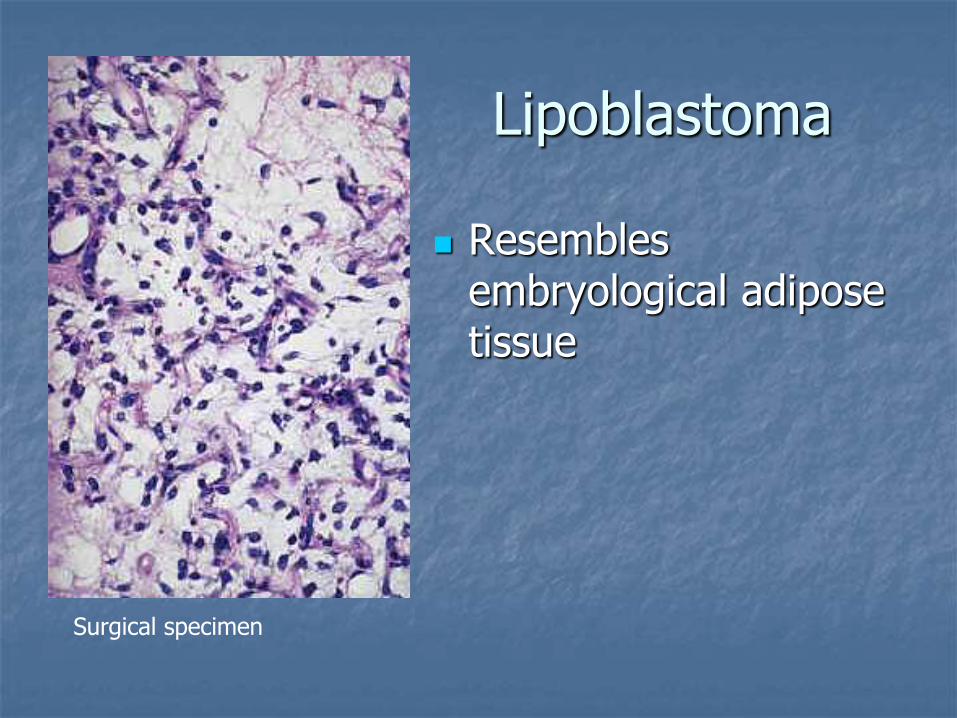
Lipoblastoma
Resembles embryological adipose tissue
Surgical specimen


Neonatal Goiter
CT shows large peripheral rim enhancing, low attenuation mass
1: 4000 live births
Female 2x = Male predominance
Delayed ossification at bone ends
Malik et al, 20026
Rovet et al, 200310

Pediatric Neck Masses
1. Congenital lesions
2. Inflammatory lesions
3. Non-inflammatory benign lesions
4. Benign neoplasms
5. Malignant neoplasms

Pediatric Neck Masses
1. Congenital lesions
2. Inflammatory lesions
3. Non-inflammatory benign lesions
4. Benign neoplasms
5. Malignant neoplasms

5. Malignant Neoplasms
Lymphoma 34 8% Hodgkin's 23 5% Non-Hodkin's 11 2% Thyroid Carcinoma 6 1% Rhabdomyosarcoma 2 Neuroblastoma 2 Fibrous histiocytoma 1 Acinic cell carcinoma 1 Histiocytosis X 1 Chloroma 1

Lymphoma
Third most common pediatric cancer
Incidence: 11-20 per million children
Geographical variance – 50 % of childhood cancers in equatorial Africa
Due to high incidence of Burkitt’s lymphoma
Male predominance 2.5:1

Beware the supraclavicular mass!
35% of patients with H&N lymphoma present with a supraclavicular mass
35% of pts with suprclavicular masses had lymphoma
Turkington et al 200522 Torsiglieri et al., 19882

Neuroblastoma
Noncontrast T1 MRI
Mass (arrow) lateral to carotid artery (arrowhead).
Gujar and Mukherji 20045

Rhabdomyosarcoma - CT
Ill defined
enhancing soft tissue density
areas of necrosis
Malik et al, 20026
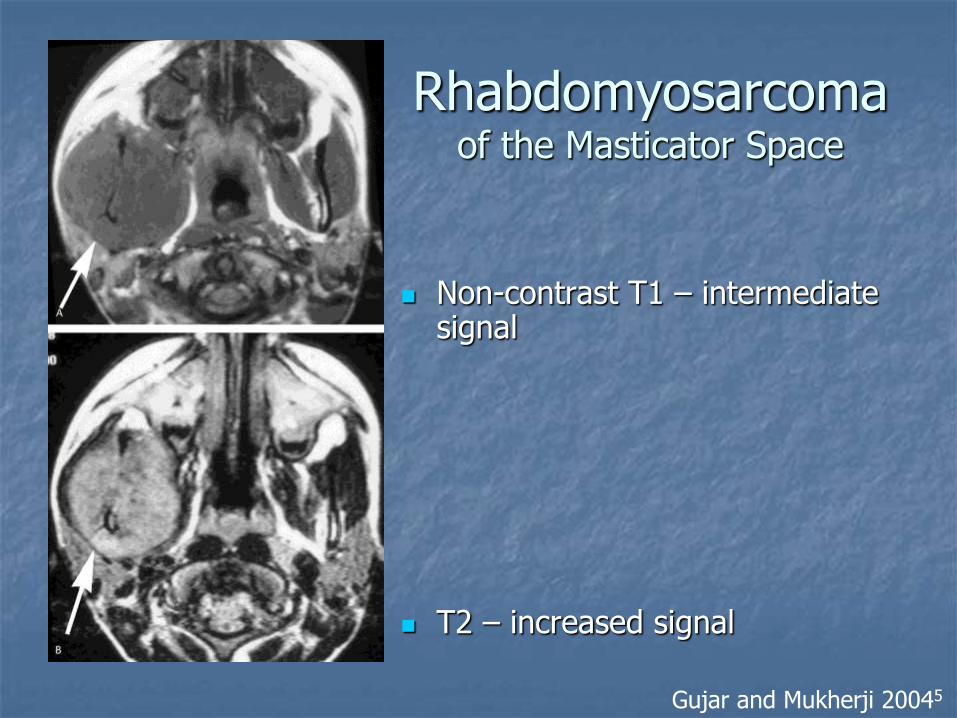
Rhabdomyosarcoma of the Masticator Space
Non-contrast T1 – intermediate signal
T2 – increased signal
Gujar and Mukherji 20045

Torsiglieri et al., 19882
Inflammatory
lesions
27%
Malignant
neoplasms, 11%
Benign neoplasms
3%
Non-infammatory
benign lesions
5%
Congenital lesions
54%
N= 445

Total % of total
Congeital lesions 244 55% Branchial cleft cyst 78 18% Thyroglossal duct cyst 73 16% Dermoid cyst 43 10% Lymphangioma 34 8% Hemangioma 10 2% Teratoma 2 Bronchogenic cyst 2 Thymic cyst 1 Myelomeningocele 1 Inflammatory lesions 118 27% Reactive lympadenopathy 71 16% Undetermined etiology 66 15% Sinus histiocytosis 5 1% Granulomatous disease 32 7% Atypical mycobacteria 20 4% Cat scratch disease 6 1% Toxoplasmosis 2 Sarcoid 2 Suppurative lympadenitis 10 2% Sialadenitis 5 1%
Non-infammatory benign lesions
23 5%
Inclusion cyst 13 3% Fibromatosis 9 2% Keliod 1 Benign neoplasms 12 3% Neurofibroma 3 1% Lipoma 3 1% Lipoblastoma 2 Paraganglioma 1 Goiter 1 Benign mixed tumor 1 Osteoblastoma 1 Malignant neoplasms 48 11% Lymphoma 34 8% Hodgkin's 23 5% Non-Hodkin's 11 2% Thyroid Carcinoma 6 1% Rhabdomyosarcoma 2 Neuroblastoma 2 Fibrous histiocytoma 1 Acinic cell carcinoma 1 Histiocytosis X 1 Chloroma 1 Total 445
Torsiglieri et al., 19882

Conclusions
Initial evaluation (H&P) Congenital, infectious, benign, malignant
Beware of tuberculosis, cat scratch disease, atypical infections
Beware of systemic symptoms
Beware the supraclavicular mass
Consider FNA or biopsy in the mass that does not resolve with treatment.
Bibliography
1. NeoReviews.org, http://neoreviews.aappublications.org/case27/case.shtml, 10/18/07.
2. Torsiglieri AJ Jr, Tom LW, Ross AJ 3rd, Wetmore RF, Handler SD, Potsic WP. Pediatric neck masses: guidelines for evaluation. Int J Pediatr Otorhinolaryngol. 1988 Dec;16(3):199-210.
3. Nicollas R, Guelfucci B, Roman S, Triglia JM. Congenital cysts and fistulas of the neck. Int J Pediatr Otorhinolaryngol. 2000 Sep 29;55(2):117-24.
4. Schroeder JW Jr, Mohyuddin N, Maddalozzo J. Branchial anomalies in the pediatric population. Otolaryngol Head Neck Surg. 2007 Aug;137(2):289-95.
5. Gujar S, Gandhi D, Mukherji SK. Pediatric head and neck masses. Top Magn Reson Imaging. 2004 Apr;15(2):95-101.
6. Malik A, Odita J, Rodriguez J, Hardjasudarma M. Pediatric neck masses: a pictorial review for practicing radiologists. Curr Probl Diagn Radiol. 2002 Jul-Aug;31(4):146-57.

Bibliography (cont)
7. ROH, JL.Lymphomas of the head and neck in the pediatric population, International journal of pediatric otorhinolaryngology, Volume 71, Issue 9, September 2007, Pages 1471-1477.
8. Moir CR. Neck Cysts, Sinuses, Thyroglossal Duct Cyts, and Branchial Cleft Anomalies, Operative Tech in Gen Surg, v 6, n 4 (Dec), 2004: 281-295.
9. Branstetter BF, Branchial Cleft Cysts, Emedicine, http://www.emedicine.com/radio/topic107.htm Oct 24, 2006.
10. Rovet JF. Congenital hypothyroidism: an analysis of persisting deficits and associated factors. Child Neuropsychol. 2002 Sep;8(3):150-62.
11. Thyroglossal Duct Cyst, Learning Radiology.com, http://www.learningradiology.com/archives06/COW%20231-Thyroglossal%20Duct%20Cyst/tgdccorrect.html, accessed 10/30/2007.

Bibliography (cont)
12. Pryor SG, Lewis JE, Weaver AL, Orvidas LJ. Pediatric dermoid cysts of the head and neck. Otolaryngol Head Neck Surg. 2005 Jun;132(6):938-42.
13. Wakhlu A, Wakhlu AK. Head and neck teratomas in children. Pediatr Surg Int. 2000;16(5-6):333-7. 14. Burezq: J Craniofac Surg, Management of Cystic Hygromas: 30 Year Experience Volume 17(4).July 2006.815-
818. 15. Head and Neck Surgery—Otolaryngology, Bailey,Calhoun, 2006, p.1213-1215 16. Gross E, Sichel JY. Congenital neck lesions. Surg Clin North Am. 2006 Apr;86(2):383-92, ix. 17. Mo JQ, Dimashkieh HH, Bove KE, GLUT1 endothelial reactivity distinguishes hepatic infantile hemangioma
from congenital hepatic vascular malformation with associated capillary proliferation. Hum Pathol. 2004 Feb;35(2):200-9.
18. MacArthur CJ , Head and neck hemangiomas of infancy. Current opinion in otolaryngology & head and neck surgery, 12/2006, Vol: 14, Issue: 6 Page: 397.
19. Becker KA, Thomas I. Epidermal Inclusion Cyst. Emedicine.com 5/10/2006. www.emedicine.com/derm/topic860.htm
20. Roy S, Fibromatosis Colli, Histopathology India.net www.histopathology-india.net/FC.htm 21. Rapkiewicz A, Le BT, Simsir A, Cangiarella J, Levine P. Spectrum of head and neck lesions diagnosed by fine-
needle aspiration cytology in the pediatric population. Cancer Cytopathology. Vol 111, Issue 4, Pages 242-251, 6 Jun 2007.
22. J R A Turkington, A Paterson, L E Sweeney, G D Thornbury. Neck Masses in Childres. BR J of Radiology, 78 (2005), 75-85.