pediatric head trauma joshua rocker, md pediatric emergency medicine schneider children’s hospital
TRANSCRIPT

Pediatric Head TraumaPediatric Head Trauma
Joshua Rocker, MD
Pediatric Emergency Medicine
Schneider Children’s Hospital

Parents present a 10 month old male to ER stating he fell down while walking and he is currently not himself.
Epidemiology of Pediatric Epidemiology of Pediatric Head InjuryHead Injury

Head Injuries: The numbers!Head Injuries: The numbers!Trauma- #1 cause of mortality and
morbidity >1y/o.
Head injury is the #1 cause of death in these traumas

Head injuries: The numbers!!Head injuries: The numbers!!600,000 ER visits
100,000 hospitalizations
7,000 deaths
29,000 permanent disability

Head Injuries: the mechanism!Head Injuries: the mechanism!Falls- 37%MVA- 18% (most fatal)Pedestrian Struck- 17%Bicycle injuries- 10%

Head Injuries: the differencesHead Injuries: the differencesAge:
Infants- fall or non-accidental
vs.
Adolescent- sports, MVAs
Sex:
males : females (2-4:1)

PathophysiologyPathophysiologyTwo phases
– Primary
– Secondary

Pathophysiology:Pathophysiology: The Box:
Blood, Brain, CSF

Pathophysiology:Pathophysiology:Cerebral Perfusion Pressure (CPP)=
Mean Arterial Pressure (MAP) –
Intracranial Pressure (ICP).

Pathophysiology- lastly…Pathophysiology- lastly…Axonal Injury-
– Primary pathological feature of traumatic head injury.
– Traumatic forces exert strain and/or torque on axons which may reversibly or irreversibly damage them.

Location, Location, LocationLocation, Location, Location(Anatomy, Anatomy, Anatomy)(Anatomy, Anatomy, Anatomy)

Case #1Case #1 Parents present with a 3 day old male who was a
product of a NSVD without any complications. His birth weight was 9lb 4oz. He now appears to be yellow tinged and has a swelling to the right side of the occiput.

Case #1Case #1Parents present with a 3 day old male who
was a product of a NSVD without any complications. His birth weight was 9lb 4oz. He now appears to be yellow tinged and has a swelling to the right side of the occiput.
Amita?? What’ya think?

ScalpScalp 5 Layers:
– Skin– Subcutaneous tissue– Galea aponeurosis– Loose areola tissue– pericranium

Skull- Skull fracturesSkull- Skull fractures Types:
– linear, diastatic, depressed
compound, basilarLinear – 75-90%
– Location key
Signs of Basilar Skull FractureSigns of Basilar Skull Fracture
Yes, this is a question to you Nikhil?

Basilar Skull FractureBasilar Skull Fracture Fx of petrous portion of
temporal bone:
hemotympanum, hemorrhagic or CSF
otorrhea, Battle sign
Fx of anterior skull base: CSF rhinorrhea, raccoon eyes

Intracranial InjuryIntracranial InjuryFunctional derangementsHemorrhagicEdemaPenetrating

Functional DerangementsFunctional DerangementsConcussion
Posttraumatic Seizures

HemorrhageHemorrhageCerebral ContusionEpiduralSubduralSubarachnoidIntracerebral Hematoma

Cerebral ContusionCerebral Contusion

Epidural HemorrhageEpidural HemorrhageLikely skull fractureLucid interval

Subdural HemorrhageSubdural HemorrhageDirect trauma or accel-decelBridging veinsOften with underlying brain
injurySeizures

Subdural HemorrhageSubdural Hemorrhage

Subdural HemorrhageSubdural Hemorrhage

Subarachnoid HemorrhageSubarachnoid Hemorrhage
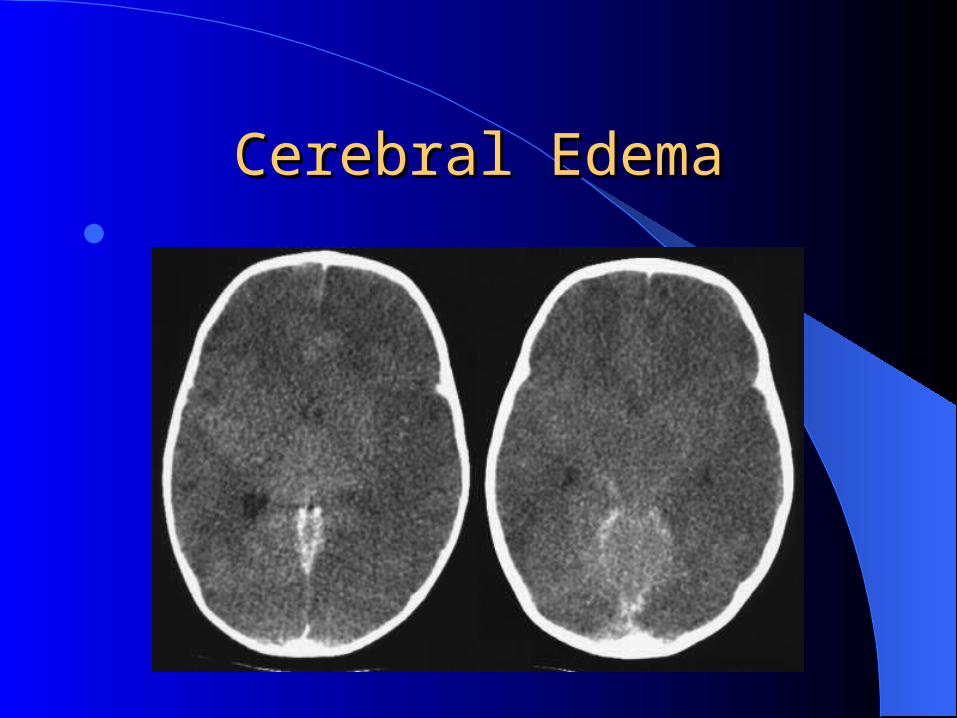
Cerebral EdemaCerebral Edema

Clinical ApproachClinical Approach History Symptoms Primary Survey
– ABCD (GCS)
Secondary Survey
Spinal Injury? Suspect Child Abuse?

Glasgow Coma ScaleGlasgow Coma Scale
Do you remember?

GCSGCS
Modified GCSModified GCS Eye Opening • Motor
– Spontaneous Normal – To speech W/D to touch– To pain W/D to pain– None Decorticate Decerebrate
Verbal None – Coos, Babbles– Cries to Pain– Moans to Pain– None

ManagementManagementFollowing lecture…to be continued…But….

Before we end…Before we end…

Non-accidental head injuries Non-accidental head injuries (aka- child abuse)(aka- child abuse)
In 2000 child abuse and neglect was responsible for 1200 deaths.
44% under 1 y/o.Head injury #1 cause of death.

Child abuse- numbersChild abuse- numbersVictims
– Median age 4.6 months– Range 7 d to 58 months
Perpetrators– 50% fathers, 20% male partner, 12% mothers

Child Abuse- Risk factorsChild Abuse- Risk factorsPerpetrators
– Young and/or single parent– Lower level of education– Unstable family structure– Stress in family– DV– Alcohol/drug abuse– depression
Victims– Multiple birth– Young age– Prematurity– Chronic illness– Difficult temperament

Child abuse- LOOK OUTChild abuse- LOOK OUT 60% with history or clinical evidence of previous abuse Retinal Hemorrhages
– Not pathognomonic (50-100% will have)– Seen in:
Birth trauma, accidental injuries, bleeding d/o, glutaric aciduria, infections, etc
Skeletal Fracture– 20-50%– Classic metaphyseal avulsion lesions (CML)– Posterior Rib
Cutaneous bruising– From autopsy- only 21%
JOSH, Please stop!!!!!!JOSH, Please stop!!!!!!
NO….

Last case!Last case! A 9 month old male with CF presents with
sleepiness after falling off the sofa (onto a hard wood floor) where the parents placed the child to sleep for the night. The family lives in a crowded one bedroom apartment with grandparents.
The father smells of alcohol.
Its 2 AM.

Case cont…Case cont…The child is sleeping.Vitals normal.Small hematoma over the temporal region.
What do you do?

CT results…CT results…
THE END!!!!!!!!THE END!!!!!!!!