pediatric bone lesions: beyond the plain radiographic evaluation
TRANSCRIPT
cfihccneipiatgHpuaoid
Pediatric Bone Lesions:Beyond the Plain Radiographic EvaluationGeetika Khanna, MD, MS,* and D. Lee Bennett, MD, MA†
Bone lesions in children are very common and includetrue bone tumors and tumor-like lesions. More than one-
half of all childhood bone neoplasms are benign.1 The mostommon benign bone lesions in children are nonossifyingbroma, osteochondroma, cortical desmoid, Langerhans cellistiocytosis, unicameral bone cyst, and aneurysmal boneyst. The most common malignant bone lesions are osteosar-oma, Ewing sarcoma, and metastatic disease, such as fromeuroblastoma. The radiograph remains the cornerstone forvaluation of the pediatric bone lesion. Radiographs providenformation on the location of the lesion within the bone, theresence and type of mineralized matrix, the nature of the
nterface between the tumor and the surrounding host bone,nd the reaction of the host bone to the presence of theumor.2 In conjunction with the age of the patient, the radio-raph is key to the differential diagnosis of a bone lesion.owever, cross-sectional imaging with computed tomogra-hy (CT) and magnetic resonance imaging (MRI) can provideseful additional information when the radiographic findingsre not diagnostic. The goal of this article is to review the rolef cross-sectional imaging modalities and imaging character-stics of common benign and malignant bone lesions in pe-iatric patients.
Imaging ModalitiesComputed TomographyAlthough radiographs are the mainstay for radiologic evalu-ation of bone tumors, one drawback of conventional radiog-raphy is its inability to detect early changes in bones withcomplex osseous anatomy. For example, 30%-50% bone de-struction of a vertebra has to be present to detect alterationsin bone architecture on plain radiographs of the spine.3,4 The
*Mallinckrodt Institute of Radiology, Washington University School of Med-icine, St Louis, MO.
†University of Iowa Roy J. and Lucille A. Carver College of Medicine, UIHC,Department of Radiology, Iowa City, IA.
Address reprint requests to Geetika Khanna, MD, MS, Mallinckrodt Instituteof Radiology, Washington University School of Medicine, 510 S. KingsHighway,CampusBox8131-MIR,St.Louis,MO63110.E-mail:khannag@
mir.wustl.edu90 0037-198X/12/$-see front matter © 2012 Elsevier Inc. All rights reserved.doi:10.1053/j.ro.2011.07.008
greater contrast and spatial resolution of CT makes it moresensitive in detection of bone lesions. CT can also be used tosupplement the information obtained from radiographswhere radiographic evaluation is limited because of superim-posing structures or complex anatomy (eg, axial skeleton).CT can provide exquisite detail regarding cortical destruc-tion, nondisplaced pathologic fractures, subtle osteoid/chon-droid matrix, and early periosteal reaction. CT has also beenshown to be better than MRI in detecting the nidus of anosteoid osteoma.5 Another major advantage of CT is the abil-ity to perform CT-guided biopsies and interventions, such asablation of osteoid osteoma.
Rapid advancements in multidetector CT technology allowfor the acquisition of isotropic datasets while virtually elimi-
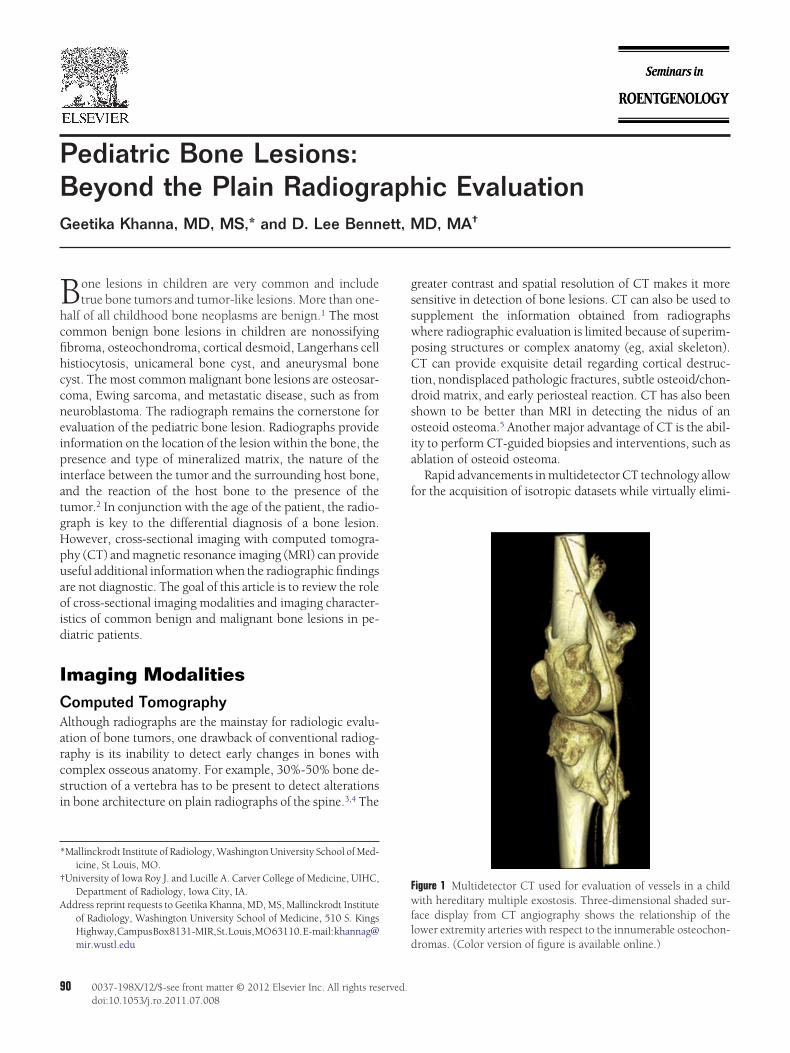
Figure 1 Multidetector CT used for evaluation of vessels in a childwith hereditary multiple exostosis. Three-dimensional shaded sur-face display from CT angiography shows the relationship of thelower extremity arteries with respect to the innumerable osteochon-
dromas. (Color version of figure is available online.)
ptnCma
tmHlMgso3r
ifying
Pediatric bone lesions 91
nating the need for sedation even in young children. Theisotropic datasets can be used to obtain multiplanar recon-structions in any plane. In addition, they can be used togenerate 3-dimensional (3D) reconstructions that can aid indiagnosis and treatment planning (Fig. 1).6 This allows the
atient to be imaged in any position, as dictated by the pa-ient’s comfort level, and also eliminates the need for rescan-ing in orthogonal projections. However, before performingT on a child, the benefit of any anticipated additional infor-ation from CT should be weighed against the risk of radi-
tion exposure to the child.
Magnetic Resonance ImagingMRI has evolved into the most accurate cross-sectional imag-ing modality for assessment of bone tumors.7 It can evaluate
Figure 2 Hypermetabolism in a nonossifying fibroma onold boy with Hodgkin’s disease shows a hypermetabolicmetastatic disease; (B) correlation with the low-dose CTwith sclerotic margins (arrow) consistent with a nonoss
Figure 3 Peritumoral edema associated with a chondrobpain shows an epiphyseal lytic lesion (arrow). The lesiosmooth periosteal reaction is present on the lateral aspeimage again shows the epiphyseal lesion with a hypointeMarked edema is present in the entire visualized tibia an
with chondroblastoma.he location of the lesion, its extent, involvement of bonearrow, and the presence of an associated soft tissue mass.owever, MRI is not specific because most bone lesions show
ow T1 and high T2 signal. To improve diagnostic accuracy,R images need to be interpreted in conjunction with radio-
raphs. In a prospective analysis of 87 consecutive musculo-keletal tumors, the tumors were correctly assessed only 55%f the time by MR alone, with malignancy overestimated in9% of the cases when MR images were interpreted withoutadiographic correlation.8
MR is the imaging modality of choice for local staging ofa suspected malignant bone tumor. The initial MRI shouldbe performed before biopsy to prevent distortion by post-biopsy changes. In addition, MRI can help determine theoptimal site and track for biopsy. The radiologist perform-
luorine-18 PET-CT performed for staging in a 15-year-arrow) in the distal right femur (A), which can simulatethe lesion to be a well-defined, intracortical lytic lesion
fibroma.
a. (A) Plain radiograph in a 17-year-old boy with kneeeographic with a sclerotic margin. A benign-appearinge proximal tibia (arrowhead). (B) Sagittal T2-weightedcorresponding to the sclerosis seen on the radiograph.
ounding soft tissues. Surgical pathology was consistent
PET. Ffocus (reveals
lastomn is g
ct of thnse rimd surr

pst
awtt
ca
FctFhwllt
92 G. Khanna and D.L. Bennett
ing the biopsy should plan the biopsy track in conjunctionwith the orthopedic surgeon. At diagnosis of a malignantbone lesion, longitudinal MRI of the entire bone is recom-mended with T1 and fat-saturated T2-weighted images toevaluate for the extent of the lesion and detect any skipmetastasis. For treatment purposes and pretreatment eval-uation, the intraosseous extent of a bone lesion (in partic-ular osteosarcoma) is most accurately measured and de-picted on the T1-weighted images.9 Axial pre- and
ostcontrast images aid in delineating the extent of theoft-tissue mass, the compartments involved, and the sta-us of the neurovascular bundle.
The lack of radiation exposure makes MR particularly suit-ble for evaluation of the pediatric skeleton. Considerationshen performing MRI in children include the need for seda-
ion in younger children and the increased difficulty in ob-aining quality images on smaller body parts.
Nuclear MedicineAlthough bone scintigraphy and positron emission tomogra-phy (PET) are excellent for evaluation of metastatic disease ora multifocal process, their lack of specificity limits their use inthe initial workup of a single bone lesion.10 Several benignbone lesions, such as fibrous dysplasia, nonossifying fi-broma, and giant cell tumors have been shown to be hyper-metabolic on PET (Fig. 2).11 Although bone scintigraphy re-mains an essential part of osteosarcoma staging, recentstudies have shown PET to have higher diagnostic accuracyfor staging of Ewing sarcoma.12
Cross-Sectional Imaging SignsImaging findings that are traditionally used to characterizebone lesions on radiography can be applied to cross sectionalmodalities as well. Additional imaging features may be rec-ognized on cross sectional imaging that can aid in the differ-ential diagnosis of bone lesions (eg, nidus detection), or bepotentially misleading (peritumoral edema).8,13 Some spe-ific imaging findings encountered with advanced imagingre discussed in the following sections.
Peritumoral EdemaPeritumoral edema can be present in both benign and malig-nant bone tumors. Peritumoral edema does not help in de-termining the aggressiveness of a lesion.14 In fact, some be-nign bone lesions in children can have extensive peritumoraledema in the bone marrow and surrounding soft tissuesmimicking an aggressive process.13 These lesions include os-teoid osteoma, stress fracture, chondroblastoma, and Lang-erhans cell histiocytosis (Fig. 3). Inflammatory changes tendto be marked in the pediatric bone because of the presence ofa loose periosteum which can be easily elevated. Tumor re-lated edema may be the only or most prominent feature ofosteoid osteoma, and in some cases can obscure the nidus onMRI.15
Peritumoral edema is most conspicuous on fat saturated
T2-weighted or short tau inversion recovery (STIR) images. nMarrow edema does not change the normal architecture ofthe marrow space and it tends to enhance uniformly. How-ever, tumors cause bone destruction, with distortion of nor-mal architecture, and tend to enhance heterogeneously. Be-cause a lesion and the surrounding edema can both enhanceon post contrast images, peritumoral edema can obscure thetrue margins of a lesion. T1-weighted images are less affectedby peritumoral edema, and have been shown to better delin-eate the margins of a lesion.16,17
Tumor MatrixThe internal appearance of a tumor depends on its cellularcomposition and its presence or absence of tumor matrix.Tumors can produce osteoid, chondroid, or fibrous ma-trix. On radiographs and CT images, osteoid matrix has ahomogeneously increased density with a “cloud-like” ap-pearance, whereas chondroid matrix is characterized bythe presence of stippled rings and arcs. Although the pres-ence and type of matrix usually can be evaluated withradiographs, CT (with its high spatial resolution) can alsoaid in improved matrix detection and characterization. CTcan also be used to determine the location of the tumormatrix, central versus peripheral, and to aid in differenti-ation of myositis ossificans from parosteal osteosarcoma.Mature osteoid matrix is located peripherally in myositisossificans; however, the mature osteoid tumor matrix ofparosteal osteosarcoma is seen centrally.18
Soft-Tissue MassCross-sectional imaging modalities are essential in detectingthe presence of and the extent of a soft tissue mass. Althoughperitumoral inflammatory changes can result in surroundingperiosteal reaction and inflammation in adjacent soft tissues,the presence of a large soft tissue mass in conjunction with alytic bone lesion is characteristic of Ewing sarcoma in thepediatric population (Fig. 4).
Fluid-Fluid LevelsT2-weighted MRI has been shown to be most sensitive indetection of fluid-fluid levels (FFLs).19 Although FFLshave been classically described with aneurysmal bonecysts (ABCs), they can be seen with other bone lesions aswell.20 Both benign and malignant bone lesions can have
FLs. Some examples include aneurysmal bone cyst, uni-ameral bone cyst, giant cell tumor, and telangiectatic os-eosarcoma. The percentage of a bone lesion occupied byFL has been shown to inversely correlate with the likeli-ood of malignancy (Figs 5 and 6).21 In a study of 83 casesith FFLs, O’Donnell and Saifuddin21 showed that if at
east two-thirds of the lesion contained FFLs 89% of theesions were benign, whereas if FFLs were present in lesshan a third of the lesion, 67% of the lesions were malig-
ant.
). The
Pediatric bone lesions 93
Cross-SectionalImaging of Specific LesionsBenign LesionsCystic LesionsUnicameral Bone Cyst. Unicameral (simple) bone cysts(UBCs) are common benign lesions in children typically oc-curring in the proximal metaphysis of tubular bones adjacentto a growth plate. They are generally discovered incidentallyor secondary to a pathologic fracture. On plain radiograph,
Figure 4 Soft-tissue mass associated with an Ewing sarcomwith a limp shows a poorly marginated lytic lesion (arrothe superior endplate of S1. The primary differential diocytosis. (B) Sagittal postcontrast T1-weighted image sha large soft-tissue mass extending into the spinal canal (*
Figure 5 Fluid-fluid levels in telangiectatic osteosarcomapatient with knee pain shows an aggressive appearing lyperiosteal reaction. The lesion is poorly marginated anmarrow replacing process with cortical destruction and
present in the mass. Surgical pathology was consistent with tethese lesions are usually central, elongated radiolucent le-sions with well-defined margins. A pathologic fracturethrough a UBC can result in a fallen fragment, a pathogno-monic sign of a UBC. Cross-sectional imaging is helpful if theradiographic findings are atypical, such as a multilocular ap-pearance, or when a UBC occurs in an atypical site. CT maybe helpful in identification of a pathologic fracture or a “fallenfragment.” CT can also be used to evaluate the extent of thelesion in anatomically complex areas, such as the pelvis.22 OnMR, the classical UBC appears as well-defined meta- or di-
Frog-leg radiograph of the pelvis in a 3-year-old patiente left side of the sacrum with a compression fracture of
s includes Ewing sarcoma versus Langerhans cell histi-arrow replacing process in the S1 vertebral body with
large soft-tissue mass is characteristic of Ewing sarcoma.
nteroposterior radiograph of the knee in a 15-year-oldn at the medial aspect of the metaphysis with sun-burste osteoid matrix. (B) Axial T2-weighted MRI shows aoft-tissue mass. Scattered fluid-fluid levels (arrows) are
a. (A)w) in thagnosiows a m
. (A) Atic lesiod somlarge s
langiectatic osteosarcoma.

wos
eeegmfimbApasbpiccsao
htiocamTcscceivbettds
94 G. Khanna and D.L. Bennett
aphyseal cystic lesion containing fluid signal intensity with athin rim of peripheral enhancement at the cyst wall on post-contrast images.23 However, UBCs can be multiloculated
ith heterogeneous intensity, fluid-fluid levels, and nodularr thick peripheral areas of enhancement especially in theetting of a healed or acute pathologic fracture.24
Aneurysmal Bone Cyst. Most ABCs seen in children are pri-mary lesions with a peak occurrence around 16 years of age.Secondary ABCs can also be seen in children, after trauma, orwith an underlying lesion, such as osteoblastoma, chondro-blastoma, or simple bone cyst.25 ABCs typically arise in anccentric metaphyseal location in long bones or the posteriorlements of the spine. As indicated by the name, an ABC is anxpansile, lytic lesion. ABCs usually have well-defined mar-ins; however, approximately 15% will have poorly definedargins. ABCs have no internal matrix and consist of bloodlled cavernous spaces. The expansile nature of the lesionay result in marked cortical thinning, so the cortex may
ecome imperceptible on plain radiographs or MRI. If theBC is rapidly expanding, it can have an aggressive appearingeriosteal reaction mimicking a malignancy. On MRI, ABCsre low in signal intensity on T1-weighted images and high inignal intensity on T2-weighted images with low signal fi-rous tissue lining the spaces. ABCs are characterized by theresence of FFLs, which are most prominent on T2-weighted
mages (Fig. 6). On postcontrast images, enhancement of theyst wall and internal septations can be seen. Although solidomponents may be present within ABCs, the presence ofolid tissue should alert the radiologist to consider a second-ry ABC, or an alternative diagnosis, such as telangiectatic
Figure 6 Fluid-fluid levels in an aneurysmal bone cyst. AAnteroposterior view of lumbar spine shows an expansiinternal matrix was identified. (B) Axial T2-weighted MRthe right transverse process, pedicle, and right side ofaneurysmal bone cyst.
steosarcoma.22 t
Cartilaginous LesionsOsteochondroma. This is a relatively common benign lesionthat arises when growth plate cartilage becomes displaced tothe metaphyseal region. Osteochondroma is an extension ofthe normal bone and shows continuity with the periosteum,cortex, and marrow of the underlying bone. The most com-mon site is around the knee joint followed by the proximalhumerus. Most osteochondromas can be diagnosed radio-graphically, by their characteristic cortical and medullarycontinuity with the native bone.26 Cross-sectional imaging is
elpful when the radiographic appearance is not characteris-ic, when the anatomy needs to be better delineated, such asn the axial skeleton, when preoperative planning is required,r when one needs to evaluate for radiographically occultomplications (Fig. 1). The 3D imaging ability of CT and MRIllows optimal depiction of the pathognomonic cortical andedullary continuity of the lesion with the parent bone.his is particularly true for lesions located in areas ofomplex anatomy, such as the axial skeleton, and for le-ions with a broad stalk. Osteochondromas can cause localomplications because of mass effect, such as bursitis,ompression of the neurovascular bundle, and pseudoan-urysm formation. Sonography is a relatively inexpensivemaging modality to evaluate for complications, such asascular compromise, pseudoaneurysm formation, orursa formation. Cross-sectional imaging is helpful tovaluate for complications like fracture or malignantransformation. MRI is the best imaging modality to assesshe thickness of the hyaline cartilage cap of an osteochon-roma. Although a thickness of more than 1.5 cm has beenuggested as an indicator of malignant transformation in
ar-old girl presented with scoliosis and back pain. (A)lesion in the right transverse process of L4 (arrow). Nos multiple FFLs throughout the lesion, which involves
ertebral body. Surgical pathology was consistent with
14-yele lyticI showthe v
he skeletally mature individual, increased thickness of the

ttitdeeirdvMtu
ttietwt
rcn
Pediatric bone lesions 95
cartilage cap is a recognized feature in the growing childand should not be viewed as a finding of malignant trans-formation in skeletally immature patients.
Enchondroma. Enchondromas are a relatively commonbenign tumor of bone in children characterized by forma-tion of hyaline cartilage.3 They are most commonly seen inhe second decade of life, and are most commonly found inhe small tubular bones of the hands and feet. These typ-cally appear as central, well-defined, expansile masseshat cause endosteal scalloping. The presence of chon-roid matrix is a characteristic finding, although it is pres-nt in only approximately 50% of enchondromas. On MRI,nchondromas appear as T1-hypointense and T2-hyper-ntense lobulated lesions with small foci of low signal cor-esponding to the stippled calcifications within the chon-roid matrix. Enchondromas can occur in association withenous malformations (Maffucci syndrome). Althoughaffucci syndrome carries a risk of malignant transforma-
ion of enchondroma into chondrosarcoma, this is un-sual in the pediatric age range.27
Chondroblastoma. Chondroblastoma is a rare benign tumorof immature cartilage, with a peak incidence between 10 and20 years of age. Nearly one-half of these tumors are diag-nosed in skeletally immature patients. Chondroblastomashave a predilection for the epiphyses of long bones andepiphyseal-like regions, with the bones around the knee joint
Figure 7 Osteoid osteoma nidus detection on CT. A 13-year-old boywith right hip pain. (A) Axial T2-weighted MRI shows a large righthip joint effusion with femoral neck edema. There is suggestion of aT2 hyperintense lesion along the posterior cortex with a centralhypointensity (arrow). (B) Axial CT image clearly shows the lyticnidus (arrow) with central mineralization at the posterior cortex ofthe right femoral neck.
being most commonly affected. Chondroblastomas can often
cross the growth plate to involve the adjacent metaphysis.28
On radiography, the lesion appears as an eccentric, lytic le-sion with a geographic border. Stippled calcifications withinthe lesion may be visible, reflecting chondroid matrix. OnMRI, the lesion appears as a lobulated low T1 signal andheterogeneous T2 signal lesion. Calcifications within thechondroid matrix will appear low signal on both T1 and T2images, whereas the noncalcified cartilage appears T2 hyper-intense (Fig. 3). Chondroblastomas can have a characteristicperipheral thin hypointense rim on MRI that corresponds tothe radiographic marginal sclerosis around the lytic lesion.29
MRI will typically show extensive edema in the surroundingbone and soft tissues, and marked reactive synovitis can alsobe present.
Osseous LesionsOsteoid Osteoma and Osteoblastoma. Osteoid osteoma(OO) is characterized by a radiographic appearance of anintracortical nidus with a variable amount of mineralization,by cortical thickening, and by reactive sclerosis. Cross-sec-tional imaging is useful if the radiographic findings are atyp-ical, the OO is located in a region of complex anatomy (eg,the posterior elements of the spine), and for image-guidedintervention.30 The differential diagnosis of an osteoid os-eoma includes other intracortical lesions, such as stress frac-ure and intracortical abscess. On the basis of cross-sectionalmaging, OO can be classified as subperiosteal, intracortical,ndosteal, and intramedullary. Thin-section CT images ob-ained with a bone algorithm and viewed in bone windowsith multiplanar reconstructions are useful for identifying
he nidus.The authors of some studies have shown that CT is supe-
ior to MRI in depicting the nidus of OO.5 On CT, OO isharacterized by a well-defined round or oval radiolucentidus. A variable amount of mineralization may be seen
Figure 8 Healing nonossifying fibroma on MRI. Sagittal T2-weightedMRI with fat saturation shows a cortically based well-defined lesion(arrow) that is hypointense to muscle. The surrounding marrowsignal is normal. This finding is consistent with a healing nonossi-
fying fibroma, which is a common incidental finding.
thombtc
FFbnlralstldmeMoIiTs
96 G. Khanna and D.L. Bennett
within the nidus. The nidus is surrounded by reactive scle-rosis, periosteal reaction, and new bone formation. On MRI,the nidus has low to intermediate signal intensity on T1-weighted images and variable signal intensity on T2-weighted images depending on the amount of mineraliza-tion. Extensive surrounding edema in the adjacent bonemarrow and soft tissues is often seen with OO, and the sig-nificant surrounding reaction can make it difficult to identifythe nidus on MRI. Intra-articular osteoid osteomas, mostcommonly seen in the hip joint, show minimal reactive cor-tical thickening but can cause synovitis that may be confusedfor an infectious or inflammatory arthropathy (Fig. 7).
Osteoblastoma differs from osteoid osteoma in having anidus larger than 1.5 cm in diameter and usually showingmore variable histologic findings.3 The most common loca-ion of osteoblastoma is in the posterior elements of the spine;ence, cross-sectional imaging is invaluable in the evaluationf these lesions. CT demonstrates a lytic lesion with osteoidatrix and periosteal reaction. MR signal characteristics can
e variable depending on the amount of mineralization,hough surrounding marrow and soft tissue edema are typi-
Figure 9 Cortical desmoid on MRI. A 4-year-old boy was r(A,B) Axial T1- and T2-weighted MR images of the knegastrocnemius. This is a characteristic location and appa different child shows a subtle lucency with a sclerotmetaphysis—cortical desmoid.
ally present.
ibro-Osseous Lesionsibrous Cortical Defect and Nonossifying Fibroma. Fi-rous cortical defect (also called benign cortical defect) andonossifying fibromas (NOFs) are the commonest benign
esions of the pediatric skeleton, often seen incidentally onadiographs. They have a characteristic radiographic appear-nce with an eccentric, cortically based, well-defined lyticesion with marginal sclerosis. As the lesions heal, increasingclerosis is seen. They are most commonly seen in the me-aphysis or metadiaphysis of the long bones. Although the 2esions are identical histologically, the term fibrous corticalefect is preferred for lesions �2 cm in size. Given the com-on occurrence of NOFs in children, it is not unusual to
ncounter them as incidental findings on MRI (Fig. 8). TheRI appearance of NOFs varies with the developmental stage
f the lesion and correlates with the radiographic appearance.n the developmental stage, NOFs are bright on T2-weightedmages. As the lesions mature, they become low in signal on2 images because of hypercellular fibrous tissue and hemo-iderin deposits.31 On MRI, the lesions are typically hypoin-
tense on T1-weighted images. T2 signal varies based on the
for MRI of femoral lesion seen at an outside institution.cortical irregularity (arrow) at the origin of the medial
e of a cortical desmoid. (C) Plain radiograph of knee ingin (arrow) at the medial aspect of the distal femoral
eferrede showearancic mar
degree of hypercellular fibrous tissue, with lesions being

tvtttlhamcLmMdw
Pediatric bone lesions 97
bright during development and decreasing in signal as theyheal. The eccentric location of the lesion abutting the cortexaids in the diagnosis of NOF. Multiple NOFs can be seen inchildren with neurofibromatosis type I. Large NOFs can becomplicated by pathologic fractures.
Cortical Desmoid. Cortical desmoids are benign self-limit-ing fibrous or fibro-osseous lesions that most frequently oc-cur in the medial supracondylar femur.32 They are most com-mon in boys in the second decade of life, although they canbe seen in younger children as well. They are believed to betug lesions secondary to traction injury at the origin of themedial head of the gastrocnemius. They likely occur becauseof chronic/repetitive injury and have a characteristic appear-ance of a well-marginated lucency with a sclerotic margin.Given their typical location and radiographic findings, theselesions should require no additional imaging or intervention.Cortical desmoids can be seen as incidental findings on crosssectional imaging, best appreciated on the axial T2-weightedMRI as an area of cortical irregularity with minimal associatedfluid signal (Fig. 9).
Fibrous Dysplasia. Fibrous dysplasia is a nonhereditary de-velopmental abnormality of bone that is usually monostotic;however, it is polyostotic in approximately 20% of cases.3
Fibrous dysplasia can develop in any bone. Radiographically,it is a well-defined, expansile, ground glass lesion that oftenhas a sclerotic rim (Fig. 10). On MRI, it is a well-definedintramedullary lesion that is T1 hypointense and T2 hyper-intense. Internal calcifications, septations, fatty areas andcysts can result in some heterogeneity of its signal character-istics on MRI. A rim of low signal can be seen correspondingto the sclerotic rim visible on radiography. The main compli-cations of fibrous dysplasia are osseous deformity and patho-logic fracture. Polyostotic fibrous dysplasia can be accompa-nied by precocious puberty and café-au-lait spots (McCuneAlbright syndrome).33
Figure 10 Fibrous dysplasia on CT. Coronal maxillofacial CT imageshows characteristic ground glass expansile lesion of the left maxilla
consistent with fibrous dysplasia.OthersLangerhans Cell Histiocytosis. Langerhans cell histiocyto-sis (LCH) is a benign round cell tumor that may present assolitary or multiple bone lesions.34 The skull, femur, ver-ebrae, pelvis, and ribs are the most common sites of in-olvement. In the tubular bones, lesions are typically me-aphyseal or diaphyseal in location. Radiographically,hese lesions typically appear as lytic lesions without ma-rix. The zone of transition can be narrow or wide, and theesions can have a more permeative appearance. MRI iselpful in determining the extent of marrow involvementnd in assessing the surrounding soft tissues as the pri-ary differential diagnosis is osteomyelitis or Ewing sar-
oma. The absence of an associated soft-tissue mass favorsCH over Ewing sarcoma. Although skeletal surveys re-ain the most widely used imaging modality, whole-bodyRI using STIR sequences has been shown to be useful for
etection and follow up multifocal skeletal involvementith LCH.35
Malignant TumorsOsteosarcomaOsteosarcoma (OS) is the most common primary malignantbone tumor in children.36 The tumor generally occurs in thesecond decade of life and typically presents as a painful mass.Pediatric OS is usually metaphyseal and medullary in origin.The most common site is in the long bones of the lowerextremity (especially around the knee joint), followed by the
Figure 11 Neuroblastoma with metastatic disease to bone. A2-year-old girl presented with limp. (A) Anteroposterior view ofthe left hip shows a moth-eaten appearance to the left femoralneck with interrupted periosteal reaction (arrow). A band ofsclerosis (arrowhead) is present in the midfemoral neck. (B)Coronal T1-weighted MRI shows loss of normal marrow signal inthe proximal epiphyseal ossification center (white arrow) and theproximal metadiaphysis. Metastatic deposits are present in thedistal femur (black arrow) as well. A hypointense line in thefemoral neck (arrowhead) represents a pathologic fracture. Pa-tient was found to have a left adrenal neuroblastoma.
humerus. Plain radiographic findings include a lytic, blastic,

cipe
EEsdooeoEm
swepmptdMed
98 G. Khanna and D.L. Bennett
or mixed aggressive bone lesion with indistinct margins, cor-tical destruction, aggressive periosteal reaction, and a softtissue mass. The tumor is characterized by production ofosteoid matrix. MRI is crucial for local staging of the malig-nancy to determine the extent of marrow involvement, trans-physeal extension, intra-articular extension, and the extent ofsoft-tissue disease. Longitudinal imaging of the entire boneshould be performed as skip metastasis can be present inapproximately 15% of cases.37 Axial T2-weighted and post-ontrast MRI help determine the soft-tissue compartmentsnvolved and the status of the neurovascular bundle. Theresence of fluid-fluid levels suggests the telangiectatic vari-ty of osteosarcoma.
wing’s Sarcomawing’s sarcoma, a primitive neuroectodermal tumor, is theecond most common primary malignant bone tumor in chil-ren. It is more common in whites than blacks with a peakccurrence in the second decade of life. Ewing’s sarcomaccurs in the axial and appendicular skeleton with aboutqual frequency, whereas the vast majority of osteosarcomasccur in the appendicular skeleton.38 Within the long bones,wing sarcoma commonly occurs within the diaphysis oretadiaphysis.36 On radiographic evaluation, it has a vari-
able but usually aggressive appearance. Imaging findingsinclude a permeative, mixed lytic/sclerotic appearancewith cortical destruction and aggressive periosteal reac-tion (spiculated or onion peel). Ewing’s sarcoma does notusually produce a mineralized osteoid matrix as seen withosteosarcoma. As in osteosarcoma, MRI is crucial for localstaging and evaluation of skip lesions. Ewing sarcoma ishypo or isointense to muscle on fluid sensitive sequencesbecause of dense cellularity. A lytic bone lesion in a childin association with a large soft-tissue mass should raiseconcern for Ewing sarcoma (Fig. 4).
Metastatic DiseaseThe 2 most common primary pediatric malignancies to pres-ent with metastatic bone lesions are neuroblastoma and leu-kemia. Neuroblastoma is the most common extracranial solidneoplasm of childhood. The most common site of metastasisin neuroblastoma is the bone marrow, occurring in 50%-60% of cases at presentation.39 On plain radiographs, meta-tatic disease appears as a poorly marginated lytic lesion,hich may have a moth-eaten appearance. In the axial skel-
ton, metastatic disease can result in a sunburst pattern oferiosteal reaction. MRI helps to determine the true extent ofarrow involvement. Neuroblastoma metastases are T1 hy-ointense, T2 hyperintense lesions that enhance on post con-rast images (Fig. 11). They may be associated with corticalestruction, periosteal reaction, and extraosseous extension.etastasis can occur in both the axial and appendicular skel-
ton, with the metaphysis being the most common site ofisease in the appendicular skeleton.
ConclusionsPlain radiography is the most important initial imaging mo-
dality in the evaluation of pediatric bone lesions. The plainradiograph provides valuable information regarding how thebone lesion affects the parent bone and the response of theparent bone to the lesion. This helps differentiate aggressivefrom nonaggressive bone lesions. Cross-sectional imagingwith MRI or CT can provide useful additional information ifthe diagnosis is uncertain on radiography. MRI and CT canalso provide helpful information for local staging, assessinglocal complications, preoperative planning, and performingimage-guided interventions. However, cross-sectional imag-ing studies should always be interpreted in conjunction withradiographs in evaluation of pediatric bone lesions.
References1. Slovis T: Caffey’s Pediatric Diagnostic Imaging (ed 11). Philadelphia,
Mosby/Elsevier, 2008, pp 2912-29692. Bennett DL, El-khoury GY: General Approach to lytic bone lesions.
Appl Radiol 33:8-17, 20043. Vlychou M, Athanasou NA: Radiological and pathological diagnosis of
paediatric bone tumours and tumour-like lesions. Pathology 40:196-216, 2008
4. Boland PJ, Lane JM, Sundaresan N: Metastatic disease of the spine. ClinOrthop Relat Res 169:95-102, 1982
5. Assoun J, Richardi G, Railhac JJ, et al: Osteoid osteoma: MR imagingversus CT. Radiology 191:217-223, 1994
6. Fayad LM, Johnson P, Fishman EK: Multidetector CT of musculoskel-etal disease in the pediatric patient: Principles, techniques, and clinicalapplications. RadioGraphics 25:603-618, 2005
7. Sundaram M, McLeod RA: MR imaging of tumor and tumorlikelesions of bone and soft tissue. AJR Am J Roentgenol 155:817-824,1990
8. Ma LD, Frassica FJ, Scott WW Jr, et al: Differentiation of benign andmalignant musculoskeletal tumors: Potential pitfalls with MR imaging.RadioGraphics 15:349-366, 1995
9. Hoffer FA, Nikanorov AY, Reddick WE, et al: Accuracy of MR imagingfor detecting epiphyseal extension of osteosarcoma. Pediatr Radiol 30:289-298, 2000
10. Aoki J, Watanabe H, Shinozaki T, et al: FDG PET of primary benign andmalignant bone tumors: Standardized uptake value in 52 lesions. Ra-diology 219:774-777, 2001
11. Goodin GS, Shulkin BL, Kaufman RA, et al: PET/CT characterization offibroosseous defects in children: 18F-FDG uptake can mimic meta-static disease. AJR Am J Roentgenol 187:1124-1128, 2006
12. Franzius C, Sciuk J, Brinkschmidt C, et al: Evaluation of chemotherapyresponse in primary bone tumors with F-18 FDG positron emissiontomography compared with histologically assessed tumor necrosis.Clin Nucl Med 25:874-881, 2000
13. Hayes CW, Conway WF, Sundaram M: Misleading aggressive MR im-aging appearance of some benign musculoskeletal lesions. Radio-Graphics 12:1119-1134, 1992; discussion: 35-36
14. Kroon HM, Bloem JL, Holscher HC, et al: MR imaging of edema accom-panying benign and malignant bone tumors. Skeletal Radiol 23:261-269, 1994
15. Ehara S, Rosenthal DI, Aoki J, et al: Peritumoral edema in osteoidosteoma on magnetic resonance imaging. Skeletal Radiol 28:265-270,1999
16. Gillespy T, 3rd, Manfrini M, Ruggieri P, et al: Staging of intraosseousextent of osteosarcoma: Correlation of preoperative CT and MRimaging with pathologic macroslides. Radiology 167:765-767,1988
17. Onikul E, Fletcher BD, Parham DM, et al: Accuracy of MR imaging forestimating intraosseous extent of osteosarcoma. AJR Am J Roentgenol167:1211-1215, 1996
18. Zeanah WR, Hudson TM: Myositis ossificans: Radiologic evaluation oftwo cases with diagnostic computed tomograms. Clin Orthop Relat Res168:187-191, 1982
19. Van Dyck P, Vanhoenacker FM, Vogel J, et al: Prevalence, extension

2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
Pediatric bone lesions 99
and characteristics of fluid-fluid levels in bone and soft tissue tumors.Eur Radiol 16:2644-2651, 2006
0. Alyas F, James SL, Davies AM, et al: The role of MR imaging in thediagnostic characterisation of appendicular bone tumours and tumour-like conditions. Eur Radiol 17:2675-2686, 2007
1. O’Donnell P, Saifuddin A: The prevalence and diagnostic significanceof fluid-fluid levels in focal lesions of bone. Skeletal Radiol 33:330-336,2004
2. Woertler K: Benign bone tumors and tumor-like lesions: Value of cross-sectional imaging. Eur Radiol 13:1820-1835, 2003
3. Sullivan RJ, Meyer JS, Dormans JP, et al: Diagnosing aneurysmal andunicameral bone cysts with magnetic resonance imaging. Clin OrthopRelat Res 366:186-190, 1999
4. Margau R, Babyn P, Cole W, et al: MR imaging of simple bone cysts inchildren: Not so simple. Pediatr Radiol 30:551-557, 2000
5. Kransdorf MJ, Sweet DE: Aneurysmal bone cyst: Concept, contro-versy, clinical presentation, and imaging. AJR Am J Roentgenol 164:573-580, 1995
6. Murphey MD, Choi JJ, Kransdorf MJ, et al: Imaging of osteochon-droma: Variants and complications with radiologic-pathologic correla-tion. RadioGraphics 20:1407-1434, 2000
7. Murphey MD, Flemming DJ, Boyea SR, et al: Enchondroma versuschondrosarcoma in the appendicular skeleton: Differentiating features.RadioGraphics 18:1213-1237, 1998; quiz: 44-45
8. Kurt AM, Unni KK, Sim FH, et al: Chondroblastoma of bone. Hum
Pathol 20:965-976, 19899. Oxtoby JW, Davies AM: MRI characteristics of chondroblastoma. ClinRadiol 51:22-26, 1996
0. Chai JW, Hong SH, Choi JY, et al: Radiologic diagnosis of osteoidosteoma: From simple to challenging findings. RadioGraphics 30:737-749, 2010
1. Jee WH, Choe BY; Kang HS, et al: Nonossifying fibroma: Characteristics atMR imaging with pathologic correlation. Radiology 209:197-202, 1998
2. Resnick D, Greenway G: Distal femoral cortical defects, irregularities,and excavations. Radiology 143:345-354, 1982
3. Dumitrescu CE, Collins MT: McCune–Albright syndrome. Orphanet JRare Dis 3:12, 2008
4. Meyer JS, Harty MP, Mahboubi S, et al: Langerhans cell histiocytosis:Presentation and evolution of radiologic findings with clinical correla-tion. RadioGraphics 15:1135-1146, 1995
5. Mentzel HJ, Kentouche K, Sauner D, et al: Comparison of whole-bodySTIR-MRI and 99mTc-methylene-diphosphonate scintigraphy in chil-dren with suspected multifocal bone lesions. Eur Radiol 14:2297-2302, 2004
6. Hoffer FA: Primary skeletal neoplasms: Osteosarcoma and Ewing sar-coma. Top Magn Reson Imaging 13:231-239, 2002
7. Sajadi KR, Heck RK, Neel MD, et al: The incidence and prognosis ofosteosarcoma skip metastases. Clin Orthop Relat Res 426:92-96, 2004
8. Arndt CA, Crist WM: Common musculoskeletal tumors of childhoodand adolescence. N Engl J Med 341:342-352, 1999
9. Hiorns MP, Owens CM: Radiology of neuroblastoma in children. Eur
Radiol 11:2071-2081, 2001