ped allergicon 2015iapkerala.org/wp-content/uploads/2015/04/ped-allergicon-2015... · allergen...
TRANSCRIPT

IAP KERALA
ALLERGY & APPLIED IMMUNOLOGY CHAPTER
PED ALLERGICON 2015
at MIMS KOZHIKODE JUNE 14
ORGANIZED BY IAP KOZHIKODE
SOUVENIR

W HAT'S INSIDE
ALLERGIC RHINOSINUSITIS- AN INDIAN PERSPECTIVE
NATURAL HISTORY OF CHILDHOOD ASTHMA
ALLERGEN SPECIFIC IMMUNOTHERAPY
ALLERGY- NATURE OR NURTURE
ACUTE SEVERE ASTHMA
FOOD ALLERGY- THE GOURMET'S DILEMMA
ANAPHYLAXIS
ALLERGIC DISORDERS OF EYE
ATOPIC DERMATITIS- A PRIMER
NON PHARMACOLOGICAL MANAGEMENT
OF PEDIATRIC ALLERGIC DISEASES
PALYNOLOGY-FOR THE CLINICIAN

Dear Colleagues,
I am extremely happy to know that IAP Kozhikode, one of our active
branches, is organizing the First State Conference of Allergy and
Applied Immunology Chapter , that is also in an AWESOME way. IAP
Kozhikode branch observed immunization day, Autism day ,World
health day and all other important days in wonderful way. Congrats
to all office bearers of IAP Kozhikode.
New subspeciality branches will give more strength to State IAP. The
main pillars of strength of State IAP are State Executive Board, 22 IAP
branches and Subspecilty branches. This year all subspecialty branch
conferences were well attended. Such meetings will also activate the
local IAP branch .
The topics of the Ped Allergicon are very practical and will be useful
for the practicing pediatricians. I whole heartedly congratulate all
the members of the organizing committee and hope that the
conference will be a memorable one.
Wishing all the best and success once again
Yours in IAP,
Dr.T.M.Anandakesavan
State President’s Message
Respected Members,
Greetings from IAP Kerala State office. I consider it a privilege and
honor to write a message for the newborn Allergy and Applied Immunology
Chapter of IAP Kerala and first conference of PED ALLERGICON 2015.
Allergic reactions are quite common in children, but of lately there is an
increase in allergic diseases which Pediatirician faces in their day to day
practice. The changing environment and food habits play a major role and
awareness is key factor. The organizers of Allergicon 2015 have selected
topics to update the practicing pediatricians on the latest investigations and
management of allergic problems. The team of Dr Sudha Krishnanunni,
Organising Chairperson, Dr Muhammed Nishil, Organising Secretary, Dr Babu
Francis, President IAP Kozhikode, Dr Krishna Mohan, Secretary IAP Kozhikode
and members of the Organising team needs special applause for the selection
of faculty.
I congratulate Dr Remesh Kumar R, President, State Allergy and Immunology
Chapter and Dr Suresh Kumar E. K, Secretary, State Allergy and Immunology
Chapter on starting this chapter and wish them all the best in future activities.
Special appreciation goes to IAP Kozhikode team for conducting this
conference as AWESOME.
Wishing the new chapter, Conference and the Organising team the very best.
Yours sincerely,
Dr Shimmy Paulos,
Secretary, IAP Kerala
State Secretary’s Message

Dear colleagues,
PEDALLERGICON 2015- the 1st State Conference of Allergy & Applied
Immunology Chapter of IAP Kerala is all geared up to cater a day of academic
excellence at Kozhikode on 14th June 2015. Allergic disorders in children have
become the ‘nuisance illness ‘ for many of the parents and for sure has brought down the quality of life for most of them. Applied Immunology has
roped in a new era of treatment options for this segment of the pediatric
population. The IAP subspecialty of Allergy & Applied Immunology is sure to
offer much more to widen the academic horizon in this domain.
The IAP fraternity at Kozhikode under the ever charming guidance of Dr
Sudha Krishnanunni & Dr Babu Francis ably supported by the secretarial
proficiency of Dr .Mohammed Nishil & Dr.Krishna Mohan are leaving no stones
unturned to make this maiden venture of Allergy & Immunology Chapter a
memorable one. Added to this is the rear guard thrust & enthusiasm from Dr
Suresh Kumar.E.K. , the most prolific organizer Kerala IAP has seen in recent
years. The presence of National stalwarts in Allergy & Immunology, Dr
Paramesh, Dr.T.U.Sukumaran & Dr Nagaraju will be an exciting experience for
the delegates.
I take this occasion to wish the delegates a great day at Kozhikode on 14 th
June & wish this souvenir released alongside proud moments at the
participants desktop in the coming days.
Sincere Regards,
Message
Dr. Remesh Kumar
President
Allergy & Applied Immunology Chapter
IAP Kerala

Respected Members of Indian academy of Pediatrics,
It is my proud privilege to welcome you all to the first Annual state
conference of Allergy and Immunology Chapter of IAP Kerala!
Allergy and immunology chapter is one of the important subspecialty chapters
of IAP. Kozhikodebranch of IAP took up the challenge to host this prestigious
event.Under the able leadership of Dr. Babu Francis (President), DrKrishna
Mohan(Secretary), DrSudhaKrishnanunni (Org.Chairman), Dr.Mohamed
Nishil(Org Secretary) and Dr Remesh Kumar.R this conference will become a
historic event of IAP.
Allergic disorders in children is an important medical problem andit is our duty
to be part of the system to tackle this major health issue.A lot of newer
developments including newer drugs and treatment protocols are coming up in
this field. I understand that the conference is trying to keep pace with the new
developments in the field of pediatric allergy and immunology.
I congratulate the organizers of this annual state conference of the Allergy
and immunology Chapter of IAP Kerala, “Ped Allergicon 2015” for selecting a variety of important topics and a galaxy of faculty from all parts of country. I
am sure this conference will be remembered for a very long time to come for
its rich academic feast .
I thank our state president Dr Ananda Kesavan and state secretary Dr
ShimmyPoulose for all the support.
Yours sincerely,
Message
Dr . Suresh Kumar.E.K
Secretary,
Allergy & Applied Immunology Chapter,
IAP Kerala

Dear colleagues,
I feel proud to be associated with Calicut IAP hosting the first state
conference of IAP allergy and applied immunology chapter.
There is world wide increasing prevalence of non-communicable diseases
which include asthma and other allergic diseases .This in turn burdens health
care systems with serious impact on global economy.This group of conditions
form a major chunk in pediatric practice and the need for keeping abreast with
current knowledge can not be overemphasized. Revisiting Strachan’s hygiene hypothesis and the role of vitamin D in the genetics of lung development
opens new vistas of research for the youngsters with a scientific bent
I am sure this academic session will equip you better in your day to day
practice.
Jai Hind
Jai IAP
Dr. Babu Francis. C. A
President, IAP Kozhikode
Message

Dear Colleagues,
Greetings from IAP Kozhikode.
I feel happy and all the more proud to be associated with PED
ALLERGICON, the first ever state conference of Allergy & Applied
Immunology chapter of IAP Kerala.
With daily sneezers, chronic wheezers and itchy kids, the number of
Pediatric allergy patients attending the daily pediatric outpatient
units are definitely on a rise. I wish all the very best to the newly
formed Allergy and Applied Immunology chapter for doing quality
work in the field of this most sought after sub speciality , Allergy and
Applied Immunology.
Special Congrats to the MIMS Team for joining hands with IAP
Kozhikode and organizing this mega event , that too in an ‘Awesome’ manner.
I thank all the eminent faculties for providing all the articles in time
and also for their valuable guidance.
Sincere Regards,
Editor’s Page...
Dr. Krishna Mohan. R
Secretary,
IAP Kozhikode.
Editor ,E- Souvenir, PED ALLERGICON
Dr. SUDHA KRISHNANUNNI
ORGANISING CHAIRPERSON
Dr. MOHAMMED NISHIL
ORGANISING SECRETARY
INAUGURATION

PED ALLERGICON , JUNE 14, 2015
SCHEDULE
Hosted by:
IAP KOZHIKODE &
DEPT: OF PEDIATRICS, MIMS KOZHIKODE

ALLERGIC RHINOSINUSITIS IN CHILDREN –
AN INDIAN PERSPECTIVE.
Dr. T.U. Sukumaran Prof: of Pediatrics, PIMS, Thiruvalla

ALLERGIC RHINOSINUSITIS IN CHILDREN – AN INDIAN PERSPECTIVE.
PED ALLERGICON 2015
hinitis is defined as inflammation of the membranes lining the nose and is
characterized by nasal congestion, rhinorrhea, sneezing, itching of the nose
and/or postnasal drainage. Atopy is an important risk factor for rhinitis and
allergic rhinitis (AR) is the most common form. Although a cause of significant and widespread
morbidity, AR is often viewed, rather erroneously as a trivial disease. It may significantly affect
the quality of life of the patient by causing fatigue, headache, cognitive impairment and other
occasional symptoms.
Epidemiology of AR in India:
In India, ISAAC study was conducted in 14 centers. Phase I included 30,879 children in the 6-7
year age group while there were 37,171 children in 13-14 year age group. Data from India
revealed that nasal symptoms were present in 12.5% children in 6-7 years age group & 18.6% in
the 13-14 years age group. Allergic rhinoconjunctivitis was seen in 3.3% and 5.6% respectively.
ISSAC study in our centre showed a prevalence 35% and 40% respectively.
Diagnosis of Allergic Rhinitis is by: 1.Clinical evaluation – History and physical
examination, 2.Lab investigations, 3.Categorisation of severity and duration and 4.Assessment
of co morbidities
CLINICAL FEATURES
Allergic rhinitis is defined as a symptomatic disorder of nose induced by IgE mediated
inflammation, after allergen exposure of the nasal mucous membrane . It is a condition
manifested by 1.Nasal blockage, 2.Running nose (Rhinorrhoea), 3.Sneezing, 4.Itching.
To diagnose Allergic rhinitis, any 2 of the above 4 symptoms must be present for >1 hr every
day for >2 wks. Also there has to be some associated symptoms such as facial pain, loss of sense
of smell, and postnasal drip. Some individuals may develop sinus infection and disturbed sleep
as well.
NASAL EXAMINATION
A careful external and internal examination of nose is essential in diagnosing allergic rhinitis.
1. A deviated nasal septum can sometimes be apparent externally.
2. Gross nasal polyps can produce expansion of nasal bones.
3. A horizontal crease above the tip of the nose called ‘Darrier’s Line’ is characteristic feature of marked allergic rhinitis. The darrier’s line is caused by the patient persistently
rubbing the nose from below upwards with the palm of the hand.
4. ‘Allergic salute’ is done to relieve itching and free oedematous turbinates from the
septum.
5. The patient may exhibit facial grimaces like nose wrinkling and mouth wrinkling which
relieves the nasal itching of the rhinitis. (Allergic Mannerism).
R

ALLERGIC RHINOSINUSITIS IN CHILDREN – AN INDIAN PERSPECTIVE.
PED ALLERGICON 2015
6. With the worsening of symptoms, many children may develop bluish-black
discolorations under the lower eye lids which are termed ‘allergic shiners’. These
discolorations are caused by venous stasis in the areolar tissue of the lower palpebral
grooves from pressure on veins by oedematous allergic mucous membranes of the nasal
and paranasal cavities.
7. An internal examination using a simple nasal speculum can show an anterior deviation of
the septum, narrowing of the nasal valve and inferior turbinate hypertrophy.
8. Nasal polyps can easily be confused with swollen inferior turbinates. Nasal polyps are
non tender and grayish, whereas swollen turbinates are tender and pale purple or pink.
ARIA classification
Co-existence of rhinitis and asthma in children:
Of all the atopic disorders, AR is most commonly associated with asthma. An editorial
entitled “Rarely dose one hear a wheeze without a sneeze” succinctly described the close link
between the two entities. Nasal symptoms have been reported to occur in 28-78% asthmatics
while 17-38% of patients with AR have co-existent asthma.
A questionnaire based study by Ashok Sha et al. from Delhi determined the co-
occurrence of AR in 646 out patient asthmatics (405 children and 241 adults) reporting to his
institute. Symptoms of rhinitis were present in 75% of the children and 80% of the adults.
Three fourths of the children and 55% of adults with asthma and associated AR had
simultaneous onset of both diseases. It was thus observed that AR occurred commonly with
asthma and could be independent risk factor for development of asthma. In another study in
111 children with AR and/or asthma, both diseases co-occurred in 83(74%), while 9 (8%) had
asthma only and 19 (17%) had AR alone. He also found that exposure to environmental
Intermittent
<4days per week
<4 weeks per year
Persistent
> or =4 days per week
And > or = 4 weeks per year
Mild
Normal sleep and no
impairment of daily
activities,sports,leisures and
normal work at school and no
troublesome symptoms.
Moderate - Severe
one or more items
Abnormal sleep
Impairment of daily activities, sports,
leisures.
Abnormal work at school and
troublesome symptoms.

ALLERGIC RHINOSINUSITIS IN CHILDREN – AN INDIAN PERSPECTIVE.
PED ALLERGICON 2015
tobacco smoke led to significant feeling of suffocation in 7/9 (78%) patients with asthma,
73/83 (88%) patients with asthma and AR and 15/19 (79%) with AR alone.
Effect sinusitis in patients with allergic rhinitis and/or asthma:
The presence of sinusitis further aggravates the morbidity caused by rhinitis and/or
asthma. Ashok Sha et al. studied 216 patients with AR and/or asthma for the occurrence of
sinusitis. All patients underwent spirometry with reversibility and CT- PNS. As a part of the
workup, both investigations were performed in all enrolled patients, prior to commencement
of standard therapy. A CT staging system for noting the extent of rhinosinusitis, with the total
score ranging from 0-24 depending on number of sinuses involved, was adopted. Twenty
seven patients had asthma only (group 1), 131 had AR (group 2) and 58 had asthma with AR
(group 3). On CT-PNS, sinusitis was present in 20 (74%), 88 (67%) and 48 (82%) of patients
respectively. Sinusitis on CT-PNS was present in more than two-thirds of 189 patients with
AR in groups 2 and 3 (136/189). Postnasal drip (62/88 vs. 15/43, p < 0.05) and sneezing
(52/88 vs. 7/43, p < 0.05) were significantly higher in these patients as compared to those
without sinusitis. Co-existent sinusitis increased the severity and morbidity caused by AR
especially, in those who were predominantly “blockers”.
Skin test reactivity in allergic rhinitis in India:
Seasonal AR, also known as hey fever, is caused by IgE mediated reaction to seasonal
aeroallergens like pollens and moulds. Length of seasonal exposure to these allergens is
dependent on geographical location. In India, there are mainly two pollen seasons viz,
February to April, and September to December. In the former season, trees are the dominant
aeroallergens; while in latter season, weeds and grasses are the dominant aeroallergens.
Moulds do not show any definite seasonal trend and are present throughout the year, but
definitely show seasonal exacerbation in summer and winter season. Indoor fungi are however
mainly perennial but depend on the source of the organism. Perennial AR is caused by
aeroallergens, which are present all the year round in the environment. These aeroallergens
are commonly found indoors. Apart from moulds, they also include dust mites, animal
allergens or certain pollens and occupational allergens in areas where they may be
predominantly present throughout the year.
Intradermal skin testing against locally prevalent common aeroallergens in our patients
with AR showed that sensitivity was highest with pollens, fungi and house dust mite, amongst
aspergilla, sensitization to A. flavus was more common than other species, All patients were
sensitive to at least three aeroallergens. In our study comparing “sneezers and runners” with “blockers”, we found that “blockers had significantly more sensitization to fungi (62%) and house dust mites (40%)(p =0.04). Sensitivity to insects (66%), kapok cotton (5%) and wool
(3%) was more in “ sneezers-runners”, but the difference was not statistically significant (Table
1). Recently, in 207 patients with AR, we replicated that sensitization to pollens was
significantly positive among patients with intermittent disease, while sensitivity to insects, fungi

ALLERGIC RHINOSINUSITIS IN CHILDREN – AN INDIAN PERSPECTIVE.
PED ALLERGICON 2015
and house dust mite was significantly more among those with persistent disease. Overall, house
dust mite was demonstrated to be the most common allergen.
MANAGEMENT
Allergic rhinitis is mainly a clinical diagnosis and management is mainly four fold.
1. Environment control,
2. Pharmacotherapy,
3. Treatment of co-morbid conditions,
4. Immunotherapy
Recognising allergy triggers and avoiding them is the first step towards controlling Allergic
symptoms. Avoid allergic triggers like dust mite, pollen grain, animal dander, cockroach,
moulds, cold air, cigarette smoke, firewood smoke, mosquito coils, etc.
Pharmacotherapy
1. Second Generation Antihistamines (SGA)
2. Intra Nasal Steroids (INS)
3. Leukotriene Inhibitors
1. Second Generation Antihistamines
It should be prescribed due to their favorable efficacy and safety rate. SGA have greater
selectivity for peripheral H1 receptors. It has anti-allergic effect independent of action at
histamine receptors and long term treatment with SGA is safe. Drugs used are Cetrizine,
Levocetrizine, Fexofenadine and Loratidine.
2. Intranasal Steroids
INS are the first line drug for treatment of moderate to severe allergic rhinitis. It is the most
efficacious medication available and it can improve all symptoms of allergic rhinitis as well
as allergic conjunctivitis. Quality of life is better compared to antihistamines. Main INS are
Budesonide, Beclomethasone, Fluticosone Propionate and Mometasone.
3.Anti-Leukotrienes (Monteleukast)
It is indicated in seasonal allergic rhinitis,pre school children and allergic rhinitis associated
with other comorbid conditions like asthma and conjunctivitis. Although combinations of
antihistamines with monteleukast is beneficial in several studies, it is not recommended.

ALLERGIC RHINOSINUSITIS IN CHILDREN – AN INDIAN PERSPECTIVE.
PED ALLERGICON 2015
Treatment of Allergic Rhinitis (ARIA Guidelines)
References
1. Allergic Rhinitis and its impact on asthma. ARIA guidelines. 1999, available at http://www.whiar.com February
28,2004.
2. Beasly R, Keil U, Von Mutius E, Pearce N. World wide variation in prevalence of symptoms of Asthma, Allergic
Rhinoconjunctivitis and atopic eczema, ISACC. Lancet 1998, 351: 1225-32
3. Ashok Sha, Ruby Pawankar, Allergic Rhinitis and co-morbid Asthma: Perspective from India- ARIA Asia-Pacific
Workshop Report, Asia Pacific Journal of Allergy and Immunology (2009) 27:71-77.
Mild
Intermittent
Moderate –Severe
Intermittent
Mild Persistent
Moderate – Severe
Persistent
Intranasal Steroids and LTRA
Oral 2nd
generation antihistamines or LTRA
Environmental control
Immunotherapy

Natural History of Childhood Asthma
Dr.H.Paramesh. MD, FAAP, (USA), FIAP, FIAMS, FIAA, FICAAI Ped. Pulmonologist and Environmentalist, Bangalore Roshan Cherian Paramesh. BDS, MSc (Glasgow) (MDS) Dr. Rashmi Cherian Paramesh.

NATURAL HISTORY OF CHILDHOOD ASTHMA
PED ALLERGICON 2015
Our understanding of asthma continues to increase over time from Bronchoconstrition
Airway hyper responsiveness Inflammation and remodeling united airway concept
phenotypes and genetics to Dietary habits in controlling and preventing asthma.
The trend of asthma after a steady increase in prevalence showing a plateau and some decrease in
prevalence in some countries including our study in Bangalore. However the incidence of
persistent asthma and persistent severe asthma is increasing sharply which are the major causes
for morbidity, mortality and economic burden
The major issues of patient and healthcare providers which needs to be addressed are –
Is it Asthma?
No one has asthma in our family
Is it contagious?
What is the duration of treatment?
Does it have steroids?
What food can be given?
Can he/she play?
Is he/she going to outgrow the disease?
The prevalence of asthma in UK under five years of age was 84.8% in 1961 (I Morrison Smith –
BMJ 1961), it is 77.7%in India (H Paramesh I.J. Ped. 2006). The diagnosis is predominantly
clinical based in this age group the stringent and loose index is not practical in developing
countries, the extrapolation of data on future risks is difficult in clinical practice.
The genetic ancestry, gene to gene interaction not only directly influences asthma but also
influence through the environmental interaction in the development of asthma. The changes in
the demography and various social factors contribute to the environment factors.
Asthma is not contagious, but children with viral infections are contagious. The predominant
viruses that are isolated in our country are RSV, par influenza type 1-3 and human meta
pneumovirus
The duration of treatment –
Quick relievers are used until symptoms subside. &
Controllers, until the inflammation subsides completely. In atopic persistent asthma, for 3
months and reduce the dose 25-50% q 3 months. Use the principle of TWO to add the controllers
with the use of quick relievers. (When quick relievers are needed more than Two times in a
week, and has disturbed sleep more than Two times in a month). Social determinants will dictate
terms in selection of medicine and route.
Address the issues of steroids side effect that inhaled steroids used in recommended dosage don’t have any ill effect on growth and it is also true that uncontrolled severe asthma can affect growth
NATURAL HISTORY OF CHILDHOOD ASTHMA
PED ALLERGICON 2015
and final adult height. While using inhaled steroid, one has to look into the systemic bio
availability of inhaled corticosteroids.
The decay of front teeth has been related to Beta-2 agonist usage than inhaled steroid.
The possible causes are a) reduced buffering capacity and salivary flow rate b) Increases
exposure of teeth to acids by extrinsic source like acidity of the medicine, acid drinks or Intrinsic
source by gastroespohgeal reflux.
Diet plays a multifaceted role in shaping the observed worldwide trends of childhood allergies.
Children should be encouraged to use more home made traditional food, fish, butter, vegetables,
fruits with less salt and carbonated drinks.
Children should be encouraged sports in school and encouraged non medical measures like
doubling the time of warming up and to breath through the nose and preferably to play in the
afternoon; 15min before any competitive sports 2 puffs of salbutamol inhalation to be used
preferably or montelukast 6hrs before.
Some of the follow up studies from birth to 6 years to 42 years showed that 70 percent of
asthmatics wheezed at 42yrs of age. Those children are atopic and poorly controlled asthmatics.
For good control of asthma needs education about disease,, avoidance of triggers,
pharmacotherapy, regular monitoring and Immunotherapy. It is noteworthy that there are only
two ways to prevent asthma, a good environment control including nutrition in pregnant
mothers, children and immunotherapy. Most of our future research is towards the preventive
measures.
Reference:
1. Paramesh H.’Epidemiology of Asthma in India’. Indian Journal of Pediatric, 2002 Vol. 69, pp. 309-312.
2. Yunginger JW, Reed CE. O Connell EJ. Melton LJ 3rd, O’ Fallon WM, Silverstein MD. A community –
based study of the epidemiology of asthma. Incidence rates, 1964-1992;146:888-894.
3. N.G Papadopoulos, H. Arakawa, K.H. Carlsen, ACustavic, H. Paramesh et al. International Consensus on
(ICON) Pediatric asthma. Allergy – 2012, 67 (8)976-997
4. Paramesh H. Asthma in children: Seasonal variation Int J of Environ health 2008: 4:410-416
5. H Paramesh The unmet challenges in child health environment Pulmonary clinics of India 2014; Vol – 1
No 1 Page 217-227
6. Global initiative for asthma 2014 www.giasthma.org
7. Manuel S.T. Kundabaka M, Shetty N, Parolia A. Asthma and dental erosion Katmandu University medical
journal 2008, Vol 6. No-3 Issue 23:370-374
8. Navneeth Godara, Ramya Godara, Megha Khullar. Impact of inhalation therapy on oral health. Lung India.
2011; 28 (4): 272-275
9. Mazie Boskabady et al. Iranian Red Crescent medical Journal 2010:14 (12) 816-821

ALLERGEN SPECIFIC IMMUNOTHERAPY
Prof. (Major) K. NAGARAJU Allergist & Immunologist Saveetha Medical College VN Allergy & Asthma research center Paediatric Allergist, Apollo Children’s Hospital Chennai

ALLERGEN SPECIFIC IMMUNOTHERAPY
PED ALLERGICON 2015
Introduction:
The dramatic changes in health-care delivery in the past decade have brought a
renewed focus on the value and indications for many therapies. Among these one is Allergen
specific immunotherapy; a treatment modality available to medical profession for IgE
mediated allergic disorders. Allergen specific immunotherapy (ASIT) refers to a gradual
immunizing process in which increasing doses of antigens responsible for causing allergic
symptoms are administered to a patient to induce increased tolerance to the allergen when
natural exposure occurs. It is also known as hypo sensitization or desensitization. The benefit
of specific immunotherapy is dependent on both the dose and the route of administration.
Although the mechanism by which this benefit occurs is not fully understood, the proposed
mechanism by which this specific immunotherapy works is by inducing allergen-specific T
regulatory cells that reduce the late-phase response to the allergen.
History
Noon introduced this technique as early as 1911 by inoculating pollen extracts in cases of
hay fever. Literature search reveals that different methods have been applied from time to
time viz. inhalation method in asthma sensitive to house dust mite and Rinkle method in
pollen hay fever. Later Ohman and Bousquet et al used the allergen immunotherapy in
asthma and allergic diseases. In India, an array of workers reported hypo sensitization in
respiratory allergy and asthma
Conditions where Immunotherapy effective & Ineffective
Immunotherapy is effective in
Allergic Rhinitis
Allergic Asthma
Insect stinging and insect sensitivity
Recently FDA approved this modality of therapy for Atopic dermatitis.
Immunotherapy is Not effective in
Eczema
Food allergy,
ALLERGEN SPECIFIC IMMUNOTHERAPY
PED ALLERGICON 2015
Latex allergy & Urticaria,
Indications for Immunotherapy
Insufficient response to pharmacotherapy.
Insufficient response to environmental control.
Significant side-effects to medical therapy.
Patients who have perennial disease.
Poor compliance to medical regimen.
Possible prevention of Asthma from Allergic Rhinitis.
Mild to moderate asthma.
Moderate to severe Allergic rhinitis
Contraindication for Immunotherapy
Absolute contraindications
Severe asthma – FEV1 < 70% with active Rx.
Relative contraindications
Contraindications for epinephrine (Beta-blocker).
Immuno deficiency / auto immune diseases.
Pregnancy. Although Pregnancy is not a contraindication, it cannot be started because in case of reactions it may affect the baby. During pregnancy maintenance therapy can be continued
.Malignancy.
Psychological
Mentally impaired patients.
Short expected life span < 5 year
Non compliant patient
Safety & Efficacy of Immunotherapy
When properly administered to an appropriate candidate, it is a safe, effective form of
therapy capable not only of reducing or preventing symptoms, but also potentially alters the
natural history of the disease by minimizing disease duration and prevention of disease
progression. The use of standardized extracts is will give optimal results. Success of
immunotherapy depends on optimal means of allergy testing, quality of allergen extract,
correct initial dose of Immunotherapy and follow-up with maintenance dose. Failure of
Immunotherapy is mainly due to inadequate environmental control. missed diagnosis (Non-
allergic rhinitis),failure to include allergen in SIT, exposure to unknown allergen, inadequate
dose of allergen injection, non-compliance of schedule, development of new allergic

ALLERGEN SPECIFIC IMMUNOTHERAPY
PED ALLERGICON 2015
sensitivities, unrealistic patient expectations for cure and some patients may not responded
favorably to immunotherapy itself.
Adverse reactions
Systemic reactions to immunotherapy occur within one hour of administration of the allergen
which is usually scattered hives and rarely severe anaphylaxis, where as local reactions can
occur up to 24 hours. Incidences of Fatal Anaphylaxis will range from 1 per 2 million
injections. Common local reactions are wheals, indurations or both mainly due to poor
injection technique. Patient should be under observation for 30 minutes to monitor allergic
reactions. Patient education is essential especially for delayed reactions. At the first step to
the reaction a tourniquet may be applied above the injection site and epinephrine may be
administered at a appropriate dose preferably by the intramuscular route. Equipment
necessary for resuscitation including bag and mask, oxygen etc. should be available at the
office while you are going to administer immunotherapy. Not even a single case of fatal
anaphylaxis was encountered in author’s ten years of practice.
Schedule of Immunotherapy
Schedules of allergen administration are selected based on the sensitivity of the patient to the
allergens in the extract. Dose ranges from 4-12ug administered subcutaneously.
Subcutaneous route of allergen administration is most widely used and well documented in
the literature. Despite the established efficacy of subcutaneous injections of causal allergens,
the therapy did not gain popularity due to risk of systemic reactions.FDA has approved for
Injection Immunotherapy from 5 yrs and above, however sublingual immunotherapy can be
used from 3 years in some cases.
Primary Immunotherapy: To start with low doses are administered which can be stepped
up gradually in dosage & frequency until maintenance dose is reached. It has to be given for
3 – 5 months. We start twice weekly regime from 1in 1,00,000 dilutions & increase slowly to
reach 1 in 10 dilutions depending upon the severity of skin test reaction to particular allergen.
Maintenance Immunotherapy: After attaining adequate control with twice weekly regime
with 1 in 10 dilutions, we used to change over to maintenance immunotherapy. To start with
twice monthly until adequate control and later change to monthly once. To get adequate
response one year of treatment is compulsory .If there is no response it can be

ALLERGEN SPECIFIC IMMUNOTHERAPY
PED ALLERGICON 2015
discontinued. Progressive improvement occurs by 2-3 years. Maintenance immunotherapy is
given for a period of 3- 5 years. Prediction of response is difficult.
Allergens used in Immunotherapy:
Allergen extracts are heterogeneous mixture of proteins and lose potency on storage. The loss
of potency affects diagnosis of allergy & immunotherapy. Concentrated aqueous extracts in
50% glycerin are stable for about 3 years, if stored in a refrigerator at 40C, but without
glycerin, they lose their potency within 6 months. Immunotherapy is effective for pollens,
fungi, animal dander, House dust mite, and cockroach and hymenoptera venom. Allergen
formulation requires, progress in standardization, efficacy and safety depend upon multiple
or single allergen mixture in single vial. For mixed allergen vaccine the following factors
must be considered; 1) the cross reactivity of the allergens, 2) the optimal dose of each
constituent and 3) enzymatic degradation of allergens. . Allergen extracts to be stored at 2-
8°C in the refrigerator for optimal efficacy.
Alternative routes
Nasal Immunotherapy is administered as spray allergen solution into the nose in a phased
manner but lack of significant immunologic response led to discontinuation of this route.
Sublingual Swallow immunotherapy (SLIT) is administered as drops of high dose allergen
solution underneath the tongue which is then swallowed. It may be started as the full
maintenance dose, without the gradual increase in dose (Primary Immunotherapy). The
common side effect of sublingual immunotherapy is local irritation in the mouth and under
the tongue (47% to 52%). but it is usually transient and does not progress to anaphylaxis. This
side effect presumably reflects local allergic reactions to the allergen extract. In the author’s
own practice local irritation & even mouth ulcers were encountered in more than 50%
patients. It has the added advantage of ease of administration, home based therapy and
avoidance of painful injections. Though SLIT is effective it has its own disadvantages
especially in our country, where it is not known whether parents are properly administering
the drops (Correct dosage & frequency), how to adjust the dose during acute illnesses such
as diarrhea & vomiting, how to carry the SLIT antigens when on holidays (Cold chain) & last
but not the least any disruption in treatment due to financial constraints.
ALLERGEN SPECIFIC IMMUNOTHERAPY
PED ALLERGICON 2015
Intra bronchial administration which was advocated initially is now avoided for general
use due to untoward side effects.
Future strategies include alum depot preparations which act as adjuvant, allergoids which
are chemically modified allergens, peptide immunotherapy which uses allergen derived T-
cell peptide epitope, recombinant allergens and anti IgE antibodies.
Oral Desensitization for food allergies are under phase II & III trials in several parts of the
world. Several studies done on Cow’s milk protein allergy and few studies for Peanut & egg
allergies are under trail. Recent results are encouraging.
Intra lymphatic immunotherapy (ILIT)
The long treatment duration and systemic reactions associated with conventional
subcutaneous immunotherapy likely impedes broad acceptance. These problems will be
overcome by Intra lymphatic immunotherapy. Allergen doses could be reduced 100 times
when administered directly in to the lymph nodes as compared with the subcutaneous route.
Confirmatory experiments in humans revealed efficient antigen pushing of lymph nodes 20
minutes after intra lymphatic injections, whereas only small antigen fractions reached the
lymph node 25 hours after subcutaneous injection.
Recent clinical trials reveal that intra lymphatic immunotherapy allows high therapeutic
efficacy with considerable reduced treatment dose and duration. Combined with its good
safety profile, ILIT is therefore likely to increase treatment compliance and socioeconomic
costs especially in our country.
Epicutaneous Immunotherapy
Epicutaneous immunotherapy is a needle free and potentially self administered treatment
modality recently preferred by several allergists. Blamoutier and collegues applied the
allergen drops onto heavily scarificated skin & demonstrated that amelioration of symptoms
after 4weeks therapy & treatment success rate around 80%. Based on this principle tape
stripping method was developed with improved efficacy.

ALLERGEN SPECIFIC IMMUNOTHERAPY
PED ALLERGICON 2015
Rush Immunotherapy
The process of inducing adequate immunological response in an accelerated pace, where in
all the doses could be given with in a period of few days is termed as Rush Immunotherapy.
Here the doses are spaced out in 2-6 hourly intervals so that maintenance dose is reached
within few days. The risk of systemic allergic reactions is high. It has to be undertaken
where facilities for intensive care and monitoring are available. Patients should be pretreated
with anti-histamines and corticosteroids.
What’s on the horizon?
Researches are on into allergen immunotherapy to seek safer and more convenient allergy
“vaccines”. Approaches include humanized monoclonal anti-IgE antibodies, which have
been shown to be effective in treating asthma and food allergies.
Anti-cytokine therapy investigations are also underway. Anti-interleukin-5 therapy
reduces the bad effects of reactivity, but doesn’t improve bronchial hyper-responsiveness.
Early trials of tumour necrosis factor alpha (TNF) blocking have shown some success, but
further work is needed on specific blockers in allergic pathways. CpG-based
immunotherapy significantly reversed both acute and chronic markers of inflammation as
well as airway hyper responsiveness. CpG DNA may provide the basis for a novel form of
immunotherapy of allergic asthma.
Future options for treating allergic disease will focus on allergen specific routes, including
further development of immunotherapy and targeting of specific mediators, an area with a
great deal of promise, especially in people with refractory disease.
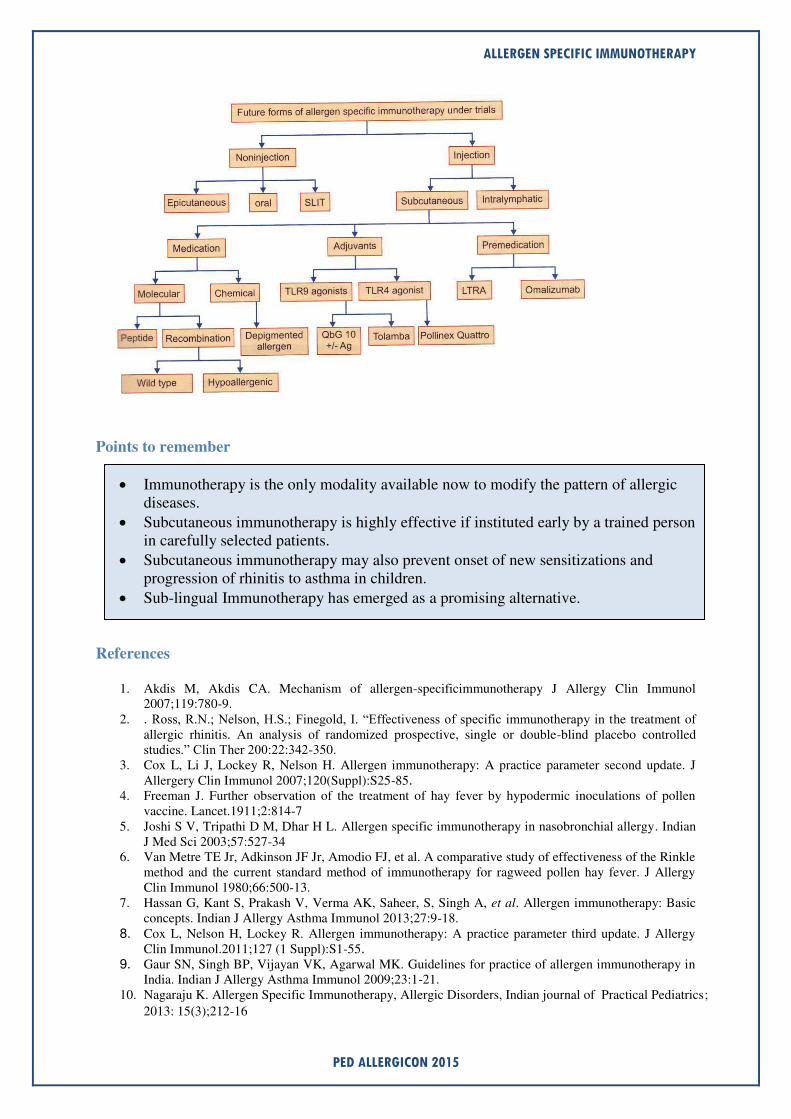
Future forms of Allergen specific immunotherapy under trial:
See flowchart below:
ALLERGEN SPECIFIC IMMUNOTHERAPY
PED ALLERGICON 2015
Points to remember
Immunotherapy is the only modality available now to modify the pattern of allergic diseases.
Subcutaneous immunotherapy is highly effective if instituted early by a trained person in carefully selected patients.
Subcutaneous immunotherapy may also prevent onset of new sensitizations and progression of rhinitis to asthma in children.
Sub-lingual Immunotherapy has emerged as a promising alternative.
References
1. Akdis M, Akdis CA. Mechanism of allergen-specificimmunotherapy J Allergy Clin Immunol 2007;119:780-9.
2. . Ross, R.N.; Nelson, H.S.; Finegold, I. “Effectiveness of specific immunotherapy in the treatment of allergic rhinitis. An analysis of randomized prospective, single or double-blind placebo controlled studies.” Clin Ther 200:22:342-350.
3. Cox L, Li J, Lockey R, Nelson H. Allergen immunotherapy: A practice parameter second update. J Allergery Clin Immunol 2007;120(Suppl):S25-85.
4. Freeman J. Further observation of the treatment of hay fever by hypodermic inoculations of pollen vaccine. Lancet.1911;2:814-7
5. Joshi S V, Tripathi D M, Dhar H L. Allergen specific immunotherapy in nasobronchial allergy. Indian J Med Sci 2003;57:527-34
6. Van Metre TE Jr, Adkinson JF Jr, Amodio FJ, et al. A comparative study of effectiveness of the Rinkle method and the current standard method of immunotherapy for ragweed pollen hay fever. J Allergy Clin Immunol 1980;66:500-13.
7. Hassan G, Kant S, Prakash V, Verma AK, Saheer, S, Singh A, et al. Allergen immunotherapy: Basic concepts. Indian J Allergy Asthma Immunol 2013;27:9-18.
8. Cox L, Nelson H, Lockey R. Allergen immunotherapy: A practice parameter third update. J Allergy Clin Immunol.2011;127 (1 Suppl):S1-55.
9. Gaur SN, Singh BP, Vijayan VK, Agarwal MK. Guidelines for practice of allergen immunotherapy in India. Indian J Allergy Asthma Immunol 2009;23:1-21.
10. Nagaraju K. Allergen Specific Immunotherapy, Allergic Disorders, Indian journal of Practical Pediatrics;
2013: 15(3);212-16

ALLERGEN SPECIFIC IMMUNOTHERAPY
PED ALLERGICON 2015
11. www. Ginasthma.org/GINA report 2014. 12. Zeinab A. El-Sayed, Ola G. El-Farghali. Allergen-specific immunotherapy in children. Egypt J Pediatr
Allergy Immunol 2012;10(2):55-67. 13. Mauro M, Russello M, Alesina R. Safety and pharmacoeconomics of a cluster administration of mite
immunotherapy compared to the traditional one. Eur Ann Allergy Clin Immunol 2006; 38: 31–34.
14. Pajno GB. Sublingual immunotherapy: The optimism and the issues. J Allergy Clin Immunol 2007;119:796-801.
15. Mailing HJ. Is sublingual immunotherapy clinically effective? Curr Opin Allergy Clin Immunol 2002;2:523-31.
16. Wilson DR, Lina MT, Durham SR. Sublingual immunotherapy for allergic rhinitis: Systematic review and meta-analysis. Allergy 2005;60:4-12.
17. Penagos M, Compalati E, Tarantini F, Baena-Cagnani R, Huerta J, Passalacqua G, et al. Meta-analysis of the efficacy of sublingual immunotherapy in pediatric patients, 3 to 18 years of age. Chest 2008;133:599-609.
18. Canonica G W, Cox L, Ruby Pawankar, Carlos E Baena-Cagnani C E B, Michael Blaiss M “Sublingual Immunotherapy: World Allergy Organization Position Paper 2013 Update”, World Allergy Organization
Journal 2014, 7:6
19. Creticos PS, Norman PS, Feldweg AM. Oral and sublingual immunotherapy for allergic rhinitis.
http://www.uptodate.com/contents/. Last updated: May, 2011. Accessed: June, 2011.
20. Senti G, Crameri R Kuster D, Pål Johansen etal: Intralymphatic immunotherapy for cat allergy induces
tolerance after only 3 injections, J Allergy Clin immunol 2012; 129; 1290- 96.
21. Senti G, Graf N, Hang S, Ruedi N etal: Epicutaneous allergen administration as a novel method of
allergen specific immunotherapy. J Allergy Clin Immunol 2009;124:997-1002
22. Senti G, von Moos S, Kündig TM. Epicutaneous allergen administration: is this the future of allergen-
specific immunotherapy? Allergy 2011; 66: 798–809.
23. Moises A. Calderon, Linda Cox, Thomas B. Casale, Philippe Moingeon, and Pascal Demoly, Multiple-allergen and single-allergen immunotherapy strategies in polysensitized patients: Looking at the published evidence. J Allergy Clin Immunol 2012;129:929-34
24. Srivastava D, Singh BP, Arora N, Gaur SN. Clinico-immunologic study on immunotherapy with mixed and single insect allergens. J Clin Immunol 2009;29:665-73.
25. Stefan Zielen, Peter Kardos, Enzo Madonini, Steroid -sparing effects with allergen specific immunotherapy in children with asthma A randomised controlled trial: J Allergy CLIN Immunol, 2010; 126: 942-9.
26. Hankin. American Academy of Allergy, Asthma & Immunology (AAAAI) 2014 conference:
Abstract 579. Presented in March , 2014
27. Lieberman etal: Epigenetic effect of allergy immunotherapy. J Allergy Cli Immunol. 2012; 130; 215-24.
28. Glovsky MM, Ghekiere L, Rejzek E: Effect of maternal immunotherapy on immediate skin test
reactivity, specific rye I IgG and IgE antibody, and total IgE of the children. Annals of Allergy 1991;
67(1):21-24
29. Alsamarai AM, Alobaidi AHA, Alwan AM, Abdulaziz ZH, Dawood ZM (2011) Systemic Adverse
Reaction to Specific Immunotherapy. J Aller Ther

Acute Severe Asthma
Dr. C. Jayakumar. Professor of Pediatrics, Govt MCH ,Kottayam

Acute Severe Asthma
PED ALLERGICON 2015
Definition
Asthma that don't improve with conventional therapy is defined as status asthmaticus.
Any form asthma , even intermittent form can exacerbate and end up in status.
Mild exacerbation
Wheeze only at the end of expiration
PEFR 70-90%of the expected
Pulsus paradoxus less than 10 mm of hg
Rate less than age appropriate cut off
Talk sentences
Minimal retraction
Alert
SpO2more than 95% with room air
PaCo2 <35 mm of hg
Moderate exacerbation
Rate increased
Alert
Speaks phrases
Intercostal,suprasternal and
Sternocleido mastoid involvement
Pulsus paradoxus 10-20 of hg
Spo2 <95%
Pao2 <40mmof Hg
PEFR 50-70%
Wheeze through out respiration
Severe exacerbation
Not alert
Talk only words
Spo2 <90%
Pulsusparadoxus 20-40mmof Hg
Severe>40mmof Hg
Silent chest
Rate very much increased
Acting of alae nasi
PEFR <50% of the personal best
Life threatening (near fatal asthma)
Comatosed
Silent chest on auscultation
Spo2 <85%
Cyanosed

Acute Severe Asthma
PED ALLERGICON 2015
Brady arrythmia/dysrythmia
Hypo tensive
Pulsus paradoxus >40mmof Hg
PaCo2 >45mmof Hg
PEFR <33%
Feeble respiratory effort
PSI
Rate <30/<20 31-45 46-60 >60
Wheeze None End Entire Entire
expiration expiration
Accessory
muscle use None ?+ + ++
Sao2 >99 96-98 93-95 <93
I:E ratio 2:1 1:1 1:2 1:3
Score 0 1 2 3
Arithmetic
0-3 normal,slight
4 -6 mild exacerbation
7-11 moderate exacerbation
>12 severe exacerbation
Red flag signs
Brady cardia
Poor pulse volume
cyanosis
Silent chest
<92%O2
Excessive accessory muscle use
Alteration of sensorium
MONITOR PSI EVERY 15-30 minutes
History
Role in mild & moderate cases only
Serious situation- don’t waste time for history taking Grade of asthma
Level of control
Dosage of controllers

Acute Severe Asthma
PED ALLERGICON 2015
Trigger
Delivery device
Adhesion and supervision
Any use of Theophyllines at all
Quick physical exam
Simultaneous with the administration of o2 and checking the pulse Oxymetry&ABG
estimation
Grunt - pneumonia
Stridor - Croup /FB
Percussion usually hyperresonant
Fever
Evidence of bacterial infection in the skin
LAB
After the stabilization
CXR not routinely taken. Done in
Localized crackles
Asymmetry
High fever
First time wheeze
Therapy
O2 at a rate of 6-8L/minute along with compressed air and salbtamol to have a
Spo2 >92% or 10-12L/minute in o2 driven salbutamol nebuliztion
Prior oxygenation -prevent ventilation perfusion mismatch that occur with more
perfusion of under aerated lung associated with β2 agonist use
β₂agonist
Cornerstone in asthma exacerbation
Nebulization/MDI
< 30 kg 2.5 mg
> 30kg 5mg in 3ml N saline given over 10-15minutes
MDI < 6years -6puffs , >6yrs -12 puffs 20 sec interval
Repeat after 20 minutes again after 20 minutes again after 20 minutes (18/36 puffs)
in 1 hr if required assessed by the patient response (RR,Spo2, word output etc)
Continuous neb no added advantage
Don’t forget to give 1st dose of steroid orally
β₂agonist S,C/IV
Terbutaline 10µgm/kg =0.02ml/kg
(max 400µgm=0.8ml)
1ml=0.5mg
IM better than s/c

Acute Severe Asthma
PED ALLERGICON 2015
iv Terbutaline 1 ml in 50 ml of 5% D
1ml= 10µgm
10µgm/kg=0.02ml/kg as a
bolus in 10 minutes
Followed by0.1µgm/kg(0.0002ml)= to 1µgm/kg (0.002ml)increasing every 30
minutes to 3µgm/kg(0.006ml) or 10µgm/kg0.02ml/kg
Candidate for parenteral Terbutaline:
Poor response to inhaled therapy
Imminent respiratory arrest
Poor response irrespective of best ventilator setting
Dangers of parenteral Terbutaline:
Hypertension
Dysrhythmias
Myocardial ischemia
IV adrenaline more side effects
Ipratropium Bromide:
<20kg or <5 years - 125µgm 0.5 ml
>20 kg - 250µgm - 1 ml
20 -30 minutes in 1 hr
Every 2-4 hrs for the first 24 hrs
Usually for the first 24 hrs only
Steroids:
Up regulate β₂ receptors.
Down regulate the inflammatory mediators.
1mg/kg for 3 days .
Maximum dose 60mg/d
More than 3 days can be continued
No need to taper in <14 days
Inj methyl prednisolone 1mg/kg 6th
hrlyor
iv hydrocortisone5mg/kg 6th
hrly can be used instead
Inj Dexamethasone 0.6mg/kg max 16 mg is another option
Magnesium sulphate
Useful in refractory asthma
25-75mg/kg in20ml N saline over 30 minutes can be repeated after 6hrs if necessary
Magnesium sulfate can be given as nebulization also at a dose of 150 mg/kg 20
minutes interval for 3 times
Insufficient data
Heliox o2 mixture
Ketamine nebulizaion

Acute Severe Asthma
PED ALLERGICON 2015
LTRA
Nebulized dose of budesonide
Contraindicated/controversial
Aminophylline
When all other therapeutic options exhausted
5mg/kg st .Then 0.5-1mg/kg /hr as infusion
Narrow therapeutic range 10-20µgm/ml
Keep around 10 µgm/ml
Seizures ,tachcardia,emesis anxiety and dysrhymias are the side effects
NPPV Prior to intubation if breathing spontaneously
can be tried
CPAP/BIPAP are the options
Mechanical Ventilation:
First or last option ? last !
Not easy
Avoid hyper inflation and Auto PEEP
Volume controlled or pressure controlled ? --- volume controlled as variable
resistance leads to hypo or hyper ventillation
Rapid weaning as the hyper ventilation is subsided
No benefit
Cough suppressants
Mucolytics
Chest physio
Antibiotics
Weaning
Last in first out
Taper the dose ad interval of SABA
PSI < 7
Child sleeping normally, playful eating normally
Poor response
Air leaks
Atelectasis
Bronchiectasis
Pneumonia
Congenital malformations
FLOW CHART
SalbutamolMDI/NEB every 20-30 minutes

Acute Severe Asthma
PED ALLERGICON 2015
Rescue steroids O/im/Ipred/dexa/methyl pred
Add ipratropium 20 -30 minutes along with SABA
Try Sc /IM terbutaline or adrenaline
Start Magnesium sulfate /magnesium sulfate nebulisation
IV Tebutaline bolus and infusion
NPPV
Inj aminophylline
Ketamine nebulzation
Heliox o2 mixture
MV
DISCHARGE:
Written asthma action plan
Check the drugs device delivery
Avoid trigger check list
Follow up next week every 2 weeks for 1month
Every 4 weeks 2 months
Then every 8weeks
Well controlled for 3 months taper ICS by 50% to keep the lowest ICS for 1 year
If still well controlled stop assuming remission

Allergy-
Is it due to nature or
nurture?
Dr. Mohandas Nair Asso: Prof: of Pediatrics, Govt: Medical College, Manjeri

ALLERGY…IS IT DUE TO NATURE OR NURTURE ?
PED ALLERGICON 2015
Worldwide, the prevalence of allergy is increasing, especially in the industrialized
world. It could be due to increased detection rate. But that alone may not be the issue. It will be
worthwhile in pondering what the real cause of allergy is. Is it part of our genetic makeup? Or is
it something we acquire? The present consensus is that both factors are responsible.
Why should we study the genetic basis of asthma/ allergy?
1. To identify various genes involved and their role
2. To develop new treatment modalities
3. Presymptomatic diagnosis and preventive strategies
4. To identify personalized treatment (pharmacogenetics)
Allergic diseases are complex genetic disorders susceptible to environmental stimuli.
Several genes are found to be associated with allergic disorders. More than 100 asthma genes are
identified, but only in about 25, association was replicated more than 5 times. Once allergic
responses have been initiated, a genetic predisposition to chronic allergic inflammation and
aberrant injury-repair responses contribute to tissue remodeling and persistent disease.
Factors favouring genetic etiology:
Strong familial predisposition is present for allergic diseases. From families where neither
parents had a history of asthma, only six percent of children suffered from asthma. In families
where one parents suffered from the condition, 20 percent of children suffered from it. And in
families where both parents had asthma, 60 percent of the children had asthma as well. This
shows that there is a strong link between asthma and genes.
Twin study for pea nut allergy: 44 pairs of fraternal (nonidentical) twins and 14 pairs of
identical twins were selected (at least one among one set of twins had pea nut allergy). They
were given pea nuts and observed for 60 minutes for allergic reactions. 65% 0f identical twins
shared the allergy, but only 7% of the fraternal twins shared the problem. The study concluded
that genetic factors responsible for more than 80% cases of pea nut allergy. Genetic engineering
may help in developing allergen free pea nuts.
Various investigative modalities like genome wide association studies and Meta analysis
of various such studies have identified various genes responsible. Unlike Mendalian inheritance,
a single gene alone is not responsible for it. So the inheritance pattern of allergy is said to be
complex.
Chromosomes and genes responsible: Genes, variation of which increases the
susceptibility to develop asthma/ allergy are so many and present in almost all chromosomes.

ALLERGY…IS IT DUE TO NATURE OR NURTURE ?
PED ALLERGICON 2015
Some of them are
1. 5q23-35 region
2. 11q13
3. HLA locus of chromosome 6
4. Chromosome 2q14 (DPP 10)
5. Chromosome 1q21 (related to barrier dysfunction)
6. Chromosome 7p14 (GPRA gene)
7. Chromosome 20p (ADAM 33 gene)
8. Chromosome 16
9. Filaggrin gene (FLG) gene
10. COL29A1gene
More and more genes responsible for allergic diseases are being identified day by day.
If allergy is genetically mediated, why the prevalence of allergic diseases is increasing
over the last few decades?
This increase is attributed to changes in environmental factors (exposure to tobacco
smoke, air pollution, indoor and outdoor allergens, respiratory viruses, obesity etc.).
Hygiene hypothesis in Asthma: It has been hypothesized that increased cleanliness,
reduced family size, and subsequent decreased microbial exposure could explain the increases in
global asthma prevalence. But this is not proven. Some investigators have the opinion that this
hypothesis hold good for atopy and not for asthma.
That means both nature and nurture has got important role in allergic diseases. They are
not mutually exclusive, but complementary to each other.
What is the inheritance pattern of allergy?
Genome wide association studies (GWAS) has thrown light on the mode of inheritance of
asthma and allergy to some extent. Asthma and allergy are caused by the complex interplay
between genetic factors and environmental exposures that occur at critical times in development.
Genes are many, combination of their interplay is exponential and it is more difficult to analyse
the interplay between genes and environment.

ALLERGY…IS IT DUE TO NATURE OR NURTURE ?
PED ALLERGICON 2015
Asthma and other allergic diseases: same disease or shared pathways?
A large multi-center study of SNPs in 14 candidate genes for wheeze and allergy
suggested that asthma and atopy are not different manifestations of the same disease. Non
immune, non allergy genes (eg. 17q21 locus) are more related to childhood asthma, but not with
atopy. At the same time, many genes are common for asthma and atopy. Thus, common alleles at
the 17q21 locus and/or ADAM33 may be specific for the development of asthma, whereas
relatively rare variants in the filaggrin gene (FLG) may be specific for atopic dermatitis.
Combination of more than one environmental factor increases the chance of developing
asthma as shown in one study. Here, use of baby formula and antibiotics early in life was
associated with an odds ratio of 7.4 (95% CI 4.5-12.0) of developing asthma. More over genetic
variants together with environmental factors seemed to play a role for allergic diseases, such as
the use of antibiotics early in life and COL29A1 variants for asthma, and farm living and NPSR1
variants for allergic eczema.
In the coming years, it is expected that a clear cut idea in this regard will be coming out.
At that time, it is expected that we can suggest specific environmental modification to those
having specific gene variations to prevent asthma and to suggest which treatment modality is
going to be most effective for a particular individual. (presymptomatic diagnosis, prevention and
personalized medication)
Food Allergy- The Gourmet’s Dilemma
Dr. Krishna Mohan. R DNB, DAA, MNAMS Pediatrician & Pediatric Allergist, Health Services, Kozhikode

FOOD ALLERGY- THE GOURMET’S DILEMMA
PED ALLERGICON 2015
e all enjoy eating our favourite foods, and for most of us the selection of
foods depends only on our own personal choices. But for a small minority
of people, food choices are restricted by immunological/non
immunological adverse reactions. Adverse reactions to foods can be true (immunologically
mediated) food allergy or non-immunological adverse reactions to foods like food poisoning,
food intolerance. A food allergy is an adverse health effect arising from a specific immune
response that occurs reproducibly on exposure to a given food. Though food allergy has been
noted in the urbanized western world for sometime, now a days it is becoming common all
round the world. On the basis of recent studies, food allergy is estimated to affect more than
1% to 2% and less than 10% of the population.1
Although more than 170 foods have been
identified as triggers of food allergy, those causing most of the significant allergic reactions
include milk, egg, peanut, tree nuts, fish, shellfish, wheat, soy, and seeds.2,3
Pathogenesis:
Food allergy is predominantly caused by IgE-mediated and/or cell mediated mechanisms. On
exposure to certain allergens, in susceptible individuals,food-specific IgE antibodies are
formed that bind to receptors on mast cells, basophils, macrophages, and dendritic cells.
When food allergens penetrate mucosal barriers and reach cell-bound IgE antibodies,
mediators are released which produces symptoms of immediate hypersensitivity . These
activated mast cells and macrophages may release several cytokines that attract and activate
other cells, such as eosinophils and lymphocytes, leading to prolonged inflammation.
Symptoms:
IgE mediated food allergies can affect a variety of target organs: the skin, manifested as
urticaria and/or angioedema4; the gastrointestinal tract, causing vomiting, abdominal pain,
and/or diarrhea; the respiratory tract, as wheezing and/or allergic rhinitis; and the
cardiovascular system resulting in hypotension and/or cardiac arrythmias. An immediate,
systemic IgE-mediated reaction is anaphylaxis and can develop into a potentially fatal
allergic reaction.
Pollen-food allergy syndrome(oral allergy syndrome) is a form of localized IgE-mediated
allergy, usually to raw fruits or vegetables, and confined to the lips, mouth, and throat.6 OAS
most commonly affects patients who are allergic to specific pollens . Symptoms include
pruritus and/or tingling of the lips, tongue, roof of the mouth, and throat with or without
swelling. Systemic clinical reactions are rare.
Food-dependent, exercise-induced anaphylaxis should be considered when ingestion of
causal food or foods and temporally related exercise result in symptoms of anaphylaxis.
Symptoms only occur with ingestion of the causal food or foods proximate to exercise and
that ingestion of the food in the absence of exercise will not result in anaphylaxis.
With non-IgE mediated (or T-cell mediated) food allergies, patients can have
reactions to food, such as atopic dermatitis flare-ups or severe vomiting and diarrhea
progressing to shock on ingestion/exposure to the offending food.
W

FOOD ALLERGY- THE GOURMET’S DILEMMA
PED ALLERGICON 2015
Diagnosis:
A thorough history and physical examination is the most important part in the assessment .
The history is especially important in evaluating acute systemic, or anaphylactic, reactions.
The following facts should be established:
Food suspected of causing the reaction and the quantity ingested
Interval between ingestion and the development of symptoms
Types of symptoms
Whether other inciting factors, such as exercise, are necessary
Interval from the last reaction to the food.
A diet diary can be helpful in identifying a specific food as the causative agent.
Allergy skin prick tests and In Vitro laboratory tests are useful for demonstrating IgE
sensitization.Some fruits and vegetables may require prick-prick skin testing with fresh
produce because labile proteins are destroyed during commercial preparation. A negative skin
test result virtually excludes an IgE mediated form of food allergy5. Conversely, the majority
of children with positive skin test responses to a food do not react when the food is ingested.
So more definitive tests, such as quantitative IgE tests or food elimination and challenge, are
often necessary to establish a diagnosis of food allergy.
In vitro serum IgE testing quantifies the amount of IgE to the food-specific protein via an
enzymatic assay. Component-resolved diagnosis (CRD) identifies the patient’s sIgE reactivity to recombinant allergenic proteins rather than whole allergen. CRD is not routinely
recommended for the diagnosis of food allergy, but CRD might be useful in certain clinical
scenarios.7
The gold standard of food allergy testing is the double-blind, placebo controlled
challenge. This should only be performed in a monitored setting where a severe reaction can
be immediately treated. The patient is given increasing doses of the suspected food at
intervals during constant observation. Once the top dose is reached the patient is observed for
period of time, anywhere from 2.5 to 4 hours for allergic symptoms.
Treatment
The only proven therapy for food allergy is strict elimination of the offending food.
But complete elimination of common foods (milk, egg, soy, wheat, rice, chicken, fish,
peanut, nuts) is very difficult because of their widespread use in a variety of processed foods.
This requires extensive education and work on the part of the parents and any other caregiver,
including babysitters, grandparents, etc, and includes reading all food labels as well as taking
special care when ordering food in restaurants, notifying schools regarding snacks/ meals,
etc. Parents of younger children with food allergies should be trained to identify early allergic
symptoms and should have antihistamines and epinephrine available at all times.
Allergen specific therapies like oral, sublingual and epicutaneous immunotherapy and
allergen non-specific therapies like Chinese herbal formula FAHF-2 and omalizumab are

FOOD ALLERGY- THE GOURMET’S DILEMMA
PED ALLERGICON 2015
tried but more data on efficacy and safety are needed before these therapies become
mainstream.
Natural course of food allergy
This is a very common question many parents are worried about.When will he/she get rid of
this food allergy.? Most children “outgrow” milk and egg allergies, but 80-90% of children
with peanut, nut, or seafood allergy retains their allergy for life.
Prevention of food allergy: Facts:
Exclusive breast feeding for 4-6 months is beneficial.
Introduction of complementary foods after the age of 4-6 months according to
normal standard weaning practices and nutrition recommendations, for all children
irrespective of atopic heredity. No need to avoid or delay8.
No need to avoid allergenic foods during pregnancy or nursing
References:
1) Chafen JJ, Newberry SJ, Riedl MA, Bravata DM, Maglione M, Suttorp MJ, et al. Diagnosing and
managing common food allergies: a systematic review. JAMA 2010;303:1848-56.
2) Sicherer SH, Munoz-Furlong A, Godbold JH, Sampson HA. US prevalence of self-reported peanut,
tree nut, and sesame allergy: 11-year follow-up. J AllergyClin Immunol 2010;125:1322-6.
3) Gupta RS, Springston EE, Warrier MR, Smith B, Kumar R, Pongracic J, et al. The prevalence, severity,
and distribution of childhood food allergy in the United States. Pediatrics 2011;128:e9-17.
4) Burks W. Skin manifestations of food allergy. Pediatrics 2003;111:1617-24.
5) Sampson HA. Food allergy.Part 2: diag: and management. J Allergy Clin Immunol 1999;103:981-9.
6) Katelaris CH. Food allergy and oral allergy or pollen-food syndrome. Curr OpinAllergy Clin Immunol
2010;10:246-51. (IV).
7) Burks AW, Tang M, Sicherer S, Muraro A, Eigenmann PA, Ebisawa M, et al.ICON: food allergy. J
Allergy Clin Immunol 2012;129:906-20. (IV).
8) Greer FR, Sicherer SH, Burks AW. American Academy of Pediatrics Committee on Nutrition,
American Academy of Pediatrics Section on Allergy and Immunology. Effects of early nutritional
interventions on the development of atopic disease in infants and children: the role of maternal dietary
restriction, breastfeeding,timing of introduction of complementary foods, and hydrolyzed formulas.
Pediatrics 2008;121:183-91. (IV).

ANAPHYLAXIS- HOW ?, WHAT ?, WHEN ?
Dr. Muhammed Nishil, MD, FNB Pediatric Intensivist,
MIMS Kozhikode

ANAPHYLAXIS: HOW? WHAT? WHEN?
PED ALLERGICON 2015
INTRODUCTION
Anaphylaxis is a potentially fatal disorder that occurs when there is a sudden
release of potent biologically active mediators from mast cells and basophils, leading
to cutaneous, cardiovascular, and gastrointestinal symptoms.
ETIOLOGY
The causes of anaphylaxis in children are different for hospital and community settings.
Food allergy is the most common cause of anaphylaxis occurring outside the hospital.
Drugs are the most common in hospital set up; latex is also a particular problem for
children undergoing operations. Vaccines, biological agents, inhalants and stinging
insects are other causes for anaphylatic reactions in children. IgE independent
anaphylaxis are also reported with certain medications like NSAIDs.
SYMPTOMS AND SIGNS
Anaphylaxis may be mild and resolve spontaneously due to endogenous production of
compensatory mediators or it may be severe and progress within minutes to respiratory
or cardiovascular compromise and death.
Common symptoms and signs of anaphylaxis include the following:
Skin/mucous membrane :Generalised hives, Itching, flushing, swollen
-lips/tongue/uvula, periorbital odema &conjuctival swelling
Respiratory: Nasal congestion, throat tightness; chest tightness; shortness of breath
GIT: Nausea, vomiting, diarrhea & crampy abdominal pain
Cardiovascular : Syncope, incontinence, dizziness, tachycardia, hypotonia &
hypotension.
DIAGNOSIS
The diagnosis of anaphylaxis is based primarily upon clinical symptoms and signs, as
well as a detailed description of the acute episode, including antecedent activities and
events occurring within the preceding minutes to hours. Diagnosis of Anaphylaxis is
highly likely when any 1 of the following 3 criteria is fulfilled:
Criterion 1
Acute onset of illness within minutes to hours in the form of skin/mucosal involvement
and either respiratory compromise or reduced BP / end organ dysfunction.
Criterion 2
Exposure to a likely allergen for that patient and two or more of the following features;
skin/ mucosal involvement, respiratory compromise, reduced BP / symptoms and signs
and persistent GI symptoms and signs.
Criterion 3
Exposure to a known allergen for that patient and reduced BP.
In Infants, anaphylaxis can be hard to recognize because they cannot describe
symptoms. Other major risk factors are those have concomitant diseases like asthma,
ANAPHYLAXIS: HOW? WHAT? WHEN?
PED ALLERGICON 2015
chronic respiratory diseases, cardiovascular diseases, mastocytosis, allergic rhinitis,
eczema, depression, cognitive dysfunction and those who are on medications like
β-Adrenergic blockers and angiotensin-converting enzyme (ACE) inhibitors. Fever,
acute infection, emotional stress and exercise are certain cofactors that amplify
anaphylaxis.
Biphasic anaphylaxis is defined as a recurrence of symptoms that develops following
the apparent resolution of the initial anaphylactic episode with no additional exposure
to the trigger. It is reported in up to 11 percent of children with anaphylaxis. They
typically occur within 8 to 10 hours after resolution of the initial symptoms, although
recurrences up to 72 hours later have been reported. Protracted anaphylaxis is defined
as an anaphylactic reaction that lasts for hours, days, or even weeks in extreme cases.
Pitfalls in diagnosis are mainly due to reluctance to diagnose in the absence of
hypotension and in the absence of skin manifestations which are seen in 20% of
anaphylatic cases.
RISK FACTORS :
Asthma and cardiovascular disease are the most important risk factors for a poor
outcome from anaphylaxis. Concurrent administration of certain medications, such as
beta-adrenergic blockers, angiotensin-converting enzyme (ACE) inhibitors, and
alpha-adrenergic blockers may increase the likelihood of severe or fatal anaphylaxis.
DIFFERENTIAL DIAGNOSIS:
Acute generalised urticaria, angioedema, acute exacerbation of asthma, syncope, panic
attacks, acute life threatening events (ALTE), food poisoning, mastocytosis, flush
syndromes, shock and red man syndrome related with vancomycin are some of the
differential diagnosis to be considered in pediatric population.
LABORATORY TESTS
The clinical diagnosis of anaphylaxis can sometimes be supported by documentation
of elevated concentrations of serum or plasma total tryptase or plasma histamine.
Elevations of these mediators are transient, It is important to obtain blood samples for
measurement soon after the onset of symptoms.
Tryptase elevated in hypotensive anaphlaxis related with medications or insect
venoms, normal levels cannot refute the diagnosis. Histamine has better correlation
with signs and symptoms of anaphylaxis than tryptase and helpful in hospital settings,
because the peak levels seen within 5 to 15 minutes often declined to baseline due to
rapid metabolism.
MANAGEMENT
Prompt assessment and treatment are critical in anaphylaxis, as respiratory or cardiac
arrest and death can occur within minutes. The cornerstones of initial management are
removal of the inciting agent, call for help, intramusclar epinephrine, supine
positioning and elevation of lower extremities, supplemental oxygen and adequate IV

ANAPHYLAXIS: HOW? WHAT? WHEN?
PED ALLERGICON 2015
fluid resuscitation.
Initially, attention should focus on airway, breathing and circulation, as well as
adequacy of mentation. Skin should be examined carefully. Threshold for intubation
must be low and should be intubated whenever indications are there. In a minority of
cases, emergency cricothyroidotomy may be required. Intubation may be difficult in
individuals in whom edema distorts the upper airway anatomical landmarks, should be
managed by the most experienced clinician available. This may require immediate
collaboration between an emergency medicine specialist and an anesthesiologist,
otolaryngologist, or intensivist with training and experience in the management of the
difficult airway.
Intravenous access should be obtained in case fluid resuscitation is required. Massive
fluid shifts can occur rapidly in anaphylaxis due to increased vascular permeability.
Fluid resuscitation should be initiated immediately in patients who present with
orthostasis, hypotension, or incomplete response to intramuscular epinephrine. Normal
saline is preferred over other solutions.
PHARMACOLOGICAL TREATMENTS
Epinephrine is the drug of choice for anaphylaxis. It decreases mediators from
inflammatory cells, reverses obstruction to airflow in the respiratory tract and reverses
cardiovascular collapse. Intramusclar injection over mid-outer thigh is preferred, the
recommended dosage is 0.01 mg/kg.Sideeffects include mild transient pharmacological
effects such anxiety,restlessness, headache, palpitation,pallor and tremor.Serious
sideeffect such as arrhythmias, hypertension, intracranial hypertension and pulmonary
edema are seen with overdose, often after IV bolus doses.There is no absolute
contraindication for epinephrine and should be given in all severity of anaphylaxis.IV
epinephrine is indicated in those cases not responding to intramuscular injections and
fluid boluses,profound hypotension and in the presence of impending shock:IV
infusion is preferred under continuous ECG monitoring.
Glucagon is used in patients receiving beta blockers who are resistant to epinephrine.
Rapid administration of IV Glucagon can induce vomiting,so airway protection should
be taken during administration.
Other adjunctive agents such as Antihistamines may relieve itches and hives but
neither relieve airway obstruction,hypotension nor inhibit release of
mediators.Systemic review on randomized control trials doesn't support its role in
anaphylaxis.Glucocorticoids may prevent biphasic or protracted reactions.Its onset of
action takes several hours,so neither preferred in initial management of anaphylaxis nor
as a substitute of epinephrine.Broncodilators such as Salbutamol Nebulization can be
considered,especially in asthamatic cases.Inhaled epinephrine can be used for stridor
related to bronchospasm if not responding to IM epinephrine.
Refractory anaphylaxis as a result of profound vasodilation can be attributed to
saturation of adrenergic receptors.Use of nonadregenic vasopressors such as
vasopressin is advisable in such a situation.Methylene blue which is an inhibitor of
nitric oxide synthase can also be tried but should be cautious in those with pulmonary

ANAPHYLAXIS: HOW? WHAT? WHEN?
PED ALLERGICON 2015
hypertension and G-6PD deficiency.
Treatment errors in the management of anaphylaxis are often due to hesitancy or
delay in administration of epinephrine.Overrelying on adjunctive therapies are also
contributory factors.Regarding observation period,most biphasic reactions occur
within first 4 -6 hours after the initial onset of symptoms.So a reasonable observation
period of 6 hours is acceptable.Long period of observation is required for those
presented with severe symptoms,who received multiple doses of epinephrine,those
with high risk factors and those who lack immediate access to medical
attention.Discharge care includes anaphylaxis emergency action plan that lists its
common symptoms and signs and contains information about prompt recognition of
anaphylaxis.Ideally,patients should be supplied with epinephrine auto
injectors,unfortunately,its not widely available in India. The pnemonic "SAFE" was
developed to remind clinicians about the basic action steps. for patients with
anaphylaxis.These steps are : Seek support, Allergen identification and
avoidance,Followup for specialty care and Epinephrine for emergencies.
In conclusion,prompt recognition and treatment are critical.Epinephrine is a lifesaving
and the drug of choice in anaphylaxis of any severity.
References
Lieberman P, Camargo CA Jr, Bohlke K, et al. Epidemiology of anaphylaxis: findings of the American
College of Allergy, Asthma and Immunology Epidemiology of Anaphylaxis Working Group. Ann
Allergy Asthma Immunol 2006; 97:596.
2. Decker WW, Campbell RL, Manivannan V, et al. The etiology and incidence of anaphylaxis in
Rochester, Minnesota: a report from the Rochester Epidemiology Project. J Allergy Clin Immunol 2008;
122:1161.
3. Lin RY, Anderson AS, Shah SN, Nurruzzaman F. Increasing anaphylaxis hospitalizations in the first 2
decades of life: New York State, 1990 -2006. Ann Allergy Asthma Immunol 2008; 101:387.
4. Poulos LM, Waters AM, Correll PK, et al. Trends in hospitalizations for anaphylaxis, angioedema, and
urticaria in Australia, 1993-1994 to 2004-2005. J Allergy Clin Immunol 2007; 120:878.
5. Sheikh A, Hippisley-Cox J, Newton J, Fenty J. Trends in national incidence, lifetime prevalence and
adrenaline prescribing for anaphylaxis in England. J R Soc Med 2008; 101:139.
6. Liew WK, Williamson E, Tang ML. Anaphylaxis fatalities and admissions in Australia. J Allergy Clin
Immunol 2009; 123:434.
7. Wood RA, Camargo CA Jr, Lieberman P, et al. Anaphylaxis in America: the prevalence and
characteristics of anaphylaxis in the United States. J Allergy Clin Immunol 2014; 133:461.
8. Ewan PW, Dugué P, Mirakian R, et al. BSACI guidelines for the investigation of suspected
anaphylaxis during general anaesthesia. Clin Exp Allergy 2010; 40:15.
9. Chacko T, Ledford D. Peri-anesthetic anaphylaxis. Immunol Allergy Clin North Am 2007; 27:213.
10. Brown SG, Mullins RJ, Gold MS. Anaphylaxis: diagnosis and management. Med J Aust 2006;
185:283.
11. Muraro A, Roberts G, Clark A, et al. The management of anaphylaxis in childhood: position paper
of the European academy of allergology and clinical immunology. Allergy 2007; 62:857.
12. Muraro A, Roberts G, Worm M, et al. Anaphylaxis: Guidelines from the European Academy of
Allergy and Clinical Immunology (in preparation). Allergy 2014.

ANAPHYLAXIS: HOW? WHAT? WHEN?
PED ALLERGICON 2015
13. Sampson HA, Mendelson L, Rosen JP. Fatal and near-fatal anaphylactic reactions to food in children
and adolescents. N Engl J Med 1992; 327:380.
14. Bock SA, Muñoz-Furlong A, Sampson HA. Fatalities due to anaphylactic reactions to foods. J
Allergy Clin Immunol 2001; 107:191.
15. Bock SA, Muñoz-Furlong A, Sampson HA. Further fatalities caused by anaphylactic reactions to
food, 2001-2006. J Allergy Clin Immunol 2007; 119:1016.
16. Pumphrey R. Anaphylaxis: can we tell who is at risk of a fatal reaction? Curr Opin Allergy Clin
Immunol 2004; 4:285.
17. The American Academy of Allergy, Asthma and Immunology. www.aaaai.org
18. The Be S.A.F.E. campaign is discussed on the website of the American College of Allergy, Asthma
and Immunology.
http://www.acaai.org/allergist/allergies/Anaphylaxis/Pages/safe-awareness-anaphylaxis.aspx

Dr V. Sujith Nayanar MBBS, MD(AIIMS), DNB, FRCS, FICO Cornea Fellow –AIIMS; New Delhi Cornea Fellow- Helsinki University Cornea and Anterior Segment Surgeon Vasan Eye Care Hospital
Allergic Disorders of Eye In
Paediatric Age Group

ALLERGIC DISORDERS OF EYE IN PEDIATRIC AGE GROUP
PED ALLERGICON 2015
he ocular surface comprises of the conjunctiva, cornea and meibomian
glands.Lacrimal gland and tear fluid plays an adjunctive key role in the ocular
surface dynamics.Ocular allergy includes a spectrum of disorders with an
overlapping symptomatology and progressive severity; these disorders include Seasonal
Allergic Conjunctivitis(SAC) and Perennial Allergic Conjunctivitis(PAC), Atopic
Keratoconjunctivitis (AKC) and Vernal Keratoconjunctivitis(VKC). SAC and PAC are
collectively most common forms of ocular allergy. Though they are not directly vision
threatening, the symptoms they cause have significant impact on the productivity and quality
of life. VKC has got vision threatening complications if not managed properly.
The triggers for allergic response include pollens, animal dander, mould spores and
other environmental allergens. It involves an acute phase triggered by mast cell degranulation
and a late phase involving allergic inflammation.
Seasonal and Perennial Allergic Conjunctivitis
Both are largely IgE mediated immediate hypersensitivity reactions. The allergen is
airborne.From the tear film it interacts with conjunctival mast cells that bear allergen specific
IgE antibodies. Degranulation of mast cellsrelease histamine and other inflammatory
mediators.
The patient presents with redness,itching,chemosis,mucoid discharge, eye lid swelling etc.
Often they have associated rhinitis and asthma. Contact lens usage and pre-existing dry eye
potentiate the symptoms.
Fig1: Severe form of conjunctivitis with chemosis
T

ALLERGIC DISORDERS OF EYE IN PEDIATRIC AGE GROUP
PED ALLERGICON 2015
Fig 2: Papillary response on the palpebral conjunctiva
General principles in the management include:
1. Avoid triggering agents
2. Goggles as physical barrier
3. Cold compresses to counter itching sensation
4. Copious use of artificial tears to dilute the allergen coming into contact with ocular
surface
5. Topical antihistamines and mast cell stabilisers(olopatadine, cromolyn sodium)
6. Topical steroids(fluoromethalone,loteprednol,dexamethasone) in quick tapering dose
in severe case
7. Topical vasoconstrictors for control of symptoms for short duration.
8. Systemic antihistamines(in severe cases)
Treatment of hypersensitivityreactions requires identifying and discontinuing the offending
agent. Sometimes if the culprit is one among many medicines then re-challenge may be
needed which should be avoided in cases with systemic anaphylaxis. Adjunctive therapy may
include cold compresses,topical antihistamines, topical mast cell stabilisers and topical
NSAIDS. In severe cases mild steroids for a shorter course may also be needed for achieving
faster control of the situation.Artificial tears are beneficial in diluting and flushing away
allergens and other inflammatory mediators presents on the ocular surface. Topical mast cell
stabilisers such as cromolyn sodium and lodoxamidetromethamine may be useful for treating
seasonal allergic conjunctivitis but their primary role is prophylactic. It requires at least 7
days treatment for its effect and hence it is not useful in acute stage Topical NSAIDS may be
useful as an adjunctive but has to be used with caution as it can lead to sterile corneal
perforations if overused,. Topical corticosteroids have to be used in severe cases for short
period.
Vernal Keratoconjunctivitis
This is usually a seasonally recurring bilateral inflammation of the cornea and conjunctiva,
predominantly in male children. They often give family history of atopy. It is often seen year

ALLERGIC DISORDERS OF EYE IN PEDIATRIC AGE GROUP
PED ALLERGICON 2015
–round in tropical countries. The pathogenesis involves both Type I and IV hypersensitivity
reactions.
Main symptoms consist of excessive itching, blepharospasm, photophobia, blurred vision and
copious ropy discharge .It may present as purely palpebral form or limbal form or involving
both. In the palpebral form, the inflammation is predominantly located in the palpebral
conjunctiva. The major sign include appearance of papillary hypertrophy mainly on the upper
palpebral conjunctiva. Giant papillae and cobble stone appearances are also common.
In limbal form,the limbal area(where conjunctiva anatomically meets cornea) is
thickened,gelatinous with opalescent mounds and vascular injection. Characteristic
whitishdots calledHorner Trantas dots, which are macro-aggregates of degenerated eosinophil
and epithelial cells, may be visible at the limbal area.
Corneal changes include punctate epithelial erosions in superior and central cornea, superior
pannus, and sterile corneal ulcers(Sheild ulcers) . Vision threatening complications include
corneal scarring and predisposition of such eyes for conditions like Keratoconus
Fig 3:Cobble stone appearance of superior palpebral conjunctiva
Fig 4:Gelatinous limbal deposits

ALLERGIC DISORDERS OF EYE IN PEDIATRIC AGE GROUP
PED ALLERGICON 2015
Fig 5: Horner Trantas spots
Mild to moderatecases of VKC can be managed withtopical mast cell stabilizers and topical
antihistamines
Climatotherapy or relocation may be tried to avoid allergens.
Starting prophylactic treatment 2 weeks before anticipated season of exacerbation can be
tried. Year round mast cell stabiliser is recommended for chronic and recurrent cases. Severe
cases need topical steroids drops for faster and effective control of inflammation. Immuno-
modulatory treatment using tacrolimus eye ointment or cyclosporine eye drops is
recommended in severe chronic cases as steroid sparing agents to avoid steroid induced
complications like cataract and increased intra ocular pressure. Supratarsal injection of
dexamethasone or triamcinolone should be considered in patients with problems for frequent
medication. It acts as depot and gives longer symptom free period up to 3-6 months.
Close monitoring of intra ocular pressures are recommended in
such cases. In cases with corneal involvement, especially in those with shield ulcers, intense
topical steroid drops are required to prevent vision threatening complications like corneal
scarring. Frequent checking of vision is adviced in such cases as they are more prone to
Keratoconus, which is progressive ectatic disease of cornea. Protective glasses will help in
reducing exposure to allergens to some extent.
Atopic Dermatitis
Atopic dermatitis is a chronic condition in genetically susceptible individuals that usually
begin in infancyor childhood. The ocular involvement if present involves eyelid skin. The
pathogenesis of atopic dermatitis involves increased IgE hypersensitivity,increased histamine
release from mast cells and basophils and impaired cell mediated immunity.
Diagnostic criteria for atopic dermatitis include pruritus, lesions on the eyelid and other sites,
family historyof other atopic disorders, personal history of asthma, allergic rhinitis, nasal
polyps and aspirin hypersensitivity. There is increased incidence of Keratoconus as well as

ALLERGIC DISORDERS OF EYE IN PEDIATRIC AGE GROUP
PED ALLERGICON 2015
staphylococcal and herpes simplex infections. Periorbital hyperpigmentation, exaggerated
eyelid folds and chronic conjunctivitis may be associated with it. Skin lesions may be
erythematous rash or eczematoid dermatitis with lichenifiction or scaly patches based on
various age of presentation.
Atopic Keratoconjunctivitis may occur in patients with history of atopic dermatitis.
AKC is primarily a type IV reaction. AKC patients are older and present with year- round
symptoms. The papillae are small to medium sized and involve superior and inferior
palpebral conjunctiva. Chronic cases have sub epithelial fibrosis of conjunctiva and corneal
vascularisation and scarring.
The management principle are same as that of VKC. In addition treatment for associated
infections like staphylococcal etiology needs to be attended to. In minority of cases which
present with severe form needs systemic treatment including immune suppression with help
of internist. Topical tacrolimus is found to be beneficial in these cases for long term
application.
Contact dermatoblepahiritis or blepharoconjunctivitis
Topical application of ophthalmic medication, cosmetics or environmental substances can
occasionally trigger a local allergic reaction. This may occur acutely as anaphylactic reaction
resulting from type I IgE mediated reaction or which begin 24 -72 hrs later as delayed
hypersensitivity reaction(typeIV).
Type I reaction often starts with acute onset redness, itching, lid swelling, chemosis,
conjunctival redness etc within minutes of exposure to allergen. In certain cases,signs of
systemic anaphylaxis may also be seen.
Delayed hypersensitivity reaction begins 24-72hrs after the exposure. Normally sensitization
by previous exposure to the offending agent is seen in such cases.
An acute eczema with erythema, leathery thickening and scaling of the lid develop. Sequelae
include hyperpigmentation, and dermal scarring. In blepharoconjunctivitis, mucoiddischarge,
and papillary conjunctivitis may also develop.

ALLERGIC DISORDERS OF EYE IN PEDIATRIC AGE GROUP
PED ALLERGICON 2015
Fig 6: Various stages of allergic dermato-blepharo conjunctivitis
Primary aim in management is to avoid allergens. Moisturising skin lotions may be used for
skin hydration. Mild corticosteroids cream for short duration may be helpful. Long term
application results in thinning of skin. Topical tacrolimus ointment is effective and useful, if
longer duration treatment is required.
The prevalence of allergic diseases on the rise due to increasing pollution. The exact
prevalence of ocular allergy is not available almost all studies rarely makes a clear distinction
between allergic rhinitis and allergic conjunctivitis. Theimpact of allergies on the quality of
life and on scholastic achievment need not be emphasised confirming the need for effective
pediatric therapies. Treatment compliance is another major factor as chronic nature of
treatment leads to doctor shopping and poor adherance to instructions especilly those
pertaining to prophylactic treatment. New treatments should be focussing on more chronic
forms of allergic conjunctivitis and provide treatment for those who are more likely to have a
more severe form of the disease and less likely to experience significant relief of the signs
and symptoms of disease from existing therapies.

ATOPIC DERMATITIS – A PRIMER
Dr. Rakhesh. SV, MD Senior Consultant Dermatologist, MIMS Hospital, Kozhikode
ATOPIC DERMATITIS – A PRIMER
PED ALLERGICON 2015
Introduction
Atopic Dermatitis is a severely pruritic chronic or chronically relapsing skin disease
that manifests for the first time in infancy or childhood. AD is often the first step in the
emergence of an allergic triad that is often referred to as the “atopic march.” This refers to a
progression of atopic disease that is believed to start with atopic dermatitis and subsequently
progresses to asthma and allergic rhinitis.
Epidemiology
The prevelance of AD in most developed countries have been reported as 15- 20%.
Over the past 30 yrs the prevelance have been increasing worldwide. Incidence of AD in an
Indian study was reported as 0.38% but in a recent study was reported as 27%. Changes in
environmental pollutants, breastfeeding pattern, increased awareness, and urbanization and
better case detection techniques are some of the reasons cited for this change
Etiopathogenesis
The disease arises as a result of a complex interplay between various genetic,
immunological and environmental factors.
Atopic dermatitis, undeniably, has a hereditary basis. . A child has a twofold
increased risk of developing AD if one parent has the disease and a threefold increased risk if
both parents are affected. Recently, it has been shown that . It has been shown that two
independent loss-of-function genetic variants (R510X and 2282de14) in the gene encoding
filaggrin are very strong predisposing factors for atopic dermatitis. Filaggrin is a key protein
that facilitates terminal differentiation of the epidermis and formation of the skin barrier
The environmental factors include (a) physical factors like sweating, climate, warm
surroundings, detergents and soap, synthetic or woollen fabrics, cigarette smoke, (b)
psychological factors, (c) certain food items (d) allergens such as house dust mite, animal
hair, pollen, plants and others such as Staphylococcus aureus .
Immunological abnormalities like excessive formation of IgE with a predisposition to
anaphylactic sensitivity, some decrease in susceptibility to delayed hypersensitivity,
abnormalities in the expression of surface molecules in antigen presenting cells and
dysregulation of cytokine mediators are often noted. The elevated IgE response and

ATOPIC DERMATITIS – A PRIMER
PED ALLERGICON 2015
eosinophilia observed in AD patients may reflect increased response of of type-2 T helper
(Th2) cytokines with a concomitant decrease in interferon –gamma (IFN-gamma) production
Clinical features
AD can be divided into 3 arbitrary phases.
i. The infantile phase (birth to two years) is characterized by intensely
pruritic erythematous papules and vesicles typically beginning on the
cheeks, forehead and scalp (fig. 1). By 8-10 months, the extensor
surfaces of arms and legs show dermatitis (fig. 2), probably due to the
friction from crawling. The diaper area is typically spared in infantile
AD, which helps to differentiate AD from infantile seborrhoeic
dermatitis.
ii. The childhood phase (two years to puberty) is characterized by
lichenified papules and plaques involving the major flexures (fig. 3)
although “inverse” patterns are also noted in some.
iii. The adult phase starts from pubery and morphologically varies from
erythematous papules and plaques to large lichenfied plaques involving
the flexures, face and neck, the upper arms and back and dorsa of
hands and feet.
Figures 1. Dermatitis involving the face in the early infantile phase

ATOPIC DERMATITIS – A PRIMER
PED ALLERGICON 2015
Figure 2. Typical distribution of dermatitis involving the extensor aspect of limbs in the later
part of infantile phase
Figure 3. Typical Flexural involvement in the childhood phase of AD
Diagnosis
The diagnosis of AD is made clinically and is based on historical features,
morphology and distribution of skin lesions, and associated clinical signs. There is no
laboratory “gold standard “for the diagnosis of AD.
One of the earliest and most recognized sets of diagnostic criteria is the 1980 Hanifin
and Rajka criteria incorporating three major and 23 minor criteria. While comprehensive and
useful for clinical trials, it is unwieldy for use in clinical practice. The UK working Party

ATOPIC DERMATITIS – A PRIMER
PED ALLERGICON 2015
distilled the Hanifin and Rajka criteria down to a core set that is suitable for epidemiological/
population based and that can be used by non-dermatologists. These consist of 1 mandatory
and 5 major criteria and do not require any laboratory testing. A 2003 consensus conference
spearheaded by the American Academy of Dermatology suggested revised Hanifin and Rajka
criteria that are more streamlined and additionally applicable to the full range of ages affected
and is well suited for use in the clinical setting ( Table 1)
Table 1: Features to be considered in the diagnosis of patients with atopic dermatitis
ESSENTIAL FEATURES—Must be present:
Pruritus
Eczema (acute, subacute, chronic)
o Typical morphology and age-specific patterns*
o Chronic or relapsing history
*Patterns include:
1. Facial, neck, and extensor involvement in infants and children
2. Current or previous flexural lesions in any age group
3. Sparing of the groin and axillary regions
IMPORTANT FEATURES—Seen in most cases, adding support to the diagnosis:
Early age of onset
Atopy
o Personal and/or family history
o Immunoglobulin E reactivity
Xerosis
ASSOCIATED FEATURES—These clinical associations help to suggest the diagnosis of
atopic dermatitis but are too nonspecific to be used for defining or detecting atopic dermatitis
for research and epidemiologic studies:
Atypical vascular responses (eg, facial pallor, white dermographism, delayed blanch
response)
Keratosis pilaris/pityriasis alba/hyperlinear palms/ichthyosis
Ocular/periorbital changes

ATOPIC DERMATITIS – A PRIMER
PED ALLERGICON 2015
Other regional findings (eg. perioral changes/periauricular lesions)
EXCLUSIONARY CONDITIONS—It should be noted that a diagnosis of atopic dermatitis
depends on excluding conditions, such as:
Scabies
Seborrheic dermatitis
Contact dermatitis (irritant or allergic)
Ichthyoses
Cutaneous T-cell lymphoma
Psoriasis
Photosensitivity dermatoses
Immune deficiency diseases
Erythroderma of other causes
Differential diagnosis
In an infant seborrhoeic dermatis is the most common differential diagnosis and at
times, very difficult to differentiate between the two. The involvement of the axilla and
napkin area weighs in favour of a diagnosis of seborrhoeic dermatitis. Scabies in infants,
especially with secondary infection and subsequent secondary infection is another common
differential which ought not to be missed. A history of itching in family contacts, the shorter
duration of history, presence of inflamed papules on the axilla, genitalia and palms and soles
(in infants) helps one to make a diagnosis f scabies. The following conditions should be
suspected when a patient is having AD like eczema but is not responding to conventional
treatment: aggammaglobulinimia , anhidrotic ectodermal dysplasia, Hyper IgE syndrome,
hypereosionphilic syndrome, Jung’s disease, cystic fibrosis, Nethertons syndrome, wishkott-
aldrich syndrome etc
Natural history and progression
Various studies have shown variable result s. Overall, the disease after its onset in
infancy, shows a stepwise reduction in severity over the next 10 -12 years and tends to clear
completely by 12- 115 yrs. Many individual however, relapse in adulthood in form of various
forms especially hand eczemas.

ATOPIC DERMATITIS – A PRIMER
PED ALLERGICON 2015
Management
` `AD requires a systematic, multipronged approach that incorportates, skin hydration,
topical glucocorticoids and identification and elimination of flare factors such as irritants,
allergens infection agents, and emotional stress. The treatment can be cantegorized into 1)
General measures and 2) specific measures
General measures
The physician should spent adequate time with the parents of the atopic child explaining
the nature of the disease, the course of the disease, the realistic goals of the therapy, the
common triggers and their avoidance. Explanation and education should also be given
regarding the applications of topical preparations and compresses
Avoid extremes of temperatures
Avoid contact with woollen apparels
Avoidance of heavy furnishing and carpets at home, avoiding furry toy to be advised
Avoid keeping pets at home
Infants and young children are more likely to have food allergies but dietary advice
should be done with caution unless compelling evidence regarding food allergy is
present
Regular bathing with luke warm water and moisturiser soaps/ syndet bars and
followed immediately by application of emollients is beneficial; Avoid addition of
antiseptic solution (“detttol”) to the baths
Emollients should be applied within 3 minutes after bath to retain hydration
Wet compresses of plain tepid water or normal saline when applied on oozing skin
remove debris and cool inflamed skin and are useful for severe, exudative lesions.
Wet dressings are especially useful in infants and children with severe atopic
dermatitis. A wet dressing is applied directly to the skin and left in place for several
hours following application of a cream or an ointment. A double layer of either
gauzes, wraps, towels or stockinettes or cotton pajamas are placed on the patient over
the affected areas, the inner layer being wet (moistened with warm water) and the
second being dry . This method can provide good symptomatic relief
Specific Measures
This includes appropriate therapy according to the severity of the disease and extent of
involvement

ATOPIC DERMATITIS – A PRIMER
PED ALLERGICON 2015
Topical therapy
Topical corticosteroids are the mainstay of treatment for AD and can be used safely if
certain precautions are taken. The choice of different potencies of topical corticosteroids will
depend on the status, site and extent of eczema. The risks and benefits of the treatment should
be explained to the parents. One percent hydrocortisone ointment is adequate for most infants
with mild to moderate eczema and should be used on the face. New topical steroids which
can be effective even when applied once a day are relatively safe e.g., desonide,
prednicarbate, fluticasone propionate and mometasone furoate. A high potency corticosteroid
can be used for a short period to control acute flares of the disease. Dry, lichenified AD may
require a mid potency steroid for 2-3 weeks such as betamethasone dipropionate ointment
0.025% twice a day. If there is superadded bacterial or fungal infection, a topical
steroid/antibiotic or steroid/antifungal preparation should be used. Adverse effects of topical
corticosteroids include atrophy, depigmentation, steroid acne, telangiactesia and rarely
suppression of the hypothalamic-pituitary-adrenal axis. Patient fears of side effects associated
with the use of topical corticosteroids for AD should be recognized and addressed to improve
adherence and avoid undertreatment.
Topical Calcineurin Inhibitors (TCI): Tacrolimus and Pimecrolimus are the new kids in
the block and is currently recommended only as second line agents for short term and
intermittent treatment of AD. Clinical situations in which topical calcineurin inhibitors may
be preferable to topical steroids include a) Recalcitrance to steroids b) Sensitive areas (eg,
face, anogenital, skin folds) c) Steroid-induced atrophy d) Long-term uninterrupted topical
steroid use. Recent recommendation of the American Academy of Dermatology on TCI
include
TCI are recommended for use on actively affected areas as a steroid-sparing
agent for the treatment of AD.
For patients with AD<2 years of age with mild to severe disease, off-label use
of 0.03% tacrolimus or 1% pimecrolimus ointment can be recommended
Patients with AD should be counseled about the possibility of burnsing
sensation and pruritus when TCI are applied on inflamed skin
The concomitant use of a topical corticosteroid with a TCI may be
recommended for the treatment of AD
Clinicians should be aware of the black-box warning on the use of TCI for
patients with AD and discuss as warranted.
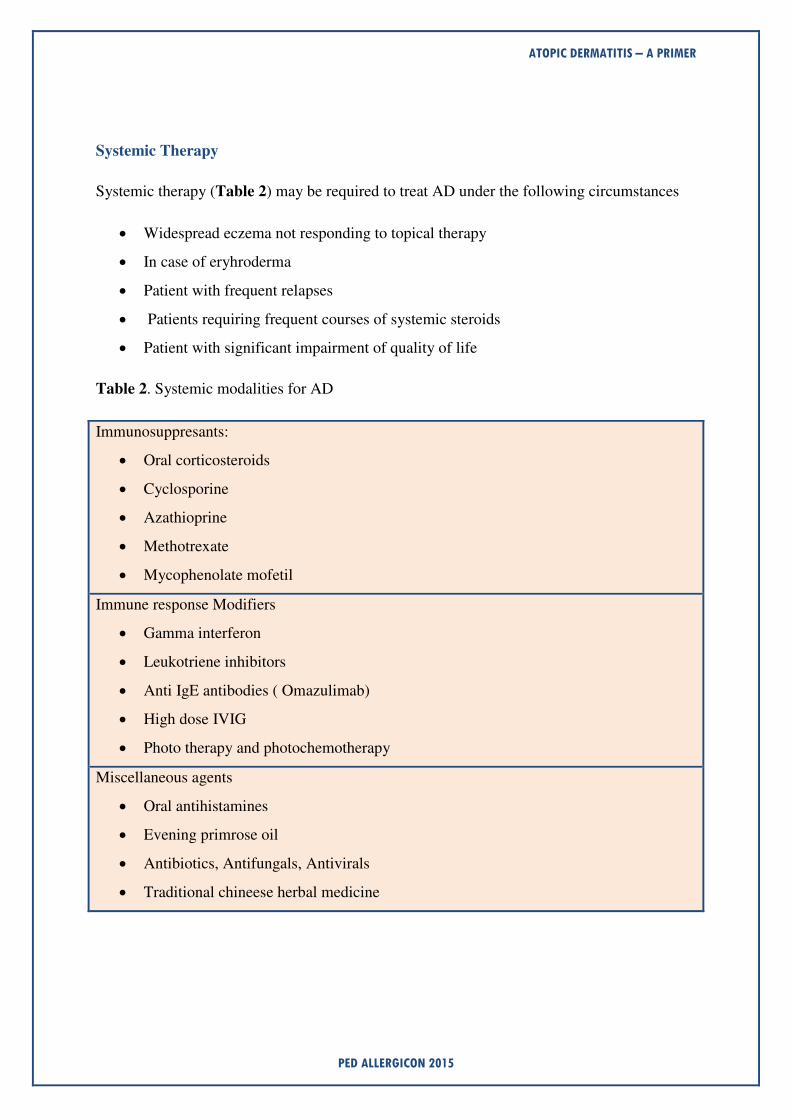
ATOPIC DERMATITIS – A PRIMER
PED ALLERGICON 2015
Systemic Therapy
Systemic therapy (Table 2) may be required to treat AD under the following circumstances
Widespread eczema not responding to topical therapy
In case of eryhroderma
Patient with frequent relapses
Patients requiring frequent courses of systemic steroids
Patient with significant impairment of quality of life
Table 2. Systemic modalities for AD
Immunosuppresants:
Oral corticosteroids
Cyclosporine
Azathioprine
Methotrexate
Mycophenolate mofetil
Immune response Modifiers
Gamma interferon
Leukotriene inhibitors
Anti IgE antibodies ( Omazulimab)
High dose IVIG
Photo therapy and photochemotherapy
Miscellaneous agents
Oral antihistamines
Evening primrose oil
Antibiotics, Antifungals, Antivirals
Traditional chineese herbal medicine

ATOPIC DERMATITIS – A PRIMER
PED ALLERGICON 2015
Systemic steroids should be avoided if possible for the treatment for AD. Their use
should be exclusively reserved for acute severe exacerbations and as a short term bridge
therapy to other systemic, steroid- sparing therapy.
Explaining the condition and its natural history to the parents of children with AD and
their proper counselling form the cornerstones of management of AD. Among the plethora of
treatment options, topical steroids, emollients and oral sedative antihistamines with systemic
antibiotics when appropriate remain as mainstay of therapeutic modalities. The TCI’s (
tacrolimus and pimecrolimus, the newer additions to the armamentarium have to stand the
test of time.

Non-pharmacological
Management of Pediatric Allergic Disorders
Dr. Parin .N. Parmar
MD , DAA, CRM Pediatric Allergy- Immunology Consultant, Rajkot, Gujarat

NON PHARMACOLOGICAL MANAGEMENT OF OF PEDIATRIC ALLERGIC DISORDERS
PED ALLERGICON 2015
ediatric allergic disorders are on the rise, both in India as well as globally. Awareness
about allergy and expertise to diagnose and manage allergic disorders are also
increasing in India [1]. With allergen avoidance measures and proper use of
medications, most of the pediatric allergic disorders can be controlled effectively. However,
most of the pharmacological agents, except allergen specific immunotherapy, offer little help
to modify natural history of allergy. Recently there has been a lot of interest in evaluating
role of non-pharmacological measures for allergic disorders, which may help to reduce drug
requirements in children with chronic allergic disorders, such as allergic rhinitis, allergic
asthma, atopic dermatitis, chronic/recurrent urticaria/angioedema, food allergies, etc.
In this article, various non-pharmacological measures for different pediatric allergic disorders
have been described as per latest scientific evidence. Avoidance of allergens and non-specific
triggers could be also considered a “non-pharmacological measure”, which is beyond the scope of this article. Please note that by following strict definition of a “drug”, saline sprays, moisturizers, nutritional supplements and artificial tears might not be considered “non-
pharmacological”; I have included them in the article mostly because of their “benign” ingredients or easy availability of similar simple alternative measures or their ability to
reduce requirements of other “active” drug requirements.
Allergic Rhinosinusitis
1. Saline nasal spray or irrigation: Use of saline solutions as nasal sprays or irrigations is
found to be safe and effective in children with allergic rhinitis as well as non-allergic
or viral rhinitis [2, 3]. Irrigations use a larger volume of saline (200-400 mL) to rinse
nasal cavities. However, sprays instil much smaller volumes of saline into nose and
yet they are equally or more effective than irrigations [3]. Regular use of nasal saline
sprays helps to reduce most of the nose symptoms, improves quality of life and
reduces requirements of medications for allergic rhinitis. Use of isotonic saline is
preferred over hypertonic saline, as per available research till date [3]. A more or less
similar procedure has been described as Jala neti in Ayurveda which has shown
encouraging results in sinusitis and other sinonasal diseases [4, 5].
There are many mechanisms by which saline nasal sprays work. They can directly
“flush out” allergens, air pollutants, irritants and thick mucous, as well as
inflammatory mediators, which are responsible for inducing symptoms. One more
important function they serve is by improving mucociliary clearance, which also
makes them useful in chronic sinusitis in addition to allergic rhinitis.
No significant side effects have been reported, even with long term use. The fact that
they are very cost-effective adds very much value to their use in developing countries.
2. Steam inhalation: Inhalation of vapour of water (steam) or heated humidified air has
been found to be helpful in patients with chronic rhinosinusitis [6]. The warming of
P

NON PHARMACOLOGICAL MANAGEMENT OF OF PEDIATRIC ALLERGIC DISORDERS
PED ALLERGICON 2015
mucous membranes produces decongestant effect and humidification helps by
reducing dryness and decreasing nasal mucous viscosity [6]. Steam inhalation may
also possibly benefit patients with allergic rhinitis [7].
Inhalation of steam generated by boiling water in a bowl is a very easy-to-perform
and cost-effective method practised by many patients. Many sophisticated electric-
driven steamers are available commercially also.
Of course, it is very important to remember that steam inhalation may not be
acceptable to children and can cause adverse events, including severe scalds [8].
There are not many studies defining role of steam inhalation in allergic rhinitis in
children; methods, duration and frequency of steam inhalation also needs to be
scientifically evaluated before making recommending its use in clinical practice.
3. Nasal Breathing Exercise : Regular nasal breathing exercise is believed to improve
ventilation in sinuses and improve distribution of intranasal medications within nasal
cavity [9]. Regular nasal breathing exercise along with medications causes much more
improvement in symptoms of allergic rhinitis as compared to taking medications
alone [9]. A study suggests that regular practice of Bhramari Pranayama could be
beneficial in chronic rhinosinusitis in adults [5]. Role of breathing techniques and
breathing exercises in improving nasal physiology is an emerging field for research.
4. Relaxation methods: Psychological stress is an important trigger for allergic rhinitis.
Regular relaxation techniques including Yoga practices have potential to reduce
inflammatory responses in stressed individuals [10]. Relaxation strategies could be an
important consideration for children and adolescents where stress is a possible trigger.
Childhood Asthma
1. Yoga, Pranayama and breathing techniques : A large number of studies have been
done worldwide to assess various effects of breathing techniques and Yoga &
Pranayama on adults and children with asthma. Many of them have shown improved
lung function parameters, improved subjective well-being, improved quality of life,
increased exercise tolerance as well as reduction in daily medication requirements, in
adults as well as children [11,12,13, 14, 15]
It should be noted that “Yoga & Pranayama” is a very comprehensive term. Different studies may have used different methods; hence it is difficult to make a unified
recommendation for asthmatic children. Ancient literature suggests Anuloma-Viloma
and Kapalbhati pranayama to be useful for chronic respiratory disorders including
bronchial asthma, which is also supported by a few researchers [14].

NON PHARMACOLOGICAL MANAGEMENT OF OF PEDIATRIC ALLERGIC DISORDERS
PED ALLERGICON 2015
However, it is always advisable that children learn such practices under guidance of
qualified and experienced experts as adverse events, although mostly mild but also a
few serious ones, have been reported [16].
2. Weight reduction in obese children: Recent research suggests that both obesity and
asthma are linked in many ways, including diet factors, poor physical activity,
abnormal chest wall mechanics, life style factors, etc. Obese asthmatic children have
poor quality of life as compared to non-obese asthmatic children. A recent review
found that weight loss resulted in improvement in asthmatic patients, including
children, although the magnitude of improvement varied [17].
It would be a good practice to encourage obese asthmatic children to achieve their
desirable weight. It will help to improve their general health as well.
3. Stress reduction: In the 21st century, the stress is no longer limited to adults, it does
affect children significantly! Commonly stress in children originates from family
stress, education, or peer pressure. Stress can trigger abnormal immune functions and
inflammatory response; also can it cause multiple endocrinological changes. Both
acute and chronic stress have been linked to asthma in children and adolescents.
Stressful events increase probabilities of having new asthma attacks significantly, the
probability increases even more if the child is chronically stressed [18].
Stress in children is often underrecognized. Hence it would be good to educate the
parents about stress factor. If it is felt that stress is an important factor in life of an
asthmatic child, a professional consultation and stress reduction strategies would help.
4. Diet factors : Various diet & nutrition factors have been linked to worsening or
improvement of childhood asthma, but only a few have shown consistency. Vitamin
D supplementation has shown immunomodulating effects in many studies. Recently
there also has been focus on role of anti-oxidants in combating oxidative stress [19].
Various micronutrients such as vitamin C, vitamin E, selenium, copper, etc have role
in combating oxidative stress, but their exact importance in allergy-asthma and doses
for supplementation are not determined. Magnesium supplementation has also been
found to improve childhood asthma [20]. A study has shown children who consume
plenty of fresh fruits and green vegetables or Mediterranean diet (a diet rich in fresh
fruits, green vegetables, whole grains, nuts & legumes – a diet rich in antioxidants)
are less likely to develop allergies and asthma as compared to other children [21].

NON PHARMACOLOGICAL MANAGEMENT OF OF PEDIATRIC ALLERGIC DISORDERS
PED ALLERGICON 2015
5. Physical exercise : Many parents restrict physical activity and sports for their
asthmatic children because of fear of exercise-induced bronchospasm. In fact,
asthmatic children should be encouraged to perform regular physical activity. Regular
submaximal physical exercise for a few weeks can improve exercise tolerance, lung
function parameters and quality of life in asthmatic children [22].
Allergic skin disorders
1. Moisturizers or emollients: In children with atopic dermatitis, regular use of
moisturizers (emollients) reduces symptoms including itching and duration. More
importantly, emollients have been shown to reduce requirements of topical
corticosteroids [23]. Dry skin is a very common finding in atopic dermatitis and
epidermal barrier function is defective. Application of moisturizers immediately after
bathing is advised in order to improve moisture content of skin. Recently, coconut oil
and virgin olive oil have been shown to have both emollient and antibacterial effects
in adults with atopic dermatitis [24].
Emollients have been also used to relieve itching in urticaria, especially contact
urticaria.

NON PHARMACOLOGICAL MANAGEMENT OF OF PEDIATRIC ALLERGIC DISORDERS
PED ALLERGICON 2015
2. Dietary supplements: Vitamin D has a controversial relationship with atopic
dermatitis. Various studies have shown that both excess and lack of vitamin D are
associated with increased incidence of atopic dermatitis [25]. However, severity of
atopic dermatitis has been inversely proportional to serum vitamin D levels [26].
Vitamin D also has a role in chronic urticaria. Many patients with chronic/recurrent
“idiopathic” urticaria/angioedema have been shown have low serum 25-
hydroxyvitamin D levels and vitamin D supplementation has been shown to be
beneficial in up to 70% of the patients [27].
Many researchers have suggested possible role of probiotics in treatment of atopic
dermatitis, however, so far the results of different trials are inconclusive [28]. It is
possible that particular strains of probiotics could be beneficial for some atopic
children. But at present, it is difficult to recommend probiotic supplementation to all
atopic dermatitis children.
3. Stress factor: There are numerous studies linking aggravation of symptoms of atopic
dermatitis and urticaria by psychosocial stress. Some researchers have suggested a
strong connection between brain and skin, based on neuroendocrinology and
neuroimmunology concepts [29]. As with allergic respiratory disorders, stress factor
should be kept in mind while evaluating children with allergic skin disorders,
especially older children and adolescents.
Food allergy
Unfortunately, the best option for children with food allergies has been elimination of
the food they are allergic to from diet. Among non-pharmacological approaches,
probiotics supplementation [30] and Traditional Chinese Medicine [31] have shown
some hope for future.
Ocular allergies
Use of artificial tears and cold compresses are part of primary management of ocular
allergic disorders [32] but they must not substitute conventional management of
ocular allergies.
To conclude, non-pharmacological measures play an important role in reducing
symptoms, improving quality of life, and decreasing requirements of medicines in
many allergic disorders in children. Parental counselling and allergy education are
very important to utilize them effectively. It must be emphasized that most of non-
pharmacological measures “help” but do not “substitute” conventional medications; role of compliance is pivotal in management of most of pediatric allergic disorders.
Of course, there a lot of scope for research in this field.

NON PHARMACOLOGICAL MANAGEMENT OF OF PEDIATRIC ALLERGIC DISORDERS
PED ALLERGICON 2015
Acknowledgement: I sincerely thank Samarth S Gohil for providing photographs for the
article.
References:
1. Prasad R, Kumar R. Allergy situation in India: What is being done? Indian J Chest Dis Allied Sci 2013;
55: 7-8.
2. Chirico G, Quartarone G, Mallefet P. Nasal congestion in infants and children: a literature review on
efficacy and safety of non-pharmacological treatments. Minerva Pediatr 2014 Dec; 66(6): 549-57.
3. Hermelingmeier KE, Weber RK, Hellmich M, Heubach CP, Mosges R. Nasal irrigation as an
adjunctive treatment in allergic rhinitis: a systemic review and meta-analysis. Am J Rhinol Allergy 26,
e119-e125, 2012; doi: 10.2500/ajra.2012.26.3787
4. Rabago D, Zgierska A, Peppard P, Bamber A. The prescribing patterns of Wisconsin family physicians
surrounding saline nasal irrigation for upper respiratory conditions. WMJ. 2009 May; 108(3): 145-50.
5. Choudhary A, Chaudhary TS, Mishra R. Effect of Yoga intervention on chronic rhinosinusitis. Int J
Bioassays. 2012; 1(12): 214-6.
6. Chester AC. Chronic sinusitis. American Family Physician 53; 1996: 877-94.
7. Baroody FM, Assanasen P, Chung J, Nacleria RM. Hot, humid air partially inhibits the nasal response
to allergen provocation. Arch Otolaryngol Head Neck Surg. 2000; 126(6): 749-54. doi:
10.1001/archotol.126.6.749.
8. Baartmans M, Kerkhof E, Vloemans J, et al. Steam inhalation therapy: severe scalds as an adverse side
effect. Br J Gen Pract. 2012 Jul; 62(600): e473-7. doi: 10.3399/bjqp12X652337.
9. Nair S. Nasal Breathing Exercise and its effect on symptoms of allergic rhinitis. Indian J Otolaryngol
Head Neck Surg. 2012 Jun; 64(2): 172-6. doi: 10.1007/s12070-011-0243-5
10. Kiecolt-Glaser JK, Christian L, Preston H, et al. Stress, Inflammation, and Yoga Practice. Psychosom
Med. 2010 Feb; 72(2): 113. doi: 10.1097/PSY.0b013e3181cb9377.
11. Jain SC, Rai L, Valecha A, et al. Effect of yoga training on exercise tolerance in adolescents with
childhood asthma. Journal of Asthma. 1991; 28(6): 437-42.
12. Vedanthan PK, Kesavalu LN, Murthy KC, Duvall K, Hall M. Clinical study of Yoga techniques in
university students with asthma: a controlled study. Allergy and Asthma Proceedings. 1998 Jan-Feb;
19(1): 3-9.
13. Saxena T, Saxena M. The effect of various breathing exercises (Pranayama) in patients with bronchial
asthma of mild to moderate severity. Int J Yoga. 2009 Jan-Jun; 2(1): 22-25.
14. Aggarwal T, Khatri A, Siddiqui SS, et al. Pranayama has additive beneficial effects along with
medication in bronchial asthma patients. J Phys Pharm Adv. 2013; 3(12): 292-7.
15. Galantino ML, Galbavy R, Quinn L. Therapeutic effects of Yoga for children: a systematic review of
the literature. Pediatr Phys Ther 2008; 20: 66-80
16. Matsushita T, Oka T. A large-scale survey of adverse events experienced in Yoga classes.
Biopsychosoc Med 2015; 9: 9. doi:10.1186/s13030-015-0037-1.
17. Eneli IU, Skybo T, Camargo CA Jr. Weight loss and asthma: a systemic review. Thorax 2008; 63: 671-
6. doi: 10.1136/thx.2007.086470.
18. Sandberg S, Paton JY, Ahola S, et al. The role of acute and chronic stress in asthma attacks in children.
The Lancet. 2000 Sep; 356(9234): 982-7.
19. Ercan H, Birben E, Dizdar EA, et al. Oxidative stress and genetic and epidemiological determinants of
oxidant injury in childhood asthma. Journal of Allergy and Clinical Immunology. 2006 Nov; 118(5):
1097-104.
20. Gontijo-Amaral C, Ribeiro MAGO, Gontijo LSC, Condino-Neto A, Ribeiro JD. Oral magnesium
supplementation in asthmatic children: a double-blind randomized placebo-controlled trial. European
Journal of Clinical Nutrition. 2007; 61: 54-60.
21. Chatzi L, Apostolaki G, Bibakis I, et al. Protective effects of fruits, vegetables and the Mediterranean
diet on asthma and allergies among children in Crete. Thorax 2007; 62: 677-83. doi:
10.1136/thx.2006.069419.

NON PHARMACOLOGICAL MANAGEMENT OF OF PEDIATRIC ALLERGIC DISORDERS
PED ALLERGICON 2015
22. Basaran S, Guler-Uysal F, Ergen N, Seydaoglu G, Bingol-Karakoc G, Ufuk Altintas D. Effects of
physical exercise on quality of life, exercise capacity and pulmonary function in children with asthma.
Journal of Rehabilitation Medicine. 2006; 38(2): 130-5.
23. Lucky AW, Leach AD, Laskarzewski P, Wenck H. Use of an emollient as a steroid-sparing agent in the
treatment of mild to moderate atopic dermatitis in children. Pediatric Dermatology. 1997 Jul; 14(4):
321-4. doi: 10.1111/j.1525-1470.1997.tb00968.x.
24. Verallo-Rowell VM, Dillaque KM, Syah-Tjundawan BS. Novel antibacterial and emollient effects of
coconut and virgin olive oils in adult atopic dermatitis. Dermatitis. 2008 Nov-Dec; 19(6): 308-15.
25. Benson AA, Toh JA, Vernon A, Jariwala SP. The role of vitamin D in the immunopathogenesis of
allergic skin diseases. Allergy. 2012; 67: 296-301.
26. Peroni DG, Piacentini GL, Cametti E, Chinellato I, Boner AL. Correlation between serum 25-
hydroxyvitamin D levels and severity of atopic dermatitis in children. Br J Dermatol 2011; 164: 1078-
82.
27. Goetz DW. Idiopathic itch, rash, and urticaria/angioedema merit serum vitamin D evaluation: a
descriptive case series. The West Virginia Medical Journal 2011; 107(1): 14-20.
28. Van Der Aa LB, Heymans HSA, Van Aalderen WMC, Sprikkelman AB. Probiotics and prebiotics in
atopic dermatitis: review of theoretical background and clinical evidence. Pediatric Allergy and
Immunology 2010 Mar; 21(2p2): e355-e367. doi: 10.1111/j.1399-3038.2009.00915.x.
29. Arck PC, Slominski A, Theoharides TC, Peters EMJ, Paus R. Neuroimmunology of stress: skin takes
center stage. Journal of Investigative Dermatology 2006; 126: 1697-704. doi: 10.1038/sj.jid.5700104.
30. Kirjavainen PV, Apostolou E, Salminen SJ, Isolauri E. New aspects of probiotics – a novel approach
in the management of food allergy. Allergy 1999; 54: 909-15.
31. Wang J, Patil SP, Yang N, et al. Safety, tolerability, and immunological effects of a food allergy herbal
formula in food allergic individuals: a randomized, double-blinded, placebo-controlled, dose
escalation, phase 1 study. Annals of Allergy, Asthma & Immunology 2010 Jul; 105(1): 75-84.e1.
32. Bielory L. Update on ocular allergy management. Expert opinion on pharmacotherapy 2002 May; 3(5):
541-53. doi: 10.1517/14656566.3.5.541.

Palynology - For the Clinician
Dr.K.P.RAJESH MD, DNB, DAA, MRCP(UK) Consultant Physician & Respiratory Allergist PVS Hospital, Kozhikode
PALYNOLOGY-FOR THE CLINICIAN
PED ALLERGICON 2015
Allergy has been known for more than a century now, but patients have suffered due
to lack of knowledge about basic mechanisms involved in allergic diseases and poor
diagnostic procedures. The rapid development in the field of immunology is of direct
significance to allergy practitioners. Detailed information on indigenous pollen and fungal
allergens is very useful in diagnosis and management of allergic patients. As allergen
avoidance is the measure of choice for the treatment of allergies and asthma in particular, all
the possible allergens are required to be characterized bio-chemically and at molecular level.
Relationship of the allergens with pathogenesis of respiratory allergies and the increase in the
prevalence are clinically relevant. Molecular studies with reference with the cross reactive
allergens are important for the proper diagnosis and treatment of the allergy.
Respiratory allergy is prevalent among all populations with increasing trend all over the
world. The latter part of the 20th century has seen an increase in the prevalence of allergic
diseases, implicating changing environment and lifestyle as significant causes. With the
alarming increase in allergic disorders, such as allergic rhinitis, bronchial asthma and atopic
dermatitis covering as high as 30% of the population worldover, there is an increasing
interest in aerobiology. For effective diagnosis and management of these ailments, a detailed
information on the daily, seasonal and annual variations of various bioparticles is essential .
The term aerobiology was coined by F.C. Meier, Plant pathologist from US in 1930s.
Aerobiology is the science of airborne bioparticles such as pollen grains,mould spores,plant
particles,dermal appendages,leaf cuticles,insect debris,house dust mite,animal dander etc;
which are microscopic in size and are universally present in the environment, both indoor and
outdoors. Among all these, pollen and fungal spores are the most predominant allergens in
the air. Primary objective of aerobiological studies is to detect and monitor the occurrence
and their relative abundance in the environment. Pollen grains are the male reproductive
structures produced by flowering plants(angiosperms) and naked seeding
plants(gymnosperms). There are some airborne pollen grains and mold spores which come in
contact with mucosa of eyes, nose, oral cavity or skin and produce immediate or delayed
allergic symptoms. Hyde and Williams from Cardiff, England coined the term Palynology in
1944 for the science of pollen and spores. Aerobiology gained importance on account of its
applications in allergy and immunology. Some basic knowledge of aerobiology is absolutely
necessary for clinicians practising allergy.
Pollen grains as aeroallergen are well studied from across the world and are important cause
of pollinosis. Respiratory system is the direct target organ of airborne pollen taken in by
inhalation. This results in immediate hypersensitivity disorders, in genetically predisposed
individuals and late hypersensitivity in others causing clinical manifestations of allergic
rhinitis, allergic alveolitis, asthma, atopic dermatitis, etc. Bostock was the first to suspect
pollen as the cause of hayfever (allergic rhinitis) . Subsequent studies from all over the world
established pollen grains as the major causative agent for respiratory allergic disorderes.
Depending on the mode of their release from the anthers in flower and pollination
mechanism, plants are distinguished into anemophilous and entomophilous. Flowers of
anemophilus plants are small inconspicuous,least attractive,do not emit fragrance,pollens are
dry, light and produced in large numbers for easy carriage by wind and are the ones usually
allergenic and clinically relevant. On the other hand, flowers of entomophilous plants are
large,attractive, emit fragrance, pollens are sticky, produced in less numbers and get easily
stuck to insect body for pollination ;nectar is produced to attract insects.The quantity of

PALYNOLOGY-FOR THE CLINICIAN
PED ALLERGICON 2015
pollen in air depends on several factors, the most important being pollen production in the
individual species.
Allergists need to know the local pattern of pollination. Peltophorum Ferrugenium(Manja
vaka),casuarinasequisetafolia(kattadimaram),ProsopisJuliflora(Sheemakkarivelam),Mallotusp
hilipensus(kumkumapoove),Ricinuscommunis(aavanakku),Oreodoxa regia(bottle palm tree)
are some plants which are clinically relevant in Kerala.
Although pollen have been widely studied as aeroallergens throughout the world, far less is
known about the fungal aerosols, which are present in much higher concentration than the
pollen grains in air. The growth of microorganisms such as bacteria and fungi, pollen in and
around buildings serves as a source of indoor biopollution.
The fungi that produce spores and get airborne are called 'aerospores'. These are implicated
in the causation of allergic diseases and infections in immunocompromised patients. Fungal
spores are responsible for both perennial and seasonal symptoms. Allergenic fungi are
generally in the asexual phase and grow best in moist places. Common fungi are
alternaria,cladosporium,aspergillus, penicillium. Indoor mold count of 1000/m3 is suggestive
of mold contamination.They are established to cause Type I hypersensitive diseases with IgE
mediated response. The common symptoms of hypersensitivity are bronchial asthma, allergic
rhinitis and atopic dermatitis.
Pollen aeroallergens and effect of environmental changes:
The dispersion of pollen in massive abundance assures the success of wind pollination as well
as its human health effects including asthma, rhinitis, atopic dermatitis, etc. Pollen prevalence
(grains per cubic meter) at any point reflects (plant) source strength and location as well as
the dynamics of the intervening environment conditions such as climatic factors, pollution
and degree of exposure. The presence of pollen, profile of species, concentration, etc depends
on various climatic factors such as temperature, humidity, wind direction, sunshine, substrate
precipitation and other seasonal factors. Because of change in the climatic conditions, the
study of variations in the diurnal and seasonal prevalence becomes very important .
Low humidity and winds,sunlight , time of day will influence pollen counts.Eg Ragweed is a
seasonal pollen and it peaks in early morning hours.Rainfall has mixed effects. Pollen can get
washed out and destroyed or they can get fragmented releasing bioaerosols and increasing
allergenicity. Hydration can induce release of submicronic allergen bearing paricles from
pollen possibly explaining asthma epdemics following thunderstorms.
Monitoring airborne pollen allergens:
Knowledge about diurnal, seasonal and annual fluctuations in airborne pollen and
fungal spores in any geographical area is essential for effective diagnosis and treatment of
allergy.
The recognition of aeroallergens is divided into two phases: 1) Collection of material and 2)
Sample analysis .

PALYNOLOGY-FOR THE CLINICIAN
PED ALLERGICON 2015
Different methods used for pollen collection include:
1. Fall out on a fixed surface through gravitational force-- Gravimetric sampler; used
only in developing countries for pollen and fungal spores , does not give diurnal
variation and is dependent on wind velocity.
2. Impaction on a rapidly moving surface-- Rotorod Sampler; used to study both pollen
and fungal spore types on continuous basis.
3. Impaction through suction of air-
4. It records the atmospheric concentration of pollen grains, fungal spores, and other
biological particles as a function of time through morphological identification.
5. Filteration – a) Burkard seven day volumetric sampler is one of the most widely
used samplers to study diurnal or seasonal trends for pollen grains as well as fungal
spores all over the world.
b)Burkard portable (slide) sampler
6. Immunochemical assays-: Radioallergosorbent (RAST) / enzyme-linked
immunosorbent assay (ELISA) inhibition type and monoclonal two-site
radioimmunosurveys are used to express air concentrations in allergy units
For analysis of data following procedures are followed:
1. Microscopic enumeration of individual particles
2. Immunochemical assays for bulk reservoirs
Direct microscopy (slides): The particles/spores are identified based on their characteristics
such as shape, size and other morphological features . It is a most dependable way to identify
most of the pollen/fungal spores.
Immunoassay : RAST and ELISA based procedures are followed. One advantage in
immunoassay for airborne microorganisms is that the amount of materials needed is much
lower. The researcher is not limited to the original amount of the sample but can culture as
much material as is needed for the various identification tests. The limitations are that a
considerable experience is needed to identify particles by their morphology and to distinguish
them from debris, and labeled antibodies for only a few clinically important microorganisms
are readily available.
Clinical application of Aerobiological surveys:
Pollen causing allergy are quite variable in different locations .Hence it is important to
identify pollinosis causing species from every region, and prepare extracts from them for
diagnosis and immunotherapy for the benefit of allergy patients.
From Southern India, studies carried out revealed that Casuarina, Chenopod/Amaranth,
Cocos, Cyperaceae, Eucalyptus, Parthenium, Peltophorum, Poaceae and Spathodia are
dominant pollen types. Pollen calendars are very useful for clinicians as well as allergic
patients to establish chronological correlation between the concentration of pollen in air and
seasonal allergic symptoms.

PALYNOLOGY-FOR THE CLINICIAN
PED ALLERGICON 2015
From South India Cassia, Ageratum, Salvadora, Ricinus, Albizia lebbeck and Artemisia
scoparia have been reported as clinically important aeroallergens , Rao et al recorded
allergenicity to Parthenium hysterophorus pollen extracts in 34% of allergic rhinitis and 12%
bronchial asthma patients from Bangalore. Agashe and Soucenadin recorded high skin
reactivity to Casuarina equisetifolia in patients from Bangalore. In Trivandrum, maximum
skin reactivity was recorded to Mallotus phillipensis (12.1%), followed by Prosopis juliflora
(6.3%).
Cross-reactive allergens in clinical allergy practice:
Progress made in the field of allergen characterization by molecular biological techniques has
now revealed that sensitization against different allergen sources can be explained as cross-
reactivity of IgE antibodies with structurally and immunologically related components
epitopes present in these allergen sources. The similarities among allergens may facilitate
allergy diagnosis in clinical practice by using a few representative cross-reactive allergens to
determine the patient's IgE reactivity profile.
Cross reactive pollen allergens.
Lolium perenne has been found to be cross-reactive with Acacia, pineapple, Olea europaea,
Dactylis glomerata, Ligustrum vulgare, Cynodon dactylon and Pinus radiata .
Platanus acerifolia has been found to cross-react with Corylus avellana, Prunus persica,
Malus domestica, Arachis hypogaea, Zea mays, Cicer arietinum, Lactuca virosa, Musa spp.,
and Apium spp.
Pollen from Japanese cypress (Chamaecyparis obtusa) cross reacts with Japanese cedar
(Cryptomeria japonica) contributing to prolonged symptoms after the cedar pollen season in
March and the following cypress pollen season in April .
Ricinus communis, commonly grown in India for its oil and abundantly present in wasteland,
cross-reacts with Hevea brasiliensis, Mercurialis annua, Olea europaea, Betula,
Zygophyllum fabago, Putranjiva roxburghii, and Ricinus (seed) from geographically distinct
locations .
Areca catechu cross-reacts with Phoenix sylvestris, Cocos nucifera, Borassus flabelifer, as
reported from India .
Cynodon dactylons (common grass) cross-reacts with Pennisetum clandestinum,
Stenotaphrum secundatum, Eragrostis, Brassica napus, Olea europaea, Ligustrum vulgare,
and Lolium perenne .
Holoptelea integrifolia and Parietaria judaica belonging to the family Urticaceae are
geographically distantly located. H. integrifolia is an important pollen allergen of India cross
reacts with P. judaica, on the other hand, is a very dominant pollen allergen of the
Mediterranean region. H. integrifolia and P. judaica pollens share cross-reactive as well as
unique epitopes .

PALYNOLOGY-FOR THE CLINICIAN
PED ALLERGICON 2015
Allergen avoidance measures:
General Measures
1. Create awareness of the importance of palynology among general public, patients and
clinicians dealing in allergy.
2. Pollen calendar giving information on the predominant pollen allergens in different
months of the year can be publicised in the newspapers and television.
3. Allergenically significant plants in an area should be identified and their plantation
discouraged.
4. Ornamentals, insect/bird pollinated and medicinally important plants which can help
in controlling pollution, should be encouraged .
5. The existing allergenically significant trees need to be replaced with non-allergenic
trees in a phased manner.
6. On medical ground, citizens should have the right to cut or demand removal of allergy
causing trees in close vicinity but should replace it with some non-allergenic trees.
Patient Measures:
1. Avoid going outdoors on days when pollen count is high.
2. Close all windows in evening, when pollen generally settle down, to minimize their
concentration.
3. Air conditioning decreases indoor pollen counts.
4. Do not plant lot of trees and shrubs around your house
5. Take bath after coming from outdoors and use fresh cloths.
6. Eliminate weeds and grasses in your house compound.
7. Electronic/ electrostatic precipitator can be Installed
Sensitisation to particular pollens can be detected by the Allergists using skin prick tests or
specific IgE following a detailed history and physical examination ; and appropriate
avoidance measures, medications and specific immunotherapy could be suggested depending
on the clinical profile. Major allergens vary from place to place. It is important for clinicians
to select only those pollen antigens for skin testing which are prevalent in a particular area in
which the patient resides.
Future trends in allergy research:
The introduction of recombinant allergens has allowed better standardization of allergen
extracts and affords the opportunity for individualized tailor made treatment.
The use of short T cell peptides for immunotherapy has the potential to stimulate
"protective" Th1 and/or T regulatory responses whilst avoiding systemic side effects
associated with cross linking of IgE on mast cells and basophils which is the risk associated
with conventional whole allergen extracts.
Asthma and allergy is a "complex" genetic disorder caused by the interactions of multiple
interacting genes. In, addition, these disorders require the presence of appropriate
environmental triggers for their expression.Thus, gene based therapy could be effective
treatment of asthma and allergy in future.

THANK YOU...
FOR PRIVATE CIRCULATION ONLY
C IAP KOZHIKODE