mild traumatic brain injury in military service personnel ... traumatic brain injury in military...
TRANSCRIPT

1
Mild Traumatic Brain Injury in Military Service Personnel: Key
Issues and Considerations
Silviya Doneva PhD
Medical Advisory Committee (MAC)
prepared by
The Health of Veterans Research Team (HVRT)
30.03.2017
1. Purpose of the Review: This report on the health of military personnel considers mild traumatic brain
injury (mTBI) and in particular, the one related to blunt head trauma. It aims to set out the current picture of mTBI amongst military personnel, including its
definition and classification, prevalence rates, markers and possible long-term consequences, comorbidity with other disorders and approaches to treatment. Information has been drawn from the most current reports published by the UK
Ministry of Defence (MoD), the World Health Organization (WHO) Collaborating Centre Task Force on Mild Traumatic Brain Injury, as well as high-impact academic
research in the field, mainly making use of US and UK military data1. Furthermore, the present report also includes exclusive data on the number of mTBI cases among the UK military for the period between the 1 April 2008 and the 31 March
2016 that we received with permission from the Department of Defence Statistics at the MoD (discussed in Section 7d)).
Being the most controversial form of TBI in terms of its cause and nature, mTBI continues to raise ardent debates among researchers and clinicians. The review recognises the lack of universal agreement in the field, and thus it attempts to
incorporate as many of the different perspectives as possible. It should be noted that although in the past ‘concussion’ has been considered synonymous for mTBI,
the present review abstains from using this term to refer to mTBI, in accordance to more recent literature on the topic (1).
2. Definitions:
a) mTBI: Traumatic Brain Injury is a very common condition resulting in over 1 million cases being registered in UK emergency departments each year (2). The majority (80%
to 90%) are characterised as mild (1,3,4). More specifically, mTBI has been defined as ‘a traumatically induced physiological disruption of brain function’ (5)
(p. 86) that is characterised by at least one array of symptoms (See Section 3 for more detail). MTBI in military settings is believed to most often follow from a blunt force trauma to the head, in particular, blast injury secondary to improvised
explosive devices (6,7). In view of the large numbers of service personnel being
1 For completeness, this report also incorporates research, based on civilian data, as well
as data from other countries, such as Australia and Canada.

2
exposed to a blast during the recent conflicts in Iraq and Afghanistan, mTBI has been referred to as a ‘service-related mental disorder’ ((8), p. 1) and a ‘signature
war injury’ for those returning from these theatres of operation (9,10). Importantly, mTBI also occurs in non-combat situations such as during contact
sports activities and road accidents. For example, in civilians it is usually caused by falls and motor vehicle collisions (11,12). MTBI is also one of the most common sports-related injuries, and as a consequence has been extensively studied among
sportsmen (See Section 5 for details). Furthermore, this is where much of the guidance for best practice in managing mTBI comes from (See Section 8c)).
Finally, mTBI is normally considered relatively innocuous with its effects disappearing within minutes (1,13). As a consequence, many patients, diagnosed with the condition, are not taken to hospital nor are they encouraged to seek
medical help.
b) mTBI as an unexplained condition: According to Rona (6), the majority of mTBIs in military settings are caused by exposure to improvised explosive devices (IED). Explosives, however, are not
unique to the recent war conflicts. Instead, exposure to bombarding is believed to be one of the causes of the signature injury during the First World War known as
the ‘shell shock’ epidemic (6,14). Some other examples of similar conditions with unexplained aetiology and unclear diagnostic criteria, reported amongst military
personnel in past wars, are the ‘effort syndrome’ that emerged during the Second World War (15) and the 1991 Gulf War Syndrome (16).
Finally, there is no consensus regarding the definition of mTBI or what it entails, with some authors using concussion interchangeably with mTBI and some making a difference, which does not necessarily agree with the distinction that others have
made between the two terms (1). Furthermore, because of the diversity in symptoms, recovery rates, long-term effects and susceptibility to treatment within
the condition, some have proposed that mTBI should be subdivided into categories and viewed as a heterogeneous condition (1,17) (see Section 3).
c) Postconcussive symptoms: Several evidence-based reviews of the literature have suggested that symptoms
of mTBI usually resolve spontaneously within about 2 weeks (18–20). If unresolved within 3 months, however, these evolve into what is known as
persistent postconcussive symptoms (or postconcussional syndrome, PCS) (21–23). The WHO’s International Statistical Classification of Diseases and Health-Related Disorders 10th edition (ICD-10; (24))2 classifies postconcussional
syndrome under ‘Mental and behavioural disorders (F00-F99)’ and more specifically under ‘Personality and behavioural disorders due to brain disease,
damage and dysfunction (F07)’. PCS could be grouped into three categories: somatic (physical), psychological (emotional and behavioural) and cognitive (thinking). Please, refer to Table 1 for all possible symptoms in each category.
2 We refer to the ICD-10 manual as the latter is used by the MoD Specialist Mental Health
Services to diagnose and assess the mental health of service personnel (e.g., (25)).

3
Table1. Postconcussive symptoms, usually reported following mTBI. The displayed
information has been based on Bagalman (26), Thompson (20), Thompson, Scott &
Dubinsky (27) and Rona (6).
Symptom Type Expression
Somatic
Headache, dizziness, ringing in the ears, visual
disturbances, sensitivity to light and noise,
disturbed sleep, lethargy, fatigue.
Cognitive
Psychological
Confusion, problems with thinking, decision
making, memory, attention, concentration,
abstract reasoning, information processing.
Depression, anxiety, mood swings, irritability,
impulsivity, loss of interest, agitation,
relationship difficulties.
Furthermore, PCS are often referred to as ‘nonspecific’ as these are not strictly associated with mTBI. For example, these have sometimes been reported to occur
prior to mTBI (14), or have been detected to a similar extent in patients with mTBI and controls suffering from a trauma without a history of such an injury (28) also
see (29,30). Therefore, it has been argued that PCS could also stem from a variety of mental and physical health conditions such as potential exposure to depleted uranium (31) or acute stress response (32). Still, it is important to note that white
matter abnormalities have been detected in some mTBI patients, suggesting that one needs to be careful when making assumptions that PCS are purely
psychological. In fact, there is evidence that in certain cases mTBI can result in serious long-term effects (See Section 5).
3. Challenges to Classification:
TBI severity is classified according to single indicators such as the Glasgow Coma Scale (GCS), duration of post-traumatic amnesia (PTA), and duration of loss of
consciousness (LOC). For example, mTBI is traditionally diagnosed by at least one of the following: amnesia for less than 24 hours post-injury, loss of consciousness for 30 minutes or less, GCS score between 13 and 15, as well as confusion or
disorientation and some transient neurological abnormalities (e.g., focal signs, seizures; (14,27)). Importantly, however, research has shown that single
indicators may be influenced by factors, unrelated to TBI severity. For example, as described by Malec et al. (33) ‘systemic or psychologic shock as well as organ system failure and fractures associated with polytrauma can extend PTA and may
affect acute assessment of GCS and LOC’ (p. 1418). Therefore, the Mayo classification has been developed as a more reliable system that uses only
positive, objective evidence for categorisation, rather than on lack of information in the patient’s record. According to this classification, mTBI should be split into two subcategories – mild (probable) and symptomatic (possible; for the full
criteria of the Mayo classification please refer to Appendix 1). The latter division accounts for the heterogeneity of mTBI that has been acknowledged by many
academics and clinicians (e.g., (1,17,34)).

4
Finally, another factor that further complicates the diagnosis of mTBI in military
settings is that the latter is normally based on self-reporting of the injury in a retrospective (See (6,14) for a discussion). Furthermore, research has
demonstrated that the temporal gap between the accident and the sufferers’ self-report could vary considerably from research to research, and it could span between several months to several years (6,35).Thus, the latter raises questions
about the reliability of such diagnosis. This is so as delayed self-reporting is subject to memory distortions which could lead to erroneous reporting,
underreporting or exaggeration of the symptoms. Recently, researchers have started to recognise these problems and to encourage the use of contemporaneous data (14).
4. Neuroimaging and biochemical markers of mTBI:
As explained earlier, mTBI symptoms are often considered of a transient nature so that the patient is most often not referred to undergo neuroimaging or further examination (1). Moreover, mTBI symptoms are not always reliable indicators to
determine the patient’s recovery, as although they might look free of the initial symptoms, the condition might have resulted in a still undiagnosed neurological
damage (See Section 5 for more details). As discussed in the previous section, because of the considerable clinical heterogeneity within mTBI, advanced
neuroimaging and biochemical markers are needed to identify and correctly classify mTBI, as well as to make predictions about its course.
Neurological abnormalities associated with mTBI normally remain undetected by conventional Computed Tomography (CT) and Magnetic Resonance Imaging (MRI)
techniques (36). Thus, these have started to be discovered only recently with the use of newer imaging methods such as Diffusion Tensor Imaging3 (DTI; (37)). DTI relies on the principle that water diffuses differently in white matter depending on
its integrity, type of tissue, presence of barriers etc., which allows quantifying patterns of water diffusion with white matter damage (38). Research using the
technique has shown that the most typical abnormalities associated with mTBI are traumatic axonal injury (TAI; and especially diffuse axonal injury4), and vascular injury (1). Furthermore, the amount of discovered TAI has been found to be a
good predictor of the impairments following mTBI (7). Finally, there is also some evidence that fluid biomarkers of neuronal, axonal and astroglial5 pathology can
be used to diagnose mTBI (41). However, cerebrospinal fluid (CSF) markers are normally preferred over blood markers, as CSF ‘is in direct contact with the extracellular matrix in the brain, and its composition reflects biochemical changes
that occur in this organ’ ((41), p. 4).
3 Two other novel neuroimaging techniques to detect white matter pathology associated
with mTBI are Diffusion MRI and Susceptibility-Weighted Imaging (SWI; see (1,7) for more
details). 4 Diffuse axonal injury is a widespread damage to the white matter which can disrupt
communication between axons. Therefore, the most common clinical outcome following
diffuse axonal injury is cognitive impairment (39). 5 Astroglia are a collection of astrocytes, which are cells essential for brain homeostasis
and communication between neurons and other cells (40).

5
The possible long-term consequences of mTBI and their respective markers are discussed in the next section.
5. Possible long–term effects of mTBI:
Although ‘once thought to be trivial in terms of [its] consequences … there is now substantial evidence that [mTBI] can lead to a number of neuropathological, neurophysiological, and neurocognitive changes’ ((13), p. 310). Thus, in some
cases PCS have been discovered to last for years and lead to a permanent disability (42,43). Therefore, it is of vital importance to acknowledge the long-
term effects of the disorder. As mentioned earlier, because of being particularly spread among sportsmen, much of the research into mTBI comes from this population. For example, most of what is known about the long-term effects of
the condition has been derived exactly by studying sportsmen who have sustained an mTBI. Details of some of the most serious long-term consequences of the
condition are given below, as reported in the literature. a) Chronic Traumatic Encephalopathy (CTE) Chronic traumatic encephalopathy (CTE) was first identified in boxers who sustained a repetitive head injury and later in other athletes participating in
contact sports. The disorder is associated with progressive neurological deterioration, it usually starts in mid-life and develops years to decades following a recovery from the head injury (37,44). CTE has a varied clinical profile, however
several reports have suggested that it commences with behavioural changes such as significant irritability and aggression, memory loss, depression or apathy and
in some cases increased suicidality (37,44). Moreover, normally the next stage is marked by neurological changes such as parkinsonism, gait and speech abnormalities. Furthermore, according to several reports, in its late stage, CTE
may clinically resemble Alzheimer’s disease or dementia (37,45). A recent post-mortem cohort study of 64 athletes and 21 military veterans, who had a history
of mTBI, shed more light on the link between mTBI and CTE (37). The results revealed that 63% of the participants in this study were diagnosed with CTE. CTE was also found to be associated with a number of neurological abnormalities –
abnormally aggregated proteins, neurofibrillary tangles6 in the frontal neocortex, multifocal axonal varicosities7, axonal loss and hyperphosphorylated tau
pathology8 that varied depending on severity (37). Thus, despite considered harmless, repetitive mTBI can be extremely dangerous and in some cases lead to ‘severe and devastating long-term consequences’ ((37) p. 62). Still, as outlined
by Rosenfeld (50), more research on the topic is required to determine the nature of the risk factors contributing to the association between CTE and mTBI.
6 Neurofibrillary tangles in the front area of the brain are an accumulation of tau, a protein
which is a primary marker for Alzheimer’s disease and other neurodegenerative diseases
associated with abnormal clusters of protein tau (46,47). 7 Axonal varicosities are swellings which appear in along the length of an axon at the point
of injury (48). 8 Hyperphosphorylated tau pathology is when there is abnormal mitosis of tau, which can
result in neurofibrillary tangles and neurodegeneration (49).

6
b) Other neurodegenerative diseases Several studies have reported that mTBI may also increase the risk of other
neurodegenerative diseases such as Alzheimer’s and Parkinson’s disease, as well as speed the progression of parkinsonian signs in general (37,51,52). For instance,
in the study explained above, McKee (37) found that 16% of their mTBI patients had Lewy body disease9, while 11% had Alzheimer’s disease. Interesting insights can also be derived from a very recent study that focused on non-athlete civilians
that had a TBI with loss of consciousness (LOC; (51)). The research included data from three longitudinal studies with a combined sample of 7130 individuals and
examined the association between TBI and a number of late-life effects, such as dementia and Alzheimer’s disease, Parkinson’s disease, the progression of parkinsonian signs and mild cognitive impairment. For the purposes of the present
review, only the results relevant to mTBI are discussed. It was found that TBI sufferers with a LOC of 1 hour or less had an increased risk for developing Lewy
bodies10 in the frontal and temporal cortex of the brain. Moreover, this was also one of the types of TBI associated with the progression of parkinsonian signs. Finally, a large proportion (more than one third) of those who sustained a TBI with
a LOC of 1 hour or less acquired the injury early in life (when they were no older than 25 years), although the condition only produced long-term neuropathological
consequences in this group in more severe TBI cases (with a LOC longer than 1 hour).
c) Cognitive impairment In some cases mTBI can also lead to cognitive impairment, causing memory loss, executive dysfunction and the slowing of one’s information processing (39,54,55). Research has demonstrated an array of neurological abnormalities associated with
cognitive impairment in mTBI. For example, using diffusion MRI, Niogi et al. (56) examined the microstructural white matter integrity and connectivity of mTBI
patients and matched controls. Their results illustrated damage in the attentional and memory tracts of the brain which was associated with a deficit in the respective cognitive domain. Furthermore, Tremblay et al. (57) compared 15
former male university-level athletes who sustained an mTBI in early adulthood with 15 male control athletes with no history of head injury. Importantly, the
comparison took place 30 years after the last recorded mTBI, which allowed examining whether a relationship could be established between brain function abnormalities found in some asymptotic athletes at young age and cognitive
decline as they grow older. Tremblay et al. (57) discovered a number of anomalies in the mTBI group such as aberrant ventricle enlargement11, neurometabolic
imbalance and lastly, cortical thinning in the frontal, temporal and parietal lobes which also correlated with episodic memory12 decline in this group. Thus, it was demonstrated that mTBI can also lead to abnormal aging marked by cognitive
9 Lewy body disease is a type of dementia, caused by Lewy body protein deposits on nerve
cells which results in a decline in cognition (37). 10 Lewy bodies are neuropathological deposits of protein in the brain cells associated with
dementia and Parkinson’s disease (53). 11 Ventricle enlargement is often found in patients with schizophrenia and most likely
indicates brain shrinkage (58). 12 Episodic memory involves being able to remember and recall life experiences, and is
referred to as autobiographical memory (59).
7
decline and disruption of white matter integrity. Still it should be noted that the association between cognitive abnormality and
white matter damage in mTBI is not confirmed by all studies, which once again reflects the heterogeneity of mTBI. To illustrate, Kinnunen et al. (55), for instance,
found a progressive increase in axial diffusivity in their mTBI sample which is a protective factor that predicts axonal recovery. However, at the same time three of the eight mTBI patients in the same study were discovered to have microbleeds
(tiny haemorrhages within the white matter) in the inner cerebral cortex which is a marker of diffuse axonal injury (55).
6. Comorbidity with psychological conditions:
Although persistent PCS are often found to co-occur with a psychological disorder, it is difficult to reconcile which condition came first. Therefore, these have been
included in the following section, labelled as ‘comorbid’13 with (rather than resultant from) mTBI.
a) PTSD: Academic research has consistently reported an association between persistent PCS and PTSD in both US and UK samples (14,29,61,62). One
example is a study done on a sample of 2525 US Army soldiers who were surveyed 3 or 4 months after returning from Iraq (61). It was found that 43.9%
of those who reported an injury involving loss of consciousness, also met the criteria for PTSD. Furthermore, when the effects of PTSD and depression were controlled for, an mTBI episode was no longer associated with the
postconcussive symptoms reported by the soldiers, except for headache. b) Stress: There are many similarities between the symptoms of persistent
mTBI/PCS and acute stress reaction14 (ASR; (32,62–64)). According to Bryant (32), ‘there are no reliable means to differentiate between symptoms involving impaired awareness that are caused by severe stress or mild traumatic brain
injury’ (p. 526). In support, a very recent study on the effects of blast-related mTBI reported a significant association between mTBI and ASR in their sample
of US military members (64). c) Depression: After PTSD, depression is the second most reported comorbid
condition with mTBI, particularly because of the attentional and memory
problems identified in both disorders (65). For instance, in the study by Hoge et al. (61) mentioned above, 22.9% of the soldiers in their sample who incurred
an injury involving loss of consciousness, also met the criteria for depression. Finally, many studies conducted with civilians have suggested that TBI, in general, increases the risk for developing depression (66–68).
7. The size of the problem - prevalence rates:
a) US: According to the US Defense Medical Surveillance System and the Theater
Medical Data Store, about 58% of all traumatic brain injuries occur in US Army
13 Comorbidity refers to the co-occurrence of two or more disorders in an individual. It has
important implications for identifying the aetiology and diagnostic criteria of conditions, as
well as for how healthcare should be provided to see an improvement (60). 14 Acute Stress Reaction involves an initial state of daze, amnesia, narrowing of attention
and disorientation (ICD-10; (24)).
8
personnel, while the remainder is evenly spread among the Navy, Marines, and Air Force (69). An overall high prevalence15 of persistent PCS has been
identified in US Armed Forces returning from the Iraq and Afghanistan wars. Although the exact percentage of those affected by mTBI post-deployment
remains unclear, research has suggested that this is between 15% (61) and 22% (70). Furthermore, a substantially higher percentage of those sustaining an mTBI are combat personnel (71), as might be expected as combat roles
increase the risk of exposure to blast and therefore an increased risk of sustaining mTBI (72).
b) UK and Canada: Much lower prevalence rates of mTBI have been reported among UK service personnel as compared to those in the US. For example, according to Rona et al. (73) the overall prevalence for those returning from
Afghanistan and Iraq is 4.4%, rising to 9.5% for combat personnel. Furthermore, more recently Jones et al. (14) reported an even lower yearly
rate of 3.2% with no significant difference between combat and other military personnel. Finally, a similarly low prevalence rate of mTBI has been identified in a recent study based on the responses of 16,193 Canadian military who were
sent to Afghanistan between 2009 and 2012 (5.2%, (10,74)16. c) Prevalence vs Incidence: Importantly, it should be noted that comparing the
frequency of mTBI cases among different samples of Armed Forces is not necessarily best expressed with prevalence proportions, as the latter do not
take into account the length of deployment for each cohort. Furthermore, Rona et al. (75) suggested that a more appropriate estimate when cross-sectional data17 is used, would be adjusting the rates for ‘person-years’ to account for
the length of deployment and therefore be able to obtain an estimate of incidence18 instead. By applying this method to a data set of 3763 UK
personnel, who have been deployed to Iraq and Afghanistan, Rona et al. (75) identified an mTBI incidence rate of 10.2 (per 100 person-years) in the UK Army and Marines and 9.0 (per 100 person-years) for all UK Armed Forces in
the sample. Therefore, although still lower than those in the US, these incidence rates were higher than the prevalence rates of mTBI previously
reported amongst similar UK samples. Thus, overall comparisons between different military populations in terms of the relative frequency of the condition should be applied with caution. As Garber et al. ((10), p.6), suggested ‘… there
is no single prevalence estimate of mTBI in a deployed military population. This highlights the need for all militaries to estimate the risk based on the nature
and duration of the deployment.’ d) Current mTBI rates according to the MoD: Following a request by the HVRT,
15 Prevalence gives a measure of how widespread a particular condition is at a single point
of time. 16 Both studies make use of the same data. 17 Cross-sectional design refers to studying the sample of interest at a single point in time.
Cross-sectional data is used to provide an estimate of the prevalence of a certain outcome
(e.g., mTBI) in the study population. Longitudinal studies, on the contrary, involve
following the same group of individuals over a period of time and therefore are used to
provide an incidence estimate (75). 18 Incidence gives a measure of the risk of contracting a condition (i.e., how many new
cases occur and how the pattern changes). Thus, to determine the incidence rate, one
needs to examine the study population for a period of time.

9
the Department of Defence Statistics at the MoD revealed the number of mTBI cases in the UK Armed Forces for the period between the 1 April 2008 and the
31 March 2016 (Reference of the request: FOI2016/07678). The data had been collated from four datasets – the Joint Trauma and Theatre Register
(JTTR); the Neurology Rehabilitation Group at the Defence Medical Rehabilitation Centre, Headley Court (NRG DMRC Database); mTBI Database (maintained by the mTBI cell at DMRC Headley Court) and the Defence Medical
Information Capability Programme (DMICP). As reported in Table 2, in the above period, 967 UK Service Personnel were
identified as having ‘a possible or definite’ mTBI, while roughly one third of those, 343, met the official diagnostic criteria for mTBI, as described in Section 3 of the present report. Importantly, in both occasions the cited figures
represent the minimum number of cases as in some occasions it was not possible to classify the severity of the injury or data could not have been
retrieved/was not available (See Appendix 2 for full details). Furthermore, as it could be seen from the data, most of the mTBI cases have been reported in Army personnel (748 people with a possible or definite mTBI) which makes
77% of the total cases; the proportions for the Royal Navy and Royal Marines (Naval Service) and the Royal Air Force are 13% and 10%, respectively.
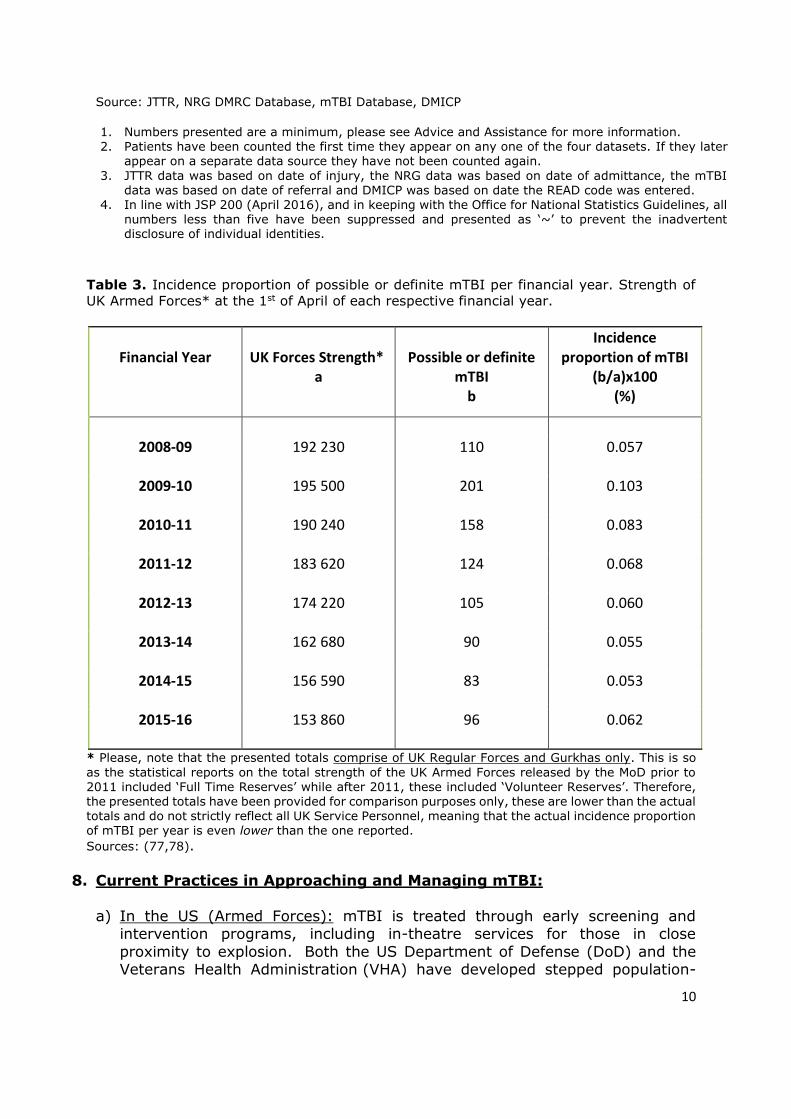
Finally, when the number of cases are broken down by type of Service and yearly period and compared to the total strength of each Service for the
respective year, it could be seen that the relative incidence of mTBI is extremely low (See Table 3). Furthermore, the increased number of mTBI cases seen in 2009-2010 corresponds to the high operational tempo in Iraq
and Afghanistan in this period, whereas the decreased numbers seen in later years coincide with the end of the UK operation in Afghanistan (Operation
HERRICK began 1 April 2006 and ended on 30 November 2014; (76)). Full detail of the response provided by the Department of Defence Statistics could be found in Appendix 2.
Table 2. UK Service Personnel Mild Traumatic Brain Injury by Service and financial year, 1
April 2008 – 31 March 2016, Numbers1,2,3,4. Table reproduced from the Department of Defence
Statistics response to request FOI2016/07678. Please refer to Appendix 2 for the full details.
All Royal Navy
and Royal
Marines
Army RAF All Royal Navy
and Royal
Marines
Army RAF
All 967 126 748 93 343 52 239 52
2008-09 110 20 81 9 36 6 25 5
2009-10 201 17 174 10 41 ~ 34 ~
2010-11 158 15 132 11 36 ~ 26 ~
2011-12 124 28 85 11 40 ~ 24 ~
2012-13 105 12 84 9 39 ~ 31 ~
2013-14 90 9 70 11 21 ~ 13 ~
2014-15 83 13 55 15 53 9 32 12
2015-16 96 12 67 17 77 8 54 15
Record possible or definite mTBI
Financial Year
mTBI that met the
concussion/mTBI criteria outlined
in JSP 950 Leaflet 2-4-3
10
Source: JTTR, NRG DMRC Database, mTBI Database, DMICP
1. Numbers presented are a minimum, please see Advice and Assistance for more information. 2. Patients have been counted the first time they appear on any one of the four datasets. If they later
appear on a separate data source they have not been counted again.
3. JTTR data was based on date of injury, the NRG data was based on date of admittance, the mTBI data was based on date of referral and DMICP was based on date the READ code was entered.
4. In line with JSP 200 (April 2016), and in keeping with the Office for National Statistics Guidelines, all numbers less than five have been suppressed and presented as ‘~’ to prevent the inadvertent disclosure of individual identities.
Table 3. Incidence proportion of possible or definite mTBI per financial year. Strength of
UK Armed Forces* at the 1st of April of each respective financial year.
Financial Year
UK Forces Strength*
a
Possible or definite
mTBI b
Incidence proportion of mTBI
(b/a)x100 (%)
2008-09
192 230 110 0.057
2009-10
195 500 201 0.103
2010-11
190 240
158 0.083
2011-12
183 620 124 0.068
2012-13
174 220 105 0.060
2013-14
162 680 90 0.055
2014-15
156 590 83 0.053
2015-16
153 860
96 0.062
* Please, note that the presented totals comprise of UK Regular Forces and Gurkhas only. This is so
as the statistical reports on the total strength of the UK Armed Forces released by the MoD prior to 2011 included ‘Full Time Reserves’ while after 2011, these included ‘Volunteer Reserves’. Therefore, the presented totals have been provided for comparison purposes only, these are lower than the actual
totals and do not strictly reflect all UK Service Personnel, meaning that the actual incidence proportion of mTBI per year is even lower than the one reported.
Sources: (77,78).
8. Current Practices in Approaching and Managing mTBI:
a) In the US (Armed Forces): mTBI is treated through early screening and intervention programs, including in-theatre services for those in close
proximity to explosion. Both the US Department of Defense (DoD) and the Veterans Health Administration (VHA) have developed stepped population-

11
based screening tools. For example, the Military Acute Concussion Evaluation (MACE) has been extensively adopted in the recent Iraq and Afghanistan
theatres of operation as a rapid, easy-to administer test, used to screen especially for blast injury secondary to improvised explosion devices (79).
MACE consists of two parts – in the first part the patient is asked questions to determine the historical context of the condition and the diagnosis. In the second part, their orientation, immediate memory, concentration, and delayed
recall are examined to screen for any neurocognitive deficits that might have occurred (80). However, despite commonly used in the military head trauma
population, MACE showed poor reliability as a screening tool for mTBI in a recent study conducted with civilians (80). Furthermore, some have raised concerns about the sensitivity of such tools in general (the screen misses 30%-
60% of TBI cases; (40) and whether population screening is really necessary, given the nonspecific nature of PCS (81).
b) In the UK: ❖ Armed Forces: In the UK, health treatment is instead provided only to those
who have experienced a moderate or severe TBI or exhibit persistent PCS
following a head trauma (14). Several research reports, based on UK military data, have shown support for the latter policy. For example, based on the
identified very small incidence rate of mTBI in their sample, Jones et al. (14) advised against the adoption of US–like in-theatre interventions, in view of
the potential for inflating the rates of symptom reporting. ❖ General primary care and recommendations: In the UK, clinical care is
usually provided either in general practices or in emergency departments,
however, patients with mTBI often receive inconsistent advice depending on the awareness of the practitioner. As mentioned earlier, the majority of
patients diagnosed with mTBI are not referred to a specialist which however, is recommended especially when PCS develop (1,2). In view of the heterogeneity of the condition and the possibility of developing PCS,
researchers have suggested that even mTBI patients might benefit from primary survey and simultaneous resuscitation, receiving care from
interdisciplinary teams, as well as being followed up at specified intervals after the injury (1,2). Although there is no agreed standard on the management and treatment of mTBI, The UK National Institute of Health and
Care Excellence (NICE) has come up with guidelines on the assessment and early management of head injury (36). However, more recently NICE started
their ‘NICE Pathways’ series which represent interactive, flowchart guides that make the information even more accessible. These incorporate all NICE guidance, quality standards and other NICE information, are updated on a
regular basis and are easily accessible online. Furthermore, the NICE ‘Pre-hospital management’19 and ‘Assessment in the emergency department’20
pathways identify the conditions when a patient who has sustained an mTBI
19 ‘Pre-hospital management’ can be accessed at
http://pathways.nice.org.uk/pathways/head-injury/pre-hospital-management-for-
patients-with-head-injury.
20 ‘Assessment in the emergency department’ can be accessed at
http://pathways.nice.org.uk/pathways/head-injury/assessment-in-the-emergency-
department-for-patients-with-head-injury.

12
is likely to be at risk and therefore requires further examinations and a specialist review. For example, according to these ‘patients presenting to the
emergency department with impaired consciousness (GCS less than 15) should be assessed immediately by a trained member of staff’ and ‘patients
who return to an emergency department within 48 hours of transfer to the community with any persistent complaint relating to the initial head injury should be seen by or discussed with a senior clinician experienced in head
injuries, and considered for a CT scan.’ ((36), p.20-21). c) Guidelines for best practice in contact sports: The US National Football League
has come up with best practice guidelines for handling mTBI in contact sports. For example, the Concussion Evaluation and Management Protocol is a procedure guideline, designed for all Clubs that stipulates simple, easy to
follow instructions regarding the provision of educational material to players, baseline testing, identification, evaluation, and management of the condition.
Importantly, the protocol also features a thorough list of signs and symptoms outlining when a player should be removed from play for an acute evaluation, as well as clear return to play rules. Additionally, the US Centers for Disease
Control and Prevention publish guidelines, specifically designed for young athletes of different age groups, parents, coaches and sports officials (82).
Despite the latter, best practice clinical pathways from injury to return to play have generally been difficult access and find in the UK and only recently such
have started to emerge. For example, the Scottish Sport Concussion Guidelines for the general public and participants in grassroots sports were only launched in 2015 (83). Finally, the need for ‘a cross-sports consensus on
the recognition and management of concussion with consistency across all sporting bodies and in conjunction with education and healthcare systems’ has
recently been recognised by the UK Faculty of Sport and Exercise Medicine (FSEM, (83)). The FSEM, together with UK National Sporting Bodies and Medical Royal Colleges are currently working towards creating common
guidelines for consistent best practice for handling mTBI. d) Educational therapy: The evidence suggests that participation in early
educational intervention programs can be particularly beneficial for alleviating PCS following mTBI. In a review of the literature on non-surgical interventions for mTBI, (84) found that simple educational interventions, where patients are
reassured about the recovery and are encouraged to slowly return to normal activity, were more effective than an intensive intervention. Moreover,
administering even a single educational session to patients with mTBI was found to be as effective as more in-depth assessment and therapy (See (84)). Furthermore, patient education is also at the basis of the rehabilitation
programme, devised by the UK Defence Medical Rehabilitation Centre (DMRC) Headley Court. There is evidence that the programme, consisting of four
phases, including psychological treatment for more persistent cases, could be beneficial for helping military personnel to regain their stability after the injury (85). Finally, there is evidence that educational therapy could be effective for
reducing PCS even if done via telephone (86,87). e) Psychological therapy: Considering the significant associations between mTBI
and other disorders such as PTSD and depression, several authors have proposed that psychological treatment could alleviate persistent PCS by addressing the comorbid conditions PCS co-occurs with (63,65,85). Some of
these approaches include modified cognitive behavioural therapy (CBT) and

13
cognitive restructuring and behavioural activation. Research has suggested that modified cognitive behavioural therapy (CBT), in particular, might be
successful in addressing persistent PCS following mTBI (88,89). Furthermore, CBT has been recommended as a therapeutic method by the US Department
of Veterans Affairs and the DoD (90). f) Medication: Research has indicated that certain drugs can have a positive
effect on mTBI. For example, methylphenidate, which is also used for the
treatment of ADHD in children, has been shown to alleviate mental fatigue by increasing the levels of dopamine and noradrenalin in the body (91).
Furthermore, there is evidence that it can improve patients’ impaired cognitive function (information processing speed, working memory and attention) following TBI (92,93), including mTBI (91). Moreover, according to findings
from animal studies, methylphenidate can also have a positive psychological impact by reducing aggression and promoting psychosocial function (See (94)
for a meta-analysis). Finally, in the context of military setting, acetylcysteine has proven efficacious in reducing the constellation of PCS and cognitive dysfunction symptoms in 81 US Service Personnel who sustained a blast-
related mTBI (95). Furthermore, no side effects were reported in this study seven days after the administration of the drug. Acetylcysteine is known for
its neuroprotective21 effects in ‘animal ischemia-reperfusion22 cerebral stroke models, rodent closed head trauma model, sensory nerve axotomy23 model
and inner ear neuronal death after noise exposure’ ((95), p. 2). 9. Conclusion:
The aim of this report was to provide a review of mTBI in military personnel by drawing information from key research studies, government reports and
relevant literature on mTBI in contact sports. Although identified as the ‘signature injury’ of the recent Afghanistan and Iraq conflicts, mTBI seems to vary considerably in prevalence among UK and US service personnel. There is still no
agreement on the classification and the aetiology of the disorder, which most likely stems from the existent heterogeneity within the condition. Furthermore, despite
being characterised by non-specific postconcussive symptoms that can manifest even in the absence of a traumatic head injury, in a minority of cases mTBI results in a serious disability, marked by clear psychical abnormalities. Future work should
focus on identifying optimal strategies to bridge the gaps in the management and treatment of mTBI; how much follow up is needed to detect PCS and whether
more serious long-term effects are likely to develop; as well as on identifying reliable markers to distinguish between the different subcategories within the condition.
21 Neuroprotective refers to helping to reduce the rate of neuronal loss. 22 Ischemia-reperfusion is tissue damage, caused by restriction of blood flow to the heart. 23 Axotomy refers to the cutting of the axon.

14
References
1. Sharp DJ, Jenkins PO. Concussion is confusing us all. Pract Neurol. 2015
Jun;15(3):172–86.
2. Kolias AG, Guilfoyle MR, Helmy A, Allanson J, Hutchinson PJ. Traumatic brain injury in adults. Pract Neurol. 2013 Aug;13(4):228–35.
3. Hou R, Moss-Morris R, Peveler R, Mogg K, Bradley BP, Belli A. When a minor head injury results in enduring symptoms: a prospective investigation of risk
factors for postconcussional syndrome after mild traumatic brain injury. J Neurol Neurosurg Psychiatry. 2012 Feb;83(2):217–23.
4. DeCuypere M, Klimo P. Spectrum of Traumatic Brain Injury from Mild to
Severe. Surg Clin North Am. 2012 Aug;92(4):939–57.
5. The American Congress of Rehabilitation Medicine. Definition of mild
traumatic brain injury. J Head Trauma Rehabil. 1993;8(3):86–7.
6. Rona RJ. Long-term consequences of mild traumatic brain injury. Br J Psychiatry. 2012 Sep 1;201(3):172–4.
7. Sharp DJ, Ham TE. Investigating white matter injury after mild traumatic brain injury: Curr Opin Neurol. 2011 Dec;24(6):558–63.
8. Murrison, A. Fighting fit: A mental health plan for servicemen and veterans. [Internet]. 2010. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data
/file/27375/20101006_mental_health_Report.pdf
9. Tanielian TL, Jaycox L, Center for Military Health Policy Research, editors.
Invisible wounds of war: psychological and cognitive injuries, their consequences, and services to assist recovery. Santa Monica, Calif.: Rand;
2008. 453 p. (Rand MG CCF).
10. Garber BG, Rusu C, Zamorski MA. Deployment-related mild traumatic brain injury, mental health problems, and post-concussive symptoms in Canadian
Armed Forces personnel. BMC Psychiatry. 2014;14(1):325.
11. Donovan J, Cancelliere C, Cassidy JD. Summary of the findings of the
International Collaboration on Mild Traumatic Brain Injury Prognosis. Chiropr Man Ther. 2014;22(1):38.
12. Cassidy JD, Carroll LJ, Peloso PM, Borg J, von Holst H, Holm L, et al. Incidence,
risk factors and prevention of mild traumatic brain injury: results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J Rehabil
Med. 2004 Feb;(43 Suppl):28–60.
13. Ryan LM, Warden DL. Post concussion syndrome. Int Rev Psychiatry. 2003

15
Nov;15(4):310–6.
14. Jones N, Fear NT, Rona R, Fertout M, Thandi G, Wessely S, et al. Mild
traumatic brain injury (mTBI) among UK military personnel whilst deployed in Afghanistan in 2011. Brain Inj. 2014 Jun;28(7):896–9.
15. Jones E, Hodgins-Vermaas R, McCartney H, Everitt B, Beech C, Poynter D, et al. Post-combat syndromes from the Boer war to the Gulf war: a cluster analysis of their nature and attribution. Bmj. 2002;324(7333):321.
16. Gray GC, Kang HK. Healthcare utilization and mortality among veterans of the Gulf War. Philos Trans R Soc B Biol Sci. 2006 Apr 29;361(1468):553–69.
17. McCrory PR, Berkovic SF. Concussion: the history of clinical and pathophysiological concepts and misconceptions. Neurology. 2001 Dec 26;57(12):2283–9.
18. Giza CC, Kutcher JS, Ashwal S, Barth J, Getchius TSD, Gioia GA, et al. Summary of evidence-based guideline update: Evaluation and management
of concussion in sports: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013 Jun 11;80(24):2250–7.
19. Grindel, S. H. Epidemiology and pathophysiology of minor traumatic brain injury. Curr Sports Med Rep. 2(1):18–23.
20. Thompson, J. M. Persistent Symptoms Following Mild Traumatic Brain Injury (mTBI) – A Resource for Clinicians and Staff. [Internet]. Veterans Affairs
Canada Research Directorate Technical Report; 2008. Available from: https://www.veterans.gc.ca/pdf/about-us/research-directorate/mtbi-report-sep08.pdf
21. Carroll L, Cassidy JD, Peloso P, Borg J, von Holst H, Holm L, et al. Prognosis for mild traumatic brain injury: results of the who collaborating centre task
force on mild traumatic brain injury. J Rehabil Med. 2004 Feb 1;36(0):84–105.
22. Rohling ML, Binder LM, Demakis GJ, Larrabee GJ, Ploetz DM, Langhinrichsen-
Rohling J. A Meta-Analysis of Neuropsychological Outcome After Mild Traumatic Brain Injury: Re-analyses and Reconsiderations of Binder et al.
(1997), Frencham et al. (2005), and Pertab et al. (2009). Clin Neuropsychol. 2011 May;25(4):608–23.
23. Frencham KAR, Fox AM, Maybery MT. Neuropsychological Studies of Mild
Traumatic Brain Injury: A Meta-Analytic Review of Research Since 1995. J Clin Exp Neuropsychol. 2005 Apr;27(3):334–51.
24. World Health Organisation [WHO]. The ICD-10 classification of mental and behavioural disorders: Clinical descriptions and diagnostic guidelines. [Internet]. Geneva: World Health Organisation.; 2016. Available from:
http://apps.who.int/classifications/icd10/browse/2016/en

16
25. Great Britain. Ministry of Defence. Background quality report: Mental health in the UK armed forces. [Internet]. 2016a. Available from:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/529409/20160613-Background_Quality_Report_MH.pdf
26. Bagalman E. Traumatic Brain Injury Among Veterans [Internet]. Washington, D.C.: Congressional Research Service; Available from: http://www.ncsl.org/documents/statefed/health/TBI_Vets2013.pdf
27. Thompson JM, Scott KC, Dubinsky L. Battlefield brain Unexplained symptoms and blast-related mild traumatic brain injury. Can Fam Physician.
2008;54(11):1549–1551.
28. Meares S, Shores EA, Taylor AJ, Batchelor J, Bryant RA, Baguley IJ, et al. Mild traumatic brain injury does not predict acute postconcussion syndrome. J
Neurol Neurosurg Psychiatry. 2008 Mar 1;79(3):300–6.
29. Dean PJA, O’Neill D, Sterr A. Post-concussion syndrome: Prevalence after mild
traumatic brain injury in comparison with a sample without head injury. Brain Inj. 2012 Jan;26(1):14–26.
30. Iverson GL. Outcome from mild traumatic brain injury: Curr Opin Psychiatry.
2005 May;18(3):301–17.
31. Fear NT, Jones E, Groom M, Greenberg N, Hull L, Hodgetts TJ, et al.
Symptoms of post-concussional syndrome are non-specifically related to mild traumatic brain injury in UK Armed Forces personnel on return from
deployment in Iraq: an analysis of self-reported data. Psychol Med. 2009 Aug;39(08):1379.
32. Bryant RA. Disentangling mild traumatic brain injury and stress reactions
[Internet]. Mass Medical Soc; 2008 [cited 2017 Mar 8]. Available from: http://www.nejm.org/doi/full/10.1056/NEJMe078235
33. Malec JF, Brown AW, Leibson CL, Flaada JT, Mandrekar JN, Diehl NN, et al. The Mayo Classification System for Traumatic Brain Injury Severity. J Neurotrauma. 2007 Sep;24(9):1417–24.
34. The Independent Medical Expert Group [IMEG]. Report and recommendations on medical and scientific aspects of the Armed Forces Compensation Scheme.
[Internet]. London: The Ministry of Defence UK; 2013. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/200140/imeg_report_2013_final.pdf.
35. Stocker RPJ, Cieply MA, Paul B, Khan H, Henry L, Kontos AP, et al. Combat-related blast exposure and traumatic brain injury influence brain glucose
metabolism during REM sleep in military veterans. NeuroImage. 2014 Oct;99:207–14.
36. National Institute for Health and Care Excellence. Head injury: assessment
and early management, (CG176). [Internet]. London: NICE; 2014. Available

17
from: https://www.nice.org.uk/guidance/cg176/resources/head-injury-assessment-and-early-management-35109755592901.
37. McKee AC, Stein TD, Nowinski CJ, Stern RA, Daneshvar DH, Alvarez VE, et al. The spectrum of disease in chronic traumatic encephalopathy. Brain. 2013
Jan 1;136(1):43–64.
38. Soares JM, Marques P, Alves V, Sousa N. A hitchhiker’s guide to diffusion tensor imaging. Front Neurosci [Internet]. 2013 [cited 2017 Mar 8];7.
Available from: http://journal.frontiersin.org/article/10.3389/fnins.2013.00031/abstract
39. Scheid R, Walther K, Guthke T, Preul C, von Cramon DY. Cognitive Sequelae of Diffuse Axonal Injury. Arch Neurol. 2006 Mar 1;63(3):418.
40. Belanger HG, Vanderploeg RD, Sayer N. Screening for Remote History of Mild
Traumatic Brain Injury in VHA: A Critical Literature Review. J Head Trauma Rehabil. 2016;31(3):204–14.
41. Zetterberg H, Smith DH, Blennow K. Biomarkers of mild traumatic brain injury in cerebrospinal fluid and blood. Nat Rev Neurol. 2013 Feb 12;9(4):201–10.
42. Brown SJ, Fann JR, Grant I. Post concussional disorder: time to acknowledge
a common source of neurobehavioral morbidity. J Neuropsychiatry Clin Neurosci. 1994;6:15–22.
43. Gouvier WD, Cubic B, Jones G, Brantley P, Cutlip Q. Postconcussion symptoms and daily stress in normal and head-injured college populations. Arch Clin
Neuropsychol. 1992;7(3):193–211.
44. Gavett BE, Stern RA, McKee AC. Chronic Traumatic Encephalopathy: A Potential Late Effect of Sport-Related Concussive and Subconcussive Head
Trauma. Clin Sports Med. 2011 Jan;30(1):179–88.
45. McKee AC, Gavett BE, Stern RA, Nowinski CJ, Cantu RC, Kowall NW, et al.
TDP-43 Proteinopathy and Motor Neuron Disease in Chronic Traumatic Encephalopathy. J Neuropathol Exp Neurol. 2010 Sep;69(9):918–29.
46. Klein RL, Lin W-L, Dickson DW, Lewis J, Hutton M, Duff K, et al. Rapid
Neurofibrillary Tangle Formation after Localized Gene Transfer of Mutated Tau. Am J Pathol. 2004 Jan;164(1):347–53.
47. Esiri MM, Pearson RC, Steele JE, Bowen DM, Powell TP. A quantitative study of the neurofibrillary tangles and the choline acetyltransferase activity in the cerebral cortex and the amygdala in Alzheimer’s disease. J Neurol Neurosurg
Psychiatry. 1990;53(2):161–165.
48. Johnson VE, Stewart W, Smith DH. Axonal pathology in traumatic brain injury.
Exp Neurol. 2013 Aug;246:35–43.
49. Gong C-X, Iqbal K. Hyperphosphorylation of microtubule-associated protein

18
tau: a promising therapeutic target for Alzheimer disease. Curr Med Chem. 2008;15(23):2321–8.
50. Rosenfeld JV, McFarlane AC, Bragge P, Armonda RA, Grimes JB, Ling GS. Blast-related traumatic brain injury. Lancet Neurol. 2013;12(9):882–893.
51. Crane PK, Gibbons LE, Dams-O’Connor K, Trittschuh E, Leverenz JB, Keene CD, et al. Association of Traumatic Brain Injury With Late-Life Neurodegenerative Conditions and Neuropathologic Findings. JAMA Neurol.
2016 Sep 1;73(9):1062.
52. Mayeux R, Ottman R, Maestre G, Ngai C, Tang MX, Ginsberg H, et al.
Synergistic effects of traumatic head injury and apolipoprotein-epsilon 4 in patients with Alzheimer’s disease. Neurology. 1995 Mar;45(3 Pt 1):555–7.
53. Lepkowsky CM. Neurocognitive disorder with Lewy bodies: Evidence-based
diagnosis and treatment. Pract Innov. 2016;1(4):234–42.
54. Ponsford J, Kinsella G. Attentional deficits following closed-head injury. J Clin
Exp Neuropsychol. 1992 Sep;14(5):822–38.
55. Kinnunen KM, Greenwood R, Powell JH, Leech R, Hawkins PC, Bonnelle V, et al. White matter damage and cognitive impairment after traumatic brain
injury. Brain. 2011 Feb 1;134(2):449–63.
56. Niogi SN, Mukherjee P, Ghajar J, Johnson CE, Kolster R, Lee H, et al.
Structural dissociation of attentional control and memory in adults with and without mild traumatic brain injury. Brain. 2008 Dec 1;131(12):3209–21.
57. Tremblay S, De Beaumont L, Henry LC, Boulanger Y, Evans AC, Bourgouin P, et al. Sports Concussions and Aging: A Neuroimaging Investigation. Cereb Cortex. 2013 May 1;23(5):1159–66.
58. Horga G, Bernacer J, Dusi N, Entis J, Chu K, Hazlett EA, et al. Correlations between ventricular enlargement and gray and white matter volumes of
cortex, thalamus, striatum, and internal capsule in schizophrenia. Eur Arch Psychiatry Clin Neurosci. 2011 Oct;261(7):467–76.
59. Tulving E, Markowitsch HJ. Episodic and declarative memory: role of the
hippocampus. Hippocampus. 1998;8(3):198–204.
60. Valderas JM, Starfield B, Sibbald B, Salisbury C, Roland M. Defining
Comorbidity: Implications for Understanding Health and Health Services. Ann Fam Med. 2009 Jul 1;7(4):357–63.
61. Hoge CW, McGurk D, Thomas JL, Cox AL, Engel CC, Castro CA. Mild traumatic
brain injury in US soldiers returning from Iraq. N Engl J Med. 2008;358(5):453–463.
62. Warden D. Military TBI during the Iraq and Afghanistan wars. J Head Trauma Rehabil. 2006;21(5):398–402.
19
63. Bryant R. Post-traumatic stress disorder vs traumatic brain injury. Dialogues Clin Neurosci. 2011;13(3):251–62.
64. Norris JN, Smith S, Harris E, Labrie DW, Ahlers ST. Characterization of acute stress reaction following an IED blast-related mild traumatic brain injury.
Brain Inj. 2015 Jul 3;29(7–8):898–904.
65. Seal KH, Bertenthal D, Samuelson K, Maguen S, Kumar S, Vasterling JJ. Association between mild traumatic brain injury and mental health problems
and self-reported cognitive dysfunction in Iraq and Afghanistan Veterans. J Rehabil Res Dev. 2016;53(2):185–98.
66. Seel RT, Kreutzer JS, Rosenthal M, Hammond FM, Corrigan JD, Black K. Depression after traumatic brain injury: A National Institute on Disability and Rehabilitation Research Model Systems multicenter investigation. Arch Phys
Med Rehabil. 2003 Feb;84(2):177–84.
67. Iverson G. Misdiagnosis of the persistent postconcussion syndrome in patients
with depression. Arch Clin Neuropsychol. 2006 May;21(4):303–10.
68. Silver JM, Kramer R, Greenwald S, Weissman M. The association between head injuries and psychiatric disorders: findings from the New Haven NIMH
Epidemiologic Catchment Area Study. Brain Inj. 2001 Jan;15(11):935–45.
69. Boyle E, Cancelliere C, Hartvigsen J, Carroll LJ, Holm LW, Cassidy JD.
Systematic Review of Prognosis After Mild Traumatic Brain Injury in the Military: Results of the International Collaboration on Mild Traumatic Brain
Injury Prognosis. Arch Phys Med Rehabil. 2014 Mar;95(3):S230–7.
70. Polusny MA, Kehle SM, Nelson NW, Erbes CR, Arbisi PA, Thuras P. Longitudinal effects of mild traumatic brain injury and posttraumatic stress disorder
comorbidity on postdeployment outcomes in National Guard soldiers deployed to Iraq. Arch Gen Psychiatry. 2011;68(1):79–89.
71. Terrio H, Brenner LA, Ivins BJ, Cho JM, Helmick K, Schwab K, et al. Traumatic Brain Injury Screening: Preliminary Findings in a US Army Brigade Combat Team. J Head Trauma Rehabil. 2009 Jan;24(1):14–23.
72. Vanderploeg RD, Belanger HG, Horner RD, Spehar AM, Powell-Cope G, Luther SL, et al. Health Outcomes Associated With Military Deployment: Mild
Traumatic Brain Injury, Blast, Trauma, and Combat Associations in the Florida National Guard. Arch Phys Med Rehabil. 2012 Nov;93(11):1887–95.
73. Rona RJ, Jones M, Fear NT, Hull L, Murphy D, Machell L, et al. Mild Traumatic
Brain Injury in UK Military Personnel Returning From Afghanistan and Iraq: Cohort and Cross-sectional Analyses. J Head Trauma Rehabil.
2012;27(1):33–44.
74. Garber BG, Rusu C, Zamorski MA, Boulos D. Occupational outcomes following mild traumatic brain injury in Canadian military personnel deployed in support
of the mission in Afghanistan: a retrospective cohort study. BMJ Open.
20
2016;6(5):e010780.
75. Rona RJ, Jones M, Fear NT, Sundin J, Hull L, Wessely S. Frequency of Mild
Traumatic Brain Injury in Iraq and Afghanistan: Are We Measuring Incidence or Prevalence? J Head Trauma Rehabil. 2012;27(1):75–82.
76. Great Britain. Ministry of Defence. Deaths in the UK Regular Armed Forces: Annual Summary and Trends Over Time, 1 January 2006 to 31 December 2015. [Internet]. 2016b. Available from:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/511812/20160331_UK_AF_Deaths_National_Statistic_2016-O.pdf
77. Rutherford T. Defence Personnel Statistics: Commons Briefing Paper SNSG02183. [Internet]. London: House of Commons Library.; 2014. Available from:
http://researchbriefings.parliament.uk/ResearchBriefing/Summary/SN02183
78. Great Britain. Ministry of Defence. UK Armed Forces Monthly Service
Personnel Statistics, 1 October 2016, 17 November 2016. [Internet]. 2016c. Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data
/file/569201/Monthly_service_personnel_statistics-_October_2016.pdf
79. McCrea M, Pliskin N, Barth J, Cox D, Fink J, French L, et al. Official Position of
the Military TBI Task Force on the Role of Neuropsychology and Rehabilitation Psychology in the Evaluation, Management, and Research of Military Veterans
with Traumatic Brain Injury. Clin Neuropsychol. 2008 Jan 28;22(1):10–26.
80. Stone ME, Safadjou S, Farber B, Velazco N, Man J, Reddy SH, et al. Utility of the Military Acute Concussion Evaluation as a screening tool for mild traumatic
brain injury in a civilian trauma population: J Trauma Acute Care Surg. 2015 Jul;79(1):147–51.
81. Vanderploeg RD, Belanger HG. Screening for a Remote History of Mild Traumatic Brain Injury: When a Good Idea Is Bad. J Head Trauma Rehabil. 2013;28(3):211–8.
82. Centers for Disease Control and Prevention. HEADS UP to Youth Sports: Athletes. [Internet]. 2017. Available from:
https://www.cdc.gov/headsup/youthsports/athletes.html
83. Faculty of Sort and Exercise Medicine [FSEM]. Scots concussion guidelines highlight the need for a UK wide approach. [Internet]. 2015. Available from:
http://www.fsem.ac.uk/news/faculty-news/2015/may/scots-concussion-guidelines-highlight-the-need-for-a-uk-wide-approach.aspx
84. Borg J, Holm L, Peloso P, Cassidy JD, Carroll L, von Holst H, et al. Non-surgical intervention and cost for mild traumatic brain injury: results of the who collaborating centre task force on mild traumatic brain injury. J Rehabil Med.
2004 Feb 1;36(0):76–83.
21
85. Brunger H, Ogden J, Malia K, Eldred C, Terblanche R, Mistlin A. Adjusting to persistent post-concussive symptoms following mild traumatic brain injury
and subsequent psycho-educational intervention: A qualitative analysis in military personnel. Brain Inj. 2014 Jan;28(1):71–80.
86. Elgmark Andersson E, Emanuelson I, Björklund R, Stålhammar DA. Mild traumatic brain injuries: the impact of early intervention on late sequelae. A randomized controlled trial. Acta Neurochir (Wien). 149(2):151–9.
87. Bell KR, Hoffman JM, Temkin NR, Powell JM, Fraser RT, Esselman PC, et al. The effect of telephone counselling on reducing post-traumatic symptoms
after mild traumatic brain injury: A randomised trial. J Neurol Neurosurg Psychiatry. 2008 Jun 5;79(11):1275–81.
88. Mittenberg W, Tremont G, Zielinski RE, Fichera S, Rayls KR. Cognitive-
behavioral prevention of postconcussion syndrome. Arch Clin Neuropsychol. 1996;11(2):139–45.
89. Silverberg ND, Hallam BJ, Rose A, Underwood H, Whitfield K, Thornton AE, et al. Cognitive-behavioral prevention of postconcussion syndrome in at-risk patients: a pilot randomized controlled trial. J Head Trauma Rehabil.
2013;28(4):313–22.
90. The Management of Concussion/mTBI Working Group. Clinical practice
guideline for management of concussion/mild traumatic brain injury. [Internet]. Washington, DC: Department of Veterans Affairs and Department
of Defense; 2009. Available from: http://www.healthquality.va.gov/guidelines/Rehab/mtbi/concussion_mtbi_full_1_0.pdf
91. Johansson B, Wentzel A-P, Andréll P, Odenstedt J, Mannheimer C, Rönnbäck L. Evaluation of dosage, safety and effects of methylphenidate on post-
traumatic brain injury symptoms with a focus on mental fatigue and pain. Brain Inj. 2014 Mar;28(3):304–10.
92. Plenger PM, Dixon CD, Castillo RM, Frankowski RF, Yablon SA, Levin HS.
Subacute methylphenidate treatment for moderate to moderately severe traumatic brain injury: a preliminary double blind placebo-controlled study.
Arch Phys Med Rehabil. 1996;77:536–40.
93. Speech TJ, Rao SM, Osmon DC, Sperry LT. A double-blind controlled study of methylphenidate treatment in closed head injury. Brain Inj. 1993;7(4):333–
8.
94. Wheaton P, Mathias JL, Vink R. Impact of pharmacological treatments on
outcome in adult rodents after traumatic brain injury: a meta-analysis. J Psychopharmacol (Oxf). 2011;25(12):1581–99.
95. Hoffer ME, Balaban C, Slade MD, Tsao JW, Hoffer B. Amelioration of Acute
Sequelae of Blast Induced Mild Traumatic Brain Injury by N-Acetyl Cysteine: A Double-Blind, Placebo Controlled Study. Fehlings M, editor. PLoS ONE. 2013

22
Jan 23;8(1):e54163.

23
Appendix 1
Table 1. The Mayo TBI Severity Classification System (taken from (33)).
A. Classify as Moderate-Severe (Definite) TBI if one or more of the following criteria apply:
1. Death due to this TBI 2. Loss of consciousness of 30 minutes or more
3. Post-traumatic anterograde amnesia of 24 hours or more 4. Worst Glasgow Coma Scale full score in first 24 hours
<13 (unless invalidated upon review, e.g., attributable to intoxication, sedation, systemic shock)
5. One or more of the following present: • Intracerebral hematoma • Subdural hematoma
• Epidural hematoma • Cerebral contusion
• Hemorrhagic contusion • Penetrating TBI (dura penetrated)
• Subarachnoid hemorrhage • Brain Stem Injury
B. If none of Criteria A apply, classify as Mild (Probable)
TBI if one or more of the following criteria apply: 1. Loss of consciousness of momentary to less than 30
minutes 2. Post-traumatic anterograde amnesia of momentary to less than 24 hours
3. Depressed, basilar or linear skull fracture (dura intact) C. If none of Criteria A or B apply, classify as Symptomatic
(Possible) TBI if one or more of the following symptoms are present: • Blurred vision
• Confusion (mental state changes) • Dazed
• Dizziness • Focal neurologic symptoms • Headache
• Nausea

24
Appendix 2
Defence Statistics (Health)
Ministry of Defence
Oak 0 West (#6028)
Abbey Wood North
Bristol BS34 8JH
United Kingdom
Telephone [MOD]:
Facsimile [MOD]:
E-mail:
+44 (0)30679 84423
+44 (0)1179 319634
Reference: FOI2016/07678
28 September 2016
Dear Dr Doneva,
Thank you for your email of 31 August 2016 requesting the following information:
“I am interested in mTBI statistics and more specifically the percentage of mTBI cases in the UK Armed Forces
(Navy, Air Force and Army), ideally for the period between 2001 and 2016, in years:
2001/2002
2002/2003

25
2003/2004
2004/2005
2005/2006
2006/2007
2007/2008
2008/2009
2009/2010
2010/2011
2011/2012
2012/2013
2013/2014
2014/2015
2015/2016
However, if not possible for as many years in that period as possible”.
I am treating your correspondence as a request for information under the Freedom of Information Act 2000.
A search for the information has now been completed within the Ministry of Defence, and I can confirm that the
information in scope of your request is held by the MOD.
However, I have to advise you that we will not be able to fully answer your request without exceeding the
appropriate limit. This is because to locate, retrieve and extract information in scope of your request, specifically
relating to identifying the number of personnel who had a Mild Traumatic Brain Injury (mTBI) prior to 2008/09
and to identify if the injuries sustained were mild or moderate/severe would exceed the cost of compliance limit.
Section 12 of the Act makes provision for public authorities to refuse requests for information where the cost of
dealing with them would exceed the appropriate limit, which for central government is set at £600. This
represents the estimated cost of one person spending 3.5 working days in determining whether the department

26
holds the information, and locating, retrieving and extracting it.
In your request you asked the MOD to provide as many years of information as possible in order to bring the cost
of compliance for your request under the limit. Please find the information you requested below for the time
period 1 April 2008 to 31 March 2016.
Section 40(2) has been applied to some of the information in order to protect personal information as governed
by the Data Protection Act 1998. This is also in line with Joint Service Publication 200 (JSP) in which numbers fewer
than five are suppressed in order to reduce the possible inadvertent disclosure of individual identities. Section 40
is an absolute exemption and there is therefore no requirement to consider the public interest in making a
decision to withhold the information.
Between 1 April 2008 and 31 March 2016, a minimum of 967 UK Service Personnel had a record of having a
possible or definite mild traumatic brain injury (mTBI). Of these, a minimum of 343 met the concussion/mTBI
criteria outlined in JSP 950 Leaflet 2-4-3 :
Patients with concussion/mTBI can present to medical personnel with a variety of symptoms which normally
manifest immediately following an event. Whilst most resolve quickly within minutes to hours some may persist
longer. To make a diagnosis of concussion/mTBI all three of the following criteria must be met:
a. A history of related head injury or involvement in a blast. b. Glasgow Coma Scale (GCS) no lower than 13 at thirty minutes post-injury. c. One or more of the following:
i. Alteration of consciousness (AOC) / mental state - this may present as a variety of transient physical, cognitive or emotional symptoms. Commonly this will include confusion, disorientation, feeling or looking dazed and difficulty concentrating.
ii. Loss of consciousness (LOC) - for no more than 30 minutes duration post-injury. iii. Post-traumatic amnesia (PTA) - for no more than 24 hours duration post-injury. iv. Transient neurological abnormalities - such as focal signs or seizures.
The number of personnel with a record of an mTBI were a minimum because:
• There were 97 personnel with a record of a traumatic brain injury where it was not possible from
the electronic data held to classify the injury into mild, moderate and severe.
• If information was entered as free text in the electronic patient record then it is not available in the
data warehouse and will not be retrieved using the search for mTBI.
The number of personnel with a record of an mTBI who met the concussion/mTBI criteria outlined in JSP 950
Leaflet 2-4-3 were a minimum as not all of the data sources used within this response contained the level of detail

27
required to identify if the criteria had been met.
Table 1 presents the number of UK Service Personnel who had a record of having a possible or
definite mild traumatic brain injury (mTBI) and of these the number that met the concussion/mTBI
criteria outlined in JSP 950 Leaflet 2-4-3. Service personnel are included once in the year where the
mTBI was first identified in one of the four datasets (see Advice and Assistance section).

28
Table 1: UK Service Personnel Mild Traumatic Brain Injury by Service and financial year, 1 April 2008 – 31 March
2016, Numbers1,2,3,4
Source: JTTR, NRG DMRC Database, mTBI Database, DMICP
1. Numbers presented are a minimum, please see Advice and Assistance for more information. 2. Patients have been counted the first time they appear on any one of the four datasets. If they later appear on a separate
data source they have not been counted again. 3. JTTR data was based on date of injury, the NRG data was based on date of admittance, the mTBI data was based on date
of referral and DMICP was based on date the READ code was entered. 4. In line with JSP 200 (April 2016), and in keeping with the Office for National Statistics Guidelines, all numbers less than five
have been suppressed and presented as ‘~’ to prevent the inadvertent disclosure of individual identities.
Under Section 16 (Advice and Assistance) you may find it helpful to note the following: The information contained within this response has been compiled from four data sources:
a. Data held on the Military Audit of Clinical Effectiveness (MACE) database on the Joint Trauma and Theatre Register (JTTR).
b. Data held by the Neurology Rehabilitation Group (NRG) at the Defence Medical Rehabilitation Centre (DMRC), Headley Court.
c. Data held on the mTBI database which is maintained by the mTBI cell at DMRC Headley Court. d. Defence Medical Information Capability Programme (DMICP) has a centralised data warehouse
of coded information. It is the source of electronic, integrated healthcare records for primary healthcare and some MOD specialist care providers.
Personnel have been counted once overall and in Table 1 in the year of the earliest record of an mTBI. Please note
that these are live databases. This means that occasionally patient records can be updated which may change the
figures presented in this response.
All Royal Navy
and Royal
Marines
Army RAF All Royal Navy
and Royal
Marines
Army RAF
All 967 126 748 93 343 52 239 52
2008-09 110 20 81 9 36 6 25 5
2009-10 201 17 174 10 41 ~ 34 ~
2010-11 158 15 132 11 36 ~ 26 ~
2011-12 124 28 85 11 40 ~ 24 ~
2012-13 105 12 84 9 39 ~ 31 ~
2013-14 90 9 70 11 21 ~ 13 ~
2014-15 83 13 55 15 53 9 32 12
2015-16 96 12 67 17 77 8 54 15
Record possible or definite mTBI
Financial Year
mTBI that met the
concussion/mTBI criteria outlined
in JSP 950 Leaflet 2-4-3

29
Please note the inclusion of patients who have subsequently died. Patients may sustain other injuries alongside
their mTBI/TBI and providing that the patients were alive at the point that they left the Royal Centre of Defence
Medicine (RCDM) they have been included in the response whether or not they have subsequently died of
connected or unconnected causes.
JTTR
An extract of the JTTR data was taken in September 2016 and was based on the following criteria: surviving UK
Service personnel who sustained an injury that contained the body region ‘head’. The list of Service personnel
with Abbreviated Injury Scale codes that would indicate they may have a TBI were reviewed by the Clinical
Information Exploitation Team who advised on their inclusion in the TBI statistics.
DMICP
An extract of data held on DMICP deployed was taken in September and a search for the following TBI Read
codes was conducted:
• DMSRC 132 – ‘Traumatic brain injury’
• DMSRC 133 – ‘Mild traumatic brain injury’ (as indicated in JSP 950 Leaflet 2-4-3)
The information presented in this response have been structured to release information into the public domain
in a way that contributes to the MOD accountability to the British public but which doesn’t risk breaching
individual’s rights to medical confidentiality. In line with JSP 200 (April 2016), and in keeping with the Office for
National Statistics Guidelines, all numbers less than five have been suppressed and presented as ‘~’ to prevent
the inadvertent disclosure of individual identities. Where there is only one cell in a row or column that is less
than five, the next smallest number (or numbers where there are tied values) has also been suppressed so that
numbers cannot simply be derived from totals.
If you are not satisfied with this response or you wish to complain about any aspect of the handling of your
request, then you should contact me in the first instance. If informal resolution is not possible and you are still
dissatisfied then you may apply for an independent internal review by contacting the Information Rights
Compliance team, 2nd Floor, MOD Main Building, Whitehall, SW1A 2HB (e-mail [email protected]). Please
note that any request for an internal review must be made within 40 working days of the date on which the
attempt to reach informal resolution has come to an end.
If you remain dissatisfied following an internal review, you may take your complaint to the Information
Commissioner under the provisions of Section 50 of the Freedom of Information Act. Please note that the
Information Commissioner will not investigate your case until the MOD internal review process has been
completed. Further details of the role and powers of the Information Commissioner can be found on the
30
Commissioner's website, http://www.ico.gov.uk.
I hope this is helpful.
Yours sincerely
Defence Statistics (Health) Head (B1)