pdf (unabridged) - asco.org - american society of clinical oncology
TRANSCRIPT
American Society of Clinical Oncology Clinical PracticeGuideline: Update on Adjuvant Endocrine Therapy forWomen With Hormone Receptor–Positive Breast CancerHarold J. Burstein, Ann Alexis Prestrud, Jerome Seidenfeld, Holly Anderson, Thomas A. Buchholz,Nancy E. Davidson, Karen E. Gelmon, Sharon H. Giordano, Clifford A. Hudis, Jennifer Malin,Eleftherios P. Mamounas, Diana Rowden, Alexander J. Solky, MaryFran R. Sowers, Vered Stearns,Eric P. Winer, Mark R. Somerfield, and Jennifer J. Griggs
From the Dana-Farber Cancer Institute,Boston, MA; American Society of Clini-cal Oncology, Alexandria, VA; BreastCancer Coalition of Rochester; Inter-lakes Oncology and Hematology, Roch-ester; Memorial Sloan-Kettering CancerCenter, New York, NY; M. D. AndersonCancer Center, Houston; Susan G.Komen for the Cure, Dallas, TX; Univer-sity of Pittsburgh Cancer Institute, Pitts-burgh, PA; British Columbia CancerAgency, Vancouver, British Columbia,Canada; Greater Los Angeles VeteransAffairs Healthcare System, Los Ange-les, CA; Aultman Health Foundation,Canton, OH; Johns Hopkins School ofMedicine, Baltimore, MD; and Univer-sity of Michigan and University of Mich-igan Comprehensive Cancer Center,Ann Arbor, MI.
Authors’ disclosures of potential con-flicts of interest and author contribu-tions are found at the end of thisarticle.
Corresponding author: American Soci-ety of Clinical Oncology, 2318 Mill Rd,Suite 800, Alexandria, VA 22314;e-mail: [email protected].
© 2010 by American Society of ClinicalOncology
A B S T R A C T
PurposeTo develop evidence-based guidelines, based on a systematic review, for endocrine therapy forpostmenopausal women with hormone receptor–positive breast cancer.
MethodsA literature search identified relevant randomized trials. Databases searched included MEDLINE,PREMEDLINE, and the Cochrane Collaboration Library, along with those of the American Societyof Clinical Oncology (ASCO) and San Antonio Breast Cancer Symposium (SABCS). The primaryoutcomes of interest were disease-free survival, overall survival, and time to contralateral breastcancer. Secondary outcomes included adverse events and quality of life. An expert panel reviewedthe literature, considering 12 major trials, and developed updated recommendations.
ResultsAn adjuvant treatment strategy incorporating an aromatase inhibitor (AI) as primary (initialendocrine therapy), sequential (using both tamoxifen and an AI in either order), or extended (AIafter 5 years of tamoxifen) therapy reduces the risk of breast cancer recurrence compared with 5years of tamoxifen alone. Data suggest that including an AI as primary monotherapy or assequential treatment after 2 to 3 years of tamoxifen yields similar outcomes. Tamoxifen and AIsdiffer in their adverse effect profiles, and these differences may inform treatment preferences.
ConclusionThe Update Committee recommends that postmenopausal women with hormone receptor–positive breast cancer consider incorporating an AI therapy at some point during adjuvanttreatment, either as upfront therapy or as sequential treatment after tamoxifen. The optimal timingand duration of endocrine treatment remain unresolved. The Update Committee supports carefulconsideration of adverse effect profiles and patient preferences in deciding whether and when toincorporate AI therapy.
INTRODUCTION
Adjuvant endocrine therapy reduces the risk ofbreast cancer recurrence and improves overallsurvival among women with hormone receptor–positive breast cancer. Tamoxifen is the historicstandard adjuvant endocrine therapy.1 On the basisof data for the role of aromatase inhibitors (AIs) astreatment for postmenopausal patients with meta-static breast cancer, multiple adjuvant trials com-paring AI-based therapy against tamoxifen wereinitiated and have been reported.
The first technology assessment for the use ofAIs in the adjuvant setting for women with hormonereceptor–positive breast cancer was published by theAmerican Society of Clinical Oncology (ASCO) in
20022 following release of early findings from theArimidex, Tamoxifen, Alone or in Combination(ATAC) trial. The technology assessment was up-dated in 20033 and 20044 on the basis of data fromtrials of primary, sequential, and extended adjuvanttreatment with AIs. Since then, additional reportsfrom large-scale trials of adjuvant endocrine therapyhave been published. Collectively, these develop-ments warranted a timely update and systematicliterature review of data on the efficacy of adju-vant endocrine therapy for women with hormonereceptor–positive breast cancer. Accordingly, theASCO Guideline Update Panel (Appendix TableA1) reconvened to develop an update.
ASCO’s practice guidelines reflect expert con-sensus based on clinical evidence and literature
© 2010 by American Society of Clinical Oncology 1

available at the time they are written and are intended to assist physi-cians in clinical decision making and to identify questions and settingsfor further research. Because of the rapid flow of scientific informationin oncology, new evidence may have emerged since the guideline wassubmitted for publication. Guidelines and assessments are not contin-ually updated and may not reflect the most recent evidence. Guide-lines address only the topics specifically identified in the guideline andare not applicable to interventions, disease, or stages of disease notspecifically identified. Guidelines cannot account for individual vari-ation among patients and cannot be considered inclusive of all propermethods of care or exclusive of other treatments. It is the responsibilityof the treating physician or other health care provider, relying onindependent experience and knowledge of the patient, to determinethe best course of treatment for the patient. Accordingly, adherence toany guideline is voluntary, with the ultimate determination regardingits application to be made by the physician in light of each patient’sindividual circumstances. ASCO guidelines describe the use of proce-dures and therapies in clinical practice and cannot be assumed toapply to the use of these interventions in the context of clinical trials.ASCO assumes no responsibility for any injury or damage to personsor property arising out of or related to any use of ASCO’s guidelines, orfor any errors or omissions.
UPDATE METHODOLOGY
Guideline Questions
In 2004, the ASCO technology assessment on the use of AIs in theadjuvant setting identified multiple unanswered questions regardingoptimal endocrine treatment for postmenopausal women.4 New dataon these remaining questions formed the foundation for this guidelineupdate. The Update Committee focused on the optimal adjuvantendocrine strategy with use of either tamoxifen, AIs, or both in se-quence; the appropriate duration of AI therapy; the long-term adverseeffects of AI therapy; identification of subpopulations who mightderive selective benefit from either AI- or tamoxifen-based treat-ments; efficacy of AIs among premenopausal women; and similaritiesor differences among commercially available third-generation AIs.
Literature Review and Analysis
Literature search strategy. The literature search for this updatewas facilitated by the systematic review completed by Cancer CareOntario (CCO) that reviewed available literature through May2007.5 ASCO guidelines staff conducted additional searches of theMEDLINE, PREMEDLINE, and Cochrane Collaboration Libraryelectronic databases for published articles from May 2007 throughFebruary 2009 (list of MEDLINE search terms, Appendix). In addi-tion, electronic databases for presentations, posters, and abstractspresented at the San Antonio Breast Cancer Symposium (SABCS) andASCO Annual Meetings in 2007 and 2008 were searched. Additionalsources were identified by hand-searching bibliographies of relevantarticles. Search terms included all the agents under consideration(“tamoxifen,” “anastrozole,” “exemestane,” “letrozole,” and “aro-matase inhibitors”) along with identified brand names (includingEuropean and North American versions). These terms were com-bined with the disease terminology “breast neoplasms,” “carcinoma,”“adenocarcinoma,” and “tumor.” The search was limited to phase IIIrandomized, controlled trials; meta-analyses; systematic reviews; and
existing practice guidelines. Other trial designs, including phase I or IItrials and either prospective or retrospective cohort studies, were ex-cluded. English-language studies available in full text and published inpeer-reviewed journals were included. Following the Update Com-mittee meeting, ASCO staff searched the programs for ASCO’s 2009Annual Meeting and the 2009 SABCS meeting to include updated datafrom the trials described therein.
Inclusion and exclusion criteria. Articles identified for inclusionin this systematic review met the following criteria: (1) the interven-tion was for the adjuvant therapy of breast cancer, (2) participantswere randomly assigned to any of the treatments described previously,and (3) reports included at least one of the following primary out-comes of interest: overall survival, disease-free survival, or breastcancer-specific survival. Three different treatment strategies wereidentified on the basis of the timing of AI therapy: initial endocrinetherapy (hereafter referred to as a primary adjuvant strategy), sequen-tial therapy with treatment divergence if the patient was disease-freefollowing 1 to 4 years of initial treatment with adjuvant endocrineagents (most often tamoxifen), or extended therapy with randomassignment if the patient was disease-free following 5 years of treat-ment with adjuvant tamoxifen. Trials that used earlier generations ofAIs, included neoadjuvant therapy, reported laboratory but not pri-mary disease-related outcomes of interest, or were not randomizedwere excluded. Trials that treated patients with metastatic breast can-cer were also excluded.
Data extraction. Reports and publications that met inclusioncriteria were identified in a first round of review by members of theASCO staff. The Update Committee co-chairs subsequently reviewedthe list of articles, and staff obtained full-text copies of papers thatsatisfied the inclusion criteria. ASCO staff completed full-text reviewof these articles, including assessment of inclusion and exclusion cri-teria. Articles that provisionally met inclusion criteria underwent dataextraction for patient characteristics, study design and quality, inter-ventions, outcomes, and adverse events. Evidence summary tableswere reviewed for accuracy and completeness by an ASCO staff mem-ber who was not involved in their original preparation.
Study quality and limitations of the literature. Twelve prospec-tive, randomized clinical trials originally identified by the co-chairswere the focus of this systematic review. These same trials were iden-tified in the CCO systematic review, as well as in a systematic reviewcompleted by the National Institute for Health Research (NIHR) inthe United Kingdom.6 No other relevant randomized studies wereidentified during the literature search and review. Four meta-analysesidentified from the search were also considered. The included trialshad varying methodologic quality.
Several important limitations of the existing literature were iden-tified. Of particular note is the timing of random assignment (Fig 1).Most of the sequential trials and all the extended trials randomlyassigned women who were free of recurrence through multipleyears of tamoxifen therapy, effectively excluding women with earlyrecurrence. For this reason, the patient populations in the sequentialand extended trials may differ importantly from one another and fromthose patients in the primary therapy studies. Another limitation is therelatively short follow-up time. Postmenopausal breast cancer is adisease with a long natural history, and disease recurrence decadesafter diagnosis is not uncommon. The longest available medianfollow-up in the trials included here is slightly more than 8 years;most studies have considerably shorter follow-up. For the majority
2 © 2010 by American Society of Clinical Oncology

TrialTime Since Random Assignment
Primary Adjuvant
Sequencing
Extended Adjuvant
60-month strategy; median follow-up 100 mos Postmenopausal, HR (+)
TAM ANA TAM + ANA
60-month strategy Median follow-up 76 mos (monotx), 71 mos (switching) Postmenopausal, HR (+)
LET TAM LET (2 yrs), TAM (3 yrs) TAM (2 yrs), LET (3 yrs)
36 month strategy Median follow-up 47.8 mos Premenopausal, ER and/ or PR (+)
TAM + GOS ANA + GOS TAM + GOS + ZOL ANA + GOS + ZOL
Primary random assignment60 month strategy; median follow-up 72 mos Postmenopausal, ER(+)/PR(+), no chemo
TAM TAM (2 yrs), ANA (3 yrs)
Randomly assigned to 2-3 yrs tx (5 yrs total)Median follow-up 64 mos Postmenopausal, ER(+), Node (+)
TAM (2-3 yrs) TAM
ANA
Primary random assignment60 month strategy; Follow-up 61 mos Postmenopausal, ER and/or PR (+)
TAM (2½ yrs), EXE (2½ yrs)
EXE
Randomly assigned to 2-3 yrs tx (5 yrs total)Median follow-up 55.7 mos Postmenopausal, ER(+) or unknown
TAM (2-3 yrs) TAM
EXE
Randomly assigned to 1-4 yrs tx (5 yrs total)Median follow-up 42 mos Postmenopausal
TAM (1-4 yrs) TAM
ANA
Randomly assigned to 3 yrs tx (5 yrs total)Median follow-up 30.1 mos Postmenopausal, hormone responsive
TAM (2 yrs) TAM
ANA
5 yrs of TAM, randomly assigned to 60 mos of txMedian follow-up 64 mos Postmenopausal, HR(+)
TAM LET
Placebo
5 yrs TAM, randomly assigned to 36 mos of txMedian follow-up 62.3 mos Postmenopausal, endocrine responsive
TAM ANA
Placebo
5 yrs of TAM, randomly assigned to 60 mos of txMedian follow-up 30 mos Postmenopausal, ER or PR (+)
TAM EXE
Placebo
-5 -4 -3 -2 -1 0 1 2 3 4 5
BIG 1-9839
ATAC118
ABCSG-1222
ABCSG-864
ITA119
TEAM32
IES120
NSAS BC-038
ARNO 95121
MA.17122
ABCSG-6a123
NSABP B-33124
Fig 1. Schema of included trials. ATAC, Arimidex, Tamoxifen, Alone or in Combination (trial); mos, months; HR (�), hormone receptor–positive; TAM, tamoxifen; ANA,anastrozole; BIG, Breast International Group; FU, follow-up; monotx, monotherapy; LET, letrozole; yrs, years; ABCSG, Austrian Breast and Colorectal Cancer StudyGroup; ER (�), estrogen receptor–positive; PR (�), progesterone receptor–positive; GOS, goserelin; ZOL, zoledronic acid; ABCSG, Austrian Breast and ColorectalCancer Study Group; Chemo, chemotherapy; ITA, Italian Tamoxifen Anastrozole (trial); tx, therapy; TEAM, Tamoxifen Exemestane Adjuvant Multinational (trial); EXE,exemestane; IES, Intergroup Exemestane Study; Unk, unknown; N-SAS, National Surgical Adjuvant Study (Group); ARNO, Arimidex-Nolvadex (trial); NSABP, NationalSurgical Adjuvant Breast and Bowel Project.
© 2010 by American Society of Clinical Oncology 3
of the efficacy outcomes across all studies, the median time to eventhas yet to be reached. The relatively modest number of events mayalso limit study conclusions.
The randomized trials for adjuvant AI therapy are large; in fact,these are some of the largest prospective cancer treatment trials everconducted. Nonetheless, the number of actual events was modestbecause of the generally favorable prognosis among eligible patients.Multiple subset analyses have been performed within these trials.Owing to the vagaries of data collection and patient participation, aswell as the distribution of clinical subsets, subgroup evaluations arehindered by relatively small sample sizes. Small sample size is also alimitation in analyzing available quality-of-life and other substudydata. These substudies frequently included fewer than 10% of pa-tients participating in the master trial. Finally, comparisons be-tween trials are hindered because of different definitions of studyend points such as disease-free survival.7 Studies were generally,but not entirely, consistent in their working definitions oftreatment- and breast cancer–related events, and they varied con-siderably in how investigators tabulated and reported efficacy andadverse effects. Specific instances of variation in efficacy definitionsinclude classification of in situ carcinoma, non– breast cancers, anddeaths from noncancer causes.
Consensus Development Based on Evidence
The Update Committee met twice, first in San Antonio in De-cember 2008 and again at ASCO Headquarters in April 2009. TheUpdate Committee was charged with updating the clinical ques-tions, reviewing evidence collected from the systematic review, anddrafting the new recommendations (Table 1). Additional work onthe guideline was primarily completed by the co-chairs and ASCOstaff. The draft guideline document was developed by the co-chairsand ASCO staff and reviewed by the entire Update Committee. Perstandard ASCO practice, the guideline was submitted to the Jour-nal of Clinical Oncology for peer review. The content of the guide-line was reviewed and approved by both the ASCO ClinicalPractice Guideline Committee and the Board of Directors be-fore publication.
Guideline and Conflicts of Interest
The Update Committee was assembled in accordance with ASCO’sConflict of Interest Management Procedures for Clinical PracticeGuidelines (“Procedures,” summarized at www.asco.org/guidelinescoi).Members completed ASCO’s disclosure form, which requires disclo-sure of financial and other interests relevant to the subject matter ofthe guideline, including relationships with commercial entitiesthat are reasonably likely to experience direct regulatory or com-mercial impact as the result of promulgation of the guideline.Categories for disclosure include employment relationships, con-sulting arrangements, stock ownership, honoraria, research fund-ing, and expert testimony. In accordance with the Procedures, themajority of the members of the Update Committee did not discloseany such relationships.
RESULTS
Summary of the Literature Review Results
The preliminary literature search identified 442 published arti-cles and 42 presentations, posters, or abstracts presented at either the
SABCS or the ASCO Annual Meeting (Fig 1). Of these, 52 provision-ally met the inclusion criteria and were obtained for full-text review.Three were excluded from data extraction for failure to meet inclusioncriteria, yielding 49 reports that underwent data extraction. These 49
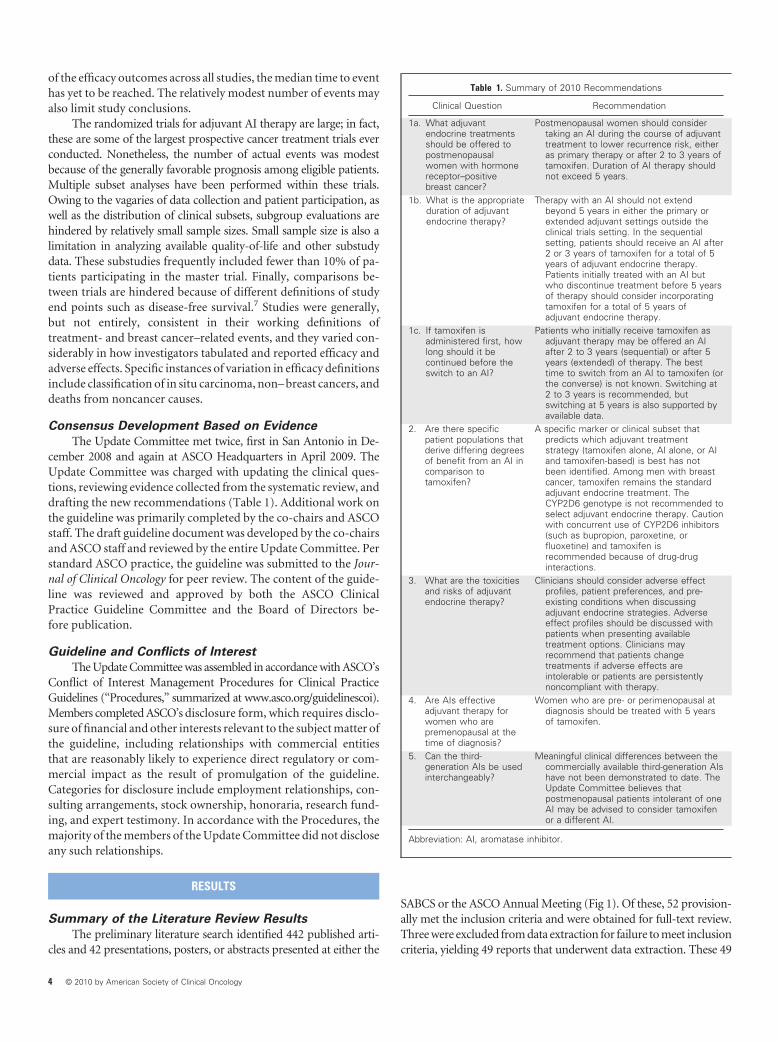
Table 1. Summary of 2010 Recommendations
Clinical Question Recommendation
1a. What adjuvantendocrine treatmentsshould be offered topostmenopausalwomen with hormonereceptor–positivebreast cancer?
Postmenopausal women should considertaking an AI during the course of adjuvanttreatment to lower recurrence risk, eitheras primary therapy or after 2 to 3 years oftamoxifen. Duration of AI therapy shouldnot exceed 5 years.
1b. What is the appropriateduration of adjuvantendocrine therapy?
Therapy with an AI should not extendbeyond 5 years in either the primary orextended adjuvant settings outside theclinical trials setting. In the sequentialsetting, patients should receive an AI after2 or 3 years of tamoxifen for a total of 5years of adjuvant endocrine therapy.Patients initially treated with an AI butwho discontinue treatment before 5 yearsof therapy should consider incorporatingtamoxifen for a total of 5 years ofadjuvant endocrine therapy.
1c. If tamoxifen isadministered first, howlong should it becontinued before theswitch to an AI?
Patients who initially receive tamoxifen asadjuvant therapy may be offered an AIafter 2 to 3 years (sequential) or after 5years (extended) of therapy. The besttime to switch from an AI to tamoxifen (orthe converse) is not known. Switching at2 to 3 years is recommended, butswitching at 5 years is also supported byavailable data.
2. Are there specificpatient populations thatderive differing degreesof benefit from an AI incomparison totamoxifen?
A specific marker or clinical subset thatpredicts which adjuvant treatmentstrategy (tamoxifen alone, AI alone, or AIand tamoxifen-based) is best has notbeen identified. Among men with breastcancer, tamoxifen remains the standardadjuvant endocrine treatment. TheCYP2D6 genotype is not recommended toselect adjuvant endocrine therapy. Cautionwith concurrent use of CYP2D6 inhibitors(such as bupropion, paroxetine, orfluoxetine) and tamoxifen isrecommended because of drug-druginteractions.
3. What are the toxicitiesand risks of adjuvantendocrine therapy?
Clinicians should consider adverse effectprofiles, patient preferences, and pre-existing conditions when discussingadjuvant endocrine strategies. Adverseeffect profiles should be discussed withpatients when presenting availabletreatment options. Clinicians mayrecommend that patients changetreatments if adverse effects areintolerable or patients are persistentlynoncompliant with therapy.
4. Are AIs effectiveadjuvant therapy forwomen who arepremenopausal at thetime of diagnosis?
Women who are pre- or perimenopausal atdiagnosis should be treated with 5 yearsof tamoxifen.
5. Can the third-generation AIs be usedinterchangeably?
Meaningful clinical differences between thecommercially available third-generation AIshave not been demonstrated to date. TheUpdate Committee believes thatpostmenopausal patients intolerant of oneAI may be advised to consider tamoxifenor a different AI.
Abbreviation: AI, aromatase inhibitor.
4 © 2010 by American Society of Clinical Oncology

reported either findings from one of the 12 trials8-50 or were systematicreviews or meta-analyses of the same.5,51-55 Thirteen additional arti-cles with primary data reports from key studies published before thedate range searched were retrieved for data to complement extraction.Five reports available after completion of the initial search, includingfour presentations from the 2009 SABCS conference, were also con-sidered; longer follow-up was presented for both the Tamoxifen Ex-emestane Adjuvant Multicenter (TEAM) trial and the IntergroupExemestane Study (IES).56,57
Twelve randomized trials, including three trials of primary ther-apy (ATAC, Breast International Group [BIG] 1-98, and AustrianBreast and Colorectal Cancer Study Group ABCSG-12), seven trials ofsequential therapy (IES, BIG 1-98, ABCSG-8, Arimidex-Nolvadex[ARNO] 95, Italian Tamoxifen Anastrozole [ITA], National SurgicalAdjuvant Study [N-SAS] BC-03, and TEAM), and three trials of ex-tended adjuvant therapy (MA.17, National Surgical Adjuvant Breastand Bowel Project NSABP B-33, and ABCSG-6a), investigated incor-poration of an AI as adjuvant therapy. All of these compared outcomesagainst the historical standard of 5 years of tamoxifen therapy, with theexception of the TEAM trial, which compared a tamoxifen sequencefollowed by an AI against an AI alone. Four meta-analyses51-53,55 andtwo systematic reviews5,54 were identified.
GUIDELINE RECOMMENDATIONS
Clinical question 1a. What adjuvant endocrine treatments shouldbe offered to postmenopausal women with hormone receptor–positivebreast cancer?
Recommendation 1a. The Update Committee recommends, onthe basis of data from randomized, controlled trials, that most post-menopausal women consider taking an AI during the course of adju-vant treatment to lower recurrence risk, either as primary therapy orafter 2 to 3 years of tamoxifen—strategies that yield equivalent out-comes in prospective studies. Duration of AI therapy should notexceed 5 years.
Literature update and discussion 1a. At the time of the last up-date, data were available from four randomized trials that evaluatedadjuvant treatment incorporating AI therapy against 5 years of tamox-ifen. On the basis of the available data, the 2004 Update Committeenoted that “adjuvant therapy for postmenopausal women with hor-mone receptor–positive breast cancer should include an AI to lowerthe risk of tumor recurrence. Neither the optimal timing nor durationof AI therapy is established.”4
Since then, reports of related studies have emerged, and datafrom the original trials have matured. In comparison to 5 years of
Table 2. Disease-Free Survival
Trial Arm
MedianFollow-Up(months
Range(months)
No. of PatientsObserved
Disease-Free SurvivalEvents
HR 95% CI P
AI Comparator
AI Comparator No. % No. %
PrimaryATAC21 ANA v TAM ITT 100 0-126 3,125 3,116 817 26.1 887 28.5 0.90 0.82 to 0.99 .025BIG 1-9842 LET v TAM ITT 76 2,463 2,459 509 20.7 565 23.0 0.88 0.78 to 0.99a .03ABCSG-1223 ANA v TAM 47.8 903 900 72 8.0 65 7.2 1.10 0.78 to 1.53 .59
SequentialBIG 1-9842 TAM/LET v LET 71 1,548 1,546 259 16.7 248 16.0 1.05 0.84 to 1.32b NR
LET/TAM v LET 71 1,540 1,546 236 15.3 248 16.0 0.96 0.76 to 1.21b NRABCSG-830 TAM/ANA v TAM ITT 72 1,865 1,849 227 12.2 261 14.1 0.85 0.71 to 1.01c,d .067ITA10 ITT 64 12-93 223 225 39 17.5 63 28 0.57 0.38 to 0.85e .005TEAM57 TAM/EXE v EXE ITT 61 4,868 4,898 714 712 0.97 0.88 to 1.08 .604IES14 ITT 55.7 0-89.7 2,352 2,372 354 455 0.76 0.66 to 0.88 � .001N-SAS BC-039 42 3.2-60 347 349 26 7.5 37 10.6 0.69 0.42 to 1.14 .14f
ARNO 9534 30.1 � 12 to � 84 489 490 38 7.8 56 11.4 0.66 0.44 to 1.00 .049Extended
MA.1726 ITTg 64 16-95 2,583 2,587 164 6.3 235 9.1 0.68 0.55 to 0.83 � .001ABCSG-6a31 62.3 386 466 30 7.8 57 12.2 0.62 0.40 to 0.96h .031NSABP B-3337 30 783 779 37 4.7 52 6.7 0.68 .07
NOTE. Percent calculated as number of events divided by number of patients observed.Abbreviations: AI, aromatase inhibitor; HR, hazard ratio; ATAC, Arimidex, Tamoxifen, Alone or in Combination (trial); ANA, anastrozole; TAM, tamoxifen; ITT, intent
to treat; BIG, Breast International Group; LET, letrozole; ABCSG, Austrian Breast and Colorectal Cancer Study Group; NR, not reported; ITA, Italian TamoxifenAnastrozole (trial); TEAM, Tamoxifen Exemestane Adjuvant Multinational (trial); EXE, exemestane; IES, Intergroup Exemestane Study; N-SAS, National SurgicalAdjuvant Study (Group); ARNO, Arimidex-Nolvadex (trial); NSABP, National Surgical Adjuvant Breast and Bowel Project.
aAnalysis includes only patients from monotherapy arms; crossovers not censored.b99% CIs used to account for multiple comparisons.cRelapse-free survival includes local and distant recurrence, contralateral breast cancer, and death without recurrence.dPatients who crossed over were censored at time of crossover.eEvent-free survival includes locoregional or distant recurrence, second primary (including contralateral breast cancer), and deaths without recurrence.fTwo different P values reported (P � .06 in abstract, P � .14 on poster).gSeventeen patients omitted from ITT analysis.hRecurrence-free survival.
© 2010 by American Society of Clinical Oncology 5
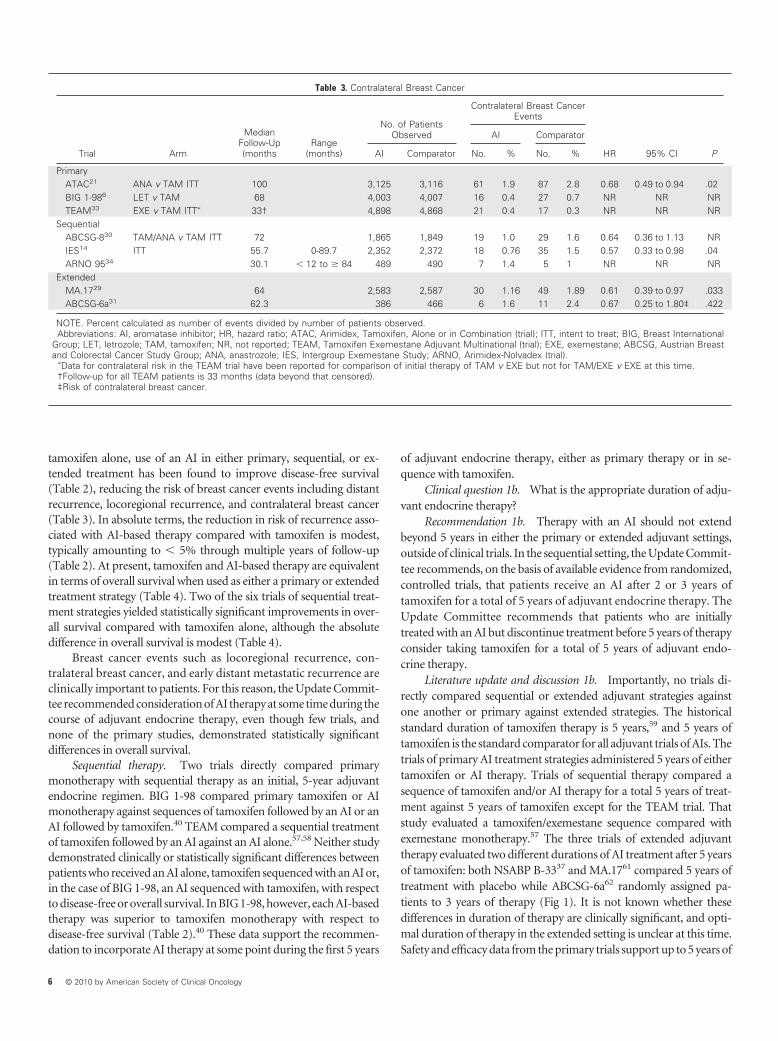
tamoxifen alone, use of an AI in either primary, sequential, or ex-tended treatment has been found to improve disease-free survival(Table 2), reducing the risk of breast cancer events including distantrecurrence, locoregional recurrence, and contralateral breast cancer(Table 3). In absolute terms, the reduction in risk of recurrence asso-ciated with AI-based therapy compared with tamoxifen is modest,typically amounting to � 5% through multiple years of follow-up(Table 2). At present, tamoxifen and AI-based therapy are equivalentin terms of overall survival when used as either a primary or extendedtreatment strategy (Table 4). Two of the six trials of sequential treat-ment strategies yielded statistically significant improvements in over-all survival compared with tamoxifen alone, although the absolutedifference in overall survival is modest (Table 4).
Breast cancer events such as locoregional recurrence, con-tralateral breast cancer, and early distant metastatic recurrence areclinically important to patients. For this reason, the Update Commit-tee recommended consideration of AI therapy at some time during thecourse of adjuvant endocrine therapy, even though few trials, andnone of the primary studies, demonstrated statistically significantdifferences in overall survival.
Sequential therapy. Two trials directly compared primarymonotherapy with sequential therapy as an initial, 5-year adjuvantendocrine regimen. BIG 1-98 compared primary tamoxifen or AImonotherapy against sequences of tamoxifen followed by an AI or anAI followed by tamoxifen.40 TEAM compared a sequential treatmentof tamoxifen followed by an AI against an AI alone.57,58 Neither studydemonstrated clinically or statistically significant differences betweenpatients who received an AI alone, tamoxifen sequenced with an AI or,in the case of BIG 1-98, an AI sequenced with tamoxifen, with respectto disease-free or overall survival. In BIG 1-98, however, each AI-basedtherapy was superior to tamoxifen monotherapy with respect todisease-free survival (Table 2).40 These data support the recommen-dation to incorporate AI therapy at some point during the first 5 years
of adjuvant endocrine therapy, either as primary therapy or in se-quence with tamoxifen.
Clinical question 1b. What is the appropriate duration of adju-vant endocrine therapy?
Recommendation 1b. Therapy with an AI should not extendbeyond 5 years in either the primary or extended adjuvant settings,outside of clinical trials. In the sequential setting, the Update Commit-tee recommends, on the basis of available evidence from randomized,controlled trials, that patients receive an AI after 2 or 3 years oftamoxifen for a total of 5 years of adjuvant endocrine therapy. TheUpdate Committee recommends that patients who are initiallytreated with an AI but discontinue treatment before 5 years of therapyconsider taking tamoxifen for a total of 5 years of adjuvant endo-crine therapy.
Literature update and discussion 1b. Importantly, no trials di-rectly compared sequential or extended adjuvant strategies againstone another or primary against extended strategies. The historicalstandard duration of tamoxifen therapy is 5 years,59 and 5 years oftamoxifen is the standard comparator for all adjuvant trials of AIs. Thetrials of primary AI treatment strategies administered 5 years of eithertamoxifen or AI therapy. Trials of sequential therapy compared asequence of tamoxifen and/or AI therapy for a total 5 years of treat-ment against 5 years of tamoxifen except for the TEAM trial. Thatstudy evaluated a tamoxifen/exemestane sequence compared withexemestane monotherapy.57 The three trials of extended adjuvanttherapy evaluated two different durations of AI treatment after 5 yearsof tamoxifen: both NSABP B-3337 and MA.1761 compared 5 years oftreatment with placebo while ABCSG-6a62 randomly assigned pa-tients to 3 years of therapy (Fig 1). It is not known whether thesedifferences in duration of therapy are clinically significant, and opti-mal duration of therapy in the extended setting is unclear at this time.Safety and efficacy data from the primary trials support up to 5 years of
Table 3. Contralateral Breast Cancer
Trial Arm
MedianFollow-Up(months
Range(months)
No. of PatientsObserved
Contralateral Breast CancerEvents
HR 95% CI P
AI Comparator
AI Comparator No. % No. %
PrimaryATAC21 ANA v TAM ITT 100 3,125 3,116 61 1.9 87 2.8 0.68 0.49 to 0.94 .02BIG 1-986 LET v TAM 68 4,003 4,007 16 0.4 27 0.7 NR NR NRTEAM33 EXE v TAM ITT� 33† 4,898 4,868 21 0.4 17 0.3 NR NR NR
SequentialABCSG-830 TAM/ANA v TAM ITT 72 1,865 1,849 19 1.0 29 1.6 0.64 0.36 to 1.13 NRIES14 ITT 55.7 0-89.7 2,352 2,372 18 0.76 35 1.5 0.57 0.33 to 0.98 .04ARNO 9534 30.1 � 12 to � 84 489 490 7 1.4 5 1 NR NR NR
ExtendedMA.1729 64 2,583 2,587 30 1.16 49 1.89 0.61 0.39 to 0.97 .033ABCSG-6a31 62.3 386 466 6 1.6 11 2.4 0.67 0.25 to 1.80‡ .422
NOTE. Percent calculated as number of events divided by number of patients observed.Abbreviations: AI, aromatase inhibitor; HR, hazard ratio; ATAC, Arimidex, Tamoxifen, Alone or in Combination (trial); ITT, intent to treat; BIG, Breast International
Group; LET, letrozole; TAM, tamoxifen; NR, not reported; TEAM, Tamoxifen Exemestane Adjuvant Multinational (trial); EXE, exemestane; ABCSG, Austrian Breastand Colorectal Cancer Study Group; ANA, anastrozole; IES, Intergroup Exemestane Study; ARNO, Arimidex-Nolvadex (trial).
�Data for contralateral risk in the TEAM trial have been reported for comparison of initial therapy of TAM v EXE but not for TAM/EXE v EXE at this time.†Follow-up for all TEAM patients is 33 months (data beyond that censored).‡Risk of contralateral breast cancer.
6 © 2010 by American Society of Clinical Oncology

AI therapy as a primary adjuvant strategy, a duration also used in twotrials of extended therapy after 5 years of tamoxifen.
The treatment regimen for patients in the sequencing trialsspanned 5 years. Thus, no data support clinical benefits for durationsof AIs longer than 2 or 3 years in the context of a sequencing strategy.In the BIG 1-98 and TEAM trials, patients who received a total of 5years of sequential therapy that included tamoxifen (2 to 3 years)followed by an AI (2 to 3 years) had clinical outcomes that were notsignificantly different from those for patients who received AI mono-therapy.40,57,58 BIG 1-98 also included an arm with an AI followed bytamoxifen with similar outcomes. These data suggest that shorterdurations of AI treatment might be as effective as longer durations inwomen who receive a total of 5 years of endocrine therapy in thecontext of a sequencing approach.
Data from randomized, controlled trials demonstrate thatwomen who receive primary AI therapy should be treated for a total of5 years; women who initially receive tamoxifen and switch to an AIshould also receive at least five total years of endocrine therapy. Noavailable data evaluate durations of AI therapy in excess of 5 yearsamong patients receiving sequential therapy. Women who receiveextended adjuvant therapy should receive 8 to 10 years of total endo-crine treatment: 5 years of tamoxifen followed by 3 to 5 years of an AI.
The Update Committee acknowledges that these recommenda-tions yield an unfamiliar pattern of different durations of adjuvantendocrine treatment based on the treatment strategy used. This is afunction of offering an AI at a different time point in accordance witheach strategy. The recommended limit on AI treatment is 5 years total,
across strategies. Two trials—MA.17R and NSABP B-42—are evalu-ating whether longer durations of AI therapy improve outcomes, butresults are not yet available.
Clinical question 1c. If tamoxifen is administered first, how longshould it be continued before the switch to an AI?
Recommendation 1c. The Update Committee recommendsthat, on the basis of available evidence from randomized, controlledtrials, patients who initially receive tamoxifen as adjuvant therapy maybe offered an AI after 2 to 3 years of therapy (sequential) or after 5 yearsof therapy (extended). The time to switch from an AI to tamoxifen (orthe converse) that maximally improves outcomes is not known fromavailable direct evidence. The Update Committee recommendsswitching at 2 to 3 years on the basis of data from sequential trials thatused this strategy. Switching at 5 years is also a strategy supported bythe extended adjuvant randomized trials.
Literature update and discussion 1c. Most, but not all, trials ofsequential therapy switched patients from tamoxifen to an AI after 2 to3 years of therapy. Some specified an exact crossover point, whileothers permitted switching within a broad window. Trials of extendedtherapy enrolled patients who already received an average of 5 years oftamoxifen (Fig 1). Of the sequencing and switching trials, only BIG1-98,63 TEAM,32 and ABCSG-864 enrolled patients before commence-ment of adjuvant endocrine therapy. The other sequencing trials andall the extended trials randomly assigned patients free of recurrenceafter multiple years of tamoxifen therapy. Data are lacking to establishthe best duration of tamoxifen therapy before switching to an AI.
Table 4. Overall Survival
Trial Arm
MedianFollow-Up(months
Range(months
No. of PatientsObserved
Overall Survival Deaths
HR 95% CI P
AI Comparator
AI Comparator No. % No. %
PrimaryATAC21 ANA v TAM ITT 100 3,125 3,116 629 20.1 624 20.0 1.00 0.89 to 1.12 .99BIG 1-9842 LET v TAM ITT 76 2,463 2,459 303 12.3 343 14.0 0.81 0.69 to 0.94� .08ABCSG-1223 ANA v TAM 47.8 903 900 27 3.0 15 1.7 1.8 0.95 to 3.38 .70
SequentialABCSG-830 TAM/ANA v TAM ITT 72 1,865 1,849 138 7.4 165 9.0 0.78 0.62 to 0.98† .032BIG 1-9842 TAM/LET v LET 71 1,548 1,546 154 9.9 137 8.9 1.13 0.83 to 1.53‡ NR
LET/TAM v LET 71 1,540 1,546 123 8.0 137 8.9 0.90 0.65 to 1.24‡ NRITA10 ITT 64 12-93 223 225 12 5.4 21 9.3 0.56 0.28 to 1.15 .1TEAM57 TAM/EXE v EXE ITT 61 4,868 4,898 NR (90.6%
survival)NR (90.5%
survival)1.00 0.89 to 1.14 .999
IES14 ITT 55.7 0-89.7 2,352 2,372 222 9.4 261 11.0 0.85 0.71 to 1.02 .08N-SAS BC-039 42 3.2-60 347 349 NR NR NR .59ARNO 9534 30.1 � 12 to � 84 489 490 15 3.1 28 5.7 0.53 0.28 to 0.99 .045
ExtendedMA.1726 ITT§ 64 16-95 2,583 2,587 154 6.0 155 6.0 0.98 0.78 to 1.22 .853ABCSG-6a31 62.3 386 466 40 10.4 55 11.8 0.89 0.59 to 1.34 .570NSABP B-3337 30 783 779 16 2.0 13 1.7 NR NR
NOTE. Percent calculated as number of events divided by number of patients observed.Abbreviations: AI, aromatase inhibitor; HR, hazard ratio; ATAC, Arimidex, Tamoxifen, Alone or in Combination (trial); ANA, anastrozole; TAM, tamoxifen; ITT, intent
to treat; BIG, Breast International Group; LET, letrozole; ABCSG, Austrian Breast and Colorectal Cancer Study Group; NR, not reported; ITA, Italian TamoxifenAnastrozole (trial); TEAM, Tamoxifen Exemestane Adjuvant Multinational (trial); EXE, exemestane; IES, Intergroup Exemestane Study; N-SAS, National SurgicalAdjuvant Study (Group); ARNO, Arimidex-Nolvadex (trial); NSABP, National Surgical Adjuvant Breast and Bowel Project.
�Analysis includes only patients from monotherapy arms; crossovers not censored.†Patients who crossed over were censored.‡99% CIs used to account for multiple comparisons.§Seventeen patients omitted from ITT analysis.
© 2010 by American Society of Clinical Oncology 7

Three trials of extended adjuvant therapy using AI treatment for3 to 5 years after 5 years of tamoxifen demonstrated that extendedtherapy can lower the risk of breast cancer recurrence (Table 2 andAppendix Table A2) and contralateral breast cancer (Table 3) but doesnot improve overall survival (Table 4). The Update Committee rec-ommends extended therapy with an AI for postmenopausal patientswho complete 5 years of tamoxifen.
For a newly diagnosed patient or a patient who has been ontamoxifen for 2 to 5 years, it is not known whether switching fromtamoxifen to an AI earlier or later is more effective for long-termdisease-free survival. Lacking direct comparative data, the UpdateCommittee recommends considering a switch from tamoxifen to anAI after 2 or 3 years of tamoxifen therapy. This recommendation isinformed by several observations. First, both ARNO 95 and ABCSG-8,which transitioned patients from tamoxifen to an AI after 2 or 3 years,demonstrated survival advantages, as did a meta-analysis of sequentialtrials30,34,65 (Table 4). Second, each AI-based arm of BIG 1-98, includ-ing those with switching at 2 years, had improved disease-free survivalrelative to 5 years of tamoxifen40 (Table 2). These findings suggest thatincorporating an AI into the adjuvant treatment regimen at somepoint during the first 5 years of endocrine therapy yields clinicalimprovements compared with 5 years of tamoxifen monotherapy,which justifies considering a switch between years 2 and 3. Data thatcompare switching at 2 to 3 or at 5 years are not available. Cliniciansand patients may reasonably opt to consider extended therapy basedon individual considerations.
Clinical question 2. Are there specific patient populations thatderivedifferingdegreesofbenefitfromanAIincomparisontotamoxifen?
Recommendation 2. Direct evidence from randomized trialsdoes not identify a specific marker or clinical subset that predictedwhich adjuvant treatment strategy, tamoxifen or AI monotherapy orsequential therapy, would maximally improve outcomes for a givenpatient. Among men with breast cancer, tamoxifen remains the stan-dard adjuvant endocrine treatment.
The Update Committee recommends against using CYP2D6genotype to select adjuvant endocrine therapy. The Update Commit-tee encourages caution with concurrent use of CYP2D6 inhibitors(such as bupropion, paroxetine, fluoxetine; Table 5) and tamoxifenbecause of the known drug-drug interactions.
Literature update and discussion 2. A vast historical experienceestablished prognostic markers for outcomes in early-stage breast
cancer treated with tamoxifen. Endocrine therapy is effective onlyamong patients with tumors that express estrogen receptor (ER)and/or progesterone receptor (PR) hormone receptors.66,67 Tumorsize, nodal status, grade, quantitative levels of hormone receptor ex-pression, HER2 overexpression, markers of proliferation, and the21-gene recurrence score68 are prognostic factors among patients whoreceive endocrine therapy.38 These prognostic markers help to definerelative risk of recurrence in the first 5 to 10 years after diagnosis.
The major trials of adjuvant AI therapy included patients withhormone receptor–positive tumors, generally irrespective of othermarkers or staging. Two trials (ABCSG-8 and ABCSG-12) limitedaccrual to patients with lower-grade tumors.22,64 Retrospective subsetanalyses (Appendix Table A3) from some trials considered a variety ofprognostic factors among patients receiving tamoxifen or AI-basedtherapy. In these retrospective studies, tumor size, nodal status, age,quantitative ER and PR levels, HER2 expression,45,65 grade, Ki-67,50
and the 21-gene recurrence score69 seem to serve as prognostic factorsfor risk of breast cancer recurrence among patients receiving eithertamoxifen or AI therapy (Table 6).
Traditional assumptions about proportionate risk reductionachieved with adjuvant therapy suggest that differences in clinicaloutcome between various treatments are likely to be of greaterabsolute magnitude among patients with higher-risk breast can-cers. Conversely, among women with lower-risk tumors, differencesin outcomes between AI-based therapies and tamoxifen, or betweenprimary or sequential use of AIs, are likely to be smaller if present at all.Emerging data from BIG 1-98 seem to validate these traditional as-sumptions among postmenopausal women treated with tamoxifenand/or AIs.38,70 However, the available retrospective subset analysesare constrained by missing data on some patients, technical limita-tions in the performance of correlative marker testing, multiple hy-pothesis testing, varying assays used by different trials, and lack ofprospective, corroborative data.
On the basis of evidence from randomized clinical trials andconsistent with the recommendation, the Update Committee recom-mended treatment with either upfront use of an AI or sequentialtherapy with tamoxifen followed by an AI (or vice versa) for post-menopausal women, irrespective of any specific clinical subset orprognostic marker studied to date in retrospective analysis.
Male breast cancer. Only women were eligible for the adjuvanttrials of postmenopausal endocrine therapy with AIs. Thus, there is noevidence to evaluate the efficacy of adjuvant AI therapy in men. Ta-moxifen remains the standard adjuvant endocrine therapy for malebreast cancer.71
CYP2D6 genotype. Accumulating data suggest that variability intamoxifen metabolism may affect serum levels of the tamoxifen me-tabolite endoxifen, which may in turn affect the likelihood of cancerrecurrence in patients treated with tamoxifen.71-78 Factors that con-tribute to this variability include concurrent use of other drugs thatinhibit the CYP2D6 isoenzyme, which converts tamoxifen to endox-ifen, and pharmacogenetic variation (polymorphisms) in CYP2D6alleles. It is not yet known whether variations in CYP2D6 genotypeaccount for differences in outcomes among patients treated with ta-moxifen. Available data on CYP2D6 pharmacogenetics are insuffi-cient to recommend testing as a tool to determine the optimaladjuvant endocrine strategy.
The Update Committee recognized the accumulating evidenceon drug-drug interactions between tamoxifen and other drugs that
Table 5. Commonly Used CYP2D6 Inhibitors
Strong inhibitorsBupropionFluoxetineParoxetineQuinidine
Moderate inhibitorsDuloxetineTerbinafine
Weak inhibitorsAmiodaroneCimetidineSertraline
Flockhart DA: http://medicine.iupui.edu/clinpharm/ddis/table.asz.
8 © 2010 by American Society of Clinical Oncology

inhibit CYP2D6 (such as bupropion, paroxetine, or fluoxetine; Table5). The evidence linking such interactions to clinically importantoutcomes for breast cancer patients, however, remains limited andindirect. Alternatives are available for both tamoxifen and CYP2D6inhibitors. The Update Committee suggests that patients clearlybenefiting from known CYP2D6 inhibitors might consider avoid-ing tamoxifen because of potential pharmacologic interactions.Conversely, women who take tamoxifen may prefer to avoid concur-rent use of known CYP2D6 inhibitors if suitable treatment alternativesare available.
Clinical question 3. What are the toxicities and risks of adjuvantendocrine therapy?
Recommendation 3. The Update Committee recommends thatclinicians consider adverse effect profiles, patient preferences, andpre-existing conditions when recommending an adjuvant endocrinestrategy for postmenopausal women. Clinicians should discuss ad-verse effect profiles when presenting available treatment options topatients. The Update Committee suggests that clinicians considerrecommending that patients change treatment if adverse effects areintolerable or if patients are persistently noncompliant with therapy.
Literature update and discussion 3. Accumulated experiencewith AIs, including data from randomized clinical trials and otherreports in the clinical literature, has increasingly clarified the adverseeffect profile for this drug class. These agents are generally well toler-ated but are associated with specific toxicities, including effects onbone, cardiovascular, and gynecologic health. The Update Committeedid not find evidence that AI therapy is less toxic or better toleratedthan tamoxifen. Both drug classes have distinct adverse effect profilesthat are relevant to individualizing therapy for patients.
Both tamoxifen and AIs are generally well-tolerated therapies.Substudies from the large, randomized trials show generally well-maintained and similar quality-of-life scores in women receiving anyof the adjuvant endocrine therapies.19,37,44,49,79-82 The differing ad-verse effect profiles are functions of differing mechanisms of action.Tamoxifen is a selective ER modulator with mixed pro- and anties-trogenic activities, while AIs achieve near complete estrogen depri-vation in postmenopausal women. The intensity and severity of themost common adverse effects are mild to moderate for the major-ity of patients; serious adverse effects are rare. The long-termadverse effect profiles for tamoxifen-treated patients are estab-lished from historical literature.83 Late effects of AI therapy remainto be fully characterized.
Appendix Tables A4 through A8 include an abbreviated list of theadverse effects tabulated from the therapies evaluated in the prospec-tive, randomized trials discussed herein. Four main categories ofsymptoms are detailed: cardiovascular, musculoskeletal, gynecologic,and climacteric.
Tamoxifen and AIs have differing effects on cardiovascularhealth. Data suggest that AIs are associated with increased cardiovas-cular disease, possibly including ischemic cardiac disease. Differencesbetween AIs and tamoxifen in the incidence of serious cardiac disease,however, are less than 1% at this time (Appendix Tables A4 andA5).41,52 In comparison to tamoxifen, AI therapy is associated with anincreased risk of both hypercholesterolemia and hypertension. Dataare insufficient to exclude clinically significant differences in cardio-vascular disease associated with the AIs. Tamoxifen is associated withan increased risk of venous thromboembolic events, giving rise to a1% to 2% greater risk of deep vein thrombosis compared with that of
women taking AIs (Appendix Table A5).52 Data on the relative inci-dence of stroke with either tamoxifen or an AI are inconclusive.Longer follow-up is required to better characterize the potential car-diac toxicity of AI therapy.
Tamoxifen and AIs have differing effects on musculoskeletalhealth and symptoms. In comparison to tamoxifen, AIs are associatedwith greater loss of bone mineral density18 and bone fracture (Appen-dix Table A6). Discontinuation of AI therapy seems to halt further lossof bone mineral density.18,22 The incidence of osteoporosis and bonefractures84 differs by approximately 2% to 4% in trials of primaryadjuvant endocrine therapy comparing tamoxifen with an AI12,20,22;the risk is increased with AI therapy. Randomized clinical trials suggestthat bisphosphonate therapy can mitigate AI-associated loss of bonedensity.22,85-87 The long-term impact of AI treatment on osteoporosisrisk and fracture risk has not been characterized.
With maturation of clinical data and accumulating clinical expe-rience, it is clear that AIs cause a musculoskeletal/arthralgia syndrome.This syndrome is characterized by bone and joint symptoms, fre-quently described by patients as pain, stiffness, or achiness that issymmetric and not associated with other signs of rheumatologicdisorders.47,88-91 The prevalence of this syndrome is unclear, though itseems widespread; most patients have mild to moderate symptoms.There are no known interventions of proven value for AI-associatedmusculoskeletal symptoms. Discontinuation of AI therapy usuallyrelieves symptoms within 8 to 10 weeks.
Tamoxifen and AIs have differing effects on gynecologic health.Adverse events are more common among women receiving tamox-ifen. In general, tamoxifen is associated with an increased risk ofuterine cancer, benign endometrial pathology (including bleeding,polyps, and hyperplasia), hysterectomy, and vaginal discharge (Ap-pendix Table A7). With 5 years of tamoxifen therapy, the risk ofuterine cancer is � 1%;30 a larger percentage of patients will havebenign endometrial findings or hysterectomy.92,93 Both tamoxifenand AIs are associated with climacteric symptoms. AIs seem to be lessassociated with hot flashes than tamoxifen (Appendix Table A8).ATAC and MA.17 both reported a lower incidence of vaginal drynessamong patients treated with tamoxifen than among those treated withAIs.79,82 IES, alternatively, documented similar rates of vaginal drynessamong both tamoxifen- and AI-treated patients,19 and the TEAMtrial57 reported a statistically higher rate of vaginal dryness in patientswho received sequential tamoxifen and exemestane compared withexemestane alone. Findings were mixed with respect to loss of libido:MA.17 and IES noted similar rates while AI-treated patients hadhigher rates in the ATAC trial.32,80,81 Patients who were given ex-tended adjuvant endocrine therapy with an AI reported more climac-teric symptoms than women given placebo therapy.
Evaluation of other adverse effects suggests no major differencesin the incidence or severity of conditions such as skin rashes, eyesymptoms, neurologic function, headache, fatigue, GI symptoms,psychiatric conditions, or cognitive function between AIs and tamox-ifen. No direct data indicate that changing drug agents or classesalleviates treatment-related symptoms. However, on the basis of lim-ited clinical experience, the Update Committee favored switchingdrugs if needed to promote compliance with therapy among patientswhose treatment-related symptoms were intolerable.
Clinical question 4. Are AIs effective adjuvant therapy forwomen who are premenopausal at the time of diagnosis?
© 2010 by American Society of Clinical Oncology 9

Recommendation 4. The Update Committee recommends thatwomen who are pre- or perimenopausal at the time of breast cancerdiagnosis be treated with 5 years of tamoxifen.
Additional considerations. The Update Committee recom-mends that clinicians use caution in evaluating menopausal status ofpatients who are pre- or perimenopausal at diagnosis. Unequivocaldetermination of menopausal status may be challenging to prove.Even among women who have not experienced menses for more than1 year, laboratory testing is inadequate because patients may recoverovarian function. This particularly applies to those patients who expe-rience chemotherapy- or tamoxifen-induced amenorrhea.
Literature update and discussion 4. AI therapy has been shown tobe effective only in postmenopausal women. In fact, this class ofdrugs is contraindicated in premenopausal women. All of theadjuvant AI trials, with the exception of ABCSG-12, excluded pre-menopausal women. All patients accrued to ABCSG-12 were treatedwith gonadotropin-releasing hormone agonist therapy to achieve apostmenopausal state and were randomly assigned to either tamox-ifen or anastrozole, each with or without zoledronic acid.23 Eligiblepatients had low-grade breast cancer with favorable prognosis, andnone received adjuvant chemotherapy, though 5% did receiveneoadjuvant chemotherapy. Thus, these patients are not necessar-ily representative of younger women with early-stage breast cancer.ABCSG-12 demonstrated equivalence with respect to time to recur-rence, disease-free survival, and overall survival between tamoxifenand AI therapy in premenopausal women given ovarian suppressiontreatments.23 Thus, there are no data at present to suggest that AI-based therapy is superior to tamoxifen-based therapy in premeno-pausal women with ovarian suppression treatments. Because oftamoxifen equivalence with AI therapy in that setting and the occa-sional failure to achieve menopausal status with ovarian suppression,the Update Committee strongly recommends tamoxifen as primaryadjuvant endocrine therapy for all pre- or perimenopausal womenand women with treatment-induced amenorrhea.
Some women who were pre- or perimenopausal at the time ofdiagnosis may become unequivocally postmenopausal in subsequentyears. For women who become postmenopausal during tamoxifentreatment after initial diagnosis of premenopausal breast cancer, theUpdate Committee suggests considering AIs as either sequential orextended adjuvant endocrine therapy. Relatively few women in thestudies of sequential or extended therapy met this description. Thus,the magnitude of benefit for introducing an AI in the subsequenttreatment of such women is not well characterized. Limited retrospec-tive data suggest that such women might benefit from extended adju-vant endocrine therapy with an AI after 5 years of tamoxifen.94
Both chemotherapy and tamoxifen can contribute to amenor-rhea. This effect may be transient or permanent, depending on thepatient’s age and therapies received. Multiple reports document lateclinical recovery of ovarian function among women with treatment-induced amenorrhea, which could render AI therapy ineffective.95,96
Cessation of menses for 1 year is the clinical hallmark of menopause.However, this clinical definition applies only to women without healthconditions, surgery of the uterus, and those taking medications thatcontribute to amenorrhea, such as chemotherapy or tamoxifen, andthus may not apply to many breast cancer patients.
At present, the role of ovarian suppression in addition to tamox-ifen for premenopausal patients is not known. The Suppression ofOvarian Function Trial (SOFT) is comparing tamoxifen, tamoxifen
plus ovarian suppression, and exemestane plus ovarian suppression,and it continues to accrue patients. Findings from this trial will furtherdefine best practices for premenopausal patients as well as those pa-tients who experience treatment-induced menopause.
Clinical question 5. Can the third-generation AIs beused interchangeably?
Recommendation 5. In the absence of direct comparisons, theUpdate Committee interprets available data as suggesting that benefitsof AI therapy represent a “class effect.” Meaningful clinical differencesbetween the commercially available third-generation AIs have notbeen demonstrated to date. In the clinical opinion of the UpdateCommittee (rather than direct evidence from randomized trials),postmenopausal patients intolerant of one AI but who are still candi-dates for adjuvant endocrine therapy may be advised to considertamoxifen or a different AI.
Literature update and discussion 5. In previous ASCO guidelineson AIs, available results were limited to reports for the principal use ofa single AI in each of the clinical settings of primary (anastrozole),sequential (exemestane), or extended (letrozole) adjuvant therapy.There are still no data from head-to-head comparisons of the AIs.However, there are data from randomized trials for each of the com-mercially available third-generation AIs for all of the adjuvant treat-ment strategies (primary, sequential, extended; Fig 1). The UpdateCommittee interprets the results with each of these agents in compar-ison to tamoxifen-based treatment as qualitatively similar with respectto efficacy and tolerability. Toxicity reports (Appendix Tables A4through A8) have not suggested obvious clinical advantages of one AIover another with respect to compliance, constitutional or meno-pausal symptoms, bone health, cardiovascular disease, or quality oflife. Anecdotal experience suggests that patients may tolerate one AIbetter than another, but patterns are neither predictable nor consis-tent. Two trials—MA.27 and Femara versus Anastrozole ClinicalEvaluation (FACE)—are directly comparing one AI against another asprimary adjuvant therapy. However, data are not yet unavailable fromeither trial.
PATIENT COMMUNICATION
The purpose of this section is to address aspects of patient-providercommunication that play a role in decision making about the use ofadjuvant endocrine therapy, the selection of agent, and barriers toadherence to treatment regimens (taking medication as prescribed)and persistence with the medication schedule (taking medication forthe full duration prescribed). Separate literature searches and UpdateCommittee members’ suggestions, rather than the systematic review,were used to prepare this section.
Patients need to be informed about risk factors for tumor recur-rence, the role of residual subclinical (that is, microscopic) disease incausing recurrence, and the potential benefit of adjuvant endocrinetherapy. Clinicians can base risk estimates in women with hormonereceptor–positive disease on well-established prognostic markers suchas stage, HER2 status, and grade. Emerging molecular diagnostic as-says such as the 21-gene recurrence score also seem to serve as prog-nostic markers in ER-positive, node-negative breast cancer.97,98 Datasummarized in this guideline provide estimates of risk reduction thatcan further inform estimates of treatment benefit. Decision tools suchas Adjuvant! Online99 quantify and communicate, in broad terms,both the risk of cancer recurrence and the benefit of various adjuvant
10 © 2010 by American Society of Clinical Oncology

endocrine treatment strategies based on a patient’s tumor character-istics, comorbidity, age, and receipt of chemotherapy.100 Adjuvant!Online also includes a feature that estimates the benefit of extendedadjuvant therapy after a 5-year course of adjuvant tamoxifen.
Rates of nonpersistence (early discontinuation of medications)in women who start taking tamoxifen are as high as 30% at 3 years afterfilling a first prescription. For example, a study of 2,816 women takingtamoxifen between 2001 and 2004 identified a 22% rate of nonpersis-tence 12 months after starting tamoxifen.101 In another study, among392 patients enrolled in Medicaid or Pharmacy Assistance programsin New Jersey between 1990 and 1996, 32% of women discontinuedadjuvant tamoxifen at 2 years and 39% at 3 years.102 Similarly, in asample of 961 women 65 years of age or older diagnosed with breastcancer in 1990 to 1994 in the Cancer Research Network, 24% discon-tinued tamoxifen after 2 years of treatment, 33% discontinued tamox-ifen after 3 years of treatment, and 50% discontinued tamoxifenbefore the end of 5 years; discontinuation was not due to recurrentdisease.103 Data from clinical trials104 and claims-based research105
indicate that persistence is no better with AIs. Physicians may under-estimate rates of nonadherence and nonpersistence, and patients maybe reluctant to disclose problems with adherence and persistence.Patient beliefs about the benefits and risks of medications are associ-ated with adherence and persistence; thus, discussing and addressingsuch beliefs is warranted.106
Adverse effects are particularly important in precipitating earlydiscontinuation of therapy. Patients experiencing treatment-relatedadverse effects are more likely to discontinue adjuvant endocrinetherapy, particularly during the first years.107,108 In another trial, ad-verse effects were the most common reason for discontinuation, par-ticularly during the first year. Among those who stopped takingtamoxifen in the first year, 70% stopped because of adverse effects.103
Patients who experience adverse effects for which they were notprepared seem to be at particularly high risk for nonpersistence.108
Similarly, musculoskeletal adverse effects of the AIs have beenshown to prompt discontinuation in more than 10% of patientswho start an AI.90 Information support for patients about antici-pated adverse effects and management of those adverse effects mayincrease persistence.98
Financial constraints are another reported cause of nonpersis-tence with adjuvant endocrine therapy. One study of patientstaking tamoxifen noted that 60% of patients who discontinuedtherapy early reported this issue as a key factor.103 It is likely thatthe out-of-pocket costs of AIs (Table 6) pose an even greaterbarrier to patients with little or no prescription coverage or who are
subject to cost-sharing strategies (ie, co-payments). Although phy-sicians are generally reluctant to discuss costs of cancer thera-pies,109 inquiring about patients’ cost concerns may help directpatients to assistance programs and create opportunities to stressthe benefits of persistence with adjuvant endocrine therapy. ASCOsupports the development of resources to facilitate patient-provider communication about costs of cancer care.110
In summary, optimal adjuvant endocrine therapy includes care-ful consideration of tumor risk, treatment benefit, treatment adverseeffects, and patient adherence. Clinicians should discuss realistic,quantitative risks of cancer recurrence and death and benefits fromcancer therapy as part of the adjuvant decision-making process. Cli-nicians should alert patients to common adverse effects of therapy andserially inquire about treatment-related toxicities, patient adherenceto therapy, and factors that may affect adherence and persistence.
HEALTH DISPARITIES
ASCO clinical practice guidelines represent expert recommendationsderived from high-quality evidence on the best practices in diseasemanagement. However, racial, ethnic, and socioeconomic disparitiesin quality of health care exist and persist in the United States. Membersof racial and ethnic minority groups and patients with fewer financialresources tend to have a higher burden of comorbid illness, are morelikely to be uninsured or underinsured, face more challenges in access-ing care, and are at greater risk of receiving poor-quality care thanother Americans.111-115
Representation of minorities in clinical trials of adjuvant endo-crine therapy is low. To date, no evidence indicates differences intherapeutic benefit between black and white women receiving adju-vant tamoxifen in the clinical trials setting. A few studies suggest thatwomen who belong to minority groups are less likely to receiveguideline-concordant endocrine therapy. One study examined pre-scribing patterns, considering 677 patients diagnosed with breastcancer in 1999 to 2000 who were treated at six hospitals in NewYork City. Findings indicated that rates of guideline-concordantadjuvant endocrine therapy prescribing were lower in Hispanic(71%) and black (75%) patients compared with non-Hispanicwhite (85%) patients.116
Only small samples of minority patients were included inpersistence studies, largely preventing an examination of correlatesand mechanisms of optimal therapy in minorities. Hispanics havelargely been omitted. In one study, nonwhite patients (who werepooled because they represented only 17% of the sample) weremore likely to stop adjuvant endocrine therapy before completingthe planned treatment course (adjusted odds ratio, 1.5; 95% CI, 1.1to 1.9).102 Other studies that addressed racial differences in adher-ence to or persistence with endocrine therapy generated mixedresults.103,108 Race was not associated with adherence or persis-tence in one recently published claims-based study of low-incomepatients (884 white and 607 black) with Medicaid; 80% of patientswho started adjuvant endocrine therapy were persistent with med-ication at 1 year of follow-up.117 Awareness of disparities in qualityof care should be considered in the context of this clinical prac-tice guideline.
Table 6. Cost of Therapies
Drug
Cost ($)
Per Unit30-DaySupply
Anastrozole (Arimidex), 1 mg 12.66 379.80Exemestane (Aromasin), 25 mg 11.38 341.40Letrozole (Femara), 2.5 mg 13.91 417.30Tamoxifen (Nolvadex), 20 mg 3.67 110.10Tamoxifen, 20 mg 0.73 21.90
NOTE. US dollars; www.drugstore.com.
© 2010 by American Society of Clinical Oncology 11

SUMMARY AND FUTURE DIRECTIONS
Incorporation of an AI improves disease-free survival in post-menopausal women with hormone receptor–positive breast can-cer compared with tamoxifen alone. Thus, the Update Committeerecommends AI therapy at some point during adjuvant treatment,either as upfront therapy or as sequential or extended treatment aftertamoxifen. The optimal timing and duration of AI treatment remainunresolved; it is unclear whether sequential treatment strategies yieldadvantages over monotherapy with AIs. The Update Committee rec-ognizes distinct adverse effect profiles of tamoxifen and AIs and be-lieves that consideration of adverse effect profiles and patientpreferences are relevant to deciding whether and when to incorporateAI therapy for individual patients.
Important and unanswered questions about adjuvant endocrinetherapy in postmenopausal women persist. The Update Committeeidentified the following issues as clinically significant for ongoingresearch studies and treatment recommendations:
● Long-term follow-up to characterize the lasting clinical effectsof AI therapy and impact on survival, survivorship, and qual-ity of life
● Comparisons of currently available AIs against one another● Determination of optimal schedules for endocrine therapy,
including duration of treatment, interrupted treatmentschedules, and sequencing
● Late adverse effects, particularly in cardiovascular and bonehealth, of AI therapy
● Strategies to improve adherence with recommended adjuvanttreatments and minimize disparities in access to therapy
● Interventions to minimize treatment-related adverse effects,including menopausal symptoms, osteoporosis, sexual dys-function, and arthralgias, among women receiving adjuvantendocrine therapy
● Comparative effectiveness analyses of adjuvant endocrinestrategies based on efficacy, toxicity, and cost
● Development of biomarker(s) for selection of endocrine strat-egies and for refining estimates of risk in postmenopausal,ER-positive breast cancer
● Identification of predictors of late (after 5 or 10 years) recur-rence to tailor durations of therapy
● Definitive analyses of the role of drug metabolism and phar-macogenetics as predictors of benefit and/or treatment op-tions in adjuvant endocrine therapy
● Incorporation of novel antiestrogens or other treatments toenhance endocrine therapy and reduce risk of recurrence
● Clarification of the relevance of AI therapy and ovarian sup-pression among women who are premenopausal at the time ofbreast cancer diagnosis
The Update Committee anticipates that the results from pro-spective randomized trials, ongoing correlative science studies, long-term follow-up from major adjuvant studies, and smaller, focusedinvestigations of related scientific and clinical questions regardingendocrine treatment will continue to inform and revise the recom-mendations for adjuvant endocrine therapy in the years ahead.
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTSOF INTEREST
Although all authors completed the disclosure declaration, the followingauthor(s) indicated a financial or other interest that is relevant to the subjectmatter under consideration in this article. Certain relationships markedwith a “U” are those for which no compensation was received; thoserelationships marked with a “C” were compensated. For a detaileddescription of the disclosure categories, or for more information aboutASCO’s conflict of interest policy, please refer to the Author DisclosureDeclaration and the Disclosures of Potential Conflicts of Interest section inInformation for Contributors.Employment or Leadership Position: None Consultant or AdvisoryRole: Jennifer Malin, Pfizer (C); Eleftherios P. Mamounas, Novartis (C),Pfizer (C) Stock Ownership: None Honoraria: Karen E. Gelmon,Novartis, Astra Zeneca, Pfizer; Eleftherios P. Mamounas, Pfizer,Novartis; Vered Stearns, AstraZeneca Research Funding: Vered Stearns,Novartis, Pfizer Expert Testimony: None Other Remuneration: None
AUTHOR CONTRIBUTIONS
Conception and design: Harold J. Burstein, Jennifer J. GriggsAdministrative support: Ann Alexis Prestrud, Jerome Seidenfeld,Mark R. SomerfieldCollection and assembly of data: Harold J. Burstein, Ann AlexisPrestrud, Jerome Seidenfeld, Jennifer J. GriggsData analysis and interpretation: Harold J. Burstein, Ann AlexisPrestrud, Jerome Seidenfeld, Holly Anderson, Thomas A. Buchholz,Nancy E. Davidson, Karen E. Gelmon, Sharon H. Giordano, Clifford A.Hudis, Jennifer Malin, Eleftherios P. Mamounas, Diana Rowden,Alexander J. Solky, MaryFran R. Sowers, Vered Stearns, Eric P. Winer,Mark R. Somerfield, Jennifer J. GriggsManuscript writing: Harold J. Burstein, Ann Alexis Prestrud, JeromeSeidenfeld, Holly Anderson, Thomas A. Buchholz, Nancy E. Davidson,Karen E. Gelmon, Sharon H. Giordano, Clifford A. Hudis, JenniferMalin, Eleftherios P. Mamounas, Diana Rowden, Alexander J. Solky,MaryFran R. Sowers, Vered Stearns, Eric P. Winer, Mark R. Somerfield,Jennifer J. GriggsFinal approval of manuscript: Harold J. Burstein, Ann Alexis Prestrud,Jerome Seidenfeld, Holly Anderson, Thomas A. Buchholz, Nancy E.Davidson, Karen E. Gelmon, Sharon H. Giordano, Clifford A. Hudis,Jennifer Malin, Eleftherios P. Mamounas, Diana Rowden, Alexander J.Solky, MaryFran R. Sowers, Vered Stearns, Eric P. Winer, Mark R.Somerfield, Jennifer J. Griggs
REFERENCES
1. National Institutes of Health ConsensusDevelopment Panel: National Institutes of HealthConsensus Development Conference statement:Adjuvant therapy for breast cancer, November 1-3,2000. J Natl Cancer Inst Monogr 30:5-15, 2001
2. Winer EP, Hudis C, Burstein HJ, et al: Amer-ican Society of Clinical Oncology technology assess-ment on the use of aromatase inhibitors as adjuvant
therapy for women with hormone receptor-positivebreast cancer: Status report 2002. J Clin Oncol20:3317-3327, 2002
3. Winer EP, Hudis C, Burstein HJ, et al: Amer-ican Society of Clinical Oncology technology assess-ment working group update: Use of aromataseinhibitors in the adjuvant setting. J Clin Oncol 21:2597-2599, 2003
4. Winer EP, Hudis C, Burstein HJ, et al: Amer-ican Society of Clinical Oncology technology assess-ment on the use of aromatase inhibitors as adjuvant
therapy for postmenopausal women with hormonereceptor-positive breast cancer: Status report 2004.J Clin Oncol 23:619-629, 2005
5. Eisen A, Trudeau M, Shelley W, et al: Aro-matase inhibitors in adjuvant therapy for hormonereceptor positive breast cancer: A systematic re-view. Cancer Treat Rev 34:157-174, 2008
6. Hind D, Ward S, De Nigris E, et al: Hormonaltherapies for early breast cancer: Systematic reviewand economic evaluation. Health Technol Assess11:iii-iv, ix-xi, 1-134, 2007
Burstein et al
12 © 2010 by American Society of Clinical Oncology

7. Hudis CA, Barlow WE, Costantino JP, et al:Proposal for standardized definitions for efficacy endpoints in adjuvant breast cancer trials: The STEEPsystem. J Clin Oncol 25:2127-2132, 2007
8. Aihara T, Hozumi Y, Suemasu K, et al: Theeffects of exemestane, anastrozole and tamoxifenon bone mineral density and bone turnover markersin postmenopausal early breast cancer patients:Preliminary results of N-SAS (national surgical adju-vant study) BC04, the TEAM Japan sub-study. Pre-sented at the 30th Annual San Antonio BreastCancer Symposium, San Antonio, TX, December13-16, 2007 (abstr 2086)
9. Aihara T, Takatsuka Y, Osumi S, et al: PhaseIII randomized adjuvant study of tamoxifen aloneversus sequential tamoxifen and anastrozole in post-menopausal women with hormone-responsivebreast cancer: N-SAS BC03 study. Presented at the31st Annual San Antonio Breast Cancer Sympo-sium, San Antonio, TX, December 10-14, 2008 (ab-str 1138)
10. Boccardo F, Rubagotti A, Guglielmini P, et al:Switching to anastrozole versus continued tamox-ifen treatment of early breast cancer: Updated re-sults of the Italian tamoxifen anastrozole (ITA) trial.Ann Oncol 17:vii10-14, 2006 (suppl 7)
11. Chapman JA, Meng D, Shepherd L, et al:Competing causes of death from a randomized trialof extended adjuvant endocrine therapy for breastcancer. J Natl Cancer Inst 100:252-260, 2008
12. Coleman RE: Long-term effects of anastro-zole on bone mineral density: Seven-year resultsfrom the ATAC trial. J Clin Oncol 26:27s, 2008(suppl; abstr 587)
13. Coleman RE, Banks LM, Girgis S, et al:Reversal of skeletal effects of endocrine treatmentsin the intergroup exemestane study. Presented atthe 31st Annual San Antonio Breast Cancer Sympo-sium, San Antonio, TX, December 10-14, 2008 (ab-str 1128)
14. Coombes RC, Kilburn LS, Snowdon CF, et al:Survival and safety of exemestane versus tamoxifenafter 2-3 years’ tamoxifen treatment (IntergroupExemestane Study): A randomised controlled trial.Lancet 369:559-570, 2007
15. Crivellari D, Sun Z, Coates AS, et al: Letro-zole compared with tamoxifen for elderly patientswith endocrine-responsive early breast cancer: TheBIG 1-98 trial. J Clin Oncol 26:1972-1979, 2008
16. Cuzick J: Hot flushes and the risk of recur-rence retrospective, exploratory results from theATAC trial. Presented at the 30th Annual San Anto-nio Breast Cancer Symposium, San Antonio, TX,December 13-16, 2007 (abstr 2069)
17. Cuzick J, Sestak I, Cella D, et al: Treatment-emergent endocrine symptoms and the risk ofbreast cancer recurrence: A retrospective analysisof the ATAC trial. Lancet Oncol 9:1143-1148, 2008
18. Eastell R, Adams JE, Coleman RE, et al:Effect of anastrozole on bone mineral density:5-year results from the anastrozole, tamoxifen,alone or in combination trial 18233230. J Clin Oncol26:1051-1057, 2008
19. Fallowfield LJ, Langridge CI, Kilburn LS, et al:Quality of life in the Intergroup Exemestane Study(IES) 5 years post-randomisation. Presented at the30th Annual San Antonio Breast Cancer Sympo-sium, San Antonio, TX, December 13-16, 2007 (ab-str 1091)
20. Forbes JF, Cuzick J, Buzdar A, et al: ATAC:100 month median follow-up (FU) shows continuedsuperior efficacy and no excess fracture risk foranastrozole (A) compared with tamoxifen (T) aftertreatment completion. Presented at the 30th Annual
San Antonio Breast Cancer Symposium, San Anto-nio, TX, December 13-16, 2007 (abstr 40)
21. Arimidex, Tamoxifen, Alone or in Combina-tion (ATAC) Trialists’ Group, Forbes JF, Cuzick J, etal: Effect of anastrozole and tamoxifen as adjuvanttreatment for early-stage breast cancer: 100-monthanalysis of the ATAC trial. Lancet Oncol 9:45-53,2008
22. Gnant M, Mlineritsch B, Luschin-EbengreuthG, et al: Adjuvant endocrine therapy plus zoledronicacid in premenopausal women with early-stagebreast cancer: 5-year follow-up of the ABCSG-12bone-mineral density substudy. Lancet Oncol 9:840-849, 2008
23. Gnant M, Mlineritsch B, Schippinger W, et al:Endocrine therapy plus zoledronic acid in premeno-pausal breast cancer. N Engl J Med 360:679-691,2009
24. Goetz M, Ames M, Gnant M, et al: Pharma-cogenetic (CYP2D6) and gene expression profiles(HOXB13/IL17BR and molecular grade index) forprediction of adjuvant endocrine therapy benefit inthe ABCSG 8 trial. Presented at the 31st Annual SanAntonio Breast Cancer Symposium, San Antonio,TX, December 10-14, 2008 (abstr 57)
25. Goss PE: Letrozole in the extended adjuvantsetting: MA.17. Breast Cancer Res Treat 105:45-53,2007 (suppl 1)
26. Goss PE, Ingle JN, Martino S, et al: Efficacyof letrozole extended adjuvant therapy according toestrogen receptor and progesterone receptor statusof the primary tumor: National Cancer Institute ofCanada Clinical Trials Group MA.17. J Clin Oncol25:2006-2011, 2007
27. Hadji P, Ziller M, Kieback D, et al: Boneeffects of exemestane vs. tamoxifen within theTEAM trial: Results of a prospective randomizedbone sub study. Presented at the 31st Annual SanAntonio Breast Cancer Symposium, San Antonio,TX, December 10-14, 2008 (abstr 1143)
28. Hozumi Y, Aihara T, Takatsuka Y, et al:Chronological changes of side effect profile of anas-trozole compared with tamoxifen in Japanese wom-en: Findings from N-SAS BC03 trial every 3 monthsafter one year of randomization. Presented at the30th Annual San Antonio Breast Cancer Sympo-sium, San Antonio, TX, December 13-16, 2007 (ab-str 3059)
29. Ingle JN, Tu D, Pater JL, et al: Intent-to-treatanalysis of the placebo-controlled trial of letrozolefor extended adjuvant therapy in early breast cancer:NCIC CTG MA.17. Ann Oncol 19:877-882, 2008
30. Jakesz R, Gnant M, Griel R, et al: Tamoxifenand anastrozole as a sequencing strategy in post-menopausal women with hormone-responsive earlybreast cancer: Updated data from the Austrianbreast and colorectal cancer study group trial 8.Presented at the 31st Annual San Antonio BreastCancer Symposium, San Antonio, TX, December10-14, 2008 (abstr 14)
31. Jakesz R, Greil R, Gnant M, et al: Extendedadjuvant therapy with anastrozole among post-menopausal breast cancer patients: Results fromthe randomized Austrian Breast and Colorectal Can-cer Study Group Trial 6a. J Natl Cancer Inst 99:1845-1853, 2007
32. Jones SE, Cantrell J, Vukelja S, et al: Com-parison of menopausal symptoms during the firstyear of adjuvant therapy with either exemestane ortamoxifen in early breast cancer: Report of a Tamox-ifen Exemestane Adjuvant Multicenter trial sub-study. J Clin Oncol 25:4765-4771, 2007
33. Jones SE, Seynaeve C, Hasenburg A, et al:Results of the first planned analysis of TEAM (ta-
moxifen exemestane adjuvant multinational) pro-spective randomized phase III trial in hormonesensitive postmenopausal early breast cancer. Pre-sented at the 31st Annual San Antonio Breast Can-cer Symposium, San Antonio, TX, December 10-14,2008 (abstr 15)
34. Kaufmann M, Jonat W, Hilfrich J, et al:Improved overall survival in postmenopausalwomen with early breast cancer after anastrozoleinitiated after treatment with tamoxifen comparedwith continued tamoxifen: The ARNO 95 Study.J Clin Oncol 25:2664-2670, 2007
35. Kieback DG, Harbeck N, Bauer W, et al:Endometrial effects of exemestane compared totamoxifen within the TEAM trial: Results of a pro-spective randomized study. J Clin Oncol 25:20s,2007 (suppl; abstract 572)
36. Koeberle D, Thuerlimann B: Letrozole asupfront endocrine therapy for postmenopausalwomen with hormone-sensitive breast cancer: BIG1-98. Breast Cancer Res Treat 105:55-66, 2007(suppl 1)
37. Mamounas EP, Jeong JH, Wickerham DL, etal: Benefit from exemestane as extended adjuvanttherapy after 5 years of adjuvant tamoxifen:Intention-to-treat analysis of the National SurgicalAdjuvant Breast And Bowel Project B-33 trial. J ClinOncol 26:1965-1971, 2008
38. Mauriac L, Keshaviah A, Debled M, et al:Predictors of early relapse in postmenopausalwomen with hormone receptor-positive breast can-cer in the BIG 1-98 trial. Ann Oncol 18:859-867,2007
39. Monnier AM: The Breast International Group1-98 trial: Big results for women with hormone-sensitive early breast cancer. Expert Rev AnticancerTher 7:627-634, 2007
40. BIG 1-98 Collaborative Group, Mouridsen H,Giobbie-Hurder A, et al: Letrozole therapy alone or insequence with tamoxifen in women with breastcancer. N Engl J Med 361:766-776, 2009
41. Mouridsen H, Keshaviah A, Coates AS, et al:Cardiovascular adverse events during adjuvant en-docrine therapy for early breast cancer using letro-zole or tamoxifen: Safety analysis of BIG 1-98 trial.J Clin Oncol 25:5715-5722, 2007
42. Mouridsen HT, Giobbie-Hurder A, Mauriac L,et al: BIG 1-98: A randomized, double blind phase IIIstudy evaluating letrozole with tamoxifen given insequence as adjuvant endocrine therapy for post-menopausal women with receptor (�) breast can-cer. Presented at the 31st Annual San AntonioBreast Cancer Symposium, San Antonio, TX, De-cember 10-14, 2008 (abstr 13)
43. Muss HB, Tu D, Ingle JN, et al: Efficacy,toxicity, and quality of life in older women withearly-stage breast cancer treated with letrozole orplacebo after 5 years of tamoxifen: NCIC CTG inter-group trial MA.17. J Clin Oncol 26:1956-1964, 2008
44. Ohsumi S, Shimozuma K, Ohashi Y, et al:Health-related quality-of-life and psychological dis-tress of postmenopausal breast cancer patientsafter surgery during the randomized trial, N-SAS BC03, comparing further tamoxifen with switching toanastrozole after adjuvant tamoxifen for 1 to 4 years:The final results. Presented at the 31st Annual SanAntonio Breast Cancer Symposium, San Antonio,TX, December 10-14, 2008 (abstr 1136)
45. Rasmussen BB, Regan MM, Lykkesfeldt AE,et al: Adjuvant letrozole versus tamoxifen accordingto centrally-assessed ERBB2 status for postmeno-pausal women with endocrine-responsive earlybreast cancer: Supplementary results from the BIG1-98 randomised trial. Lancet Oncol 9:23-28, 2008
ASCO Guideline for Adjuvant Endocrine Therapy for Breast Cancer
© 2010 by American Society of Clinical Oncology 13

46. Schilder CM, Seynaeve C, Linn SC, et al:Effects of tamoxifen and exemestane on cognitivefunctioning of postmenopausal patients with earlybreast cancer: Results from the TEAM trial. Pre-sented at the 31st Annual San Antonio Breast Can-cer Symposium, San Antonio, TX, December 10-14,2008 (abstr 1133)
47. Sestak I, Cuzick J, Sapunar F, et al: Riskfactors for joint symptoms in patients enrolled in theATAC trial: A retrospective, exploratory analysis.Lancet Oncol 9:866-872, 2008
48. Takehara M, Ohsumi S, Takei H, et al:Health-related quality of life and psychological dis-tress in Japanese patients with breast cancertreated with tamoxifen, exemestane or anastrozolefor adjuvant therapy: A phase III randomized studyof National Surgical Adjuvant Study of Breast Cancer(N-SAS BC) 04. Presented at the 30th Annual SanAntonio Breast Cancer Symposium, San Antonio,TX, December 13-16, 2007 (abstr 2088)
49. van Nes JG, Voskuil DW, van Leeuwen FE,et al: Quality of life in relation to hormonal treatmentof postmenopausal women in the Dutch TamoxifenExemestane Adjuvant Multicentre (TEAM) trial. Pre-sented at the 31st Annual San Antonio Breast Can-cer Symposium, San Antonio, TX, December 10-14,2008 (abstr 21)
50. Viale G, Giobbie-Hurder A, Regan MM, et al:Prognostic and predictive value of centrally re-viewed Ki-67 labeling index in postmenopausalwomen with endocrine-responsive breast cancer:Results from Breast International Group Trial 1-98comparing adjuvant tamoxifen with letrozole. J ClinOncol 26:5569-5575, 2008
51. Aydiner A, Tas F: Meta-analysis of trialscomparing anastrozole and tamoxifen for adjuvanttreatment of postmenopausal women with earlybreast cancer. Trials 9:47, 2008
52. Cuppone F, Bria E, Verma S, et al: Do adju-vant aromatase inhibitors increase the cardiovascu-lar risk in postmenopausal women with early breastcancer? Meta-analysis of randomized trials. Cancer112:260-267, 2008
53. Ingle JN, Dowsett M, Cuzick J, et al: Aro-matase inhibitors versus tamoxifen as adjuvant ther-apy for postmenopausal women with estrogenreceptor positive breast cancer: Meta-analyses ofrandomized trials of monotherapy and switchingstrategies. Presented at the 31st Annual San Anto-nio Breast Cancer Symposium, San Antonio, TX,December 10-14, 2008 (abstr 12)
54. Kalder M, Hadji P: Bone health in postmeno-pausal women (PMW) with hormone-sensitivebreast cancer (HSBC) receiving adjuvant aromataseinhibitor (AI) therapy. J Clin Oncol 26:611s, 2008(suppl; abstr 11556)
55. Vakaet LA: Meta-analysis of side effects(SEs) of aromatase inhibitors (AI) and of tamoxifen(TAM) in large randomized clinical trials (RCT). J ClinOncol 25:595s, 2007 (suppl; abstr 11015)
56. Bliss JM, Kilburn LS, Coleman RE, et al:Disease related outcome with long term follow-up:An updated analysis of the Intergroup ExemestaneStudy (IES). Presented at the 32nd Annual SanAntonio Breast Cancer Symposium, San Antonio,TX, December 9-13, 2009
57. Rea D, Hasenburg A, Seynaeve C, et al: Fiveyears of exemestane as initial therapy compared to5 years of tamoxifen followed by exemestane: TheTEAM Trial, a prospective, randomized, phase III trialin postmenopausal women with hormone-sensitiveearly breast cancer. Presented at the 32nd AnnualSan Antonio Breast Cancer Symposium, San Anto-nio, TX, December 9-13, 2009
58. Reference deleted59. Fisher B, Dignam J, Bryant J, et al: Five
versus more than five years of tamoxifen for lymphnode-negative breast cancer: Updated findings fromthe National Surgical Adjuvant Breast and BowelProject B-14 randomized trial. J Natl Cancer Inst93:684-690, 2001
60. Reference deleted61. Goss PE, Ingle JN, Martino S, et al: A ran-
domized trial of letrozole in postmenopausal womenafter five years of tamoxifen therapy for early-stagebreast cancer. N Engl J Med 349:1793-1802, 2003
62. Jakesz R, Samonigg H, Greil R, et al: Ex-tended adjuvant treatment with anastrozole: Resultsfrom the Austrian Breast and Colorectal CancerStudy Group Trial 6a (ABCSG-6a). J Clin Oncol23:10s, 2005 (suppl: abstr 527)
63. Breast International Group (BIG) 1-98 Collab-orative Group, Thurlimann B, Keshaviah A, et al: Acomparison of letrozole and tamoxifen in postmeno-pausal women with early breast cancer. N EnglJ Med 353:2747-2757, 2005
64. Jakesz R, Gnant M, Greil R, et al: Thebenefits of sequencing adjuvant tamoxifen andanastrozole in postmenopausal women withhormone-responsive early breast cancer: 5 year-analysis of ABCSG Trial 8. Presented at the 28thAnnual San Antonio Breast Cancer Symposium, SanAntonio, TX, December 8-11, 2005 (abstr 13)
65. Dowsett M, Cuzick J, Ingle J, et al: Meta-analysis of breast cancer outcomes in adjuvant trialsof aromatase inhibitors versus tamoxifen. J ClinOncol 28:509-518, 2010
66. Early Breast Cancer Trialists’ CollaborativeGroup (EBCTCG): Effects of chemotherapy and hor-monal therapy for early breast cancer on recurrenceand 15-year survival: An overview of the randomisedtrials. Lancet 365:1687-1717, 2005
67. Fisher B, Anderson S, Tan-Chiu E, et al:Tamoxifen and chemotherapy for axillary node-negative, estrogen receptor-negative breast cancer:Findings from National Surgical Adjuvant Breast andBowel Project B-23. J Clin Oncol 19:931-942, 2001
68. Paik S, Shak S, Tang G, et al: A multigeneassay to predict recurrence of tamoxifen-treated,node-negative breast cancer. N Engl J Med 351:2817-2826, 2004
69. Dowsett M, Cuzick J, Wale C, et al: Risk ofdistant recurrence using oncotype DX in postmeno-pausal primary breast cancer patients treated withanastrozole or tamoxifen: A Trans ATAC study.Presented at the 31st Annual San Antonio BreastCancer Symposium, San Antonio, TX, December10-14, 2008 (abstr 53)
70. Viale G, Regan MM, Dell’Orto P, et al: Cen-tral review of ER, PgR and HER2 in BIG 1-98evaluating letrozole vs letrozole followed by tamox-ifen vs tamoxifen followed by letrozole as adjuvantendocrine therapy for postmenopausal women withhormone receptor-positive breast cancer. CancerRes Treat 69:504s, 2009 (suppl; abstr 76)
71. Giordano SH, Perkins GH, Broglio K, et al:Adjuvant systemic therapy for male breast carci-noma. Cancer 104:2359-2364, 2005
72. Technology Evaluation Center (Blue CrossBlue Shield Association): CYP2D6 Pharmacogenom-ics of Tamoxifen Treatment, 2008. http://www.bcbs.com/blueresources/tec/vols/23/23_01.pdf
73. Albain K, Barlow WE, Shak S, et al: Prognos-tic and predictive value of the 21-gene recurrencescore assay in postmenopausal, node-positive, ER-positive breast cancer (S8814,INT0100). Presentedat the 30th Annual San Antonio Breast Cancer
Symposium, San Antonio, TX, December 13-16,2007 (abstr 10)
74. Borges S, Desta Z, Li L, et al: Quantitativeeffect of CYP2D6 genotype and inhibitors on tamox-ifen metabolism: Implication for optimization ofbreast cancer treatment. Clin Pharmacol Ther 80:61-74, 2006
75. Goetz MP, Knox SK, Suman VJ, et al: Theimpact of cytochrome P450 2D6 metabolism inwomen receiving adjuvant tamoxifen. Breast CancerRes Treat 101:113-121, 2007
76. Goetz MP, Rae JM, Suman VJ, et al: Phar-macogenetics of tamoxifen biotransformation is as-sociated with clinical outcomes of efficacy and hotflashes. J Clin Oncol 23:9312-9318, 2005
77. Gonzalez-Santiago S, Zarate R, Haba-Rodríguez J, et al: CYP2D6*4 polymorphism asblood predictive biomarker of breast cancer relapsein patients receiving adjuvant tamoxifen. J Clin On-col 25:25s, 2007 (suppl; abstr 590)
78. Schroth W, Goetz MP, Hamann U, et al:Association between CYP2D6 polymorphisms andoutcomes among women with early stage breastcancer treated with tamoxifen. JAMA 302:1429-1436, 2009
79. Cella D, Fallowfield L, Barker P, et al: Qualityof life of postmenopausal women in the ATAC(“Arimidex”, tamoxifen, alone or in combination) trialafter completion of 5 years’ adjuvant treatment forearly breast cancer. Breast Cancer Res Treat 100:273-284, 2006
80. Fallowfield L, Cella D, Cuzick J, et al: Qualityof life of postmenopausal women in the Arimidex,Tamoxifen, Alone or in Combination (ATAC) Adju-vant Breast Cancer Trial. J Clin Oncol 22:4261-4271,2004
81. Fallowfield LJ, Bliss JM, Porter LS, et al:Quality of life in the intergroup exemestane study: Arandomized trial of exemestane versus continuedtamoxifen after 2 to 3 years of tamoxifen in post-menopausal women with primary breast cancer.J Clin Oncol 24:910-917, 2006
82. Whelan TJ, Goss PE, Ingle JN, et al: Assess-ment of quality of life in MA.17: A randomized,placebo-controlled trial of letrozole after 5 years oftamoxifen in postmenopausal women. J Clin Oncol23:6931-6940, 2005
83. Osborne CK: Tamoxifen in the treatment ofbreast cancer. N Engl J Med 339:1609-1618, 1998
84. Rabaglio M, Sun Z, Price KN, et al: Bonefractures among postmenopausal patients withendocrine-responsive early breast cancer treatedwith 5 years of letrozole or tamoxifen in the BIG 1-98trial. Ann Oncol 20:1489-1498, 2009
85. Brufsky A, Harker WG, Beck JT, et al:Zoledronic acid inhibits adjuvant letrozole-inducedbone loss in postmenopausal women with earlybreast cancer. J Clin Oncol 25:829-836, 2007
86. Bundred NJ, Campbell ID, Davidson N, et al:Effective inhibition of aromatase inhibitor-associatedbone loss by zoledronic acid in postmenopausalwomen with early breast cancer receiving adjuvantletrozole: ZO-FAST Study results. Cancer 112:1001-1010, 2008
87. Hillner BE, Ingle JN, Chlebowski RT, et al:American Society of Clinical Oncology 2003 updateon the role of bisphosphonates and bone healthissues in women with breast cancer. J Clin Oncol21:4042-4057, 2003
88. Burstein HJ, Winer EP: Aromatase inhibitorsand arthralgias: A new frontier in symptom manage-ment for breast cancer survivors. J Clin Oncol 25:3797-3799, 2007
Burstein et al
14 © 2010 by American Society of Clinical Oncology
89. Crew KD, Greenlee H, Capodice J, et al:Prevalence of joint symptoms in postmenopausalwomen taking aromatase inhibitors for early-stagebreast cancer. J Clin Oncol 25:3877-3883, 2007
90. Henry NL, Giles JT, Ang D, et al: Prospectivecharacterization of musculoskeletal symptoms inearly stage breast cancer patients treated with aro-matase inhibitors. Breast Cancer Res Treat 111:365-372, 2008
91. Sestak I, Sapunar F, Cuzick J: Aromataseinhibitor-induced carpal tunnel syndrome: ResultsFrom the ATAC trial. J Clin Oncol 27:4961-4965,2009
92. Bertelli G, Hall E, Ireland E, et al: Long-termendometrial effects in postmenopausal women withearly breast cancer participating in the IntergroupExemestane Study (IES): A randomised controlledtrial of exemestane versus continued tamoxifenafter 2-3 years tamoxifen. Ann Oncol 21:498-505,2010
93. Duffy SR, Distler W, Howell A, et al: A lowerincidence of gynecologic adverse events and inter-ventions with anastrozole than with tamoxifen in theATAC trial. Am J Obstet Gynecol 200:80.e1-7, 2009
94. Goss PE, Ingle JN, Martino S, et al: Out-comes of women who were premenopausal atdiagnosis of early stage breast cancer in the NCICCTG MA.17 trial. Cancer Res Treat 69:487s, 2009(suppl; abstr 13)
95. Burstein HJ, Mayer E, Patridge AH, et al:Inadvertent use of aromatase inhibitors in patientswith breast cancer with residual ovarian function:Cases and lessons. Clin Breast Cancer 7:158-161,2006
96. Smith IE, Dowsett M, Yap YS, et al: Adjuvantaromatase inhibitors for early breast cancer afterchemotherapy-induced amenorrhoea: Caution andsuggested guidelines. J Clin Oncol 24:2444-2447,2006
97. Harris L, Fritsche H, Mennel R, et al: Amer-ican Society of Clinical Oncology 2007 update ofrecommendations for the use of tumor markers inbreast cancer. J Clin Oncol 25:5287-5312, 2007
98. Haynes RB, Ackloo E, Sahota N, et al: Inter-ventions for enhancing medication adherence. Co-chrane Database Syst Rev 2: CD000011, 2008
99. Adjuvant! Online. http://www.adjuvantonline.com
100. Ravdin PM: A computer program to assist inmaking breast cancer adjuvant therapy decisions.Semin Oncol 23:43-50, 1996 (suppl 1)
101. Barron TI, Connolly R, Bennett K, et al: Earlydiscontinuation of tamoxifen: A lesson for oncolo-gists. Cancer 109:832-839, 2007
102. Partridge AH, Wang PS, Winer EP, et al:Nonadherence to adjuvant tamoxifen therapy inwomen with primary breast cancer. J Clin Oncol21:602-606, 2003
103. Owusu C, Buist DS, Field TS, et al: Predictorsof tamoxifen discontinuation among older womenwith estrogen receptor-positive breast cancer. J ClinOncol 26:549-555, 2008
104. Chlebowski RT, Geller ML: Adherence toendocrine therapy for breast cancer. Oncology 71:1-9, 2006
105. Partridge AH, LaFountain A, Mayer E, et al:Adherence to initial adjuvant anastrozole therapyamong women with early-stage breast cancer. J ClinOncol 26:556-562, 2008
106. Horne R, Weinman J: Patients’ beliefs aboutprescribed medicines and their role in adherence totreatment in chronic physical illness. J PsychosomRes 47:555-567, 1999
107. Demissie S, Silliman RA, Lash TL: Adjuvanttamoxifen: Predictors of use, side effects, and dis-continuation in older women. J Clin Oncol 19:322-328, 2001
108. Kahn KL, Schneider EC, Malin JL, et al:Patient centered experiences in breast cancer: Pre-dicting long-term adherence to tamoxifen use. MedCare 45:431-439, 2007
109. Schrag D, Hanger M: Medical oncologists’views on communicating with patients about chem-otherapy costs: A pilot survey. J Clin Oncol 25:233-237, 2007
110. Meropol NJ, Schrag D, Smith TJ, et al:American Society of Clinical Oncology guidancestatement: The cost of cancer care. J Clin Oncol27:3868-3874, 2009
111. U.S. Cancer Statistics Working Group:United States Cancer Statistics: 1999-2002, Inci-dence and Mortality Web-based Report. U.S. De-partment of Health and Human Services, Centersfor Disease Control and Prevention and NationalCancer Institute Atlanta, 2005. http://apps.nccd.cdc.gov/uscs/
112. American Cancer Society. Cancer Factsand Figures for African Americans 2005-2006. At-lanta, 2005. http://www.cancer.org/downloads/STT/CAFF2005AACorrPWSecured.pdf
113. Mead H, Cartwright-Smith L, Jones K, et al:Racial and Ethnic Disparities in U.S. Health Care: AChartbook. New York, NY, The CommonwealthFund, 2008
114. Ries LA, Eisner MP, Kossary CL, et al: SEERCancer Statistics Review, 1973-1997. National Can-cer Institute. Bethesda, MD, 2000. http://seer.cancer.gov/csr/1973_1997/
115. Smedley BD, Stith AY, Nelson AR: UnequalTreatment: Confronting Racial and Ethnic Disparitiesin Health Care. Washington, DC, National Acade-mies Press, 2003
116. Bickell NA, Wang JJ, Oluwole S, et al:Missed opportunities: Racial disparities in adjuvantbreast cancer treatment. J Clin Oncol 24:1357-1362,2006
117. Kimmick G, Anderson R, Camacho F, et al:Adjuvant hormonal therapy use among insured, low-income women with breast cancer. J Clin Oncol27:3445-3451, 2009
118. Baum M, Budzar AU, Cuzick J, et al: Anas-trozole alone or in combination with tamoxifen ver-sus tamoxifen alone for adjuvant treatment ofpostmenopausal women with early breast cancer:First results of the ATAC randomised trial. Lancet359:2131-2139, 2002
119. Boccardo F, Rubagotti A, Amoroso D, et al:Anastrozole appears to be superior to tamoxifen inwomen already receiving adjuvant tamoxifen treat-ment. Breast Cancer Res Treat 82, 2003 (abstr 3)
120. Coombes RC, Hall E, Gibson LJ, et al: Arandomized trial of exemestane after two to threeyears of tamoxifen therapy in postmenopausalwomen with primary breast cancer. N Engl J Med350:1081-1092, 2004
121. Jakesz R, Jonat W, Gnant M, et al: Switchingof postmenopausal women with endocrine-responsive early breast cancer to anastrozole after 2years’ adjuvant tamoxifen: combined results ofABCSG trial 8 and ARNO 95 trial. Lancet 366:455-462, 2005
122. Goss PE, Ingle JN, Martino S, et al: A ran-domized trial of letrozole in postmenopausal womenafter five years of tamoxifen therapy for early-stagebreast cancer. N Engl J Med 349:1793-1802, 2003
123. Jakesz R, Samonigg H, Greil R, et al: Ex-tended adjuvant treatment with anastrozole: Resultsfrom the Austrian Breast and Colorectal CancerStudy Group Trial 6a (ABCSG-6a) . J Clin Oncol23:10s, 2005 (suppl; abstr 527)
124. Mamounas EP, Jeong JH, Wickerham L, etal: Benefit from exemestane (EXE) as extendedadjuvant therapy after 5 years of tamoxifen (TAM):Intent-to-treat analysis of NSABP B-33. Breast Can-cer Res Treat 100:A49, 2006 (suppl 1)
■ ■ ■
Acknowledgment
The Update Committee thanks Kaitlin Einhaus; Karen Hagerty; Christina H. Jagielski; Carol Palackdharry; Richard Theriault, DO; LindaVahdat, MD; Robert Langdon, MD; and Sandra Swain, MD; the external reviewers for the Journal of Clinical Oncology, and the AmericanSociety of Clinical Oncology Board of Directors and Clinical Practice Guideline Committee for their thoughtful reviews of earlier drafts.
Appendix
Search Strategy for MEDLINE (PUBMED)
(Breast neoplasms[mesh] NOT (“Breast Neoplasms, Male”[Mesh] OR “Phyllodes Tumor”[Mesh] OR “Carcinoma, Ductal, Breast”[Mesh]) OR (“Breast”[Mesh] AND (“Carcinoma”[Mesh] OR “Adenocarcinoma”[Mesh] OR “Neoplasms”[Mesh]))) OR ((breast[tiab]OR mammary[tiab]) AND (cancer[tiab] OR cancers[tiab] OR tumor[tiab] OR tumors[tiab] OR tumour[tiab] OR tumours[tiab] ORmalignan*[tiab] OR carcinoma[tiab] OR carcinomas[tiab] OR adenocarcinoma[tiab] OR adenocarcinomas[tiab])) AND
((“Aromatase Inhibitors”[Mesh] OR aromatase inhibitors[nm] OR “aromatase inhibitor”[TIAB] OR “aromatase inhibitors”[TIAB] OR “aromatase inhibition”[TIAB] OR “anastrozole ”[Substance Name] OR anastrozole [tiab] OR arimedex[tiab] OR “letrozole”
ASCO Guideline for Adjuvant Endocrine Therapy for Breast Cancer
© 2010 by American Society of Clinical Oncology 15

[Substance Name] OR “letrozole ”[tiab] OR femara[tiab] OR aromasil[tiab]OR exemestane [Substance Name] OR “exemestane”[tiab]OR aromasin[tiab] OR aromasine[TIAB] OR Tamoxifen[Mesh] OR Tamoxifen[substance name] OR “Tamoxifen”[tiab] OR novaldex[tiab]) NOT (aminoglutethimide[mesh] OR aminoglutethimide[tiab])) AND
(((randomized controlled trial[pt] OR controlled clinical trial[pt] OR randomized controlled trials[mh] OR clinical trial[pt] OR“clinical trial”[tiab] OR “clinical trials”[tiab] OR clinical trials as topic[mh] OR controlled clinical trials as topic[mh] OR randomizedcontrolled trials as topic[mh] OR clinical trials, phase II as topic[mh] OR clinical trials, phase III as topic[mh] OR clinical trials, phase IVas topic[mh] OR clinical trial, phase II[pt] OR clinical trial, phase III[pt] OR clinical trial, phase IV[pt] OR random allocation[mh] OR“random allocation”[tiab] OR “randomly allocated”[tiab] OR double-blind method[mh] OR single-blind method[mh]) OR ((random-[tiab] OR randomly[tiab] OR randomized[tiab] OR randomised[tiab] OR randomization[tiab] OR randomisation[tiab]) AND (clini-cal[tiab] OR control[tiab] OR controlled[tiab] or control groups[mh])) OR ((single[tiab] OR single-[tiab] OR double[tiab] ORdouble-[tiab] OR triple[tiab] OR triple-[tiab] OR multi[tiab] OR multi-[tiab]OR evaluator[tiab] OR assessor[tiab] OR interviewer-[tiab]) AND (mask[tiab] OR masked[tiab] OR masking[tiab] OR blind[tiab] OR blinded[tiab] OR blinding[tiab])) OR ((placebos[mh]OR placebo[tiab] OR placebos[tiab] OR random[tiab] OR randomly[tiab] OR randomized[tiab] OR randomised[tiab] OR randomiza-tion[tiab] OR randomization[tiab]) AND (research design[mh] OR “comparative study”[tiab] OR comparative study[pt] OR evaluationstudies as topic[mh:noexp] OR evaluation studies[pt] OR “evaluation study”[tiab] OR “evaluation studies”[tiab] OR validation studiesas topic[mh] OR follow-up studies[mh] OR “follow-up study”[tiab] OR “follow up study”[tiab] OR “follow-up studies”[tiab] OR“follow up studies”[tiab] OR prospective studies[mh] OR prospective[tiab] OR epidemiologic research design[mh] OR epidemiologicmethods[mh] OR epidemiologic study characteristics as topic[mh] OR epidemiologic studies[mh] OR intervention studies[mh] ORcross-over studies[mh]))) NOT (clinical trial, phase I[pt] OR clinical trials, phase I as topic[mh]) NOT (animals[mh] NOT hu-mans[mh])) AND English[la]
Table A1. Update Committee Members
Member Affiliation
Harold J. Burstein, MD, PhD, Co-Chair Dana-Farber Cancer InstituteJennifer J. Griggs, MD, MPH, Co-Chair University of Michigan Comprehensive Cancer CenterHolly Anderson, RN, BSN, Patient Representative Breast Cancer Coalition of RochesterDiana Rowden, MS, Patient Representative Susan G. Komen for the CureThomas A. Buchholz, MD M. D. Anderson Cancer CenterNancy E. Davidson, MD University of Pittsburgh Cancer InstituteKaren A. Gelmon, MD British Columbia Cancer AgencySharon Hermes Giordano, MD M. D. Anderson Cancer CenterClifford Hudis, MD Memorial Sloan-Kettering Cancer CenterJennifer Malin, MD, PhD Greater Los Angeles Veterans Affairs Healthcare SystemEleftherios P. Mamounas, MD Aultman Health FoundationAlexander J. Solky, MD Interlakes Oncology and HematologyMaryFran R. Sowers, PhD University of MichiganVered Stearns, MD Johns Hopkins School of MedicineEric P. Winer, MD Dana-Farber Cancer Institute
Burstein et al
16 © 2010 by American Society of Clinical Oncology
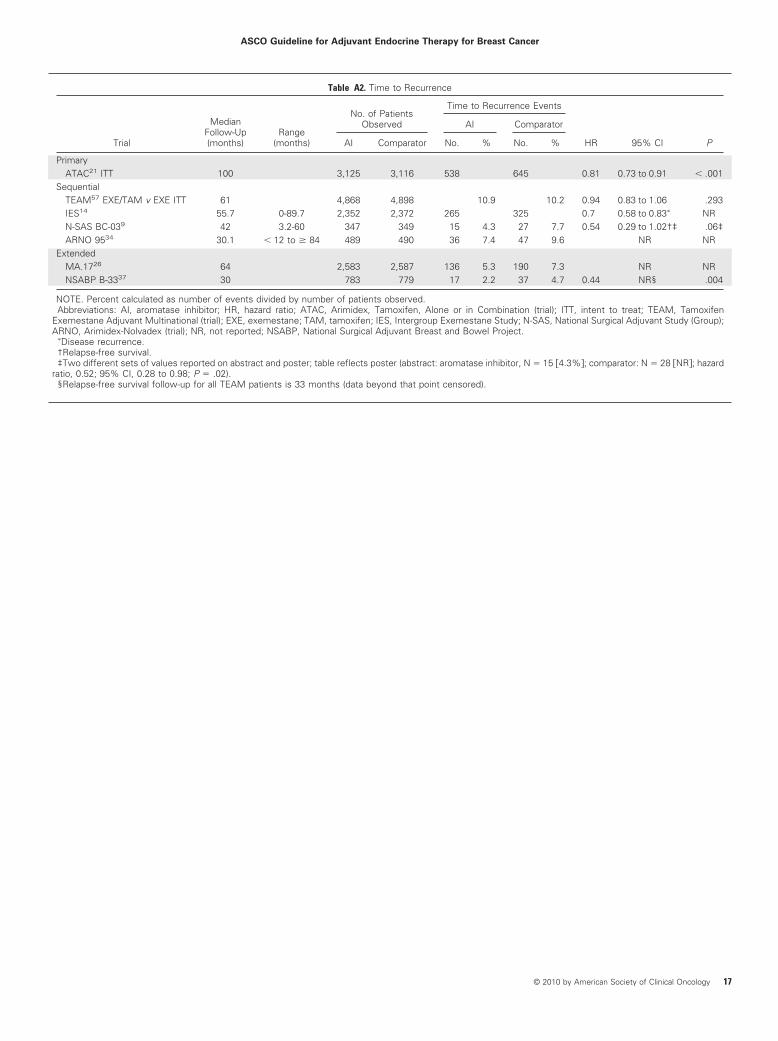
Table A2. Time to Recurrence
Trial
MedianFollow-Up(months)
Range(months)
No. of PatientsObserved
Time to Recurrence Events
HR 95% CI P
AI Comparator
AI Comparator No. % No. %
PrimaryATAC21 ITT 100 3,125 3,116 538 645 0.81 0.73 to 0.91 � .001
SequentialTEAM57 EXE/TAM v EXE ITT 61 4,868 4,898 10.9 10.2 0.94 0.83 to 1.06 .293IES14 55.7 0-89.7 2,352 2,372 265 325 0.7 0.58 to 0.83� NRN-SAS BC-039 42 3.2-60 347 349 15 4.3 27 7.7 0.54 0.29 to 1.02†‡ .06‡ARNO 9534 30.1 � 12 to � 84 489 490 36 7.4 47 9.6 NR NR
ExtendedMA.1726 64 2,583 2,587 136 5.3 190 7.3 NR NRNSABP B-3337 30 783 779 17 2.2 37 4.7 0.44 NR§ .004
NOTE. Percent calculated as number of events divided by number of patients observed.Abbreviations: AI, aromatase inhibitor; HR, hazard ratio; ATAC, Arimidex, Tamoxifen, Alone or in Combination (trial); ITT, intent to treat; TEAM, Tamoxifen
Exemestane Adjuvant Multinational (trial); EXE, exemestane; TAM, tamoxifen; IES, Intergroup Exemestane Study; N-SAS, National Surgical Adjuvant Study (Group);ARNO, Arimidex-Nolvadex (trial); NR, not reported; NSABP, National Surgical Adjuvant Breast and Bowel Project.
�Disease recurrence.†Relapse-free survival.‡Two different sets of values reported on abstract and poster; table reflects poster (abstract: aromatase inhibitor, N � 15 �4.3%�; comparator: N � 28 �NR�; hazard
ratio, 0.52; 95% CI, 0.28 to 0.98; P � .02).§Relapse-free survival follow-up for all TEAM patients is 33 months (data beyond that point censored).
ASCO Guideline for Adjuvant Endocrine Therapy for Breast Cancer
© 2010 by American Society of Clinical Oncology 17

Table A3. Disease-Free Survival Subset Analyses
Trial
MedianFollow-Up(months)
Range(months)
No. of PatientsObserved
Disease-Free Survival Events
HR 95% CI P
AI Comparator
AI Comparator No. % No. %
PrimaryATAC21,65 (Goss PE, et al: J Natl
Cancer Inst 97:1262-1271,2005) ANA v TAM ITT 100 0-126 3,125 3,116 817 26.1 887 28.5 0.90 0.82 to 0.99 .025
Hormone receptor–positive 100 0-126 2,618 2,598 618 23.6 702 27.0 0.85 0.76 to 0.94 .003ANA v TAM ITT 68 Total: 9,366 402 12.9 498 16.0 0.79 0.70 to 0.90� � .001Node-positive 68 NR NR NR 0.84 0.70 to 1.00Node-negative 68 NR NR NR 0.68 0.55 to 0.84Node-unknown 68 NR NR NR 0.48 0.23 to 1.00 NRER-positive/PR-positive 68 Total: 5,719 191 10 222 12 0.84 0.69 to 1.02� .07ER-positive/PR-negative 68 Total: 1,372 50 11 102 24 0.43 0.31 to 0.61� � .001ER-negative/PR-positive 68 Total: 220 17 27 25 33 0.79 0.43 to 1.47� .5ER-negative/PR-negative 68 Total: 703 66 28 79 32 0.90 0.65 to 1.25� .5ER-positive/PR-unknown 68 Total: 518 22 13 20 11 1.29 0.71 to 2.37� .4ER- and PR-unknown 68 Total: 743 46 19 47 19 0.96 0.64 to 1.44� .8
BIG 1-9842,45,50 LET v TAM 76 2,463 2,459 509 20.7 565 23.0 0.88 0.78 to 0.99 .03Node-negative or node-unknown 71 1,376 1,404 200 14.5 227 16.2 0.89 0.74 to 1.08 NR†Node-positive 71 1,050 1,017 303 28.9 332 32.6 0.83 0.71 to 0.98 NRERBB2-negative 51 1,648 1,646 178 1.08 240 14.6 0.72 0.59 to 0.87 NRERBB2-positive 51 134 105 27 20.1 32 30.5 0.62 0.37 to 1.03 NRLow Ki-67 51 730 703 56 7.7 66 9.4 0.81 0.57 to 1.15 .09 (for interaction
between lowand high Ki-67)
High Ki-67 51 631 621 66 10.5 115 18.5 0.53 0.39 to 0.72ER-positive/PR-positive 25.8 2,542 2,513 179 7 208 8.3 0.84 0.49 to 1.03 .09†ER-positive/PR-negative 25.8 808 823 89 11 107 13 0.83 0.62 to 1.10 .18†ER-positive/PR-unknown 25.8 579 575 70 12.1 92 16 0.72 0.53 to 0.98 .04†
SequentialBIG 1-9842 TAM/LET v LET 71 1,548 1,546 259 16.7 248 16.0 1.05 0.84 to 1.32‡ NR
Node-negative or node-unknown 71 894 886 100 11.2 102 11.5 0.96 0.67 to 1.38 NRNode-positive 71 635 645 154 24.2 145 22.5 1.13 0.84 to 1.52 NRLET/TAM v LET 71 1,540 1,546 236 15.3 248 16.0 0.96 0.76 to 1.21‡ NRNode-negative or node-unknown 71 920 886 101 102 0.97 0.67 to 1.39 NRNode-positive 71 611 645 135 145 0.98 0.72 to 1.59 NR
IES14 ITT 55.7 0-89.7 2,352 2,372 354 455 0.76 0.66 to 0.88 � .001Node-negative 55.7 0-89.7 1,217 1,230 NR NR 0.74 0.58 to 0.94 NRNode-positive 55.7 0-89.7 1,050 1,039 NR NR 0.72 0.61 to 0.86 NRER-positive/ER-unknown 55.7 0-89.7 2,296 2,306 339 14.8 439 19.0 0.75 0.65 to 0.87 � .001ER and PR high NR NR NR NR NR 0.686 NR
ExtendedMA.1726 ITT§ 64 16-95 2,583 2,587 164 6.3 235 9.1 0.68 0.55 to 0.83 � .001
Node-positive 64 1,174 1,194 91.7 DFS at4 years
87.8 DFS at4 years
0.74 0.58 to 0.94 .01
Node-negative 64 1,295 1,281 97.0 DFS at4 years
94.6 DFS at4 years
0.51 0.35 to 0.75 � .001
ITT§ 30 2,583 2,587 92 3.6 155 6.0 0.58 0.45 to 0.76 � .001ER-positive/PR-positive 30 1,907 1,902 60 3.0 117 6.0 0.49 0.36 to 0.67 NRER-positive/PR-negative 30 309 327 19 6.0 17 5.0 1.21 0.63 to 2.34 NRER-negative/PR-positive 30 100 100 4 4.0 5 5.0 0.56 0.15 to 2.12 NR
NSABP B-3337 30 783 779 37 4.7 52 6.7 0.68 .07Node-positive 30 Total: 755 NR NR 0.5 0.30 to 0.86 .01Node-negative 30 Total: 807 NR NR 1.13 NR .74ER-positive and PR-positive 30 Total: 1,266 NR NR 0.7 NR .15ER-positive or PR-positive 30 Total: 248 NR NR 0.52 NR .17
NOTE. Percent calculated as number of events divided by number of patients observed.Abbreviations: AI, aromatase inhibitor; HR, hazard ratio; ATAC, Arimidex, Tamoxifen, Alone or in Combination (trial); ANA, anastrozole; TAM, tamoxifen; ITT, intent
to treat; NR, not reported; ER, estrogen receptor; PR, progesterone receptor; BIG, Breast International Group; LET, letrozole; IES, Intergroup Exemestane Study;DFS, disease-free survival; NSABP, National Surgical Adjuvant Breast and Bowel Project.
�Time to recurrence.†Relapse-free survival, local and distant recurrence, contralateral breast cancer, and death without recurrence.‡99% CIs used to account for multiple comparisons.§Seventeen patients omitted from ITT analysis.
Burstein et al
18 © 2010 by American Society of Clinical Oncology

Table A4. Adverse Cardiovascular (cardiovascular deaths, ischemic cardiac disease, hypertension, high cholesterol) Effects
Trial
MedianFollow-Up(months) Arm
No. ofPatients
Cardiovascular Events
All CardiacEvents
Grades3 to 5
CardiacEvents
CardiovascularDeaths
AllIschemicCardiacDisease
Grades3 to 5
IschemicCardiacDisease
Any GradeHypertension
HighCholesterol
No. % No. % No. % No. % No. % No. % No. %
ATAC (Howell A, et al:Lancet 365:60-62, 2005;Arimidex, Tamoxifen,Alone or in CombinationTrialists’ Group, et al:Lancet Oncol 7:633-643)2006 68 ANA 3,092 49 2 127 4.10 402 13 278 9
TAM 3,094 46 1 104 3.40 349 11 108 3OR NR 1.23 1.18 2.7395% CI NR 0.95 to 1.60 0.69 to 1.44 2.02 to 3.69P NR .1 .04 � .001
BIG 1-9815,36,41 30.1 LET 3,975 140 5.7 96 2.4 54 2.2 45 1.1 150 3.8 43.60�
TAM 3,988 127 5.2 57 1.4 45 1.8 29 0.7 135 3.4 19.20RR NR 1.68 NR 1.55 1.11 NRP .45 .001 .42 .06 .37
ABCSG-830 75 TAM/ANA 1,469 127 6.5TAM 1,453 130 6.0P .479
ITA10 (Boccardo F, et al:J Clin Oncol 23:5138-5147, 2005)
64 ANA 223 17 7.6† 19 9.3�
TAM 225 14 6.2 6 4.0P .6 .04
TEAM57 61 TAM/EXE 4,814 60 1.2‡ 215 4.5 134 2.8EXE 4,852 77 1.6 293 6.0 227 4.7P .183 .001 � .001
IES14 55.7 EXE 2,320 382 16.5§ 23 1 14 � 1 185 8.0 185 8 830 35.8 166 7.2TAM 2,338 350 15.0 18 � 1 13 � 1 162 6.9 162 6.9 772 33.0 141 6.0P .16 NR NR .17 .17 .05 .12
ARNO 9534 30.1 ANA 445 9 2.0TAM 452 4 0.9
N-SAS BC-039 42 TAM/ANA 347 0.6¶TAM 349 0.9
MA.1725 30 LET 2,572 5.80 16.00Placebo 2,577 5.60 16.00P .76 .79
Abbreviations: ATAC, Arimidex, Tamoxifen, Alone or in Combination (trial); ANA, anastrozole; TAM, tamoxifen; OR, odds ratio; NR, not reported; BIG, BreastInternational Group; LET, letrozole; RR, risk ratio; ABCSG, Austrian Breast and Colorectal Cancer Study Group; ITA, Italian Tamoxifen Anastrozole (trial); TEAM,Tamoxifen Exemestane Adjuvant Multinational (trial); EXE, exemestane; IES, Intergroup Exemestane Study; ARNO, Arimidex-Nolvadex (trial); N-SAS, NationalSurgical Adjuvant Study (Group).
�Lipid metabolism disorder.†Cardiovascular disease.‡Myocardial ischemia/infarction.§Excludes venous thromboembolic events.¶Heart disease.
ASCO Guideline for Adjuvant Endocrine Therapy for Breast Cancer
© 2010 by American Society of Clinical Oncology 19
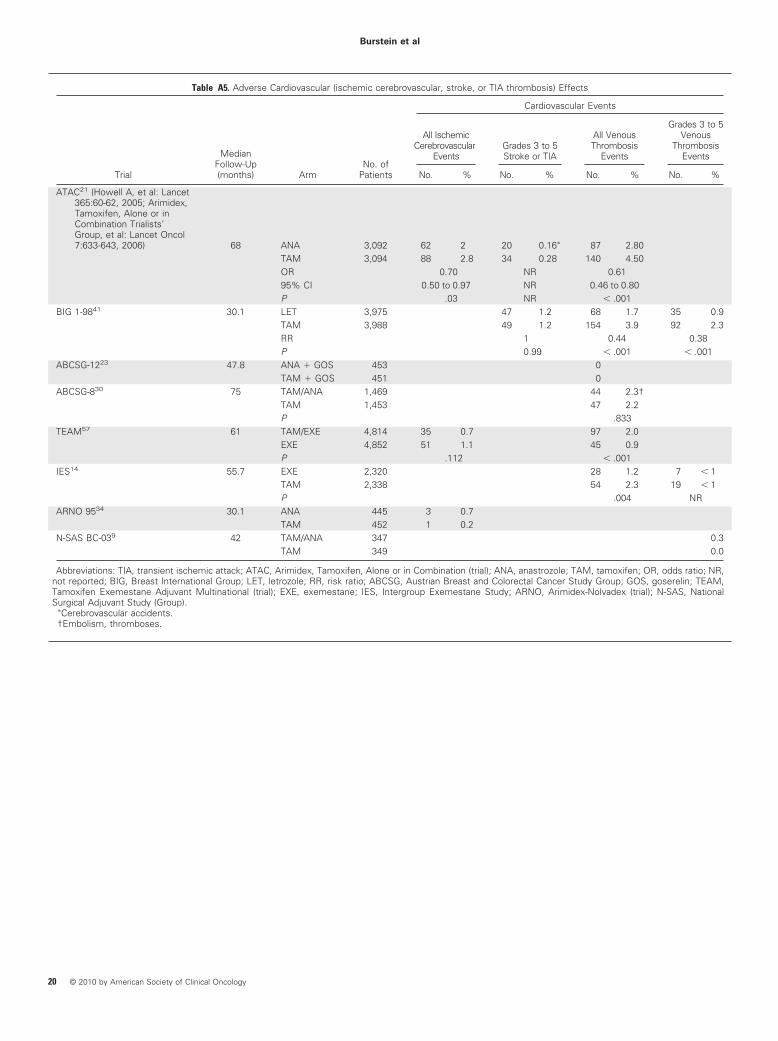
Table A5. Adverse Cardiovascular (ischemic cerebrovascular, stroke, or TIA thrombosis) Effects
Trial
MedianFollow-Up(months) Arm
No. ofPatients
Cardiovascular Events
All IschemicCerebrovascular
EventsGrades 3 to 5Stroke or TIA
All VenousThrombosis
Events
Grades 3 to 5Venous
ThrombosisEvents
No. % No. % No. % No. %
ATAC21 (Howell A, et al: Lancet365:60-62, 2005; Arimidex,Tamoxifen, Alone or inCombination Trialists’Group, et al: Lancet Oncol7:633-643, 2006) 68 ANA 3,092 62 2 20 0.16� 87 2.80
TAM 3,094 88 2.8 34 0.28 140 4.50OR 0.70 NR 0.6195% CI 0.50 to 0.97 NR 0.46 to 0.80P .03 NR � .001
BIG 1-9841 30.1 LET 3,975 47 1.2 68 1.7 35 0.9TAM 3,988 49 1.2 154 3.9 92 2.3RR 1 0.44 0.38P 0.99 � .001 � .001
ABCSG-1223 47.8 ANA � GOS 453 0TAM � GOS 451 0
ABCSG-830 75 TAM/ANA 1,469 44 2.3†TAM 1,453 47 2.2P .833
TEAM57 61 TAM/EXE 4,814 35 0.7 97 2.0EXE 4,852 51 1.1 45 0.9P .112 � .001
IES14 55.7 EXE 2,320 28 1.2 7 � 1TAM 2,338 54 2.3 19 � 1P .004 NR
ARNO 9534 30.1 ANA 445 3 0.7TAM 452 1 0.2
N-SAS BC-039 42 TAM/ANA 347 0.3TAM 349 0.0
Abbreviations: TIA, transient ischemic attack; ATAC, Arimidex, Tamoxifen, Alone or in Combination (trial); ANA, anastrozole; TAM, tamoxifen; OR, odds ratio; NR,not reported; BIG, Breast International Group; LET, letrozole; RR, risk ratio; ABCSG, Austrian Breast and Colorectal Cancer Study Group; GOS, goserelin; TEAM,Tamoxifen Exemestane Adjuvant Multinational (trial); EXE, exemestane; IES, Intergroup Exemestane Study; ARNO, Arimidex-Nolvadex (trial); N-SAS, NationalSurgical Adjuvant Study (Group).
�Cerebrovascular accidents.†Embolism, thromboses.
Burstein et al
20 © 2010 by American Society of Clinical Oncology

Table A6. Adverse Musculoskeletal Effects
Trial
MedianFollow-Up(months) Arm
No. ofPatients
Musculoskeletal Events
Bone PainMusculoskeletal
Pain Arthralgia OsteoporosisFracture
Rate
Decreasein HipBMD
Decreasein
LumbarSpineBMD
No. % No. % No. % No. % No. %
ATAC18,21 (Howell A, et al:Lancet 365:60-62,2005; Arimidex,Tamoxifen, Alone or inCombination Trialists’Group, et al: LancetOncol 7:633-643, 2006) 68 ANA 3,092 132 4a 1,100 35.6 325 11b 375 12.1 �7.24c �6.08c
TAM 3,094 235 8 911 29.4 226 7 234 7.6 0.74 �2.77OR 0.54 1.32 1.49 1.55 NR NR95% CI 0.41 to 0.72 1.19 to 1.47 1.18 to 1.88 1.25 to 1.77 NR NRP � .001 � .001 � .001 � .001 NR NR
BIG 1-9815,36 30.1 LET 3,975 196 8TAM 3,988 132 5.4P � .001
ABCSG-1223 47.8 ANA � GOS 451 128 28.3 112 4.7 1 0.2 �7.8%d
TAM � GOS 453 94 20.8 52 11.5 1 0.2 �4.5%ABCSG-830 75 TAM/ANA 1,469 223 11.4e 69 3.5
TAM 1,453 179 8.2 35 1.6P � .001 � .001
ITA10 64 ANA 223 22 9.9f
TAM 225 15 6.7P .2
TEAM57 61 TAM/EXE 4,814 302 6.3g 961 20.0 259 5.4 170 3.5EXE 4,852 188 3.9 1,140 23.5 478 9.9 249 5.1P � .001 � .001 � .001 � .001
IES13,14 55.7 EXE 2,320 488 21.0 432 18.6 169 7.3 100 4.3 �2.799 �3.726TAM 2,338 376 16.1 275 11.8 128 5.5 73 3.1 �1.011 �0.412P � .001 � .001 .01 .03 NR NR
N-SAS BC-039 42 TAM/ANA 347 50.4TAM 349 31.8
ARNO 9534 30.1 ANA 445 52 11.7h 13 2.9 10 2.2TAM 452 22 4.9 4 0.9 10 2.2
ABCSG-6a31 62.3 ANA 387 86 18.3i
Placebo 469 95 24.5OR 1.5595% CI 1.11 to 2.17P .009
NSABP B-3337 30 EXE 799 0.50j 1.00j 28Placebo 799 0.70 0.50 20P NR NR .33
MA.1725 (Goss PE, et al:J Natl Cancer Inst 97:1262-1271, 2005) 30 LET 2,572 5 15k 25 8.10 5.30 �3.60%l �5.35%l
Placebo 2,577 6 12 21 6 4.60 �0.71% �0.70%P .67 .004 � .001 .003 .25 .044 .008
Abbreviations: BMD, bone mineral density; ATAC, Arimidex, Tamoxifen, Alone or in Combination (trial); ANA, anastrozole; TAM, tamoxifen; OR, odds ratio; NR, notreported; BIG, Breast International Group; LET, letrozole; ABCSG, Austrian Breast and Colorectal Cancer Study Group; GOS, goserelin; ITA, Italian TamoxifenAnastrozole (trial); TEAM, Tamoxifen Exemestane Adjuvant Multinational (trial); EXE, exemestane; IES, Intergroup Exemestane Study; N-SAS, National SurgicalAdjuvant Study (Group); ARNO, Arimidex-Nolvadex (trial); NSABP, National Surgical Adjuvant Breast and Bowel Project.
aMuscle cramps.bOsteoporosis or osteopenia.cChange in BMD from baseline to year 5.dChanges at 60 months.eBone or joint disorder.fIncludes both musculoskeletal disorders and bone fractures.gMuscle cramps/disorders.hBoth arthralgia and bone pain.iGrades 1 to 4 only.jGrades 3 and 4 only.kMuscle pain.lBMD from 24 months: N (LET) � 122; N (placebo) � 104 cases only.
ASCO Guideline for Adjuvant Endocrine Therapy for Breast Cancer
© 2010 by American Society of Clinical Oncology 21

Table A7. Adverse Gynecologic Effects
Trial
MedianFollow-Up(months) Arm
No. ofPatients
Gynecologic Events
GynecologicDisorders Vaginal Bleeding
VaginalDischarge
EndometrialBiopsy
EndometrialCancer
UterinePolyps
No. % No. % No. % No. % No. % No. %
ATAC (Howell A, et al: Lancet365:60-62, 2005) 68 ANA 3,092 95 3a 167 5.4 109 3.5 5 0.2
TAM 3,094 324 10 317 10.2 408 13.2 17 0.8OR 0.27 0.50 0.24 0.2995% CI 0.20 to 0.37 0.41 to 0.61 0.19 to 0.30 0.11 to 0.80P � .001 � .001 � .001 .02
BIG 1-986,36 25.8 LET 3,975 3.3 2.3 6 0.1TAM 3,988 6.6 9.1 15 0.3P � .001 � .001 NR
ABCSG-1223 47.8 ANA � GOS 453 1 0.2TAM � GOS 451 5 1.1
ABCSG-830 75 TAM/ANA 442 22.6TAM 681 31.2P � .001
ITA10 64 ANA 223 16 7.2b
TAM 225 9 4.0P .1
TEAM57 61 TAM/EXE 4,814 94 2.0c 243 5.0 402 8.4 187 3.9d 17 0.4EXE 4,852 64 1.3 114 2.3 123 2.5 20 0.4 7 0.1P .017 � .001 � .001 � .001 .040
IES6,14 55.7 EXE 2,320 91 4.6 65 2.8 1 � 0.1e 5 0.2 24 1.2f
TAM 2,338 131 6.5 91 3.9 20 0.9 11 0.5 65 (3.2)P .008 .04 � .001 NR � .001
N-SAS BC-039 42 TAM/ANA 347 9.2g 16.1 0TAM 349 8.0 24.4 0.3
ARNO 9534 30.1 ANA 445 7 1.6 8 1.8e 0 4 0.9TAM 452 9 2.0 39 8.6 2 0.4 15 3.3
ABCSG-6a31 62.3 ANA 387 3 0.8h 23 59Placbeo 469 1 0.2 13 2.8OR 3.84 2.3495% CI 1.40 to 37.06 1.17 to 4.68P .245 .017
MA.176 (Goss PE, et al:J Natl Cancer Inst 97:1262-1271, 2005) 30 LET 2,572 145 6.0 4
Placebo 2,577 196 8.0 11P .005 .12
Abbreviations: ATAC, Arimidex, Tamoxifen, Alone or in Combination (trial); ANA, anastrozole; TAM, tamoxifen; OR, odds ratio; BIG, Breast International Group; LET,letrozole; NR, not reported; ABCSG, Austrian Breast and Colorectal Cancer Study Group; GOS, goserelin; ITA, Italian Tamoxifen Anastrozole (trial); TEAM, TamoxifenExemestane Adjuvant Multinational (trial); EXE, exemestane; IES, Intergroup Exemestane Study; N-SAS, National Surgical Adjuvant Study (Group); ARNO,Arimidex-Nolvadex (trial).
aGynecologic events.bGynecologic symptoms.cOther vulvovaginal disorders.dEndometrial abnormalities.eEndometrial hyperplasia.fUterine fibroids or polyps.gGenital bleeding.hGrades 1 and 2 only.
Burstein et al
22 © 2010 by American Society of Clinical Oncology

Table A8. Adverse Climacteric Effects
Trial
MedianFollow-Up(months) Arm
No. ofPatients
Climacteric Symptoms
Hot FlashesFatigue/Asthenia
MoodDisturbance
DecreasedLibido
Nauseaand
Vomiting HeadacheCognitiveDisorder
GISymptoms
No. % No. % No. % No. % No. % No. % No. % No. %
ATAC (Howell A, et al:Lancet 365:60-62,2005; Arimidex,Tamoxifen, Aloneor in CombinationTrialists’ Group, etal: Lancet Oncol7:633-643, 2006) 68 ANA 3,092 1,104 35.7 575 18.6 597 19.3 39 1 393 12.7 265 9a
TAM 3,094 1,264 40.9 544 17.6 554 17.9 12 � 1 384 12.4 216 7OR 0.80 1.07 1.10 3.28 1.03 1.2595% CI 0.73 to 0.89 0.94 to 1.22 0.97 to 1.25 1.4 to 7.7 0.88 to 1.19 0.98 to 1.60P � .001 .3 .2 � .001 .7 .02
BIG 1-9836 25.8 LET 3,975 33.5TAM 3,988 38P � .001
ABCSG- 1223 47.8 ANA � GOS 453 25 5.5 93 20.5 97 21.4b 32 7.1 63 13.9 3 0.7TAM � GOS 451 28 6.2 70 15.5 70 15.5 23 5.1 59 13.1 0
ABCSG-830 75 ANA/TAM 1,469 80 4.1c 67 3.4TAM 1,453 51 2.3 82 3.8P .001 .616
ITA10 64 ANA 223 4 1.8 26 11.7d
TAM 225 0 15 6.6P .045 .07
TEAM57 61 TAM/EXE 4,814 2,127 44.2EXE 4,852 1,812 37.3P � .001
IES14,19 55.7 EXE 2,320 957 41.3 526 22.7 228 9.8e 50.6 225 9.7 416 17.9 97 4.2a
TAM 2,338 903 38.6 522 22.3 205 8.8 56.9 248 10.6 363 15.5 51 2.2P .07 .78 .21 .30 .03 � .001
N-SAS BC-039 42 TAM/ANA 347 36.3 26.5 20.5f 18.2TAM 349 44.7 25.5 18.1 16.0
ARNO 9534 30.1 ANA 445 29 6.5TAM 452 29 6.4
ABCSG-6a31 62.3 ANA 387 151 39.0g 41 10.6h 32 8.3 16 4.1a
Placebo 469 105 22.4 20 4.3 11 2.3 12 2.6OR 2.44 2.82 3.97 1.7395% CI 1.80 to 3.31 1.62 to 4.90 1.97 to 7.9 0.81 to 3.70P � .001 � .001 � .001 .159
NSABP B-3337 30 EXE 799 0.90i
Placebo 799 0.50P NR
MA.17 (Goss PE, etal: J Natl CancerInst 97:1262-1271, 2005) 30 LET 2,572 1,486 58 999 39 272 16j
Placebo 2,577 1,383 54 998 39 249 15P .003 .95 NR
Abbreviations: ATAC, Arimidex, Tamoxifen, Alone or in Combination (trial); ANA, anastrozole; TAM, tamoxifen; OR, odds ratio; BIG, Breast International Group; LET,letrozole; ABCSG, Austrian Breast and Colorectal Cancer Study Group; GOS, goserelin; ITA, Italian Tamoxifen Anastrozole (trial); TEAM, Tamoxifen ExemestaneAdjuvant Multinational (trial); EXE, exemestane; IES, Intergroup Exemestane Study; N-SAS, National Surgical Adjuvant Study (Group); ARNO, Arimidex-Nolvadex(trial); NSABP, National Surgical Adjuvant Breast and Bowel Project; NR, not reported.
aDiarrhea.bDepression or sleep disturbance.cNeurologic or psychiatric disorder.dGI complaints.eDepression.fMood fluctuations.gGrade 1 only.hGrades 1 to 4.iGrade 3 or 4 toxicity.jSubset analysis: N (LET) � 1,813; N (placebo) � 1,799.
ASCO Guideline for Adjuvant Endocrine Therapy for Breast Cancer
© 2010 by American Society of Clinical Oncology 23

Potentially relevant publicationsidentified by electronic searching
and screened for retrieval(n = 484)
Excluded(n = 432)
Other articles recommended by panel members or identified by hand-searching
(n = 13)
Articles retrieved in full copyfor detailed evaluation
(n = 52)
Articles that met selectioncriteria for data extraction
(n = 49)
Excluded(n = 0)
Articles that met selectioncriteria for data extraction
(n = 13)
Excluded(n = 3)
Articles included fordata extraction
(n = 62)
Fig A1. Quorum diagram. Inclusion and exclusion of publications identified for this systematic review.
Burstein et al
24 © 2010 by American Society of Clinical Oncology