pca: against rx + adt as standard of...
TRANSCRIPT

PCa: against RX + ADT as standard of care
N. Mottet
Urology department
St Etienne
Chairman EAU-ESTRO-SIOG prostate cancer guidelines

Disclosures

A dogma for locally advanced PCa "RX + ADT: standard of care "
The correct wording MUST be:
"RX + ADT: standard of care for locally advanced PCa" . . .
. . . . if RX is considered.
Outside this, purely speculative . . .NO RCT at all ! treatment of voiding problems Easier follow upBetter outcome ?Better salvage TTT ?

1. D’Amico. JAMA 1998; 2. Thomson. J Urol 2007; 3. Mottet EAU guidelines 2016; 4. NCCN guidelines 2015; 5. Joniau Eur Urol 2015
What are we talking about ?No real consensus definition !
Guidelines Year Definition
D’Amico1 1998 ≥T2c or Gleason 8-10 or PSA >20 ng/ml
AUA2 2007 cT2 or Gleason 8-10 or PSA >20 ng/ml
EAU3 2015 Localized: T2c or Gleason > 7 or PSA >20 ng/mlLocally advanced: cT3 -4 or cN1
NCCN4 2015 High risk: T3a or Gleason 8-10 or PSA >20 ng/mlVery high risk: T3b-T4, primary grade Gleason 5, > 4 biopsies with Gleason 8-10
Joniau5 2015 PSA > 20 ng/ml or cT3–4 or Gleason > 7

cT3 @ 15 years
Ward BJU Int 2005
CSS
cT2
cT3
cT3
pT2
pT3
pN+
ADT: adjuvant: 51% / salvage: 26%RX: adjuvant: 16% / salvage: 15%
Remember: CSSRTOG 92-02 8 years: 90%EORTC 22863: 10 years: 89%RTOG 8531: 10 years: 84%
90% @ 10 years
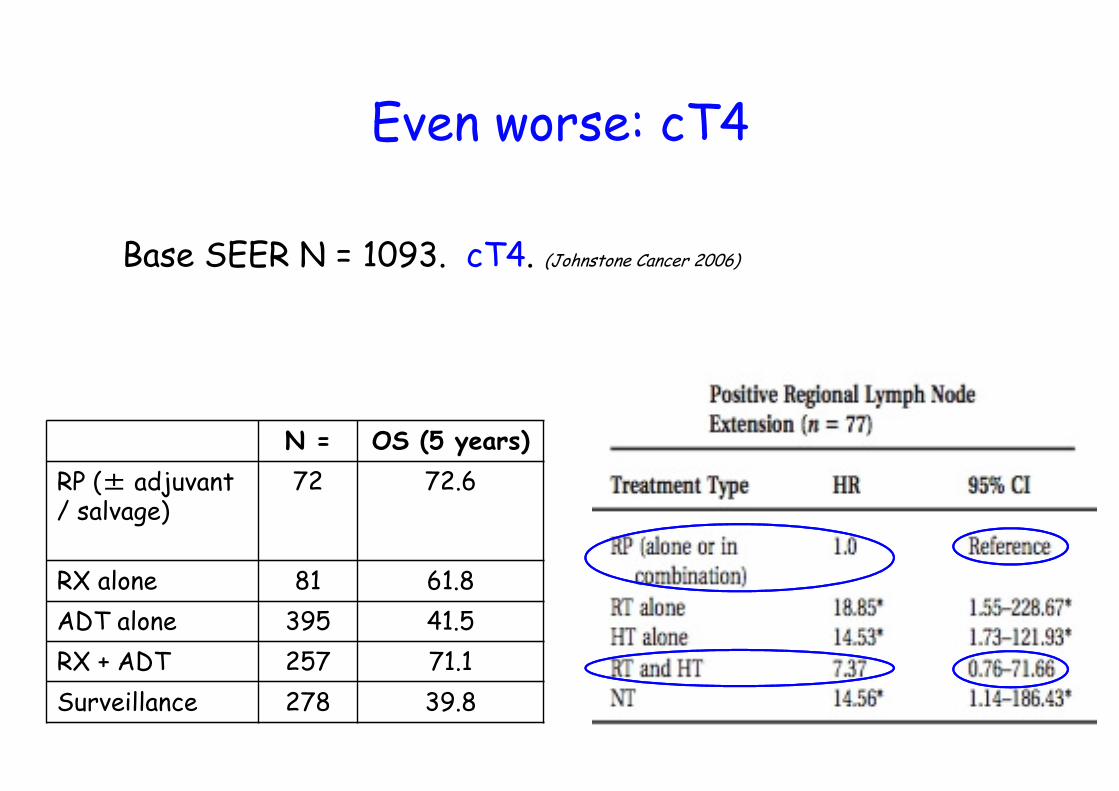
Even worse: cT4
Base SEER N = 1093. cT4. (Johnstone Cancer 2006)
N = OS (5 years)
RP (± adjuvant / salvage)
72 72.6
RX alone 81 61.8
ADT alone 395 41.5
RX + ADT 257 71.1
Surveillance 278 39.8

Surgery . . . Only if extended
Margins: key objective R0
Margins, Gleason > 7, pN: RFS risk factors Karakiewicz Urology 2005
Margins / pT: only independent risk factors for RFS Budaus J Urol 2010

pN+: Local treatment important
Engel Eur Urol 2010
Multivariate (adjusted for age, pT, G, pN)OS: HR: 2.04 si RP stopped
RP stopped PR done
N = 250 688
T3 44.7% 47.7%
N+ 2-3 44% 32%
N+ ≥ 4 28% 17.2%
Overall survival

pN+: Local treatment important
N = 158 pN+ Steuber BJU Int 2011
50: RP stopped / 108: RP done
ADT adjuvant: 92% / salvage: 8%
Overall Paire comparison (38/arm)
+ PR
- PR

RP in advanced PCa: outcome
Same surgeon Gontero Eur Urol 2007
51 cT3, N0-1 / 152 cT1-2
Other cohort (Ward BJU Int 2005) No real difference cT3 / cT1-2
cT1-2 ≥ cT3 cN0-1
N = 152 51
transfusion 29% 47%
Intensive care unit 0% 6%
Hospital stay 7 d 9 d
Lymphocele 3% 12%
Ureteral injury 0 6%
Bladder neck stenosis 18.5% 27%
Full continence @ 1 year 78% 80%
Severe incontinence @ 1 year
10% 16%

Surgery vs radiotherapy ? ? ? Wallis Eur Urol 2016
Meta-analysis from 95 791 patients
OS CSS

Surgery vs radiotherapy ? ? ?
Major limitations - NO RCT
- comparison as a whole [no stratification] (RX + ADT in intermediate / high risk: standard: never mentioned / specificaly analysed)
- No information on RX template / dose
- Only restrospective data

Retrospective / prospective data
Dugenais. Curr Cardiol Rep 2000
β-carotene and CV mortality
PROTEC ( Hamdy N Engl J med 2016 )
To solve this question . . . . .
But NOT in locally advanced !
BUT SPCG 15

EAU-ESTRO-SIOG guidelines