pauline norris (university of otago, new zealand): insight in the new zealand health care system,...
TRANSCRIPT

Insight into the New Zealand health
care system, with a focus on
medicines
Pauline Norris
Professor of Social Pharmacy
University of Otago

• Land area similar to Finland• NZ: 268,000km2
• Finland: 338,000km2
• Population similar to Finland• NZ: 4,570,000
• Finland: 5,477,000

Economy and Health
New Zealand Finland
GDP/person $36,152 $40,838
Gini index 36.2 25.9
Life Expectancy 83.2 (f) 79.5 (m) 83.3 (f) 76.24 (m)
Infant Mortality 4.65 3.38

Health System
New Zealand Finland
Expenditure (US$, PPP) 3182 3374
Expenditure as % of GDP 10.3 9.0
Out of pocket spending as
proportion of total
household consumption
1.8 2.9

New Zealand Health System
• Tax funded: government allocates funding from income tax, sales tax and other taxes to Health
• Ministry of Health: central agency, policy, regulatory functions (including licensing of medicines, pharmacovigilance, classification of medicines)
• Funding allocated by government to 20 District Health Boards (DHBs) (according to a formula based on population and other factors)

District Health Boards
• Responsible for health services in their region
• Provide services (mainly hospitals) and contract with private providers: community pharmacies, primary care doctors (general practitioners), home care providers etc.

Patient charges
• Public Hospital care free (including medicines taken while in hospital)
• Primary care: doctors’ visits (about NZ$40 -$60: 39 Euros) and prescriptions ($5, 3.26 Euro per item)
• Patients register with a regular GP, but can go to any pharmacy

Private hospitals and insurance
• Private hospitals provide only small range of surgery, specialists consultations
• Life-threatening problems always dealt with in public sector
• Private health insurance (30.8% of population, but small contribution to healthcare funding)

Medicines

Medicines reimbursement
• Since 1941, government has been the major funder of medicines
• 1941 – late 1980s: government administered the reimbursement but did not actively manage expenditure
• 1980s: fiscal problems, expenditure growing rapidly, patient charges introduced and increased
• 1993: PHARMAC established to take advantage of monopsony position of government

PHARMAC
• Goal: “Secure for eligible people in need of pharmaceuticals, the best health outcomes that can reasonably be achieved, and from within the amount of funding provided.”
• Must work within an annual budget
• Politically independent
• Advised by Pharmacology and Therapeutics Advisory Committee (but this advice is not binding)
• About 105 staff

PHARMAC’s role
• Referred to as government’s “Drug buying agency” but really more like “government’s personal shopper”
• Evaluating, bargaining, decision-making
• Budget holding

Strategies
• Being an active buyer: controlling access to reimbursement
• Positive list: Pharmaceutical Schedule of medicines that will be reimbursed, and prices (approx. 2000 products)
• Reimbursed only if prescribed (although many also available OTC)
• Extensive use of cost-utility analysis

Decision Criteria• The health needs of all eligible people;
• The particular health needs of Māori and Pacific peoples;
• The availability and suitability of existing medicines, therapeutic medical devices and related products and related things;
• The clinical benefits and risks of pharmaceuticals;
• The cost-effectiveness of meeting health needs by funding pharmaceuticals rather than using other publicly funded health & disability support services;
• The budgetary impact (in terms of the pharmaceutical budget and the Government’s overall health budget) of any changes to the Schedule;
• The direct cost to health service users;
• The Government’s priorities for health funding
• Such other criteria as PHARMAC thinks fit

• Increasing price competition:
• Reference pricing (of groups of medicines, such as ACE inhibitors)• Paying the same amount for drugs with similar outcomes (whether patent
or generic)
• Patients pay any cost above the reference price
• Targetting
• Bundling of contracts
• Sole supplier and Preferred supplier agreements (for one year)
• Cost-sharing with companies
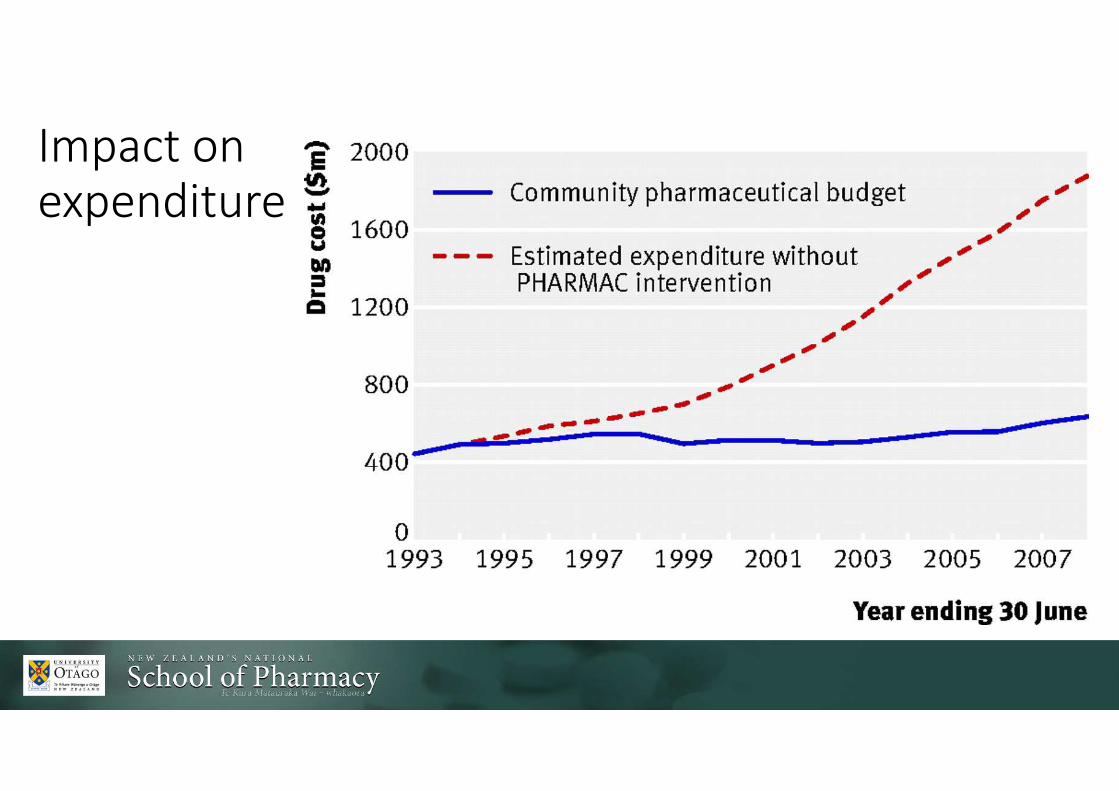
Impact on
expenditure


Responses to PHARMAC
• 1990s: turbulent period
• Legal challenges, lobbying, media campaigns, opposition from doctors and patients

Current situation
• Survived many different governments, many health reforms
• Overruled only twice in 22 years (Interferon B and Herceptin)
• Occasional controversies, but mostly “business as usual”
• Good working relationships between PHARMAC and pharmaceutical industry:
“both groups are aware of each others’ positions, and willing to work together in a pragmatic manner within the political reality that exists in New Zealand”
• Started with community medicines, then hospital medicines, medical devices in the future

Why has it worked?
• Is PHARMAC, like the Kiwi, unique to New Zealand? (Davis, 2004)
• Statutory independence
• Capped budget
• Very little pharmaceutical industry in New Zealand

Do people get the medicines
they need?

Range of medicines reimbursed
• More medicines reimbursed with small increases in expenditure
• Comparison of NZ, Australia, UK and VA system in the US (Ragupathy et al. 2012) showed that PHARMAC subsidized the fewest entities, the oldest entities and the fewest innovative entities
• Aaltonen et al (2010) found the share of licensed and launched innovative medicines was significantly smaller in New Zealand than in Finland, but clinically relevant differences were rarely found

Can people afford reimbursed medicines?
• Ethnic and socioeconomic inequalities in health
• Reducing these is key priority for health system

• PHARMAC does not set prescription charges for patients: these are decided by government
• Much lower in New Zealand than Finland (3.26 Euros per item)
• Flat rate irrespective of condition, medicine, age (except children), income
• Recent research shows much lower than expected use of medicines by Maori
• Prescription charges are likely to be one reason for this
Future Challenges to access to medicines in
New Zealand
• Expensive new medicines
• Aging population?
• Trans-Pacific Partnership Agreement (TPPA)
• How to target funding to reduce the impact of inequality

References
• http://www.pharmac.health.nz/assets/factsheet-01-introduction-to-pharmac.pdf
• Davis, P., "Tough but fair"? The active management of the New Zealand drug benefits scheme by an independent Crown agency. Australian Health Review, 2004. 28(2): p. 171-181.
• Gauld, R., Ahead of Its Time? Reflecting on New Zealand’s Pharmac Following Its 20th Anniversary.PharmacoEconomics, 2014. 32: p. 937-942.
• Aaltonen, K., et al., The impact of pharmaceutical cost containment policies on the range of medicines available and subsidised in Finland and New Zealand. Value in Health, in press. 13(1): p. 148-156.
• Ragupathy, R., et al., Key Informants’ Perceptions Of How PHARMAC Operates In New Zealand. International Journal of Health Technology Assessment, 2012. 28(4): p. 367-373.
• Ragupathy, R., et al., A 3-dimensional view of access to licensed and subsidized medicines under single-payer systems in the US, the UK, Australia and New Zealand. PharmacoEconomics, 2012. 30(11): p. 1051-1065.
• Cumming, J., N. Mays, and J. Daube, How New Zealand has contained expenditure on drugs. BMJ, 2010. 340(may18_1): p. c2441-.
• Health at a Glance 2013 OECD INDICATORS