patrÍcia maria fernandestaurus.unicamp.br/bitstream/reposip/322216/1/fernandes...66 crânios secos...
TRANSCRIPT

PATRÍCIA MARIA FERNANDES
AVALIAÇÃO DAS DIMENSÕES DA FOSSA INCISIVA EM CRÂNIOS
SECOS HUMANOS ATRAVÉS DE RADIOGRAFIA OCLUSAL E
TOMOGRAFIA COMPUTADORIZADA FEIXE CÔNICO
EVALUATION OF INCISIVE FOSSAE DIMENSIONS ON HUMAN DRY SKULLS
BY OCCLUSAL RADIOGRAPHY AND CONE-BEAM COMPUTED
TOMOGRAPHY
Piracicaba
2017
UNIVERSIDADE ESTADUAL DE CAMPINAS
FACULDADE DE ODONTOLOGIA DE PIRACICABA
PATRÍCIA MARIA FERNANDES
AVALIAÇÃO DAS DIMENSÕES DA FOSSA INCISIVA EM CRÂNIOS
SECOS HUMANOS ATRAVÉS DE RADIOGRAFIA OCLUSAL E
TOMOGRAFIA COMPUTADORIZADA FEIXE CÔNICO
EVALUATION OF INCISIVE FOSSAE DIMENSIONS ON HUMAN DRY SKULLS
BY OCCLUSAL RADIOGRAPHY AND CONE-BEAM COMPUTED
TOMOGRAPHY
Dissertação apresentada à Faculdade de
Odontologia de Piracicaba da Universidade
Estadual de Campinas como parte dos
requisitos exigidos para a obtenção do título de
Mestra em Estomatopatologia, na Área de
Estomatologia.
Dissertation presented to the Piracicaba Dental
School of the University of Campinas, in partial
fulfillment of the requirements for the degree of
Master of Stomatopathology in the area of
Stomatology.
Orientador: Prof. Dr. Márcio Ajudarte
Lopes
Este exemplar corresponde à versão final
da dissertação defendida pela aluna
Patrícia Maria Fernandes e orientada pelo
Prof. Dr. Márcio Ajudarte Lopes
Piracicaba
2017



DEDICATÓRIA
À Deus, minha fonte de fé e perseverança, por iluminar os meus caminhos e me
proteger;
Às grandes responsáveis pelo êxito desta etapa, às pessoas que mais amo e
admiro: minhas mães, Ana e Inez.
AGRADECIMENTOS
À Universidade Estadual de Campinas, na pessoa do Magnífico Reitor, Prof. Dr. José
Tadeu Jorge.
À Faculdade de Odontologia de Piracicaba, na pessoa de seu Diretor, Prof. Dr.
Guilherme Elias Pessanha Henriques e seu Diretor Associado, Prof. Dr. Francisco
Haiter Neto.
À Profa. Dra. Cínthia Pereira Machado Tabchoury, Coordenadora Geral da Pós-
graduação da Faculdade de Odontologia de Piracicaba.
Ao Coordenador do Programa de Pós-graduação em Estomatopatologia e também
meu orientador, Prof. Dr. Márcio Ajudarte Lopes, pela oportunidade de cursar o
mestrado, pela paciência quase infinita, pelos ensinamentos e pelas oportunidades.
Aprendemos com o Prof. Márcio, não apenas as questões do domínio de nossa
especialidade, mas também como podemos ser líderes, com propriedade sem sermos
arrogantes, de forma que sejamos respeitados e admirados pelos que nos cercam.
Ao Prof. Dr. Alan Roger dos Santos Silva, que me proporcionou a primeira
oportunidade na área da estomatologia. Embora não tenhamos trabalhado próximos
no período do mestrado, serei sempre grata pelas primeiras oportunidades cedidas,
pelo modo cordial pelo qual sempre nos tratamos e pela relação amistosa que
mantemos.
Aos demais Profs. Drs. do Programa de Pós-graduação em Estomatopatolgia da
Faculdade de Odontologia de Piracicaba: Oslei Paes de Almeida, Pablo Augustin
Vargas, Jacks Jorge Junior, Ricardo Della Coletta e Edgard Graner.
Aos professores da Área de Anatomia da Faculdade de Odontologia de Piracicaba,
Ana Cláudia Rossi e Felippe Bevilacqua Prado, por ceder o material necessário para
a realização deste estudo, pela disponibilidade, parceria e amizade.
À equipe do Orocentro, Daniele, Cida, Rogério, Maria Aparecida, Bete, Érika e
professores Márcio e Alan, pela acolhida e infinitos ensinamentos. O Orocentro é
quase uma utopia. E o trabalho lá realizado é, acima de tudo, um serviço ao próximo.

À equipe do CEON, Diego, Renata, Isabel, Pedro, Silvana, Juliana, Ana Carolina, Iara,
Brigida e Dr. Vinícius, pela sintonia de trabalho que temos. Lutamos muito para
oferecer aos pacientes com câncer a melhor abordagem, mais humana e
multidisciplinar possível, de forma a tentar amenizar ao máximo seu sofrimento.
Aos pacientes atendidos no Orocentro e Ceon, que nos ensinam tanto sobre a vida.
Todo o trabalho que é realizado, tanto em pesquisa quanto no atendimento, tem como
missão e objetivo final o benefício àquele que nos procura.
Aos meus amigos e colegas de pós-graduação, pela amizade e companheirismo.
Acredito que a grande diversidade cultural que existe entre nós seja o maior presente
que recebemos. Conhecemos o mundo sem sair da FOP, aprendemos novos
costumes e modos de falar, nos amparamos uns aos outros, pois, apesar de oriundos
de lugares distantes entre si, temos todos o mesmo objetivo. Agradeço em especial
meu amigo Vinícius que, além de ótimo profissional e pessoa generosa, foi meu
parceiro e primeiro incentivador para a realização deste trabalho.
Às minhas mães, Ana e Inez, por sempre acreditarem nos meus sonhos e objetivos
mesmo quando estes estavam muito além de nossas possibilidades. Agradeço por
aceitarem cada novo desafio de coração aberto e confiantes de que tudo é parte de
um plano maior.
Aos meus irmãos de coração, Jefferson e Robson, que me acompanham desde que
nasci e que, de forma generosa, trabalharam e cederam de diversas formas para que
meu irmão e eu tivéssemos sempre as melhores oportunidades. Agradeço também
ao meu irmão Gustavo, que apesar de todas as divergências de gênio e opinião,
sabemos que sempre poderemos nos apoiar um no outro.
Ao meu namorado e amigo, Henrique, por todo comprometimento e generosidade,
pelo exemplo que é de coragem e determinação. Agradeço também à sua família:
mãe, pai e avó por me acolherem em Piracicaba e fazerem me sentir em casa.

RESUMO
A fossa incisiva é uma estrutura anatômica localizada na linha média de maxila
anterior, posterior aos incisivos centrais. Além dos feixes neurovasculares
provenientes do canal incisivo, a fossa incisiva também abriga estruturas vestigiais,
que favorecem o surgimento de lesões nesta região. Entre as alterações que podem
ocorrer nesta área, a mais comum é o cisto do ducto nasopalatino (CDNP). Devido à
grande variação anatômica da fossa incisiva, o diagnóstico diferencial entre uma fossa
incisiva alargada e lesões císticas, que acometem a maxila anterior pode ser
desafiador. O objetivo deste estudo foi determinar as dimensões da fossa incisiva em
crânios secos humanos e em suas respectivas imagens radiográficas oclusais (RO) e
em imagens de tomografia computadorizada cone-beam (TCCB). Foram selecionados
66 crânios secos humanos, os quais foram submetidos a RO de maxila. As medidas
lineares relativas a largura (medida látero-lateral) e comprimento (medida ântero-
posterior) da fossa incisiva foram aferidas nos crânios e nas RO. Os crânios que
apresentaram largura mínima da fossa incisiva de 6 mm nas RO, foram submetidos
ao exame de TCCB e tiveram as medidas da fossa incisiva aferidas novamente. A
largura média das fossas incisivas nos crânios foi de 5,18 mm e o comprimento médio
foi de 8,22 mm. Nas RO, a largura média foi de 5,05 mm e o comprimento médio foi
de 9,23 mm. Os 13 casos avaliados por TCCB tiveram largura média de 6,00 mm e
comprimento médio de 6,66 mm. A RO de maxila se mostrou um exame confiável para
a determinação da largura da fossa incisiva (p=0,1046) porém, apresentou limitações
em reproduzir o comprimento (p=0,005). Em casos com largura ≥ 6 mm, a TCCB pode
contribuir para uma melhor avaliação das características anatômicas da fossa incisiva,
evitando intervenções mais invasivas.
Palavras-chave: Cisto do ducto nasopalatino, fossa incisiva, radiografia oclusal,
tomografia computadorizada.

ABSTRACT
The incisive fossa is an anatomical structure located in the midline anterior maxilla,
posterior to the anterior teeth. Aside the neurovascular bundle from the incisive
channel, the incisive fossa also keep vestigial structures that contribute to the
development of lesions in this region. Among the alterations that can occur in this area,
the most common is the nasopalatine duct cyst (NDC). Due to a wide anatomic
variation of incisive fossa, the differential diagnosis between an enlarged incisive fossa
and cystic lesions that occur in anterior maxilla can be a challenge. The aim of this
study was to determine the incisive fossa dimensions in human dry skulls as well as
its dimensions on occlusal radiographic (OR) and cone-beam computed tomography
(CBCT) images. It was selected 66 human dry skulls which were submitted to OR of
maxilla. The linear measurements corresponding to width and length of incisive fossa
were assessed on dry skulls and on OR. The dry skulls which presented incisive fossa
width equal or greater than 6 mm on OR, were submitted to CBCT and its measures
were assessed again. The incisive fossa of dry skulls revealed a mean width of 5.18
mm and mean of length of 8.22 mm. The OR revealed a mean width of 5.05 mm and
mean length of 9.23 mm. In the 13 cases evaluated by CBCT, the mean width was
6.00 mm and the mean length was 6.66 mm. The OR showed to be a reliable exam to
determine the incisive fossa width observed on dry skulls (p=0.1046), although it had
limitations in reproducing the length (p=0.005). In the cases with width ≥ 6 mm, the
CBCT can contribute to a better evaluation of anatomic features of incisive fossa,
avoiding invasive interventions.
Keywords: Nasopalatine duct cyst, incisive fossa, occlusal radiography, cone-beam
computed tomography.
SUMÁRIO
1. INTRODUÇÃO...........................................................................................10
2. ARTIGO: EVALUATION OF INCISIVE FOSSAE DIMENSIONS ON
HUMAN DRY SKULLS BY OCCLUSAL RADIOGRAPHY AND
CONE-BEAM COMPUTED TOMOGRAPHY………………………….…….15
3. CONCLUSÃO...………………………………………………………..………..28
REFERÊNCIAS*.........................................................................................29
APÊNDICE1 – Figuras complementares ………..………………..…….…...32
ANEXO 1 – Certificado do Comitê de Ética em Pesquisa……………........34

10
1. INTRODUÇÃO
A formação da face e da cavidade oral dos humanos se dá entre a quarta
e oitava semanas de vida intrauterina. Uma das etapas que faz parte deste processo
é a construção do palato, que se dá em dois momentos distintos: pelo
desenvolvimento do palato primário e secundário (Allard et al., 1981).
O palato primário compõe a região anterior da maxila e é a estrutura que
dará origem à porção anterior do palato duro nos adultos. É formado pela fusão das
saliências nasais medianas, por volta da sétima semana de vida intrauterina. O palato
secundário, por sua vez, dará origem à porção posterior do palato duro e é formado
pelos processos palatinos laterais bilaterais que se projetam ínfero-medialmente e de
forma paralela à língua. Com o desenvolvimento da mandíbula, a língua toma uma
posição mais inferior, acomodando-se em seu leito e permitindo que os processos
palatinos laterais finalmente possam se fundir, dando origem à rafe palatina mediana
(Neville; 2004, Moore; 2012).
Posteriormente, há o desenvolvimento de osso no palato primário e
secundário, formando assim o palato duro como é conhecido nos indivíduos adultos.
As porções dos processos palatinos laterais que estão posteriores ao septo nasal não
são calcificadas, pois irão formar o palato mole e a úvula. Tais eventos ocorrem entre
a sexta e oitava semanas de vida intrauterina. Embora a formação do palato promova
a separação entre cavidade bucal e cavidade nasal, dois trajetos mantêm uma
comunicação entre o epitélio nasal e oral no momento da união dos palatos primário
e secundário: os canais incisivos (Allard et al., 1981; Neville; 2004, Moore; 2012).
Os canais incisivos são ductos intra-ósseos que contém em seu interior o
nervo nasopalatino, ramos da artéria palatina descendente e esfenopalatina além de
uma estrutura epitelial de padrão heterogêneo, uni ou bilateral, denominada ducto
nasopalatino (Allard et al.,1981; Neville; 2004). Tais ductos se originam no assoalho
da cavidade nasal, bilateralmente, se projetam ínfero-anteriormente, fundindo-se em
forma de “Y” antes de desembocar na região anterior de palato duro, em uma região
logo abaixo da papila incisiva, chamada de fossa incisiva (Allard et al.,1981; Neville;
2004). A fossa incisiva é uma depressão “em forma de funil” encontrada no palato
duro imediatamente posterior ao processo alveolar da maxila e aos incisivos centrais
superiores, logo acima da papila incisiva (Chamda et al., 1980). A fossa incisiva pode
abrigar lesões provenientes dos elementos vestigiais contidos no interior dos canais

11
incisivos. Alterações patológicas que podem ser observadas nessa região incluem:
cistos radiculares, cistos dentígeros, cistos palatinos medianos ou cistos da papila
incisiva, fístulas oronasais e buco-sinusais, além do cisto do ducto nasopalatino
(CDNP). Este último é considerado o cisto não-odontogênico de maior frequência na
maxila (Moss et al., 2000; Grossmann et al. 2007; Falci et al., 2013).
O cisto do ducto nasopalatino ocorre na linha média do palato anterior, logo
abaixo na papila incisiva, posterior aos incisivos centrais superiores (Shear M., 2007;
Dedhia et al., 2013). A etiologia do CDNP ainda é controversa na literatura e alguns
fatores etiológicos sugeridos incluem trauma, infecção do ducto nasopalatino,
retenção de muco por glândulas salivares menores presentes na região, derivação do
epitélio do órgão de Jacobson. Porém, é mais aceito que essa lesão represente uma
degeneração cística espontânea de remanescentes do ducto nasopalatino (Saunders
et al., 1968; Bodin et al., 1986; Tsuneki et al., 2013; Cecchetti et al., 2013; Falci et al.,
2013; Sane et al., 2014).
Clinicamente, os CDNP são lesões de crescimento lento e assintomáticas
sendo descobertas, ocasionalmente, através de exames clínicos e/ou radiográficos
realizados para outras finalidades (Allard et al.,1981; Shear M., 2007; Suter et al.,
2011; Cecchetti et al., 2013;). Há predileção pelo gênero masculino em uma relação
de 2:1 e, apesar de ocorrer mais comumente entre a terceira e quinta décadas de
vida, pode manifestar-se em qualquer idade (Swanson et al.,1991; Grossmann et
al.,2007; Nonaka et al.,2011; Cecchetti et al.,2013). Há uma frequência aumentada do
CDNP na raça negra, para ambos gêneros, ainda que se mantenha a predominância
em homens (Hertzanu et al., 1985; Swanson et al.,1991). Lesões agressivas,
representadas pelo rápido crescimento, sintomáticas e de maior diâmetro foram
reportadas especialmente em jovens negros oriundos da África do Sul (Nortje et
al.,1978; Hertzanu et al., 1985).
Se infectado, o CDNP pode gerar dor e tumefação na região anterior de
palato, com formação de fístula e drenagem de secreção fibrinopurulenta (Allard et
al.,1981; Suter et al.,2011). Apesar da dor ser um achado incomum, esta pode ser
explicada devido à expansão cística no interior do canal incisivo com consequente
compressão dos nervos palatinos (Allard et al.,1981). Parece não haver relação direta
entre presença e intensidade dos sintomas com as dimensões da lesão (Suter et
al.,2011). Os dentes ântero-superiores costumam responder positivamente ao teste
de vitalidade pulpar e, radiograficamente, a lâmina dura destes dentes está
12
preservada (Allard et al.,1981; Suter et al.,2011; Dedhia et al.,2013) exceto nas lesões
de grandes dimensões que, apesar de raras, podem se estender para assoalho nasal,
causando destruição óssea, reabsorção radicular, necrose pulpar e deslocamento dos
dentes envolvidos, podendo levar até um comprometimento estético facial importante
com protrusão nasolabial (Tanaka et al.,2008).
Tanto para diagnóstico do CDNP quanto para avaliação das estruturas
normais da região anterior de maxila, as radiografias panorâmicas, oclusais e
tomografias computadorizadas são exames de imagem bastante usados (Killey et al.,
1972; Chamda et al., 1980).
Em radiografias panorâmicas e oclusais, o CDNP se apresenta como uma
área radiolúcida de forma arredondada, ovóide, pêra invertida ou ainda em formato de
“coração”, resultante da sobreposição da espinha nasal e chanframento da lesão pelo
septo nasal (Suter et al., 2011; Sane et al., 2014).
Em cortes axiais de tomografia computadorizada, o CDNP se apresenta
como uma área hipodensa, arredondada, bem circunscrita na linha média da maxila
em íntima relação com os ápices dos incisivos centrais superiores estendendo-se
lateralmente de maneira simétrica (Schiff et al.,1969; Nonaka et al.,2011; Dedhia et
al.,2013).
Estruturas normais da região anterior de maxila também podem ser
visualizadas através de radiografias oclusais e cortes axiais de tomografia
computadorizada. A fossa incisiva pode se apresentar como uma região radiolúcida
mais alongada em relação à imagem do CDNP, podendo apresentar menor
radiolucidez devido à menor profundidade ou demonstrar septos ósseos em seu
interior. Porém, muitas vezes, a fossa incisiva se apresenta radiograficamente muito
semelhante à lesões císticas (Abrams et al., 1963).
Devido à grande variação anatômica dos canais incisivos e da fossa
incisiva, é comum existir dificuldades para diferenciar um pequeno CDNP de uma
fossa incisiva alargada (Anneroth et al.,1986; Bodin et al.,1986; Neville;2004).
Concomitantemente a este fato, a técnica radiográfica empregada para diagnóstico
pode gerar confusão, uma vez que a magnificação das imagens em radiografias
panorâmicas e a angulação dos aparelhos radiográficos para tomadas periapicais e
oclusais podem alterar o tamanho aparente da área avaliada, gerando dúvidas quanto
ao diagnóstico (Swanson et al.,1991; Srivastava et al., 2013).

13
Em um dos primeiros estudos do gênero, Roper-Hall e colaboradores, em
1938, mensuraram as dimensões da fossa incisiva de 2.162 crânios secos e a
incidência de CDNP nesses crânios. A largura (medida látero-lateral) encontrada foi
de 3 mm, altura de 2 a 3 mm e o comprimento (medida ântero-posterior) de 3 mm. A
presença de lesões císticas foi considerada rara. Tal trabalho não avaliou os crânios
radiograficamente e, mesmo assim, extrapolou-se para a prática clínica que imagens
radiolúcidas na região de fossa incisiva, com até 6 mm de diâmetro e na ausência de
sintomas deveriam ser consideradas como fossa incisiva dentro dos padrões de
normalidade. Até os dias atuais esse conceito é usado pelos clínicos. Em 1972, Killey
& Kay, avaliaram as dimensões de 2.394 fossas incisivas em crânios secos, obtendo
médias de 4-5 mm de largura e 4 mm de comprimento. Os autores também realizaram
um estudo comparativo entre as medições realizadas em crânios secos humanos com
medições realizadas em radiografias, constatando que as distorções do tamanho da
fossa incisiva são mínimas em radiografias. Além disso, foram relatados apenas dois
casos de CDNP em sua amostra. Chamda & Shear, em 1980, avaliaram as dimensões
da fossa incisiva e a frequência de CDNP em 960 crânios secos humanos
provenientes de pessoas de raça negra. Deste total, 200 crânios foram selecionados
para análise radiográfica visando-se estabelecer uma correlação entre os achados
radiográficos e as medições realizadas diretamente das peças anatômicas. As médias
das medições da fossa incisiva nos crânios secos foram de 4,79 mm de largura, 4,44
mm de altura, 10,19 mm de comprimento. As médias encontradas nas medições
realizadas nas radiografias foram de 4,50 mm de largura e comprimento de 11,67 mm.
Segundo os autores, os resultados indicaram que as formas de medição foram
significantemente diferentes e que é inválido extrapolar uma medição a partir de outra.
Infelizmente, o método exato para a obtenção das medidas nas radiografias não foi
descrito. Nesse artigo, foram relatados 13 casos de CDNP na amostra.
As dimensões do CDNP podem variar de pequenas lesões com diâmetro
menor que 6 mm a lesões potencialmente destrutivas com grandes dimensões
(Neville, 2004). Swanson et al, em 1991, analisaram 334 casos de CDNP e
encontraram que o diâmetro médio dos cistos nas análises radiográficas era de
17.1mm, porém, 75% das lesões possuíam um diâmetro menor que 20 mm. Suter e
colaboradores em 2011 encontraram, através de tomografias computadorizadas de
feixe cônico, um diâmetro médio de 15 mm em 25 casos de CDNP. Hertzanu e
colaboradores em 1985 aferiram os diâmetros médios de 114 casos de CDNP.

14
Desses, 30 casos eram provenientes de pacientes negros e todos cistos excederam
30 mm de diâmetro, sugerindo um componente de agressividade na raça negra.
Entretanto, outras características clínicas e radiográficas, além das
dimensões, podem ser utilizadas para diferenciar um CDNP de uma fossa alargada.
Sinais e sintomas como edema e dor na região parece ser um fator importante a ser
considerado para diagnóstico final e, consequentemente, intervenção cirúrgica
(Swanson et al., 1991).
Abrams e colaboradores, em 1963, estabeleceram alguns critérios
radiográficos que também podem ser utilizados para essa diferenciação tais como: as
margens de um cisto são mais bem definidas do que as de uma fossa ou forame
normais, os cistos verdadeiros são frequentemente mais esféricos que a fossa, o
forame ou fossa incisiva normal, em geral, não possui halo cortical bem demarcado
em seus limites anterior e posterior. Entretanto, mesmo com critérios bem
estabelecidos, uma diferenciação radiológica entre um CDNP e uma fossa incisiva
alargada pode ser difícil e levar a diagnósticos incorretos, já que um CDNP infectado
pode apresentar-se com um padrão radiográfico incomum, com radiolucidez menor,
contornos incompletos e bordas difusas (Bodin et al., 1986).
Tendo em vista este cenário desafiador em termos de diagnóstico clínico-
radiográfico e os poucos estudos publicados sobre o tema, esta dissertação se propôs
a determinar as dimensões da fossa incisiva em crânios secos humanos, em suas
respectivas imagens radiográficas oclusais e em imagens de tomografia
computadorizada cone-beam.
15
2. ARTIGO: EVALUATION OF INCISIVE FOSSAE DIMENSIONS ON HUMAN
DRY SKULLS BY OCCLUSAL RADIOGRAPHY AND CONE-BEAM
COMPUTED TOMOGRAPHY
Artigo submetido ao periódico Oral Surgery Oral Medicine Oral Pathology Oral
Radiology
Patrícia Maria Fernandes, DDS 1
Vinícius Rabelo Torregrossa DDS, MsC1
Alan Roger Santos-Silva, DDS , PhD1
Ana Cláudia Rossi, DDS, PhD2
Felippe Bevilacqua Prado, DDS, PhD2
Marcio Ajudarte Lopes DDS, PhD1
1Department of Oral Diagnosis, Piracicaba Dental School, University of Campinas,
Piracicaba, Brazil.
2 Department of Morphology, Piracicaba Dental School, University of Campinas,
Piracicaba, Brazil.
Correspondence.
Marcio Ajudarte Lopes, Department of Oral Diagnosis, Piracicaba Dental School,
University of Campinas, Avenida Limeira 901, Caixa Postal 52, Piracicaba – SP, CEP:
13414-903, Brasil. e-mail:[email protected].

16
Abstract
Objective: To determine the dimensions of the incisive fossae in human dry skulls, in
their respective occlusal radiographs images and in cone-beam computed tomography
images.
Study design: 66 human dry skulls were submitted to maxillary occlusal radiography
(OR). The linear measurements corresponding to width and length of incisive fossae
were assessed on dry skulls and on OR. The cases, which presented incisive fossae
width equal or greater than 6 mm on OR were submitted to cone-beam computed
tomography (CBCT) and their measures were assessed again.
Results: The dry skulls revealed mean value for incisive fossae width of 5.18 mm and
for length of 8.22 mm. The OR measurements revealed mean value width of 5.05 mm
and mean length of 9.23 mm. The CBCT measurements revealed mean value width of
6.00 mm and mean length of 6.66 mm.
Conclusion: The OR showed to be a reliable exam to reproduce the incisive fossae
width (p=0,1046), although it had limitations in evaluating the length (p=0.005). In the
cases with width ≥ 6 mm, the CBCT can contribute to a better evaluation of anatomic
features of incisive fossae, avoiding invasive interventions.
Keywords: Nasopalatine duct cyst, incisive fossa, occlusal radiography, cone-beam
computed tomography.
17
Introduction
The incisive fossa is an anatomical structure that is located in the midline
anterior palate, behind the anterior upper teeth and below the incisive papilla. It is a
funnel-shaped bone depression where emerges the incisive channels5. These
channels connect the floor of the nasal cavity with the oral cavity and they contain a
neurovascular bundle, aside the nasopalatine duct2,5,8. Some lesions can appear in
this region and the most common alteration in the incisive fossa is the nasopalatine
duct cyst6,7,9.
The nasopalatine duct cyst (NDC) is a developmental, epithelial and a non-
odontogenic cyst. It is the most common non-odontogenic cyst in oral cavities,
representing up to 1% of all cysts that occur in the maxilla8,14. An NDC can develop
along the entire length of the nasopalatine duct, including in the incisive fossa region15.
Usually, there are no symptoms or signs associated with this lesion, having
been discovered by routine radiographs7,13,16. When it is possible to see some clinical
manifestation, it is more common to note a swelling in the anterior palate and
occasionally, suppuration. When there is pain, it is usually due to an infection or a
compression of the nasopalatine nerve by dentures8,17.
The occlusal radiography is a very useful examination in order to evaluate
the anterior maxilla6,13. The NDC image usually appears as a well-delimited, round-
shaped lesion, in the incisive fossa region. When the lesion is present, radiographic
images associated with the clinical symptoms and signs are enough to establish a
clinical diagnosis of an NDC, which must be confirmed by histopathology4,15. A normal
incisive fossa can appear on maxillary occlusal radiographs as an elongated
radiolucent region. Nevertheless, it can also demonstrate the same radiographic
aspect as is observed in NDCs4.
Anatomical variations that are present in the incisive foramen and the
incisive fossa can lead to a misdiagnosis of a small NDC, which can easily be mistaken
for an enlarged incisive fossa in radiographic images3,4,12. Normally, the NDC size on
a radiographic image is around 1 cm to 2 cm18. Since 1938, after a study by Roper-
Hall, it has been considered that radiolucent images in the incisive fossa region, being
up to 6 mm in diameter, with a lack of symptoms or signs, are regarded as an enlarged
fossa inside of the normality8,1. Other studies have warned of the fact that the
dimensions as shown by radiographs may exhibit some distortion and they do not

18
represent the correct dimensions5,10,19. In borderline cases, when the incisive fossa
structure is around 6 mm and the patient is asymptomatic, a correct diagnosis can be
a challenge. There are few studies on this subject and there is not a consensus about
the best moment for a surgical intervention. An unnecessary surgical approach can
result in damages at different levels for the affected individuals4,17,18.
Therefore, the aim of this study was to determine the dimensions of the
incisive fossae in human dry skulls, their respective occlusal radiographic and cone-
beam computed tomographic images.
Materials and Methods
Sample and Exclusion Criteria
This study was approved by the local Ethics Committee of Piracicaba Dental
School (Protocol 125/2015), University of Campinas, São Paulo, Brazil.
All the dry skulls used in this study were from Anatomy Area of Piracicaba
Dental School. It was available 93 pieces and those that presented malformations,
fractures or defects around the incisive fossa area were excluded.
After applying the exclusion criteria, it reached the final number of 66 dry
skulls. The whole sample was from the Brazilian population, although their ethnic
information was not available. All dry skulls were from adults with age ranging from 20
to 70 years, being 38 males, 25 females and in 3 cases the gender was not available.
Most of them were edentulous representing 74% of the sample, 23% were partial
toothed and 3% were toothed.
Examiners
All of the steps needed to verify the linear measurements, both in the dry
skulls, as well as in the occlusal radiography and in the computed tomography, were
performed by two previously calibrated examiners. Each measurement was performed
twice, by the same examiner, considering a minimum range of seven days between
the two evaluations.
Dry Skulls
The incisive fossae of the dry skulls had their dimensions concerning the

19
mesiodistal width and the anteroposterior length measured directly on the skulls by a
digital caliper (Starrett – Série 727, Indústria e Comércio Ltda, Itu, São Paulo, Brasil).
Maxillary Occlusal Radiographs
All of the 66 human dry skulls were submitted to maxillary occlusal
radiographs and to perform them, the dry skulls were stabilized by a wooden wedge
which was positioned below the occipital bone.
The radiographic equipment (Sommo Pantográfico de Parede, GNATUS
Equipamentos Médico-Odontológicos Ltda, Ribeirão Preto, São Paulo, Brasil) with a
power of 70kVp and 7mA was used, as well as Insight Radiographic Films (IO-41,
Occlusal, Kodak, NY, USA) measuring 5.7 x 7.6 cm. An occlusal positioner (FPX,
Prisma Instrumentos Odontológicos, Pirituba, São Paulo, Brasil) was also used.
An exposure time of 0.32 seconds was performed. The distance from the x-
ray source to the x-ray film was 40 cm, using a horizontal angle of 0º and a vertical
angle of 65º, according to the occlusal positioner. The processing stage was performed
by an automatic processor (Gendex GXP, Gendex Dental System, Hatfield,
Pennsylvania, USA).
After the processing, the radiographic films were scanned by using an
optical scanner with a transparency reader (HP ScanJet G4050, Hewlett-Packard
Company®, Washington, USA) with a resolution of 300 dpi in 100% of their original
size. The scanned images were archived in a Tagged-Image File Format (TIFF). They
were analyzed in a personal computer and in a dimmed room with ambient light
conditions at a 30 cm distance from the computer screen.
For the evaluations of the linear measurements of the incisive fossae on the
radiographs, the scanned images were submitted to the Image-J-Link Program
(http://rsbweb.nih.gov/ij/index.html). The mesiodistal widths and the anteroposterior
lengths were both performed by an electronic ruler tool.
Cone-Beam Computed Tomography (CBCT) of the Maxilla
The CBCT procedure was performed only in those cases that presented a
mesiodistal width of the incisive fossa ≥ 6 mm on the occlusal radiography. A total of
13/66 cases were submitted to the CBCT procedure. An axial section was used for the
evaluations of the anterior maxilla.
The Cone-Beam Tomographic equipment (Sirona Dental Systems® GmbH,

20
Bensheim, Germany) was used with a voxel size of 0.125 mm, with a field of view of
6x6 cm and with an exposure dose of 6 mGy.
For the analyzes of the linear measurements by the CBCT procedure, the
lowest axial section was selected, that is, the one closest to the palate, in a way that
the outlines of the incisive fossae were all well defined. The anatomical linear
measurements concerning the mesiodistal widths and the anteroposterior lengths of
the incisive fossae were all measured by an electronic ruler tool that was in the
Tomographic Software (Galaxis Galileos Sidexis – Sirona Dental Systems®, Charlotte,
NC, USA).
Statistical Analysis
Data corresponding to mean values ± standard deviation of three replicates
of width and length dimensions were calculated. Intrarater and interrater reliability was
verified by the Intraclass Correlation Coefficient (ICC) and by Kappa test, respectively.
All measurements made directly on dry skulls were statistically compared with those
obtained from the scanned images of maxillary occlusal radiographs and CBCT using
the Tukey-Kramer Test. The level of significance was 5% (P ≤ 0.05).
Results
Dry Skulls
The measurements that were carried out on the dry skulls revealed that the
mean value for the incisive fossae widths was 5.18 mm (CI 95% 5.01-5.36; SD: 1.44)
and for the lengths it was 8.22 mm (CI 95% 7.9 – 8.54; SD: 2.69). The values ranged
from 2.23 mm to 12.46 mm for the widths and from 2.93 mm to 15.72 mm for the
lengths. For the incisive fossae widths, 89.55% of the dry skulls showed
measurements below 6 mm, 8.9% showed measurements of between 6 to 10 mm, and
1.49% showed measurements above 10 mm. For the incisive fossae lengths, 21.21%
showed measurements below 6 mm, 53.03% showed measurements of between 6 to
10 mm, and 25.75% showed measurements above 10 mm. The Intraclass Correlation
Coefficients were 0.94 and 0.96 for the widths and the lengths, respectively, for
Examiner Number 1. They were 0.94 and 0.91 for the widths and the lengths,
respectively, for Examiner Number 2. For the Interclass Correlations, the Kappa test
revealed values of 0.88 for the incisive fossae widths and 0.95 for the incisive fossae
21
lengths.
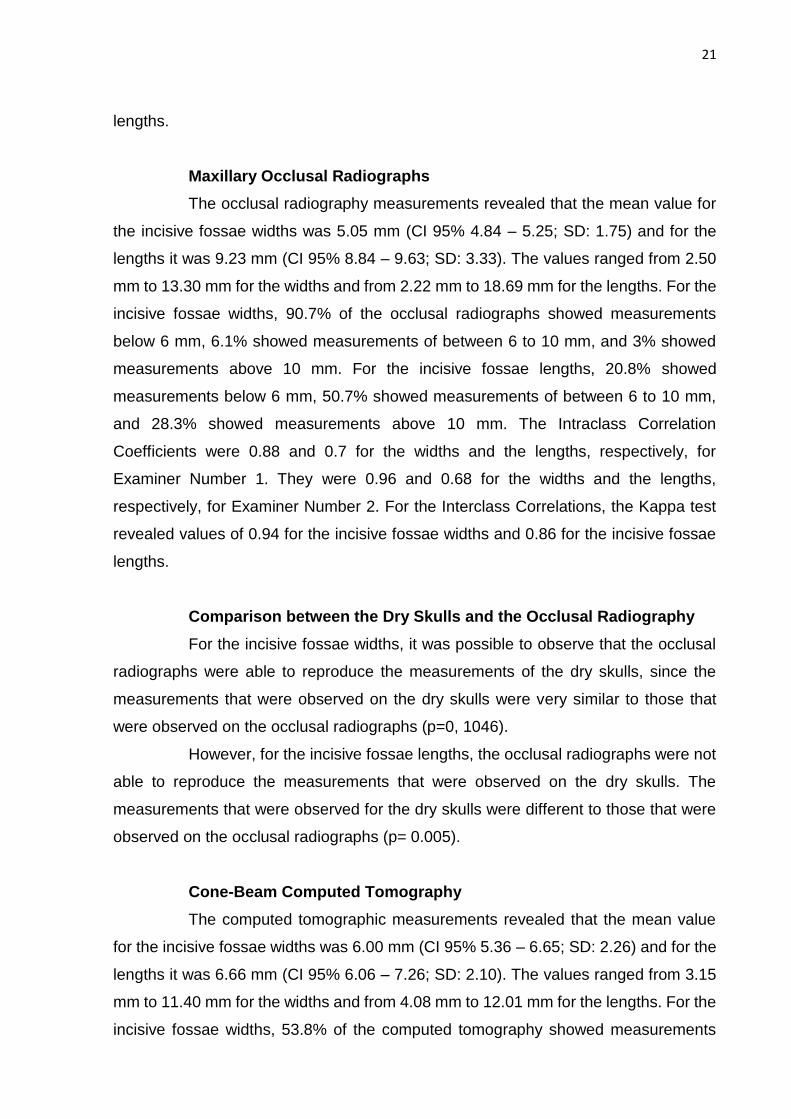
Maxillary Occlusal Radiographs
The occlusal radiography measurements revealed that the mean value for
the incisive fossae widths was 5.05 mm (CI 95% 4.84 – 5.25; SD: 1.75) and for the
lengths it was 9.23 mm (CI 95% 8.84 – 9.63; SD: 3.33). The values ranged from 2.50
mm to 13.30 mm for the widths and from 2.22 mm to 18.69 mm for the lengths. For the
incisive fossae widths, 90.7% of the occlusal radiographs showed measurements
below 6 mm, 6.1% showed measurements of between 6 to 10 mm, and 3% showed
measurements above 10 mm. For the incisive fossae lengths, 20.8% showed
measurements below 6 mm, 50.7% showed measurements of between 6 to 10 mm,
and 28.3% showed measurements above 10 mm. The Intraclass Correlation
Coefficients were 0.88 and 0.7 for the widths and the lengths, respectively, for
Examiner Number 1. They were 0.96 and 0.68 for the widths and the lengths,
respectively, for Examiner Number 2. For the Interclass Correlations, the Kappa test
revealed values of 0.94 for the incisive fossae widths and 0.86 for the incisive fossae
lengths.
Comparison between the Dry Skulls and the Occlusal Radiography
For the incisive fossae widths, it was possible to observe that the occlusal
radiographs were able to reproduce the measurements of the dry skulls, since the
measurements that were observed on the dry skulls were very similar to those that
were observed on the occlusal radiographs (p=0, 1046).
However, for the incisive fossae lengths, the occlusal radiographs were not
able to reproduce the measurements that were observed on the dry skulls. The
measurements that were observed for the dry skulls were different to those that were
observed on the occlusal radiographs (p= 0.005).
Cone-Beam Computed Tomography
The computed tomographic measurements revealed that the mean value
for the incisive fossae widths was 6.00 mm (CI 95% 5.36 – 6.65; SD: 2.26) and for the
lengths it was 6.66 mm (CI 95% 6.06 – 7.26; SD: 2.10). The values ranged from 3.15
mm to 11.40 mm for the widths and from 4.08 mm to 12.01 mm for the lengths. For the
incisive fossae widths, 53.8% of the computed tomography showed measurements
22
below 6 mm, 30.7% showed measurements of between 6 to 10 mm, and 15.3%
showed measurements above 10 mm. For the incisive fossae lengths, 46% showed
measurements below 6mm, 38.4% showed measurements of between 6 to 10 mm,
and 23% showed measurements above 10 mm. The Intraclass Correlation Coefficients
were 0.99 and 0.97 for the widths and the lengths, respectively, for Examiner Number
1. They were 0.99 and 0.98 for the widths and the lengths, respectively, for Examiner
Number 2.
For the Interclass Correlations, the Kappa test revealed values of 0.99 for
the incisive fossae widths and 0.99 for the incisive fossae lengths.
In figure 1, it is possible to observe the image of the dry skull, its respective
occlusal radiography and CBCT. All of the above results are summarized in Table 1.
Discussion
Previous studies, when measuring the linear anatomical measurements of
the incisive fossae, have found width values of around 3 to 5 mm and of 3 to 4 mm for
the lengths in the dry skulls10,11. Our results have demonstrated a mean width that was
similar (5.18 mm), but the lengths have demonstrated higher values on the dry skulls
when in comparison to these anterior papers (8.22 mm), though the examiners were
in agreement with their measurements (k=0.95). However, our study has found results
very similar to Chamda & Shear´s paper (1980), which checked the linear
measurements of the incisive fossae on dry skulls and their radiographs. They found
a mean width of 4.74 mm and a mean length of 10.19 mm on the dry skulls and a mean
width of 4.5 mm and a mean length of 11.67 mm on the radiographs. In their sample,
there were only negroid skulls. Maybe this racial segment presents larger dimensions
of the incisive fossae. Unfortunately, we did not have any racial information in our
sample.
Another interesting aspect is that, in this study, the width values in the dry
skulls and in the occlusal radiographs were very close, showing that the radiographic
examinations were able to reproduce the widths of the incisive fossae. But as far as
the length values were concerned, the values in the dry skulls when in comparison to
the occlusal radiographs were disparate. Chamda & Shear found the same results.
These findings can possibly be explained by the fact that in the radiographic images,
it was difficult to delimit the anterior border of the incisive fossae. In our analyzes, some
factors may have contributed to this, such as a nasal spine overlap, the presence of

23
dental alveoli in the repair processes, shallow fossae, among others. These results
have reinstated the conclusion that occlusal radiography is a recommended
examination with which to evaluate the widths of the incisive fossae, but there is a
tendency to overestimate the lengths, due to a lack of defined anterior limits. Anyway,
in general, there were no difficulties in evaluating the widths and these values are
enough to measure the diameters of the incisive fossae or of the cystic lesions. This
kept occlusal radiography as being a reliable examination in order to evaluate the
anterior maxilla region. In addition, it should also be taken into consideration that
radiographs are a low cost examination, with a low radiation exposure, having an easy
access, and being applicable in most cases.
In those borderline cases where the measurements are around 6 mm, the
CBCT procedures can contribute to a better delimitation of the limits, a better
visualization of the anatomical aspects and the relationships with other structures.
However, the CBCT procedures must be done only in those cases where the
radiographic examinations generate doubts.
As far as the presence of lesions in the sample was concerned, six dry
skulls with potential cyst lesions were found. A previous study found 2 cases in their
sample from more than 2000 dry skulls and another study found 13 cases in their
sample from 960 dry skulls. These two articles did not describe which criteria were
used to arrive at these conclusions5,11. It is important to remember that correct
diagnoses of cystic lesions should be considered, not only the dimensions in the
incisive fossae region, but also the radiographic features, together with signs and
symptoms, if they were also present. In this study, suggestive diagnoses have been
established when considering the measurements and the anatomical features. Six
skulls were considered to have potential cystic lesions. Two of them presented widths
and lengths over 1 cm. Four other skulls represented borderline cases with
measurements of around 6 mm, but they had cystic features, such as radiolucent areas
with round shapes, with well-demitted limits on the radiographic and computed
tomographic examinations. Although normal incisive fossae in occlusal radiographs
can have a very similar aspect with cystic lesions, they can also appear with longer
shapes and with osseous septa in their interiors. Furthermore, the radiopaque halo
may not be so clear1. Authors that have reviewed histopathological confirmed cases of
NDC have found mean diameters that, in the same way, have exceeded 1 cm17,18.
Swanson et al., in 1991, analyzed more than 300 cases of NDC and in 116 cases the
24
mean diameter was around 17 mm. In a few cases, the cysts had 6 mm or less, and
inside them, only one case was asymptomatic.
When considering all of the factors that are involved in the clinical and
radiological diagnoses of cystic lesions in anterior maxilla, we should consider that
radiolucent areas of up to 6 mm on the occlusal radiographs, with no signs or
symptoms, should be better characterized as enlarged incisive fossae inside of the
normal patterns. Radiolucent areas with measurements of up to 10 mm must be
periodically monitored and clinical and radiological features should be correlated.
Radiolucent areas that exceed 10 mm should be considered as being potential cystic
lesions.
References
1. Chamda RA, Shear M. Dimensions of incisive fossae on dry skulls and radiographs.
Int J Oral Surg 1980 Dec;9(6):452-7.
2. Allard RH, van der Kwast WA, van dW, I. Nasopalatine duct cyst. Review of the
literature and report of 22 cases. Int J Oral Surg 1981 Dec;10(6):447-61.
3. Francolí, J. E., Marqués, N. A., Aytés, L. B., Escoda, C. G., & Gay-escoda, P. C.
(2008). Nasopalatine duct cyst : Report of 22 cases and review of the literature,
13(7), 438–443.
4. Dedhia P, Dedhia S, Dhokar A, Desai A. Nasopalatine duct cyst. Case Rep Dent
2013;2013:869516.
5. Falci SG, Verli FD, Consolaro A, Santos CR. Morphological characterization of the
nasopalatine region in human fetuses and its association to pathologies. J Appl
Oral Sci 2013;21(3):250-5.
6. Grossmann SM, Machado VC, Xavier GM, Moura MD, Gomez RS, Aguiar MC, et
al. Demographic profile of odontogenic and selected nonodontogenic cysts in a
Brazilian population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007
Dec;104(6):e35-e41.Abrams AM, Howell FV, Bullock WK. Nasopalatine cysts. Oral
Surg Oral Med Oral Pathol 1963 Mar;16:306-32.
7. Perumal CJ. An unusually large destructive nasopalatine duct cyst: a case report.
J Maxillofac Oral Surg. 2013 Mar;12(1):100-4. doi: 10.1007/s12663-011-0201-5.
PubMed PMID: 24431822; PubMed Central PMCID: PMC3589506.
8. Sane VD, Gadre KS, Halli R, Singh V, Doshi P, Saddiwal R, et al. Role of cone-
beam computed tomography in diagnosis and management of nasopalatine duct

25
cyst. J Craniofac Surg 2014 Jan;25(1):e92-e94.
9. Nonaka CF, Henriques AC, de Matos FR, de Souza LB, Pinto LP. Nonodontogenic
cysts of the oral and maxillofacial region: demographic profile in a Brazilian
population over a 40-year period. Eur Arch Otorhinolaryngol 2011 Jun;268(6):917-
22.
10. Schiff BA, Krinstein G, Stoopack JC. An extremely large and facially distorting
nasopalatine duct cyst. Oral Surg.Oral Med.Oral Pathol. 27[5], 590-594. 1969.
11. Suter, V. G. A., & Dent, M. (2011). The Nasopalatine Duct Cyst : An Analysis of the
Relation Between Clinical Symptoms , Cyst Dimensions , and Involvement of
Neighboring Anatomical Structures Using Cone Beam Computed Tomography.
YJOMS, 69(10), 2595–2603. http://doi.org/10.1016/j.joms.2010.11.032
12. Bodin I, Isacsson G, Julin P. Cysts of the nasopalatine duct. Int J Oral Maxillofac
Surg 1986 Dec;15(6):696-706.
13. Anneroth G, Hall G, Stuge U. Nasopalatine duct cyst. Int J Oral Maxillofac Surg
1986 Oct;15(5):572-80.
14. Neville, Brad W; Damm, DD; Allen, CM; Chi, AC; (2016). Patologia Oral &
Maxilofacial (4nd ed.). Rio de Janeiro: Guanabara Koogan.
15. Suter, V. G. A., Warnakulasuriya, S., Reichart, P. A., & Bornstein, M. M. (2015).
Radiographic volume analysis as a novel tool to determine nasopalatine duct cyst
dimensions and its association with presenting symptoms and postoperative
complications, 1611–1618. http://doi.org/10.1007/s00784-014-1391-2
16. Abrams AM, Howell FV, Bullock WK. Nasopalatine cysts. Oral Surg Oral Med Oral
Pathol 1963 Mar;16:306-32.
17. Hopper-Hall, H. (1938). Cyst of developmental origin in the premaxillary region with
special reference to their diagnosis. Br. Denta. J, 65, 405–434.
18. Swanson KS, Kaugars GE, Gunsolley JC. Nasopalatine duct cyst: an analysis of
334 cases. J Oral Maxillofac Surg 1991 Mar;49(3):268-71.
19. Killey HC, Kay LW. Bening cystic lesions of the jaws. 2nd ed. Churchill Livingstone,
Edinburgh and London: 1972.
26
TABLE
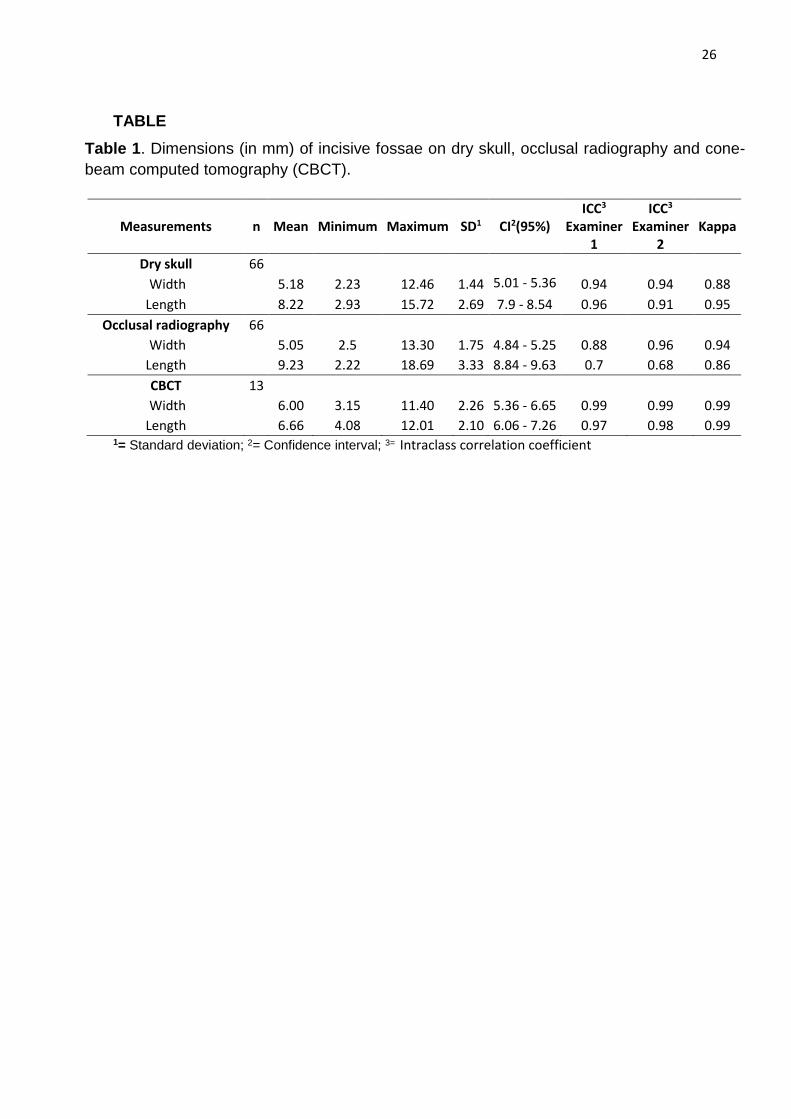
Table 1. Dimensions (in mm) of incisive fossae on dry skull, occlusal radiography and cone-
beam computed tomography (CBCT).
1= Standard deviation; 2= Confidence interval; 3= Intraclass correlation coefficient
Measurements n Mean Minimum Maximum SD1 CI2(95%) ICC3
Examiner 1
ICC3 Examiner
2 Kappa
Dry skull 66
Width 5.18 2.23 12.46 1.44 5.01 - 5.36 0.94 0.94 0.88
Length 8.22 2.93 15.72 2.69 7.9 - 8.54 0.96 0.91 0.95
Occlusal radiography 66
Width 5.05 2.5 13.30 1.75 4.84 - 5.25 0.88 0.96 0.94
Length 9.23 2.22 18.69 3.33 8.84 - 9.63 0.7 0.68 0.86
CBCT 13
Width 6.00 3.15 11.40 2.26 5.36 - 6.65 0.99 0.99 0.99
Length 6.66 4.08 12.01 2.10 6.06 - 7.26 0.97 0.98 0.99

27
FIGURES
Figure 1. The same dry skull observed by axial view (A), its occlusal radiography (B) and cone-
beam computed tomography by axial section (C). This dry skull presented width of 11 mm and
length of 13 mm in measurements performed on the dry skull.

28
3. CONCLUSÃO
1 – As dimensões da fossa incisiva aferidas nos crânios secos
demonstraram média de 5,18 mm de largura e 8,22 mm de comprimento. Já na
radiografia oclusal de maxila, a fossa incisiva demonstrou largura média de 5,05 mm
e comprimento médio de 9,23 mm. As medições realizadas nas imagens da
tomografia computadorizada demonstraram média de largura de 6,00 mm e de
comprimento de 6,66 mm. Em todos os métodos utilizados para aferir as dimensões
da fossa incisiva, tanto nos crânios secos quanto nos exames de imagem, a maioria
das fossas demonstrou medidas de largura e comprimento menores que 6 mm.
2 - A radiografia oclusal mostrou-se ser um exame confiável para a
determinação da largura (medida linear látero-lateral) da fossa incisiva, porém
apresentou limitações para a determinação do comprimento (medida linear ântero-
posterior).
3 - Em casos em que a largura da fossa incisiva, na radiografia oclusal,
excede 6 mm, o exame de TCCB pode ser útil para melhor avaliação das
características anatômicas da fossa, além de melhor determinação da medida do
comprimento.
29
REFERÊNCIAS*
Abrams AM, Howell FV, Bullock WK. Nasopalatine cysts. Oral Surg Oral Med Oral
Pathol 1963 Mar;16:306-32.
Allard RH, van der Kwast WA, van dW, I. Nasopalatine duct cyst. Review of the
literature and report of 22 cases. Int J Oral Surg 1981 Dec;10(6):447-61.
Anneroth G, Hall G, Stuge U. Nasopalatine duct cyst. Int J Oral Maxillofac Surg 1986
Oct;15(5):572-80.
Bodin I, Isacsson G, Julin P. Cysts of the nasopalatine duct. Int J Oral Maxillofac Surg
1986 Dec;15(6):696-706.
Cecchetti F, Giada M, Marco C, Germano F, Arcuri C, Ennio B. Nasopalatine duct cyst:
report of 52 cases in a retrospective epidemiological study. Journal of Surgery 1[2],
14-17. 2013.
Chamda RA, Shear M. Dimensions of incisive fossae on dry skulls and radiographs.
Int J Oral Surg 1980 Dec;9(6):452-7.
Dedhia P, Dedhia S, Dhokar A, Desai A. Nasopalatine duct cyst. Case Rep Dent
2013;2013:869516.
Falci SG, Verli FD, Consolaro A, Santos CR. Morphological characterization of the
nasopalatine region in human fetuses and its association to pathologies. J Appl Oral
Sci 2013;21(3):250-5.
Grossmann SM, Machado VC, Xavier GM, Moura MD, Gomez RS, Aguiar MC, et al.
Demographic profile of odontogenic and selected nonodontogenic cysts in a Brazilian
population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007 Dec;104(6):e35-
e41.
Hertzanu Y, Cohen M, Mendelsohn DB. Nasopalatine duct cyst. Clin Radiol 1985
Mar;36(2):153-8.
*De acordo com as normas da UNICAMP/FOP, baseadas na padronização do International Committee of Medical Journal Editors
– Vancouver Group. Abreviatura dos periódicos em conformidade com o PubMed.

30
Killey HC, Kay LW. Bening cystic lesions of the jaws. 2nd ed. Churchill Livingstone,
Edinburgh and London: 1972.
Moore K L., PERSAUD T.V.N. Embriologia Clínica. 9ª Edição. Elsevier, 2012. 560p.
Moss HD, Hellstein JW, Johnson JD. Endodontic considerations of the nasopalatine
duct region. J Endod 2000 Feb;26(2):107-10.
Neville, Brad W; Damm, DD; Allen, CM; Chi, AC; (2016). Patologia Oral & Maxilofacial
(4nd ed.). Rio de Janeiro: Guanabara Koogan.
Nonaka CF, Henriques AC, de Matos FR, de Souza LB, Pinto LP. Nonodontogenic
cysts of the oral and maxillofacial region: demographic profile in a Brazilian population
over a 40-year period. Eur Arch Otorhinolaryngol 2011 Jun;268(6):917-22.
Nortje CJ, Farman AG. Nasopalatine duct cyst. An aggressive condition in adolescent
Negroes from South Africa? Int J Oral Surg 1978 Apr;7(2):65-72.
Roper-Hall HT. Cyst of developmental origin in the premaxillary region with special
reference to their diagnosis. Br.Dent.J. 65, 405-434. 1938.
Sane VD, Gadre KS, Halli R, Singh V, Doshi P, Saddiwal R, et al. Role of cone-beam
computed tomography in diagnosis and management of nasopalatine duct cyst. J
Craniofac Surg 2014 Jan;25(1):e92-e94.
Saunders LA, Wisniewski H, Soumerai S. Extensive incisive canal cyst. Report of a
case. Oral Surg Oral Med Oral Pathol 1968 Sep;26(3):284-90.
Schiff BA, Krinstein G, Stoopack JC. An extremely large and facially distorting
nasopalatine duct cyst. Oral Surg.Oral Med.Oral Pathol. 27[5], 590-594. 1969.
Shear M, Speight P. Cysts of the oral and maxillofacial region, 4th edn. Blackwell
Publishing Ltd., Oxford, pp 108-118. 2007.
Srivastava S, Misra N, Agarwal R, Pandey P. Nasopalatine canal cyst: often missed.
BMJ Case Rep 2013;2013.
Suter VG, Sendi P, Reichart PA, Bornstein MM. The nasopalatine duct cyst: an
analysis of the relation between clinical symptoms, cyst dimensions, and involvement
of neighboring anatomical structures using cone beam computed tomography. J Oral
Maxillofac Surg 2011 Oct;69(10):2595-603.
31
Swanson KS, Kaugars GE, Gunsolley JC. Nasopalatine duct cyst: an analysis of 334
cases. J Oral Maxillofac Surg 1991 Mar;49(3):268-71.
Tanaka S, Iida S, Murakami S, Kishino M, Yamada C, Okura M. Extensive
nasopalatine duct cyst causing nasolabial protrusion. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod 2008 Oct;106(4):e46-e50.
Tsuneki M, Maruyama S, Yamazaki M, Abe T, Adeola HA, Cheng J, et al. Inflammatory
histopathogenesis of nasopalatine duct cyst: a clinicopathological study of 41 cases.
Oral Dis 2013 May;19(4):415-24.
32
APÊNDICE 1 - Figuras complementares
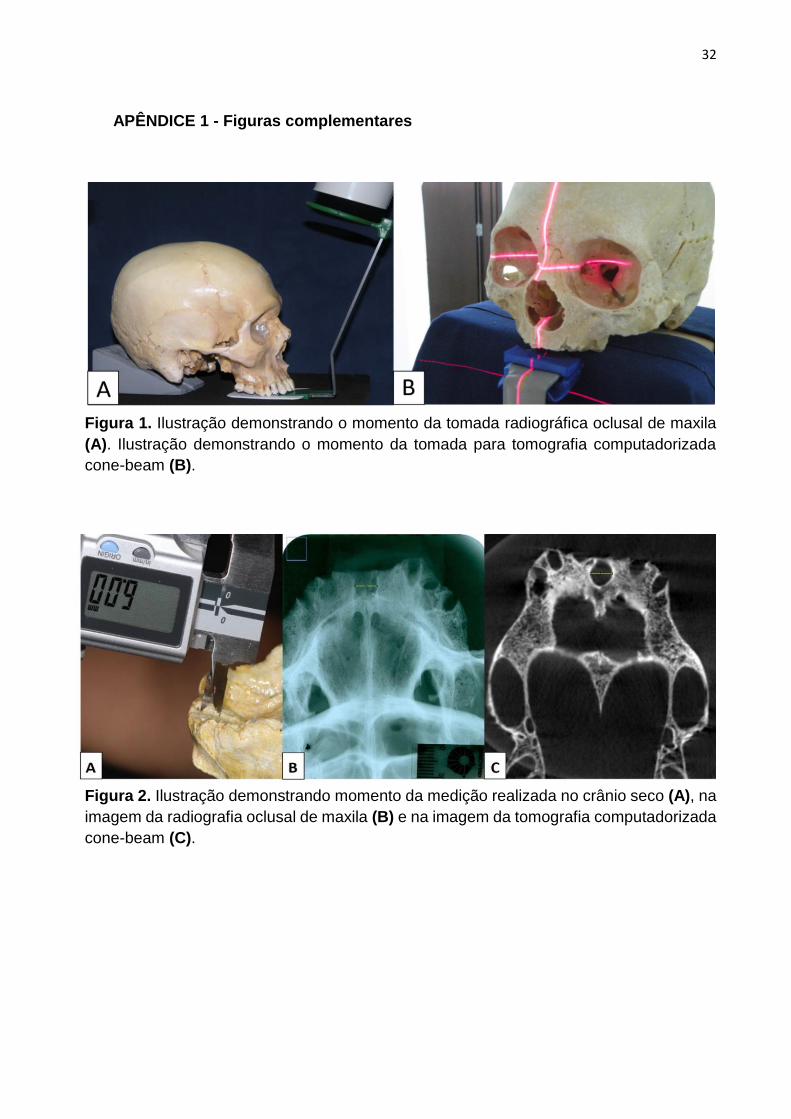
Figura 1. Ilustração demonstrando o momento da tomada radiográfica oclusal de maxila
(A). Ilustração demonstrando o momento da tomada para tomografia computadorizada
cone-beam (B).
Figura 2. Ilustração demonstrando momento da medição realizada no crânio seco (A), na
imagem da radiografia oclusal de maxila (B) e na imagem da tomografia computadorizada
cone-beam (C).
33
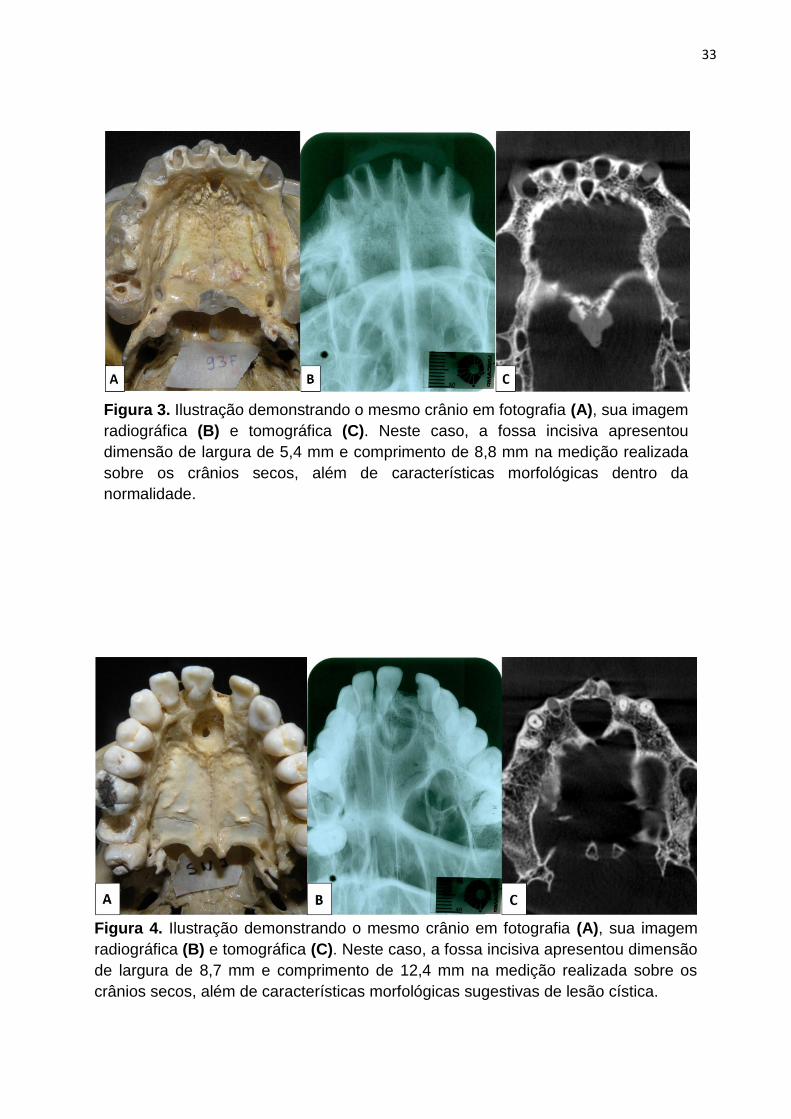
Figura 3. Ilustração demonstrando o mesmo crânio em fotografia (A), sua imagem
radiográfica (B) e tomográfica (C). Neste caso, a fossa incisiva apresentou
dimensão de largura de 5,4 mm e comprimento de 8,8 mm na medição realizada
sobre os crânios secos, além de características morfológicas dentro da
normalidade.
Figura 4. Ilustração demonstrando o mesmo crânio em fotografia (A), sua imagem
radiográfica (B) e tomográfica (C). Neste caso, a fossa incisiva apresentou dimensão
de largura de 8,7 mm e comprimento de 12,4 mm na medição realizada sobre os
crânios secos, além de características morfológicas sugestivas de lesão cística.

34
ANEXO 1 - Certificado do Comitê de Ética em Pesquisa