patients' expectancies and hospital outcome
TRANSCRIPT

PATIENTS’ EXPECTANCIES AND HOSPITAL OUTCOME’ PAUL J. MARTIN^ ARTHUR L. STERNE
JOSEPH E. MOORE CAROLE J. LINDSEY
Larue D. Carter Memorial Hospital, Indianapolis, Indiana
Although it is widely held that patients’ expectancies for therapeutic gain are related causally to treatment outcome, a recent review of expectancy research found scant evidence for the hypothesized expectancy-outcome relationship. Supportive findings were reported only in studies with serious methodological weaknesses. This study tested the relationship between the prognostic expectancies of hospitalized schizophrenic patients and several objective measures of hospital outcome. I t also tested the hy othesis that expectancies may bear primarily a predictive, not causal, refationship to outcome. Multiple regression analyses found patients’ expectancies to be correlated significantly with 8 of 15 measures of posthospital adjustment and with 14 of 15 measures of prehos ital adjustment. The findings supported the expectancy-outcome relationstip and also were consistent with a pre- dictive interpretation of patients’ expectancies.
After medical research determined that pharmacologically inert agents could have a therapeutic impact (placebo effect), a similar phenomenon was hypothesized in psychiatric treatments. It was suggested that patients’ expectancies for therapeu- tic gain may be associated with success in psychotherapy. Some researchers (Bednar, 1970; Frank, Gliedman, Imber, Stone, & Nash, 1959, for example) took strong positions contending that patient expectancies for relief may be one of a limited number of primary determinants of treatment success.
Despite these conclusions, the results of empirical studies of the link between patients’ expectancies and improvement in treatment (psychotherapy primarily) have been disheartening. In a recent review of published expectancy research Wilkins (1973) found very little convincing evidence of a significant expectancy- outcome relationship. The studies that reported positive findings were seriously flawed by subjectivity of outcome measures, possible confounds with therapists’ expectancies for gain, and other methodological weaknesses. When care was taken in other studies to avoid these problems, the significant expectancy-outcome relationship evaporated. The reviewer concluded that critical studies that success- fully related patients’ expectancies to objective measures of treatment outcome were yet to be reported. In fact, the overall findings were sufficiently discouraging to cause the reviewer to align himself with Cartwright and Cartwright’s (1958) position that “expectancy of therapeutic gain” should be abandoned as an ex- planatory concept.
The study reported here approached the expectancy-outcome relationship in a manner quite different from most reported to date. It employed: (1) multiple measures of expectancy as opposed t o the unitary measures used most commonly; (2) multivariate analytic techniques as opposed to the univariate analyses of virtually all previous studies; (3) multiple objective measures of treatment outcome as opposed to the limited, often unitary and subjective, measures of outcome utilized in previous research; and (4) a large, diagnostically homogeneous sample of seriously disturbed hospitalized patients in contrast with the relatively small sample of heterogeneous, minimally disturbed outpatients commonly used in expectancy
‘This research was conducted as part of an ongoing follow-up program at Carter Hospital and waa supported in part by grants from the Association for the Advancement of Mental Health R e search and Education, Inc., Indiana OliS, and by research grant No. M H 2341702 awarded by the National Institute of Mental Healti, D.H.E.W. The authors wish to express their gratitude to Ms. Nancy Acree and the Follow-Up Research Group for invaluable assistance in the data collection phases of this study. Computer services provided by t,he Indiana University Com uting facilities.
*Requests for reprints should be sent to Paul J. Martin, Follow-Up Project, farue D. Carter Memorial Hospital, 1315 West 10th Street, Indianapolis, Indiana 46202.
254

Patients’ Expectancies and Hospital Outcome 255
research. It also adopted and tested one aspect of a less cumbersome interpretation of the expectancy-outcome relationship. Specifically, patients’ expectancies pri- marily may predict rather than facilitate or cause improvement in treatment. On what basis are expectancies formed? Purely hope, determination to recover, or other motivational constructs? Probably not. It is more likely that they derive largely from the patients’ knowledge of their usual adjustment, their perceptions of their maladjustment or symptoms prior to treatment, and the objective in- formation given them by physicians and other professionals on the improvements that they can anticipate realistically as a result of treatment. Thus, their ex- pectancies should have specifiable, measurable pretreatment determinants that relate to these considerations and allow the patients to make generally accurate (but imperfect) predictions with regard to therapeutic success.
The first predicted that patients’ expectancies would be correlated significantly with objective measures of their adjustment after hospital treatment ; the second predicted a significant correlation of expectan- cies and pretreatment adjustment at hospital admission.
Two hypotheses were tested.
METHOD Setting
The study was conducted at a 220-bed intensive treatment psychiatric training and research hospital adjacent to a large, midwestern university medical center complex. The hospital admits acutely disturbed patients, primarily from the middle social classes, who are grappling for the first time with serious psychiatric dis- order that requires hospitalization or who are readmissions who have been hospital- ized previously at this facility. Patients are admitted on physician’s referral only. The treatments employed by the hospital are consistent with those widely accepted in current clinical psychiatric practice. The average length of stay for adult patients is approximately 80 to 90 days. Subjects
The Ss were 84 acutely disturbed schizophrenic patients who were admitted for treatment in 1972. All participated on a voluntary basis and were unaware of the nature of the study and the hypotheses to be tested. The Ss were generally representative of the hospital’s usual patient population. Of the 84 Ss, 35 were male and 49 female. Eighty-five percent were voluntary admissions ; the remainder were committed temporarily. The average age for the sample was approximately 29 years. Thirty-seven of the Ss were single, 28 married, and 19 divorced or separa- ted. Approximately 85% were Caucasian. The majority had a high school education. Expectancy Measures
Patients’ prognostic expectancies were measured on the day of the patients’ admission to the hospital, usually within the first hours after they had entered the hospital admission ward. The expectancies were measured as soon as possible after admission in order to minimize the potential influence of contact with staff and other patients. None of the patients had met their therapists at the time of measurement of expectancies. Patients’ expectancies were measured with the Patient Prognostic Expectancy Inventory (PPEI) , a 15-item inventory that asked the patients to report their anticipations re improvement in a variety of areas. The inventory items reflected clinical symptoms and behavioral abnormalities commonly observed in seriously disturbed, but not necessarily schizophrenic, patients. For each item Ss used a 4-point response scale (“none’’ to “great’’) to report their expectancies for improvement through hospital treatment. Scores on the 15 PPEI items were taken as a reflection of Ss’ expectancies for improvement. Adjustment Measures
Patients’ prehospital and posthospital adjustment was measured by test and diagnostic interview data. During the week of admission and again during the
Journal of Clinical Psychology, January, 1977, Vol. 33, N o . 1.
week that preceeded discharge the Ss were given the Minnesota Multiphasic Personality Inventory (MMPI) and a diagnostic interview by two independent clinicians who were unfamiliar with the Xs, the presenting symptoms, and treat- ment regimes during hospital stay. After each interview the Ss were rated on the Brief Psychiatric Rating Scale (BPRS) (Overall & Gorham, 1962). The BPRS is an 18-item scale used by an interviewer to rate patient psychopathology in several different content areas. It yields a total score that can range from 18 to 126. Differences between interviewers in BPRS total scores were resolved by averaging.
Fifteen measures of adjustment were derived from the MMPI and BPRS data. Of the 15, 12 measured adjustment a t specific levels. These were T scores on all MMPI scales except SI. The remaining measures reflected adjustment at global levels. These were the number of significantly elevated MMPI scales (T score of 70 or more), the number of MMPI Critical Items endorsed, and total scores on the BPRS. Statistical Analyses
Multiple regression analyses that utilized the CDC 6600 version of the Xtatisti- cal Package for the Social Sciences (SPSS) , version 6.0, subroutine regression, were used to test the association of Ss’ expectancy scores with scores on the measures of pre- and posthospital adjustment.
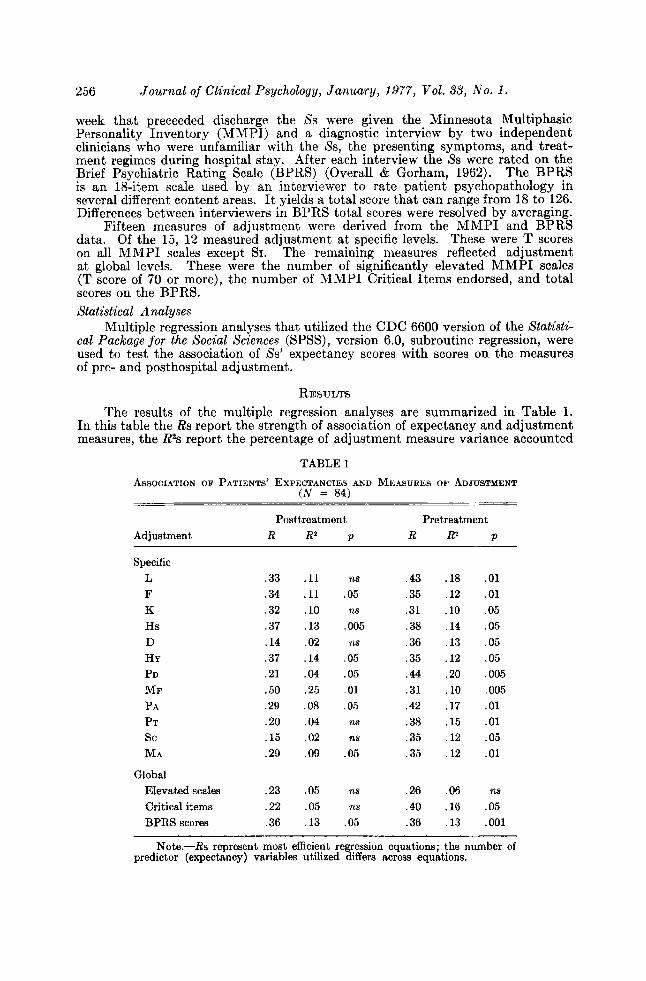
RESULTS The results of the multiple regression analyses are summarized in Table 1.
In this table the Rs report the strength of association of expectancy and adjustment measures, the R2s report the percentage of adjustment measure variance accounted
TABLE 1
( N = 84) ASSOCIATION OF PATIENTS’ EXPECTANCIES AND MEASURES OF ADJUSTMENT
Postt,reatment Pretreatment Adjustment R R2 p R R? p
Specific L F K Hs D HY
MF PD
PA PT sc MA
Global Elevated scales Critical items BPRS scores
.33
.34
.32
.37
.14
.37
.21
.50
.29
.20
.15
.29
.23
.22
.36
. l l
. l l
.10
.13
.02
.14
.04
.25
.08
.04
.02
.09
.05
.05
.13
ns .43 .05 .35 ns .31
,005 .38 ns .36
.05 .35
.05 .44
. 01 .31
.05 .42 125 .38 ns .35
.05 .35
ns .26 ns .40
.05 .36
.18
.12
.10
.14
.13
.12
.20
.10
.17
.15
.12
.12
.06
.16
.13
. O l
. O l
.05
.05
.05
.05 ,005 ,005 . O l . O l .05 . O l
125
.05
. O O l
Note.-& represent most efficient regression equations; the number of predictor (expectancy) variables utilized differs across equations.

Patients’ Expectancies and Hospital Outcome 257
for by the expectancy measures, and the ps reflect the overall goodness of fit of the regression equations. The first part of the table deals with the link between patients’ expectancies and posthospital adjustment. It can be seen that the expectancy measures were associated significantly with 8 of 15 outcome measures. The Rs ranged from .15 to .50 and averaged approximately .29. The second part of the table is concerned with the association of patients’ expectancies and prehospital adjustment. The findings show that the patients’ expectancies were correlated significantly with all but one of the measures of prehospital adjustment. The Rs ranged from .26 to .44 and averaged approximately .36.
DISCUSSION The analyses found significant links between patients’ expectancies and ob-
jective measures of posthospital adjustment that were independent of patients’ and therapists’ direct estimates of recovery. These findings provide confirmation for the hypothesized association of expectancies and treatment outcome and help fill the data gap noted by Wilkins (1973).
The findings differ from those previously reported; the differences are believed attributable to the methodological considerations noted earlier in this report, i. e., multiple expectancy measures, multivariate analytic techniques, multiple measures of outcome, and diagnostically homogeneous Ss. In light of the extensively documented complexity of psychiatric disturbances and treatments (particularly psychotherapy; see Luborsky et al., 1971, for example), and the equally complex issues involved in the assessment of treatment outcome it seems paradoxical that almost all researchers have employed a univariate approach to the expectancy- outcome relationship. There seems to be little or no a-priori reason to believe that expectancies would be significantly less complex than the constructs to which they reputedly are linked, and the highly consistent use of a single measure of expectancy and univariate analyses (usually product-moment correlation or chi square) in previous studies is something of a puzzlement. The basic nature of the issues and constructs involved in the hypothesized expectancy-outcome relationship (Cart- Wright & Cartwright, 1958; Frank, 1968) seems to demand use of multivariate methodology, and the findings of the present study vis-a-vis univariate approaches substantiate the complex nature of the relationship sought.
It is probable that the diagnostic homogeneity and severity of disturbance of the patient sample also played a substantial role in the findings reported here. In most expectancy studies the Ss were not selected on the basis of diagnoses and seemingly were heterogeneous. Also, the Ss were drawn from outpatient populations in most cases and thus were likely to have displayed minimal pretreatment dis- turbance, It is possible that these factors had the combined effects of maximizing inter-S variability on measures of outcome while they minimized the amount of improvement that could be realized (a “floor effect” that resulted from minimal pretreatment disturbance). Both factors would militate against a valid assessment of the relationship between expectancy and treatment outcome.
The results also found significant links between patients’ expectancies and 14 of 15 measures of pretreatment adjustment. These findings suggest that the patients closely considered their pretreatment pat,hology in reporting their ex- pectancies re improvement through hospitalization. It is possible that pretreat- ment maladjustment was a determinant of the reported expectancies, and the findings thus are consistent with an interpretation of patients’ expectancies as predictions based on specifiable determinants. It should be noted, however, that the findings do not necessarily argue against causal interpretations. It might be argued that patients were aware of their problem areas, were highly motivated to work on these in treatment, and their expectancies reflected their insight and motivation, which could help determine or “cause” improvement. This issue cannot be resolved on the basis of the data reported here and awaits further research.

258 Journal of Clinical Psychology, January, 1977, VoE. 33, No. 1.
REFERENCES BEDNAR, R. L. Persuasibility and the power of belief. Personnel and Guidance Journal, 1970, 48,
647-652. CARTWRIGHT, D. S., & CARTWRIGHT, R. D. Journal
of Counseling Psychology, 1958, 6, 174-177. FRANK, J. D. The influence of patients’ and therapists’ expectations on the outcome of psycho-
therapy. British Journal of Medical Psychology, 1968, 41, 349-356. FRANK, J. D., GLIEDMAN, L. H., IMBER, S. D., STONE, A. R., & NASH E. H. Patients’ expectancies
and relearning &s factors determining improvement in psychotherapy. American Journal of
OVERALL, J. E., & GORHAM, D. R. The Brief Psychiatric Rating Scale. Psychological Reports,
WILKINS, W. Expectancy of therapeutic gain: an empirical and conceptual critique. Journal of
Faith and improvement in psychotherapy.
Psychiatry, 1959, 116, 961-968.
1962, 10, 799-812.
Consulting and Clinical Psychology, 1973, 40, 69-77.
THE DELAYED IMPACT OF GROUP THERAPISTS’ INTERVENTIONS MICHAEL P. NICHOLS’
Emory University
The direct and delayed impact of therapist interventions on 21 clients in three outpatient therapy groups was examined. Sessions one and five of each group were taped with every therapist intervention analyzed according to the Group Therapist Interventions Scale and every client utterance rated on the Experiencing Scale and categorized by the Group Immediacy Scale. It was hypothesized that therapists would have a delayed rather than direct in- fluence on group process measures. When pairs of therapist-patient state- ments were examined, little immediate impact was evident. However, a pro- found delayed impact of group leaders was inferred from the finding that as therapist interventions became more forceful over the first five sessions, pa- tients’ level and immediacy of experiencing became more intense.
One of the least-studied aspects of group therapy is the impact of leader inter- ventions on subsequent interactions in the group. This is unfortunate because questions that deal with the influence of technique are of particular interest to group therapists. At present the bulk of research in this field is either too complex to answer practical questions or relates to variables more relevant to planning than to conducting groups (Bednar & Lawlis, 1971). Thus there are numerous studies of desirable patient characteristics and studies that compare overall treat- ment strategies, but few that examine the effectiveness of specific techniques for leading groups. In what is perhaps the best- known study of group treatment, Lieberman, Yalom, and Miles (1970) examined leadership styles in 17 different encounter groups. Their findings underscored the profound influence of leaders’ techniques on the outcome of group treatment. However, their data relate to the differential effectiveness of broad leadership styles rather than to the discrete effects of specific leader behaviors.
One difficulty in determining the impact of specific techniques is that the therapist’s influence on a group is more indirect than is the case in individual treatment (Yalom, 1970). Not only are there more participants in a group, but the possibilities for therapeutic influence are also fundamentally different. In individual treatment, interventions are likely to exert a direct and immediate impact on the patient. Although the effect may be cumulative, it is reflected in the patient’s direct responses to the therapist. This is not so in group therapy, where the most meaningful therapeutic opportunities evolve from social interaction among group members. Hence, the group leader’s most significant contributions
University, Atlanta, Georgia 30322. 1Requests for reprints should be sent to Michael P. Nichols, Psychology Department, Emory