patient safety - northern lincolnshire and goole … be removed from the agenda. e) ic annual report...
TRANSCRIPT

NLG(13)430
DATE 26 November 2013
REPORT FOR Trust Board of Directors – Part A
REPORT FROM Infection Prevention & Control Committee
CONTACT OFFICER Professor Carrock Sewell
SUBJECT Minutes of the Committee meeting – 18 November 2013
BACKGROUND DOCUMENT (IF ANY) None
REPORT PREVIOUSLY CONSIDERED BY & DATE(S) None
EXECUTIVE COMMENT (INCLUDING KEY ISSUES OF NOTE OR, WHERE RELEVANT, CONCERN AND / OR NED CHALLENGE THAT THE BOARD NEED TO BE MADE AWARE OF)
None
HAVE THE STAFF SIDE BEEN CONSULTED ON THE PROPOSALS?
N/A
HAVE THE RELEVANT SERVICE USERS/CARERS BEEN CONSULTED ON THE PROPOSALS?
N/A
ARE THERE ANY FINANCIAL CONSEQUENCES ARISING FROM THE RECOMMENDATIONS?
N/A
IF YES, HAVE THESE BEEN AGREED WITH THE RELEVANT BUDGET HOLDER AND DIRECTOR OF FINANCE, AND HAVE ANY FUNDING ISSUES BEEN RESOLVED?
N/A
ARE THERE ANY LEGAL IMPLICATIONS ARISING FROM THIS PAPER THAT THE BOARD NEED TO BE MADE AWARE OF?
N/A
WHERE RELEVANT, HAS PROPER CONSIDERATION BEEN GIVEN TO THE NHS CONSTITUTION IN ANY DECISIONS OR ACTIONS PROPOSED?
WHERE RELEVANT, HAS PROPER CONSIDERATION BEEN GIVEN TO SUSTAINABILITY IMPLICATIONS (QUALITY & FINANCIAL) & CLIMATE CHANGE?
THE PROPOSAL OR ARRANGEMENTS OUTLINED IN THIS PAPER SUPPORT THE ACHIEVEMENT OF THE TRUST OBJECTIVE(S) AND COMPLIANCE WITH THE REGULATORY STANDARDS LISTED
N/A
N/A
N/A
ACTION REQUIRED BY THE BOARD
The Board is asked to note the Minutes.

INFECTION PREVENTION & CONTROL COMMITTEE
Minutes of the Infection Prevention and Control Committee held on 18 November 2013 at 12.00 noon – 2.00 pm in the West Arch Boardroom, DPOW with vtc to Modular Meeting
Room, SGH
PRESENT: Mr Neil Gammon Non-Executive Director (Chair) Dr Peter Cowling Consultant Microbiologist Viv Duncanson Senior Nurse, Infection Control/Assistant DIPC Dr Karen Dunderdale Chief Nurse Kirsty Edmondson-Jones Deputy Director of Facilities Karen Jackson Chief Executive Greta Johnson Community Services Infection Control Nurse Andy Karvot Consultant Antimicrobial Pharmacist Professor Carrock Sewell Acting Medical Director Linda Taylor Public Health England Dr Anthony Vicca Consultant Microbiologist Karen Wilson Assistant Director of Operations, Central Operations Group 1. Apologies for Absence
Apologies for absence were received from: Karen Griffiths (Deputy Director, Diagnostics & Therapeutics) Dr Jim Whittingham (Chairman) Wendy Booth (Director of Clinical and Quality Assurance) Catherine Wylie (Quality Manager, NLCCG)
2. Minutes of the Previous Meeting – 16 September 2013
The Committee agreed that point 7 of the previous minutes should read:- 1) Annual self-assessment 2) Quarterly joint Facilities/IC Report 3) Annual derogation of Risk Report Viv Duncanson highlighted a typing error at point 3(g), ICNBs should in fact read IPCNs. The Committee ratified the remainder of the minutes.
Action: Leanne Glasson to amend the minutes of 16 September 2013 as above
3. Matters Arising and Outstanding Actions
a) Post-op wound infection update (Minute 3(a) refers)

Dr Peter Cowling informed the Committee that due to difficulties in respect of arranging the A3 Orthopaedic Wound Infection meeting, he was unable to attend the meeting and the meeting went ahead without him on Monday, 04 November. Dr Cowling explained that Professor Carrock Sewell chaired the A3 meeting and Dr Cowling therefore handed this matter over to Professor Sewell. Professor Sewell explained that there was some initial confusion with the title of the A3 meeting, as the meeting was in respect of joint infections, however Professor Sewell went on to inform the Committee that it was agreed, at the A3 meeting, that when any major joint infections occur they should be subject to a Root Cause Analysis (“RCA”). Professor Sewell explained that Viv Duncanson was putting together an RCA template. Viv confirmed that she had drafted the RCA template and will be sending it out for comments this week.
Action: Viv Duncanson to produce RCA template
b) HSDU incident update (Minute 3(b) refers)
As Wendy Booth had given her apologies for the Committee meeting, Viv Duncanson explained that she was aware that following the HSDU visit it was decided that a follow-up inspection would take place in 6 months. Viv explained that approximately 3 months had now passed since the visit therefore the follow-up inspection would be due to go ahead by March 14. Viv informed the Committee that the purpose of the follow-up inspection was to ensure that certain processes were still being following and that progress was continuing to be made/sustained. The Committee agreed that they were happy for this item to be brought back to the meeting on 17 March 2014, after the follow-up inspection had taken place, with the specific aim of finalising this issue at that time.
Action: Wendy Booth to ensure that follow-up inspection is carried out by Mar 14 and report to the Committee in March 2014
c) Progress report E-prescribing (Minute 3(d) refers)
Andy Karvot, in the absence of Karen Griffiths informed the Committee that e-prescribing had only been rolled out in DPOW Ward B7 and DPOW Theatres as there were issues with the interface, in particular that it was not intuitive. Andy explained that a team had been trying to improve the issues however he was unsure of the present position. Neil Gammon explained that he thought the initial issues with the system were the lack of resources available to improve it. Karen Jackson informed the Committee that she had taken the issue of resources forward with Karen Griffiths and they had agreed to pilot the system on two other wards at SGH to determine if there were problems relating to the usage of the system. Karen explained that they were hoping to get the system on the two other SGH wards by the end of November and therefore suggested that the Committee be updated on this item in January 2014. The Committee agreed to keep this item on matters arising for the meeting in January 2014.
Action: Karen Griffiths to pilot system on two SGH wards for field testing and update the Committee in January 2014
d) Water Action Plan (Minute 3(e) refers)
Kirsty Edmondson-Jones informed the Committee that this item was purely for information only as it had been brought to the previous Committee meeting and was subsequently taken back to the Water Safety Group meeting.

The Committee confirmed they had no further comments on this item and agreed that it could be removed from the agenda. e) IC Annual Report (Minute 3(g) refers)
Neil Gammon informed the Committee that the Infection Control Annual Report had been received by the Trust Board in September and therefore confirmed that this item could be removed from the ICC agenda.
f) Bank Staff Training (Minute 3(h) refers) Viv Duncanson informed the Committee that as there had been problems with the bank staff training this had been put on the agenda for the Workforce Review Group meeting. Karen Dunderdale explained that she was attending the next Workforce Review Group meeting and would therefore raise this issue. The Committee agreed that this specific item could be removed from the agenda as it would be reported within future IC reports.
g) Segregation & Intra-Hospital Transfer of Patients Policy (Minute 5.5.1 refers) Viv Duncanson informed the Committee that following a further discussion in respect of this policy, the Segregation & intra-hospital transfer of patients Policy could be taken off the infection control web site as it had been incorporated into the overall Bed Management Policy. The Committee agreed this item could be removed from the agenda.
h) Register of Derogations (Minute 5.5.3 refers) It had not been decided whether all approved derogations from Trust IC policy were to be added to the risk register only or whether a separate register of derogations was required. The Committee agreed that this point needed clarifying with Wendy Booth. Viv Duncanson confirmed that she would report the outcome back to the Committee at the next meeting. Action: Viv Duncanson to clarify with Wendy Booth i) Antimicrobial Update (Minute 8 and 8.1 refers) Professor Carrock Sewell informed the Committee that Lisa and a team from Dashboard were working on the system in order to include a feature that would flag up any issues in terms of prescribing, including details of who prescribed what, within 12 hours from the creation of the prescription. Professor Sewell explained that Andy Karvot was currently looking at a timetable (potentially mid-December) of when he could go and look at the wards in order that this could be up and running as soon as possible. Andy Karvot confirmed that he aimed to pilot the AMU by 25 November and allow a fortnight to analyse how it works and if it meets the necessary standards. Dr Peter Cowling explained that he felt it was important that Pharmacy were made aware that Anaesthetists often write prescription details on their own drug charts as opposed to the notes. Professor Sewell explained that the team were working on a drop-down menu in order that the correct department could be chosen. In respect of Nurses and Good Antimicrobial Stewardship, Viv Duncanson explained that this was on the next Nursing Midwifery Advice Forum (“NMAF”) meeting agenda. Andy Karvot informed the Committee that the paper from Public Health England details everything the Trust and prescribers should be doing in order to promote good antimicrobial stewardship. Andy also explained that the paper provides a framework to identify if prescribers are fit for purpose. The Committee agreed that this should be taken to the Antimicrobial Steering Group (“AMG”) meeting and brought back to the Committee once AMG had had the opportunity to review this and provide advice as required. Andy Karvot explained that at the last Committee meeting he produced a paper requesting the assistance of WebV for antibiotic audit systems (minute 4.1 refers), however the Committee agreed he needed to look at the resources required for this with

Karen Griffiths. Andy explained that he had looked into this with Karen Griffiths and WebV and it had been confirmed that it may only involve one day’s work therefore this was moving forward. Professor Sewell informed the Committee that he felt the Rapid Response Audits were going to be taken forward before the WebV developments as the WebV team were extremely pressured with a high workload. The Committee agreed that the Rapid Response Audit would be added to items for discussion at the next Committee meeting in January 14.
4. Items for Discussion 4.1 Trust Delivery Plan: Healthcare-Associated Infections 2013/14: 6-monthly
Progress Report
The progress report had been circulated prior to the meeting. Viv Duncanson highlighted a number of issues.
Page 6 – Viv confirmed the deep clean schedule was working well and a lot of progress had been made. Outstanding areas are now easily identifiable. Page 3 – Concerning the hygiene code, Viv confirmed that the Waste Disposal Policy had been ratified and so this item was now complete. There were just a few outstanding DPOW wards with no hand hygiene sinks in the patient bays. . Viv explained that the need for hand hygiene bays was detailed on every refurbishment plan as water infrastructure would need to be relayed to each bay. Page 7 - In respect of Viral Gastroenteritis, Viv explained that the Trust had enrolled on a National research project in order to look at identifying the source of each outbreak and to monitor the effectiveness of bay and ward closures. Page 14 – Viv gave an overview of the recent project that had been carried out by the IPCN’s which had looked at assessing patients who had been in hospital for 21 days for risk factors for acquiring an infection The final report had been shared with the Chief Nurse. Viv explained that an electronic nursing document had been produced with mandatory fields in order to ensure matters are escalated correctly. The Committee agreed that they would like to see the report; the report is attached to these minutes at Appendix A. Page 15 – Viv updated the Committee on the mandatory training assessment module. l. Viv confirmed that the assessment incorporated all of the key mandatory elements necessary for infection control awareness and that the assessment only took 7-8 minutes to complete. If staff could achieve over 85% they would not need to attend mandatory training for that year. Viv explained that there was an issue with the system linking electronically to OLM however resolution was imminent. Viv agreed to keep the Committee updated on any progress made in respect of this. Kirsty Edmondson-Jones explained that some of the amber items on the report will always be ongoing items and she therefore felt that they should be changed to green; the Committee agreed with this point.
Action: Viv to change relevant ongoing amber items to green and update IPC Committee on training progress.
4.2 Infection Prevention & Control Annual Programme 2013/14: 6-monthly Progress
Report
The progress report had been circulated to the Committee members prior to the meeting. Viv highlighted a number of issues to the Committee:-
Page 6 – Viv explained that this could be updated in respect of the Orthopaedic Wound Infection issue as per minute 3(a) above. Page 5 – The Pseudomonas in taps section could be changed to green.
Page 8 – The Mandatory Training section could be changed to amber as slight progress had been made. Page 11 – In respect of implementing an invasive device service, 2 clinical nurse specialists were recruited who were now competent in inserting PICC lines, It was noted that there had been 2 occasions where a PICC had been placed in patients that had prevented hospital admissions . There were still some minor actions outstanding so this item was to remain amber. Page 12 – The section in respect of augmented care could be changed to green as this had been passed to the Water Safety Group.
5. Standing Items 5.1 MRSA Action Plan (Minute 5.1 refers) Viv Duncanson informed the Committee that there were 3 points to note:-
1) 13.04.14 – In respect of the hand hygiene audits in A&E at DPOW, there had been significant earlier improvement which had not been sustained. The item was therefore changed back to amber.
2) 13.03.01 – Viv Duncanson requested the Committee’s agreement to the number of attempts for catheterisation before escalation. The Committee agreed that the number of attempts for catheterisation should be the same as peripheral (3 times). Viv confirmed she would update the catheterisation policy accordingly.
3) 13.06.14 – Following arbitration NLAG were responsible for this MRSA infection and
a DIPC review meeting was being held on Friday, 22 November. Viv confirmed she would update the Committee accordingly.
Viv confirmed that there were 2 hospital acquired MRSA bacteraemia cases to date.
5.2 C Difficile Action Plan (Minute 5.2 refers)
Viv Duncanson updated the Committee on the following:- 1) 13.02.02 – Awards had been presented to a number of wards for achieving 100 day
free of C.difficile. There have also been certificates awarded to a number of wards for being 200/300 days C.diff free. 1 year certificates are due to be awarded at the end of December 2013. Karen Jackson explained that accumulation would need to be taken into account next year as some wards may in fact be 400/500 days C.diff free; Viv confirmed she would look into this.
2) 13.17.03 – Viv explained that she and Dr Vicca had met with Bioquell to look at taking the usage of HPV forward. Dr Vicca explained that there were issues in respect of the logistics of this therefore it had not moved forward. The Committee agreed that they were to remain aware of this item.
3) 13.01.09 – Antimicrobial prescribing can be updated following the earlier discussion
(minute 3(i)). Viv confirmed that there were 14 recorded hospital acquired C.diff cases to date.
5.3 Governance Datix Report – Infection Control related incidents – Q2 – 2013/14
(Minute 5.3 refers)
The Committee perused the report and confirmed that no worrying trends appeared however the Committee agreed they would like Wendy Booth to confirm how the risks are graded and bring this item back to the next Committee meeting under matters arising.
Action: Wendy Booth to confirm how risks are graded
5.4 Incident/Outbreak Quarterly Report: July – September 2013
Viv Duncanson informed the Committee that this report was to highlight surveillance of incidents is being carried out other than C.diff and MRSA (Viv has produced an amended report following the Committee meeting – this report is attached to these minutes at Appendix B)
5.5 Update Site Specific Groups (Minute 5.4 refers)
Karen Wilson informed the Committee that the deep clean of Ward 23 at SGH had not yet taken place because of a lack of nursing support to move patients out of the bays. Karen confirmed that once nursing support was available this would be carried out.
5.6 Risk Assessments – Summary of Risk Register
The Committee agreed that Wendy Booth’s input and guidance was required on this item.
Action: Wendy Booth
5.6.1 Notice of Derogation & Risk Assessment – Peripheral Cannulas
The Committee agreed that they were happy with this derogation and for the policy to be amended in respect of allowing 2% chlorhexidine and 70% alcohol swabs for all vascular devices.
Action: Viv Duncanson to amend policy following approved derogation
6. Policies/Items for ratification 6.1 Benchtop Steam Sterilisers
The policy had been the commented on by the relevant disciplines. Dr Vicca informed the Committee that he felt if ’21 years’ remained for retention of records within the policy then Synergy would similarly have to change their policy to 21 years. Kirsty Edmondson-Jones confirmed she would seek clarification on this; subject to this point the Committee approved the policy.
Action: Kirsty Edmondson-Jones to clarify 21 years issue 6.2 Viral Haemorrhagic Fevers
The Committee approved this updated policy and the concept of linking to national guidance.
6.3 New Builds Refurbishment Reconfiguration Guidelines The Committee approved this updated policy. 6.4 Final Terms of Reference – Water Safety Group (Minute 3(e) refers) The Terms of Reference were ratified by the Committee. 7. Keogh Report – ICC Oversight Actions (Minute 6 refers)
Viv Duncanson updated the Committee in respect of the hand hygiene campaign and infection control notice boards. Viv explained that she was extremely anxious in respect of hand hygiene at the point of care as the steel alcohol rub dispenser holders had been going missing which were constantly requiring replenishing. Viv confirmed that she had spoken with the company who provides the holders in order to look at screwing them to the bed frame and she was awaiting their feedback on this. Viv informed the Committee that she has ensured that spare holders had been provided in all areas in order to avoid being caught on audits without hand hygiene at the point of care.

8. ICC Self-Assessment Framework (Minute 7 refers)
The Committee went through the self-assessment framework and confirmed that they were happy with each point. Neil Gammon raised the issue that the Committee Terms of Reference may require reviewing given the appointment of the Assistant Medical Directors. Dr Peter Cowling also explained that when a review of the Terms of Reference is carried out he feels that it needs to be considered whether or not the Committee has sufficient representation from Consultants. The Committee agreed that this would be discussed at the next meeting. Dr Cowling also explained that he felt it was important that ‘prevention’ was included in the title of the Committee; the Committee agreed that the name would be changed to the Infection Control & Prevention Committee.
9. Infection Control Mandatory Training
Viv Duncanson informed the Committee that infection control mandatory training, across all areas, was at 74%.
10. Highlight Report for the Trust Board
The Committee confirmed that there were 3 items to add to the Highlight Report for the Trust Board:-
1) Rapid Response Audit for antimicrobials 2) C.diff free certificates/awards – 1 year awards at end of December 2013 3) Committee name change – Infection Prevention & Control Committee
Action: Neil Gammon and Professor Carrock Sewell to liaise in respect of producing Highlight Report
11. Review of Action Log
The Committee perused the Action Log and made several amendments following updates. The Committee agreed that the amended Action Log would be produced at the next meeting, together with the actions from this meeting. Action: Leanne Glasson to update Action Log
12. Items for Information 12.1 ICC Group Minutes – DPOW 12.2 ICC Group Minutes – SGH 12.3 Final Water Safety Plan (Minute 3(e) refers) 12.4 DPOW C Diff Action Plan 12.5 Minutes of the Antimicrobial Steering Group 13. Any Other Business
Andy Karvot informed the Committee that today was European Antibiotic Awareness Day. Neil Gammon requested that the next Committee meeting scheduled for Monday, 20 January 2014 (1.00 pm – 3.00 pm) be rearranged to Friday, 17 January 2014 (12.30 pm – 2.30 pm) given that he has longstanding commitments; the Committee were agreeable to this. Leanne Glasson confirmed she would email the Committee with the meeting details, as shown at paragraph 14 below.

14. Date & Time of Next Meeting
Friday, 17 January 2014 12.30 pm – 2.30 pm (Trust Meeting Room, SGH with vtc to Small Meeting Room, DPOW)
Appendix A – 21 day infection prevention final report Appendix B – amended Incident/Outbreak Quarterly Report (item 5.4)

Appendix A
Infection Prevention Control Report – 21 day Assessment Project
Aim
The aim of the project was to identify patients who have been an inpatient for 21 days in order
that a pro-active approach could be made in the form of an assessment to identify factors for the
prevention of the acquisition of Healthcare Associated Infection.
For each patient who met the 21 day criteria, the IPCN would visit the ward to perform the risk
assessment which involved the nursing team. Where issues / potential issues of practice were
noted a prompt / reminder would be given to the nursing team which was also recorded in the
patients notes and on a bespoke database.
The Wards that were included in the project were:
Medical Wards DPOW (excluding AMU)
Medical wards SGH (excluding MAU)
Surgical & Orthopaedic trauma wards DPOW
Surgical & Orthopaedic trauma wards SGH
Methodology
The project was conducted over a 3 month period Aug – Oct 2013. On a daily basis (Mon – Fri
where resources allowed), the Infection Control Data Officer produced a report highlighting any
patients who met the 21 day in-patient criteria which was sent to the IPCN’s. A retrospective
report was also completed on a Monday to identify any patients who had met the criteria over
the week end period.
On receipt of the patient details report, the IPCN would visit the ward to carry out a one-off
assessment which consisted of reviewing: the microbiology history, patient documentation and
observation charts, talking to the patient and staff.
Following the assessment the IPCN would discuss the findings with the relevant staff members;
complete the designated advice / escalation sticker and place in the patient’s documentation.
The ’21-day’ database was also completed.
Results
There were a total of 373 patients reviewed as
part of the 21 day project;
188 Patients were at Diana Princess of Wales
Hospital and 185 patients at Scunthorpe General
Hospital.
DPOW 188
SGH 185
Total 373
21 Days - Non compliance issue
58 57
45
41
28 2826 25
2118
1412
9 9
0
10
20
30
40
50
60
70
Rev
iew N
utriti
onal N
eeds
Use
rev
iew /
stop d
ates
Rec
ord V
IP S
core
Ass
ess
need o
f Unir
ary
Cat
heter
Switc
h from
Iv to
(? c
an IV
be
rem
oved)
Pat
ient u
sing a
ntimic
robia
l body
was
h
Ref
er to
Inva
sive
Dev
ices
Pra
ctiti
oner
Obta
in s
wab
for C &
S if
sig
n of i
nfect
ion
Mai
ntain
Tru
st W
ound Rec
ord
Can
nula In
sertio
n Rec
ord
Rev
iew n
eed O
ther
Inva
sive
Dev
ices
See
k Consu
ltant A
dvice
Ref
er to
Tis
sue
Via
bility
Nurs
e
Ref
er to
Oth
er N
urse
Spec
ialis
t
Themes
Occu
ren
ce
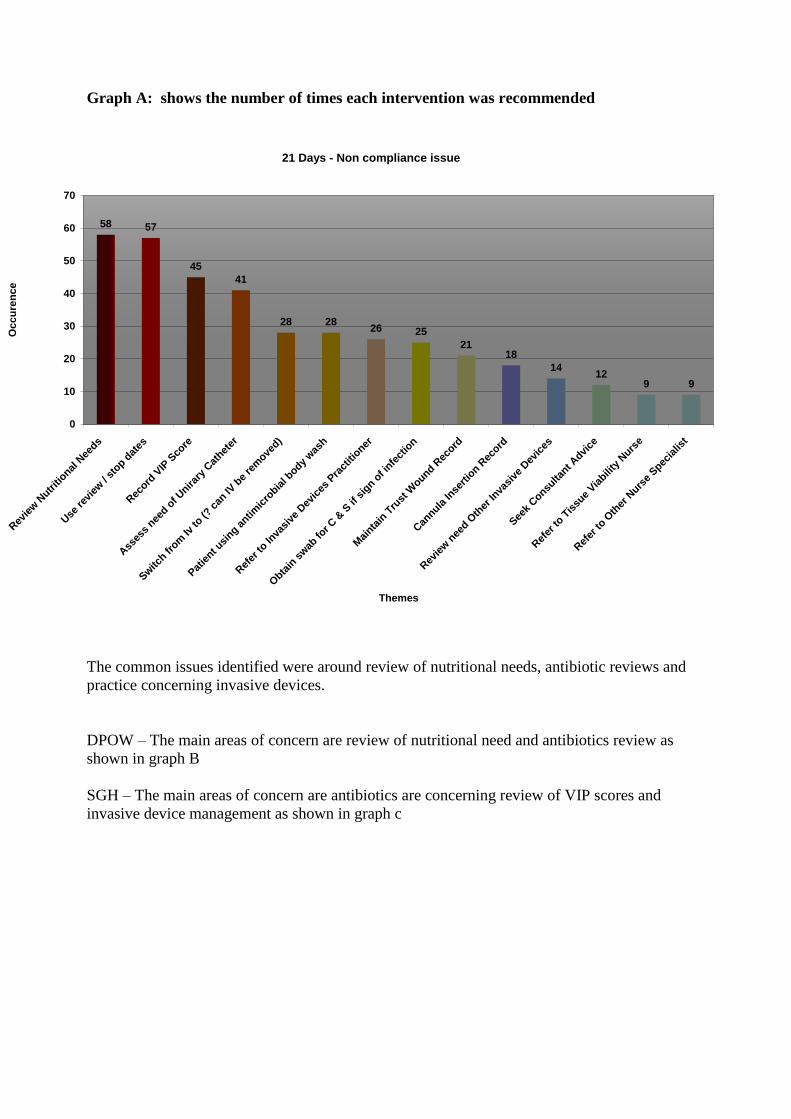
Graph A: shows the number of times each intervention was recommended
The common issues identified were around review of nutritional needs, antibiotic reviews and
practice concerning invasive devices.
DPOW – The main areas of concern are review of nutritional need and antibiotics review as
shown in graph B
SGH – The main areas of concern are antibiotics are concerning review of VIP scores and
invasive device management as shown in graph c

21 Days - Non compliance issue - DPOW
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
Rev
iew N
utriti
onal N
eeds
Use
rev
iew /
stop d
ates
Obta
in s
wab
for C
& S
if s
ign o
f infe
ctio
n
Rec
ord V
IP S
core
Mai
ntain
Tru
st W
ound Rec
ord
Ass
ess
need o
f Unira
ry C
athet
er
Rev
iew n
eed O
ther
Inva
sive
Dev
ices
Switc
h from
Iv to
(? c
an IV
be
rem
oved)
Can
nula In
sertio
n Rec
ord
Ref
er to
Inva
sive
Dev
ices
Pra
ctiti
oner
Ref
er to
Tis
sue
Viabili
ty N
urse
Ref
er to
Oth
er N
urse
Specia
list
Seek
Consu
ltant A
dvice
Patie
nt usi
ng antim
icro
bial b
ody was
h
Themes
Perc
en
tag
e
21 Days - Non compliance issue - SGH
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%
16.00%
Use
rev
iew /
stop d
ates
Rec
ord V
IP S
core
Ass
ess
need o
f Unira
ry C
athet
er
Patie
nt usi
ng antim
icro
bial b
ody was
h
Ref
er to
Inva
sive
Dev
ices
Pra
ctiti
oner
Switc
h from
Iv to
(? c
an IV
be
rem
oved)
Rev
iew N
utriti
onal N
eeds
Can
nula In
sertio
n Rec
ord
Obta
in s
wab
for C
& S
if s
ign o
f infe
ctio
n
Seek
Consu
ltant A
dvice
Mai
ntain
Tru
st W
ound Rec
ord
Rev
iew n
eed O
ther
Inva
sive
Dev
ices
Ref
er to
Tis
sue
Viabili
ty N
urse
Ref
er to
Oth
er N
urse
Specia
list
Themes
Perc
en
tag
e
Graph B: Themes / Non Compliance issues -DPOW
Graph C: Themes / Non Compliance issues – SGH

Table A: Themes identified at DPOW
DPOW
Review Nutritional Needs 42 23.20%
Use review / stop dates 26 14.36%
Obtain swab for C & S if sign of infection 18 9.94%
Record VIP Score 15 8.29%
Maintain Trust Wound Record 15 8.29%
Assess need of Urinary Catheter 14 7.73%
Review need Other Invasive Devices 9 4.97%
Switch from Iv to (? can IV be removed) 9 4.97%
Cannula Insertion Record 7 3.87%
Refer to Invasive Devices Practitioner 6 3.31%
Refer to Tissue Viability Nurse 6 3.31%
Refer to Other Nurse Specialist 6 3.31%
Seek Consultant Advice 5 2.76%
Patient using antimicrobial body wash 3 1.66%
Table B: Themes identified at SGH
SGH
Use review / stop dates 31 14.76%
Record VIP Score 30 14.29%
Assess need of Urinary Catheter 27 12.86%
Patient using antimicrobial body wash 25 11.90%
Refer to Invasive Devices Practitioner 20 9.52%
Switch from Iv to (? can IV be removed) 19 9.05%
Review Nutritional Needs 16 7.62%
Cannula Insertion Record 11 5.24%
Obtain swab for C & S if sign of infection 7 3.33%
Seek Consultant Advice 7 3.33%
Maintain Trust Wound Record 6 2.86%
Review need Other Invasive Devices 5 2.38%
Refer to Tissue Viability Nurse 3 1.43%
Refer to Other Nurse Specialist 3 1.43%
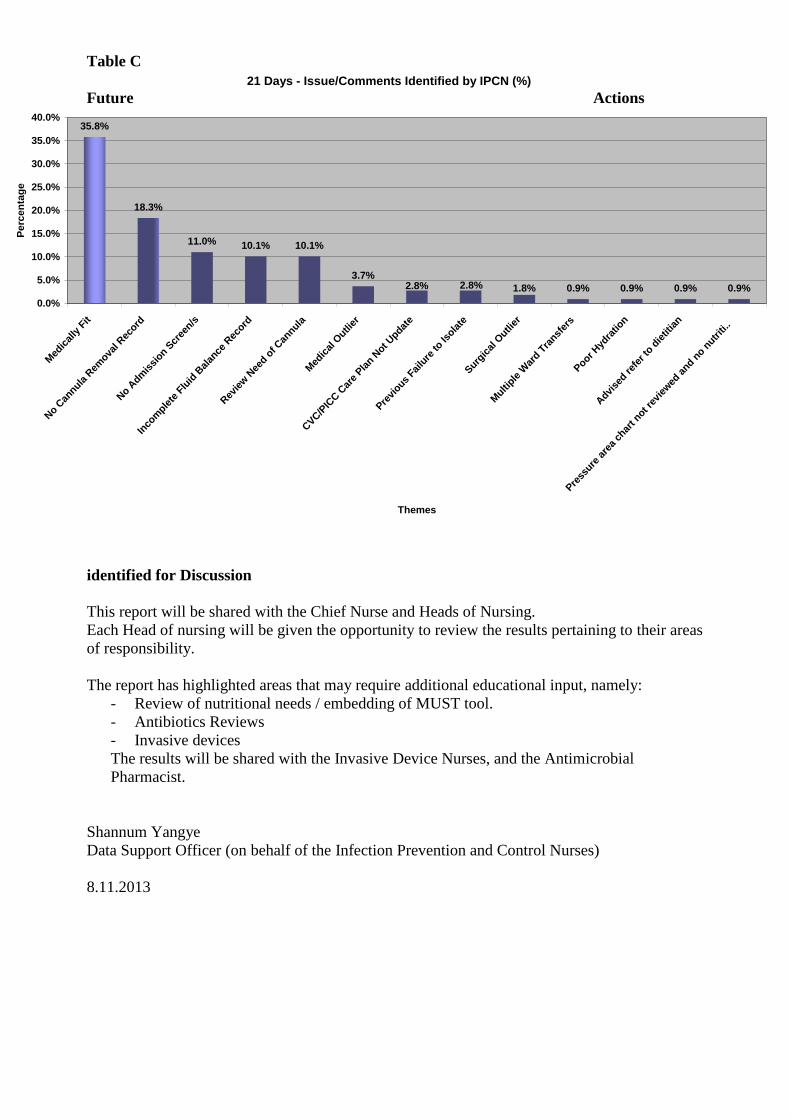
In addition to the predetermined interventions the IPCN’s also identified a number of additional
issues (see table C below)
The most prominent issue highlighted is the number of “medically fit patients”.
21 Days - Issue/Comments Identified by IPCN (%)
35.8%
18.3%
11.0% 10.1% 10.1%
3.7%
0.9% 0.9% 0.9% 0.9%1.8%2.8%2.8%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
Med
ical
ly F
it
No C
annula
Rem
oval R
ecord
No A
dmis
sion S
cree
n/s
Inco
mple
te F
luid
Bal
ance
Rec
ord
Rev
iew
Nee
d of C
annula
Med
ical
Outli
er
CVC/P
ICC C
are
Pla
n Not U
pdate
Pre
vious
Failu
re to
Isola
teSurg
ical
Outli
er
Multi
ple W
ard T
ransf
ers
Poor
Hyd
ratio
n
Advi
sed r
efer
to d
ietit
ian
Pre
ssure
are
a ch
art n
ot rev
iewed
and n
o nutr
iti..
Themes
Pe
rcen
tag
e
Table C
Future Actions
identified for Discussion
This report will be shared with the Chief Nurse and Heads of Nursing.
Each Head of nursing will be given the opportunity to review the results pertaining to their areas
of responsibility.
The report has highlighted areas that may require additional educational input, namely:
- Review of nutritional needs / embedding of MUST tool.
- Antibiotics Reviews
- Invasive devices
The results will be shared with the Invasive Device Nurses, and the Antimicrobial
Pharmacist.
Shannum Yangye
Data Support Officer (on behalf of the Infection Prevention and Control Nurses)
8.11.2013

Appendix B
BOARD SUB-COMMITTEE FRONT SHEET:
INFECTION CONTROL COMMITTEE
DATE OF MEETING
18 November 2013
REPORT FOR
Infection Control Committee
REPORT FROM
Infection Prevention & Control Team
SUBJECT
Incident/Outbreak Quarterly Report: July - Sep 2013
CONTACT OFFICER
Viv Duncanson, ADIPC
OTHER GROUPS WHO HAVE CONSIDERED PAPER (Where applicable)
N/A
EXECUTIVE COMMENT (including key issues of note or, where relevant, concerns that the committee need to be made aware of)
The purpose of this report is to bring the following to the attention of the Infection Control Committee:
Outbreak/Incident occurrence
C. difficile, MRSA and orthopaedic wound infection surveillance data
INFECTION CONTROL COMMITTEE ACTION REQUIRED
Infection Control Committee to note the report and review trends.

INFECTION CONTROL REPORT TO INFECTION CONTROL COMMITTEE INCIDENTS/OUTBREAKS
PERIOD OF REPORT: Jul – Sep 2013 1. INCIDENTS/INVESTIGATIONS
a. Ward 24: Period of increased incidence of C. difficile (Apr -July 2013)
A cluster of 3 hospital-acquired cases of C.difficile had been noted on Ward 24 SGH in addition to a community-acquired case that had also been nursed on the ward. This was reviewed by the C. difficile Action Group and resulted in a deep clean of the ward, ward-focused antibiotic audits and continued requests for typing of isolates. In addition, a ward visit by senior nursing management and the ADIPC to review practice was undertaken and attendance by ward staff at C. difficile training sessions reviewed. The potential to introduce mandatory electronic bed management system for use of the side rooms and inclusion of antibiotics on the ward round/board round was also to be explored. A review of several of these actions revealed that the standard of the deep clean had been poor with a room that had apparently been completed still having a dirty and sticky patient bed table. On escalation to the Deep Clean Team Supervisor it appeared that the team had not been informed that this was an infection clean and it was uncertain as to whether the steam cleaner had been used. It was noted, however, that the C. difficile checklist was in use and commodes were clean. A review of the number of staff that had attended C. difficile training showed that 26 of 29 staff had attended. Actions arising from this incident have been included on the site-specific C. difficile action plan and monitoring is ongoing.
b. Disney Ward: Group A Strep (July 2013)
On 22/07/13 the ICT were made aware of 3 cases of Group A streptococcus on Disney ward. Investigation revealed that all swabs were taken on admission and were from different body sites. None of the children were on the ward at the same time and no further action was deemed necessary.
c. MAU: Glutamate Dehydrogenase (GDH) (July 2013)
A DART notification was received of 3 cases of GDH (Glutamate Dehydrogenise) on MAU in July 2013. On investigation it was found that all patients had been admitted with diarrhoea but were isolated on admission. All patients were admitted on different days and into different side rooms. Cross infection was not deemed to be a factor and no further action was taken.
d. ITU: Stenotrophomonas maltophilia in 2 patients (August 2013)
2 patients on ICU were found to have Stenotrophomonas maltophilia. Both had been treated with antibiotics and cross infection was not thought to have occurred.
e. Ward 26: Potential Exposure of Patients to Open TB (August 2013)
On 22/08/2013 the ICT were notified of a patient who had been on Ward 26 whilst actively symptomatic for TB but untreated. Investigation revealed that the patient had been exposed to others and therefore a list of potential contacts was collected. Following an Incident Meeting, risk assessments were carried out for each admission episode. In view that the index case was related to a local college TB incident, it was decided that the TB should be considered infectious and the normal 8 hour contact time should, therefore be reduced. Arrangements were put in place for the Respiratory Nurse to visit all contact patients and all babies to be offered a baby check by the paediatric team. A later update from the Respiratory Nurse Specialist revealed that all adults, including patients, partners and staff had tested negative and babies were all negative on the first round of testing. However, one partner had been untested due to difficulties in getting time off work

and, although he had reported that he was well with no signs to suggest TB had signalled his intent to undergo testing in the near future. Another 3 female patients had had ‘inform and advice letters’ hand delivered to them but none had made any contact with the team. There had also been no contact from any other staff members other than those tested. As such, no further arrangements were made to extend contact tracing at that point.
f. C1K: Bay Closure due to Diarrhoea (August 2013)
A bay was closed on 04/08/13 in response to a number of patients developing loose stools. 2 patients were isolated in side rooms and 2 others remained in the bay. The bay was reviewed on the following day and cleaned before being re-opened.
g. A&E: Alleged Poor Infection Control Practice (September 2013)
On the 10/09/2013 the ICT received a phone call from an IPCN from Buckinghamshire CCG regarding an MRSA bacteraemia case that she had been involved in. Although the root cause of the bacteraemia was not related to this incident the Buckinghamshire IPCN wished to bring one of the findings from the RCA to the attention of the SGH IPCNs in that the patient’s wife had alleged poor practice in the SGH A&E dept. The background to the allegation was established in that the patient had been on holiday in Scunthorpe and attended A & E with a blocked catheter on 27/07/2013. He was re- catheterised and discharged on the same day. During the catheterisation procedure it is alleged that the catheter was dropped on the floor and then re-used. On investigation, the clinician who had carried out the procedure maintained that the patient was re-catheterised using an aseptic technique and denied that the catheter was dropped and re-used. The wife did not wish to pursue a formal complaint and the Buckinghamshire IPCN did not require/request feedback following the investigation by the SGH IPCN.
h. Ward 18: High Pseudomonas Count in Hand Wash Sink (September 2013)
On 30/09/2013 Facilities contacted the ICT regarding counts found on random sampling of sinks on Ward 18. One sink in the Day Case area yielded a count of 58 cfu/100mls which is high. The ward was therefore visited together with Facilities where it was stated that the sink was only used for hand hygiene but staff did note that there was a smell from time to time. Disposal of any waste down the sink was denied. The sink was put out of action and a cleaning regime commenced until negative results were received. The fact that routine flushing returns have not been received from this ward was made known to the Head of Nursing.
2. Outbreaks
Ward Bay Closed Open Cause Staff
Affected Patients Affected
22 Ward 17/09/2013 26/09/2013 D&V 2 9
3. Surveillance a. Clostridium difficile
Current Rate/10,000 bed days
1.2
2012 2013
HAI CAI HAI (3 numeric days)
CAI
DPOW (3 numeric
days)
SGH & GDH
(Pre-48hrs)
DPOW SGH & GDH
DPOW SGH GDH DPOW SGH GDH
Jul 0 1 0 1 1 2 0 0 0 0
Aug 1 1 0 1 2 0 1 0 1 0
Sep 1 2 1 2 0 1 0 0 2 0
TOTAL 2 4 1 4 3 3 1 0 3 0

b. MRSA Bacteraemias: Jul - Sep 2013 DPOW
SGH
GOOLE
TOTAL
No of Trust-acquired 0 1* 0 1
No CAI (3 numeric days) pre-admission acquired 0 3 0 3
No Other Hospital-Acquired 0 0 0 0
No Uncertain 0 0 0 0
No of bacteraemia 0 4 0 4 *Community-acquired MRSA attributed to NLAG
c. MSSA Bacteraemias: Jul - Sep 2013 DPOW
SGH
GDH
TOTAL
No of Trust-acquired 3 0 0 3
No CAI (3 numeric days) pre-admission acquired 9 6 0 15
No Other Hospital-Acquired 0 1 0 1
No Uncertain 0 0 0 0
No of bacteraemia 12 7 0 19
d. Surveillance of Surgical Site Infection (SSSI) Current Quarter: Apr - Jun 2013
Hip Replacement Knee Replacement Repair Neck of Femur
DPOW SGH GDH DPOW SGH GDH DPOW SGH GDH
Current Period: No of operations
40 31 17 37 36 35 53 50 0
Current Period: No of infections from patients undergoing surgery this quarter
0 0 0 1 1 0 0 1 0
Cumulative Data for period [Jul–Sept 2008 to Apr - Jun 2013
Cumulative Total No of Operations for Last 5 years
962 616 733 1079 706 1107 544 1130 6
Cumulative Total Number of Infections For Last 5 years
7 6 1 13 4 4 4 14 0
Cumulative Total Infection Rate For Last 5 years
0.7% 0.9% 0.7% 1.2% 0.5% 0.6% 0.7% 1.2% 0%
National Average Infection Rate For Last 5 years
1.2% 1.2% 1.2% 1.7% 1.7% 1.7% 1.8% 1.8% 1.8%
Report Prepared by: Ruth Leckie Date: 11 October 2013 – updated 19 November 2013 On Behalf of the Infection Control Team