patient safety and compensation harm · 2019-07-20 · –is an incident which did not reach the...
TRANSCRIPT
PATIENT SAFETY AND
COMPENSATION
HARM
PROUDLY HOSTED BY THE
MDPCZ & HPAZ
DR. M R BILLA : REGISTRAR/CEO
ADV. F P KHUMALO : HOD LEGAL AND REGULATORY AFFAIRS

• CChallenges:
– Delivering safer and quality care in complex, pressurised and fast-moving healthcare
environments.
– In such environments, things can often go wrong.
– Patient Safety Incident Reporting and Learning Systems is used to identify patient
safety issues
• Cornerstone of patient safety strategies.
– By learning from these systems, errors can be corrected to
• prevent reoccurrence and
• ensure that patient safety,
• quality of care and health outcomes of patients are improved.
PATIENT SAFETY

• The impact of medico-legal litigations threatens the vision of Government of
– “Achieving a long and healthy life for all South Africans”
• WHO recommendation for Uniform National Reporting System of Adverse events
related to patient safety must be implemented
• National Department of Health (NDoH) developed the
– National Guideline for Patient Safety Incident Reporting and Learning System
• to guide the health system in dealing with patient safety incident reporting.
• Every health establishment should have a Patient Safety Incident Reporting and
Learning system as stipulated in this Guideline.
• Data from the system will be used to develop National action plans to improve
patient safety to ensure that all South Africans receive safe health care.
THE MINISTERIAL MEDICO- LEGAL COMMITTEE
• Lapses in patient safety are a major health care quality problem.
• These lapses in patient safety are referred to as patient safety incidents (PSI).
• PSI is an event or circumstance that could have resulted or did result in harm to a
patient as a result of the health care services provided, and not due to the underlying health condition.
• These are considered incidents.
– near miss,
– no harm incident or
– harmful incident (adverse event).
• A large majority of these lapses are the unintended results of highly complex and
imperfect health care delivery systems.
• Professional errors, at risk behaviour and reckless misconduct or negligent behaviour
contribute to patient safety incidents (PSI).
• All health-care professionals should report PSIs as soon as they become aware of it to
ensure that optimal learning take place.
Pharmaceuticals
PATIENT SAFETY INCIDENT
Competitor
Contoso Pharmaceuticals
IMPROVED PATIENT SAFETY
Competitor
Improved Patient Safety
Improved patient
satisfaction with health services
Reduction of avoidable mortality
Reduction of harm
encountered during care
Reduction in litigations
Reduced health care costs
Contoso Pharmaceuticals
REPORTING PATIENT SAFETY INCIDENTS
Competitor
• Report and record all patient safety incidents
• Report all incidents that resulted in serious harm or death (Severity
Assessment Code 1 incidents) within 24 hours to management or sub-
district/district and provincial office
• Commence and/or participate in the open disclosure process as
appropriate
• Participate in the investigation of incidents as required
• Finalise Severity Assessment Code 1 incident reports within sixty
working days
• Participate in the implementation of recommendations arising from
the investigation of incidents
• Encourage colleagues to report incidents that have been identified
– Use of reporting tool – to be discussed later
Contoso Pharmaceuticals
DEFINITION OF TERMS USED
Competitor
• Patient Safety:
– is the reduction of risk of unnecessary harm associated with
healthcare to an acceptable minimum.
• Near miss:
– is an incident which did not reach the patient.
• No harm incident:
– is an incident which reached a patient but no discernible harm
resulted.
• Harmful incident (adverse event):
– is an incident that results in harm to a patient that is related to
medical management, in contrast to disease complications or
underlying disease.

Contoso Pharmaceuticals
DEFINITION OF TERMS USED
Competitor
• Incident type:
– a descriptive term for a category made up of incidents of a
common nature, grouped because of shared, agreed
features
• Harm:
– implies impairment of structure or function of the body
and/or any deleterious effect arising there from, including
disease, injury, suffering, disability and death, and may be
physical, social or psychological.
• Degree of harm:
– is the severity and duration of any harm, and any treatment
implications, that result from an incident.
Contoso Pharmaceuticals
DEFINITION OF TERMS
Competitor
• Incident outcomes:
– all impacts upon a patient or an organisation wholly or partially attributable to
an incident
• Organisational outcome:
– the impact upon an organisation which is wholly or partially attributable to an
incident.
• Patient outcome:
– is the impact upon a patient which is wholly or partially attributable to an
incident
• Resulting actions:
– identify immediate or indirect action taken that relates to the patient or the
organization to improve the situation or prevent the reoccurrence of an incident.
• Minimal Information model:
– refers to a minimal common architecture for the core concepts considered tobe essential for information and comparison purposes of PSI reports
Pharmaceuticals
PRINCIPLES OF PATIENT SAFETY INCIDENT
Competitor
• Just Culture
• Confidential
• Timely
• Responsive
• Openness about failures
• Emphasis on learning

Pharmaceuticals
MARKERS OF NURSING CAREMarkers of Nursing Care
Pressure Ulcers
Patient Falls
Patient Safety

Pharmaceuticals
Competitor
PATIENT FALLS
o We have been tracking this for the last two years or so as a way ofmeasuring the quality of nursing care in the hospital.
o The plan is to focus more on the intrinsic factors, which I assume maybe
related to the clinical condition of the patient and the medication theyare taking.
o Appropriate measures need to be taken to prevent such falls. We will
develop new measures and protocols on how to prevent these falls. “
Inpatient falls are common and remain a great challenge for the NHS.
o Falls in hospital are the most commonly reported patient safety incidents,
with more than 240,000 reported in acute hospitals and mental healthtrusts in England and Wales every year (that is over 600 a day).”
PURPOSE OF THE PROJECT
o To do a retrospective study of the number of patient falls in the hospital
o To analyse the factors leading to patient falls in the hospital and group these into extrinsic and intrinsic factors
o To determine if these falls could have been prevented if appropriate measures were taken to prevent them, if any
o To develop strategies on how to prevent these patient falls
ls
OBJECTIVES OF STUDY
Pharmaceuticals
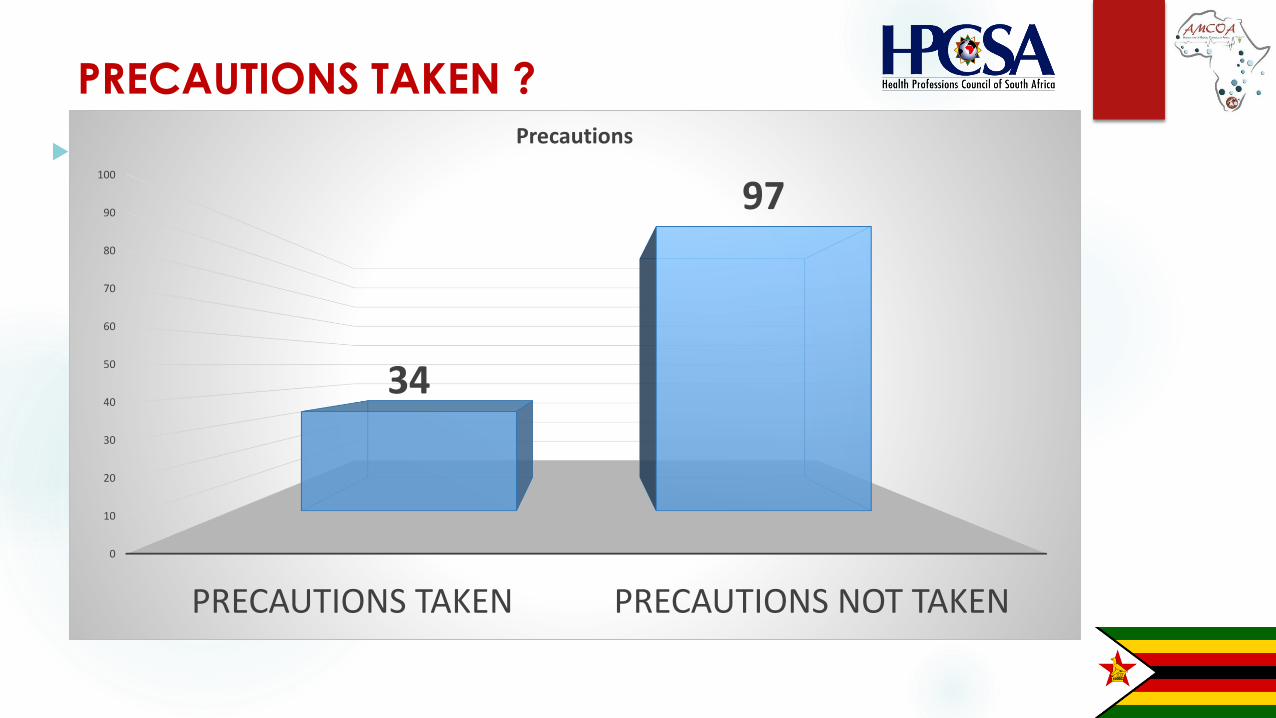
PRECAUTIONS TAKEN ?
Competitor
Precautions taken ?
0
10
20
30
40
50
60
70
80
90
100
PRECAUTIONS TAKEN PRECAUTIONS NOT TAKEN
34
97
Precautions
Pharmaceuticals
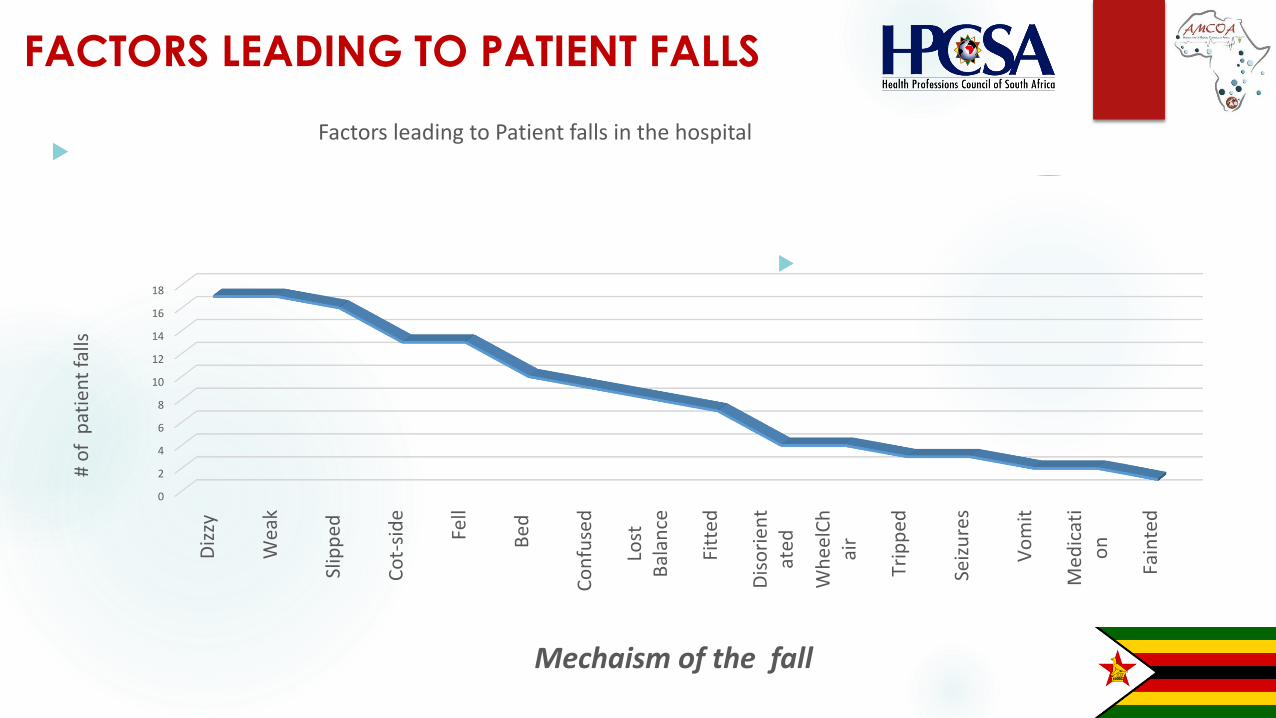
FACTORS LEADING TO PATIENT FALLS
Competitor
0
2
4
6
8
10
12
14
16
18
Diz
zy
Wea
k
Slip
ped
Co
t-si
de
Fell
Bed
Co
nfu
sed
Lost
Bal
ance
Fitt
ed
Dis
ori
en
tat
ed
Wh
eelC
hai
r
Trip
ped
Seiz
ure
s
Vo
mit
Med
icat
io
n
Fain
ted
# o
f p
atie
nt
falls
Mechaism of the fall
Factors leading to Patient falls in the hospital

Pharmaceuticals
FACTORS LEADING TO PATIENT FALLS CONT….
Competitor
71
60
Intrinsic Extrinsic
Pharmaceuticals
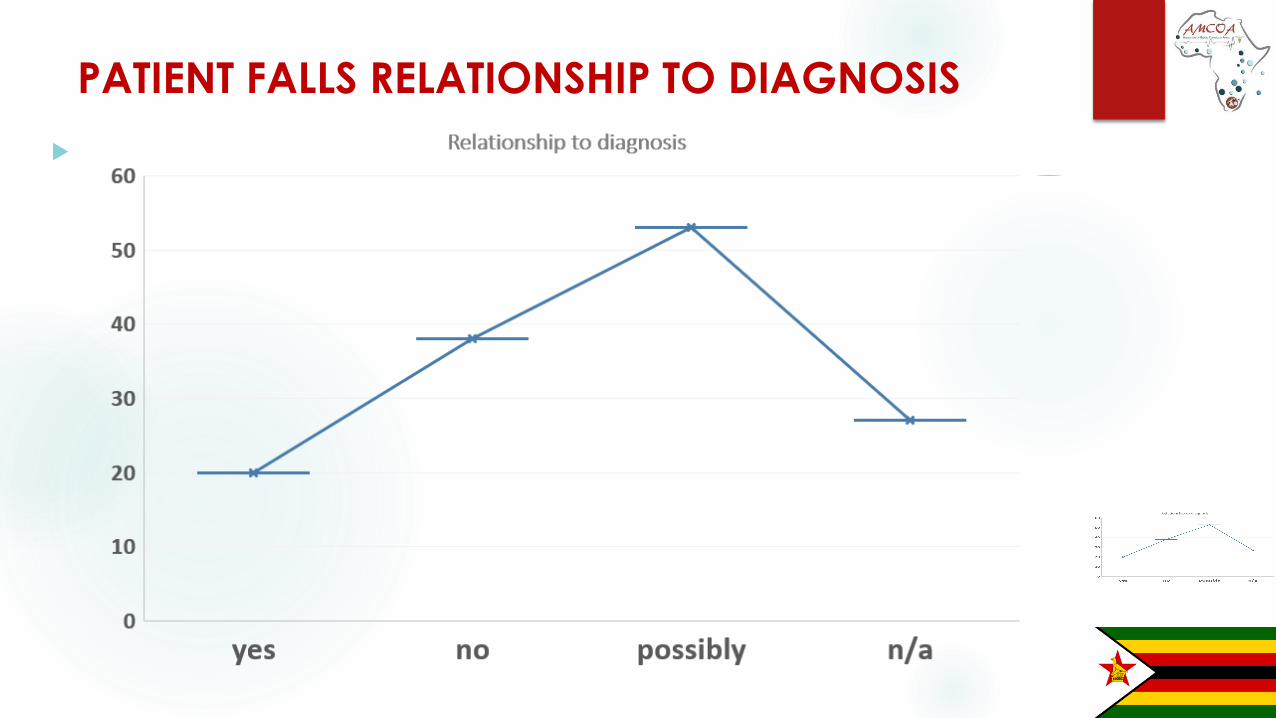
PATIENT FALLS RELATIONSHIP TO DIAGNOSIS
Patient Falls Relationship to
Diagnosis
Pharmaceuticals
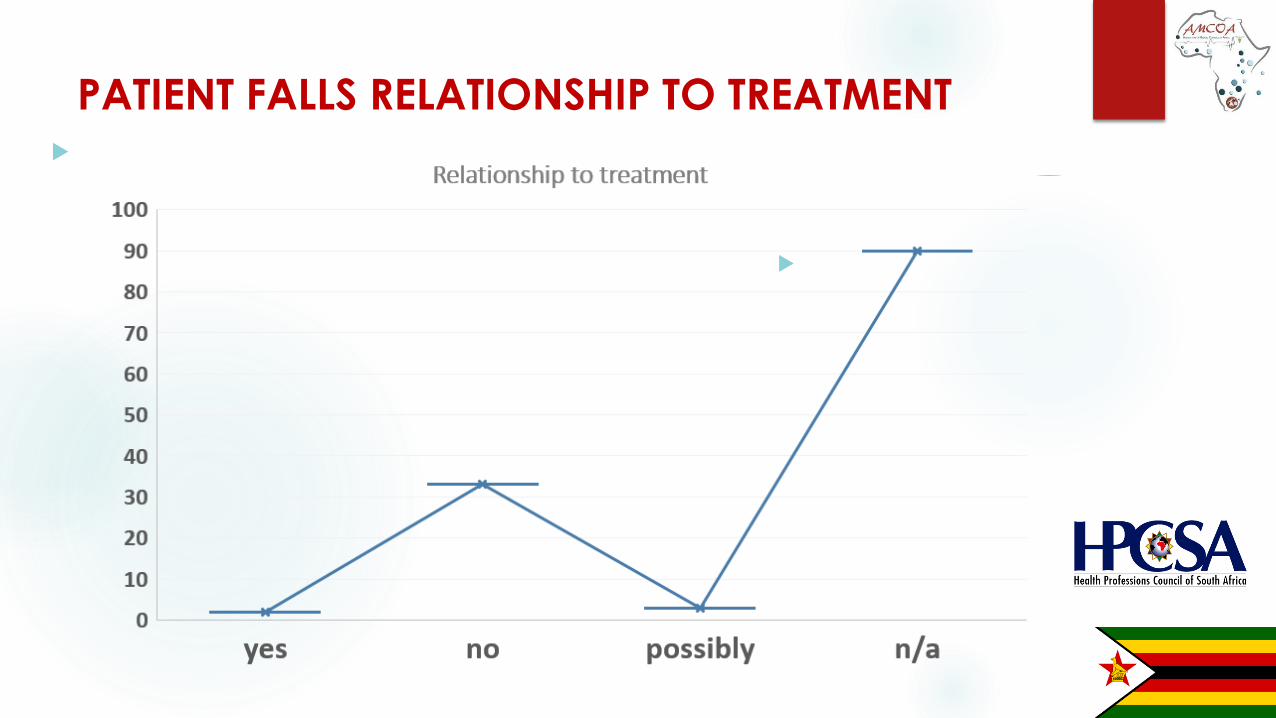
PATIENT FALLS RELATIONSHIP TO TREATMENT
Competitor

Pharmaceuticals
Competitor
Serious Adverse Event Reporting Tool
DrMS Reporting Form for Safety
Incident_php.htm
http://www.123contactform.com/form-
2440797/DrMS-Reporting-Form-For-Safety-
Incident

SOUTH AFRICAN LAW REFORM COMMISSION 2017
Competitor
Investigation into escalating medical claims

Pharmaceuticals
SOULS CLEOPAS VS PREMIER OF GAUTENG
Competitor
• The Minister of Justice and Correctional Services (the Minister) wrote to
the Chairperson of the SALRC on 16 January 2015.
• The Minister wrote the said letter in reaction to a request to the
Department of Justice and Constitutional Development (DOJCD) for
legislation to address the matters raised in the case of
– Souls Cleopas and the Premier of Gauteng unreported case
09/41967, Gauteng South High Court, April 2014 (Souls Cleopas case).
• The case was brought on the basis of negligent medical treatment that
the plaintiff had received from staff at Gauteng hospitals

• An official from the Office of the State Attorney: Johannesburg, requested
a meeting with the SALRC via the DOJCD on the increase in claims based
on medical negligence against the State.
• As a result of this meeting the SALRC agreed to look into :
– the manner in which compensation for medical malpractice is
determined and paid,
– the influence of the common law ―once and for all rule‖ on medico-
legal claims and
– lump sum payments as part of an investigation into medico-legal claims
against the state.
ESCALATING MEDICAL CLAIMS
Competitor

Pharmaceuticals
MEDICAL CLAIMS PAID OUT PER PROVINCE
Competitor
Province 2010/11 2011/12 2012/13 2013/14
Gauteng R 8 291 000.00 R 30 930 758.24 R 124 846 892.41 R 153 612 355.49
Eastern Cape R 10 260 049.00 R 25 336 038.35 R 44 743 495.84 R 49 513 108.93
Northern Cape R 6 810 428.00 R 705 000.00 R - R 7 107 000.00
KwaZulu Natal R 22 695 078.06 R 10 762 367.72 R 14 767 477.56 R 205 312 356.94
Western Cape R 9 210 000.00 R 15 860 000.00 R 11 710 000.00 R 15 680 000.00
Mahikeng R 12 550 000.00 R 753 602.57 R 7 899 232.50 R 698 940.17
Limpopo R 8 229 068.81 R 3 457 954.27 R 6 844 259.18 R 21 959 395.55
Free State R 256 081.57 R 988 604.43 R 327 192.00 R 673 373.00
Mpumalanga R 17 229 427.00 R 13 252 319.44 R 11 310 058.70 R 44 408 386.64
TOTAL R 95 531 132.44 R 102 046 645.02 R 222 448 608.19 R 498 964 916.72

• No legislation currently exists in South Africa to specifically address legal claims in the
medical field, which means that claims based on medical negligence are dealt with
under the common law.
• The escalation in medical negligence litigation, and in particular the increase in the
size of the damages sought and awarded, has become a major cause for concern in
the public and private health sectors.
• There is an urgent need to undertake reform of the law in order to regulate a system
that will become paralysed if no action is taken. It is crucial to cut down on litigationthat consumes time and money. Apart from the impact of medical litigation on the
public purse, the negative effect of such litigation on the rendering of health services inthe private sector must also be considered.
NEED FOR LAW REFORM
Competitor

• Regardless of the nature of the changes, legislation will be required to
effect such changes.
• Developing legislation in this field will aid in furthering the
implementation of broader government policy - Development Plan
(NDP) offers a long-term perspective
• Doctors turning to ―defensive medicine: Claassen & Verschoor
NEED FOR LAW REFORM
• The SALRC has called for inputs after it conducted an investigation into medico-legal
claims, especially claims against the state
• Its purpose is to initiate and stimulate debate, to seek proposals for reform and to serve as
a basis for further deliberation by the Commission
• The comment of any person on any issue contained in the issue paper or in respect of a
related issue which may need inclusion in the debate is sought.
• Such comment is of vital importance to the Commission, as it will assist in providing
direction with regard to the scope and focus of the investigation
• Respondents are requested to submit written comment, representations or requests to the
Commission by no later than 30 September 2017.
SOUTH AFRICAN LAW REFORM COMMISSION
PAPER
S
A media report on the summit commented that:
– The Minister of Health, addressing the summit, expressed his
concern that the lawsuit crisis that South Africa finds itself in
is ―what led to the collapse of the Australian health system15 years ago‖. He also referred to the ―US [that] had a
similar crisis in the 1970s and 1980s.‖
MEDICO-LEGAL SUMMIT OF MARCH 2015
Pharmaceuticals
MEDICAL MALPRACTICE WORKSHOP – MARCH
2017
Competitor
The Minister of Health reportedly made the following remarks at the summit:3
The nature of the crisis is that our country is experiencing a very sharp increase – actually an
explosion in medical malpractice litigation – which is not in keeping with generally known trends
of negligence or malpractice. … The cost of medical malpractice claims has skyrocketed and the
number of claims increased substantially. … [T]he crisis we are faced with is not a crisis of public
healthcare. It is a crisis faced by everybody in the healthcare profession – public and private.
Medical Malpractice Workshop of March 2017
Pharmaceuticals
COMPENSATION FOR HARM
Competitor

The golden tread in legislative framework establishing medical or health regulators of
different jurisdiction is that they exist to protect the public
• This public protection is achieved by ensuring that only competently educated and trained health practitioners are allowed to practice their profession;
• How do regulators satisfy themselves that a health practitioner is competently educated and trained?
• By setting the standards or get involved in setting the standards for education and training and monitor the implementation of such standards
THE ROLE OF A MEDICAL OR HEALTH REGULATOR IN
PATIENT SAFETY
Competitor
• By recognizing the qualifications for which the education standards have been set (entitling the holder thereof to practice);
• By ensuring that only registered/licensed persons are allowed to practice their profession in their respective jurisdiction;
• By setting and enforcing the standards for professional practice and professional conduct/ethical conduct;
THE ROLE OF A MEDICAL OR HEALTH REGULATOR IN
PATIENT SAFETY CONT…

Pharmaceuticals
THE ROLE OF A MEDICAL OR HEALTH REGULATOR IN
PATIENT SAFETY CONT…
CompetitorWhat happens when standards for professional practice and
professional/ethical conduct are violated?
• Regulators take disciplinary actions against offending health practitioners and if found guilty health practitioners face disciplinary sanctions ranging from a caution to removal of a name from the register of health practitioners;
Pharmaceuticals
THE ROLE OF A MEDICAL OR HEALTH REGULATOR IN
PATIENT SAFETY CONT…
CompetitorAre disciplinary processes effective in dealing with medical
malpractice ?
• AMCOA member countries experience-let us have a brief discussion (5 minutes)
Pharmaceuticals
MEDICAL MALPRACTICE: A REGULATORY SLIPPERY
SLOPE
Competitor
Who should regulate medical malpractice?
• Is it the Department of health (seeing that often hospitals are facing civil litigation for compensation for harm);
• Is it the criminal justice system (seeing that health practitioners are facing criminal charges for culpable homicide- van Der Waldt case);
• Is it medical or health regulators (seeing that they set standard for professional practice and professional conduct);
Is there a medical malpractice crisis?
According to Masada (Masada ST.2004, Australia’s “Most Extreme Case”: A new
Alternative for US medical Malpractice Liability Reform, Pacific Rim Law & Policy
Journal, 163(2004)), medical malpractice crisis refers to a drastic surge in health care
providers’ liability insurance premiums that ultimately has encumbered patients
access to affordable health care.
• More than one-fourth of U.S. adults have experienced a medical error within the pasttwo years, despite the fact that the United States spends much more on health carethan any other country (Sage WM. 2003, Medical Liability and Patient Safety, HealthLaw 22:4);
• The Gauteng Department of Health and Social Development faced malpracticeclaims totalling R573 million in 2009 – 2010 (Pepper M, Slabbert MN.2011. Is South
Africa on the verge of a medical malpractice litigation storm?, June 2011, Vol. 4, No.
1 SAJBL)
MEDICAL MALPRACTICE: A REGULATORY SLIPPERY
SLOPE
Pharmaceuticals
MEDICAL MALPRACTICE: A REGULATORY SLIPPERY
SLOPE
Competitor
Is there a medical malpractice crisis?
• In 2011 the Medical Protection Society (MPS) was assisting more than
895 members in South Africa who had ongoing negligence claims,
while there were more than 1 000 open files that were potential claims
awaiting assessment (Pepper supra);
• This represented an increase of nearly 550% compared with 10 years
ago; and the number of claims over R5 million had increased by 900%
in the past 5 years, with several topping the R30 million mark(Pepper
supra);
Pharmaceuticals
MEDICAL MALPRACTICE: A REGULATORY SLIPPERY
SLOPE
Is there a medical malpractice crisis?
• The annual premium charged by the Medical Protection Society for
malpractice cover increased three-fold between 2008 and 2013, with
neurosurgery now classified as 'super high risk’.
• The annual premium (R250 900 for 2013) was second only to that for
obstetricians (R254 230) (Roytowski D, et al. 2014, Impressions of
defensive medical practice and medical litigation among South African
neurosurgeons, SAMJ, S. Afr. med. j. vol.104 n.11 Cape Town Nov. 2014)
• The scale of the problem is reflected in South Africa's highest-ever
medical damages settlement of R25 million in June 2013, to a patient
who had undergone neurosurgery (Roytowski D, et al supra)

Is there a medical malpractice crisis?
What are the consequences of an increase in litigation?
According to Roytowski D, et al supra, the net result of increased litigation and increasedpremiums is thought to have amongst others, the following consequences where
medical practice is concerned:
a) A change in practice to more defensive behaviour, with the effect of increasingcosts to patients and funders, ultimately driving up healthcare inflation;
b) Limiting practice to patients and conditions that are thought to be 'lower risk'
rather than taking on complex or surgically demanding cases; and
c) Discouraging specialisation in high-risk disciplines and seeking activities withreduced liability risk, such as non-clinical legal, insurance or road accident fund
work.
als
MEDICAL MALPRACTICE: A REGULATORY SLIPPERY
SLOPE
Is there a medical malpractice crisis?
What are other challenges of a delict/fault/tort based malpractice system?
litigation is often a lengthy process;
Other patient are not compensated because their injuries were not negligently caused;
Indigent patient do not afford litigation costs;
When compensation is finally made, up to 25% of the claim is paid to lawyers;
Health budgets in most cases do not include the cost of claims and litigation for medical
malpractice and thus funds appropriated for health services are depleted;
MEDICAL MALPRACTICE: A REGULATORY SLIPPERY
SLOPE

Pharmaceuticals
COMPENSATION FOR HARM: AN ALTERNATIVE TO
TRADITIONAL LITIGATION
CompetitorWhat are the alternatives to tradition litigation for compensation for harm?
• We have seen that at the centre of medical malpractice crisis is an
increase in litigation;
• there is consensus that where patients have suffered harm compensation
must be made;
• there is a view that compensation for harm should not always be an
outcome of costly litigation
Pharmaceuticals
COMPENSATION FOR HARM: AN ALTERNATIVE TO
TRADITIONAL LITIGATION
Competitor
What are the alternatives to tradition litigation for compensation for harm?
• What if there was a system where an incident of medical malpractice would be investigated by a
multidisciplinary committee/task team (comprising of clinical experts, legal experts, health
economist/actuaries) and where a claim is found to be legitimate, compensation is awarded to a
victim without a need to go to court and prove fault- A ‘no fault liability’.
• In South Africa a National Health Litigation Authority Bill, was drafted in 2012 “To provide for the
establishment of the National Health Litigation Authority; to provide for appropriate redress for loss
or damage arising out of medical negligence from the public and private health establishment
and where applicable, provide for appropriate redress, including monitory compensation; and to
provide for matters connected therewith.”.
PWhat are the alternatives to tradition litigation for compensation for harm?
• National Health Litigation Authority Bill is still under consideration;
• In the UK, the Secretary of State for Health, signed Order (in 1995) establishing and
constituting the National Health Service Litigation Authority “to exercise on behalf of
the Secretary of State certain of his functions in connection with the establishment
and, subsequently, the administration of a scheme under section 21 of the National
Health Service and Community Care Act 1990 for meeting liabilities of health service
bodies to third parties for loss, damage or injury arising out of the exercise by those
bodies of their functions.
COMPENSATION FOR HARM: AN ALTERNATIVE TO
TRADITIONAL LITIGATION
PWhat are the alternatives to tradition litigation for compensation for harm?
• In 1974 New Zealand replaced a delict/tort-based system for compensating
medical injuries with a government-funded compensation system which prohibited
medical malpractice litigation(Bismark M and Paterson R. 2006, No-Fault
Compensation In New Zealand: Harmonizing Injury Compensation, Provider
Accountability, And Patient Safety, HEALTH A F FA I R S, Vo l u m e 2 5 , Nu m b e r 1);
• In 2005 New Zealand expanded eligibility for compensation to all “treatment
injuries,” thus creating a true no-fault compensation system (Bismark supra);
• The benefit of the New Zealand system is that it offers more-timely compensation to
a greater number of injured patients and more-effective processes for complaintresolution and provider accountability (Bismark supra);
COMPENSATION FOR HARM: AN ALTERNATIVE TO
TRADITIONAL LITIGATION
PHow does New Zealand claim process work?
The New Zealand’s Accident Compensation Corporation (ACC) system is one ofthe simplest in the world for patients to navigate, and although the eligibility criteria
have changed, the decision-making process remains much the same (Bismark
supra);
Claims are decided in the ACC’s national claims unit, based on information
provided by patients and their providers, and advice from independent clinical
advisers (Bismark supra);
Straightforward claims can be processed in weeks, with a statutory requirement fordecisions to be made within nine months (Bismark supra);
Historically, the ACC has accepted around 40 percent of all claims. Dissatisfied
claimants may request a review of the decision, and if this fails, they have a right of
court appeal (Bismark supra);
COMPENSATION FOR HARM: AN ALTERNATIVE TO
TRADITIONAL LITIGATION
PHow is the ACC financed and what kind of entitlements are paid?
The ACC is financed through general taxation and an employer levy (Bismark supra);
A fixed award schedule means that claimants with similar disabilities receive similar compensation(Bismark supra);
Entitlements fall into four categories (Bismark supra):
(1) Treatment and rehabilitation includes the cost of pharmaceuticals, disability aids, child care, homemodifications, and vocational retraining. Most treatment costs are already covered by New Zealand’suniversal health care system.
(2) Compensation for loss of earnings includes weekly compensation of 80 percent of the claimant’searnings at the time of injury, up to a set maximum. (High earners can purchase additional first-partyincome protection insurance.)
(3) Lump-sum compensation—a onetime payment of up to US$70,000 to compensate for permanentimpairment resulting from an injury—is paid in addition to any other ACC entitlements.
(4) Support for dependents-takes the form of a funeral grant and a survivor’s grant paid to surviving spousesand children under age eighteen.
COMPENSATION FOR HARM: AN ALTERNATIVE TO
TRADITIONAL LITIGATION
What are some of the benefits of a no fault system?
Reduction of barriers to compensation;
Reduction of costs (no litigation;
Increase in disclosure of errors as health practitioners would not be threatened by
litigation;
Reduce instances of practice of defensive medicine;
Encourage specialization in arrears considered high risk because of litigation;
Increased quality of care as cases are analysed for purposes of improvement and
not defence preparation;
Any other benefits?
COMPENSATION FOR HARM: AN ALTERNATIVE TO
TRADITIONAL LITIGATION

THANK YOU