patient case module 4 date of preparation: june 2015 hq/eff/15/0024h
TRANSCRIPT


PATIENT CASE
Module 4
Date of preparation: June 2015 HQ/EFF/15/0024h

A case of breakthrough cancer pain in a patient with prostate cancerDr Andrew DaviesConsultant in Palliative MedicineSt. Luke’s Cancer Centre, Guildford (UK)
Oncology referral

Patient history
Male65 years oldRetired quantity surveyorNo significant past medical historyDiagnosed locally advanced prostate cancer 2012 – treated with anti-androgen therapy, radiotherapyDiagnosed metastatic prostate cancer 2014 – treated with further anti-androgen therapy, chemotherapyCurrent treatment dexamethasone
Current pain/illnesses
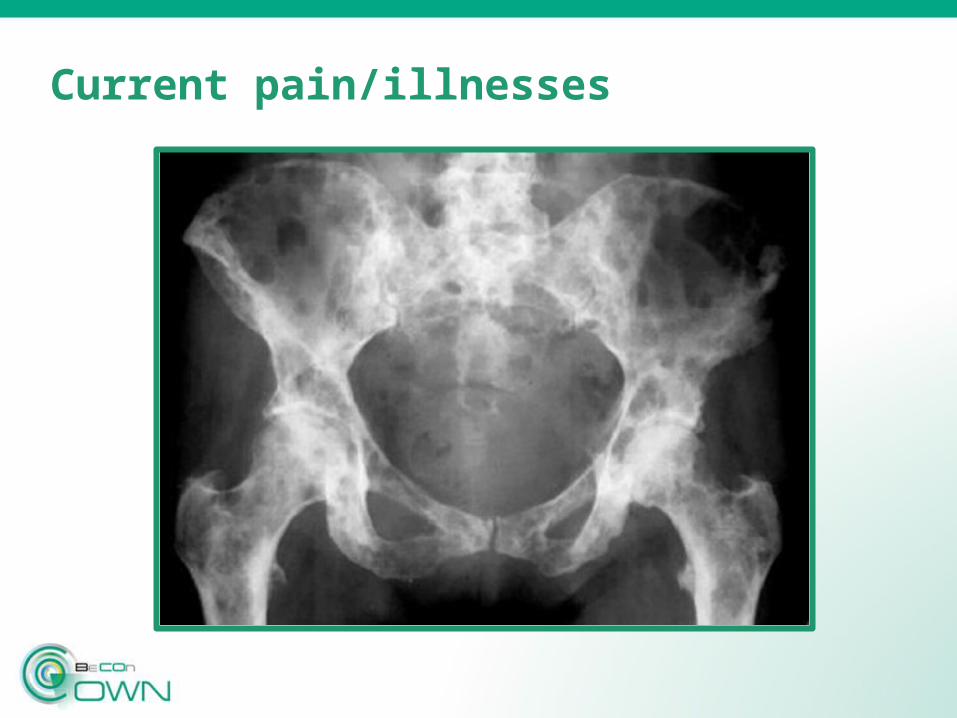
Pain pelvis for 3/12 – pain present all the time (“mild” in intensity), but worse on walking (“severe” in intensity)
Pain prevents him walking his dog (or walking > 10 m for any reason); no pain at night (sleeps well)
Current medication – modified release morphine sulfate 30 mg twice a day, immediate release morphine sulfate 10 mg as required
Clinical oncologist gave a course palliative radiotherapy to pelvis (no effect)
Current pain/illnesses

Clinical examination and pain assessment
Patient looks well
ECOG performance status 4 (limited by pain)
No bone tenderness
No neurological signs
[BAT – Breakthrough Pain Assessment Tool completed]
Clinical judgment
Breakthrough pain – volitional, incident sub-type
Therapeutic approach
Modified release morphine sulfate titrated to 40 mg twice a day
Oral transmucosal (sublingual) fentanyl citrate prescribed / titrated to 400 mcg as required – to be taken when quick pain relief required, and prior to walking (short episodes); dose titrated to optimal dose (i.e. effect vs side effects)
Oral immediate release morphine titrated to 7.5 mg as required – to be taken prior to walking (longer episodes); dose titrated to optimal dose (i.e. effect vs. side effects)
Follow-up
Patient reviewed on weekly basis (shared care between palliative care team and general practitioner)
Exercise tolerance increased to 100 m (no adverse effects from increased dose of morphine)
Oral transmucosal fentanyl citrate effective treatment for BTcP (quicker onset of action, better effect, shorter duration of effect - as compared to oral morphine)
Oncology review regarding role of bisphosphonate / alternative anti-cancer treatment – referred by palliative care team

Conclusions
BTcP improved with a combination of strategies (i.e. increase in background medication, use of transmucosal fentanyl citrate formulation)
Multidisciplinary team engagement is essential for optimal management of BTcP
Thank you