patient and person-centred care - 1000 lives plus · patient & family centred care ... •―19...
TRANSCRIPT
Insert name of
presentation on Master
Slide
Patient and Person-centred
Care
Wednesday, 7th November 2012

“Croeso” “Välkomna”
Welcome13-30-13.40 Brief introduction- set the scene (Annette Bartley)
13.40-14.00 Models of Person Centred Care in Jonkoping. (Anette Nilsson)
14.00-14.05 Learning from Sweden: The Journey so far.
14.05-14.25 Terry Watkins and Karen Newman will present on Aneurin Bevan
Health Board ‗100,000 days - Every day counts for Megan‘ campaign launched
in September 2012.
14.25-14.45 Heather Piggott will showcase the ‗Freda‘ model launched in
September 2012 in Betsi Cadwaladr Health Board.
14.45-15.00 Panel discussion Q&A
15.00-15.15 Refreshments
15.15-15.45 A Better Life for Elderly People. (Anette Nilsson & 10 mins Q&A)
15.45 16.00 Wales‘ person centred care journey (Jan Davies)
1 6.00-16.15 Action planning & Facilitated discussion (Annette Bartley)
16.15-16.30 Summary and close.

Session Aims• The 1000 Lives Plus programme launched in May 2010 and has previously
organised three person centred care master classes and a number of other
opportunities/activities designed to support the spread of person centred care
within NHS Wales organisations.
• The Master class aims to showcase international expertise, profile Welsh
local developments and facilitate learning and sharing of person centred care
ideas and methodologies.
• The Master class brings together staff from NHS organisations in Wales,
along with key stakeholders (including academics, partner organisations and
improvement colleagues).
• The 1000 Lives Plus team will also be at the event, offering support and
networking opportunities across health boards and trusts.
• To stimulate discussion and promote ACTION to drive forward the patient and
person centred care agenda across Wales

Patient & family centred care
– People are treated with respect and dignity.
– Health care providers communicate and share complete and unbiased information with patients and families in ways that are affirming and useful.
– Individuals and families build on their strengths through participation in experiences that enhance control and independence.
– Collaboration among patients, families, and providers occurs in policy and program development and professional education, as well as in the delivery of care.Source: Institute for Family Centred Care, Bethesda USA
Annette Bartley Consutling Limited 2012

The Reality in Practice

The “what” and the “how” of
healthcare
Rela
tional
Transactional
Warm but chaotic Everything works
Unpleasant and inefficient
“Cold comfort farm”
Efficient but impersonal
Coordinated, integratedWarm, fed, watered “Battery chicks?”
Annette Bartley Consutling Limited 2012

Patient and Family Engagement
Communication Information Collaboration Participation
©Annette Bartley Consutling Limited 2012

A Powerful Evolution
Do it to me.Do it for me.
Do it with me.Martha HaywardPatient Advocate
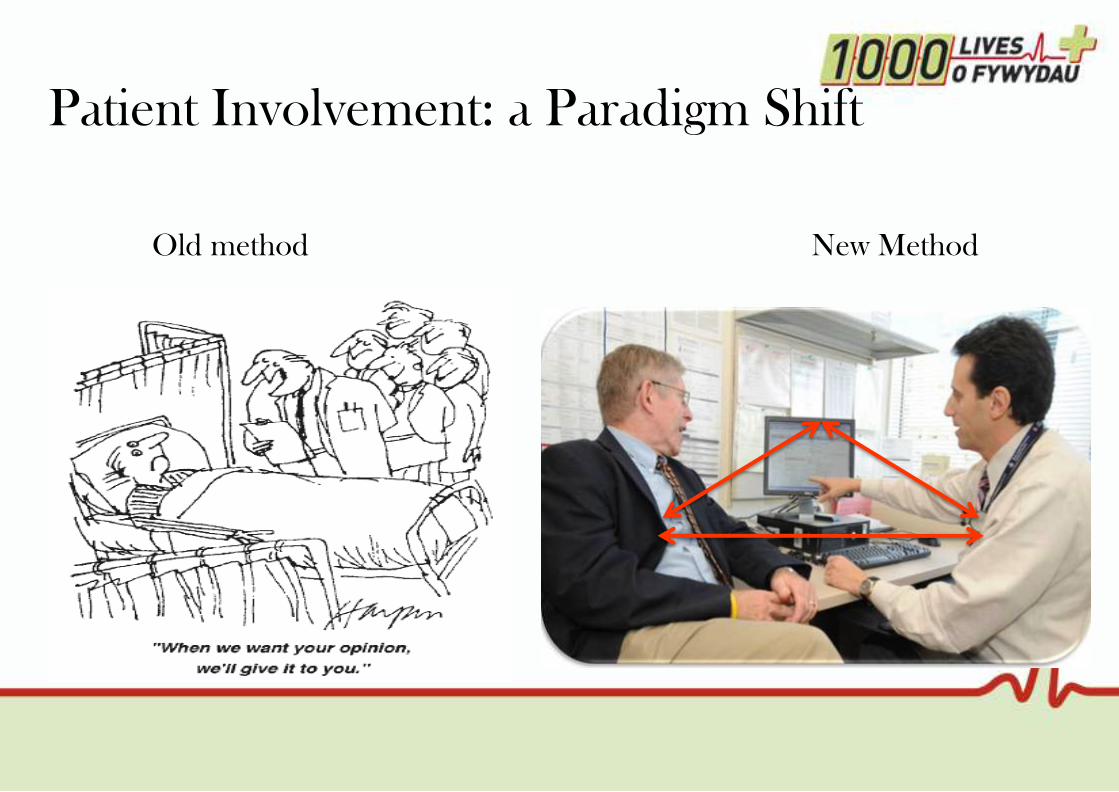
Patient Involvement: a Paradigm Shift
Old method New Method

ANETTE NILSSON
Models of Person Centred Care in Jonkoping.

Person-centred care
Anette Nilsson Qulturum
Jönköping County Council
& SALAR (Swedish Association of
Local Authorities and Regions)
QULTURUM

– Person centred care is about seeing and understanding the
persons need and act from that perspective.
Deeper understanding of every single person who meet the person
QULTURUM

See me
• Maintain someone's personality, despite failing health
(from me to patient…)
• What is meaningful to me?
• What is important to know about me when you meet me?
• How do I become a part of the discussions about me?
(nothing about me without me)
• How to create a working climate where it is ok to do the ―little
extra‖
QULTURUM

Science + Context = Result
Improvement in our heart from
the patient‘s perspective
QULTURUM

‖A true discovery is not about
seeking new horizons,
but seeing the old with new eyes‖
Marcel Proust
QULTURUM
Microsystem – Aim
• To develop front line units in order to provide and support
exceptional care for patients and families while continuously
improving (together with patients and families)
• To create a workplace that engages everyone with high
vitality and joy of work
• To make measurable improvements into outcomes for
patients, families and staff
QULTURUM

QULTURUM
LEAN
Ref; Henriks, Nilsson, Bojestig, Edvinsson, Berger

From ―theory‖ to ―praxis‖…
and back again
QULTURUM
Better patient,
population outcome
Better system
performance
Better professional
development
Everyone
Ref; Paul Batalden
Looking carefully
at the clinical
microsystem…
As a home for
connecting…

Who are we here for?
QULTURUM
We are here to increase
value for our inhabitants…
It's all about values

QULTURUM
Head
Heart
Hands
Patient centred care
TCAB
Network – Your care
What do we want to accomplish by
focusing on patient-focused care?
QULTURUM
• Improve the quality of patient care
• Improve the quality of patient service
• Well prepared and knowledgeable healthcare team meet well
prepared patients & families
• Increase staff satisfaction
• Increase efficiency

An interesting question, on what do nurses and
doctors spend their time during a working day
QULTURUM
Hur fördelar sjuksköterskor sin tid?
Others
20%
Improvement
work 5%
Administration,
information,
communication
40%
Direct patient time
35%

Goal
Safe and involved patient.
Safe nursing care, and
employee satisfaction,
through more interaction
with the patient
Patient focused care
Medicin C
County hospital Ryhov

This is how we interact with our patients:
We listen to and respect our patients
We care and show that we care.
We are interested in and try to understand our patients.
We give our patients information.
We are honest and sincere to our patients.
This is how we interact with each other:
We listen to and respect each other.
We care for each other and show that we care.
We are honest and sincere to each other.
We are positive and happy.
We share our knowledge with each other.
Our values

Improvement from the patients perspective = better
employees satisfaction
Kände du dig väl omhändertagen vid
ankomsten till vår avdelning?
Mål 100 % fullständigt
0%
20%
40%
60%
80%
100%
jan febr mars maj sept jan
2011 2012
%
nej /delvis
ja, nästan helt
ja, fullständigt
Frågor om upplevd trygghet
hos patienten.
Mål 100 % nästan helt eller fullständigt.
0%
20%
40%
60%
80%
100%
feb mars maj sep jan april
2012
%
nej, delvis
ja nästan helt, fullständigt
PersonalnöjdhetMål: 90 % värde 5-7, 10 % värde 4
0%
20%
40%
60%
80%
100%
jan febr mars maj sept jan april sept
2011 2012
Om du tänker på allt som har med din
arbetstillfredsställelse och arbetsmiljö att göra, hur nöjd
är du då?
1= minst nöjd, 7=mest nöjd
%
värde 1-3
värde 4
värde 5-7

QULTURUM
―Every system is
perfectly designed
for the results it
gives‖Don Berwick

Using the model for improvement
QULTURUM
What are we trying to accomplish? Goal !
How will we know that a change is an improvement?
Measure !
What change can we make that will resultin improvement?
Ideas !
Test !Act Plan
DoStudyPDSA-cycle

ESTHER network – like
grandchildren
Always the best for Esther in
the microsystem!
QULTURUM

Passion for life – A social movement
QULTURUM

Passion for Life – Aims
QULTURUM
• To develop conditions for a full healthy life with a high quality
of life for elderly people
• To test procedures to find new methods that can affect the
overall goal we all probably aim for:
best possible life – throughout life

Passion for Life – Goals
QULTURUM
• To incite senior citizens to take their own responsibility for
preventive work for as rich and healthy life as possible
• To find messengers who can communicate knowledge and
methods and spread ideas

Passion for Life – Strategy
QULTURUM
By modern
methods of quality development
incite people to go
from
words and knowledge
to
action and changed lifestyle

Passion for Life – how is it done?
QULTURUM
We met in six
life cafés,
which are rooms of possibilities
where everybody‘s experiences
contribute to improvements
On the way …
QULTURUM
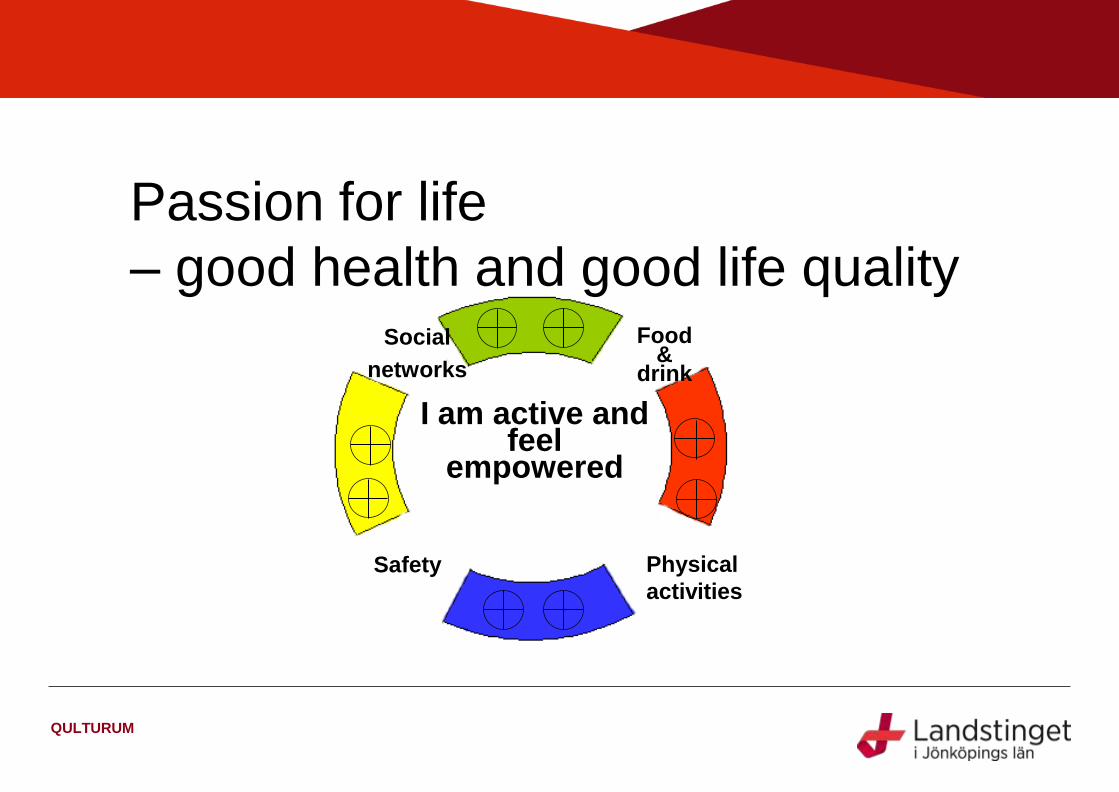
Food &
drink
Social
networks
Safety Physical
activities
I am active and feel
empowered
Passion for life
– good health and good life quality

Constant renewal is necessary
QULTURUM
P
P
P
P
D
D
D
D
S
S
S
S
A
A
A
A
I must all the time strive upwards
towards new goals – it is the joint
result of the small improvements that
lead to the goal
When I have made a change
it is important not to fall back
to old habits and patterns

Passion for life – Life Café 2
QULTURUM
Do I prepare for a safe way
of living by creating
conditions for a long-term
home furnishing in terms of
safety, accessibility etc.?
Goal:
A long-term home
furnishing for quality of life
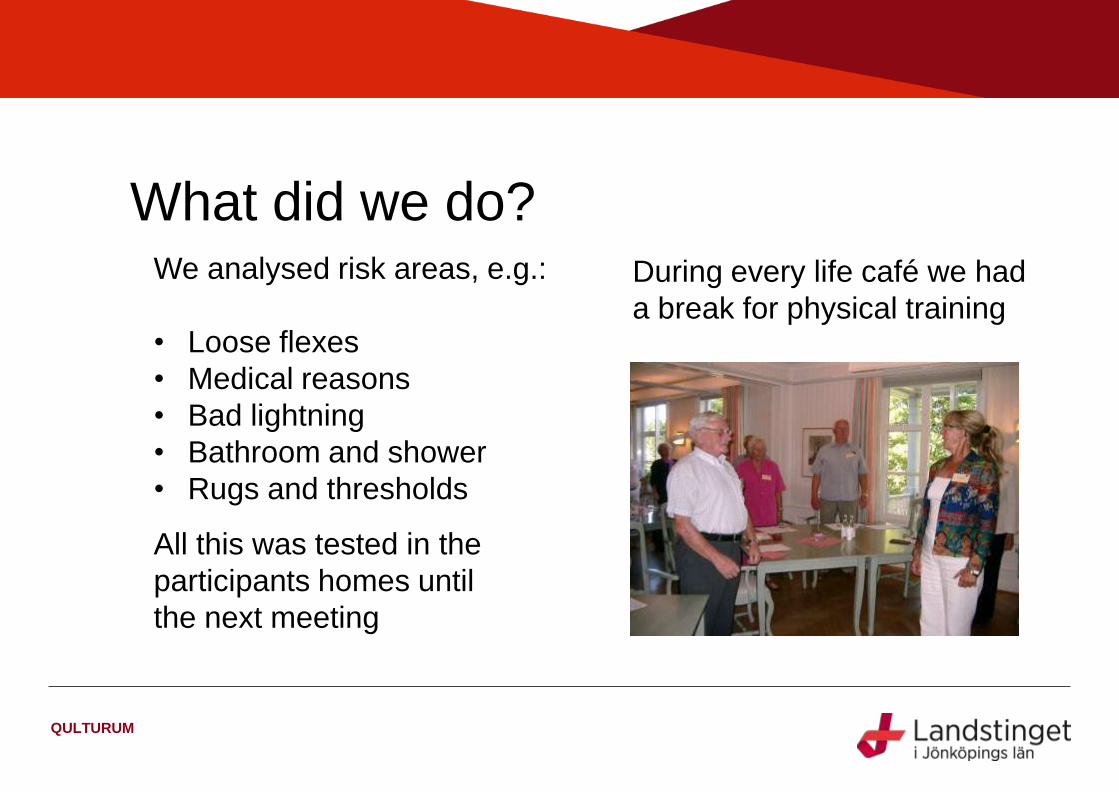
What did we do?
QULTURUM
All this was tested in the
participants homes until
the next meeting
We analysed risk areas, e.g.:
• Loose flexes
• Medical reasons
• Bad lightning
• Bathroom and shower
• Rugs and thresholds
During every life café we had
a break for physical training

A day when we shared ‖life recipes‖
Storytelling
QULTURUM

Some years later…
QULTURUM
…what does Ruth and her friends from the pilot project have to say?
• ―An understanding of how important it is to be able to affect my daily life by being
observant at home and my way of life with exercise and right diet.‖
• ―The joyfulness of spreading the message to others has been inspiring and fun.‖
• ―Passion for Life has given me joy and enriches my everyday.‖
• ―19 of 20 say they would recommend a friend to participate in a Passion for life circle‖
• ―Increased training has improved my physical fitness.‖

– Person centred care is about seeing and understanding the persons
need and act from that perspective.
Deeper understanding of every single person who meet the person
QULTURUM
Learning from Sweden:
The Journey so far.
Terry Watkins and Karen Newman will present on Aneurin Bevan Health Board
‗100,000 days - Every day counts for Megan‘ campaign launched in September
2012.
Heather Piggott will showcase the ‗Freda‘ (fairness, respect, equity, dignity,
autonomy) model launched in September 2012 in Betsi Cadwaladr Health
Board.

Presented By: Terry Watkins
Karen Newman
Date: 07th November 2012
Venue: Llandudno
Every Day Counts
For Megan
Giving back 100,000 days to our Citizens

• A fictitious patient who uses our services
• The person who challenges what we do
• Our integrity, honesty, trust & expectation
• Megan represents us, we are the patients
• The measure of success for our citizens
• Driver for change & collaboration
• The link between service provider & user
Every Day Counts
For Megan
Who is Megan?

• Patient centred care, ―get in and get out safely‖
• People who don‘t need to be admitted to hospital
receive their care in community settings
• People who need to go into hospital receive safe,
effective care as quickly as possible
• People who are ready to leave hospital are supported
to return home safely, and without delay
• Whole systems approach to patient care
• Efficient and effective (Adding Value) getting it right!
Every Day Counts
For Megan
Why the campaign is a priority for us.

Programme Overview
Every Day Counts
For Megan
QI programme contributing bed days 100KD initial scope
1000 Lives + Clinical Lead
Safe Timely Return Home (STRH) √ Nimal Balaratnam
Fractured Neck of Femur (NOF) √ Gordon Gillespie
Hospital Acquired Infection (HAI) √ Liz Waters
Enhanced Recovery After Surgery (ERAS) √ Peter Lewis
Chronic Conditions – Cardiac Failure √ Jackie Austin
Chronic Conditions – Diabetes Dave Minton/Leo Pinto
Chronic Conditions – Chronic Airways Disease Jackie Abbey/Patrick Flood-Page
Frequent Service Users Rowland Hughes
Gwent Frailty Programme Pradeep Khanna
Possible inclusion of “Cellulites” in the New Year.

• Monthly Challenge & Support review CEO, Excecutive Lead, Programme Mgr, Corporate.
• Oversight Board - 6 week review with Chief Exec, Divisional Mgrs, General Mgt, Clinical leads, Senior nurse‘s.
• Measurement review currently being planned for a monthly review with key stakeholders.
• Ward level operational meetings every 2 weeks.
• Ward corporate support & PDSA reviews weekly/fortnightly
• Three main risks:-– The length of stay remains the same / some patients in the wrong place.
– The overall bed configuration will continue to be inflexible (High Occupancy)
– Opening SCCC in Llanfrechfa in 2018 with 444 new beds will result in an
unbalance of resources and will be un-affordable
Every Day Counts
For Megan
Governance & Risk

Every Day Counts
For Megan Safe Timely Return Home (STRH)
Passing the Baton

• Started the (STRH) programme in September 2012
• 6 Pilot wards on three hospital sites in ABHB
• 2 Year roll-out of designed learning sets (4 x 30)
• 272,000 days to go at on 30 wards
• 15 Community & 15 Acute wards to be targeted
• 300+ staff will be involved with this programme
• Supported from ABCi (New Department 2013)
Scope of (STRH)
Every Day Counts
For Megan

• IHI & 1000 Lives + Improvement methodology
• Development of driver diagram at ward level (½ day)
• Supported by PDSA cycles developed by the teams
• Using collaborative reviews ―whole systems approach‖,
Mapping the patient journey end to end
• Corporate resource on the ward every week x 2
• Patient surveys and shadowing key to success
• ―KO AWATEA Good practice‖ learn from New Zealand
STRH Pilot Wards
- Development of driver diagrams
- Supported by PDSA cycles
- Process Mapping
Every Day Counts
For Megan
Methodology
Every Day Counts
For Megan
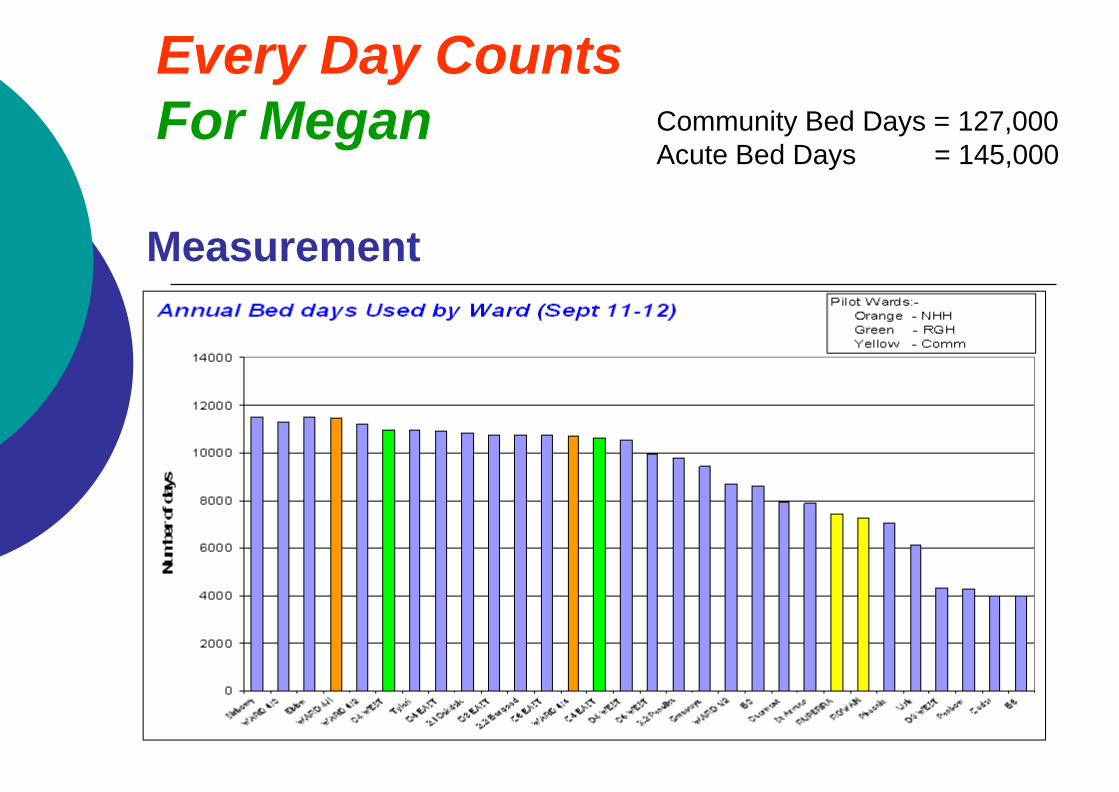
Measurement
Community Bed Days = 127,000
Acute Bed Days = 145,000

Communication
• Internet page
• Nye's News
• Medical Directors Blog
• Chief Executive Blog
• Video Clips
• Local notice boards
• Staff Briefings
• Executive Team Visits
Every Day Counts
For Megan
Every Day Counts
For Megan
Safe Timely Return Home (STRH)
Thank you for your time
QUESTIONS
Introducing Freda
Heather Piggott
Deputy Director of Nursing
and Patient Services.
Betsi Cadwaladr University Health Board

Who is Freda?
19/11/2012 55

BCUHB Values
• Fairness
• Respect
• Equality
• Dignity
• Autonomy
19/11/2012 56

Freda and NICE
Guidance
NICE guidance:
• Knowing the patient as an individual: their values and beliefs
• Essential requirements of care: emotional support, fundamentals of care
• Tailoring healthcare to individual patients
• Continuity of care and relationships
• Enabling patients to actively participate in their care
19/11/2012 57

What will Freda
do for BCUHB?
• Freda is about seeing things through
patients‘ eyes.
• Co-operation between secondary,
primary and community care.
• Identifying gaps in systems and improving
quality of whole system of care in North
Wales
• Participation of all staff
19/11/2012 58

What will Freda do for
BCUHB?
19/11/2012 59
• Stories, values, vision
• Dialogue with patients and carers to
determine priorities
• Planning at all levels linked to public
priorities
• Shared organizational values
• Patient Centred Message brings care,
policy and strategy together.

What will Freda do for
BCUHB?
• Gives staff authority
to question any
action or decision if
not in the interest of
Freda
• ‟What does Freda
need/want?‟
• „What is important to
Freda when she gets
sick‟
• „What is important to
Freda when she
comes home from
hospital ?‟
19/11/2012 60
What‟s the Plan for
Freda?
• Launched at the BCUHB improvement event
September 2012
• Strategic Nursing and Midwifery Committee
October 2012
• National Improvement event November 2012
• BCUHB Board meeting November 2012
• Roll out to Clinical Programme Groups
December 2012-January 2013
19/11/2012 61

In the future
• Consolidate
• Evaluate
• Develop Freda‘s family
• Links to Local Authorities
• Links to third sector organisations
• Links to Education providers
19/11/2012 62

Thank-you
• Questions?
19/11/2012 63

ANETTE NILSSON
A Better Life for Elderly People.
Insert name of presentation on Master Slide

Better life for elderly sick people
”I can grow old in security and retain my independance with access to good health and social care”
Anette Nilsson SKL, project manager – national management program
SALAR
20 county councils/regions – population between 127 000 and 2 019 000 inhabitants
290 municipalities – population between 2 500 and 829 000 inhabitants
Municipal/county/regional councils elected every four years
Local self-government
Right to levy taxes on incomes and charge users for their services

For many elderly people …life is like a dance…but…

Mind the gap – from now to new
Healthy elderly
People at risk
Chronic disease
Multidisease
Special needs health and social care300 000

Challenges
• Increasing number of elderly people
• Elderly people with multiple conditions and complex needs
• New expectations and demands
• Limited resources

• Challenges
• Government agenda
• SALAR Agreements
• Strategies
• Action
• Quality Registries
• Performanced based bonus
Large scale change in the health and social care system

New ways of working
• 500, 000 leaders and co-
workers have to take action
• Preventative
• Based on evidence
• Structured
• Knowledge of results
• Continuous improvements

Cost breakdown health and social care
Average among elderly multi decease during 18 months, 100% = 412 000 sek.
Slutenvård (4 inläggningar)
Kommunal hemtjänst (15 tim/mån för 60% av de äldre)
Öppen specialistvård (7 besök)
Akutbesök på sjukhus (4 besök)
Vårdcentral exkl. hemsjukvård (4 läkarbesök, 4
distriktsköterskebesök)
Hemsjukvårdsbesök vårdcentral (11 besök för ca 50 %
av de äldre)
Kommunal hemsjukvård (17 besök för ca 50% av de
äldre)
Dagvård/växelvård/korttidsvård

• Evidence based practise
• Structured way of working
• From the perspective ofthe individual
• Using results for improvements
• Continuously improving
Changes that make a difference
2010 2013 2014 2015 20162011 2012

What do we want to achieve?
2010 2013 2014 2015 20162011 2012
• Preventative
• Palliative
• Dementia
• Pharmaceutical
• Intgrated care
• Leadership
• Analysis
• Participation in qualityregistries
• Risk assessments
• Dialogue with patient at the end of life
• Pharmaceutical treatment for elderly people is correct
• Individual perspective and responsibility for the wholeprocess
Online data

Senior alert - prevention
The same person is at risk in all areas – why working with all of them simultaneously is effectiv.
• Fall
• Malnutrition
• Preassure ulcers
• Oral health
• Preventative working method
• Make result transparent
• Work to improve
www.senioralert.se
”I know that a risk assesment has been done””We take preventive action to make me feel good”
”I can feel that it makes a difference”

Registration
Systematic way of working
Improvement work
Analyze and reflect about results
IT-supportIntroductionManualsAccess and support
Risk? Treatment? Result?
Vad vill vi åstadkomma?
Hur vet vi att en förändring är en förbättring?
Vilka förändringar kan leda till en förbättring?
Mål !
Mått !
Idéer !
Test !
Agera Planera
GöraStudera
PGSA-cirkeln
Senior alert – four processes
Amount of careplan in patients with risk
0%20%40%60%80%
100%
jan-1
0
feb-1
0
mar-
10
apr-
10
maj-10
jun-1
0
jul-10
aug-1
0
sep-1
0
okt-
10
nov-1
0
dec-1
0
jan-1
1
feb-1
1
mar-
11
apr-
11
maj-11
jun-1
1
jul-11
aug-1
1
sep-1
1
okt-
11
nov-1
1
dec-1
1
Hospital 1 Hospital 2 Hospital 3 County council TargetRelevant preventive activities?

SÄBO Sjukhus
ASIH Åtvidaberg

Key activities 2012
• Four quality registries
• The practice of leadership (ca 320)
• Memberdialogue
• Development of indicators
• Web based qualitativemonitoring
• Show results
• Senior Advisory Board
• Improvment leader’s network(ca 65)

The practice of leadership - from word to action –national manageprogram
• Building leadership teams from Primary Care Clinics, Hospitals and Social Care Organisations
• Cooperation and integration to reach the goals – online data
• Exchange of experience

The key – always start from the elderlys point of view and work togehter!

JAN DAVIES
Wales’ person centred care journey

Insert name of presentation on Master Slide
Wales’ person-centred care
journey
Wednesday, 7th November
Presenter: Janet Davies, 1000 Lives Plus Co-Director

“We all have two jobs: to
do our job and to
improve it.”
“The focus revolves
around delivery of a
service that patients want
and need, rather than
what professionals feel
they should have.”

Quality Delivery Plan
“The best judge of the quality of service
given is the recipient.”
ACTION 5: During 2012 Welsh
Government will develop a national
approach to measuring health service user
experience.

Patient Experience
Framework
• Phase 1 – National Survey for Wales
• Phase 2 – Set of national principles
• Phase 3 – Development of consistent
approach to measure health service user
experience

Principles
• ‗Real-time‘ feedback
• Patients‘ voices heard by Boards
• Inclusivity
• Learning from national surveys
• Drawing on expertise

ANNETTE BARTLEY
Next Steps-
Facilitated Action Planning and
discussion
Insert name of presentation on Master Slide

Action Planning Session
Hunches TheoriesIdeas
Changes That Result in Improvement
A P
S D
A P
S D
Very Small Scale Test
Follow-up Tests
Wide-Scale Tests of Change
Implementation of Change
What are we trying toaccomplish?
How will we know that achange is an improvement?
What change can we make thatwill result in improvement?
Model for Improvement
So what three things will you take
away and test?
• Over the next 20 mins
• In your teams/or as individuals
• Take time out to consider the information
you have heard
• Plan your tests of change
• Feedback and discussion

In summary
• Online resources available on the 1000
lives plus website
• New case studies developed monthly
• Follow us on Twitter @1000LivesPlus
• If you would like to profile an example in
your area please contact the 1000 lives
plus team
Nothing about me without me
Annette Bartley Consutling Limited 2012

PFCC requires a fundamental shift
of focusWe are asking staff,
patients and families to
re-learn how to work
with one another and to
recognize and adjust the
professional and cultural
models that they have
learned.
Annette Bartley Consutling Limited 2012

You are…You are what people see when they arrive here.
Yours are the eyes they look into when they‘re frightened and lonely. Yours are the voices people hear when they are in the lifts and when they try to sleep and when they try to forget their problems. You are what they hear on their way to appointments that could affect their destinies and what they hear after they leave those appointments.
Yours are the comments people hear when you think they can‘t. Yours is the intelligence and caring that people hope they‘ll find here. If you‘re noisy, so is the hospital. If you‘re rude, so is the hospital. And if you‘re wonderful – so is the hospital.
No visitors, no patients can ever know the real you, the you that you know is there — unless you let them see it. All they can know is what they see and hear and experience.
And so I have a stake in your attitude and in the collective attitudes of everyone who works at Cooley Dickinson Hospital. We are judged by your performance. It is judged by the care you give, the attention you pay and the courtesies you extend.
Thank you for all you are doing. CEO Cooley Dickinson Healthcare Org
