pathophysiology and myocardial...
TRANSCRIPT
PATHOPHYSIOLOGY AND NATURAL HISTORYMYOCARDIAL INFARCTION
Prognostic significance and natural history of leftventricular thrombi in patients with acute anteriormyocardial infarction: a two-dimensionalechocardiographic studyPAOLO SPIRITO, M.D., PAOLO BELLOTTI, M.D., FRANCESCO CHIARELLA, M.D.,STEFANO DOMENICUCCI, M.D., ANGELA SEMENTA, M.D., AND CARLO VECCHIO, M.D.
ABSTRACT Fifty-eight patients with transmural anterior myocardial infarction were prospectivelystudied with serial two-dimensional echocardiography to determine the clinical implications andprognostic significance of detection of left ventricular thrombus during acute myocardial infarction, theincidence of systemic embolization, and the possible occurrence of spontaneous regression of leftventricular thrombi. Patients were not treated with anticoagulants or platelet inhibitors during the acutephase of infarction or during follow-up. Two-dimensional echocardiograms were obtained within 24 hrof myocardial infarction, every 24 hr until day 5, every 48 hr until day 15, and every month for afollow-up of 2 to 11 months (mean 7), in the surviving patients; a total of 774 echocardiograms wereobtained. Left ventricular thrombi were identified in 24 (41 %) of the 58 study patients, and developedwithin 48 hr of infarction in 11 of these patients. Ten (91%) of the 11 patients with early thrombusformation died during hospitalization or during follow-up, while only two (15%) of the 13 whodeveloped a thrombus after 48 hr of infarction died (p < .005). Incidence of Killip class III or IV, totallactic dehydrogenase values, and extent of wall motion abnormalities were significantly higher inpatients who developed a thrombus within 48 hr of infarction than in patients without thrombus. On theother hand, in patients who developed a thrombus after 48 hr of infarction, these parameters were notsignificantly different from those in patients who did not develop a thrombus. Spontaneous regressionof thrombi was documented in three (20%) of the 15 patients who survived the acute phase ofmyocardial infarction. The incidence of clinically evident systemic embolic events was low: one of the24 patients with left ventricular thrombus experienced transient ischemic attacks, and no embolicevents were detected in patients without thrombus. We conclude that development of left ventricularthrombi within 2 days of acute anterior myocardial infarction occurs in patients with the most extensiveinfarcts and is predictive of high mortality. Our data also demonstrate that spontaneous regression ofthrombi may occur. Finally, in our study patients, none of whom were treated with anticoagulants or
platelet inhibitors, the incidence of clinically evident systemic embolic events was low.Circulation 72, No. 4, 774-780, 1985.
TWO-DIMENSIONAL ECHOCARDIOGRAPHY hasrecently demonstrated that left ventricular thrombi arecommon in patients with acute anterior myocardialinfarction.1-5 However, the clinical implications andprognostic significance of detection of thrombi duringacute myocardial infarction, the incidence of systemicembolization, and the possible occurrence of sponta-neous regression of left ventricular thrombus have notyet been investigated in prospective studies conducted
From the Divisione di Cardiologia and Servizio di Anatomia edIstologia Patologica, Ente Ospedaliero Ospedali Galliera, Genoa, Italy.
Address for correspondence: Dr. Paolo Spirito, Divisione di Cardio-logia, Ente Ospedaliero, Ospedali Galliera, Via Volta 8. 16128 Genoa,Italy.
Received Dec. 31, 1984; revision accepted May 30. 1985.
in a large population of patients not treated with anti-coagulants. Therefore, it is not known if the detectionof left ventricular thrombi during acute anterior myo-cardial infarction should alter the course of treatment.To address these questions, we obtained serial two-dimensional echocardiograms, at short intervals, in theacute phase and during the months after anterior myo-cardial infarction in a consecutive series of patientswho were not treated with anticoagulants or plateletinhibitors.
MethodsSelection and characterization of patients. Fifty-nine con-
secutive patients admitted to the coronary care unit of the EnteOspedaliero Ospedali Galliera within 24 hr of transmural anteri-
CIRCULATION774
by guest on April 19, 2018
http://circ.ahajournals.org/D
ownloaded from

PATHOPHYSIOLOGY AND NATURAL HISTORY-MYOCARDIAL INFARCTION
or myocardial infarction and who had no evidence of prioranterior myocardial infarction entered the study. A satisfactoryvisualization of the left ventricular cavity in the echocardio-graphic apical views could not be obtained in one patient, whowas excluded from further study. The remaining 58 patientscomprise our study population.
The patients ranged in age from 35 to 87 years (mean 63); 44(76%) were men. The diagnosis of acute anterior myocardialinfarction was documented in each patient by a typical history ofchest pain, serial electrocardiographic changes, and serial ele-vation of serum enzymes. The electrocardiographic criterion fordiagnosis of transmural infarction was the appearance of Qwaves of greater than 0.04 sec in the anterior precordial leads.Total creatine kinase (CK) and CK-MB activity was measuredon admission, at 12 hr after the onset of symptoms, and thenevery 4 hr for the next 16 hr. Total lactic dehydrogenase (LDH)activity was measured on admission, and daily for the first 3hospital days. By clinical criteria, each study patient was as-signed to the highest (most severe) Killip class6 he reachedduring hospitalization. In patients who developed left ventricu-lar thrombi, Killip class was also assessed at the time of the firstechocardiographic detection of thrombus. Four patients hadelectrocardiographic documentation of a prior inferior infarc-tion in addition to the acute anterior infarct. By design, no studypatient was treated with anticoagulants or platelet inhibitors inthe acute phase of infarction or during the follow-up period.
Two-dimensional echocardiography. An Advanced Tech-nology Laboratory (ATL) Mark 300 mechanical sector scannerwith a 3 MHz transducer was used to perform the echocardio-graphic studies. Two-dimensional echocardiographic imageswere recorded on a Panasonic NW-8200 videotape. A Sony U-matic videotape VO-5800 PS was used to review the studies inslow-motion and real-time modes. In each patient, two-dimen-sional echocardiograms were obtained within 24 hr of acuteinfarction, every 24 hr until day 5, every 48 hr until day 15, andevery month for a follow-up of 2 to 11 months (mean 7) in thesurviving patients. A total of 774 two-dimensional echocardio-grams were obtained in the 58 study patients.
Images were obtained in the parasternal long- and short-axisand apical two- and four-chamber views with the use of standardtransducer positions. In most studies, images were also obtainedfrom the apical short-axis view and from sector orientationsintermediate between the two- and four-chamber views. Rou-tinely, while recording from the apical views, depth was adjust-ed to examine the left ventricular apex more thoroughly. Multi-ple gain and reject settings were also used to improve definitionof the epicardium, endocardium, and margins of the thrombus.
Left ventricular thrombus was diagnosed when an echodensemass with defined margins was visualized contiguous to theendocardial surface, and it was clearly identifiable throughoutthe cardiac cycle."- 7, 8 Multiple sector orientations from theapical windows were used to differentiate left ventricularthrombi from muscle trabeculations, chordal structures, andfalse masses that may result from oblique angulation of theultrasound beam through the left ventricular wall.7 Agreementof two observers who were blinded to each other's interpretationwas required before an echocardiogram was considered positivefor left ventricular thrombus. To minimize false-positive diag-noses, studies in which there was observer disagreement thatpersisted after joint review of the study were considered nega-tive for thrombus.9 However, our protocol provided for serialtwo-dimensional echocardiograms obtained at short intervals ineach patient, and the comparison of sequential echocardiogramswas helpful in reducing the number of equivocal studies. Echo-cardiograms were considered equivocal, and therefore negativefor left ventricular thrombus in only two of the 58 studypatients.
The serial echocardiograms obtained in each patient werealso analyzed with regard to shape of the left ventricular throm-bus, and thrombi were classified either as mural, when theywere flat and parallel to the endocardial surface, or protruding,when they were spherical and projected into the left ventricularcavity.7
Left ventricular wall motion analysis. Left ventricular wallmotion was assessed from the combined analysis of the echocar-diographic apical two- and four-chamber views. In these two-dimensional planes, the left ventricle was divided into ninesegments that identified the left ventricular apex, the basal andmidventricular regions of the interventricular septum, and theposterolateral, inferior, and lateral free walls. 10 1 l Wall motionin each segment was classified as normal, hypokinetic, akinetic,dyskinetic, or hyperkinetic on the basis of a visual assessment ofleft ventricular wall movement during systole. A wall motionindex was calculated according to the method of Gibson et al . 1 lin which a numerical score is assigned to each segment on thebasis of the severity of the wall motion abnormalities as follows:normal, 0; hypokinetic, + 1; akinetic, + 2; dyskinetic, + 3; andhyperkinetic, - 1. A left ventricular wall motion index was thencalculated by adding the scores from each segment and dividingby the number of segments analyzed. In each patient, left ven-tricular wall motion was assessed twice, from the echocardio-gram recorded on day 1 of infarction and from the echocardio-gram obtained 30 days after infarction. In patients who diedwithin 30 days of suffering myocardial infarction, the secondassessment of wall motion was made from the last echocardio-gram recorded before death. In the 58 study patients, a total of116 echocardiograms were analyzed to calculate wall motionindex. Of the 1044 possible left ventricular segments, 960(92%) were considered adequate for analysis.
Statistical analysis. Continuous data were expressed asmean + SD. Differences between two means were analyzed bythe unpaired or paired Student's t test, as appropriate. Differ-ences between three means were tested by the one-way analysisof variance. Differences between proportions were analyzed bythe chi-square test.
ResultsIncidence of left ventricular thrombi and prognosis. Left
ventricular thrombi were identified in 24 (41 %) of the58 study patients, and were either confined to the leftventricular apex, or extended from the apex over theinterventricular septum. The thrombus was protrudingin 14 (58%) of the patients, and mural in 10 (42%). Innone of the patients did the thrombus show vigorousmobility within the left ventricular cavity during thecardiac cycle. In each patient, left ventricular throm-bus was associated with adjacent wall motion abnor-malities. Incidence of Killip class III or IV, peak totalLDH values, extent of wall motion abnormalities, andmortality were significantly higher in patients who de-veloped thrombi than in patients who did not (table 1).
However, during the course of the study a relation-ship became evident within the group of patients withthrombi between time of development of thrombus andclinical outcome. Ten (91%) of the 11 patients whodeveloped thrombi within 48 hr of acute infarction diedduring hospitalization (eight patients), or during fol-
Vol. 72, No. 4, October 1985 775
by guest on April 19, 2018
http://circ.ahajournals.org/D
ownloaded from
SPIRITO et al.
TABLE 1Clinical data and wall motion index in patients with and without left ventricular thrombus (LVT) after acute myocardial infarction
Killipclass
Wall motionSex III or IV WindexA Mortality
Age (No. of CK MB LDH (No. ofindeXA
_ (No. of(years) men) (IU/I) (IU/I) (IU/I) patients) Day 1 Day 30 patients)
Patients withLVT (n = 24) 63± 12 21 (88%) 2410+832 275+91 1902+639 10 (42%) 0.46+0.23 0.67±0.34 12 (50%)
Patients withoutLVT (n = 34) 64 ± 13 23 (68%) 1935 886 232 146 1440± 582D 4 (02%)' 0.31 0.26B 0.35± 0.26D 4 (12%c)D
AWall motion index was calculated from the echocardiograms obtained on day and on day 30 of myocardial infarction (or from the lastechocardiogram recorded before death in patients who died within 30 days of infarction).
Bp < .05 compared with patients with LVT; cp < .025 compared with patients with LVT; "p < .01 compared with patients with LVT.
low-up (two patients), while only two (15%) of the 13who developed thrombi after 48 hr of acute infarctiondied (p < .005). We therefore decided to further ana-
lyze our clinical and echocardiographic findings in
these two subgroups of patients (the group with earlyand that with late development of thrombus). Datafrom these two patient subgroups were also comparedwith those obtained in patients who did not develop leftventricular thrombi.
Peak CK and CK-MB values did not differ signifi-cantly among the three study groups. Peak total LDHvalues were significantly higher in patients who devel-oped a thrombus early during myocardial infarctionthan in patients who did not develop a thrombus, whilein patients with late-developing thrombus this variabledid not differ significantly from that in the other twogroups (table 2). Incidence of Killip classes III or IVand mortality were also significantly higher in patientswith early-developing thrombi than in patients withoutthrombi, while in patients who developed thrombi late,these variables did not differ significantly from thosein patients without thrombi (table 2; figures 1 and 2).
Wall motion indexes calculated from the echocar-diograms obtained on day 1 and day 30 of infarction(or from the last echocardiogram obtained before death
in patients who died within 30 days of infarction) were
significantly higher (indicating more extensive wallmotion abnormalities) in patients who developed a
thrombus early than in patients without thrombus (ta-ble 3). In patients with late thrombus formation, wallmotion index obtained on day 1 of infarction was not
significantly different from that in the other twogroups; wall motion index obtained on day 30 was
significantly lower than that in patients with early-developing thrombi, but higher than that in patientswithout thrombi.
In addition, wall motion indexes obtained at thesetwo times during the course of infarction were com-
pared within each group of patients. In patients whodeveloped an early thrombus, left ventricular wall mo-
tion was significantly more compromised at the time ofits second assessment than at the first assessment,while in patients who developed a thrombus late and inpatients without thrombi, wall motion indexes did notdiffer significantly at the first and second assessments(table 3).We also analyzed the relationship between patient
clinical condition (Killip class) at the time when a
thrombus was first detected and subsequent patientclinical course. Of the 11 patients who developed
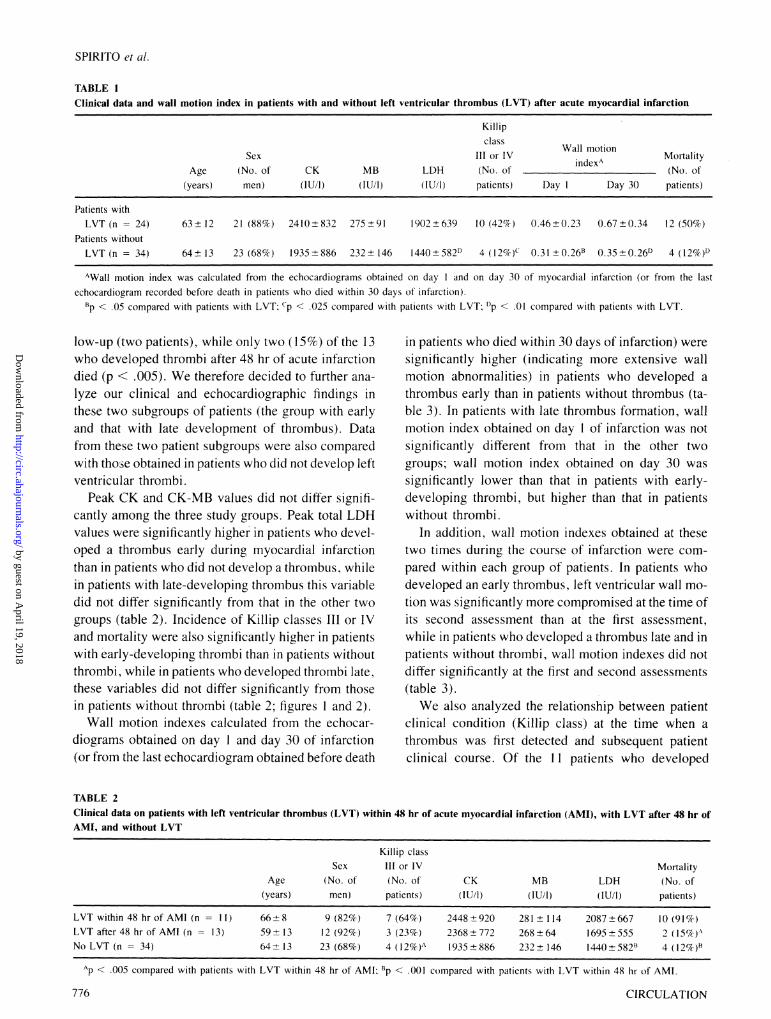
TABLE 2Clinical data on patients with left ventricular thrombus (LVT) within 48 hr of acute myocardial infarction (AMI), with LVT after 48 hr ofAMI, and without LVT
Killip classSex III or IV Mortality
Age (No. of (No. of CK MB LDH (No. of(years) men) patients) (IU/I) (IU/l) (IU/l) patients)
LVT within 48 hr of AMI (n = 11) 66+8 9 (82%) 7 (64%) 2448+920 281±+ 114 2087+667 10 (91%)LVT after 48 hr of AMI (n 13) 59 13 12 (92%) 3 (23%) 2368+772 268+64 1695+555 2 (15%).No LVT (n = 34) 64 13 23 (68%) 4 (12% )A 1935+886 232 146 1440±582B 4 (12%)B
Ap < .005 compared with patients with LVT within 48 hr of AMI; Bp < .001 coimpared with patients with LVT within 48 hr of AMI.
776 CIRCULATION
by guest on April 19, 2018
http://circ.ahajournals.org/D
ownloaded from
PATHOPHYSIOLOGY AND NATURAL HISTORY-MYOCARDIAL INFARCTION
80 r* p< 0.005r ~ N.S. 1 N.S.-----
70
C~
In
c
CD
CL
4._0
(7111
60 F
50 F
40
30 F
20
10 F
0
LVT within LVT after No LVT48 hours 48 hoursof AMI of AMI
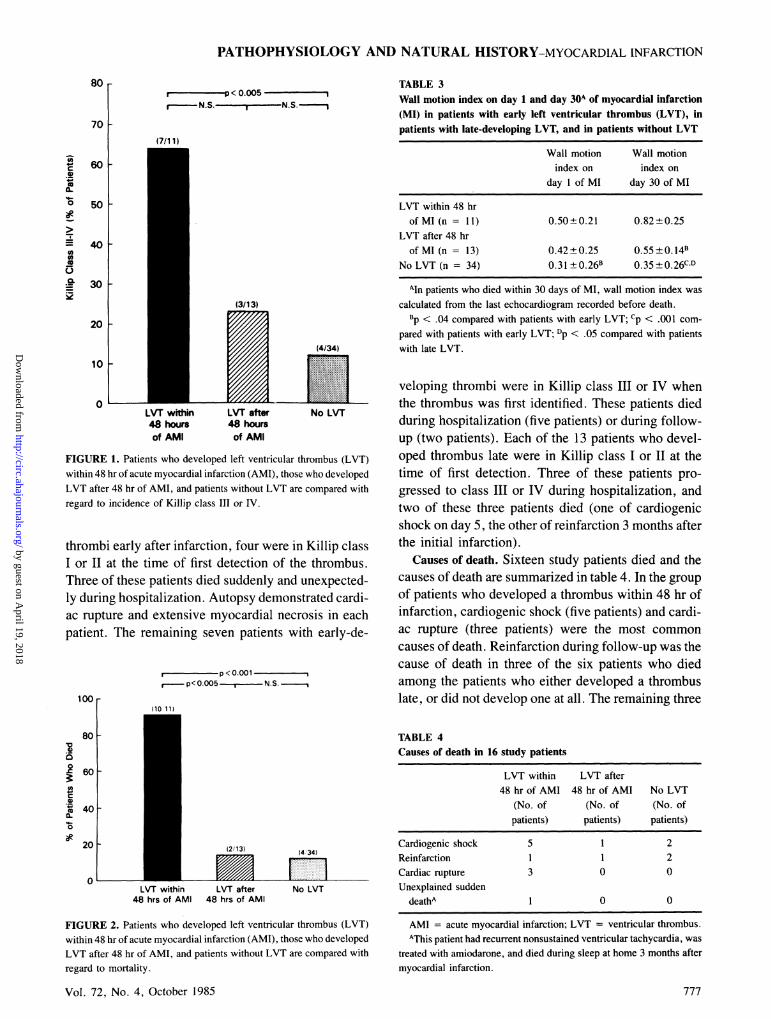
FIGURE 1. Patients who developed left ventricular thrombus (LVT)within 48 hr of acute myocardial infarction (AMI), those who developedLVT after 48 hr of AMI, and patients without LVT are compared withregard to incidence of Killip class Ill or IV.
thrombi early after infarction, four were in Killip classI or II at the time of first detection of the thrombus.Three of these patients died suddenly and unexpected-ly during hospitalization. Autopsy demonstrated cardi-ac rupture and extensive myocardial necrosis in eachpatient. The remaining seven patients with early-de-
,p < 0.001p< 0.005 , N.S.
100
80
0
0.C 60
o
0
20
/~~~~ ~ ~~~~~2/13)(4. 34)
LVT within LVT after No LVT48 hrs of AMI 48 hrs of AMI
FIGURE 2. Patients who developed left ventricular thrombus (LVT)within 48 hr of acute myocardial infarction (AMI), those who developedLVT after 48 hr of AMI, and patients without LVT are compared with
regard to mortality.
Vol. 72, No. 4, October 1985
TABLE 3Wall motion index on day 1 and day 30A of myocardial infarction(MI) in patients with early left ventricular thrombus (LVT), inpatients with late-developing LVT, and in patients without LVT
Wall motion Wall motionindex on index on
day 1 of MI day 30 of MI
LVT within 48 hrof MI (n = 1 1) 0.50±0.21 0.82± 0.25
LVT after 48 hrof MI (n = 13) 0.42+0.25 0.55±0.141
No LVT (n = 34) 0.31 ±0.26B 0.35-0.26CD
Aln patients who died within 30 days of MI, wall motion index wascalculated from the last echocardiogram recorded before death.
Bp < .04 compared with patients with early LVT; cp < .001 com-pared with patients with early LVT; Dp < .05 compared with patientswith late LVT.
veloping thrombi were in Killip class III or IV whenthe thrombus was first identified. These patients diedduring hospitalization (five patients) or during follow-up (two patients). Each of the 13 patients who devel-oped thrombus late were in Killip class I or II at thetime of first detection. Three of these patients pro-gressed to class III or IV during hospitalization, andtwo of these three patients died (one of cardiogenicshock on day 5, the other of reinfarction 3 months afterthe initial infarction).
Causes of death. Sixteen study patients died and thecauses of death are summarized in table 4. In the groupof patients who developed a thrombus within 48 hr ofinfarction, cardiogenic shock (five patients) and cardi-ac rupture (three patients) were the most commoncauses of death. Reinfarction during follow-up was thecause of death in three of the six patients who diedamong the patients who either developed a thrombuslate, or did not develop one at all. The remaining three
TABLE 4Causes of death in 16 study patients
LVT within LVT after48 hr of AMI 48 hr of AMI No LVT
(No. of (No. of (No. ofpatients) patients) patients)
Cardiogenic shock 5 1 2Reinfarction 1 1 2Cardiac rupture 3 0 0Unexplained sudden
deathA 1 0 0
AMI = acute myocardial infarction; LVT = ventricular thrombus.AThis patient had recurrent nonsustained ventricular tachycardia, was
treated with amiodarone, and died during sleep at home 3 months aftermyocardial infarction.
777
by guest on April 19, 2018
http://circ.ahajournals.org/D
ownloaded from
SPIRITO et al.
patients in this group died of cardiogenic shock (twodied within 24 hr of acute infarction and the third diedon day 5).
Autopsy. Autopsies were performed in 13 of the 16study patients who died. -In 12 of the 13 patients,autopsy findings confirmed the echocardiographic in-terpretation (positive for left ventricular thrombus innine patients and negative in three). In one patient,autopsy identified a thrombus that had not been detect-ed by echocardiography.
In each patient, the location of the thrombus withinthe left ventricular cavity as verified at autopsy was inagreement with that predicted by echocardiography.
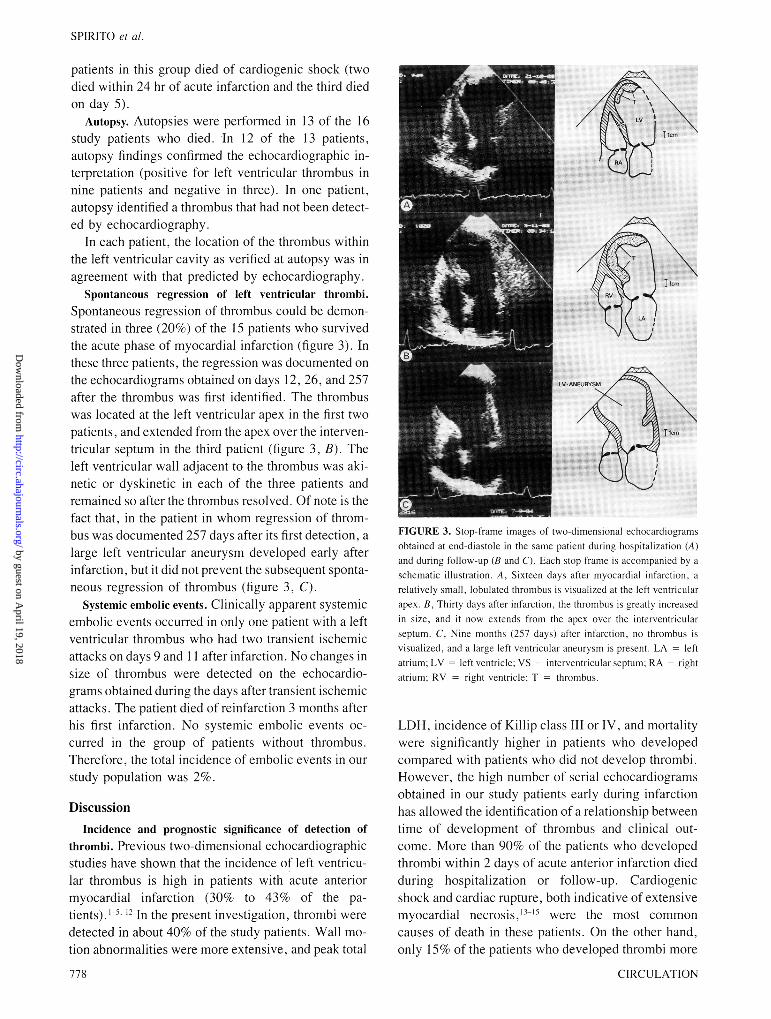
Spontaneous regression of left ventricular thrombi.Spontaneous regression of thrombus could be demon-strated in three (20%) of the 15 patients who survivedthe acute phase of myocardial infarction (figure 3). Inthese three patients, the regression was documented onthe echocardiograms obtained on days 12, 26, and 257after the thrombus was first identified. The thrombuswas located at the left ventricular apex in the first twopatients, and extended from the apex over the interven-tricular septum in the third patient (figure 3, B). Theleft ventricular wall adjacent to the thrombus was aki-netic or dyskinetic in each of the three patients andremained so after the thrombus resolved. Of note is thefact that, in the patient in whom regression of throm-bus was documented 257 days after its first detection, alarge left ventricular aneurysm developed early afterinfarction, but it did not prevent the subsequent sponta-neous regression of thrombus (figure 3, C).
Systemic embolic events. Clinically apparent systemicembolic events occurred in only one patient with a leftventricular thrombus who had two transient ischemicattacks on days 9 and 1 1 after infarction. No changes insize of thrombus were detected on the echocardio-grams obtained during the days after transient ischemicattacks. The patient died of reinfarction 3 months afterhis first infarction. No systemic embolic events oc-curred in the group of patients without thrombus.Therefore, the total incidence of embolic events in ourstudy population was 2%.
DiscussionIncidence and prognostic significance of detection of
thrombi. Previous two-dimensional echocardiographicstudies have shown that the incidence of left ventricu-lar thrombus is high in patients with acute anteriormyocardial infarction (30% to 43% of the pa-tients).'-', 12In the present investigation, thrombi weredetected in about 40% of the study patients. Wall mo-tion abnormalities were more extensive, and peak total
778
FIGURE 3. Stop frame images of two-dimensional echocardiogramsobtained at end-diastole in the same patient during hospitalization (A)and during follow-up (B and C). Each stop fiame is accompanied by aschematic illustration. A. Sixteen days after myocardial inlfai-ction. arelatively small, lobulated thrombus is visualized at the left ventricularapex. B, Thirty days after infarctioni, the thrombus is greatly increasedin size, and it now extends from the apex over the interventricularseptum. C. Nine months (257 days) after infarction, no thrombus isvisualized. and a large left ventricular aneurysm is present. LA leftatrium; LV left ventricle; VS = interventrictular septuLmn; RA rightatrium; RV right ventricle; T = thronmbus,
LDH, incidence of Killip class III or IV, and mortalitywere significantly higher in patients who developedcompared with patients who did not develop thrombi.However, the high number of serial echocardiogramsobtained in our study patients early during infarctionhas allowed the identification of a relationship betweentime of development of thrombus and clinical out-come. More than 90% of the patients who developedthrombi within 2 days of acute anterior infarction diedduring hospitalization or follow-up. Cardiogenicshock and cardiac rupture, both indicative of extensivemyocardial necrosis, --," were the most commoncauses of death in these patients. On the other hand,only 15% of the patients who developed thrombi more
CIRCULATION
by guest on April 19, 2018
http://circ.ahajournals.org/D
ownloaded from

PATHOPHYSIOLOGY AND NATURAL HISTORY-MYOCARDIAL INFARCTION
than 2 days after acute infarction died, and their mor-tality rate was not different from that of patients whodid not develop thrombi. Furthermore, the analysis ofclinical variables and left ventricular contractility inthese patient subgroups substantiated the conclusionthat the time of development of thrombus after acutemyocardial infarction identifies subsets of patientswith different clinical profiles and outcome. For exam-ple, in the group of patients who developed a thrombusearly, incidence of Killip class III or IV, peak totalLDH, and extent of wall motion abnormalities weresignificantly higher compared with those in patientswho did not develop a thrombus. On the other hand,patients who developed a thrombus late did not differsignificantly from patients without thrombi with re-gard to Killip class, enzyme values, and left ventricu-lar wall motion (assessed in the acute phase of infarc-tion). These findings demonstrate that development ofleft ventricular thrombus within 48 hr of myocardialinfarction occurs in patients with the most exten-sive infarcts and is associated with particularly highmortality.
Although the majority of patients with acute myo-cardial infarction and large infarcts usually presentwith or progress to Killip class III or IV, about 15% ofpatients with extensive myocardial damage and highpulmonary pressures are not identified on the basis ofclinical evaluation, but only by means of invasivehemodynamic measurements. 16 Four of our study pa-tients who developed left ventricular thrombus within48 hr of myocardial infarction had been assigned byclinical criteria to Killip class I or IL at the time ofadmission. Of note is the fact that three of these fourpatients died suddenly and unexpectedly during hospi-talization. Autopsy demonstrated cardiac rupture andextensive myocardial necrosis in each of these threepatients. This finding would suggest that echocardio-graphic detection of early formation of thrombus dur-ing acute anterior infarction may identify a subset ofpatients whose poor prognosis would not be predictedon the basis of their clinical presentation.
Spontaneous regression of thrombus. Spontaneous re-gression of left ventricular thrombus in patients withmyocardial infarction who are not treated with anti-coagulants has been previously reported in three pa-tients.5 17 In our study, thrombus resolved in three ofthe 15 patients (20%) who survived the acute phase ofinfarction. The period of time between formation ofthe thrombus and its spontaneous regression was great-ly variable in these three patients, ranging from a mini-mum of 12 days to a maximum of 9 months. The leftventricular segments contiguous to the thrombus were
Vol. 72, No. 4, October 1985
akinetic or dyskinetic in each patient and remained soafter the thrombus resolved. Regression of thrombuswas not associated with clinically evident embolicevents in any of the three patients. During follow-up,one of these patients developed a large left ventricularaneurysm associated with poor global left ventricularcontractility and, interestingly, the presence of thislarge aneurysm did not prevent subsequent spontane-ous regression of thrombus (figure 3).
Incidence of systemic embolic events. The incidence ofclinically apparent systemic embolic events in patientswith myocardial infarction and echocardiographic doc-umentation of left ventricular thrombus is controver-sial, and the available data are from small numbers ofpatients, the majority of whom were treated with anti-coagulants. Asinger et al.' reported no evidence ofsystemic embolization during a mean follow-up of 9months in nine patients with anterior myocardial in-farction and left ventricular thrombus, seven of whomwere treated with anticoagulants. In a preliminarystudy, Kothari et al.'2 reported one embolic event in 1 1patients who received anticoagulants and one embolicevent in eight patients not treated with anticoagulants;no data on follow-up were provided. In contrast, Keat-ing et al.3 reported embolic events in six of sevenpatients who were not treated with anticoagulants(mean follow-up 1 month) and no embolic events innine patients on anticoagulants (mean follow-up 1 1months). More recently, Weinreich et al.5 reportedsystemic embolization in seven of 18 patients who didnot receive anticoagulants and in none of 25 patientstreated with anticoagulants (minimum follow-up 6months).None of our 58 study patients was treated with anti-
coagulants or platelet inhibitors during the acute phaseof infarction or follow-up. The incidence of clinicallyapparent systemic embolic events was low, with onlyone patient with left ventricular thrombus having tran-sient ischemic attacks. No embolic events occurred inthe remaining patients with or without thrombus dur-ing a mean follow-up of 7 months. Therefore, in ourstudy population the total incidence of clinically appar-ent systemic embolic events was 2%. While this inci-dence is in agreement with the 0.6% to 6.4% reportedin several large series of patients with myocardial in-farction,'820 it contrasts with the substantially higherincidence of systemic embolization identified by Keat-ing et al.', and Weinreich et al.5 in study populationssimilar to ours. We do not have a definite explanationfor these conflicting findings. Our study patients werea consecutive series, and no patient was treated witheither anticoagulants or platelet inhibitors; therefore,
779
by guest on April 19, 2018
http://circ.ahajournals.org/D
ownloaded from

SPIRITO et al.
our results should not be importantly affected by selec-tion factors. Several investigators have described thevigorous mobility of left ventricular thrombi within theleft ventricular cavity as an echocardiographic featureassociated with embolization.2'-24 None of the thrombiidentified in our study patients showed vigorous mo-bility during the cardiac cycle. This morphologic fea-ture could explain, in part, the relatively low incidenceof embolic events in our population. However, largerprospective studies are needed to define the clinicaland echocardiographic profile of patients with myocar-dial infarction and left ventricular thrombus who arepotentially at higher risk of systemic embolization andwho may benefit from treatment with anticoagulants.
In conclusion, our findings indicate that develop-ment of left ventricular thrombus within 2 days ofacute anterior myocardial infarction occurs in patientswith the most extensive infarcts and is predictive ofhigh mortality. Our study also demonstrates that spon-taneous regression of thrombus may occur in patientswith myocardial infarction, despite the persistence ofsevere wall motion abnormalities. Finally, in our studypatients with left ventricular thrombi, none of whomwere treated with anticoagulants or platelet inhibitors,the incidence of clinically apparent systemic embolicevents was low.
References1. Asinger RW, Mikell FL, Elsperger J, Hodges M: Incidence of left
ventricular thrombosis after acute transmural myocardial infarc-tion. N Engl J Med 305: 297, 1981
2. Friedman MJ, Caiison K, Marcus FI, Woolfenden JM: Clinicalcorrelations in patients with acute myocardial infarction and leftventricular thrombus detected by two-dimensional echocardiog-raphy. Am J Med 72: 894, 1982
3. Keating EC, Gross SA, Schlamowitz RA, Glassman J, Mazur JH,Pitt WA, Miller D: Mural thrombi in myocardial infarctions. Pro-spective evaluation by two-dimensional echocardiography. Am JMed 74: 989, 1983
4. Visser CA, Kan G, Lie KI, Durrer D: Left ventricular thrombusfollowing acute myocardial infarction: a prospective serial echocar-diographic study of 96 patients. Eur J Cardiol 4: 333, 1983
5. Weinreich DJ, Burke JF, Pauletto FJ: Left ventricular muralthrombi complicating acute myocardial infarction. Long-term fol-low-up with serial echocardiography. Ann Intern Med 100: 789,1984
6. Killip T, Kimball JT: Treatment of myocardial infarction in a
coronary care unit. A two year experience with 250 patients. Am JCardiol 20: 457, 1967
7. Asinger RW, Mikell FL, Sharma B, Hodges M: Observations ondetecting left ventricular thrombus with two-dimensional echocar-diography: emphasis on avoidance of false positive diagnoses. AmJ Cardiol 47: 145, 1981
8. Mikell FL, Asinger RW, Elsperger JK, Anderson RW, Hodges M:Regional stasis of blood in the dysfunctional left ventricle: echocar-diographic detection and differentiation from early thrombosis.Circulation 66: 755, 1982
9. Stratton JR, Lighty GW Jr, Pearlman AS, Ritchie JL: Detection ofleft ventricular thrombus by two-dimensional echocardiography:sensitivity, specificity, and causes of uncertainty. Circulation 66:156, 1982
10. Heger JJ, Weyman AE, Wann SL, Rogers EW, Dillon JC, Feigen-baum H: Cross-sectional echocardiographic analysis of the extentof left ventricular asynergy in acute myocardial infarction. Circula-tion 61: 1113, 1980
11. Gibson RS, Bishop HL, Stamm RB, Crampton RS, Beller GA,Martin RP: Value of early two-dimensional echocardiography inpatients with acute myocardial infarction. Am J Cardiol 49: 1 1 10,1982
12. Kothari AJ, Paczkowski K, Baker KM, Schreck SC, Butcher RJ,Kline DM, Menapace FJ: Ventricular thrombi in acute myocardialinfarction: incidence, complications, and effects of anticoagula-tion. J Am Coll Cardiol 3: 601, 1984 (abst)
13. Page DL, Caulfield JB, Kastor JA, DeSanctis RW, Sanders CA:Myocardial changes associated with cardiogenic shock. N Engl JMed 285: 133, 1971
14. Gutovitz AL, Sobel BE, Roberts R: Progressive nature of myocar-dial injury in selected patients with cardiogenic shock. Am J Car-diol 41: 469, 1978
15. London RE, London SB: Rupture of the heart. A critical analysis of47 consecutive autopsy cases. Circulation 31: 202, 1965
16. Forrester JS, Diamond G, Swan HJC: Bedside diagnosis of latentcardiac complications in acutely ill patients. JAMA 30: 338, 1972
17. Tramarin R, Pozzoli M, Febo 0, Opasich C, Cobelli F, SpecchiaG: Echocardiographic assessment of therapy efficacy in left ven-tricular thrombosis post myocardial infarction. Circulation 68(suppl III): 111-331, 1983 (abst)
18. Wright IS, Marple CD, Beck DF: Report of the committee for theevaluation of anticoagulants in the treatment of coronary thrombo-sis with myocardial infarction. Am Heart J 36: 801, 1948
19. Hilden T, Raaschov F, Iversen K, Schwartz M: Anticoagulants inacute myocardial infarction. Lancet 2: 327, 1961
20. Veterans Administration Hospital Investigators: Anticoagulants inacute myocardial infarction: results of a cooperative clinical trial.JAMA 225: 724, 1973
21. DeMaria AN, Bommer W, Neumann A, Grehl T, Weinart L,DeNardo S, Amsterdam EA, Mason DT: Left ventricular thrombiidentified by cross-sectional echocardiography. Ann Intern Med90: 14, 1979
22. Nagvi N, Popp RL, Coltart DJ: Diagnosis of left ventricular throm-bosis by two-dimensional echocardiography. Eur J Cardiol 11:235, 1980
23. Visser CA, Kan G, Meltzer RS, Roelandt J, Durrer D: Two-dimen-sional echocardiographic features of left ventricular thrombi caus-ing peripheral embolization. Circulation 68(suppl III): 111-111,1983 (abst)
24. Haugland MJ, Asinger RW, Mikell FL, Elsperger J, Hodges M:Embolic potential of left ventricular thrombi detected by two-di-mensional echocardiography. Circulation 70: 588, 1984
CIRCULATION780
by guest on April 19, 2018
http://circ.ahajournals.org/D
ownloaded from

P Spirito, P Bellotti, F Chiarella, S Domenicucci, A Sementa and C Vecchioacute anterior myocardial infarction: a two-dimensional echocardiographic study.
Prognostic significance and natural history of left ventricular thrombi in patients with
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1985 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.72.4.774
1985;72:774-780Circulation.
http://circ.ahajournals.org/content/72/4/774the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on April 19, 2018
http://circ.ahajournals.org/D
ownloaded from