pathophysiology and ecg manifestations of coronary heart...
TRANSCRIPT
Pipin Ardhianto
Cardiovascular Department
Medical Faculty of Diponegoro University
Pathophysiology and ECG ManifestationsOf
Coronary Heart Disease

Definition of Acute Coronary
Syndrome
A syndrome largely due to coronary atheroclerosis
plaque rupture or erosion, which is further subdivided
into presentations with and without ST-segment
elevation on the ECG.
Antman, E M. 2004

Causes of ACS
Atherosclerosis Cause
> 95% ACS because of disruption of plaque
Platelet agregation
Intracoronary thrombus
Non Atherosclerosis Cause
Vasculitis syndrome
Coronary emboli (IE, prosthetic valve)
Congenital anomali of coronary artery
Coronary trauma or aneurysm
Spasm
Increased blood viscosity
Increased myocardial demand
Hurst, 2011

4
Heart attack, Stroke etc
“STRESS“ testing only detects THIS
Usually begin in later childhood

Pathophysiology of Atheroscelrotic (1)
Hurst, 2011

Pathophysiology of Atheroscelrotic (2)
Zubrycki, M. J Physiol Pharmacol. 2014

When will the plaque be ruptured?
Vulnerable plaque:
Plaques with large lipid core
Thin fibrous cap covering lipid core
High density of macrophage, matrix metalloproteinase and inflammatory cell
Holroyd, 2003

8Stable VS Unstable Plaque


APPROACH
Identifying those with chest pain suggestive of
IHD/ACS.
Thorough history required:
Character of pain
Onset and duration
Location and radiation
Aggravating and relieving factors
Autonomic symptoms
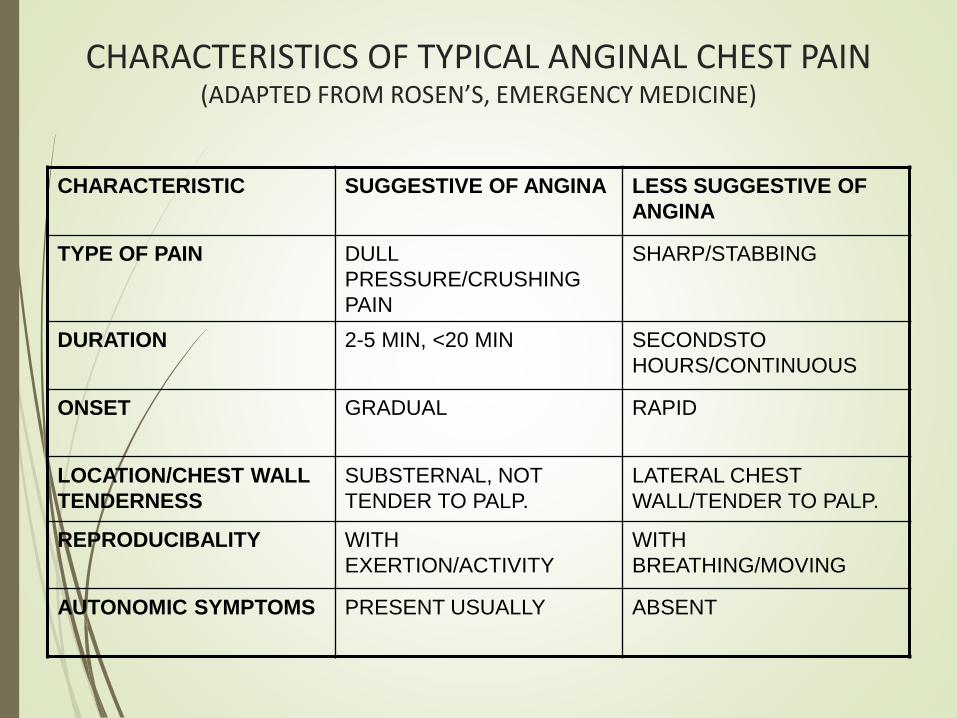
CHARACTERISTICS OF TYPICAL ANGINAL CHEST PAIN (ADAPTED FROM ROSEN’S, EMERGENCY MEDICINE)
CHARACTERISTIC SUGGESTIVE OF ANGINA LESS SUGGESTIVE OF
ANGINA
TYPE OF PAIN DULL
PRESSURE/CRUSHING
PAIN
SHARP/STABBING
DURATION 2-5 MIN, <20 MIN SECONDSTO
HOURS/CONTINUOUS
ONSET GRADUAL RAPID
LOCATION/CHEST WALL
TENDERNESS
SUBSTERNAL, NOT
TENDER TO PALP.
LATERAL CHEST
WALL/TENDER TO PALP.
REPRODUCIBALITY WITH
EXERTION/ACTIVITY
WITH
BREATHING/MOVING
AUTONOMIC SYMPTOMS PRESENT USUALLY ABSENT

Wu Et al. J of Am Physycian. 2009
How To Deal With?

ECG Manifestation of ACS

Subendocardial ischemia : ST depression (horizontal/downsloping), T
wave inversion
Transmural ischemia : ST elevation
ECG abnormalities of ischemia
“Diastolic Injury Current Theory” “Systolic Injury Current Theory”
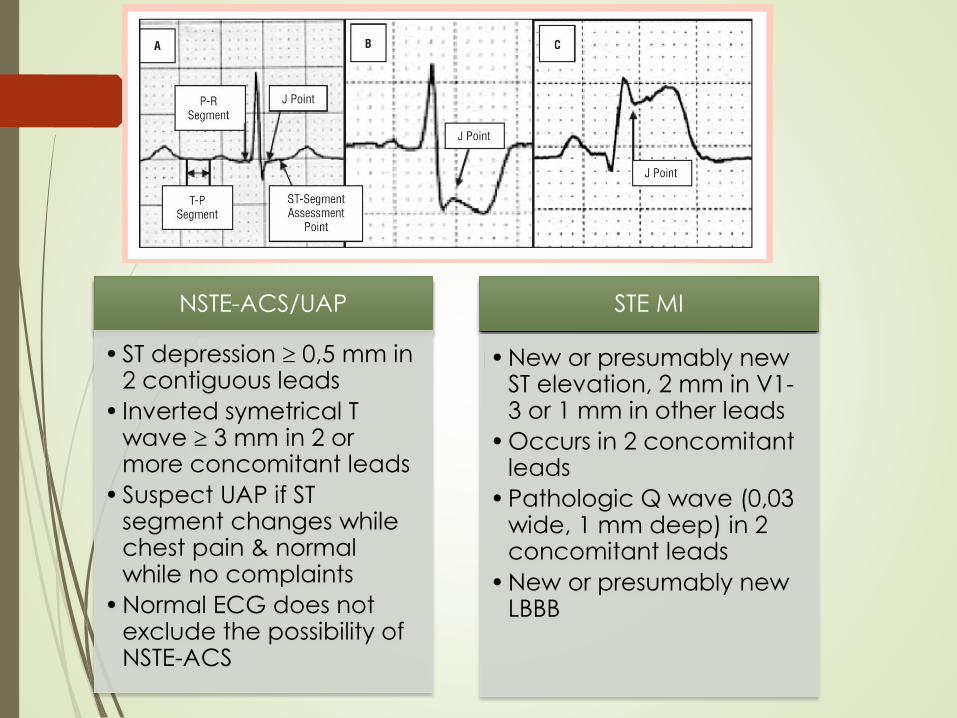
NSTE-ACS/UAP
•ST depression 0,5 mm in 2 contiguous leads
• Inverted symetrical T wave 3 mm in 2 or more concomitant leads
•Suspect UAP if ST segment changes while chest pain & normal while no complaints
•Normal ECG does not exclude the possibility of NSTE-ACS
STE MI
•New or presumably new ST elevation, 2 mm in V1-3 or 1 mm in other leads
•Occurs in 2 concomitant leads
•Pathologic Q wave (0,03 wide, 1 mm deep) in 2 concomitant leads
•New or presumably new LBBB

A = Normal
B = Acute
ST elevation/tall T
C = Hours
ST elevation
R wave, Q wave begins
D = Day 1-2
T wave Biphasic
Deeper Q wave
E = Days later
ST normalizes
T wave inverted
F = Weeks later
ST & T normal
Q wave persists
ECG evolution of Acute STEMI
Pathophysiologic of Heart Disease: Acute
Coronary Syndromes, Lilly, 4th ed, 2007


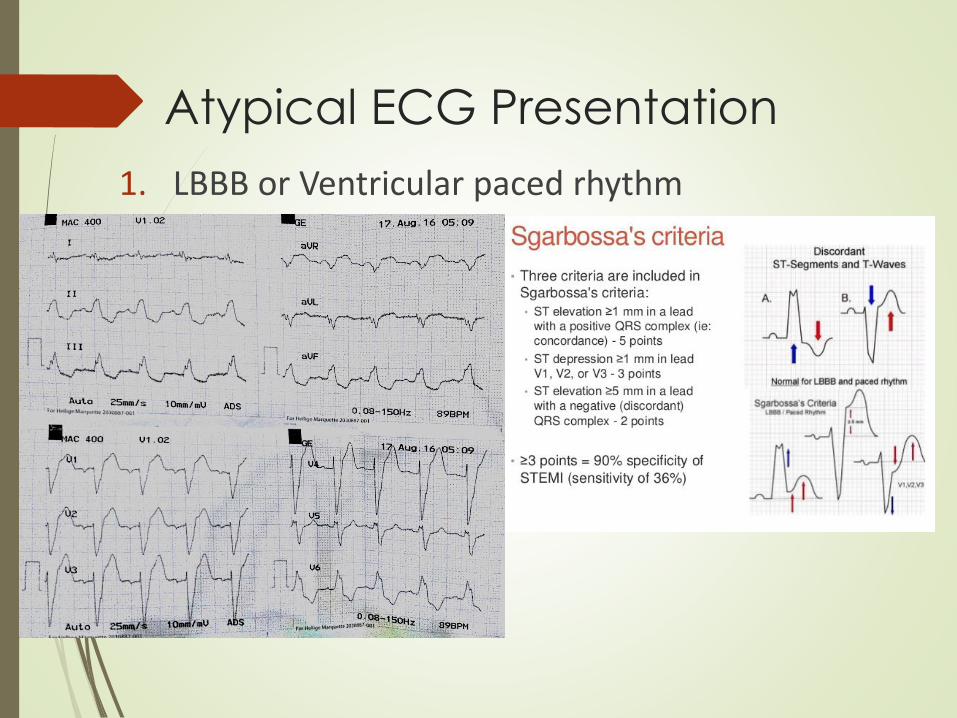
Atypical ECG Presentation
1. LBBB or Ventricular paced rhythm

Atypical ECG Presentation
2. Isolated posterior myocardial infarction
Infarct in Infero-basal area
Often correspondent to LCx territory
Isolated ST depression in V1 – V3
Use additionl posterior chest lead to confirm posterior infart ( ST elevation > 0.05mm )

Atypical ECG Presentation
3. Left Main Coronary Oclusion
ST segment elevation in lead aVR or V1
St depression in eight or more other leads
Accompanied with hemodynamics compromise
CARDIAC
CATHETHERIZATOIN

PREVENSI KARDIOVASKULAR
A. ASPIRIN dan ANTI KOAGULAN
Aspirin diberikan secara rutin dan terus menerus pada pasien pasca serangan jantung.
Bersama dengan nitrat merupakan obat yang penting bagi kegawat daruratan PJK
Bertujuan sebagai anti beku darah
Dosis : 80 - 320 mg

B=BLOOD PRESSURE & BODY WEIGHT
Target tekanan darah < 140/90 mmHg• mengubah pola hidup• terapi obat
Kelebihan berat badan dan obesitas
• Kelebihan berat badan ( BMI > 25 kg/m2 ), obesitas ( BMI > 30 kg/m2 ) mengurangi berat badan dengan diet yang benardan meningkatkan aktivitas fisik
• Penurunan berat badanmenurunkan tekanan darah, kadarkolesterol, glukosa darah
• Lingkar pinggang : indeks klinis obesitas dan pantauanpenurunan BB Lingkar pinggang pria > 94 cm dan wanita > 80 cm merupakanindikasi penurunan BB

C= CHOLESTEROL and CIGARETES CESSATION
• Target kadar total kolesterol < 190 mg/dL dan kolesterolLDL < 100 mg/dL
• Kadar kolesterol HDL dan trigliserida tidak sebagai target terapi
• HDL < 40 mg/dL, Trigliserida > 180 mg/dL meningkatkanrisiko
• Mengubah pola hidup• terapi obat : HMG Co A reductase inhibitor (statin)

D = DIET and DIABETES
• Memilih makanan sehat1. mengurangi lemak total hingga < 30 % dari total asupan energi,
asam lemak jenuh < 1/3 dari total lemak dan kolesterol < 300 mg
per hari
2. mengganti asam lemak jenuh dengan lemak tidak jenuh dari
sayuran dan makanan laut
3. meningkatkan asupan buah, sereal dan sayuran
4. mengurangi total asupan kalori bila berat badan perlu
diturunkan
5. mengurangi asupan garam dan alkohol bila tekanan darah
tinggi
• Glukosa darahTarget kontrol glukosa darah pada diabetes yakni :
kadar glukosa darah puasa 91 – 120 mg/dL,
post prandial 136 – 160 mg/dL,
HbA1C < 7 % dan menghidari hipoglikemia

E. EDUCATION and EXERCISEEDUCATION
- Pencegahan Primersasaran : kelompok resiko tinggi
tujuan : mencegah/mengurangi kejadian PJK
- Pencegahan SekunderSasaran : kelompok pasien PJK
Tujuan : mencegah komplikasi
- Pencegahan TersierSasaran : kelompok pasien PJK dengan komplikasi
Tujuan : mencegah mortalitas dan morbiditas
EXERCISE
Olahraga aerobik minimal 30 menit yang dilakukan minimal 5 x / minggu
27

F = FUNHindari stress berlebihan, perbanyak aktivitas rekreasi yang menyenangkan
G = Genetic conselingTerutama terhadap pasien dengan keluarga penyakit jantung prematur.
28

Framingham Heart StudyMurabito et al Circulation 1993; 88: 2548-54
Patients (%)
Women
0
Men
20 40 60
62 %
46 %
First clinical presentation of coronary artery disease is frequently an
acute coronary syndrome. i.e. can be the last …
Clinical presentation of coronary disease
Courtasy of John Deanfield

Take Home Messages
ACS largely due to atherosclerosis plaque rupture or erosion
Atherosclerosis plaque last a lifetime
ECG is the mainstay to determine ACS
Pay attention to normal ECG but relevant symptom or Atypical ECG changes on admission.
Serial ECG may help
Prevention is all the core
30