pathology of gastrointestinal system part i
TRANSCRIPT

PATHOLOGY OFGASTROINTESTINAL SYSTEM
PART I
Peerayut Sitthichaiyakul, M.D.

Content
• Pathology of Oral Cavity• Pathology of Salivary glands• Pathology of Esophgus• Pathology of Stomach

ORAL CAVITYORAL CAVITY
• Inflammatory and Reactive lesions
• Infections
• Oral Manifestations of Systemic Disease
• Tumor and precancerous lesion

Inflammatory/Reactive Lesions
• Fibrous proliferative lesions– Irritation Fibroma
– Pyogenic Granuloma
• Aphthous Ulcer (Canker Sores)– Mononulcear infiltration




Infections
• Herpes Simplex Virus Infections– Acute Herpetic Gingivostomatitis
– Recurrent Herpetic Stomatitis
– HSV‐1, HSV‐2
– Tzanck Test
– Intranuclear Inclusions
– Multinucleated giant cells
• Oral candidiasis (Trush)


Oral Manifestation of Systemic Diseases
• Scarlet fever – Rasberry tongue
– Strawberry tongue
• Measles– Koplik spot
• Infectious Mononucleosis– Pharyngitis and Tonsillitis

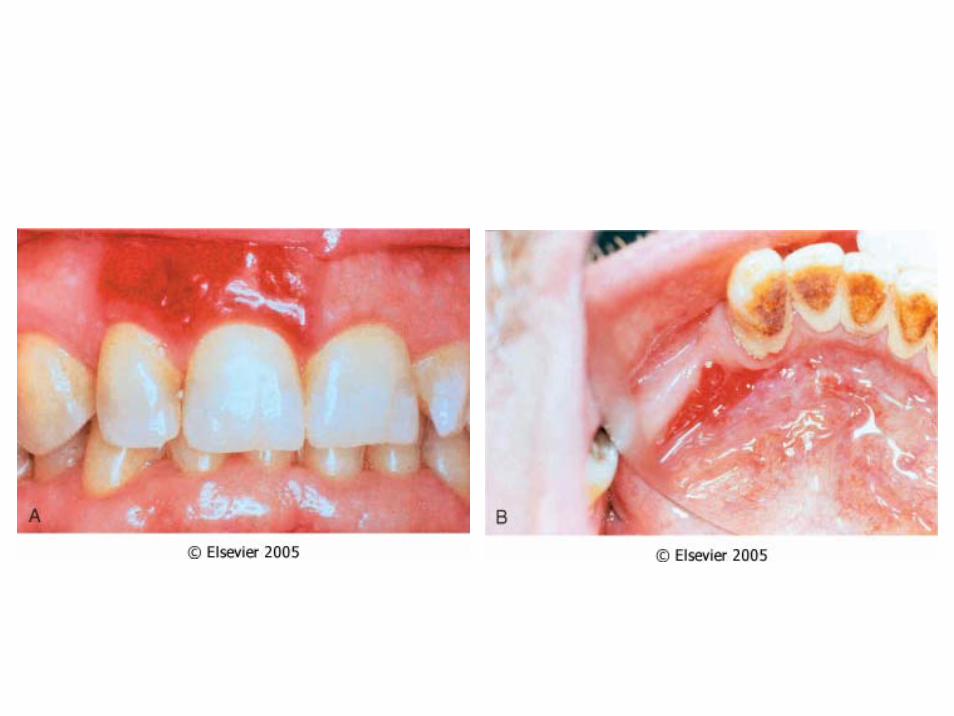
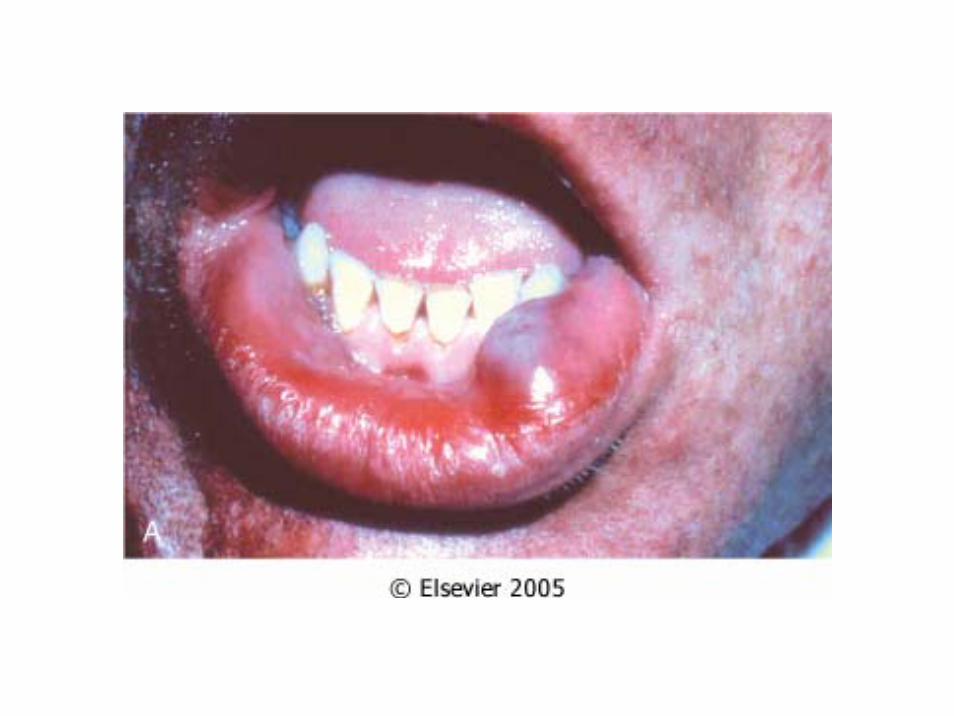
• HIV/AIDS– Oral infection
– Kaposi sarcoma
– Hairy Leukoplakia
• Dermatologic Conditions
• Hematologic Disorders– Pancytopenia
– Leukemia

• Melanotic Pigmentation– Addition disease
– Hemochromatosis
– Peutz‐Jegher syndrome
• Pregnancy– Pyogenic granuloma (pregnancy tumor)

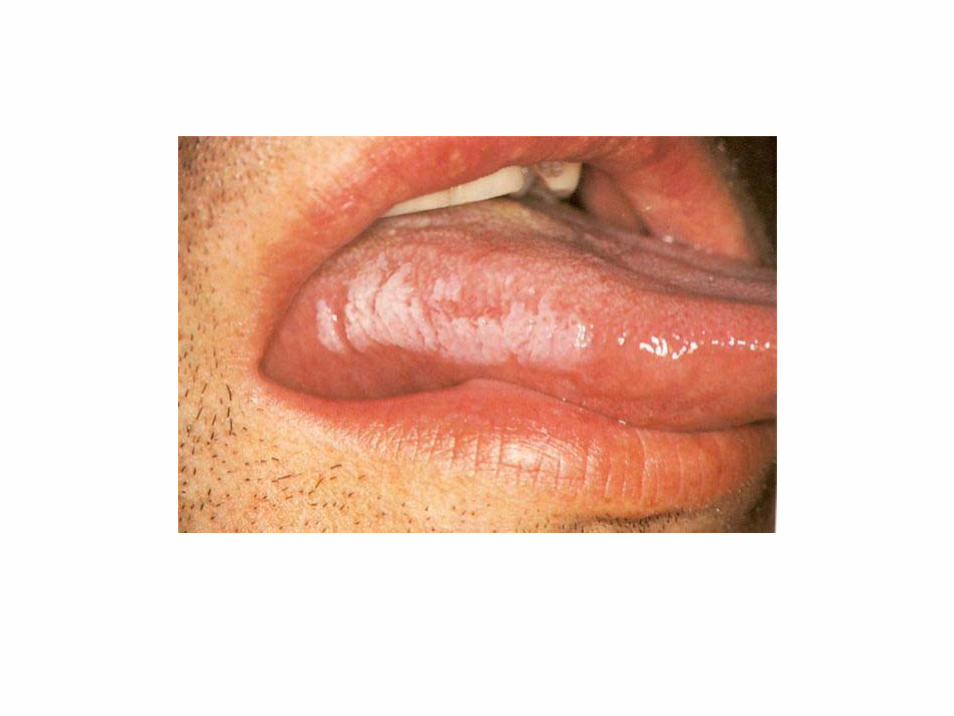
• Hairy Leukoplakia– 80% HIV infection
– White, patches, hyperkeratotic thickenings
– Lateral border of tongue
– EBV infection

Tumor and Precancerous Lesion
• Leukoplakia and Erythroplakia– Leukoplakia: white patches or plaques that cannot be scraped off and cannot be characterized clinically or pathologically as other diseases
– Erythroplakia: red, velvety, eroded area
– Speckled leukoerythroplakia
– Multifactorial, use of tobacco


• Squamous cell carcinoma– Most common head and neck cancer
– Most common site: oral cavity
– Multifactorial
– Chronic abuser of alcohol and tobacco
– Location: ventral surface of tongue, floor of mouth, lower lip, soft palate and gingiva



Patholgy of Salivary Glands
• Inflammation (Sialadenitis)
• Neoplasms

Inflammation
• Mucocele– Most common lesion of the salivary gland
– Lower lip
– Fluctuant swellings of lower lip
• Sialolithiasis and nonspecific sialadenitis– Bacterial infections: S. aureus, S. viridans
– Sialolithiasis


Neoplasm
• Benign tumors– Pleomorphic adenoma
– Warthin tumor
• Malignant tumors– Mucoepidermoid carcinoma
– Adenocarcinoma, not otherwise specified

• Pleomorphic adenoma– Mixed tumor
– Major salivary gland
– Derived from ductal and myoepithelial cells
– Ronded, demarcated mass
– Malignant transformation• Carcinoma ex pleomorphic adenoma



• Warthin tumor (papillary cystadenomalymphomatosum)– Major salivary gland
– Round to oval, encapsulated mass
– Double layers of neoplastic epithelial cells
– Dense lymphoid stroma


• Mucoepidermoid carcinoma– Mixture of squamous cells, mucus‐secreting cells and intermediate cells
– Major salivary gland
• Adenoid cystic carcinoma– Minor salivary gland
– Tubular, solid, cribiform patterns
– Small cells: dark, compact nuclei




Pathology of Esophagus
• Congenital anomalies
• Lesions Associated with Motor Dysfunction
• Esophageal varices
• Esophagitis
• Tumors

Congenital anomalies
• Ectopic tissue
• Atresia and fistula– Associated with congenital heart disease andother gastrointestinal tract malformations
• Webs, rings and stenosis
Lesions Associated with Motor Dysfunction
• Achalasia– Failure to relax
– Aperistalsis of the esophagus
– Partial or incomplete relaxation of the loweresophageal sphincter (LES) with swallowing
– Increased resting tone of the LES
– Proximal esophageal dilation, dysphagia, andregurgitation


– Risk of esophageal carcinoma is 2 to 7%.
– Manometry: Manometry shows aperistalsis,impaired relaxation of the LES, and increased LESresting tone.
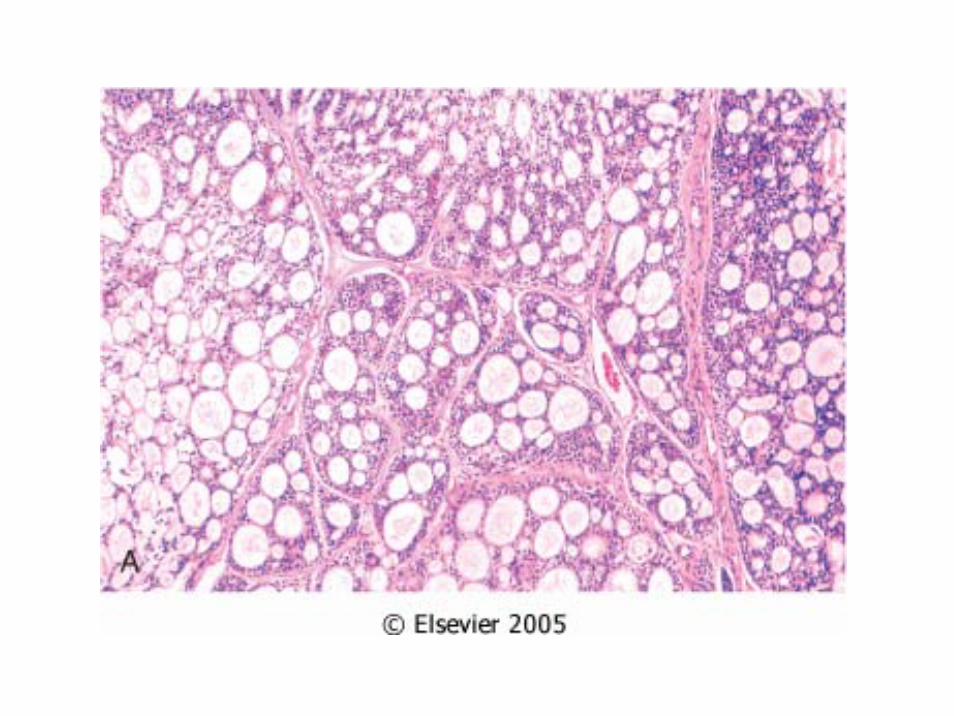
– Morphologic features include:• Dilated esophagus above LES
• Thickened (muscular hypertrophy) or thinned(distention) muscular wall
• Diminished myenteric ganglia
• Secondary mucosal damage

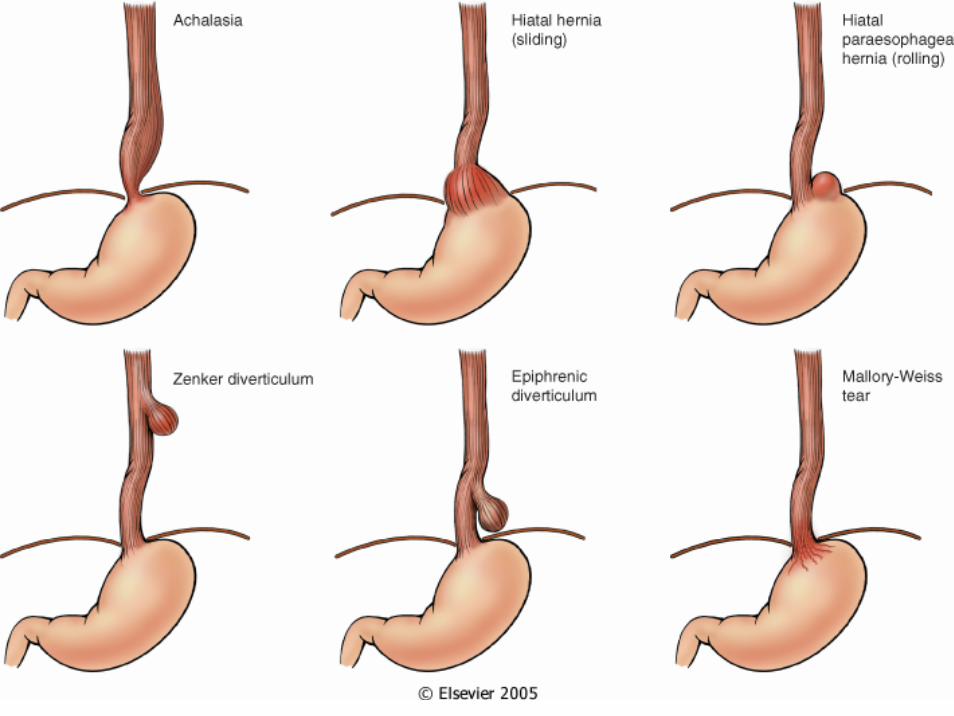
• Hiatal hernia
– Sac‐like dilation of stomach with protrusion abovethe diaphragm
– Sliding (axial) hiatal hernia (90% of cases):Shortened esophagus, traction of upper stomachinto thorax
– Paraesophageal hiatal hernia (rolling hernia)(<10% of cases): Cardia of stomach dissectsalongside esophagus into thorax

• Diverticula
– Pharyngopharyngeal (Zenker) diverticulum: In theupper esophagus, the presumed result of motordysfunction
– Traction diverticulum: More distal location,attributed to fibrosing mediastinal processes orabnormal motility
– Epiphrenic diverticulum: Immediately aboveesophageal sphincter, unclear cause

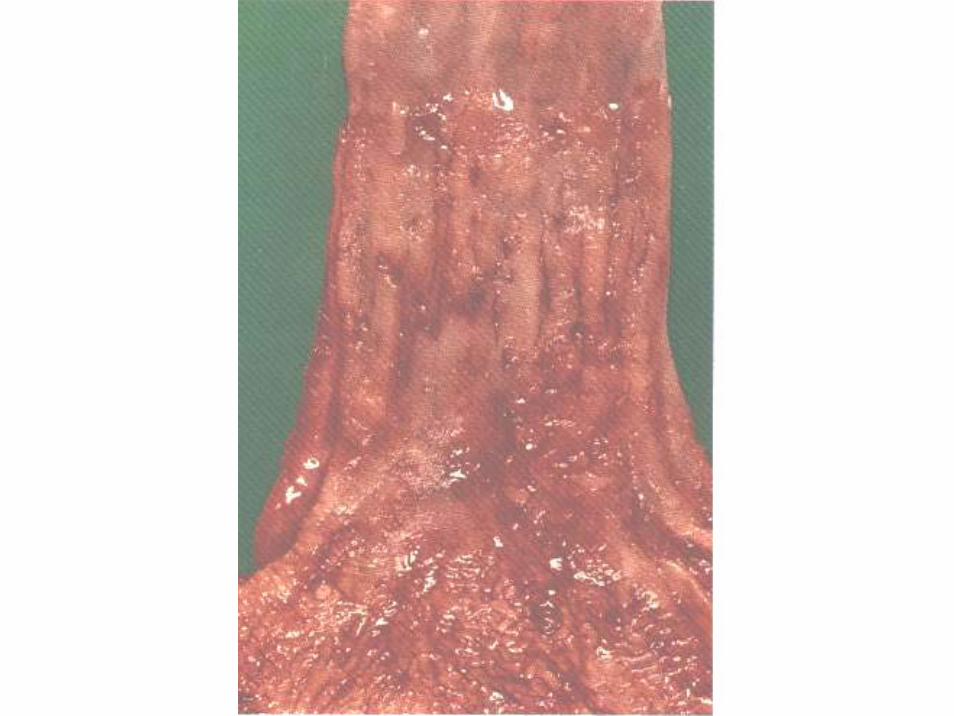
• Laceration (Mallory‐Weiss syndrome)– Longitudinal tears in the esophagus at theesophagogastric junction, attributed to episodesof excessive vomiting
– Most frequently seen in alcoholics
– Massive hematemesis, inflammation, residualulcer, mediastinitis, or peritonitis


Esophageal Varices
• 90% of cirrhotic patients
• Prolonged and severe portal hypertension
• Formation of collateral bypass channels:through the coronary veins of the stomachinto esophageal subepithelial and submucosalveins (varices) and thence to the azygousveins and systemic circulation

• clinically silent until rupture
• Hematemesis—fatality rate is 40% for eachepisode of bleeding, with a 90% chance ofrecurrence within a year in survivors



Esophgitis
• Reflux esophagitis (Gastroesophageal Reflux Disease : GERD)– Reflux of gastric contents– Decreased efficacy of esophageal antirefluxmechanisms
– Presence of a sliding hiatal hernia– Delayed gastric emptying and increased gastricvolume
– Reduced reparative capability of the esophagealmucosa

– Symptoms include dysphagia, heartburn,regurgitation of sour brash, hematemesis, andmelena.
– Stricture or Barrett esophagus can develop asa result of reflux esophagitis.

• Barette esophgus– Replacement of the distal esophageal squamousepithelium by a metaplastic columnarepithelium
– Inflammation and ulceration of squamousmucosa; differentiate into more resistantgastric‐type or intestinal‐type epithelium
– Risk of adenocarcinoma is 30 times normal


• Infectious and chemical esophagitis– Ingestion of mucosal irritants
– Cytotoxic anticancer therapy
– Infection: HSV, CMV, Candida
– Uremia

Tumors
• Benign tumors– Polyp – Lipoma– Papilloma
• Malignant tumors– Squamous cell carcinoma– Adenocarcinoma

• Squamous cell carcinoma–Pathogenesis is multifactorial– Insidious onset–Dysphagia, obstruction, weight loss,hemorrhage,
– Sepsis secondary to ulceration, fistulaformation into respiratory tree withaspiration



• Adenocarcinoma–One half of esophageal cancers
–Majority of cases arise from the Barrette mucosa


Pathology of Stomach
• Congenital anomalies
• Gastritis
• Peptic Ulcer Disease
• Miscellaneous Conditions
• Tumors

Congenital Anomalies
• Pancreatic heterotopia• Diaphragmatic hernia
–Pulmonary hypoplasia
• Congenital hypertrophic pyloric stenosis–Hypertrophy and possibly hyperplasia ofcircular muscle of the muscularis propria ofthe pyloris
–Visible peritalsis, palpable mass

Gastritis
• Acute gastritis– Acute mucosal inflammatory process– Etiologiy includes:
• Chronic and heavy use of nonsteroidal anti‐inflammatorydrugs(NSAIDs), particularly aspirin
• Excessive alcohol consumption• Heavy smoking• Severe stress (bums, trauma, surgery)• Ischemia and shock• Ingestion of acid or alkali• Gastric irradiation• Mechanical trauma, Post‐distal gastrectomy
• Mechanisms of action include– Increased acid production with back‐diffusion– Decreased production of surface bicarbonate buffer– Reduced mucosal blood flow, disruption of mucus layer– Direct damage to mucosal epithelium
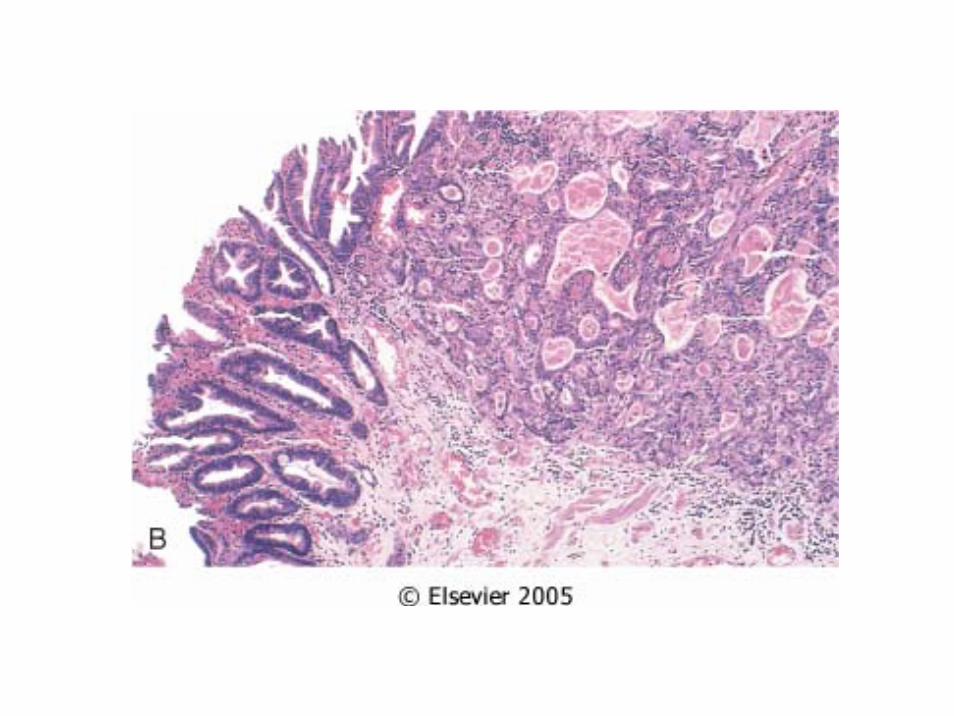
• Morphologic findings include– Moderate edema and hyperemia– Entry of neutrophils into the epithelial layer (activity)– Sloughing of the superficial epithelium (erosion)– Hemorrhage (acute hemorrhagic erosive gastritis)



• Chronic gastritis– The presence of chronic mucosal inflammatorychanges leading eventually to mucosal atrophyand epithelial metaplasia

– Etiologic associations are as follows:• Chronic infection, especially Helicobacter pylori
• Immunologic: Antibodies to parietal cells
• Toxic: alcohol and tobacco usage
• Postsurgical: postantrectomy reflux of bile
• Motor/mechanical: obstruction, atony
• Radiation
• Granulomatous conditions: Crohn disease
• Graft‐versus‐host disease, uremia, amyloidosi



– Microscopic findings are as follows:• Infiltrate of lymphocytes and plasma cells in laminapropria, involving either the superficial portion (fundus)or the entire mucosal thickness
• Activity (intraepithelial neutrophilic infiltrate)• Regenerative change• Variable atrophy• Metaplasia to intestinal‐type epithelium• Dysplasia• H. pylori

• Clinical Findings– Few symptoms: Nausea, vomiting, or upperabdominal discomfort
– Pernicious anemia occurs in autoimmunegastritis. Laboratory findings include gastrichypochlorhydria and serum hypergastrinemia.
Peptic Ulcer Disease
• Peptic ulcer– Breach in the mucosa of the alimentary tract thatextends through the muscularis mucosa into thesubmucosa or deeper
– Imbalance between the gastroduodenal mucosaldefense mechanisms and damaging forces

• Mucosal defense forces consist of– Surface mucus secretion
– Bicarbonate secretion into mucus
– Mucosal blood flow
– Apical epithelial cell transport systems
– Epithelial regeneration
– Role of prostaglandins

‐ H. pylori: Major factor in pathogenesis‐ H. pylori does not invade the tissue. It induces inflammation by increase production of cytokine
‐ Bacterial gene products cause epithelial cell injury and induction of inflammation
‐ H. pylori secretes urease (breakdown urea to ammonium chloride), protease, orphospholipases.
‐ Enhance gastric secretion and impairs duodenal bicarbonate production

– 98% found in duodenum and stomach, in a ratio of 4:1.
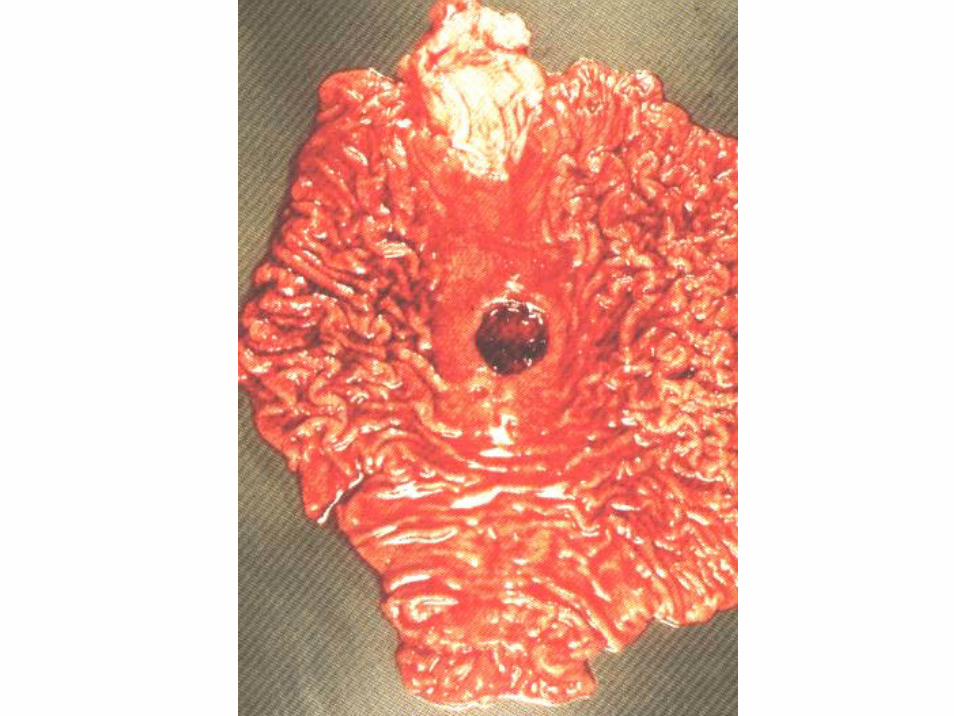
– Gross findings include a sharply punched‐outdefect with slightly overhanging mucosalborders and smooth, clean ulcer base.
–Malignant transformation is rare and relatedto underlying gastritis.

– Epigastric gnawing, burning, or aching painoccurs, which is worse at night and 1 to 3hours after meals.
– Nausea, vomiting, and weight loss occur.
– Complications include hemorrhage, anemia,perforation, and obstruction.



• Acute gastric ulceration–Acute gastric ulceration refers to focal,acutely developing gastric mucosal defectsappearing during severe stress (stressulcer).
–Curling ulcers: shock; extensive burns orsevere trauma
–Cushing ulcers: elevated intracranialpressure, as in trauma or surgery

Tumors
• Benign tumors– Polyps
– Adenoma
• Malignant tumors– Gastric carcinoma
– Lymphoma
– Carcinoids tumor
– Mesenchymal tumors


– Gross locations of carcinoma are:• Pylorus and antrum, 50 to 60%• Cardia, 25%• Body and fundus, 15 to 25%• Lesser curvature is involved in 40% and greater curvature in 12%.
– Factors associated with increased incidence of gastriccarcinoma
• Diet: use of preservatives (nitrosamines), lack of fresh fruit andvegetables
• Cigarette smoking increases risk 1.5‐ to 3.0‐fold• Infection by H. pylori leading to chronic gastritis• Autoimmune gastritis• Partial gastrectomy permitting gastroduodenal reflux

–Classification is according to the following:• Depth of invasion: greatest impact on clinical outcome
• Macroscopic growth pattern: exophytic, flat or depressed, or excavated. Uncommonly, diffuse invasion throughout the wall creates a rigid thickened stomach: linitis plastica.

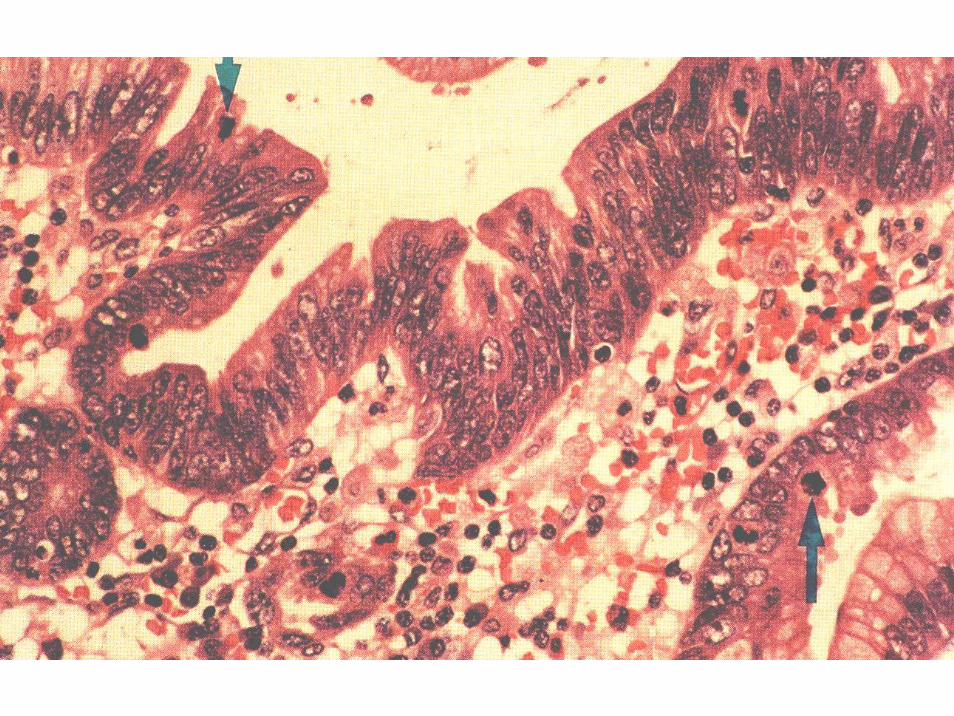
• Histologic subtype:
– Intestinal type: Gland‐forming columnar epithelium; usually polypoid expansile growth pattern
– Diffuse type: poorly differentiated, single signet‐ring cells; mucin producing; infiltrative growth pattern
– Dissemination: Dissemination to ovaries generates Krukenberg tumors.





• Clinical Findings– Insidious diseases– Initially asymptomatic.– Findings include weight loss, abdominal pain, anorexia,vomiting, altered bowel habits, dysphagia, anemia, and hemorrhage.
• Prognosis depends only on depth of invasion– Resected early gastric cancer, 90 to 95% 5‐year survival– Advanced disease, less than 15% 5‐year survival

• Less common gastric cancers– Lymphoma
– Gastrointestinal stromal tumors



