pathology and treatment by fiona nicholson. alzheimer’s disease overview history of ad diagnosis...
TRANSCRIPT

Pathology and Treatment
By Fiona
Nicholson

Alzheimer’s Disease Overview
History of AD Diagnosis of AD Stages Risk Factors Physiology Treatment
History of AD Alzheimer’s disease was
characterized by Dr. Alois Alzheimer in 1906 after performing an autopsy on his patient, Mrs. Auguste D. who was thought to have “amnesiac writing disorder.”
Dr. Alzheimer noted “peculiar formations” (amyloid plaques) and “dense bundles” (neurofibrillary tangles).
During the autopsy, a substance was noted that was later characterized as the beta-amyloid protein.
Auguste D.
Dr. Alois Alzheimer
How common is Alzheimer’s? Out of all the
neurogenerative diseases, Alzheimer’s has the highest prevalence at 1.450/100,000
The incidence and prevalence of this disease increases with age; between the ages of 65-69, the prevalence is 1.53%, and between the ages of 80-85, the prevalence increases to 25-30% of the population

Diagnosis of AD
No direct confirmatory test exists Diagnosis of AD is based on careful clinical
assessment which can include medical interviews
Laboratory tests are conducted to eliminate the possibility of other diseases that can mimic the AD
Neuropsychological tests are conducted to assess the cognitive symptoms
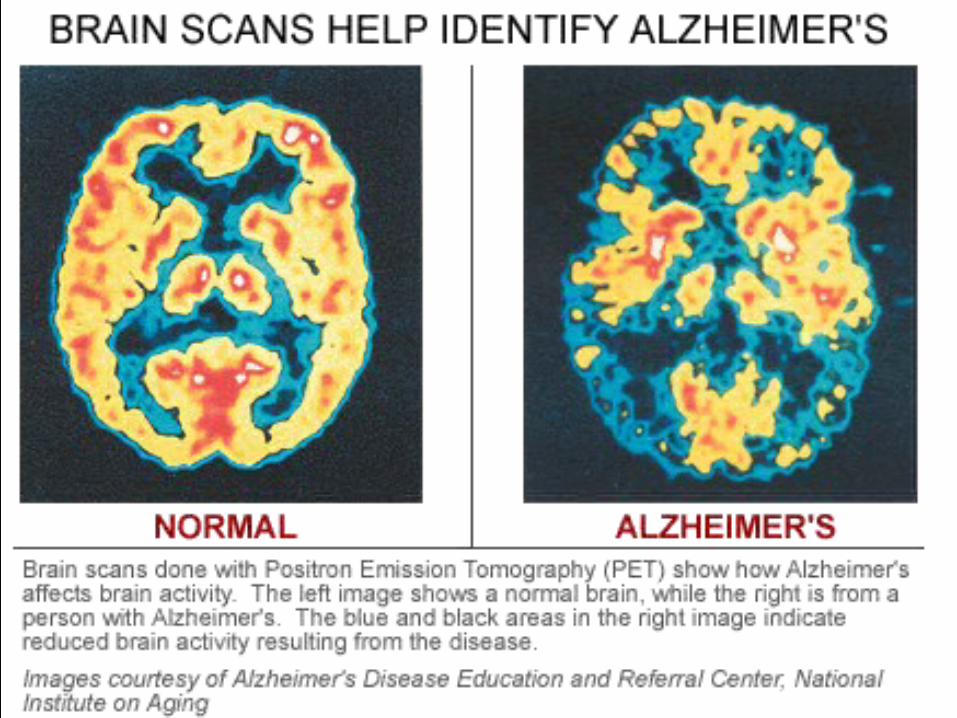
Brain scans can show the progression of AD and how the disease influences brain activity
Stages of Alzheimer’s Disease Stage 1: No impairment
No memory problems are evident to a health care professional during an interview
Stage 2: Very mild cognitive declinePatients may feel they have memory lapses (such as forgetting keys), but these are not evident during a medical interview
Stage 3: Mild cognitive declineFriends, family, and coworkers notice memory decline, and the decline is measurable in a clinical setting. Examples are decreased ability to remember names when introduced to new people, losing or misplacing a valuable object, and reading a passage and retaining little information
Stage 4: Moderate cognitive decline (early to mid stage AD)AD is able to be diagnosed at this stage, and decreased cognitive ability is very evident in the following areas: decreased ability to recall information about recent occasion, decreased ability to perform mental arithmetic, impaired ability to pay pills and manage finances, reduced memory of personal history. Patients may seem withdrawn in complex situations
Stages of Alzheimer’s Disease Stage 5: Moderately severe cognitive decline (moderate or mid-
stage AD)Major deficits in memory and difficulty in cognitive function; AD patients require some assistance with daily activities. Patients may not be able to recall their phone number or current address and can be confused about what day or the week or what season it is. Patients maintain knowledge about themselves, such as their name and the names of close family members.
Stage 6: Severe cognitive decline (moderately severe AD)Memory deficits worsen and personality changes are evident. Patients tend to lose awareness of recent events, cannot recollect personality history accurately, need help with everyday activities, and can wander and become lost.
Stage 7: Very severe cognitive decline (severe or late-stage AD)Patients lose the ability to respond to the environment, lose the ability to speak, and lose control over their movement.

Risk Factors for AD
Age Genetics Lifestyle Head trauma Clinical depression Down’s syndrome Environmental toxins

What causes AD?
According to Goodman and Gilman, AD is “characterized by marked atrophy of the cerebral cortex and loss of cortical and subcortical neurons.” (p. 538)
Areas of the brain affected:
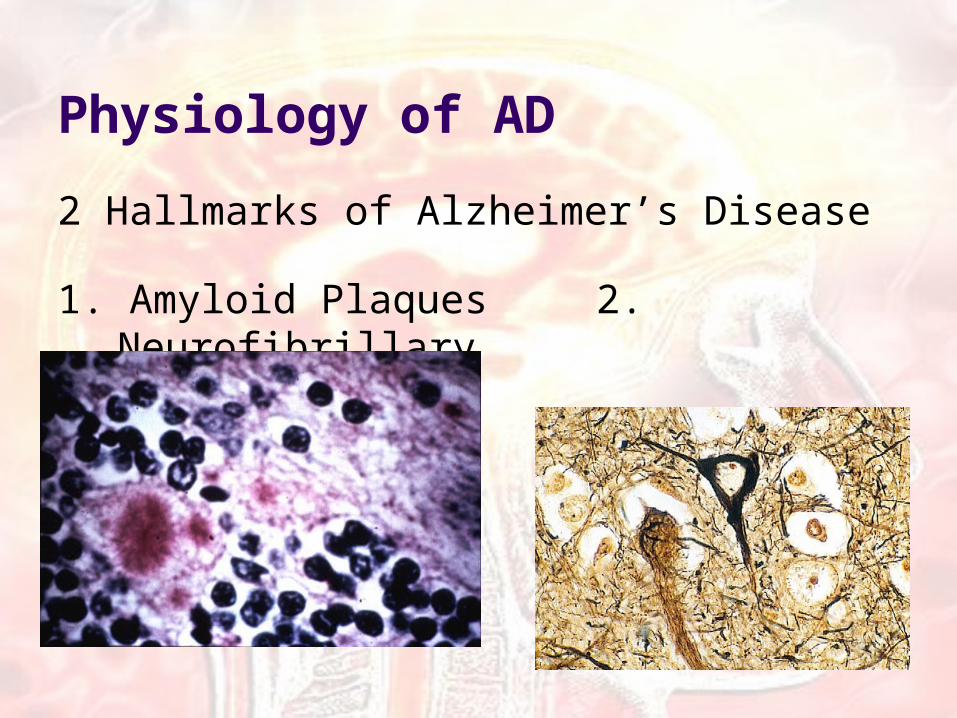
Physiology of AD
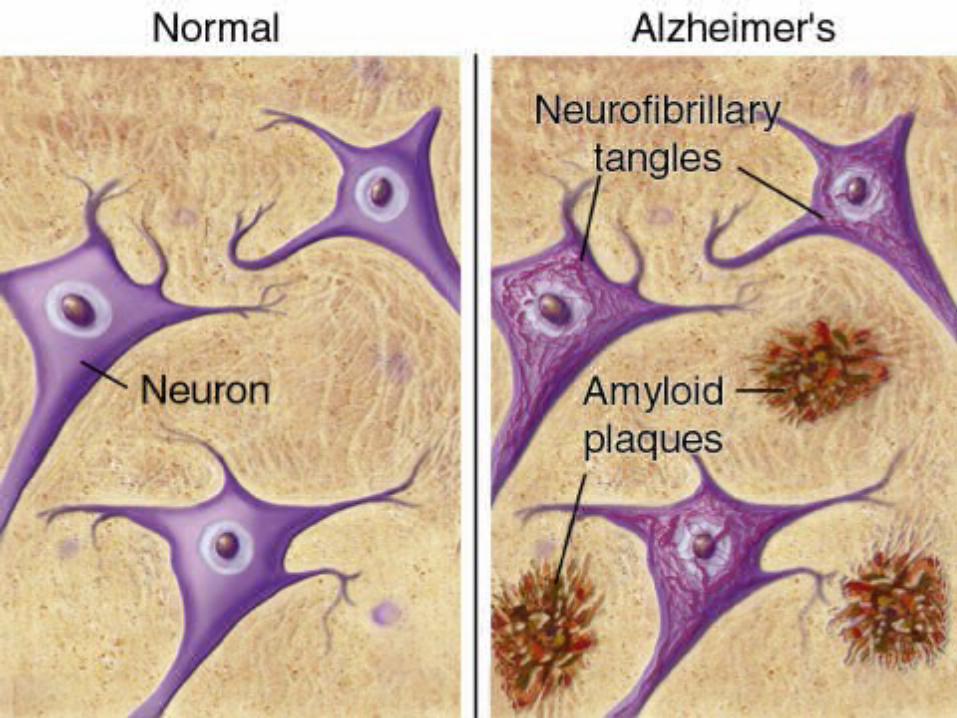
2 Hallmarks of Alzheimer’s Disease
1. Amyloid Plaques 2. Neurofibrillary
tangles

Amyloid Plaques Found in the spaces
between nerve cells Composed of an
insoluble protein peptide called beta-amyloid, other proteins, and remnants of other brain cells (neurons, non-nerve cells, and glial cells)
Plaques develop in the brain in many people as they age, but in AD patients, plaques develop in the cognitive areas.

Neurofibrillary Tangles
Tangles develop inside nerve cells
Abnormal collections of twisted protein fibers
Protein threads are composed of the hyperphosphorylated tau protein
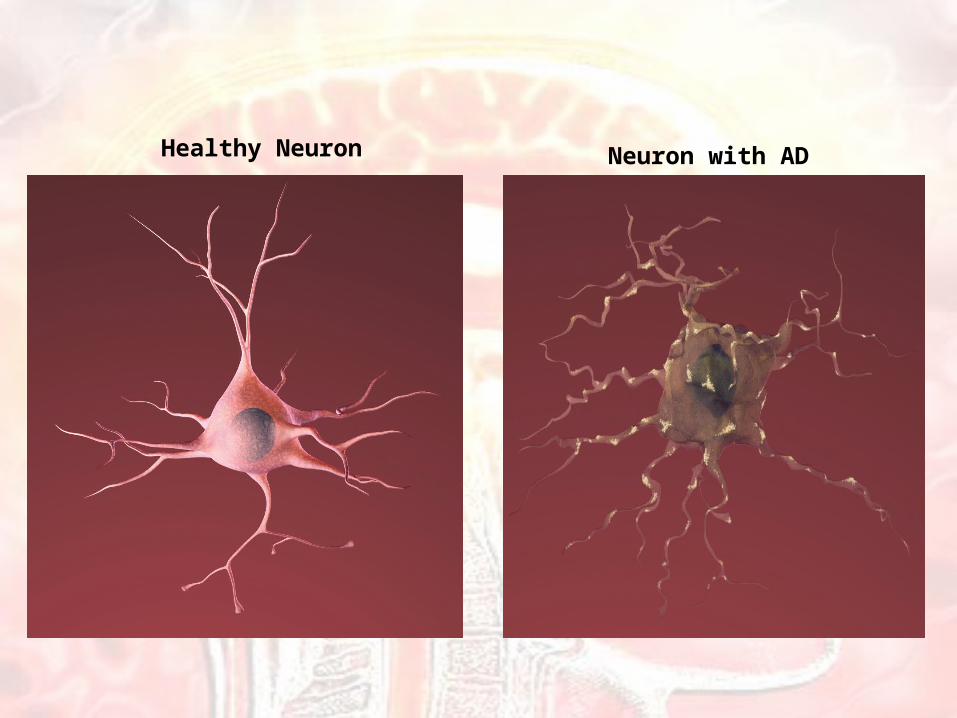
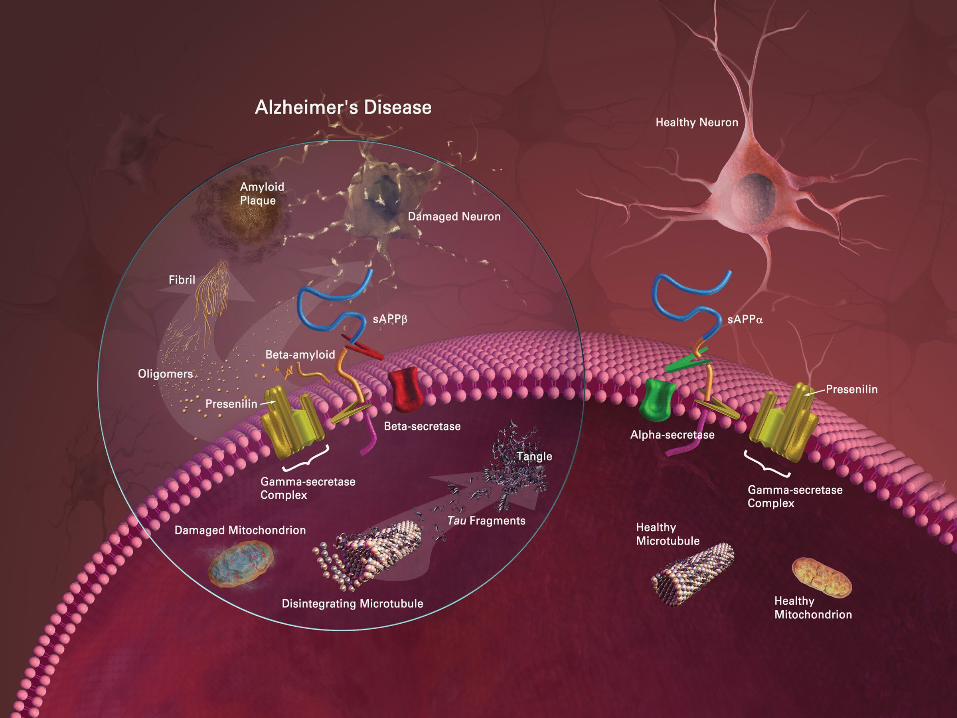
Healthy Neuron Neuron with AD
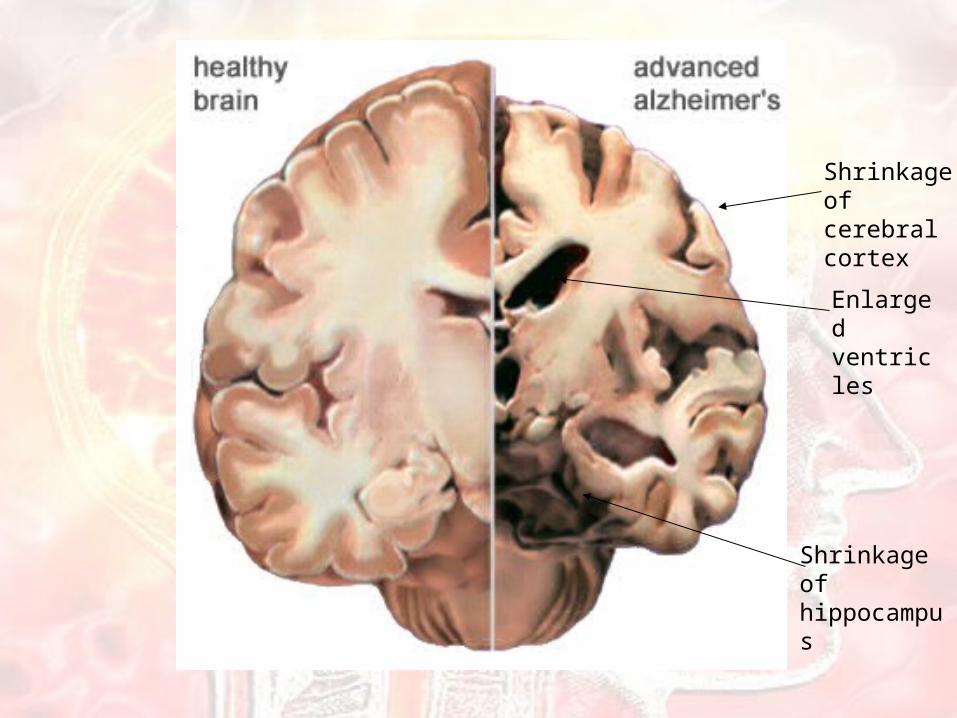
Shrinkage of cerebral cortex
Enlarged ventricles
Shrinkage of hippocampus
Three Hypotheses Concerning AD Development
1. Amyloid Cascade Hypothesis
2. Tau Hypothesis3. Cholinergic Hypothesis

Amyloid Cascade Hypothesis The initiating event that leads to the formation of
plaques is an excess of Αβ peptides. Patients with missense mutations in the APP,
Presenilin 1, and Presenilin 2 genes (“Alzheimer’s genes”) are prone to overproduction.
Patients without AD genes start to overproduce Αβ peptides from a failure of metabolism.
The response to the excess of Αβ peptides involves an inflammatory response and free radical formation.
This toxic cascade, induced by amyloid accumulation, eventually leads to the organization into plaques.
Tau Hypothesis
In healthy neurons, Tau normally has a certain amount of phosphate molecules attached, and binds to microtubules and stabilizes them.
In an AD neuron, tau is hyperphosphorylated which disengages the protein from the microtubules.
The resulting detached tau proteins group together and form tangles. The microtubules disintegrate, which leads to the collapse of the neuron’s transport system.

Cholinergic Hypothesis
Acetylcholine biosynthesis is reduced in the presence of plaques and tangles.
Because less of a neurotransmitter (acetylcholine) is synthesized, this leads to a loss of neurons.
Thus, even more brain cells are lost than usual, which can lead to AD.
There is no cure for Alzheimer’s disease!
The following treatments can alleviate symptoms or slow the
progression of the disease.
Treatment1. Symptomatic Treatments:
a) Acetylcholinesterase Inhibitorsb) NMDA-receptor Antagonists
2. Disease-modifying Treatments:a) Inhibition of amyloid formationb) Inhibition of abeta aggregationc) Tau phosphorylation inhibitors
3. Other Therapies: a) Gingko bilobab) Estrogen therapy for womenc) Anti-inflammatory drugs: aspirin
4. Life Style Changesa) Stress controlb) Monitor Dietc) Cognitive Stimulation
5. Psychotic Treatments:a) Antidepressants b) Anti-anxiety medicine c) Antipsychotics

1a) Acetylcholinesterase Inhibitors “Smart drugs” Decrease the rate that Ach
is broken down, therefore increasing Ach concentration
Treatment with these drugs does not cure Alzheimer’s, but they do help to alleviate symptoms
These drugs have to be able to cross the blood brain barrier sufficiently
More beneficial in early stages of Alzheimer’s versus later stages
Disadvantages: With long term use, these
drugs increase the overall level of Ach in the body which causes gastrointestinal side effects
bradycardia, hypotension, hypersecretion, bronchoconstriction, GIT hypermotility, and decrease intraocular pressure.
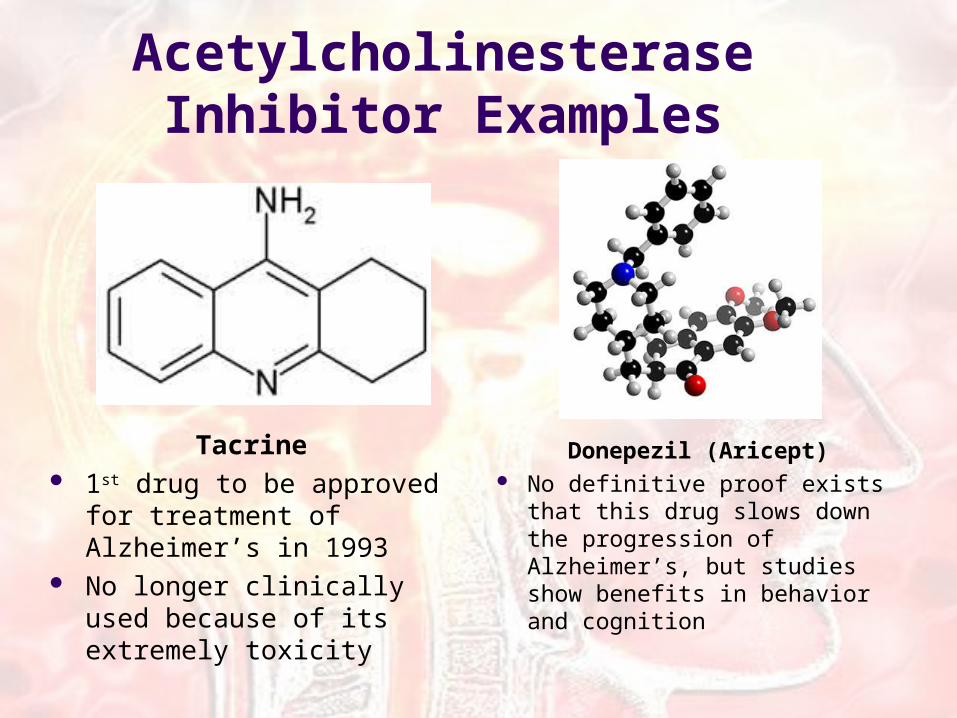
Acetylcholinesterase Inhibitor Examples
Tacrine 1st drug to be approved for
treatment of Alzheimer’s in 1993
No longer clinically used because of its extremely toxicity
Donepezil (Aricept) No definitive proof exists that
this drug slows down the progression of Alzheimer’s, but studies show benefits in behavior and cognition

Acetylcholinesterase Inhibitor Examples
Galantamine (Razadyne) Treatment for mild to
moderate Alzheimer’s Extracted from daffodils or
snow-drop bulbs
Rivastigmine (Exelon) significant treatment effects
on the cognitive (thinking and memory), functional (activities of daily living) and behavioral problems have been observed
Treatment for mild to moderate dementia
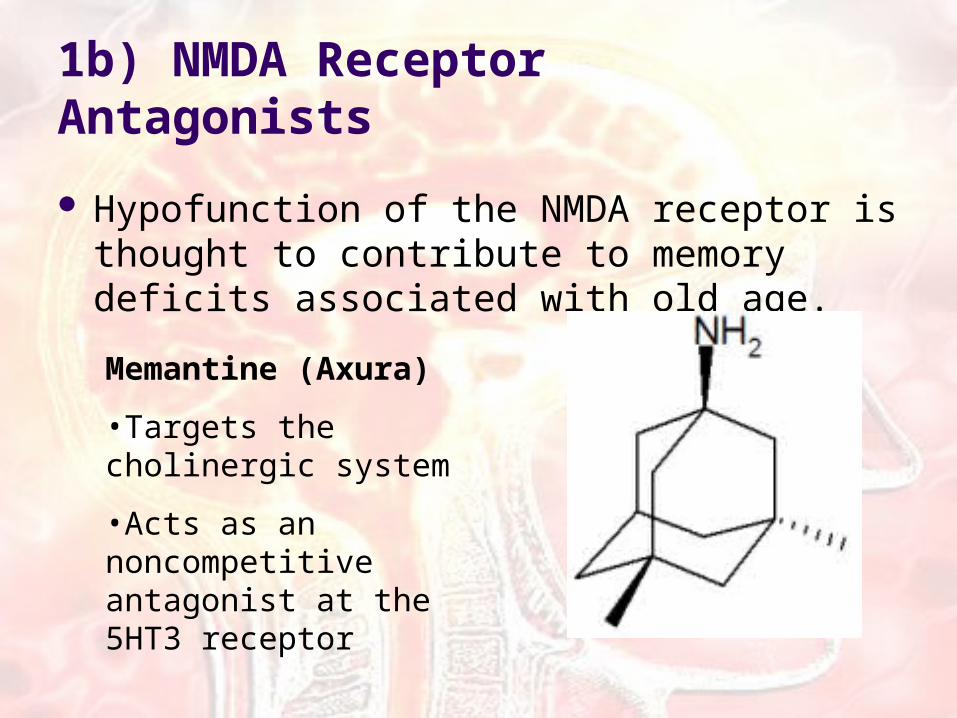
1b) NMDA Receptor Antagonists
Hypofunction of the NMDA receptor is thought to contribute to memory deficits associated with old age.
Memantine (Axura)
•Targets the cholinergic system
•Acts as an noncompetitive antagonist at the 5HT3 receptor
2) Disease-modifying Treatments:
Used to treat moderate to severe forms of ADa) Inhibition of amyloid formation
to inhibit the toxic cascade that leads to amyloid formationb) Inhibition of abeta aggregation
to inhibit the overproduction of the abeta peptidec) Tau phosphorylation inhibitors
to prevent hyperphosphorylation of Tau proteins and maintain microtubules
3a) Other Therapies: Ginkgo Biloba
Ginkgo biloba is thought to improve thinking, learning, and memory in AD patients
Ginkgo has antioxidant properties and increases
Ginkgo is used preventively because it is thought to delay the onset of AD in patients that are at higher risk
4. Life Style Changes
a) Stress controlb) Monitor Dietc) Cognitive Stimulation d) Social and Visual Stimulation
5. Psychotic Treatments
Applicable in later stages of ADa) Antidepressants b) Anti-anxiety medicine c) Antipsychotics
Noteworthy Cases of AD
Ronald Reagan
Charlton Heston
Rita Hayworth