pathology 430/827 bladder cancer etiology, classification, and diversity david m. berman, md, phd...
TRANSCRIPT

Pathology 430/827
Bladder cancerEtiology, classification, and diversity
David M. Berman, MD, PhDPathology and Molecular MedicineQueen’s Cancer Research [email protected]

Objectives
1. Recognize who gets bladder cancer and why

Objectives
1. Recognize who gets bladder cancer and why2. Recognize different types of bladder cancers
A. Two genomic pathways cause bladder cancerB. Bladder cancers can change (“progress”) over
timeI. GradeII. Stage

Objectives
1. Recognize who gets bladder cancer and why2. Recognize different types of bladder cancers
A. Two genomic pathways cause bladder cancerB. Bladder cancers can change (“progress”) over time
I. GradeII. Stage
3. Understand concept of epithelial differentiation and how it produces different types of bladder cancer cells

Epidemiology
• 4th most common cancer in men, – Affecting ~3% of men in Western countries– 3x less frequent in women– Peak age 75yrs

Epidemiology
In 2013 in US & Canada, –~80,000 new cases –~16,000 deaths

Recurrence
• Up to 70% of cases recur.• Estimated $3 billion annually U.S.,
– Biggest expense = surveillance (cystoscopies).

Urinary bladder:A urine storage system
Lumen
(optional)

(niche?)
Epithelial architecture
(basal)
Intermediate Cell

Uroplakins form permeability barrier
Min G et al. J Cell Sci 2003;116:4087-4094
©2003 by The Company of Biologists Ltd

Differentiation in urothelial carcinoma
Three cell layers of benign urothelium
He X et al., 2009 Stem Cells, 27:1487
Uroplakins
Basal cells repopulate
Superficial cells protect
Intermediate cells mature
Epidemiology
336,000 cases/yr ~3,000 cases/yrOlder male

Jemal A et al. Cancer statistics, 2007. CA Cancer J Clin. 2007
Presentation

Jemal A et al. Cancer statistics, 2007. CA Cancer J Clin. 2007
5-year survival

Recurrence
$$$$$$$$$

Symptoms
>
Hematuria (>75%) Dysuria (~10%)

RISK
SmokingStrong (~50%)
OccupationStrong (~25%)

Iatrogenic Schistosomes
RISK

RISK
FamilyHistory
Muir Torre Syndrome
Arsenic

• Common (75%)
• Recur (50%)
• Local treatment

• Uncommon (25%)
• Usually progress

Radical treatmentLocal treatment

Progression and classification of urothelial carcinoma
Grade Low or High High
Grade High High
85%

Bladder Cancer Staging
STAGE Primary tumour (T) Regional Lymph Nodes (N) Distant Metastasis (M)
0 Ta or Tis 0 0
I T1 0 0
II T2 0 0
III T3 or T4a 0 0
IV T4b AND/OR N1-N3 AND/OR M1

Survival rates by stage
Stage Relative 5-year Survival Rate
0 98%I 88%II 63%III 46%IV 15%

Non-invasive papillary urothelial carcinoma

Papillary urothelial neoplasia
Fibrovascular cores
Urothelium

Low grade non-invasivepapillary urothelial carcinoma
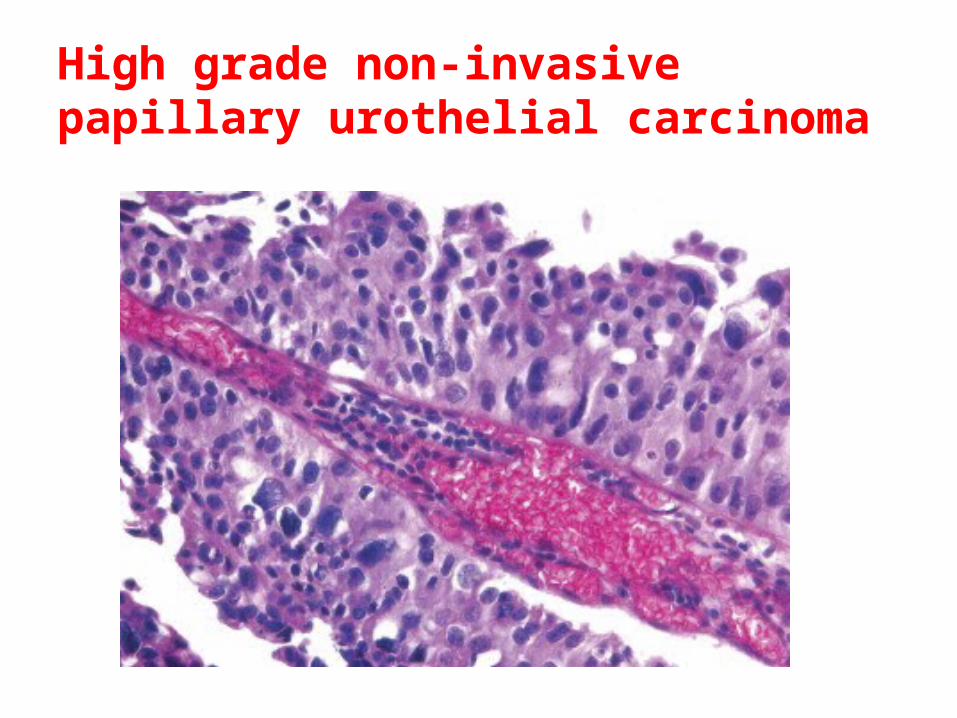
High grade non-invasivepapillary urothelial carcinoma

Invasive urothelial carcinoma

Flat/invasive urothelial carcinoma
Benign
Carcinomain situ (CIS)

Invasive urothelial carcinoma

Two Pathways
Urothelial Hyperplasia
Flat CIS
PUNLMPLG Papillary UrCa
Superficial inv. Muscle inv. UrCa
H-RAS/FGFR3 Activation
P53/RB Inactivation
Normal Urothelium
Papillary/Noninvasive
Flat/Invasive
Loss of CDKN2A

HRAS/FGFR3+
P53/RB-

• Sweden (Lund) • Texas (MD Anderson • TCGA (U.S.)
Studies describing molecular subtypes

Non-invasive Invasive
•Urobasal A (Lund) ~ Luminal (Texas) ~ Group B (TCGA)
• Urobasal B (Sweden)
• Squamous-like (Sweden) , Basal (Texas)
Molecular Subtypes

Different cell types within a bladder cancer

Hypothetical link between injury and cancer

Activation of Sox9 by bladder injury
Ling et al., 2009 Cancer Research

Autocrine loop linking injury to bladder cancer
Ling et al., 2009 Cancer Research

Epithelial differentiation in cancer
Epigenetic changes
Epigenetic changes
(Basal cell)
Intermediate Cell

Urothelial differentiation inUrothelial Carcinoma Xenografts
BenignUrothelium
SW780 Cell LineXenograft

67 Kd Laminin Receptor: Surface marker of tumor “basal cells”
But not in vitro
He X et al., 2009 Stem Cells, 27:1487

SW780 Human Bladder cancer xenograft
Single cell digest
FACS
Inject 10 sites, 2-20k cells each
67LR+ (13%)
67LR+
67LR_
CK17
CK1767LR- (87%)
67LR expression in vivo identifies basal-like bladder cancer cells
He X et al., 2009 Stem Cells, 27:1487
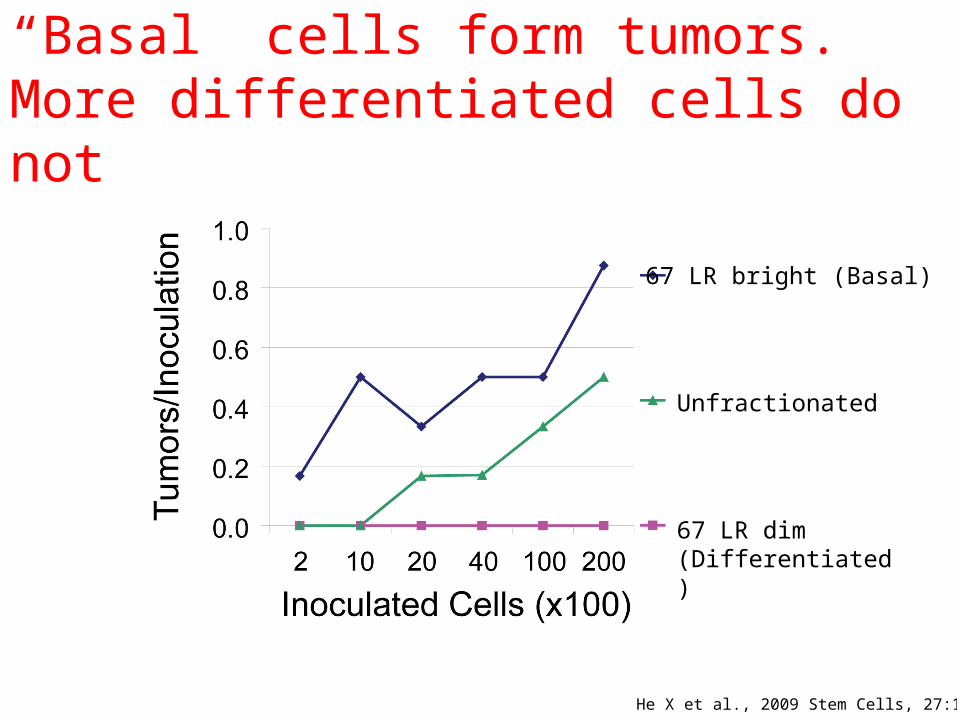
“Basal” cells form tumors. More differentiated cells do not
67 LR bright (Basal)
Unfractionated
67 LR dim (Differentiated)
He X et al., 2009 Stem Cells, 27:1487

Gene Expression Programs in Basal-like Urothelial Cancer Cells
Migration
Angiogenesis
Apoptosis Proliferation
Signaling pathways•Jak-STAT•Notch•FAK•mTOR •EGFR•Wnt •TGF beta
67LR+
67LR_
CK17
CK17
He X et al., 2009 Stem Cells, 27:1487

Conclusions
• Two pathways of bladder cancer– Genomic differences between cancers
• Epithelial injury is a risk factor• Molecular links exist between injury repair
and cancer• Bladder cancers differentiate in a manner
similar to benign urothelium– Genomic differences within cancers