pathological gambling: barriers to treatment and the experience of self-change jachen c. nett and...
Post on 18-Dec-2015
214 views
TRANSCRIPT

Pathological gambling: Barriers to treatment and the experience of self-change
Jachen C. Nett and Sina Schatzmann
Gambling Prevention and Research: From Legislation to Action Centre du Jeu Excessif, Lausanne
1st-2nd March 2005
University of Applied Sciences Berne
School of Social Work (HSA Berne)
Institute for Social Planning and Social Management (ISS)
1st March 2005 HSA Berne, ISS 2
Proceeding
• Brief description of the study– goals and applied methods– description of the sample– definitions and classification
• Selected results with respect to– processes of self-change– barriers to treatment
• Open forum (questions & discussion)
1st March 2005 HSA Berne, ISS 3
Study’s title: Casino legislation und „self-recovery“ from problem gambling
Central goals of the research project:• To explore the situation and perspectives of past
and current problem gamblers in Switzerland with special reference to the implementation of the new casino legislation and to processes of “self-recovery” from pathological gambling
• To get information about how the different prevention activities instigated by the casinos are valued by exponents of the target group
• To create a baseline data set for the longitudinal observation of individual self-change processes among problem gamblers
1st March 2005 HSA Berne, ISS 4
Used data base
• Telephone interviews with people who are affected by past or current gambling problems (february 2002 - march 2003)
• Recruitment of the sample (N=64) :– by mediation of a psychiatrist in Zurich– by Media calls (German speaking part
of Switzerland)– by large-scale distribution of flyers
(German speaking part of Switzerland)
1st March 2005 HSA Berne, ISS 5
Applied instruments
• Introductory questionnaire
• Questionnaire version A (for former problem or
pathological gamblers)
• Questionnaire version B (for current problem or pathological gamblers)
Applied scales: SOGS Gambling Screening (Lesieur & Blume, 1987), CAGE Alcohol Screening (Ewing, 1970), NODS Gambling Screening (Gerstein et al., 1999), KFG Petrys & Bauligs (1996) short questionnaire about gambling behaviour, Items of the Geneva-prevalence-study of Osiek et al. (1999), Items of Klingemann (1988a/b)
1st March 2005 HSA Berne, ISS 6
Definitions of the central terms
• Problem gamblers: SOGS ≥ 3 (life-time), pathological gamblers: SOGS ≥ 5 (life-time)
• Current problem/pathological gambling = gambling behaviour with currently negative consequences , former problem/pathological gambling = no or gambling behaviour with currently no negative consequences after having had gambling problems before
• Processes of self-change = self initiated changes in the perception, attitude, and practice of one’s gambling behaviour
• Auto-remission = a substantial (self initiated) change in the gambling behaviour, i.e. a clear turning away from excessive and uncontrolled gambling.
1st March 2005 HSA Berne, ISS 7
Characteristics of the sample
• 7 women, 57 men• Mean age: 43 (range: 26 to 70)• ¾ are of Swiss nationality • Singles (41%) and divorced/separated (28%) individuals are
overrepresented in the sample• Educational level is comparable with standard population
(lowest level is underrepresented)• Income: 61% earn between CHF 4000 and 9000• Unemployed subjects are overrepresented (22%)• 61 of the 64 subjects interviewed show life-time prevalence
of problem or pathological gambling (mean SOGS score = 9.9)
• Main type of game played: 50 Slot-machine players, 10 table players (casino) and 4 other kind of gambling
1st March 2005 HSA Berne, ISS 8
Gambling behaviour
Classification of the interviewed problem (n=2) and pathological gamblers (n=61) according to the following criteria:
– showing currently a highly pathological gambling behaviour (n=15)
– being at the stage of giving up gambling (n=22)
– showing a controlled gambling behaviour (n=12)
– definitely (?) having quit gambling (n=14)
1st March 2005 HSA Berne, ISS 9
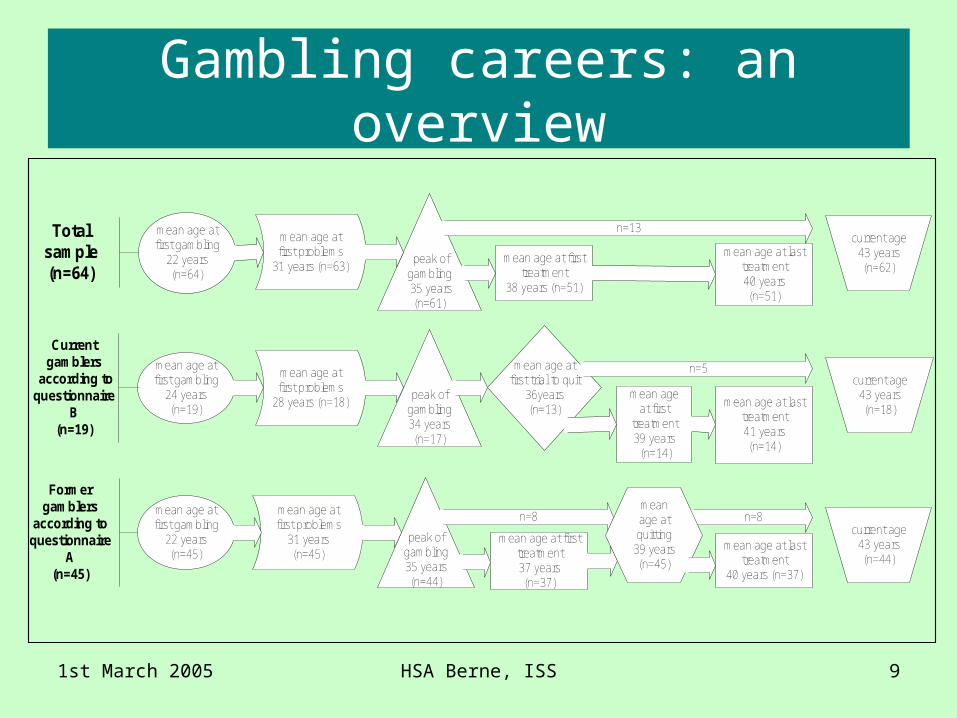
Gambling careers: an overview
mean age at lasttreatment
40 years (n=37)
mean age at firsttreatment37 years(n=37)
mean age atfirst gambling
22 years(n=45)
mean age atfirst problems
31 years(n=45)
peak ofgambling35 years(n=44)
mean age at lasttreatment40 years(n=51)
mean age at firsttreatment
38 years (n=51)
mean age atfirst gambling
22 years(n=64)
mean age atfirst problems
31 years (n=63) peak ofgambling 35 years
(n=61)
mean age at lasttreatment41 years(n=14)
mean ageat first
treatment39 years (n=14)
mean age atfirst trial to quit
36years(n=13)
mean age atfirst gambling
24 years(n=19)
mean age atfirst problems
28 years (n=18)peak of
gambling34 years(n=17)
n=13current age
43 years(n=62)
Totalsample(n=64)
n=5
n=8current age
43 years(n=44)
current age43 years(n=18)
Formergamblers
according toquestionnaire
A(n=45)
Currentgamblers
according toquestionnaire
B(n=19)
n=8meanage atquitting
39 years(n=45)
1st March 2005 HSA Berne, ISS 10
Most successful recovery attempt (failed)
• Multiple recovery attempts in the past (up to 50)
• Mean age: 35.6 years• Mean duration: 1 ½ years• Reasons of failure: discontinuation
of social support, incitation to re-entry by fellow gamblers, situational changes, overwhelming temptation
1st March 2005 HSA Berne, ISS 11
Successful recovery
• Mean age: 39 years• About 5 years after peak of gambling• Reasons of success: admitting the
existence of gambling problems, high degree of negative consequences, professional help seeking, situational changes
• Coping with the temptation to gamble again: active distraction, cognitive coping, repression
1st March 2005 HSA Berne, ISS 12
Recovery attempts vs. successful recovery
• Different motivation to quit: Problem gamblers who fail to quit have less severe problems than problem gamblers who succeed in quitting
• Different quitting plans: Problem gamblers who fail to quit have less strict quitting plans than problem gamblers who succeed in quitting
• Different life events in the past twelve months before quitting: Problem gamblers who fail to quit and problem gamblers who succeed in quitting do not differ in the number of life events they experienced in the past twelve month before quitting. However the character of live events differs: Especially the actual or threatening loss of close social relationships seems to contribute to a successful quitting
1st March 2005 HSA Berne, ISS 13
Experience with addiction related intervention
Objective criteria for not having experienced such an intervention:
• Life-long: No contact with any addiction related institution or with another institution, for which an explicit addiction related benefit has been mentioned
• Before remission: During the two years before remission no more than one contact to any institution and no experience at all with in-patient institutions
• Former problem gambler who accomplish both of the criteria would therefore count as auto-remitted individuals.
1st March 2005 HSA Berne, ISS 14
Experience with addiction related intervention
Objective classification:• 20 cases show no experience of any addiction
related intervention• Among these, there are 10 “objectively auto-
remitted“ cases• 44 cases show some experience of an addiction
related intervention
Subjective perception of such interventions:• 33 individuals report on no significant effects of
the intervention• Accordingly, 18 cases count as “subjectively auto-
remitted“
1st March 2005 HSA Berne, ISS 15
Experience with addiction related intervention
• Objective auto-remission rate: 53%, subjective auto-remission rate: 76.5%
• Individuals without any experience with addiction related intervention suffer from less severe gambling problems than those with such an experience
• „Social pressure“ as a motivation to quit is mentioned more often by auto-remitted gamblers (n=10) than by those who recovered with professional support (n=16). The latter group more often refers to the „omission of gambling possibilities“ as a motivation to quit
1st March 2005 HSA Berne, ISS 16
Experience with intervention
Problem gamblers interviewed reported following intervention experience:
• Out-patient psychiatric therapy• Out-patient psychological therapy• Social services and welfare institutions• In-patient psychiatric therapy• Self-help-groups, addiction counseling,
financial dept counseling, alcohol or drug clinic, family counseling
1st March 2005 HSA Berne, ISS 17
Objective barriers to treatment
• Lack of gambling specific treatment options
• Lack of knowledge by some professional helpers
1st March 2005 HSA Berne, ISS 18
Subjective barriers to treatment
• Denial of gambling problems• Overestimation of one‘s own
capabilities• No supposed benefit from
professional help • Fear/Shyness• Pride• Lack of knowledge of available
professional help
1st March 2005 HSA Berne, ISS 19
Main lessons
• Most important barrier to treatment: denial of gambling problems (How can professional helpers counter this barrier?)
• Auto-remission of problem gambling seems to be a fairly common fact in Switzerland (How can professional helpers support and learn from this group of former gamblers?)
1st March 2005 HSA Berne, ISS 20
Literature
• Ewing, J.A. (1984). Detecting alcoholism: the CAGE questionnaire, JAMA, 252, 1905-1907.
• Gerstein, D. et al. (1999b). NORC DSM-IV Screen for gambling problems (NODS). In: D. Gertein et al. (Eds.). Gambling impact and behavior study. Report to the national gambling impact study com mission. National Opinion Research Center at the University of Chicago. pp.18.
• Klingemann, H.K. (1988a). Autoremission bei Alkohol- oder Opiateabhängigen: Narratives Lebenslaufinterview. Lausanne: Schweizerische Fachstelle für Alkoholprobleme.
• Klingemann, H.K. (1988b). Autoremission bei Alkohol- oder Opiateabhängigen: Fragebogen für das telefonische Screeninginterview. Lausanne: Schweizersiche Fachstelle für Alkoholprobleme.
• Lesieur, H.R., & Blume, S.B. (1987). The south oaks gambling screen (SOGS): a new instrument for the identification of pathological gamblers, Am J Psychiatry, 144, 1184-1188.
• Osiek, C., Bondolfi, G., & Ferrero, F. (1999). Etude de prévalance du jeu pathologique en Suisse. Département de psychiatrie, Hôpitaux Universitaires de Genève.
• Petry, J. & Baulig, T. (1996b). Kurzfragebogen zum Glücksspielverhalten (KFG). In: J. Petry (Hg.). Psychotherapie der Glücksspielsucht. Weinheim: Psychologie Verlags Union. pp. 300.
1st March 2005 HSA Berne, ISS 21
Background Information
• A detailed report is available at: http://www.hsa.bfh.ch/forschung/pdf/Schlussbericht_Spielsucht_Voll.pdf
• At different stages of the project there was a cooperation with the Institute for Social and Preventive Medicine of the University of Zurich. The research team of this Institute on the other hand worked together with Dr A. Canziani, a practising psychiatrist specialised in treatment of gambling problems in Zurich
• Financial support: The research received financial support from the department for health and social issues of the canton Bern, from the DO-REsearch –Program set up for Universities of applied sciences, and, from the Swiss Casinos Holding (DORE: Swiss National Funds and Office for Professional Education and Technology (BBT= Bundesamt für Berufsbildung und Technologie)