passport to placement aero success we strive for excellence
TRANSCRIPT

Passport to Placement
Aero S
uccess
We S
trive for Excellence
Fulton County Department of Family and Children Services
Placement Passport
Child’s Name:___________
Placement: ____________ ____________ ____________
CONFIDENTIAL INFORMATION **This Placement Passport is to be kept by you as long as this child is in your care. Remember……When this child leaves your care, this Passport travels with the Child.
Fulton County Department of Family and Children Services
PLACEMENT PASSPORT TABLE OF CONTENTS
● PHOTO OF CHILD● ALL ABOUT ME!● MY PERSONAL DIRECTORY●PLACEMENT PASSPORT CHECKLIST● PLACEMENT PRESENTATION FORM● INITIAL CUSTODY FORM● COURT ORDER● FOSTER CHILD INFORMATION SHEET (469)● PASSPORT AGREEMENT FOR PLACEMENT● CLOTHING ALLOWANCE (Form 58)● SCHOOL ENROLLMENT FORM● CONSENT FOR MEDICAL AND DENTAL FORM● PHYSICAL EXAMNATION/DENTAL (IF APPLICABLE)● CPA/CCI PASSPORT PLACEMENT AGREEMENT● AGREEMENT SUPPLEMENT (FORM 40, DFCS ONLY)● DAYCARE FORM (FORM 57/1027)● PASSPORT FOR WOMEN, INFANT AND CHILDREN● GRADY ASSESSMENT/ PSYCHOLOGICAL (AGENCY USE ONLY)● PERSONAL PROPERTY INVENTORY (Entering Home)● PERSONAL PROPERTY INVENTORY (Exiting Home)
●
This Passport Belongs To:
PLACEMENT PASSPORT
Fulton County Department of Family and Children Services
Name: Nickname:
Date of Birth:
***This Placement Passport is to be kept by you as long as this child is in your care. Remember….when this child leaves your care, this Passport travels with the child.
4-PlyProviderFoster ParentResource CenterFoster Care Unit
Fulton County Department of Family and Children ServicesALL ABOUT ME!
Name: DOB:
Nickname: AGE:
School: Grade:
Weight: Height:
Hair Color: Eye Color:
Clothing Size: Shoe Size:
Favorite Color: Favorite Activity:
Things I Like to do:
What are my fears:
Places I like to go: Favorite Animals:4-PlyProviderFoster ParentResource CenterFoster Care Unit
Things I dislike doing:
Fulton County Department of Family and Children Services
Important Person’s Name:
Relationship
Address Phone Number &
My Personal Directory
Important People in My Life
***This Placement Passport is to be kept by you as long as this child is in your care. Remember...
when this child leaves your care, this Passport travels with the child.
4-PlyProviderFoster ParentResource CenterFoster Care Unit
Fulton County Department of Family and Children Services PLACEMENT PASSPORT CHECKLIST
NEW TO CARE □ DISRUPTION □ PLAN MOVE □ RESPITE □
Child NAME: ______________________________________ DOB: _______________ AGE: ______ GENDER:___________ PARTNERSHIPPARENT/CPA/CCI __________________________________________ DATE PLACED: __________________________
DATE RECEIVED DATE EXPECTEDBIRTH CERTIFICATE ( ) _______________ ______________
COURT ORDER ( ) _______________ ______________
SOCIAL SECURITY CARD (IF APPLICABLE) ( ) _______________ ______________
INITIAL CONTACT FORM ( ) _______________ ______________
EYE, EAR, DENTAL FORM ( ) _______________ ______________
CONSENT FOR MEDICAL OR DENTAL/MEDICAID CARD ( ) _______________ ______________
PHYSICAL EXAMINATION/DENTAL (If applicable) ( ) _______________ ______________
HOSPITAL DISCHARGE FORM (FAX TO HOSPITAL) ( ) _______________ ______________
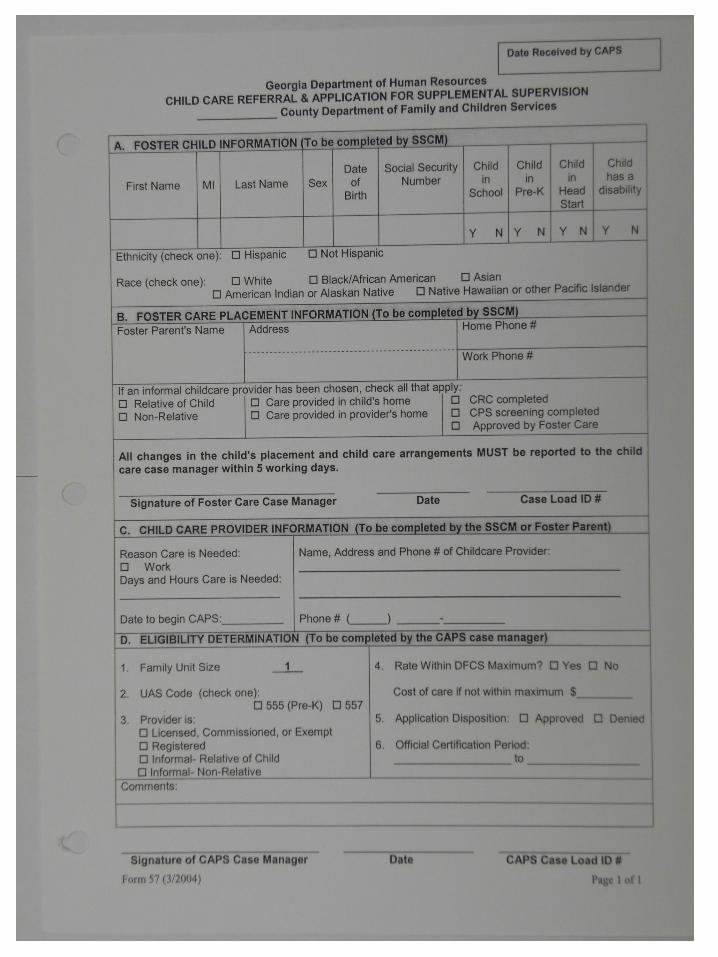
DAY CARE FORM (FORM 57/1027) ( ) _______________ ______________
FOSTER CHILD INFORMATIN SHEET (FORM 469) ( ) _______________ ______________
AGREEMENT SUPPLEMENT (FORM 40) (DFCS ONLY) ( ) _______________ ______________
INSTITUTIONAL AGREEMENT (PRIVATE AGENCY/GROUP HOME) ( ) _______________ ______________
AGENCY APPLICATION (IF APPLICABLE) ( ) _______________ ______________
WIC ( ) _______________ ______________
CLOTHING (FORM 48) ( ) _________________ _____________
SCHOOL ENROLLMENT ( ) _______________ ______________
GRADY ASSESSMENT / PSYCHOLOGICAL (Agency use only) ( ) _______________ ______________
*******************************************************************************************************************************************************************
PRO CASE MANAGER SIGNATURE: _________________________________________ DATE: ____________ TIME: _________________
PLACEMENT ASSISTANT SIGNATURE: ______________________________________ DATE: ____________ TIME: _________________
SUPERVISOR SIGNATURE: ________________________________________________ DATE: ____________ TIME: _________________
PARTNERSHIP PARENT/CPA SIGNATURE: __________________________________ DATE: ____________ TIME: _________________
4-PlyProviderFoster ParentResource CenterFoster Care Unit
Fulton County Department of Family and Children ServicesPLACEMENT PRESENTATION FORM
DATE: ___________________
CHILD’S NAME____________D.O.B:_____________AGE:______GENDER:_______
CASE NUMBER (if applicable): _________________________________________________________________________________________________________________
*Circumstances that brought child into Agency custody: _________________________
Family Resource Center Placement Assistance Unit (404) 762-4000 for School Records
Placement Assistance assigned to: ___________________Mobile:________________ (Name)Child’s Case Manager:_______________Office:______________Mobile: ___________CM Supervisor:_____________________Office:______________Mobile:___________Administrator:______________________Office:______________Mobile:___________
Fulton County 24-Hour Hotline (404-699-4399)(For all after hour’s emergencies regarding children in placement)
*****************************************************************************************************The initial FTM and Family Visitation will occur the same day as the Court hearings, Resource/Provider are expected to bring Child/Children to all pending Court Hearings.Name of School: __________________Addres____________________Grade:______ (Address) (City) (Zip)
Daycare/After School Program/Camp: ______________________________________ (Name / Address / Phone)*Known Medical Conditions/Concerns:____________________________________________________________________________________________________________
*Does this child have medication with Him/Her now? □ YES□NO
*Type of Placement □ DFCS □ CPA □ CCI Agency Name: _______________ Placement Name: ______________________________________________________
Address: _____________________________________________________________ (Address) (City) (Zip)
Phone/Contact Number's): _______________________________________________
PLACEMENT RESOURCE SUPERVISOR OR DESIGNEE: ____________________
4-PlyProviderFoster ParentResource CenterFoster Care Unit
Fulton County Department of Family and Children Services
INITIAL CUSTODY FORM
Date: ______________________
To: ________________________
In the Interest of:
Child: ___________________________ DOB: _________________
Child: ___________________________ DOB: _________________
Child: _ ____________ DOB: _________________Child DOB: _________________
By order of the Fulton County Juvenile Court the above named child (ren) are in the custody of Fulton County Department of Family and Children services.The above named child (ren) has (have) been placed in foster care by order of the Fulton County Juvenile Court and placed in a foster home for care.The Probable Cause (72 hour hearing)/FTM is scheduled for ________________________, after which a Family. (Date, Time, and Location)Team Meeting (FTM) will be held with all concerned parties invited. You may invite anyone that you feel has a vested interest in your family (i.e. relatives, teachers, neighbors, pastor etc.). We would like to strongly encourage you to attend these proceedings.If you have any questions or need any assistance, you may contact the following.
_________________, CPS Case Manager: Office: ______________ Cell: __________
_________________, CPS Supervisor: Office: _________________ Cell: __________
_________________, CPS Administrator: Office: _______________ Cell:___________
_________________, PLC Case Manager Office: _______________Cell: __________
_________________, PLC Supervisor Office: __________________Cell: _______ _________________,PLC Administrator: Office: ________________ Cell: ___________4-Ply
ProviderFoster ParentResource CenterFoster Care Unit

Fulton County Department of Family and Children Services
FOSTER CHILD INFORMATION SHEET
Child’s Name: _______________DOB: ______________ Age:________
Name Child likes to be called: __________________________
Medical history (disorders, allergies, dental history): ___________________________
Psychological and Social History: _________________________________________
School History (Last school attended, achievement level, school adjustment): ____________________________________________________________________________________
Why is child in foster care? ____________________________________________________________________________________
History of foster care (other families: where (city or part of town), and why child was moved): ____________________________________________________________________________________
Does child have special toy or object? Yes No Is it in his/her possession now? Yes No
Sleep patterns and rituals: _______________ Food preferences and dislikes: _____________________
Are pictures of natural family available? Yes No Does child have them with him/her now? Yes NoWhere is Paternal Family? _____________________________________________________________________________________Who are the members? _____________________________________________________________________________________Where is Maternal Family _____________________________________________________________________________________Who are the members? _____________________________________________________________________________________
Are siblings in foster care? Yes No Where? ________________________________________________
What are the plans for this child? __________________________________________________________
What are the Child’s current and past behaviors? ________________________________________________________________
Why is the Child coming from one placement to another? ___________________________________________________________
What is the Disruption? _____________________________________________________________________________________
Who is the assigned Doctor? ___________________________________ What is the Therapist Name? ______________________
Who does the Child receive counseling from? ___________________________________________________________________
Religious preferences (if any): _________________________________
Clothing preferences (colors and styles): ____________________________________________________
Favorite Foods? _______________________ Foods Child is allergic too (how long) _________________
Is child allergic to dairy products? ____Yes _____No
What is child’s bedtime? _______________ What clothing does child like to sleep in? _______________
Does child like to have a bedtime story read to him/her? Yes No If so Favorite book: ________________
Information provided by: _________________________ Date assigned to Casemanager: _____________
4-PlyProviderFoster ParentResource CenterFoster Care Unit

Fulton County Department of Family and Children Service
PASSPORT AGREEMENT FOR PLACEMENT WITH PARTNERSHIP PARENTS
NEW TO CARE □ DISRUPTION □ PLAN MOVE □ RESPITE □
PARTNERSHIP PARENT: _______________________ DATE PLACED: ____________
CHILD NAME: ___________________ DOB: __________ AGE: ______ GENDER: ____
CHILD NAME: ___________________ DOB: __________ AGE: ______GENDER: ____
CHILD NAME: ___________________ DOB: __________ AGE: ______GENDER: ____
CHILD NAME: ___________________ DOB: __________AGE: _______ GENDER: ___
CHILD NAME: ___________________ DOB: _________ AGE: _______ GENDER: ____
______________________, partnership parent with Fulton County(PARTNERSHIP PARENT NAME)
Department of Family and Children Services have agreed to accept the child/children listed above into his/her home for placement.
PARTNERSHIP PARENT SIGNATURE: __________________ DATE: ____________
PRO CM: ___________________________________________ DATE: ____________
PRO SUPERVISOR: _________________________________ DATE: ____________
________________________________________________________________________
If you are in need of immediate assistant within the next 48 hours, please contact:
CPS/PLC CM: ______________________OFFICE: ____________MOBILE:__________
CPS/PLC SUPERVISOR: _____________OFFICE:_____________MOBILE:_________
ADMINISTRATOR: ___________________OFFICE:_____________MOBILE:_________
4-PlyProviderFoster ParentResource CenterFoster Care Unit
Fulton County Department of Family and Children Services
Clothing Allowance
TO: __________________________________
FROM: __________________________________
RE: __________________________________
DATE: __________________________________
Dear ____________________________
I hereby authorize _____________________________________________to (Partnership Parent/CPA/CCI)purchase the following articles of clothing:
For _______________________DOB: ____________Age: ____ Sex: ______ (Child’s Name)
not to exceed the sum of $______________.
(Amount)Signed: ___________________________ Date: ________________
Supervisor’s Approval: ______________ Date: _________________ (Supervisor’s Signature)
CPS/PLC CM: ________________________Office: _____________Mobile: __________
CPS/PLC Supervisor: __________________Office: _____________Mobile: __________
Administrator: ________________________Office: _____________Mobile: __________
Form 584-PlyProviderFoster ParentResource CenterFoster Care Unit
Fulton County Department of Family and Children Services
SCHOOL ENROLLMENT FORM
DATE: ________________________________________
TO: ___________________________________________
FROM: FULTON COUNTY FAMILY RESOURCE CENTER
CHILD NAME: _________________ DOB: ______________ AGE: _____________
CHILD NAME: _________________ DOB: ______________ AGE: _____________
CHILD NAME: _________________ DOB: ______________AGE: ______________
CHILD NAME: _________________ DOB: ______________ AGE: ___________
The child/children listed above are in the legal custody of Fulton County Department of Family and Children Services. The child/children are currently placed in the home/Agency of: __________________________ (Agency Name Only)
________________________________________________________(PARTNERSHIP PARENT/CPA/CCI)
________________________________________________________ ADDRESS CITY ZIP
________________________________________________________PHONE NUMBER
_________________________________ is authorized to enroll the above named child/children in school. If you have additional questions, please contact me at the telephone number listed below.
CPS/PLC CM: __________________ OFFICE: _____________MOBILE:_________
CPS/PLC SUPERVISOR: _________ OFFICE: _____________MOBILE:_________
ADMINISTRATOR: ______________ OFFICE: _____________MOBILE:_________
***************************************************************************************************OFFICE LOCATION: FULTON COUNTY FAMILY RESOURCE CENTER (404) 762-4000
If you are in need of immediate assistant within the next 48 hours, please contact:PRO CM: _______________________OFFICE: _____________MOBILE: _______
PRO SUPERVISOR: ______________OFFICE: _____________MOBILE: ________
4-PlyProviderFoster ParentResource CenterFoster Care Unit
Fulton County Department of Family and Children Services
CONSENT FOR MEDICAL AND DENTAL CARE OF A FOSTER CHILD
CHILD’S NAME: __________________DATE OF BIRTH: _____________
MEDICAID NUMBER: ________________________
__________________________________County Department of Family (County)
and Children Services having legal custody of ______________________________________________________ does (CHILD’S NAME)
hereby give consent to _______________________________________ (PARTNERSHIP PARENT/ CPA/CCI)
and such agents of_________________________________________ with
whom the child may be placed in____________________ (PARTNERSHIP PARENT/ CPA/CCI)
Foster Care to authorize routine medical and dental care. All copies of medical records will be forwarded to assigned Case Manager.
Any request to authorize emergency medical treatment, such as emergency surgery, general anesthesia and blood transfusions, if necessary, shall be forwarded to the assigned Case Manager, Supervisor, Administrator or Program Director for prior approval.
________________________________________ Signature of Authorizing RepresentativeFulton County Department of Family and Children Services
_____________________________ Date
4-PlyProviderFoster ParentResource CenterFoster Care Unit
Fulton County Department of Family and Children Services
CPA/CCI PASSPORT PLACEMENT AGREEMENT
CHILD’S NAME: _______________ DOB: ___________ AGE: ____ GENDER: _____
CHILD’S SOCIAL SECURITY NUMBER__________SHINES CASE NUMBER: ______
CHILD’S MEDICAID NUMBER: _________________ DATE PLACED: _____________
NAME OF CPA/CCI:_________________________________________________ ADDRESS OF CPA/CCI: __________________________________________________
CITY__________________________ STATE: _____________ COUNTY: ___________
CONTACT PERSON: __________________TELEPHONE NUMBER: _____________
EMAIL ADDRESS: ______________________________________________________
This is an agreement between____________________________________ (NAME OF CPA/CCI AGENCY)and Fulton County Department of Family and Children
Service.______________________________________________________
(NAME OF CPA/CCI AGENCY)
agrees to provide care for _______________________________________.
(NAME OF CHILD)
The child’s per diem rate is currently $ ___________ per day.
RBWO CATEGORY:______________________
*************************************************************************************
If you have any questions, as it relates to this agreed, please contact the PRO CM or PRO Supervisor at the telephone numbers listed below.
PRO SUPERVISOR: _____________________TELEPHONE NUMBER: ___________
CPA/CCI CM: __________________________ TELEPHONE NUMBER: ___________
CPA/CCI SUPERVISOR: _________________TELEPHONE NUMBER: ___________
3-PlyProviderResource CenterFoster Care Unit
For contractual issues contact your Regional Supervisor
Opum Main (404)657-3572
3-PlyProviderResource CenterFoster Care Unit
OFFICE LOCATION: FULTON COUNTY FAMILY RESOURCE CENTER (404) 762-4000
Fulton County Department of Family and Children ServicesAGREEMENT SUPPLEMENT
(DFCS Foster Parent) _________________County Department of Family and Children ServicesCase Number: _____________________
(Foster Home)
I have this date (Received into) my home (Released from)__________________________DOB: _____________CASE # ____________
__________________________DOB: _____________CASE # ____________
__________________________DOB: _____________CASE # ____________
__________________________DOB: _____________CASE # ____________
__________________________DOB: _____________CASE # ____________
__________________________DOB: _____________CASE # ____________
From/To: ______________________________, ____________________County (NAME OF PERSON)
Department of Family and Children Services for/from foster care in accordance
with the agreement with the ____________________County Department of
Family and Children Services to provide Foster Care.
Signed: ______________________________
(Foster Father)
______________________________
(Foster Mother)
Date: ______________________ ______________________________ Representative of the _____________County Department of Family and Children ServicesForm 40
3-PlyFoster ParentResource CenterFoster Care Unit
Fulton County Department of Family and Children Services
PASSPORT FOR WOMEN, INFANT, AND CHILDREN SERVICES
TO: _______________________ COUNTY HEALTH DEPARTMENT
Name of Health Dept: _____________________Address: _______________Phone: ________
FROM: FULTON COUNTY FAMILY RESOURCE CENTER _________________________________________ (PRO CM NAME/TELEPHONE NUMBER)
DATE: _______________________
REASON: ____________________
CHILD NAME: _________________________DOB: __________ AGE: ______ GENDER: ____
CHILD NAME: _________________________ DOB: ___________AGE: ______ GENDER: ____
CHILD NAME: __________________________DOB: __________ AGE: _______GENDER: __
The child/children listed above are in the legal custody of Fulton County Department of Family and Children Services. The child/children are currently placed in the home of:
________________________________________(Partnership Parent/CPA/CCI)
________________________________________ Address City Zip
________________________________________(Phone Number)
________________________________ is responsible for the daily care of the child/children listed (PARTNERSHIP PARENT/ CPA/CCI NAME)
above Fulton County Family Resource Center is giving permission for _______________________ (PARTNERSHIP PARENT/ CPA/CCI NAME)
to receive WOMEN, INFANT, AND CHILDREN vouchers for the child/children listed above. If you are in need of immediate assistant within the next 48 hours, please contact:
CPS/PLC CM: ______________________ OFFICE: ________________MOBILE:____________
CPS/PLC SUPERVISOR: _____________ OFFICE: ________________MOBILE:____________
ADMINISTRATOR:___________________OFFICE:_________________MOBILE: ____________
4-PlyProviderFoster ParentResource CenterFoster Care Unit
Fulton County Department of Family and Children ServicesPersonal Property Inventory (Entering Home)
Child’s Name: Date:
Item Description Quantity Comments
4-PlyProviderFoster ParentResource CenterFoster Care Unit
Fulton County Department of Family and Children Services
Personal Property Inventory (Exiting Home)
Child’s Name: Date:
Item Description Quantity Comments
4-PlyProviderFoster ParentResource CenterFoster Care Unit