pass‐mrcog | physiologygynecology.sbmu.ac.ir/uploads/4_6037625812218282636.pdf · pass‐mrcog |...
TRANSCRIPT



PASS‐MRCOG | Physiology
Question 1 Angiogenesis and collagen deposition are features of which stage of wound healing? A) Haemostasis B) Proliferation C) Inflammation D) Maturation E) Remodelling Correct Answer:
Proliferation
Explanation: Collagen deposition and angiogenesis are features of the proliferation (or
granulation) stage. This stage involves fibroblasts laying down new extracellular matrix.
Reptilelialisation also occurs.
Question 2 The amniotic fluid volume peaks at around 900ml. At what gestation does the amniotic fluid reach its maximum volume? A) 28 weeks B) 32 weeks C) 35 weeks D) 38 weeks E) 40 weeks Correct Answer:
35 weeks
Explanation: The amniotic fluid volume increases up to week 35 of gestation and then
decreases from then to term.
Question 3 According to the UK food standards agency which of the following RDIs (recommended daily intake) is 3 times higher in pregnancy than the non‐pregnant state? A) Iron B) Vitamin A C) Folic Acid D) Vitamin C E) Vitamin D

PASS‐MRCOG | Physiology
Correct Answer:
Folic Acid
Explanation: The RDI for folate increases 3 fold for the first trimester of pregnancy.
Vitamin C and iron RDIs are increased but less than double
Question 4 A patient asks you how long it will be before her C‐section wound is "at full strength." What is the typical time taken for wounds closed by primary intention to reach full tensile strength? A) 3 weeks B) 6 weeks C) 12 weeks D) 24 weeks E) 36 weeks Correct Answer:
12 weeks
Explanation: Remodeling is usually underway by week 3. Maximum tensile wound strength is
typically achieved by week 12.
Question 5 Which of the following statements regarding thyroid function testing in pregnancy is true? A) TSH levels increase in pregnancy B) TSH levels remain constant through the trimesters C) Total T3 levels drop in pregnancy D) Free T3 levels drop during pregnancy E) Thyroid hormone binding globulin levels drop during pregnancy Correct Answer: Free T3 levels drop during pregnancy Explanation: Maternal FreeT4 (FT4) and Free T3 (FT3) rather than total hormone concentrations must be measured in pregnancy. This is because Total T4 and Total T3 increase in pregnancy due to increased serum concentrations of thyroid hormone binding proteins.
It is only the FT3 and FT4 fraction (not the bound fraction) than can enter cells and modify metabolism. Trimester-specific reference ranges for FT3 and FT4 need to be used.

PASS‐MRCOG | Physiology
TSH levels are typically lower in pregnancy and there is a different reference range for each trimester.
Question 6 Regarding heart rate in pregnancy which of the following statements is true? A) Heart rate decreases by 15 beats per minute B) Heart rate remains constant C) Heart rate increases by 15 beats per minute D) Heart rate increases by 25 beats per minute E) None of the above Correct Answer: Heart rate increases by 15 beats per minute Explanation: During pregnancy heart rate increases by approximately 15 beats per minute above baseline
Question 7 What percentage of haemoglobin is HbF in the newborn? A) <0.5% B) 1‐2% C) 10‐20% D) 25‐50% E) 50‐90% Correct Answer: 50‐90% Explanation: Different sources quote varying levels. Often 90% is quoted. Electrophoresis studies have shown around 70% of haemoglobin is HbF at birth
Question 8 Cardiac output is calculated by A) End diastolic volume X End systolic volume B) End diastolic volume ‐ End systolic volume C) End diastolic volume X Stroke volume D) Stroke Volume X Heart Rate E) End Systolic Volume X Heart Rate

PASS‐MRCOG | Physiology
Correct Answer: Stroke Volume X Heart Rate Explanation: Cardiac Output = Stroke Volume X Heart Rate Stroke Volume = End Diastolic Volume ‐ End systolic volume
Question 9 What is the average lifespan of a basophil (white blood cell)? A) 3‐4 days B) 10‐14 days C) 30 days D) 60 days E) 120 days Correct Answer: 3‐4 days Explanation: Blood Cells Blood Cell Lifespans
Red Blood Cells 120 days Platelets 5‐9 days White blood cells 2‐5 days
Neutrophils (up to 5 days) Basophils (2 to 3 days) Eosinophls (2 to 5 days) Monocytes (1 to 5 days) Lymphocytes (variable)
Question 10 Oxytocin causes increased myometrial contractions via which of the following messenger pathways? A) Activates phospholipase‐C which produces IP3 which triggers intracellular Calcium ion release B) Releases cAMP that triggers intracellular Calcium ion release C) Releases protein kinase A that triggers intracellular Calcium ion release D) Releases protein kinase A that triggers extracellular Calcium ion release E) None of the above

PASS‐MRCOG | Physiology
Correct Answer: Activates phospholipase‐C which produces IP3 which triggers intracellular Calcium ion release
Explanation: Oxytocin activates phospholipase C to produce inositol 1,4,5‐trisphosphate (IP3),
which releases Ca2+ from intracellular stores.
There are thought to be other mechanisms by which myometrium is stimulated by Oxytocin
including increased sensitisation of the myometrium and increased calcium entry into cells.
cAMP and Protein Kinase A inhibit myometrial contractility.
Question 11 Where in the kidney is the majority of Bicarbonate reabsorbed A) Bowmans Capsule B) Proximal Convoluted Tubule C) Descending Loop of Henle D) Ascending Loop of Henle E) Distal Convoluted Tubule Correct Answer: Proximal Convoluted Tubule Explanation: If you are unsure when asked where in the kidney the majority of reabsorption of
ANY ion occurs then put the PCT as your answer.
As you can see from the list below it is the main reabsorption (termed reabsorption as primary
absorption takes place in the intestines) site for almost all ions.
The PCT reabsorbs the following:
Glucose 100% Amino Acids 100% Carboxylate 100% Bicarbinate 85% Phosphate 85% Potassium 65% Sodium 65% Urea 50% Calcium, Magnesium and Water variable reabsorption through nephron

PASS‐MRCOG | Physiology
Question 12 What is the primary form of haemoglobin in a 6 week old foetus? A) Hb Gower 1 B) Hb Gower 2 C) Hb Portland 1 D) Hb Portland 2 E) HbF Correct Answer: Hb Gower 1 Explanation: For the first 10‐12 weeks of fetal development Embryonic Haemoglobin (HbE) is
the primary form of haemoglobin. It is produced by the Yolk Sac from the 1st week of
pregnancy until birth.
It is a tetramer consisting of Gower 1, Gower 2, Portland 1 and Portland 2. Of these four
subtypes Gower 1 is the primary form.
After 10‐12 weeks Fetal Haemoglobin (HbF) becomes the primary form and comprises 50‐90%
of haemoglobin at birth. It is almost completely replaced by adult haemoglobin by 6 months of
age.
Question 13 Placental production of hPL, hCG, Oestragen and Progesterone are examples of which type of mechanism A) Endocrine B) Exocrine C) Apocrine D) Autocrine E) Intracrine Correct Answer: Endocrine
Explanation: Hormones that are secreted into the circulation at one site but have effects on
distal target organs are endocrine as is the case with the hormones above.

PASS‐MRCOG | Physiology
Autocrine and Intracrine messengers act within the same cell.
Exocrine glands secrete their products into ducts. Apocrine is a histological term used to
describe some types of exocrine gland.
Question 14 Regarding the closure of the ductus arteriosus (DA) after birth which of the following most accurately describes the mechanisms leading to closure of the DA? A) Increased arterial pO2, decreased bradykinin & decreased Prostaglandin E2 B) Increased arterial pO2, decreased bradykinin & decreased Prostaglandin E1 C) Increased arterial pO2, increased bradykinin & decreased Prostaglandin E2 D) Increased arterial pO2, increased bradykinin & increased Prostaglandin E2 E) None of the above Correct Answer: Increased arterial pO2, increased bradykinin & decreased Prostaglandin E2
Explanation: Normal closure of the ductus arteriosus (DA) is brought about by a number of
mechanisms.
Upon delivery the new born babies first breath inflates the lungs and this causes a rise in pO2.
Oxygen is known to cause constriction of the DA in vivo and in vitro. In addition the decreased
vascular resistance means the pressure within the lumen of the DA drops aiding closure.
In addition on inflation of the lungs, the lungs produce bradykinin which stimulates smooth
muscle constriction of the ductus.
The most important factor is thought to be the drop in Prostaglandin E2. Prostaglandin E2
maintains patency of the Ductus in the unborn child but after birth is metabolised in the lungs
and its levels fall rapidly within 3 hours of birth.

PASS‐MRCOG | Physiology
Question 15 What is the typical volume increase from a non‐pregnant to term uterus? A) 10ml to 5000ml B) 100ml to 500ml C) 1000ml to 5000ml D) 10ml to 1000ml E) 40ml to 1200ml Correct Answer: 10ml to 5000ml Explanation: Uterine Growth
Non‐pregnant uterus
Weight 40‐50g Volume approx 10ml
Term uterus
Weight 1100‐1200g Volume approx 5000ml
Question 16 Which of the following is a potent stimulator of Aldosterone A) Alkolosis B) Acidosis C) Hypokalaemia D) Hyperkalaemia E) Hypernatraemia Correct Answer: Hyperkalaemia Explanation: Hyperkalaemia is arguably the most potent stimulator of Aldosterone.
Juxtaglomerular cells will also secrete Renin (that will ultimately stimulate aldosterone
production) in response to Hyponatreamia and hypotension.

PASS‐MRCOG | Physiology
Question 17 Following parturition uterine contractions called Afterpains may typically continue for how long? A) 2‐3 hours B) 12‐24 hours C) 7‐14 days D) 21‐28 days E) None of the above Correct Answer: None of the above Explanation: Afterpains may continue for 2‐3 days (so none of the above).
Breastfeeding may intensify pain due to stimulation of Oxytocin which causes uterine
contractions
Question 18 At what gestational age does the luteo‐placental shift occur? A) 1‐2 weeks B) 6‐8 weeks C) 18‐20 weeks D) 24‐28 weeks E) 32‐36 weeks Correct Answer: 6‐8 weeks Explanation: The luteo‐placental shift refers to the point in time where the placenta takes over
from the corpus luteum as the chief site for production of oestrogen and progesterone in
sufficient amounts to maintain pregnancy.
This typically occurs around 6‐8 weeks gestation

PASS‐MRCOG | Physiology
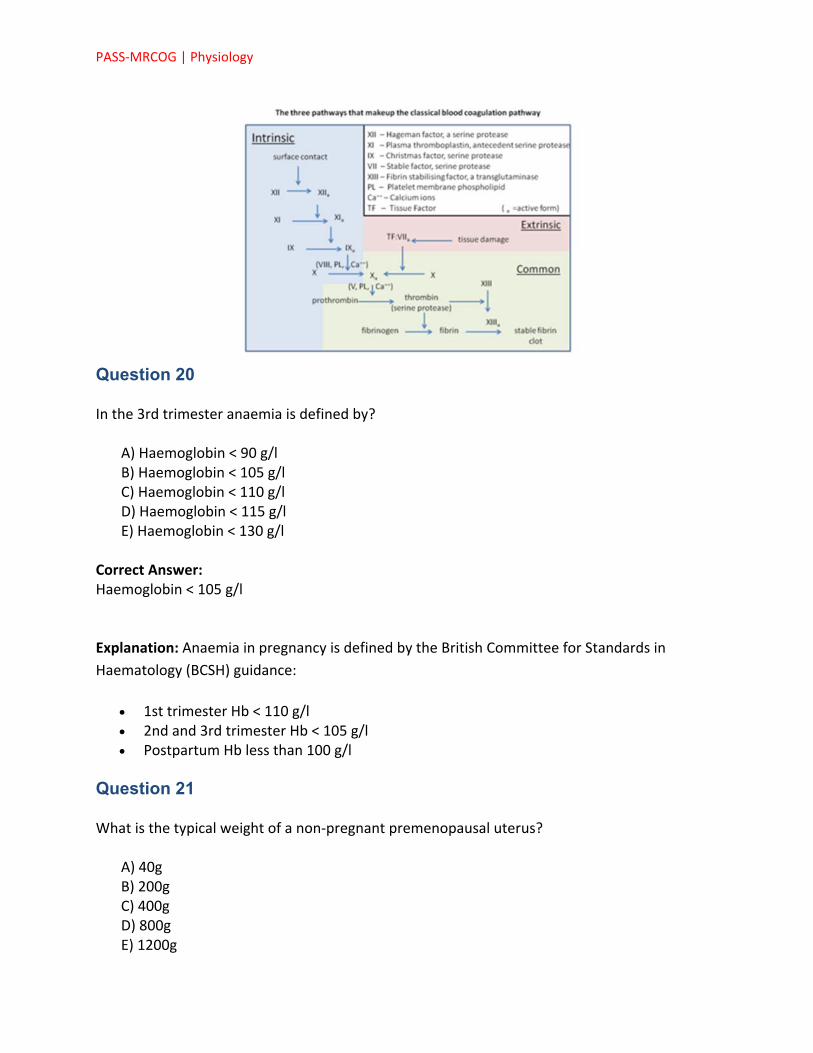
Question 19 During wound healing the clotting cascade is activated. Which of the following activates the intrinsic pathway? A) Fibrin B) Damaged endothelium C) Tissue Factor D) Thrombin E) Prothrombin Correct Answer: Damaged endothelium Explanation: The clotting cascade can be activated either by damaged endothelium (Intrinsic
pathway) or Tissue Factor (Extrinsic pathway)
Image sourced from Wikipedia
PASS‐MRCOG | Physiology
Question 20 In the 3rd trimester anaemia is defined by? A) Haemoglobin < 90 g/l B) Haemoglobin < 105 g/l C) Haemoglobin < 110 g/l D) Haemoglobin < 115 g/l E) Haemoglobin < 130 g/l Correct Answer: Haemoglobin < 105 g/l Explanation: Anaemia in pregnancy is defined by the British Committee for Standards in
Haematology (BCSH) guidance:
1st trimester Hb < 110 g/l 2nd and 3rd trimester Hb < 105 g/l Postpartum Hb less than 100 g/l
Question 21 What is the typical weight of a non‐pregnant premenopausal uterus? A) 40g B) 200g C) 400g D) 800g E) 1200g

PASS‐MRCOG | Physiology
Correct Answer: 40g Explanation: Uterine Growth
Non‐pregnant uterus
Weight 40‐50g Volume approx 10ml
Term uterus
Weight 1100‐1200g Volume approx 5000ml
Question 22 You review a 58 year old patient in clinic. She asks what the results of her recent DEXA scan are. You note her hip BMD hip T‐score is ‐1.4. You note she has a history of olecranon fracture 4 years ago. What is her classification according to WHO criteria? A) Normal bone density B) Osteopenia C) Severe Osteopenia D) Osteoporosis E) Severe Osteoporosis Correct Answer: Osteopenia Explanation: Her T‐score puts her in the osteopenic range.
The presence of fragility fractures is more important in the osteoporotic patient. Olecranon
frature is not a typical fragility fracture.
Question 23 Which of the following is a primary site of Prostaglandin E2 (PGE2) production? A) Corpus Luteum B) Ductus Venosus C) Placenta D) Hypothalamus E) Maternal liver

PASS‐MRCOG | Physiology
Correct Answer: Placenta Explanation: Prostaglandins are produced in almost all nucleated cells. The placenta and ductus
arteriosus in particular have high quantities of the COX enzyme isoforms required for synthesis
of PGE2.
Question 24 Which of the following lung function values is unchanged in pregnancy? A) FRC B) ERV C) FEV1 D) Tidal Volume E) ERV Correct Answer: FEV1 Explanation: FEV1 and FVC are unchanged. FEV1/FVC ratio remains the same in pregnancy
Question 25 During pregnancy which hormone(s) inhibit lactogenesis? A) Prolactin B) Oxytocin C) Oestrogen and Progesterone D) Prolactin and hPL (human Placental Lactogen) E) Oxytocin and hPL
Correct Answer: Oestrogen and Progesterone Explanation: Prolactin levels rise steadily during pregnancy during which time it promotes
mammary growth (along with the other hormones mentioned below). Oestrogen and
progesterone inhibit lactogenesis and it is only with the loss of these placental steroid
hormones at term that Prolactin exhibits its lactogenic effect.

PASS‐MRCOG | Physiology
Question 26 In the earliest phase of wound healing platelets are held together by what?
A) Fibroblasts B) Type 2 Collagen C) Type 1 Collagen D) PGE1 E) Fibrin
Correct Answer: Fibrin Explanation: The 1st stage of wound healing is haemostasis. Even in incised wounds a small
haematoma forms. Here the clotting cascade is activated by tissue factor and endothelial cells
resulting in activation of platelets. This results in platelet aggregation and the laying down of a
fibrin mesh that is cross linked and holds the platelets in place.

PASS‐MRCOG | Physiology
Question 27 Regarding cardiac examination during pregnancy which of the following findings should be considered pathological
A) Diastolic murmur B) T‐wave flattening in lead III on ECG C) Systolic murmur D) Left axis deviation on ECG E) Third heart sound
Correct Answer: Diastolic murmur Explanation: Diastolic murmurs should be considered pathological until proven otherwise.
The following are common and typically benign findings in pregnancy:
A third heart sound after mid‐pregnancy. Systolic flow murmurs are common. Left axis deviation on ECG is common, Sagging ST segments and inversion or flattening of the T wave in lead III may also occur
Question 28 During pregnancy the GFR changes as follows:
A) GFR remains the same B) GFR decreases by 15% C) GFR increases by 15% D) GFR decreases by 40% E) GFR increases by 40%
Correct Answer: GFR increases by 40% Explanation: GFR increases by about 40% during pregnancy and that is typically apparent by the
end of the 1st trimester.

PASS‐MRCOG | Physiology
Question 29 Where in the kidney is the majority of Bicarbonate reabsorbed
A) Bowmans Capsule B) Proximal Convoluted Tubule C) Loop of Henle D) Distal Convoluted Tubule E) Collecting Duct
Correct Answer: Proximal Convoluted Tubule Explanation: If you are asked where in the kidney the majority of reabsorption of ANY ion
occurs then put the PCT as your answer.
As you can see from the list below it is the main reabsorption (termed reabsorption as primary
absorption takes place in the intestines) site for almost all ions.
The PCT reabsorbs the following:
Glucose 100% Amino Acids 100% Carboxylate 100% Bicarbinate 85% Phosphate 85% Potassium 65% Sodium 65% Urea 50% Calcium, Magnesium and Water variable reabsorption throughout nephron
Question 30 During wound healing collagen alignment along tension lines is part of which phase?
A) Haemostasis B) Inflammation C) Granulation D) Proliferation E) Remodelling
Correct Answer: Proliferation

PASS‐MRCOG | Physiology
Explanation: Realignmnet of collagen is part of the remodeling phase. Remodeling is usually
underway by week 3. Maximum tensile wound strength is typically achieved by week 12.
Question 31 Which of the following tests is used to detect antibodies or complement bound to red blood cell antigens in vivo?
A) Direct Coombs B) Indirect Coombs C) Guthrie D) Mantoux E) Heaf
Correct Answer: Direct Coombs Explanation: This describes the direct Coombs test
Question 32 Which of the following hormones inhibits Galactopoiesis and Lactogenesis postpartum?
A) Oxytocin B) Progesterone C) Dopamine D) hPL E) Prolactin
Correct Answer: Dopamine Explanation: Galactopoiesis and Lactogenesis are stimulated by Prolactin. Dopamine released
under hypothalamic control inhibits Prolactin production.
Note estrogen and progesterone inhibit lactogenesis up until term.
Question 33 Several mechanisms have been proposed as to what causes closure of the Ductus Arteriosus (DA) at Parturition. Which of the following is the most important in maintaining the patency of the DA during pregnancy?

PASS‐MRCOG | Physiology
A) Oxytocin B) Progesterone and Oestragen C) PGE2 D) PGE1 E) Prolactin
Correct Answer: PGE2 Explanation: Prostaglandin E1 and E2 help maintain the patency of the DA during pregnancy.
PGE2 is by far the most potent and important. It is produced in large quantities by the placenta
and the DA itself.
Question 34 You review a patient who is 34 weeks pregnant. She complains of gradually worsening itching over the past 6 weeks particularly to the hands and feet which is worse at night. You order some bloods. Which of the following would you normally expect to increase in the 3rd trimester?
A) ALT B) ALP C) Bilirubin D) Albumin E) Calcium
Correct Answer: ALP Explanation: ALP can rise to up to 3 times the normal non‐pregnant value in the 3rd trimester.
All of the other tests above typically decrease during pregnancy.
Question 35 Lactogenesis at term is stimulated by which hormone?
A) Oxytocin B) hPL C) Progesterone D) Prolactin E) Dopamine

PASS‐MRCOG | Physiology
Correct Answer: Prolactin
Explanation: Lactation
Oxytocin stimulates the milk ejection reflex (let‐down) in response to suckling. Galactopoiesis is maintained via the action of Prolactin. Alveolar gland proliferation and differentiation occurs under the actions of Oestragens,
Progesterone, HPL and prolactin. Prolactin stimulates Lactogenesis when not inhibited
Question 36 Regarding the use of Erythropoietin (recombinant human erythropoietin AKA rHuEPO) in pregnancy which of the following statements is correct?
A) rHuEPO has been shown to be have adverse maternal effects when used
antenatally B) rHuEPO has been shown to be have adverse fetal effects when used antenatally C) rHuEPO has been shown to be have adverse neonatal effects when used
antenatally D) The use of rHuEPO is only recommended for non‐end‐stage renal anaemia E) None of the above
Correct Answer: None of the above Explanation: The Greentop Guidelines state the following:
Recombinant human erythropoietin (rHuEPO) is mostly used in the anaemia of end‐stage renal
disease. rHuEPO has been used both antenatally and postpartum in women without end‐stage
renal disease without any adverse maternal, fetal or neonatal effects.
Use rHuEPO in clinical practice for non‐end‐stage renal anaemia is still to be established and
should only be used in the context of a controlled clinical trial.
PASS‐MRCOG | Physiology
Question 37 During wound healing the clotting cascade is activated. Which of the following activates the extrinsic pathway?
A) Damaged endothelium B) Thromboxane A2 C) Prostaglandin E2 D) Tissue Factor E) Fibrin
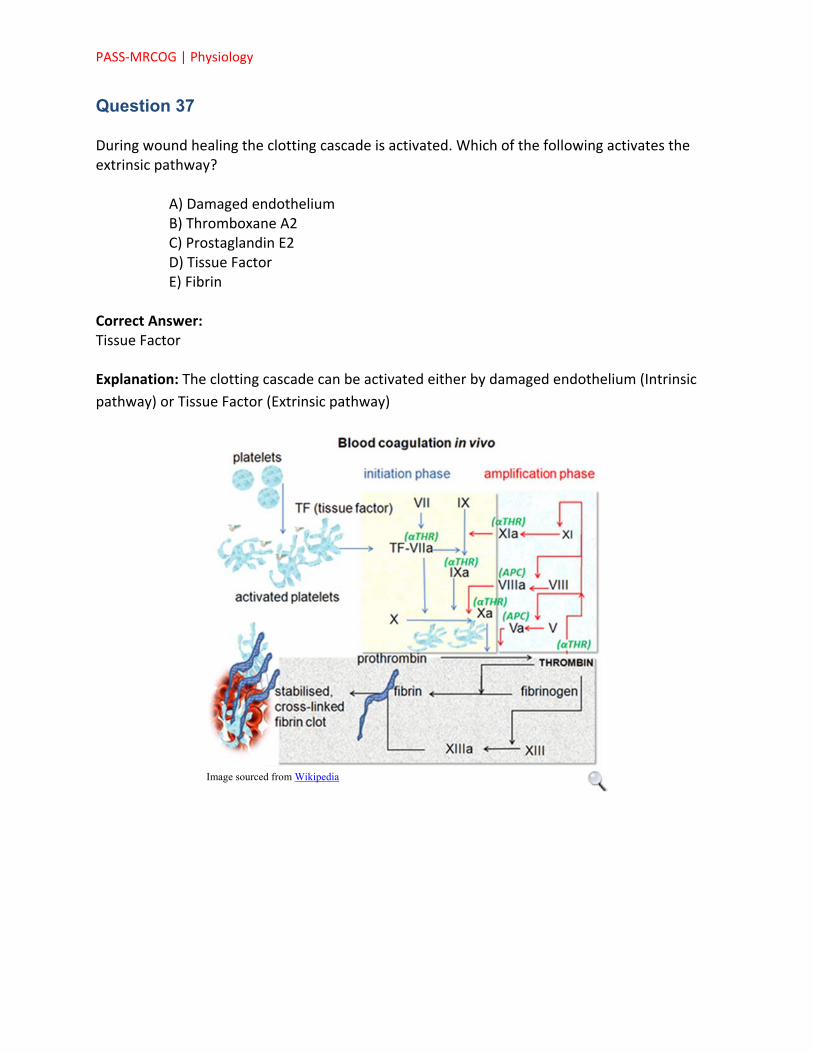
Correct Answer: Tissue Factor Explanation: The clotting cascade can be activated either by damaged endothelium (Intrinsic
pathway) or Tissue Factor (Extrinsic pathway)
Image sourced from Wikipedia

PASS‐MRCOG | Physiology
Question 38 During wound healing the clotting cascade is activated. Which of the following activates the extrinsic pathway?
A) Shortening of the cervix B) Dilatation of the cervix C) Descent of the baby D) Birth of the baby E) Expulsion of the placenta and membranes
Correct Answer: Expulsion of the placenta and membranes Explanation: The third stage lasts from the delivery of baby to the delivery of placenta and
membranes
Question 39 Which of the following is the primary stimulator of uterine involution following child birth??
A) Oxytocin B) Prolactin C) FSH D) Progesterone E) LH
Correct Answer: Oxytocin

PASS‐MRCOG | Physiology
Explanation: Oxytocin is the primary stimulus for uterine involution following childbirth.
Question 40 A 52 year old patient attends clinic for the results of her bone density scan. Her T‐score is ‐2.2. She tells you she has previously fractured her 5th metatarsal and patella following a fall from a bike. You diagnose her as:
A) Normal bone density B) Osteopenic C) Severely Osteopenic D) Osteoporosis E) Severely Osteoporotic
Correct Answer: Osteopenic Explanation: The fracture history here is irrelevant especially considering neither are fragility
fractures.
T‐score 0 to ‐1 Normal bone density
T‐score ‐1 to ‐2.5 Osteopenia
T‐score ‐2.5 or less Osteoporosis
Question 41 Pregnant patients are at higher risk of thromboembolism due to a hypercoaguable state. Which of the following clotting factors reduces during pregnancy?
A) Factor II B) Factor VII C) Fibrinogen D) Factor X E) Factor XI
Correct Answer: Factor XI Explanation: he hyper‐coaguable state is thought to result primarily from the increased levels
of factor VII and fibrinogen. Other clotting factors also rise (VIII,IX,X,XII) and physiological
anticoagulants such as Protein S level reduce.
Clotting factors XI and XIII reduce during pregnancy

PASS‐MRCOG | Physiology
Question 42 When using the MDRD formula to calculate GFR (Glomerular filtration rate) which of the following is not factored into the equation?
A) Creatinine B) Urea C) Sex D) Age E) Ethnic Background
Correct Answer: Urea Explanation: The MDRD takes ethnicity into account as GFR is increased by 1.2 if the patient is
of black ethnicity. Urea is not used.
Question 43 Where in the kidney is the majority of Sodium and Glucose reabsorbed
A) Bowmans Capsule B) Loop of Henle C) Proximal Tubule D) Distal Tuble E) Collecting Duct
Correct Answer: Proximal Tubule Explanation: Remember PCT is the main site for Reabsorption for all ions!
As you can see from the list below it is the main reabsorption (termed reabsorption as primary
absorption takes place in the intestines) site for almost all ions.
The PCT reabsorbs the following:
Glucose 100% Amino Acids 100% Carboxylate 100% Bicarbinate 85% Phosphate 85% Potassium 65%

PASS‐MRCOG | Physiology
Sodium 65% Urea 50% Calcium, Magnesium and Water variable reabsorption throughout nephron
Question 44 At what gestation does the fetus typically start swallowing? A) 6 weeks B) 12 weeks C) 18 weeks D) 24 weeks E) 32 weeks Correct Answer: 12 weeks
Explanation: Amniotic Fluid
Fetal contribution to amniotic fluid Fetal Urine
First fetal urine produced at 8‐11 weeks By term fetus produces approximately 800ml urine per day
Fetal Swallowing
Fetus starts swallowing 12 weeks 250ml swallowed per day
Fetal Lung Secretions
300ml/day by 2nd trimester
Question 45 Dilatation of the uterine cervix at parturition is primarily achieved by: A) Muscle relaxation under the influence of oestriol B) Prostaglandin E1 mediated Interleukin release C) Constriction of cervical small vessels D) Macrophage mediated collagen degradation E) Degradation of type I collagen by interstitial collagenase

PASS‐MRCOG | Physiology
Correct Answer: Degradation of type I collagen by interstitial collagenase Explanation: Cervical ripening refers to the softening of the cervix prior to labour. It is a
complex process that involves the following processes (the key point is type 1 collagen
breakdown by collegenase):
Increased activity of metalloproteinases 2 & 9 that degrade extracellular matrix proteins.
Cervical collagenase and elastase also increase and degradation of collagen increases, leading to decreased collagen content in the cervix.
Increased oestrogen leads to increased collagenase activity ‐ Increase COX2 causing increased prostaglandin E2 (PGE2) in the cervix
PGE2 leads to:
Increase in collagen degradation
Increase in hyaluronic acid
Increase in chemotaxis for leukocytes, which causes increased collagen degradation
Increase in stimulation of interleukin (IL)8 release
Prostaglandin F2‐alpha is also involved in the process via its ability to stimulate an increase in
glycosaminoglycans.
Question 46 What is the typical oxygen consumption in a 75kg non‐pregnant women? A) 5ml/min B) 15ml/min C) 50ml/min D) 150ml/min E) 250ml/min Correct Answer: 250ml/min Explanation: The typical Oxygen Consumption (VO2) is 250ml/min.
In pregnancy this increases by around 20% to 300ml/min

PASS‐MRCOG | Physiology
Question 47 Regarding blood volume in pregnancy which of the following statements is TRUE? A) Blood volume remains constant B) Blood Volume increases by approximately 5% C) Blood Volume increases by approximately 10‐15% D) Blood Volume increases by approximately 20‐25% E) Blood Volume slowly increases by 40‐50% Correct Answer: Blood Volume slowly increases by 40‐50% Explanation: During pregnancy blood volume increases slowly by 40‐50%. The increase is
thought to be due to increased Aldosterone. The rise in volume mostly occurs during the 1st
trimester
Question 48 What is the primary form of haemoglobin in a 18 week old foetus? A) Hb Gower 1 B) Hb Gower 2 C) Hb Portland 1 D) Hb Portland 2 E) HbF Correct Answer: HbF Explanation: The cut off here is 10‐12 weeks of fetal development.
Prior to 12 weeks Embryonic Haemoglobin (mainly Hb Gower 1) is the primary form After 12 weeks Fetal Haemoglobin (HbF) is the primary form
Question 49 What is the typical peak change in oxygen consumption in a pregnant vs a non‐pregnant women? A) 5% B) 20% C) 60%

PASS‐MRCOG | Physiology
D) 100% E) 120% Correct Answer: 20% Explanation: The typical Oxygen Consumption (VO2) is 250ml/min.
In pregnancy this increases by around 20% (or 50ml/min) to 300ml/min
Question 50 Which structure is the primary mechanism for shunting blood away from the fetal pulmonary circulation? A) Foramen Ovale B) Ductus Arteriosis C) Arteria Umbilicalis D) Ductus Venosus E) Umbilical Arteries Correct Answer: Foramen Ovale Explanation: Blood enters the right atrium of the fetal heart and most passes through the
foramen ovale into the left atrium. From there it is pumped through the aorta. The foramen
ovale is the major structure for bypassing the fetal pulmonary circulation.
Some of the blood in the right atrium does enters the right ventricle and then into the
pulmonary artery however most of this passes through the ductus arteriosus into the aorta thus
bypassing the fetal pulmonary circulation.
Question 51 Which of the following changes to biliary physiology occurs during pregnancy?
A) Increased canalicular excretion B) Increased water content of bile C) Increased contractility of gallbladder D) Increased lithogenic index E) Increased rate of gallbladder emptying

PASS‐MRCOG | Physiology
Correct Answer: Increased lithogenic index Explanation: The lithogenic index increases in pregnancy hence the greater risk of gallstones.
Lithogenicity refers to the promotion of calculi formation and the lithogenic index is a
numerical measure of the relative lithogenicity of bile.
Question 52 Which of the following is responsible for Aquaporin‐2 protein channel openings in the collecting duct? A) Angiotensin B) Angiotensin II C) ADH D) Aldosterone E) Renin Correct Answer: ADH
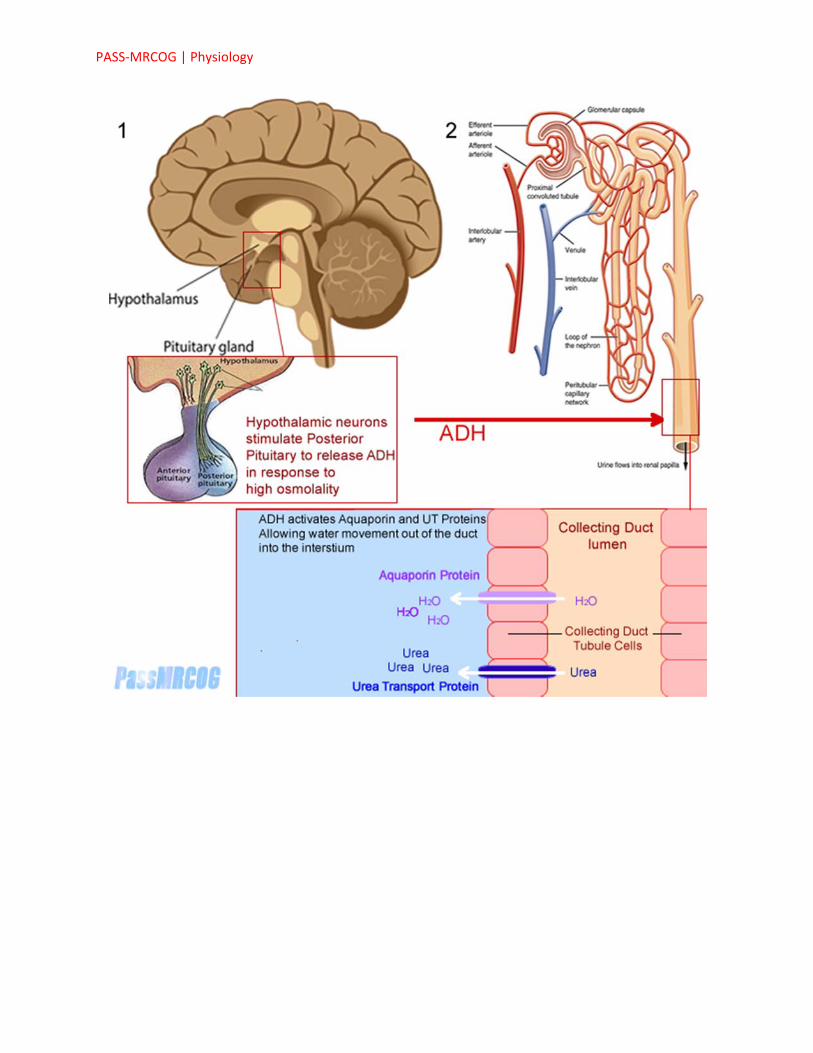
Explanation: Vasopressin
Vasopressin (also known as Arginine Vasopressin, AVP, Anti‐Diuretic Hormone and ADH) is released from the posterior pituitary gland and promotes water retention by the following methods
Insertion of water channel proteins called aquaporins into the collecting duct and DCT Increased activity of urea transport proteins in the collecting duct promoting urea flow
out of the collecting duct and water via increased osmotic gradient Increased sodium reabsorption across the ascending loop of Henle
Stimulation Receptors in the Hypothalamus detect increases in serum osmolality and stimulate the posterior pituitary to secrete ADH. This is the main stimulus. Vasopressin is also a vasoconstrictor and is stimulated when decreases in plasma volume are detected by baroreceptors in the atria and carotid sinus
PASS‐MRCOG | Physiology

PASS‐MRCOG | Physiology
Question 53 Aldosterone promotes water retention via which of the following mechanisms? A) Up‐regulation of Aquaporin protein channels in the collecting duct B) Up‐regulation of urea transport proteins in the collecting duct C) Down‐regulation of urea transport channels in the collecting duct D) Up‐regulation of the sodium/potassium pumps in the distal tubule and collecting duct E) Stimulation of Potassium resorption in the tubular lumen Correct Answer: Up‐regulation of the sodium/potassium pumps in the distal tubule and collecting duct Explanation: Aldosterone stimulates Sodium resorption in the kidney via the mechanisms
described below. Up‐regulation of Aquaporin and Urea Transport proteins are mechanisms of
water retention stimulated by Vasopressin (ADH).
Question 54 During the inflammatory phase of wound healing what is the predominant cell type found in the wound during the first 48 hours? A) Macrophages B) Polymorphonuclear Neutrophils (PMNs) C) Fibroblast D) Lymphocytes E) B‐cells Correct Answer: Polymorphonuclear Neutrophils (PMNs) Explanation: During the inflammatory phase (which overlaps the haemostasis phase)
fibronectin and growth factors attract PMNs to the wound site. These are the predominant cell
type for the first 2 days.
PMNs phagocytise debris and kill bacteria via free radicals (AKA respiratory burst). They also
break down damaged tissue. PMNs typically undergo apoptosis after 48 hours. They are then
engulfed and degraded by macrophages. Macrophages therefore become the predominant cell
type in the wound on days 3‐4.

PASS‐MRCOG | Physiology
Question 55 What is the average lifespan of a red blood cell? A) 3‐4 days B) 10‐14 days C) 30 days D) 90 days E) 120 days Correct Answer: 120 days Explanation: Blood Cell Lifespans
Red Blood Cells 120 days Platelets 5‐9 days White blood cells 2‐5 days
Neutrophils (up to 5 days)
Basophils (2 to 3 days)
Eosinophls (2 to 5 days)
Monocytes (1 to 5 days)
Lymphocytes (variable)
Question 56 Apatientattendsthematernityunitasherwatershavebrokenbutshehasn'thadcontractions.Sheis39+6weeksgestation.Speculumexaminationconfirmsprelabourruptureofmembranes.Whatisthelikelihoodofspontaneouslabourstartingwithin24hours?A)5%B)25%C)40%D)60%E)90%CorrectAnswer:60%

PASS‐MRCOG | Physiology
Explanation:PROM
PrelabourRuptureofMembranes
Riskofseriousneonatalinfection1%(vs0.5%forwomenwithintactmembranes) 60%ofpatientswithPROMwillgointolabourwithin24hrs Inductionappropriateif>24hourspostruptureandpatientslabourhasn'tstarted
Question 57 Where in the kidney is the majority of Potassium and Phosphate reabsorbed A) PCT B) DCT C) Ascending Loop of Henle D) Descending Loop of Henle E) Collecting Duct Correct Answer: PCT Explanation: As you can see from the list below it is the main reabsorption (termed
reabsorption as primary absorption takes place in the intestines) site for almost all ions.
The PCT reabsorbs the following:
Glucose 100% Amino Acids 100% Carboxylate 100% Bicarbinate 85% Phosphate 85% Potassium 65% Sodium 65% Urea 50% Calcium, Magnesium and Water variable reabsorption throughout nephron
Question 58 What is the average lifespan of a platelet? A) 3‐4 days B) 5‐9 days C) 14‐21 days

PASS‐MRCOG | Physiology
D) 30 days E) 30 days Correct Answer: 5‐9 days Explanation: Blood Cell Lifespans
Red Blood Cells 120 days Platelets 5‐9 days White blood cells 2‐5 days
Neutrophils (up to 5 days) Basophils (2 to 3 days) Eosinophls (2 to 5 days) Monocytes (1 to 5 days) Lymphocytes (variable)
Question 59 Which of the following increases during pregnancy? A) Total Lung Capacity B) Functional Residual Capacity C) Expiratory Reserve Volume D) Tidal Volume E) Vital Capacity Correct Answer: Tidal Volume
Explanation: Tidal Volume increases by approximately 50% Vital Capacity is unchanged The others decrease
Question 60 During the inflammatory phase of wound healing what is the predominant cell type found in the wound during days 3‐4? A) Macrophages B) Monocytes C) Monomorphonuclear Neutrophils (MMNs)
PASS‐MRCOG | Physiology
D) NK Cells E) Polymorphonuclear Neutrophils (PMNs) Correct Answer: Macrophages
Explanation: PMNs phagocytise debris and kill bacteria via free radicals (AKA respiratory burst). They also break down damaged tissue. PMNs typically undergo apoptosis after 48 hours. They are then engulfed and degraded by macrophages. Macrophages therefore become the predominant cell type in the wound on days 3‐4.
Question 61 What percentage of haemoglobin is HbF by 6 months of age? A) <2% B) 5‐10% C) 20‐25% D) 50% E) 70‐90% Correct Answer: <2%
Explanation: By 6 months of age most fetal haemoglobin has been replaced by adult haemoglobin. Electrophoresis suggests <2% is typically HbF.
Question 62 99% of body calcium is in what form? A) Calcium Bicarbonate B) Calcium Gluconate C) Calcium Phosphate D) Calcium Carbonate E) Calcium Hydroxide Correct Answer: Calcium Phosphate
Explanation: 99% of body calcium is stored in the skeleton as Calcium Phosphate salts. There are several calcium phosphate salts. The most abundant in bone is Hydroxylapatite

PASS‐MRCOG | Physiology
Question 63 Minute ventilation in pregnancy increases due to which of the following? A) Effects of gravid uterus on diaphragm B) Dliutional anaemia C) Increased renal excretion of bicarbonate D) Increased circulating oestragen E) Increased circulating progesterone Correct Answer: Increased circulating progesterone
Explanation: This is thought to be the result of increased circulating progesterone. Progesterone is known to directly stimulate ventilation by sensitizing the CNS respiratory centres to CO2. Increased minute ventilation "blows off" CO2 and as a result pCO2 is reduced. pH homeostasis is maintained via increased renal excretion of bicarbonate.
Question 64 Upregulation of urea movement through urea transport proteins in the collecting duct is an effect of which of the following A) Angiotensin B) Angiotensin II C) Aldosterone D) Renin E) Vasopressin Correct Answer: Vasopressin
Explanation: This is an effect of Vasopressin (ADH).
Question 65 What is the maximum normal menstrual blood loss? A) 35‐40ml B) 60‐65ml C) 80‐85ml D) 150‐200ml E) 350‐400ml

PASS‐MRCOG | Physiology
Correct Answer: 80‐85ml Explanation: The maximum normal blood loss is 80ml
Question 66 Which of the following would you expect to be raised in pregnancy? A) Albumin B) ALT C) ALP D) AST E) Bilirubin Correct Answer: ALP Explanation: Raised during pregnancy
Alkaline phosphatase (ALP) Gamma GT (GGT)
Decreased during Pregnancy
The transaminases (AST and ALT) Bilirubin Albumin
Question 67 In reducing the risk of blood transfusion in pregnancy and labour which of the following strategies is recommended? A) A Hb of less than 10.5g/l should prompt haematinics and exclusion of haemaglobinaopathies B) Cell salvage is recommended for all women undergoing c‐section with a Hb of 10.5g/l or less C) Anaemia not due to haematinic deficiency should be managed with parenteral iron D) Recombinant human erythropoietin (rHuEPO) should be used for anaemia correction where oral iron isn't tolerated and parenteral iron is unacceptable to the patient. E) Pre‐autologous blood deposit taken and stored for later use

PASS‐MRCOG | Physiology
Correct Answer: Hb of less than 10.5g/l should prompt haematinics and exclusion of haemaglobinaopathies Explanation: he RCOG green top guidelines advise the following:
If haemoglobin < 10.5 g/dl in the antenatal period, consider haematinic deficiency once haemoglobinopathies have been excluded. Oral iron is 1st line treatment for iron deficiency.
Cell salvage is recommended for women in whom an intraoperative blood loss of more than 1500 ml is anticipated
Anaemia not due to haematinic deficiency will not respond to any form of iron. This should be managed with transfusion
Recombinant human erythropoietin (rHuEPO) is used in end stage renal failure. Its role in other situations is still to be established and should only be used as part of a controlled trial
In pregnancy, pre‐autologous deposit is not recommended according to the RCOG guidelines. In theory patients can have their own blood taken and deposited for up to 5 weeks but concerns have been raised over placental insufficiency and inadequate correction of blood loss caused by the procedure.
Question 68 You review a patient who is 34 weeks pregnant she complains of gradually worsening itching over the past 6 weeks particularly to the hands and feet which is worse at night. What is the likely cause? A) Primary biliary cirrhosis B) Obstetric cholestasis C) Polymorphic eruption of pregnancy D) Pemphigoid Gestationis E) Eczema Correct Answer: Obstetric cholestasis Explanation: This sounds fairly typical of obstetric cholestasis. This usually occurs in the 3rd trimester and gets worse towards term. Itching of the hands and feet is common. Jaundice may also be present

PASS‐MRCOG | Physiology
Question 69 Which GFR calculator is recommended by NICE? A) Shwartz Formula B) CKD‐EPI Formula C) MDRD formula D) Mayo Quadratic Formula E) PANG Formula Correct Answer: MDRD formula Explanation: The MDRD formula is recommended by NICE It should be noted GFR estimations are not advised in pregnancy. In this case a 24 hour urinary creatinine measurement is suggested as gold standard testing for the purpose of renal function assessment.
Question 70 What is the average volume of blood loss during the menstrual cycle A) 35‐40ml B) 60‐65ml C) 80‐85ml D) 150‐200ml E) 350‐400ml Correct Answer: 35‐40ml Explanation: The average menstrual blood loss is 35‐40ml The maximum normal blood loss is 80ml
Question 71 At what stage of fetal development does fetal haemoglobin (HbF) replace embryonic haemoglobin (HbE) as the primary form of haemoglobin? A) 4‐6 weeks B) 10‐12 weeks C) 20‐24 weeks D) 32‐36 weeks E) At Birth

PASS‐MRCOG | Physiology
Correct Answer: 10‐12 weeks
Explanation: Heamoglobin
Embryonic Haemoglobin
Haemoglobin Gower 1 (HbE Gower‐1) Haemoglobin Gower 2 (HbE Gower‐2) Haemoglobin Portland I (HbE Portland‐1) Haemoglobin Portland II (HbE Portland‐2)
Fetal Haemoglobin (haemoglobin F, HbF)
Primary form of Haemoglobin from 10‐12 weeks of fetal development At birth composes 50‐90% of haemoglobin By 6 months of age Adult haemoglobin is primary form
Question 72 At what gestation does the fetus start producing urine? A) 2‐4 weeks B) 5‐7 weeks C) 8‐11 weeks D) 12‐16 weeks E) 18‐22 weeks Correct Answer: 8‐11 weeks
Explanation: Amniotic Fluid
Fetal contribution to amniotic fluid Fetal Urine
First fetal urine produced at 8-11 weeks By term fetus produces approximately 800ml urine per day
Fetal Swallowing
Fetus starts swallowing 12 weeks 250ml swallowed per day

PASS‐MRCOG | Physiology
Fetal Lung Secretions
300ml/day by 2nd trimester
Question 73 Maternal blood flow through the uterine artery at term is approximately A) 30ml/min B) 45ml/min C) 175ml/min D) 300ml/min E) 750ml/min Correct Answer: 750ml/min Explanation: Uterine artery blood flow increases from approximately 45ml/min in the non‐pregnant state to around 750ml/min at term. At term this can account for approximately 12% of maternal cardiac output.
Question 74 Following parturition how long does involution of the uterus take? A) 24‐72 hours B) 1‐2 weeks C) 4‐6 weeks D) 12‐16 weeks E) None of the above Correct Answer: 4‐6 weeks Explanation: Involution of the uterus takes 4‐6 weeks
Question 75 Which of the following is the main reason for active management of the 3rd stage of labour? A) Reduce fetal distress B) Reduce risk of perineal tearing C) Prevent postpartum haemorrhage D) Reduce risk of jaundice in the newborn E) Reduce risk of anaemia in the newborn

PASS‐MRCOG | Physiology
Correct Answer: Prevent postpartum haemorrhage Explanation: World Health Organization, the International Federation of Gynaecology and Obstetrics and the International Confederation of Midwives recommend active management of the third stage of labour in all vaginal deliveries to help to prevent postpartum haemorrhage.
Question 76 Which of the following is a pro‐thrombotic agent? A) Protein C B) Protein S C) Anti‐Thrombin III D) Thromboplastin E) Plasmin Correct Answer: Thromboplastin Explanation: All of the above are anti‐thrombotic except Thromboplastin which is pro‐thrombotic.
Question 77 Which of the following statements is true regarding renal blood flow in pregnancy? A) Decreases by approximately 25% B) Remains constant C) Increases by approximately 10% D) Increases by approximately 25% E) Increases by approximately 50% Correct Answer: Increases by approximately 50% Explanation: Because of the increased cardiac output and blood volume renal blood flow and GFR increases by approximately 50‐60%.
PASS‐MRCOG | Physiology
Question 78 Which of the following statements regarding the placenta and feto‐maternal circulation are FALSE? A) Deoxygenated fetal blood arrives at the placenta via 2 umbilical arteries B) Oxygenated blood returns to the fetus via a single umbilical vein C) There is no direct mixing of fetal and maternal blood at the placenta D) At term the placenta receives 70% of uterine blood flow E) In the umbilical vein the pressure is approximately 20 mmHg Correct Answer: At term the placenta receives 70% of uterine blood flow Explanation: At term the placenta receives around 90% of uterine blood flow
Question 79 Regarding cardiac output in pregnancy which of the following statements is TRUE? A) Cardiac Output decreases by approximately 10‐15% during pregnancy B) Cardiac Output remains constant C) Cardiac Output increases by approximately 10‐15% during pregnancy D) Cardiac Output increases by approximately 40‐50% during pregnancy E) None of the above Correct Answer: Cardiac Output increases by approximately 40‐50% during pregnancy Explanation: Cardiac Output increases by 40‐50% during pregnancy
Question 80 What is the typical weight of a term uterus? A) 40g B) 200g C) 400g D) 800g E) 1200g Correct Answer: 1200g

PASS‐MRCOG | Physiology
Explanation: Uterine Growth
Non-pregnant uterus
Weight 40-50g Volume approx 10ml
Term uterus
Weight 1100-1200g Volume approx 5000ml
Question 81 Breast milk is produced by the secretions of the epithelial cells of the acinar. Which of the following is an accurate estimate of mature breast milk composition? A) Fat 4%, Protein 1%, Sugar 7% B) Fat 10% Protein 4% Sugar 20% C) Fat 10% Protein 10% Sugar 30% D) Fat 18% Protein 5% Sugar 5% E) Fat 18% Protein 15% Sugar 1% Correct Answer: Fat 4%, Protein 1%, Sugar 7%
Explanation: Although Colostrum may have higher protein composition and lower sugar concentration mature breast milk contains approximately 1% Protein, 4% fat and 7% sugar.
Question 82 Which of the following prolongs Prothrombin time? A) Factor V deficiency B) Von Willebrand disease C) Hemophilia D) Aspirin therapy E) Protein C Deficiency Correct Answer: Factor V deficiency

PASS‐MRCOG | Physiology
Explanation: Causes of prolonged Prothrombin time (PT) and also INR (INR is a ratio of PT):
Factor V deficiency Warfarin therapy Liver Failure DIC
Note Protein C is an anticoagulant and deficiency results in a hyper‐coaguable state and tendency towards thrombosis. The other options increase bleeding time but not via the PT which evaluates the extrinsic pathway of the clotting cascade.
Question 83 The primary stimulus for ADH (anti‐diuretic hormone AKA Vasopressin) release is? A) Low serum osmolality B) High serum osmolality C) Low blood volume D) High Blood volume E) Reduced ECF volume Correct Answer: High serum osmolality
Explanation: Increasing serum concentration i.e. high osmolality is the primary stimulus. Decreased blood volume/reduced ECF does also stimulate ADH but the hypothalamus is less sensitive to this