parenting behaviors during risky driving by teens with attention-deficit/hyperactivity disorder
TRANSCRIPT

Available online at www.sciencedirect.com
ScienceDirectBehavior Therapy 45 (2014) 168–176
www.elsevier.com/locate/bt
Parenting Behaviors During Risky Driving by Teens WithAttention-Deficit/Hyperactivity Disorder
Nicole K. SchatzGregory A. FabianoKaren L. Morris
Jennifer M. ShucardUniversity at Buffalo, SUNY
Brittany A. LeoCourtney Bieniek
Buffalo State College
Parenting practices for teen drivers with ADHD wereobserved via a video monitor installed in vehicles. All teenshad recently completed a driver education course and were inthe driving permit stage of a graduated driver-licensingprogram. Parent behaviors were coded during drives whenteens were driving safely and during drives when teensengaged in risky driving. The overall frequency of positiveparenting strategies was low, regardless of whether teensdrove safely or engaged in risky driving. Although the rate ofnegative feedback was also low, parents engaged in signifi-cantly more criticism and were rated by an observer to appearangrier when teens were driving in a risky manner. No otherdifferences in parent behaviors associated with the quality ofteen driving were observed. The inconsistencies betweenobserved parenting behaviors and those parenting practicesrecommended as effective with teens with ADHD arediscussed. The need for further research addressing effective
This research was supported by a grant from the Eunice KennedyShriver National Institute of Child Health and Human Develop-ment (R01HD058588).
Address correspondence to Nicole K. Schatz, Department ofCounseling, School & Educational Psychology, University atBuffalo, SUNY, 3rd Floor, Diefendorf Hall, 3435 Main Street,Buffalo, New York 14214; e-mail: [email protected]/45/168-176/$1.00/0© 2013 Association for Behavioral and Cognitive Therapies. Published byElsevier Ltd. All rights reserved.
strategies for teaching teens with ADHD to drive ishighlighted.
Keywords: ADHD; adolescents; parenting; driving
ACCIDENTAL INJURY IS THE LEADING CAUSE of death forteens in the United States, and 73% of accidentalinjuries resulting in a teen’s death from 1999 to 2006were attributable to automobile crashes (Minino,2010). Compared to the general population, teendrivers are involved in a disproportionately highnumber of fatal motor vehicle crashes. Based on 2006data, only 6.4%of all licensed drivers were teenagers,but they were involved in 12.9% of all fatalautomobile crashes (Compton & Ellison-Potter,2008). Furthermore, young drivers are involved insignificantly more automobile crashes involving afatality than are drivers from any other age group(Compton & Ellison-Potter). Not only are teendrivers more likely to be involved in seriousautomobile crashes, they also are more often thecause of such events. In an investigation of data from795 serious motor vehicle crashes involving teendrivers, the cause of the crashwas deemed to be drivererror on the part of the teen in more than 75% ofcases (Curry, Hafetz, Kallan, Winston, & Durbin,2011).Risk of negative driving outcomes is even greater
amongadolescentswith attention-deficit/hyperactivity

169parent ing dur ing r i s ky teen dr iv ing
disorder (ADHD). Young drivers with ADHD areinvolved in more motor vehicle crashes than typicallydeveloping teen drivers, and are more likely to befound at fault for crashes (Barkley & Cox, 2007;Barkley, Guevremont, Anastopoulos, DuPual, &Shelton, 1993; Barkley, Murphy, & Kwasnik,1996). Young drivers with ADHD receive moretraffic citations than drivers without ADHD, aremore likely to have their licenses suspended, driveillegally, and demonstrate poorer performance dur-ing simulated driving (Barkley et al., 1993; Barkley etal., 1996; Biederman et al., 2007; Fischer, Barkley,Smallish, & Fletcher, 2007; Thompson, Molina,Pelham, & Gnagy, 2007).Although there is considerable evidence that teens
with ADHD experience more negative driving out-comes relative to typically developing teens, little isknown about specific steps families of novice teendriverswithADHDmay take to improve safety. Therehave been few studies addressing effective strategiesfor parents teaching teens with ADHD to drive. Thereis some evidence regarding strategies for reducingdriving risk among typically developing teens in thegeneral population. For example, teens who delayobtaining adriver’s license have better outcomes, as doteens whose parents set stricter limits related to when,where, and with whom teens are allowed to drive(Hartos, Eitel, & Simons-Morton, 2001). Greaterparent-teen agreement regarding driving restrictionsalso appears to contribute to fewer negative drivingoutcomes (Beck, Hartos, & Simons-Morton, 2006).Although these parenting strategies appear to beassociated with improved driving outcomes fortypically developing teens, teen drivers with ADHDhave reliably worse outcomes relative to typicallydeveloping teen drivers, and a different or moreintense approach may be necessary when teachingteenswithADHD todrive. Furthermore, the strategiesdescribed above are implemented following licensure;for families of teenagers with ADHD, who are knownto have worse outcomes, interventions may need tooccur during the permitted driving stage and continueuntil safe driving practices have been achieved.Supervised driving practice may be a situation in
which it is especially important for parents to engage ineffective parenting practices. During supervised driv-ing practice, parents are arguably the most active inmonitoring and providing instruction related todriving, and thismay be a period of timewhen parentshave significant influence on teen driving outcomes.Unfortunately, very little is known about how parentsapproach driving practice with their teens withADHD. Robin (2006) suggested that effective parent-ing of teens with ADHD involves more positivefeedback than negative; however, parents of adoles-cents with ADHD engage in more negative parenting
practices than do parents of children without ADHD(Barkley, Anastopoulos, Guevremont, & Fletcher,1992). To the extent that these negative parent-teeninteractions alsooccur during superviseddriving, theremay be a negative effect on the quality of teen driving.The primary aim of the current study was to
provide an initial look at parents’ use of effectiveparenting strategies during supervised driving practicewith teenswithADHD.Through in vivo observationsof parent-supervised teen driving practice, particularattention was focused on the extent to which parentsengaged in positive parenting strategies (e.g., praise,effective commands, and coaching) as opposed tonegative parenting strategies (e.g., criticism andnegative comments). To investigate whether parentsresponded differently depending on the quality of teendriving, parent behaviors during drives in which teensengaged in risky driving were compared to parentbehaviors during drives in which teens drove moresafely. It was hypothesized that parents would engagein significantly more negative behaviors, and fewerpositive behaviors, following a risky driving behaviorthan they would following nonrisky driving. Parentbehaviors prior to risky driving were not expected todiffer fromparent behaviors prior to nonrisky driving.
Methodparticipants
Participants in this study represented a subset ofparticipants from a larger, ongoing, randomizedcontrol trial. Driving behaviors of participants in thelarger study are tracked longitudinally followingparticipation in a driver education program. Partic-ipants were recruited through radio advertisementsand flyers distributed to high schools and communityproviders in western New York. Study procedureswere approved by the Child and Youth InstitutionalReview Board. As incentive to participate, teens wereenrolled in a 10-week driver education course free ofcharge. Participants were also provided with $75stipends for completing follow-up assessments.To be eligible to participate, teens were required to
have obtained a learner’s driving permit. Additionally,the teen and at least one parent needed to be willing toparticipate in the project. All teens met currentDiagnostic and Statistical Manual of Mental Disor-ders, Fourth Edition, Text Revision (DSM-IV-TR;APA, 2000) diagnostic criteria for ADHD–CombinedType according to current evidence-based assessmentguidelines (Pelham, Fabiano, & Massetti, 2005).ADHD diagnoses as well as diagnoses of comorbidconditionswere determined according toDSM-IV-TRcriteria.This study included teens who had been randomly
assigned to participate in the control group of thelarger study and who had completed the 4-week
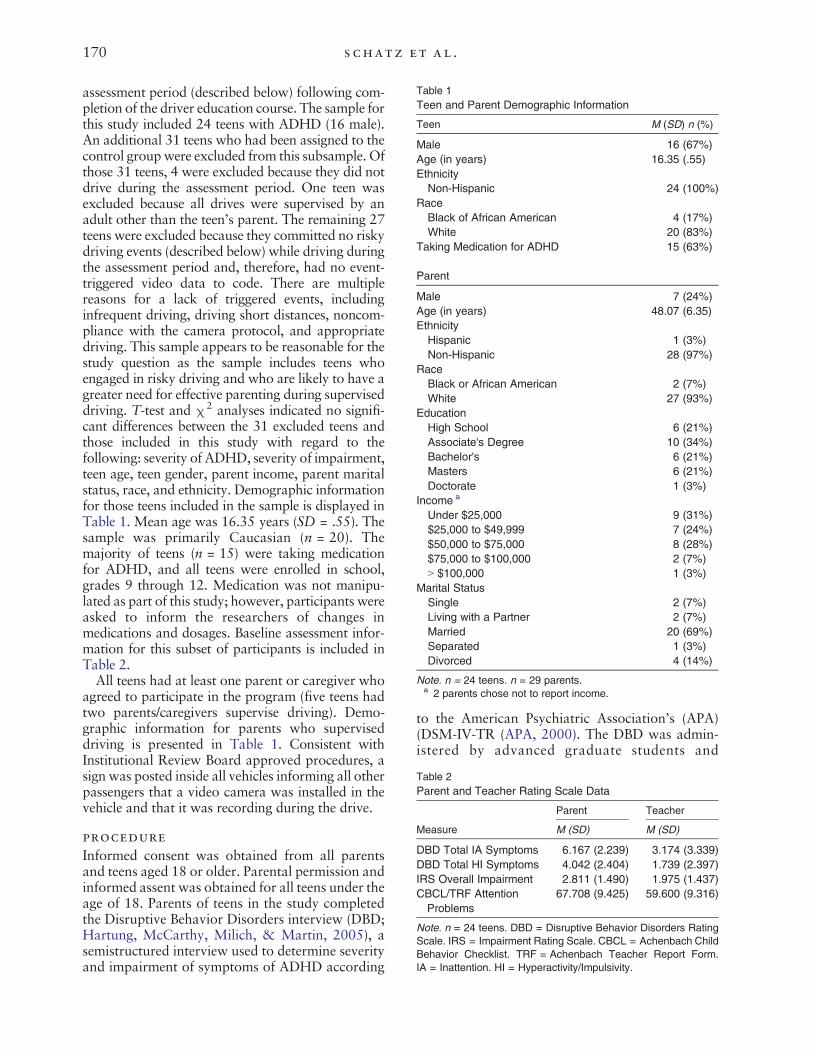
Table 1Teen and Parent Demographic Information
Teen M (SD) n (%)
Male 16 (67%)Age (in years) 16.35 (.55)EthnicityNon-Hispanic 24 (100%)
RaceBlack of African American 4 (17%)White 20 (83%)
Taking Medication for ADHD 15 (63%)
Parent
Male 7 (24%)Age (in years) 48.07 (6.35)EthnicityHispanic 1 (3%)Non-Hispanic 28 (97%)
RaceBlack or African American 2 (7%)White 27 (93%)
EducationHigh School 6 (21%)Associate's Degree 10 (34%)Bachelor's 6 (21%)Masters 6 (21%)Doctorate 1 (3%)
Income a
Under $25,000 9 (31%)$25,000 to $49,999 7 (24%)$50,000 to $75,000 8 (28%)$75,000 to $100,000 2 (7%)N $100,000 1 (3%)
Marital StatusSingle 2 (7%)Living with a Partner 2 (7%)Married 20 (69%)Separated 1 (3%)Divorced 4 (14%)
Note. n = 24 teens. n = 29 parents.a 2 parents chose not to report income.
Table 2Parent and Teacher Rating Scale Data
Parent Teacher
Measure M (SD) M (SD)
DBD Total IA Symptoms 6.167 (2.239) 3.174 (3.339)DBD Total HI Symptoms 4.042 (2.404) 1.739 (2.397)IRS Overall Impairment 2.811 (1.490) 1.975 (1.437)CBCL/TRF AttentionProblems
67.708 (9.425) 59.600 (9.316)
Note. n = 24 teens. DBD = Disruptive Behavior Disorders RatingScale. IRS = Impairment Rating Scale. CBCL = Achenbach ChildBehavior Checklist. TRF = Achenbach Teacher Report Form.IA = Inattention. HI = Hyperactivity/Impulsivity.
170 schatz et al .
assessment period (described below) following com-pletion of the driver education course. The sample forthis study included 24 teens with ADHD (16 male).An additional 31 teens who had been assigned to thecontrol groupwere excluded from this subsample. Ofthose 31 teens, 4 were excluded because they did notdrive during the assessment period. One teen wasexcluded because all drives were supervised by anadult other than the teen’s parent. The remaining 27teens were excluded because they committed no riskydriving events (described below) while driving duringthe assessment period and, therefore, had no event-triggered video data to code. There are multiplereasons for a lack of triggered events, includinginfrequent driving, driving short distances, noncom-pliance with the camera protocol, and appropriatedriving. This sample appears to be reasonable for thestudy question as the sample includes teens whoengaged in risky driving and who are likely to have agreater need for effective parenting during superviseddriving. T-test and χ2 analyses indicated no signifi-cant differences between the 31 excluded teens andthose included in this study with regard to thefollowing: severity of ADHD, severity of impairment,teen age, teen gender, parent income, parent maritalstatus, race, and ethnicity. Demographic informationfor those teens included in the sample is displayed inTable 1. Mean age was 16.35 years (SD = .55). Thesample was primarily Caucasian (n = 20). Themajority of teens (n = 15) were taking medicationfor ADHD, and all teens were enrolled in school,grades 9 through 12. Medication was not manipu-lated as part of this study; however, participants wereasked to inform the researchers of changes inmedications and dosages. Baseline assessment infor-mation for this subset of participants is included inTable 2.All teens had at least one parent or caregiver who
agreed to participate in the program (five teens hadtwo parents/caregivers supervise driving). Demo-graphic information for parents who superviseddriving is presented in Table 1. Consistent withInstitutional Review Board approved procedures, asign was posted inside all vehicles informing all otherpassengers that a video camera was installed in thevehicle and that it was recording during the drive.
procedure
Informed consent was obtained from all parentsand teens aged 18 or older. Parental permission andinformed assent was obtained for all teens under theage of 18. Parents of teens in the study completedthe Disruptive Behavior Disorders interview (DBD;Hartung, McCarthy, Milich, & Martin, 2005), asemistructured interview used to determine severityand impairment of symptoms of ADHD according
to the American Psychiatric Association’s (APA)(DSM-IV-TR (APA, 2000). The DBD was admin-istered by advanced graduate students and

171parent ing dur ing r i s ky teen dr iv ing
postdoctoral fellows who were supervised by aPh.D.-level psychologist. Parents and teachers werealso asked to complete the DBD rating scale ofADHD symptoms (Evans et al., 2012; Pelham,Gnagy, Greenslade, & Milich, 1992), the ChildBehavior Checklist (Achenbach & Rescorla, 2001),and the Impairment Rating Scale (Evans et al.;Fabiano et al., 2006). Additionally, cliniciansconducted a review of records (e.g., elementaryand high school report cards, psychoeducationalreports) when available. Teens with conditions(e.g., seizures, psychotic disorder, pervasive devel-opmental disorder, IQ b 70) that would impairdriving or otherwise cause them to be inappropriateparticipants for this intervention were not enrolledin the study. Information from the ImpairmentRating Scale, CBCL, and the DBD interview wasreviewed to determine ADHD status and eligibilityto participate, but it was not included in analyses.Following assessment to establish eligibility, teens
were enrolled in a 10-week driver education programthat included weekly classroom instruction andone-on-one driving practice with an instructor. Dataregarding parent and teen behavior during teendriving was obtained over the course of a 4-weekperiod following the completion of the drivereducation program through the use of an on-boardvideo monitor, the T-Eye ADR3000 Mobile EventData Recorder (kcicommunications.com/mobile/teye.html), installed in all teens’ vehicles. Teens wereinstructed to turn the T-Eye device on each time theydrove. The T-Eye device allowed for video observa-tions of the driver’s view of the road, and video andaudio recording of the vehicle’s interior cabin. TheT-Eye device was activated by sudden changes in thevehicle’s trajectory (e.g., abrupt stops, fast starts,swerves, and collisions), which will be referred to as“driving events.” The device was also sensitive torelatively small bumps in the road and would betriggered even though the driver had not engaged inrisky driving. These false positives will be referred toas “nonevents.” Bumps in the road were only codedas nonevents in situations when the driver did notappear to be at fault for triggering the camera.Instances in which teens did not appropriatelyanticipate and slow down for large bumps in theroad were coded as events due to imprudent speed.Each video was coded for teen behavior, parentbehavior, and other aspects of the driving situation(e.g., cause of driving event, speed, etc.).
measuresObjective Measure of Parent and Teen DrivingBehaviorThe T-Eye ADR3000 Mobile Event Data Recorderincluded two cameras that recorded a forward view
of the road as well as a view of the driver and thevehicle cabin. In addition to capturing video, themonitor system recorded vehicle speed. The mon-itor included a three-axis accelerometer that, whentriggered, saved video related to risky driving events(e.g., hard brakes, fast starts, swerves, collisions, orother events that result in an abrupt change in thevelocity of the vehicle) and nonevents (e.g., drivingover a small bump in the road). When triggered,the monitor system saved the video for approxi-mately 30 seconds prior to the risky driving eventor nonevent and approximately 10 seconds follow-ing the event or nonevent.
video coding procedures
For each participant included in this subsample, allvideos associated with risky driving events duringparent-supervised driving were included in the dataset.Nonevent videoswere randomly selected fromallavailable nonevent videos for each participant in thedata set. An equal number of event and noneventvideos per participant were coded.Frequency counts were obtained for the following
parent behaviors: labeled praise, unlabeled praise,appropriate commands, inappropriate commands,negative talk, and coaching. Definitions for all parentbehaviors except coaching were adapted from thebehavioral definitions in the Manual for the DyadicParent-Child Interaction Coding System, ThirdEdition (DPICS; Eyberg, Nelson, Duke, & Boggs,2005). Labeled praise was defined as any time aparent gave the teen positive feedback about aspecific behavior. To qualify as labeled praise, theparents’ statement had to identify a specific teenbehavior and describe the behavior in a positivemanner (e.g., “Good job slowing down before thatturn.”). Unlabeled praise included instances ofpositive statements by the parent about the teenthat did not identify a specific teen behavior (e.g.,“Good job”). Instances of parents giving short,specific, easily understood instructionswere coded asappropriate commands (e.g., “Begin slowing downfor the stop sign now”). Commands issued in theform of a question, vague commands, and othercommands issued in a manner that would not beexpected to facilitate teen compliancewere labeled asinappropriate commands (e.g., “Don’t you think youshould slow down now?”). Negative talk wasdefined as any instance of a parent making criticalor disapproving comments about the teen driver(e.g., “That was terrible!”). Coaching was defined asany statement by the parent designed to teach orexplain driving that would not otherwise be coded asan instance of praise, as a command, or as negativetalk (e.g., “If it were snowing, you would need todrive slower than you are now”).

172 schatz et al .
In addition to frequency count variables, overalllevels of parent and teen anger throughout thecourse of each video were rated on a Likert scaleranging from 1 (not at all angry) to 5 (extremelyangry). Parent and teen anxiety levels were rated ona similar scale ranging from 1 (not at all anxious) to5 (extremely anxious).Videos were coded by undergraduate research
assistants as well as postdoctoral and master’s-levelstaff. Twenty percent of videos were recoded by asecond coder to establish reliability. Because it waslikely clear to coders whether videos did or did notcontain risky driving events, it was not possible forcoders to be blinded to video type by event ornonevent. Additionally, coders were not blind to thepurpose of the study.Following the guidelines of Shrout and Fleiss
(1979), intraclass correlations (ICCs) were calculatedusing a one-way random effects model. Using criteriarecommended by Cicchetti (1994), ICCs for themajority of codes indicate interrater reliabilityranging from good (Appropriate Commands ICC =.721, Negative Talk ICC = .723, Parent AnxietyICC = .616, and Teen Anxiety ICC = .707) toexcellent (Coaching ICC = .821, Parent AngerICC = .814, and Teen Anger ICC = .823). The ICCfor unlabeled praise fell in the fair range (UnlabeledPraise ICC = .489). An ICC for labeled praise couldnot be calculated because no instances of labeledpraise were observed in the subset of videos coded forreliability (only one instance of labeled praise wasobserved across all videos in the data set). Further-more, a series of one-sample t-tests of variablesrepresenting the difference between raters for eachbehavior code yielded all nonsignificant results andindicated that the averages of the differences betweenraters for each individual code across all videos arenot statistically different from zero. After consider-ation of these data, interrater reliability for allvariables was deemed acceptable for the plannedanalyses.Two types of summary scores were created using
the frequency count data. First, the frequency countsfor all observed positive and negative parentingbehaviors (i.e., labeled praise, unlabeled praise,appropriate commands, negative talk, and coaching)across all videoswithin eachparticipantwere summedto yield the total number of observed parentingbehaviors across all videos for each individual teen.Ratio scores for positive parenting (i.e., labeled praise,unlabeled praise, appropriate commands, and coach-ing) and negative talk were then calculated. For eachparticipant the combined total of all positive parent-ing behaviors across all videoswas divided by the sumof all parenting behaviors to create a score for eachparticipant reflecting the proportion of observed
parenting behaviors that were coded as positive. Asimilar score was calculated reflecting the proportionof parenting behaviors coded as negative talk. Thesepositive parenting and negative talk ratio scores werecalculated separately for event and nonevent videos.The second type of summary score represents the
frequency of positive parenting and negative parent-ing, while controlling for video length and number ofvideos per participant. Video clipswere divided at thetime of the event or nonevent and separate frequencycounts were obtained for parenting behaviorsobserved prior to the event or nonevent and forparenting behaviors observed during and after theevent or nonevent. Inmost cases, video clips included30 seconds prior to the event or nonevent and10 seconds following the event or nonevent; how-ever, there were several clips of shorter duration dueto the occurrence of an event or nonevent in closetime proximity to either the beginning or the end of adrive. As with the positive ratio score describedabove, the frequency counts for all positive parentingbehaviors were summed into a single composite.Because of variability in video length, frequencycounts of positive parenting behaviors and negativetalk for each video were divided by the video length(in seconds) to create variables reflecting the rate ofthe behaviors per second of video. Due to variabilityin the number of video clips per participant, averagescores were created to reflect the average rates ofpositive parenting behaviors and negative talk persecond both before and after events or noneventsacross all videos for individual participants. Averagepositive parenting and negative talk frequency scoreswere calculated separately for event and noneventvideos.
ResultsAcross all participants, datawere available for a totalof 91 risky driving events and 91 nonevents. Themajority of risky driving events were due to hardbrakes (n = 31) and sharp turns (n = 25). Otherrisky driving events were attributed to hard acceler-ation, swerves, striking curbs, and imprudent speed.The number of risky driving events per teen rangedfrom1 to 14 (M = 3.792, SD = 3.036). Themajorityof teens (75%) had 5 or fewer events and one teenhad 14 total risky driving events. The accompanyingparent tended to be female during driving events(80%) andduring nonevents (84%).Due to the smallsample size and relatively low frequency of maleparents supervising driving, data formale and femaleparents were combined in analyses.The frequency of driving-related parenting behav-
iors (i.e., labeled praise, unlabeled praise, appropri-ate commands, negative talk, and coaching) wasrelatively low across all videos. Only one instance of

173parent ing dur ing r i s ky teen dr iv ing
labeled praise was observed across all event andnonevent videos. To measure the rate at whichparents engaged in at least one positive or instructivebehavior (e.g., labeled praise, unlabeled praise,appropriate commands, and coaching) across videosfor each participant, the number of videos in which aparent engaged in at least one of these behaviors wasdivided by the total number of videos. For videoswith an event, the average proportion of videos withat least one observed positive parenting behavioracross participants was .499 (SD = .364). For videoswith no risky driving events, the average proportionwas .402 (SD = .412). In other words, parents didnot engage in any observed positive or instructivebehaviors during 50% of the videos with a riskydriving event and 60% of videos without a drivingevent. To measure the rate at which parents madecritical comments towards their teens, the number ofevent and nonevent videos inwhich a parent engagedin negative talk was divided by the total number ofevent and nonevent videos, respectively. For theaverage teen, the average proportion of videos withat least one instance of negative talk was .189 (SD =.343) for nonevent videos and .519 (SD = .370) forevent videos.
comparison of the relative frequencyof positive parenting and negative talkbetween events and nonevents
Paired-sample t-tests comparing the average positiveparenting ratio scores to the average negative talkratio scores for event and nonevent videos wereconducted to compare the relative frequency ofpositive parenting and negative talk. For noneventvideos, the average proportion of parenting behaviors
Table 3Wilcoxon Signed-Rank Tests and Effect Sizes Comparing AveragParent Behaviors During Events and Non-Events
Events None
Mean (SD) Mean
Parent BehaviorsPositive Parenting Before .002 (.004) .009Negative Talk Before .019 (.028) .011Positive Parenting After .003 (.004) .003Negative Talk After .074 (.088) .022
Emotions During Entire ClipParent Anger 2.033 (1.041) 1.339Teen Anger 1.734 (.862) 1.112Parent Anxiety 1.990 (.927) 1.423Teen Anxiety 1.679 (.767) 1.416
Note. N = 24. Alpha levels determined according to a modified Bonferparent/teen emotions) according to procedures outlined by Holm (197Positive Parenting includes Labeled Praise, Unlabeled Praise, Appropri*p b .025. **p b .017. ***p b .013.
coded as positive parenting behaviors (M = .532,SD = .443) was significantly greater than the averageproportion of behaviors coded as negative talk (M =.219, SD = .338, t = 2.351, p = .028). For eventvideos, there was no significant difference betweenthe average proportion of parenting behaviors codedas positive parenting (M = .447, SD = .373) and theaverage proportion of videos coded as negative talk(M = .512, SD = .376, t = -.443, p = .662). In otherwords, despite the overall low rate of positiveparenting behaviors, parents engaged in relativelymore positive parenting behaviors than negativeparenting behaviors during nonevent videos. Duringevent videos, there was no significant difference in therelative frequency of positive and negative parentingbehaviors.
comparison of parenting behaviors beforeand after events and nonevents
Frequency scores for positive parenting and negativetalk observed following the occurrence of drivingevents were compared with frequency scores forpositive parenting and negative talk followingnonevents. Standard t-tests to compare mean fre-quency of parenting behaviors during events andnonevents could not be performed due to violationsof the assumption of normality, given the low rateof the parenting behaviors. Therefore, Wilcoxonsigned-rank tests were performed (see Table 3 forresults). Following suggested procedures in Jaccardand Guilamo-Ramos (2002) for grouping individualanalyses into families of related analyses, we groupedthe parenting behavior analyses into one family andthe parent and teen emotions analyses into a secondfamily. Experiment-wise error was then addressed
e Parent and Teen Emotions and Per-Second Frequency of
vent Cohen’s
(SD) Z p d
(.038) -0.672 0.501 -0.259(.027) -2.273 0.023 0.291(.007) -0.104 0.918 0.000(.038) -2.799*** 0.005 0.767
(.589) -2.702** 0.007 0.821(.415) -3.297*** 0.001 0.919(.691) -2.137 0.033 0.694(.689) -1.426 0.154 0.361
roni procedure within families of analyses (parent behaviors and9) and recommended by Jaccard and Guilamo-Ramos (2002).ate Commands, and Coaching.

174 schatz et al .
within families of analyses using the sequentiallyrejective test described by Holm (1979) and recom-mendedby Jaccard andGuilamo-Ramos. Therewereno significant differences in parenting behaviorsduring events and during nonevents with respect topositive parenting behaviors. There were, however,differences with regard to negative talk. Parentsengaged in significantly more negative talk followingevents than they did following nonevent (Z = -2.799,p = .005).Anger and anxiety ratings for parents and teens
during event and nonevent videos were also com-pared. Again, due to violations of the assumption ofnormality, Wilcoxon signed-rank tests were per-formed (see Table 3 for results). Parentswere rated assignificantly angrier (Z = -2.702, p = .007) duringevent videos than during nonevent videos. Teenswere also rated as angrier (Z = -3.297, p = .001)during event videos than during nonevent videos.Ratings of parent and teen anxiety, however, did notsignificantly differ between event and noneventvideos.
DiscussionThe results presented in this paper serve as an initialstep toward addressing the significant gap in existingresearch regarding the learning experiences of teendrivers with ADHD. These results also provide a firstlook at the parenting strategies employed by parentsof teens with ADHD during an important functionalactivity and developmental transition— superviseddriving. Findings were, in part, consistent withhypotheses. The only observed differences in parentbehavior between videos in which teens were drivingpoorly (event videos) and videos in which teens weredriving safely (nonevent videos) were with regard toparents’ anger and their use of negative and criticalcomments. Although ratings of overall levels of angerand anxiety were relatively low across event andnonevent videos, parents were rated as significantlyangrier during videos with a driving event. Parentsresponded to risky driving events withmore negativetalk than parents used in response to nonevents. Nodifferences between events and nonevents wereobserved with regard to positive parenting behaviors(e.g., praise, commands, coaching). Parents rarelypraised teens for a jobwell done (only one instance oflabeled praise occurred in all the videos analyzed)and provided teens with instructions related todriving at a low rate. Although rates of positiveparenting were low during both events and non-events, parents engaged in relatively more positiveparenting than negative talk during nonevents. Therewas no significant difference, however, between ratesof positive parenting and negative talk observedduring events due to the higher frequency of negative
parenting observed during events than was observedduring nonevent videos.The patterns of parenting behaviors observed in
this study may be problematic because they runcounter to behavior management principles thathave been recommended as efficacious for teens withADHD. More specifically, behavioral interventionsfor adolescents with ADHD recommend that parentsprovide teens with frequent feedback regarding theirperformance (Robin, 2006). Furthermore, parentsare advised to provide relatively more positivefeedback regarding appropriate teen behaviors thannegative feedback regarding behaviors needingimprovement (Robin). The parenting behaviorsobserved during this study were not consistent withthese recommendations and parents gave littlefeedback to teens regarding driving performance.This may be considered a missed opportunity forparents to provide constructive feedback and preventsimilar teen driving errors in the future. Withoutappropriate feedback from parents about what theyare doing well and about what actions they need totake to improve, young drivers with ADHD maystruggle todevelopappropriate driving skills throughsupervised practice. Additionally, parents may havebeen able to prevent some instances of risky teendriving through the effective use of coaching andinstruction during the time leading up to the riskydriving event.Parents and teens were also rated as appearing
angrier during drives with a risky driving event. Itwill be important for future research to investigatethe extent to which negative parent-teen communi-cation during driving practice might contribute torisk for teendriving errors, as it is possible that parentand teen anger served as an antecedent for subse-quent risky teen driving behaviors. Additionally, itwill be important for future researchers to addressgender differences in parenting during drivingpractice, something that was not possible with thecurrent data. Given that mothers and fathers appearto behave differently from each other duringinteractions with their ADHD teens (Edwards,Barkley, Laneri, Fletcher, & Metevia, 2001), theremay be differences in parenting strategies duringsupervised driving for mothers and fathers.These findings must be considered within the
context of the limitations of this study. All teens whoparticipated in this study had completed a drivereducation course, and parenting strategies may bedifferent among parents of teens who have notcompleted driver education. Coders were not blindto the purpose of the study or to the classification(event versus nonevent) of videos. To limit confoundsrelated to coder bias, the behavior codes wereadapted from a well-established behavior coding

175parent ing dur ing r i s ky teen dr iv ing
system and were designed to maximize coderobjectivity. As an additional limitation, these find-ings are based on data froma relatively small numberof teens with ADHD. Due to the small sample size,there was insufficient power to compare drivingperformance of teens who take medication forADHD and those who do not. To the extent thatstimulantmedications forADHDare associatedwithimproved teen behavior and driving performance,the use of prescribed medications may indirectlycontribute to parents’ behaviors during superviseddriving. Also related to sample size, there were anumber of teens participating in the larger studywhoare not represented in this smaller data set becausethey did not have video from risky driving events. Itwas outside the scope of this study to identify whysome teens had risky driving events and others didnot and it will be important for future studies toidentify factors that contribute to safer drivingamong teens with ADHD. It may be that effectiveparenting contributed to safer driving among teenswithout risky driving events. On the other hand,some teens may have driven less than others and hadfewer opportunities for a risky driving event to occur.Alternatively, previously observed group differencesin risky driving between teens with ADHD andcontrol group teens may be the result of very poordriving among a subset of teens with ADHD ratherthan poor driving across all teens with ADHD (see acomparable pattern of outcomes inMcGehee, Raby,Carney, Lee,&Reyes, 2007). These are all issues thatneed to be addressed in future studies.This study is also limited by the lack of a
comparison group of teen drivers without ADHD.Because of this, it is not possible to ascertain if theparenting practices observed during driving videos arespecific to parents of teenswithADHDor if all parentswould behave similarly. Regardless of whether theparenting practices observed in this study are uniqueto parents of teens with ADHD, the data presentedhere suggest that parents frequently engage inparenting practices during supervised driving practicethat existing research and theory would suggest areunlikely to promote compliance and cooperation(Dishion, Nelson, & Bullock, 2004). Thus, thereappears to be amismatch between parenting practicesand the needs of teen drivers with ADHD. Morespecifically, due to well-established risk for negativedriving outcomes among teens with ADHD (Barkleyet al., 1993; Barkley et al., 1996; Jerome, Segal, &Habinski, 2006), this group of novice drivers may bein greater need of effective instruction and parentingrelated to safe driving than are teens without ADHD.It is also important to note that the patterns of
positive and negative parenting behaviors observedduring this study may not be unique to parent-teen
interactions during driving. Instead, the observedparenting behaviors may be an extension of thetypical manner in which the parents interact withtheir teens in day-to-day life. After years of increasedconflict with their child with ADHD (Barkley et al.,1992), parents may attempt to avoid conflict bysetting fewer limits and providing less monitoring,similar to the pattern identified by Dishion et al.(2004). This pattern may apply to parenting behaviorduring driving as well as in other situations. Given thepotentially severe consequences to teens’ safety aswellas the safety of passengers and other motorists,supervised driving practice is a time when teens maybe especially in need of effective parental monitoringand management.Additional research is necessary to determine how
parents may effectively instruct teens with ADHDduring driving practice. Such research could lead tointerventions that significantly reduce the risk ofaccidents and injury among teendriverswithADHD.This initial study suggests that parenting practicesobserved in other studies of parent-teen interactionsalso appear to occur during supervised drivingpractice. Additionally, this study begins to identifypotential target behaviors for interventions that maycontribute to safer driving practices among teenswith ADHD by improving the effectiveness ofparenting during supervised driving.
Conflict of Interest StatementThe authors declare that there are no conflicts of interest.
References
Achenbach, T.M.,&Rescorla, L. (2001).Manual for theASEBAschool-age forms & profiles. Burlington: University ofVermon, Research Center for Children, Youth, and Families.
American Psychiatric Association. (2000). Diagnostic andstatistical manual of mental disorders (4th ed., text rev.).Washington, DC: Author.
Barkley, R., Anastopoulos, A., Guevremont, D., & Fletcher, K.(1992). Adolescents with attention deficit hyperactivitydisorder: Mother-adolescent interactions, family beliefs andconflicts, andmaternal psychopathology. Journal of AbnormalChild Psychology, 20(3), 263–288. http://dx.doi.org/10.1007/bf00916692
Barkley, R. A., & Cox, D. (2007). A review of driving risksand impairments associated with attention-deficit/hyperac-tivity disorder and the effects of stimulant medication ondriving performance. Journal of Safety Research, 38,113–128. http://dx.doi.org/10.1016/j.jsr.2006.09.004.
Barkley, R. A., Guevremont, D. C., Anastopoulos, A. D.,DuPaul, G. J., & Shelton, T. L. (1993). Driving-related risksand outcomes of attention deficit hyperactivity disorder inadolescents and young adults: A 3- to 5-year follow-upsurvey. Pediatrics, 92(2), 212.
Barkley, R. A., Murphy, K. R., & Kwasnik, D. (1996). Motorvehicle driving competencies and risks in teens and youngadults with attention deficit hyperactivity disorder. Pediatrics,98(6), 1089–1095.

176 schatz et al .
Beck, K. H., Hartos, J. L., & Simons-Morton, B. G. (2006).Relation of parent-teen agreement on restrictions to teen riskydriving over 9 months.American Journal of Health Behavior,30(5), 533–543. http://dx.doi.org/10.5993/ajhb.30.5.10
Biederman, J., Fried, R., Monuteaux, M., Reimer, B., Coughlin,J., Surman, C., … Faraone, S. (2007). A laboratory drivingsimulation for assessment of driving behavior in adults withADHD: a controlled study. Annals of General Psychiatry,6(1), 1–7. http://dx.doi.org/10.1186/1744-859x-6-4
Cicchetti, D. V. (1994). Guidelines, criteria, and rules of thumbfor evaluating normed and standardized assessment instru-ments in psychology. Psychological Assessment, 6(4),284–290. http://dx.doi.org/10.1037/1040-3590.6.4.284
Compton, R. R., & Ellison-Potter, P. (2008).Teen driver crashes:A report to congress. (DOT HS 811 005). Washington, DC:National Highway Traffic Safety Administration.
Curry, A. E., Hafetz, J., Kallan, M. J., Winston, F. K., & Durbin,D. R. (2011). Prevalence of teen driver errors leading to seriousmotor vehicle crashes. Accident Analysis & Prevention, 43(4),1285–1290. http://dx.doi.org/10.1016/j.aap.2010.10.019
Dishion, T. J., Nelson, S. E., & Bullock, B. M. (2004). Prematureadolescent autonomy: Parent disengagement and deviantpeer process in the amplification of problem behaviour.Journal of Adolescence, 27(5), 515–530. http://dx.doi.org/10.1016/j.adolescence.2004.06.005
Edwards, G., Barkley, R. A., Laneri, M., Fletcher, K., &Metevia,L. (2001). Parent–adolescent conflict in teenagers with adhdand odd. Journal of Abnormal Child Psychology, 29(6),557–572. http://dx.doi.org/10.1023/a:1012285326937
Evans, S. W., Brady, C. E., Harrison, J. R., Bunford, N., Kern,L., State, T., & Andrews, C. (2012). Measuring ADHD andODD symptoms and impairment using high schoolteachers' ratings. Journal of Clinical Child & AdolescentPsychology, 42(2), 197–207. http://dx.doi.org/10.1080/15374416.2012.738456
Eyberg, S. M., Nelson, M. M., Duke, M., & Boggs, S. R.(2005). Manual for the Dyadic Parent-Child InteractionCoding System (3rd ed.). Retrieved September 14, 2012.
Fabiano,G.A., Pelham, J.W.E.,Waschbusch,D.A.,Gnagy, E.M.,Lahey, B. B., Chronis, A. M.,… Burrows-MacLean, L. (2006).A practical measure of impairment: Psychometric properties ofthe impairment rating scale in samples of childrenwith attentiondeficit hyperactivity disorder and two school-based samples.Journal of Clinical Child & Adolescent Psychology, 35(3),369–385. http://dx.doi.org/10.1207/s15374424jccp3503_3
Fischer, M., Barkley, R. A., Smallish, L., & Fletcher, K. (2007).Hyperactive children as young adults: Driving abilities, safedriving behavior, and adverse driving outcomes. AccidentAnalysis & Prevention, 39(1), 94–105. http://dx.doi.org/10.1016/j.aap.2006.06.008
Hartos, J., Eitel, P., & Simons-Morton, B. (2001). Doparent-imposed delayed licensure and restricted drivingreduce risky driving behaviors among newly licensed teens?
Prevention Science, 2(2), 113–122. http://dx.doi.org/10.1023/a:1011595714636
Hartung, C., McCarthy, D., Milich, R., & Martin, C. (2005).Parent–adolescent agreement on disruptive behaviorsymptoms: A multitrait-multimethod model. Journal ofPsychopathology and Behavioral Assessment, 27(3),159–168. http://dx.doi.org/10.1007/s10862-005-0632-8
Holm, S. (1979). A simple sequentially rejective multiple testprocedure. Scandinavian Journal of Statistics, 6(2), 65–70.http://dx.doi.org/10.2307/4615733
Jaccard, J., & Guilamo-Ramos, V. (2002). Analysis of varianceframeworks in clinical child and adolescent psychology: Issuesand recommendations. Journal ofClinicalChild andAdolescentPsychology, 31(1), 130–146. http://dx.doi.org/10.1207/153744202753441747
Jerome, L., Segal, A., & Habinski, L. (2006). What we knowabout adhd anddriving risk: A literature review,meta-analysisand critique. Journal of the Canadian Academy of Child andAdolescent Psychiatry, 15(3), 105–125.
McGehee, D. V., Raby,M., Carney, C., Lee, J. D., &Reyes,M. L.(2007). Extending parental mentoring using an event-triggeredvideo intervention in rural teen drivers. Journal of SafetyResearch, 38(2), 215–227. http://dx.doi.org/10.1016/j.jsr.2007.02.009
Minino, A. (2010). Mortality among teenagers aged 12-19years: United States, 1999-2006 (Data Brief No. 37).Retrieved from http://www.cdc.gov/nchs/data/databriefs/db37.pdf
Pelham, W. E., Gnagy, E. M., Greenslade, K. E., & Milich, R.(1992). Teacher ratings of DSM-III-R symptoms for thedisruptive behavior disorders. Journal of the AmericanAcademy ofChild&Adolescent Psychiatry, 31(2), 210–218.
Pelham, W. E. Jr., Fabiano, G. A., & Massetti, G. M. (2005).Evidence-based assessment of attention deficit hyperactivitydisorder in children and adolescents. Journal of Clinical Childand Adolescent Psychology, 34(3), 449–476. http://dx.doi.org/10.1207/s15374424jccp3403_5
Robin, A. (2006). Training families with adolescents with adhd. InR. A. Barkley (Ed.), Attention-deficit hyperactivity disorder: Ahandbook for diagnosis and treatment (3rd ed., pp. 499–546).New York, NY: Guilford Press.
Shrout, P. E., & Fleiss, J. L. (1979). Intraclass correlations: Usesin assessing rater reliability. Psychological Bulletin, 86(2),420–428. http://dx.doi.org/10.1037/0033-2909.86.2.420
Thompson, A. L., Molina, B. S. G., Pelham, W., Jr., & Gnagy,E. M. (2007). Risky driving in adolescents and young adultswith childhood ADHD. Journal of Pediatric Psychology,32(7), 745–759. http://dx.doi.org/10.1093/jpepsy/jsm002
RECEIVED: April 4, 2013ACCEPTED: August 23, 2013Available online 5 September 2013