“papanicolaou was penniless off the ship. he was selling ... guidelines 2012 asc-us repeat pap @ 6...
TRANSCRIPT

1
Rana HodaSyed Hoda
Papanicolaou Cytology LaboratoryCornell University, New York
The Pap Test: Current Criteria and Changing Concepts
La prueba de Papanicolaou: Criterios actuales y conceptos cambiantes
“Papanicolaou was penniless off the ship. He was selling carpets to survive. He was a terrible salesman, and he finally got a research job at Cornell…”
Sid Mukherjee: The Emperor of All Maladies
Cervical Cancer: Incidence & Mortality
123456789
1011121314
75-7
9
80-8
4 85 86 87 88 89 90 91 92 93 94 95 96 97 98 9920
00
123456789
1011121314
75-7
9
80-8
4 85 86 87 88 89 90 91 92 93 94 95 96 97 98 9920
00
Incidence
Mortality
American Cancer Society, 2014
The Pap Test:biggest success story in
cancer screening
“Pap”
Pap smear was routine for all women admitted to The New York Hospital in 1939Pap smear was routine for all women admitted to The New York Hospital in 1939
Cervical Cancer in United States
In USA
12,360 new cases of cervical ca in 2014
~ 4,000 deaths in 2014
Saslow, CA Cancer J Clin 2012
Cervical Cancer in Argentina
In Argentina, cervical cancer is the #2 cause of cancer deaths in young women
Squamous carcinoma is most common
5-year-survival with early detection: >90%
WHO 6
2
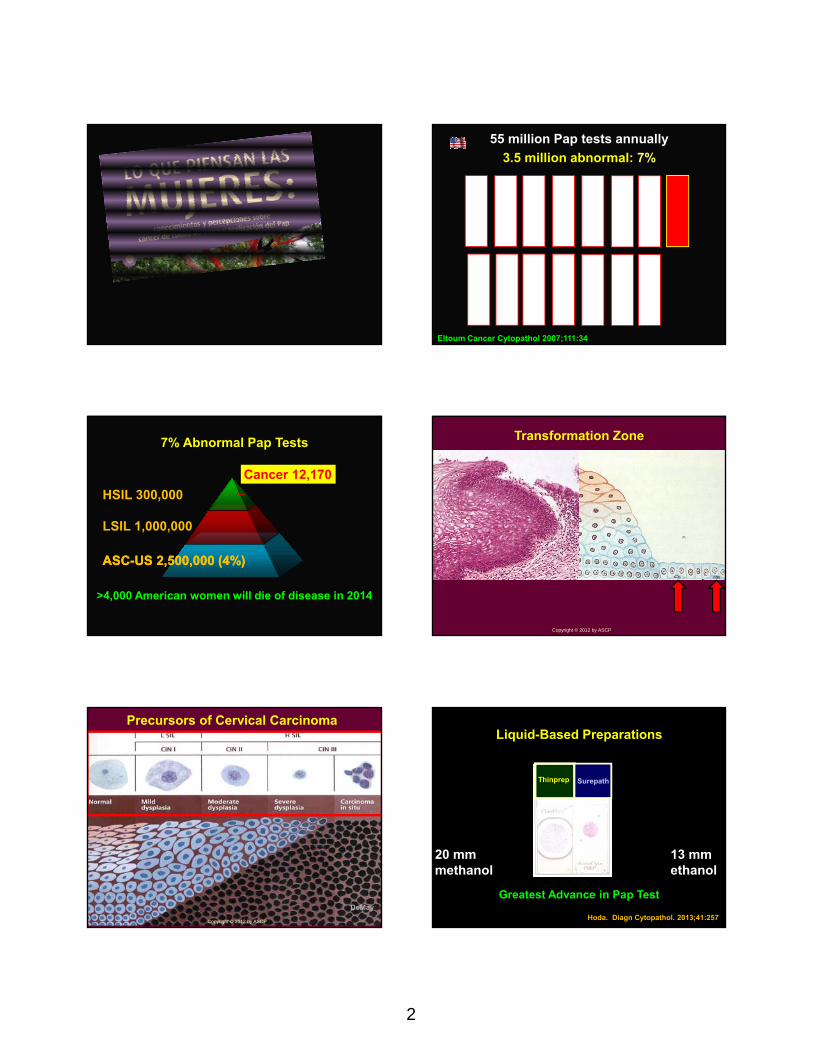
55 million Pap tests annually
3.5 million abnormal: 7%
Eltoum Cancer Cytopathol 2007;111:34
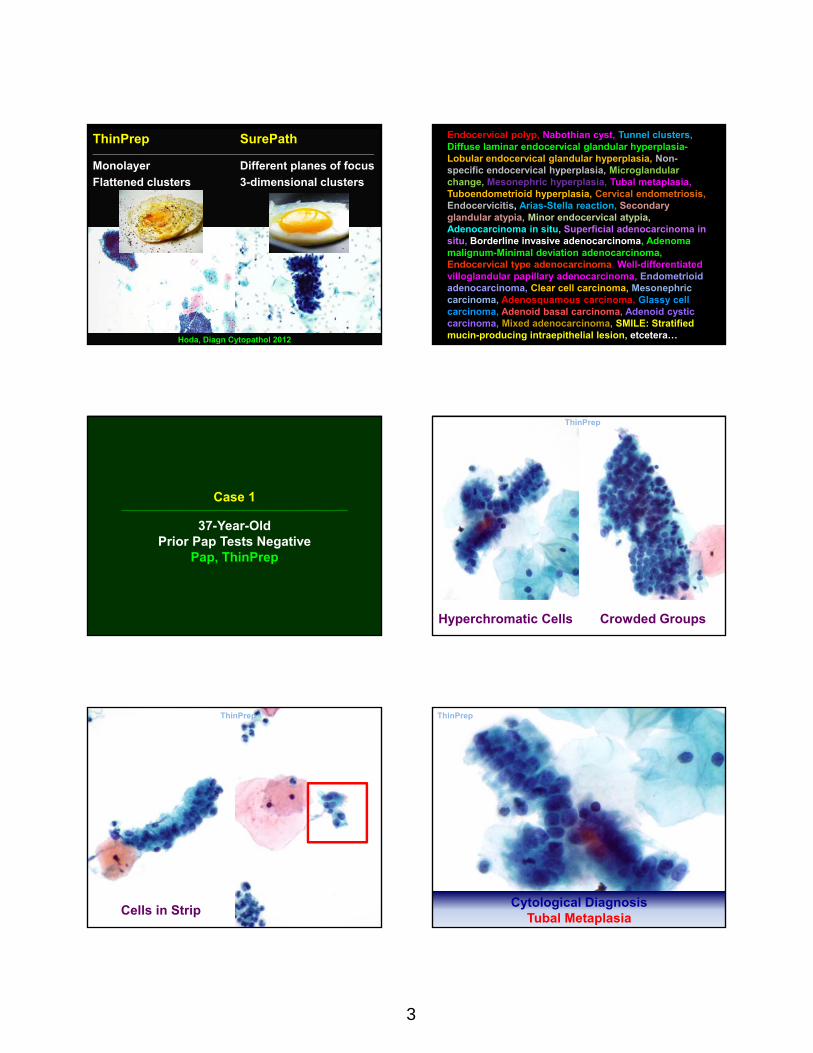
ASC-US 2,500,000 (4%)ASC-US 2,500,000 (4%)
LSIL 1,000,000
HSIL 300,000
7% Abnormal Pap Tests
Cancer 12,170
>4,000 American women will die of disease in 2014
Transformation Zone
Copyright © 2012 by ASCP
Precursors of Cervical Carcinoma
DeMay
Copyright © 2012 by ASCP
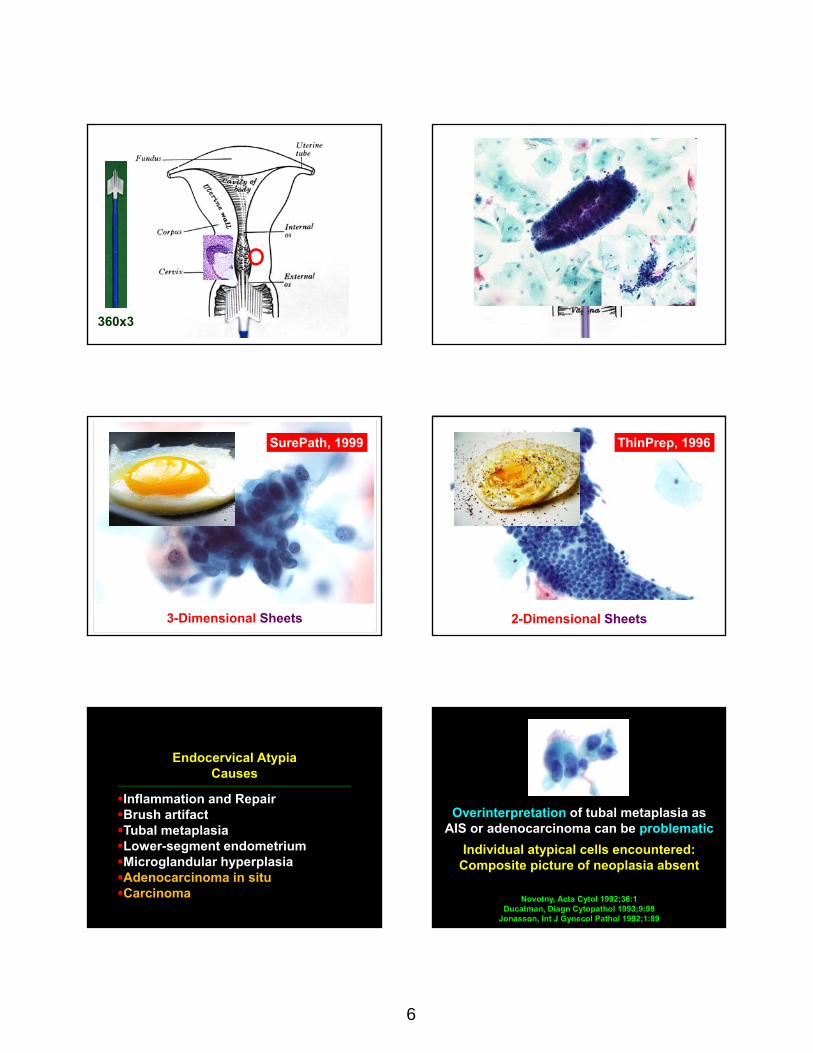
Liquid-Based Preparations
20 mm 13 mmmethanol ethanol
Thinprep Surepath
Greatest Advance in Pap Test
Hoda. Diagn Cytopathol. 2013;41:257
3
ThinPrep SurePath______________________________________________________________________________________
Monolayer Different planes of focus
Flattened clusters 3-dimensional clusters
Hoda, Diagn Cytopathol 2012
Endocervical polyp, Nabothian cyst, Tunnel clusters, Diffuse laminar endocervical glandular hyperplasia-Lobular endocervical glandular hyperplasia, Non-specific endocervical hyperplasia, Microglandularchange, Mesonephric hyperplasia, Tubal metaplasia, Tuboendometrioid hyperplasia, Cervical endometriosis, Endocervicitis, Arias-Stella reaction, Secondary glandular atypia, Minor endocervical atypia, Adenocarcinoma in situ, Superficial adenocarcinoma in situ, Borderline invasive adenocarcinoma, Adenoma malignum-Minimal deviation adenocarcinoma, Endocervical type adenocarcinoma, Well-differentiated villoglandular papillary adenocarcinoma, Endometrioidadenocarcinoma, Clear cell carcinoma, Mesonephriccarcinoma, Adenosquamous carcinoma, Glassy cell carcinoma, Adenoid basal carcinoma, Adenoid cystic carcinoma, Mixed adenocarcinoma, SMILE: Stratified mucin-producing intraepithelial lesion, etcetera…
Case 1_______________________________________________________________________________
37-Year-Old Prior Pap Tests Negative
Pap, ThinPrep
Crowded GroupsHyperchromatic Cells
ThinPrep
Cells in Strip
ThinPrep
Cytological DiagnosisTubal Metaplasia
ThinPrep

4
Tubal metaplasia seen in 30-100% of normal endocervixBabkowski, Am J Clin Pathol 1994;101:376
Jonasson, Int J Gynecol Pathology 1992;11:89
Ciliated, mucinous, intercalated
R
Endocervical Cell
50m2AIS: 75m2
IIIIIIIII
Endocervical Cell
Age: 35+
IIIIIIIII
Ciliated Endocervical Cell
Tubo-endometrioid metaplasiaTubal metaplasia sans cilia, post-cone
_____Glandular “Crowding”
Palmate Folds

5
sterile
I“septic”I“spinnbarkeit”
Nuclear “Nipple”
Progesterone Effect
Koizumi, Diagn Cytopathol 1998;15:161
Ramsey
uuII uuII uuII
uuII uuIIBirth Infancy Puberty
Adult Ectropion Menopause
Transformation Zone
Physiological Ectopy
360
Day 14
Gray’s Anatomy
90
6
360x3
SurePath, 1999
3-Dimensional Sheets 2-Dimensional Sheets
ThinPrep, 1996
Endocervical AtypiaCauses
_______________________________________________________________________________________________
Inflammation and RepairBrush artifactTubal metaplasiaLower-segment endometriumMicroglandular hyperplasiaAdenocarcinoma in situCarcinoma Novotny, Acta Cytol 1992;36:1
Ducatman, Diagn Cytopathol 1993;9:98Jonasson, Int J Gynecol Pathol 1992;1:89
Overinterpretation of tubal metaplasia as AIS or adenocarcinoma can be problematic
Individual atypical cells encountered:Composite picture of neoplasia absent

7
?
1
Repair
2
Low-Grade Squamous Intraepithelial Lesion, LSIL
3
Adenocarcinoma In Situ
4
Benign Endometrial Cells
5
Endometrial Adenocarcinoma

8
6
High Grade Squamous Intraepithelial Lesion, HSIL
Vermeer
Bethesda System Abnormalities in Pap test
ASC-US ASC-H LSIL HSIL
squamous
invasive squamous cancer
LSIL-H
Case #2_________________________________
30-year-old woman with previous
normal Paps
TP
Diagnosis: Atypical Squamous Cells of Undetermined Significance, ASC-US
ASC-US, Most cases of ASC
Cytological features suggestive of LSIL
~4-5% of all abnormal Pap diagnoses
HPV +, ~ 50%
HSIL, 5-17%

9
Types of ASCUS
ASCUS, NOS
ASCUS in atrophy
ASCUS, atypical parakeratosis
Spectrum of lesions ranges from reactive to invasive carcinoma
Hoda. Cytojournal. 2008 Apr 24;5:10TP
ASCUS, NOS
ASC-USAtypical Parakeratosis
TP
ASCUS in Atrophy
SP
Koilocyte-like PKbi- or multinucleation
Steinman Acta Cytol. 2008;52:279
ASCUS FeaturesHormonal Rx Candida
Moriarty, Archiv Pathol Lab Med 2009;133:1272 SP
ASC-H mimics

10
ASCCP Guidelines 2012 ASC-US
Repeat Pap @ 6 & 12 moDetects 73% HSIL
Colposcopy
HPV-DNA testDetects 93% HSIL
Screening Guidelines for Prevention & Early Detection of Cervical Cancer, 2012
__________________________________
Updated, for Pap screening & in the management of adolescents & young
women with abnormal cytology
Am J Clin Pathol 2012;137:516
Summary of Recommendations
Age < 21 y:
No screening
HPV test should not be used with ASC-US
Age 21-29 y: Cytology alone x 3y
Age 30-65: HPV & cytology ‘‘cotesting’’ x 5y Age > 65 y: No screening with negative hx
After hysterectomy: No screening
Saslow, CA Cancer J Clin 2012. Am J Clin Pathol 2012;137:516
Human Papillomavirus (HPV)__________________________________
Oncogenic virus that causes >99% of cervical cancer
There are of 14 types of high-risk HPV
HPV16 or HPV18 infection carries a high risk & are detected in ~70% of cervical cancers
Wright & Schiffman NEJM 2003;348:489. Saslow AJCP, 2012;137:516
HPV test is FDA-approved for…__________________________________
Primary screening, 2014
Cobas HPV test screening starts at 25 yrs
Reflex HPV Test: HR-HPV DNA test, 1999
For triage of ASC-US to determine need for colposcopy
Primary Adjunctive Screening: DNAwithPapTest, 2003
Women ≥30 to detect (-) of HPV
Available HPV Tests__________________________________
Hybrid Capture 2 [(HC2), Qiagen, MD)
Cervista (Hologic, Bedford, MA)
Aptima (Hologic, Bedford, MA)
Cobas (Roche System, Pleasanton, CA)
11
HC2 vs. Cobas HPV Test__________________________________
Both provide pooled results for hrHPV
Cobas HPV Test:
Simultaneously provides HPV16/HPV18 identification
Less cross-reactivity with lrHPV types
Screening with HPV Testing vs. Pap Test for the detection of ≥CIN2
__________________________________
Sensitivity
HPV DNA testing ~92%
Pap test (LBP) ~60%
Specificity
HPV DNA testing ~94%
Pap test (LBP) ~97%
Wright & Schiffman NEJM 2003;348:489. Saslow AJCP, 2012;137:516
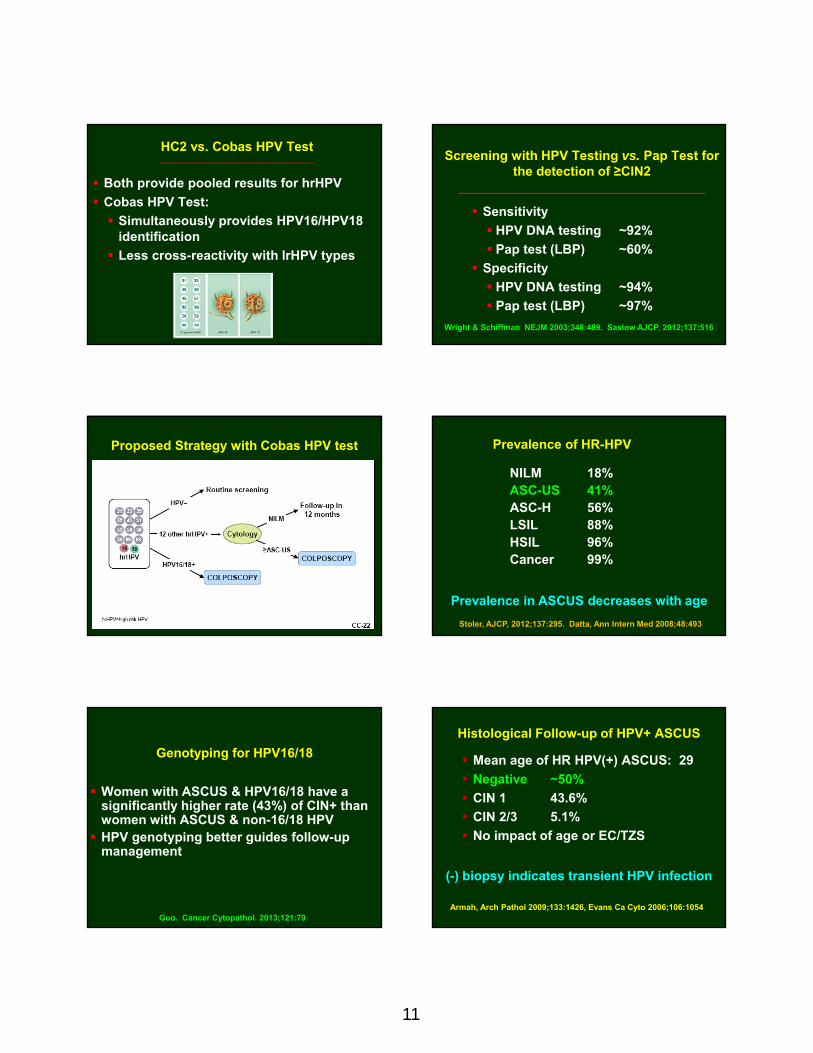
Proposed Strategy with Cobas HPV test Prevalence of HR-HPV
NILM 18%ASC-US 41%ASC-H 56% LSIL 88%HSIL 96%Cancer 99%
Stoler, AJCP, 2012;137:295. Datta, Ann Intern Med 2008;48:493
Prevalence in ASCUS decreases with age
Genotyping for HPV16/18
Women with ASCUS & HPV16/18 have a significantly higher rate (43%) of CIN+ than women with ASCUS & non-16/18 HPV HPV genotyping better guides follow-up
management
Guo. Cancer Cytopathol. 2013;121:79
Histological Follow-up of HPV+ ASCUS
Mean age of HR HPV(+) ASCUS: 29
Negative ~50%
CIN 1 43.6%
CIN 2/3 5.1%
No impact of age or EC/TZS
Armah, Arch Pathol 2009;133:1426, Evans Ca Cyto 2006;106:1054
(-) biopsy indicates transient HPV infection

12
HPV (-), Cytology ASC-US
Risk of precancerous lesions is low
Recommend continued routine screening
Saslow. Am J Clin Pathol 2012;137:516; Hoda, USCAP abstract 2014
HPV (+), Cytology (-)
Repeat co-testing in 12 months
HPV 16/18 genotyping
Case #3________________________________
37-year-old woman
All prior Paps: Normal
Diagnosis: Atypical Squamous Cells, cannot exclude High-Grade Dysplasia, ASC-H
TPASC-H Definition,per Bethesda 2001
________________________________
Changes suggestive of HSIL,
but lacks definitive criteria
~5-10% of all ASC
0.3-0.6% of all Pap diagnoses
HPV +, ~ 65%
HSIL, 24-68%
Selvaggi. Diagn Cyto. 2013;41:943; Sherman, Cancer Cyto 2006;108:298
ASCCP Guidelines 2006 ASC-H
Colposcopy
28% may require > one bx
ASC-HSyncytia, disorganized cells
TPSP
Coarse nuclear chromatin is associated with HSIL, 84%
Gupta. Diagn Cytopathol. 2013;41:520

13
ASC-H, Hyperchromatic crowded groups
TP“Steep sides” & “straight edges”SP
ASC-H, Small “walnutty” atypical metaplastc cells
Histiocytes
IUD cell
Reactive
ASC-H mimics
MGH
ASC-H & Histological Correlation________________________________
HSIL 52%
CIN 2 20%
CIN 3 32%
Premenopausal 65%
Postmenopausal 35%
LSIL 23%
Benign 25%
Selvaggi. Diagn Cytopathol. 2013;41:943
ASC-US
~90% of ASC
HPV 16/18: 50%
HSIL 5–17%
HPV triage
ASC-H
~10% of ASCHPV 16/18: <85%HSIL 24–68%> colposcopy
Hoda & Hoda. Fundamentals of Pap Test Cytology, 2007
Case #4________________________________
28-year-old Woman
Routine Pap Test
14
TP
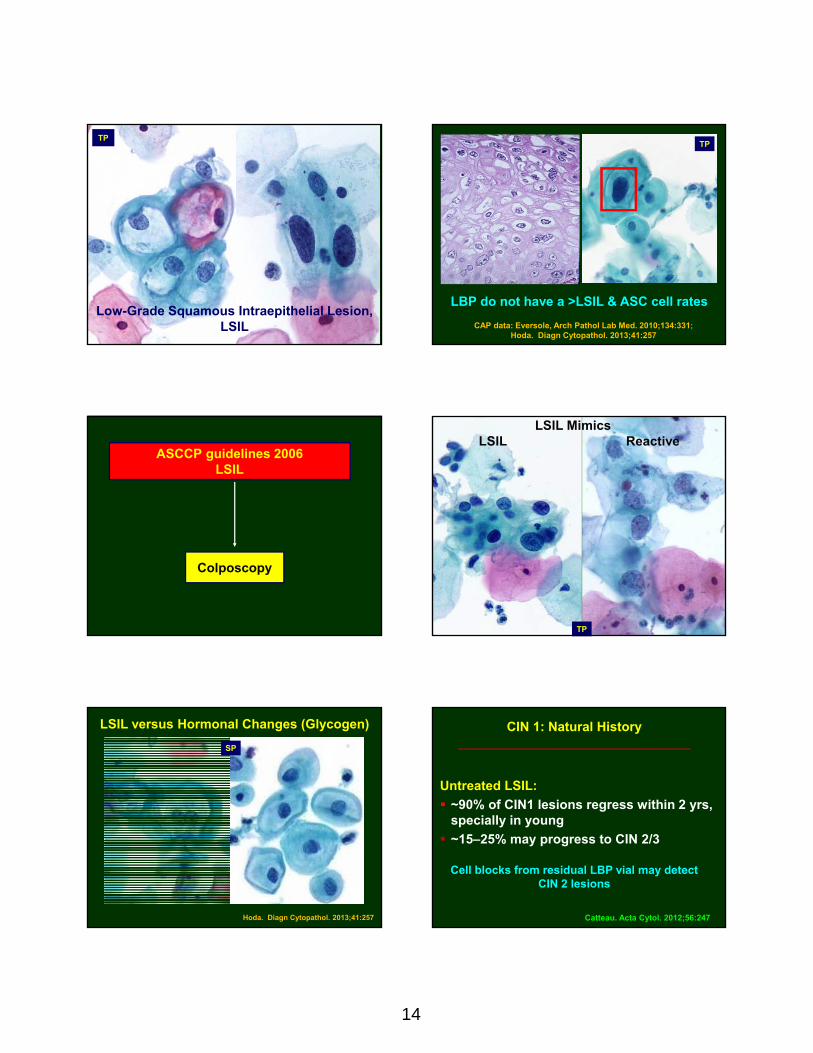
Low-Grade Squamous Intraepithelial Lesion, LSIL
TP
LBP do not have a >LSIL & ASC cell rates
CAP data: Eversole, Arch Pathol Lab Med. 2010;134:331; Hoda. Diagn Cytopathol. 2013;41:257
ASCCP guidelines 2006 LSIL
Colposcopy
LSIL MimicsLSIL Reactive
TP
LSIL versus Hormonal Changes (Glycogen)
SP
Hoda. Diagn Cytopathol. 2013;41:257
Untreated LSIL:
~90% of CIN1 lesions regress within 2 yrs, specially in young
~15–25% may progress to CIN 2/3
CIN 1: Natural History________________________________
Cell blocks from residual LBP vial may detectCIN 2 lesions
Catteau. Acta Cytol. 2012;56:247

15
CINtec Plus Test (Roche Lab, Heidelberg, Germany)
p16INK4a is a cellular kinase inhibitor believed to be a surrogate marker for active HPV infection
p16INK4a is a marker for underlying HSIL
Ki-67 is nuclear antigen & cell proliferation marker expressed in all cell cycle phases except G0
Coexpression of p16INK4a & Ki-67 identifies deregulated cells
Waldstrom. Cancer Cytopathol. 2013;121:136
CINtec PLUS test
p16INK4a stain the cytoplasm brown & Ki-67 stain nucleus red
Sensitivity for detection of CIN3 in LSIL samples is high, 95.8%
CINtec + CINtec in LSIL
Borderline Category between LSIL & HSIL
LSIL, Cannot Exclude HSIL (LSIL-H)
The discrepancy rate between low- and high-grade lesions ranges from 9.8 to 15%
TBS, 2008
LSIL, cannot exclude HSIL (LSIL-H)
Elsheikh Cancer Cyto 2006;108:277
Atypical keratinized cells
LSIL-H
HSIL-like cells with unequivocal LSIL
0.15% - 0.35% Paps
Risk of: hrHPV & histologic CIN 2/3
LSIL-H 90% 30%
HSIL 96% 70%
LSIL 80% 13%
ASC-H 54% 17%
Baron. Am J Clin Pathol. 2014;141:239Walavalkar. Cancer Cytopathol. 2014;122:123
Case #5________________________________
Routine Pap in a 37-year-old
with
Intra-Uterine Device

16
High-Grade Squamous Intraepithelial Lesion ~HSIL
TP
HSIL
Uncommon diagnosis, <1%
proportion in age ≥ 30 years
HSIL Carries a high risk of significant disease
Biopsy follow-up
70%-75% CIN 2/3
1%-2% Cervical ca
HSIL Criteria, Bethesda 2001
Syncytia N:C Metaplastic-type cells
TP TP
Nuclei: coarse chromatin, grooves, irregular
HSIL, Syncytia
HSILSP
Small “walnutty” cells, Nuclei 2-3x interm. cell nucleus, Look in empty spaces Bare nuclei
TPHSIL

17
CIN2 versus CIN3
Subclassifying is not crucial
47% of CIN2 Paps were CIN2 on biopsy
53% discordant, most were LSIL on biopsy
Howell, Diagn Cytopathol 2004;30:362
HSIL Involving Endocervical glands
SP
Features HSIL in EC glands AIS
_________________________________________
Central cell polarity - +
Overlapping + -
Nucleoli micro prominent
‘Feathering’ - +
p63 + -
Apoptosis -/+ +
Mitoses -/+ +
High N:C + +
p16 overexpressed + +
Kir. J Cytol. 2012;29:121; Wood Diag Cytopathol 2007;35:12 AIS vs HSIL in ECG
25% to 75% of cases have both
HSIL Small cell ca
TTF1 +Hoda, USCAP Poster 2012
39%
31%
10%
20%
Most Common Pap Dx Preceding HSIL on Bx
44.5% of Pap Preceding HSIL on Bx were diagnosed as HSIL

18
Missed HSIL cases: Small, pale cells
Khalbuss. Cytojournal. 2013 Aug 30;10
Differential Diagnosis
HSILImmature Squamous
Metaplasia
Atrophy HSIL, Syncytia
Basal Cell Sheets in Atrophy Mimic HSIL
TP
TP
LUS vs HSIL
HSIL
Benign Endometrial Cells Mimic HSIL
TP
EMC
SP
Hoda. Diagn Cytopathol. 2013;41:257
TP
IUD vs HSIL
Pinto, Acta Cytol. 2012;56:109. Ge, Acta Cytol. 2012;56:55

19
False-Positive for HSIL
Atrophic vaginitis
Repair
HSV
Crothers. Arch Pathol Lab Med. 2014;138:613
HSVrepairAV
ASCCP Guidelines 2006 HSIL
Colposcopy
5-year CIN 2+ risk after 2 negative cotests(hrHPV + Pap) is 1.5% & is more reassuring against recurrent CIN 2+ than either (-) Pap or HPV test alone
Katki. J Low Genit Tract Dis. 2013;17(5 Suppl 1):S78
Role of HPV Test in HSIL________________________________
Segunda parte del Curso Corto
Case 6________________________________
48-year-old womanroutine Pap test
ThinPrep
------
TP

20
Squamous carcinoma
TP SP
Differential Diagnosis
TP
Repair Non-keratinizing sq. ca
Fiber cell
Squamous Cell Ca, Keratinizing
Tadpole cell
Background in atrophy mimics Squamous Ca
Selvaggi Diagn Cyto 2002:27:362
TP
ASC-US ASC-H
LSILHSIL
Squamous Ca
29% increase in incidence in recent years
Dr. Pap

21
Case #7________________________________________________
64-year-old, postmenopausal
Prior Paps: negative
History: Breast cancer, 2004
Medications: Estrogen 5 years until 2002
ThinPrep
Cellular, mucin, architecture variability
Loose sheets,
mucinous cytoplasm
Nuclei, palisaded, lobate,
irregular, nucleoli
Strips, columnar cells & dark oval nuclei
Cytological Diagnosis__________________________________________________
Atypical Glandular Cellsof Endocervical Origin
AGC, EC
AGC: Initial Workup_____________________________________________________________________________________
ECC: Dissolved on processingEMBx: Endometrial polyp
HPV: Negative
22
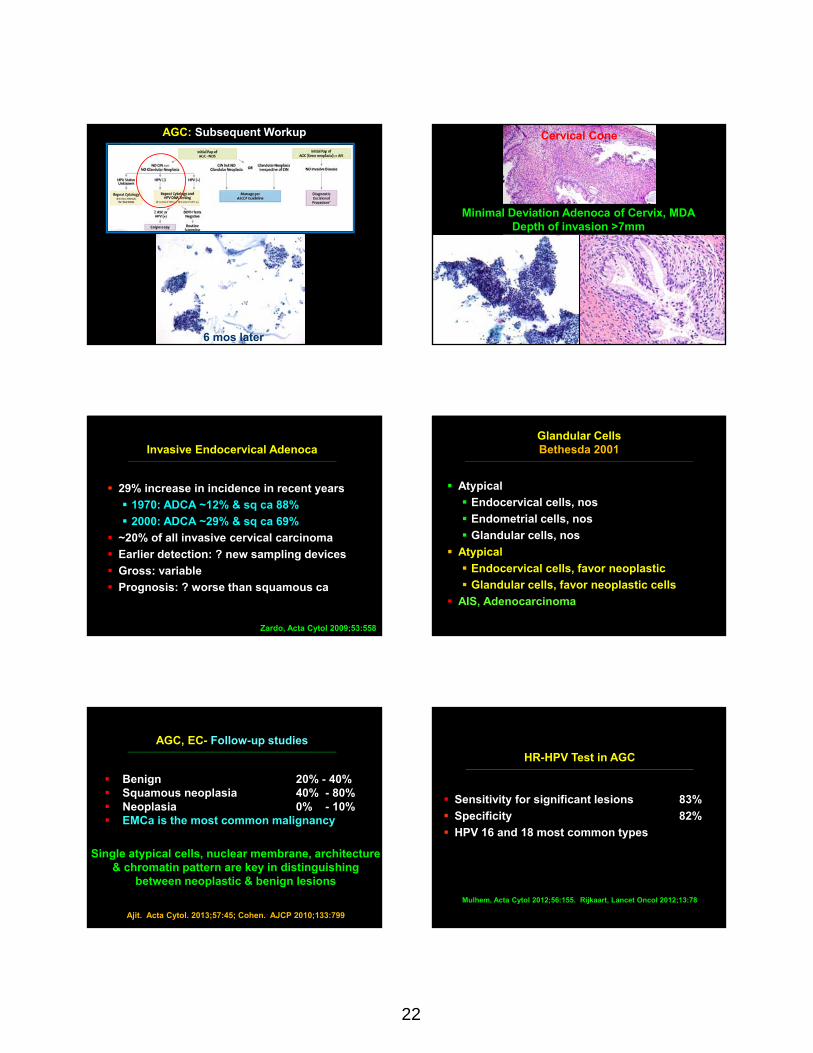
AGC: Subsequent Workup_____________________________________________________________________________________
6 mos later
Cervical Cone
Minimal Deviation Adenoca of Cervix, MDADepth of invasion >7mm
Invasive Endocervical Adenoca_____________________________________________________________________________________
29% increase in incidence in recent years
1970: ADCA ~12% & sq ca 88%
2000: ADCA ~29% & sq ca 69%
~20% of all invasive cervical carcinoma
Earlier detection: ? new sampling devices
Gross: variable
Prognosis: ? worse than squamous ca
Zardo, Acta Cytol 2009;53:558
Glandular CellsBethesda 2001
____________________________________________________________________________________
Atypical
Endocervical cells, nos
Endometrial cells, nos
Glandular cells, nos
Atypical
Endocervical cells, favor neoplastic
Glandular cells, favor neoplastic cells
AIS, Adenocarcinoma
AGC, EC- Follow-up studies_____________________________________________________________________________________
Benign 20% - 40% Squamous neoplasia 40% - 80% Neoplasia 0% - 10% EMCa is the most common malignancy
Ajit. Acta Cytol. 2013;57:45; Cohen. AJCP 2010;133:799
Single atypical cells, nuclear membrane, architecture & chromatin pattern are key in distinguishing
between neoplastic & benign lesions
HR-HPV Test in AGC____________________________________________________________________________________
Sensitivity for significant lesions 83%
Specificity 82%
HPV 16 and 18 most common types
Mulhem, Acta Cytol 2012;56:155. Rijkaart, Lancet Oncol 2012;13:78
23
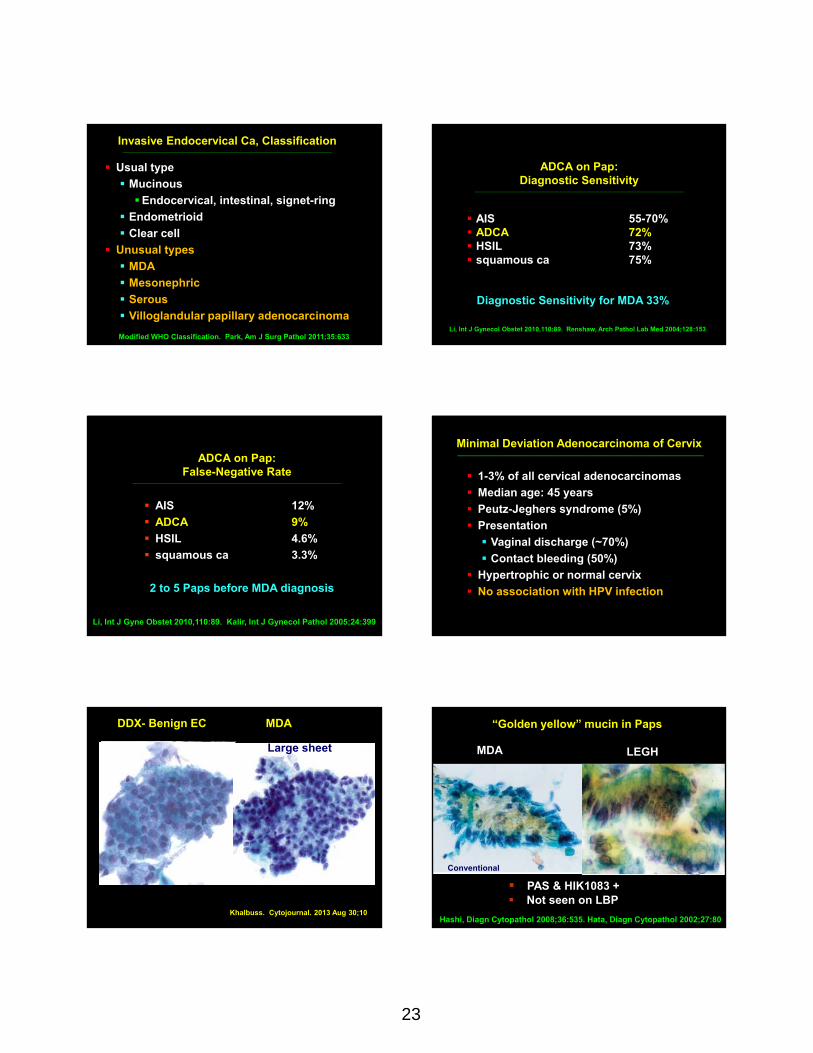
Usual type
Mucinous
Endocervical, intestinal, signet-ring
Endometrioid
Clear cell
Unusual types
MDA
Mesonephric
Serous
Villoglandular papillary adenocarcinoma
Invasive Endocervical Ca, Classification_____________________________________________________________________________________
Modified WHO Classification. Park, Am J Surg Pathol 2011;35:633
ADCA on Pap: Diagnostic Sensitivity
_____________________________________________________________________________________
AIS 55-70% ADCA 72% HSIL 73% squamous ca 75%
Li, Int J Gynecol Obstet 2010,110:89. Renshaw, Arch Pathol Lab Med 2004;128:153
Diagnostic Sensitivity for MDA 33%
ADCA on Pap: False-Negative Rate
_____________________________________________________________________________________
AIS 12%
ADCA 9%
HSIL 4.6%
squamous ca 3.3%
Li, Int J Gyne Obstet 2010,110:89. Kalir, Int J Gynecol Pathol 2005;24:399
2 to 5 Paps before MDA diagnosis
Minimal Deviation Adenocarcinoma of Cervix
1-3% of all cervical adenocarcinomas
Median age: 45 years
Peutz-Jeghers syndrome (5%)
Presentation
Vaginal discharge (~70%)
Contact bleeding (50%)
Hypertrophic or normal cervix
No association with HPV infection
___________________________________________________________________
MDA
CS - MDA
DDX- Benign EC
Khalbuss. Cytojournal. 2013 Aug 30;10
Large sheet
“Golden yellow” mucin in Paps
Hashi, Diagn Cytopathol 2008;36:535. Hata, Diagn Cytopathol 2002;27:80
PAS & HIK1083 + Not seen on LBP
Conventional Pink mucin in normal EC
MDA LEGH

24
Review of Histologically-proven MDA from 1975-2009
Precise pre-op diagnosis:
by Pap & bx remains difficult
IHC: CEA, Ki67, AB/PAS, HIK1083 & SMA
Tsuji, Histopathol 2011;59:55. Li, Int J Gynecol Obstet 2010,110:89
_____________________________________________________________________Treatment of MDA
Radical hysterectomy
_____________________________________________________________
MDAon Liquid-Based Preps
Diagnostic dilemma Golden-yellow mucin not seen HPV test & p16 are negative
Case #8_____________________________________________________________________________________
36-year-old, Pap, ThinPrep
Previous Paps: Negative
Clinically: Ectropion
ThinPrep
Clean background, HCG & sheets
ThinPrep
Palisading
Nuclei dark, oval, chromocenters, high N/C

25
Cytological Diagnosis_____________________________________________________________________________________
Adenoca In Situ of Endocervix
AIS
Colposcopy, Cervical & Endometrial Biopsies Followed
Biopsies: Negative
Ectropion LEGH
__________________________________________________________
Cone: AIS
Repeat Pap 4 weeks later: AIS
At transformation zone Precursor of adenocarcinoma Symptomatic: 3% Incidence 0.61/100,000 Multifocal-multicentric in 50% Rx: Cone, Hysterectomy
_______________________________________________________________________________
AISBasics
_____________________________________________________________________________________
Zardo, Acta Cytol 2009;53:558
ECA ~43, AIS ~37 AIS > ECA: ~13 yrs CIS to Squamous ca: ~18 yrs AIS usually adjacent to ECA HPV: 18 & 16
________________________________________________________________________
AIS & ECARelationship
_____________________________________________________________________________________
Zardo, Acta Cytol 2009;53:558. Plaxe, Gynecol Oncol 1999;75:55
AIS 55-70% ECA 72% HSIL 73% Squamous ca 75%
AIS on PapSensitivity
_____________________________________________________________________________________
Xing. Cancer Cyto. 2014;122:8; Hoda. Diagn Cytopathol. 2011;39:730
Cell blocks may detect a significantly more endocervical or endometrial adenocarcinoma
compared with the ThinPrep alone (36% vs 8%)

26
AIS 12% ECA 9% HSIL 4.6% Squamous ca 3.3%
AIS on PapFalse-negative
_____________________________________________________________________________________
AIS not detectable by Pap if TZ spared, 54% vs. 25%, p = 0.036
Kalir, Int J Gynecol Pathol 2005;24:399
Clean background hyperchromatic crowded groups Columnar monomorphous cells Nuclei crowded, molded Stippled chromatin Nucleoli Feathering, rosettes, strips Apoptosis & mitosis_____________________________________________________________________________________
AISDiagnostic Criteria
_____________________________________________________________________________________
Hoda & Hoda. Fundamentals of Pap Test Cytology, 2007.
ThinPrep
Hyperchromatic crowded groups & sheets
Clean background Columnar, crowded cells
Rosettes, Nuclei, nucleoli Apoptosis & Mitosis
Conventional
• Best criterion, PPV 73%
• Feathering & HPV+ =
glandular neoplasia
“Feathering” in Glandular Neoplasia
Rabelo‐Santos, Cytopathol 2008;19:34
Tubal metaplasia Lower uterine segment Reactive endocervical cells Invasive ECA HSIL involving endocervical glands
AISDifferential Diagnosis
_____________________________________________________________________________________
Hoda & Hoda, Fundamentals of Pap Test Cytology, Springer, 2007
27
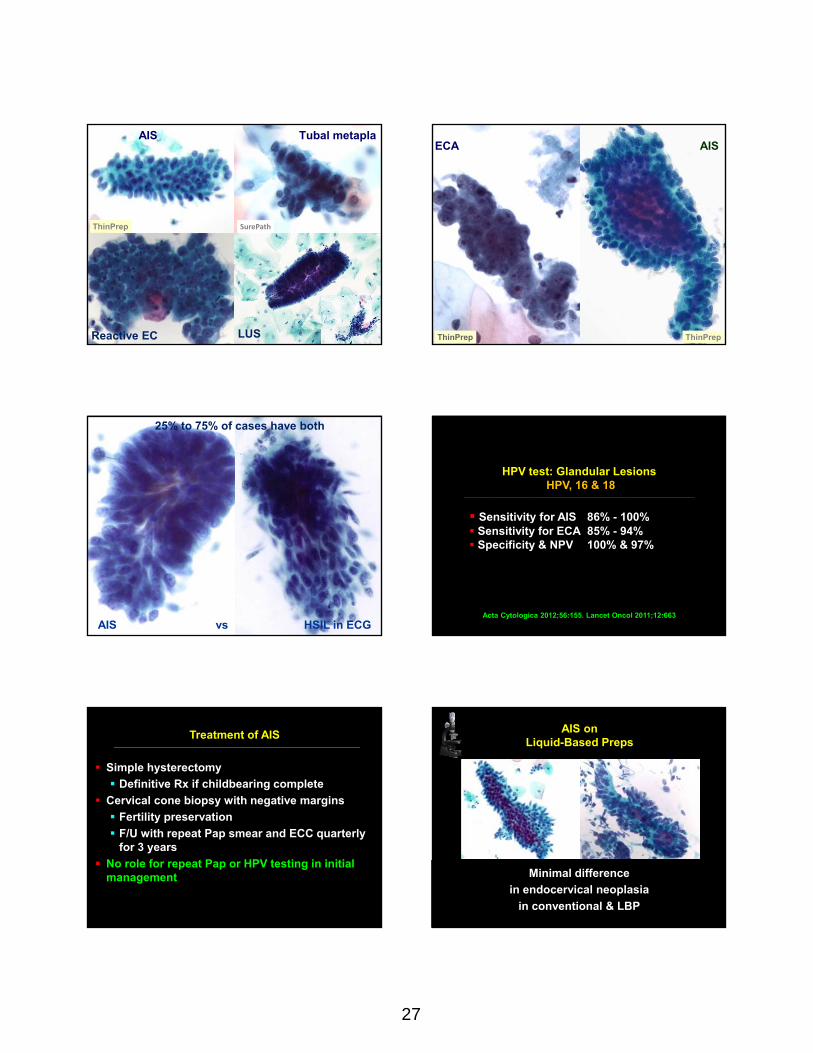
Tubal metapla
SurePath
Reactive EC LUS
AIS
ThinPrep
ECA AIS
ThinPrep ThinPrep
AIS vs HSIL in ECG
25% to 75% of cases have both
HPV test: Glandular LesionsHPV, 16 & 18
_____________________________________________________________________________________
Sensitivity for AIS 86% - 100% Sensitivity for ECA 85% - 94% Specificity & NPV 100% & 97%
Acta Cytologica 2012;56:155. Lancet Oncol 2011;12:663
Treatment of AIS
Simple hysterectomy
Definitive Rx if childbearing complete
Cervical cone biopsy with negative margins
Fertility preservation
F/U with repeat Pap smear and ECC quarterly for 3 years
No role for repeat Pap or HPV testing in initial management
___________________________________________________________________
Minimal difference
in endocervical neoplasia
in conventional & LBP
AIS onLiquid-Based Preps

28
17-year-old
Two previous normal Paps
Pap, ThinPrep
Case 9_________________________________________________________
TeenagerRoutine Pap
ThinPrep
mitosissmooth-contoured papillary
featheringThinPrep
Reported as Negative,
Reactive Endocervical Cells
Cytological Diagnosis_________________________________________________________
ECA Villoglandular Type
Biopsy performed
Hoda. Diagn Cytopathol. 2010;38:633
ECA with Villoglandular ComponentHPV-negative, p16 focally+
Hysterectomy: 2 positive lymph nodes
Why (-)?
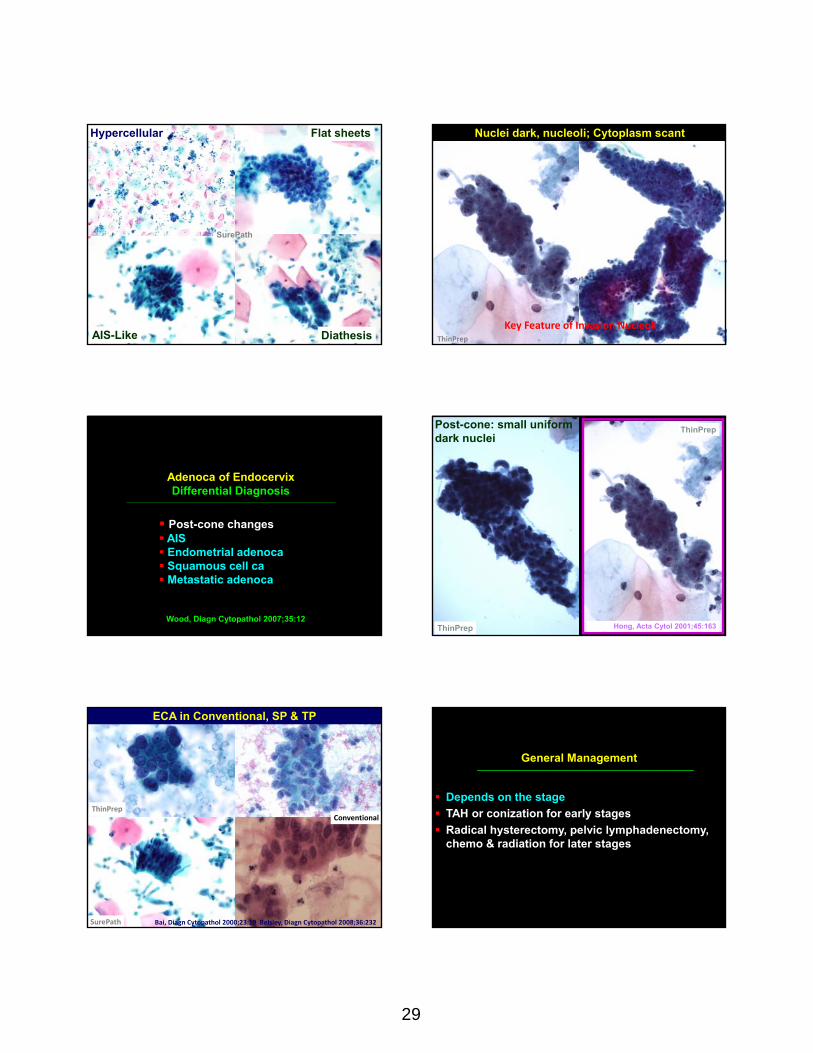
Cytology of Adenoca of Endocervix_____________________________________________________________________________________
Hypercellular
Flat sheets
Nuclei: large, pleomorphic, macronucleoli
Chromatin: uneven
Cytoplasm: finely vacuolated
Diathesis: necrotic, bloody, proteinaceous
Many features of AIS, lack of cohesion
29
Hypercellular Flat sheets
DiathesisAIS-Like
SurePath
Nuclei dark, nucleoli; Cytoplasm scant
Key Feature of Invasion NucleoliThinPrep
Post-cone changes AIS Endometrial adenoca Squamous cell ca Metastatic adenoca
Adenoca of EndocervixDifferential Diagnosis
_____________________________________________________________________________________
Wood, Diagn Cytopathol 2007;35:12Hong, Acta Cytol 2001;45:163
Post-cone: small uniform dark nuclei
ThinPrep
ThinPrep
SurePath
ThinPrepConventional
ECA in Conventional, SP & TP
Bai, Diagn Cytopathol 2000;23:19 Belsley, Diagn Cytopathol 2008;36:232
General Management
Depends on the stage
TAH or conization for early stages
Radical hysterectomy, pelvic lymphadenectomy, chemo & radiation for later stages
___________________________________________________________

30
2012 Cervical Cancer Screening Guidelines
ACS/ACOG/ASCCP
21 yrs: Routine screening starts
21-29 yrs: every 3-yrs
30-65 yrs: Screen every 5 years with Pap/HPV
>65 yrs: No screening if adequate prior screening
___________________________________________________________
Screening guidelines are appropriate as rate of HSIL is very low (0.5%) in young & risk for invasive
carcinoma is minimal
Ma. Cancer Cytopathol. 2013;121:432
Characteristic appearance HPV-status unreliable Cytology: key role in detection
EC CaOn Liquid-Based Prep
Case 10
______________________________________________________
65-year-old
Vaginal Bleeding
SurePath
Granular Background
Diagnosis______________________________________________________
Endometrial Adenocarcinoma
Clinical Presentation of Endometrial Carcinoma
Bleeding
Watery discharge
Increase in size of uterus
Pain

31
Endometrial Adenocarcinoma on Pap______________________________________________________
Sensitivity <50% Specificity <97% +Pap in 25% of asymptomatic patients
+Pap = higher grade, larger, thicker >5mm
Norimatsu. Diagn Cyto. 2013;4:120; Watanabe Cancer Cytopathol 2009;117:254
Liquid-Based Preparation Better
Cytology of Endometrial Adenocarcinoma______________________________________________________
Single cells, tight clusters
Variable nuclear size
Hyperchromatic nuclei
Nucleoli
Polarity, less with increase in grade
Diathesis in 33%
ThinPrep-Sensitivity:73%, Specificity:100% & Positive Predictive Value:100% in endometrial carcinoma
Zhou. Diagn Cytopathol. 2013;41:408
Watery Diathesis inEndometrial Carcinoma
Selvaggi, Diagn Cytopathol 2005;33:162
ThinPrepConventional
“glue-like”
Cytology of Endometrial Carcinoma______________________________________________________
Cytoarchitectural criteria more useful, especially for the endometrial hyp; erplasia & low-grade carcinoma
For atypical glandular cell diagnoses, the Cellient Cell Block has higher rate of endocervical or endometrial carcinoma diagnoses than ThinPrep, 36% vs 8%
Zing. Cancer Cytopathol. 2014;122:8; Nambu. Diagn Cytopathol. 2012;40:701
Papillary Serous Carcinoma
Mixed Mullerian Tumor
Clear CellCarcinomaEndometriod Carcinoma

32
Endocervical Carcinoma Endometrial Carcinoma
3-dimension clusters rounded > cytoplasm watery diathesis
2-dimension clusters columnar < cytoplasm bloody diathesis
7% associated with Actinomyces
TP
Use of IUD reduces risk of endometrial carcinoma Cellular immunity is protective?
Castellsagué. Lancet Oncol. 2011;12:1023
Accurate Diagnosis by“Pattern Recognition”
Lesson
_____________________________________________
Case 11________________________________
26-Year-Old Post-Coital Bleeding
Pap Test, ThinPrep
ThinPrep

33
Hypercellular Single & Clustered Cells
Dirty Necrosis & Malignant Cells “Cigar” Nuclei
Diagnosis:Metastatic Colonic Carcinoma
Metastases in Paps_______________________________
Rare, <1% Rarely a primary event
Usually primary is known Symptom: bleeding
Khalbuss. Cytojournal. 2013;10:17 Hoda. Acta Cytol. 2004;48:586

34
Direct Extension, Usually Rectum
Childs Recurrent colorectal carcinoma detected by routine cervicovaginal pap testing. Low Genit Tract Dis 2005;9:236
From Peritoneum, via Fallopian Tube
Gupta Extrauterine malignancies. Role of pap smearsin diagnosis and management. Acta Cytol 1999;43:806
Metastasis, Distant Sites
Mousavi Isolated cervical metastasis of breast cancer: a case report and literature review. J Low Genit Tract Dis 2007;11:276
Most Common Metastases in Paps_______________________________
Breast Colon
Urinary bladderEndometrium
Ovary
Otsuka. Br J Cancer. 2013;109:603. Hoda. Diagn Cyto. 2005;33:58
Psammoma Bodies_______________________________________________
Spherical bodies, Calcified concentrically
Neoplastic: Papillary carcinoma
Non-neoplastic: Endosalpingiosis
Calcified IUD debris mimics psammoma
Meisels
Gupta. Cytomorphological features of extra-genital metastases in SurePath™ cervical liquid-based cytology: a series of 8 cases. Cytopathology. 2013;24:123
Metastatic Merkel Cell Carcinoma
Hoda , Acta Cytol 2004;48:586
35
Consider Metastatic Carcinoma…_____________________________________
…if cytology of lesional cells does not match that of cervix or endometrium
Gioradano et al Cervical smear in diagnosis of extrauterine malignancy metastatic to the cervix: 3 case reports Diagn Cytopathol 2010;38:41
“In 1951, at the age of 30, Henrietta Lacks, was diagnosed with cervical cancer. Her doctor took a small tissue sample without her consent. A scientist put that sample into a test tube. Although Henrietta died 8 months later, her cells–HeLa Cells—are still alive…”
Rebecca Skloot: The Immortal Life of Henrietta Lacks
“…HeLa Cells helped develop polio vaccine, & treatment for herpes, leukemia, hemophilia & Parkinson's; & led to cloning, in vitro fertilization, & gene mapping.
“Since 2001, 5 Nobel Prizes have been awarded for research involving HeLaCells”
Rebecca Skloot: The Immortal Life of Henrietta Lacks