painless jaundice . . . painful diagnoses: radiologic ...painless jaundice . . . painful diagnoses:...
TRANSCRIPT
David M. DudzinskiGillian Lieberman, MD
Painless Jaundice . . . Painful Diagnoses:
Radiologic Evaluation of Periampullary Malignancies
David M. Dudzinski, Harvard Medical School Year IIIGillian Lieberman, MD
September 2004
2
David M. DudzinskiGillian Lieberman, MD
ED Presentation; BIDMC w/u85MMay 2004, presented to OSH ED s/p fall • Scleral icterus noted. • CT for workup of fall revealed pancreatic mass.
Referred to BIDMC• No abdominal pain or back pain. Jaundice over
past several days = “painless jaundice”– No pruritis, weight loss, or other GI symptoms
• Exam: “palpable, firm mass in the right upper quadrant, compatible with a Courvoisier’s gallbladder”
• Labs: indicative of obstructive jaundice– Bilirubin (total) 18.3 mg/dL (ref. 0-1.5 mg/dL)– Alkaline phosphatase 749 IU/L (ref. 39-117 IU/L)
PATIENT #1: FS
3
David M. DudzinskiGillian Lieberman, MD
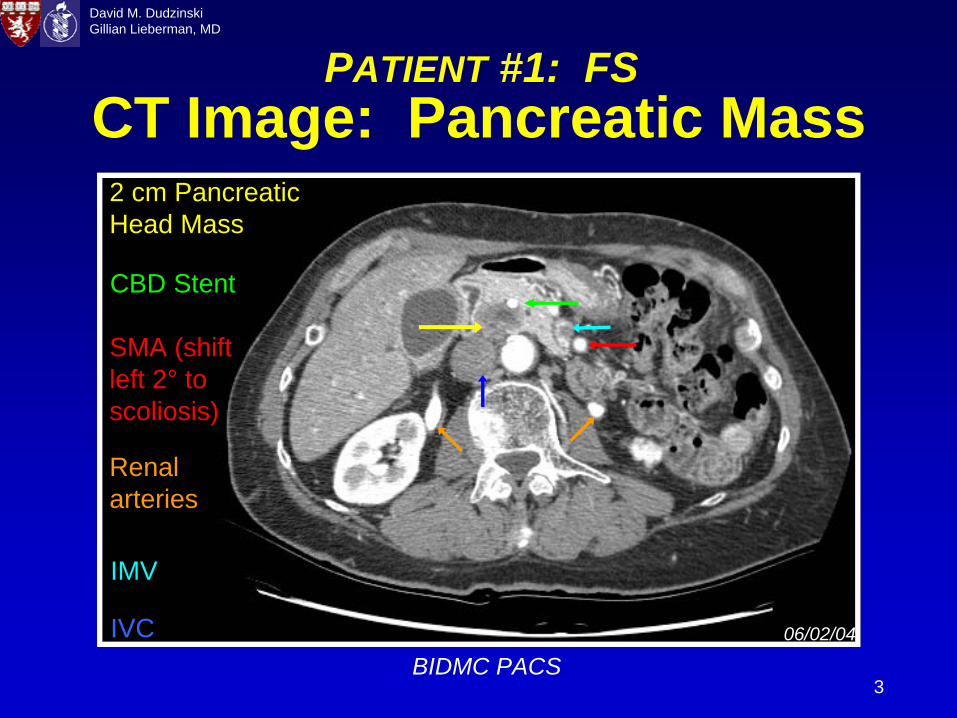
CT Image: Pancreatic Mass
BIDMC PACS
IMV
06/02/04
Renal arteries
2 cm Pancreatic Head Mass
CBD Stent
SMA (shift left 2° to scoliosis)
IVC
PATIENT #1: FS
4
David M. DudzinskiGillian Lieberman, MD
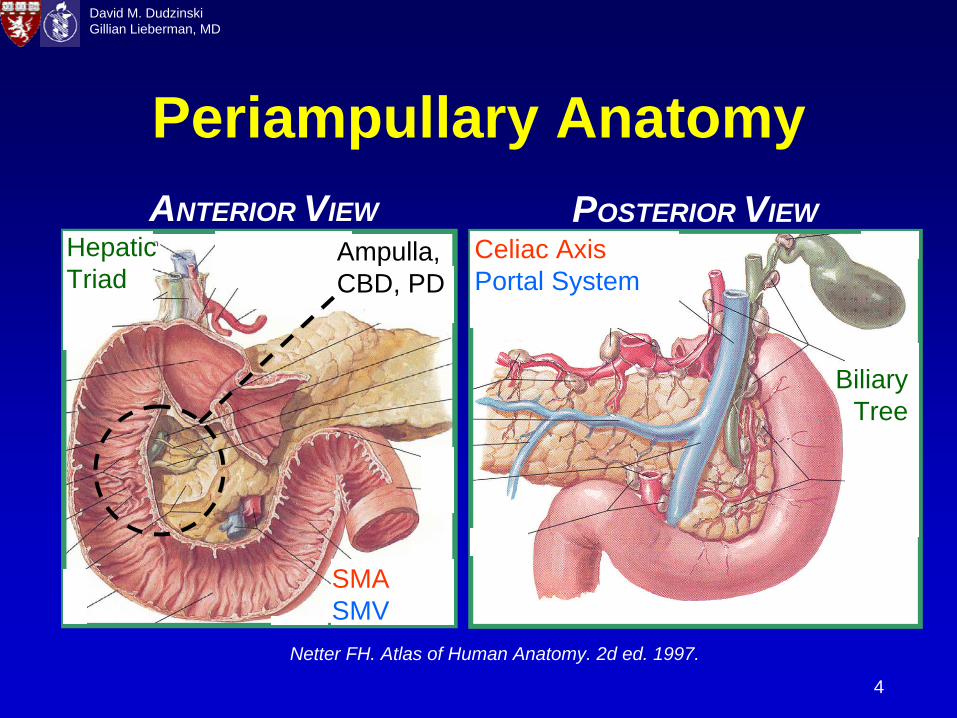
Periampullary Anatomy
Netter FH. Atlas of Human Anatomy. 2d ed. 1997.
ANTERIOR VIEW POSTERIOR VIEW
Biliary Tree
SMA SMV
Celiac Axis Portal System
Hepatic Triad
Ampulla, CBD, PD
5
David M. DudzinskiGillian Lieberman, MD
Periampullary Mass LesionsDifferential diagnoses based on imaging • Malignant neoplasms• Focal pancreatitis• Benign neoplasms• Pancreas pseudocyst, traumatic cyst, necrosis• Abscess• Biloma, Hematoma• Lymphadenopathy• Aneurysm• Duodenal cyst, polyp, diverticulum
Overlap with DDx of obstructive jaundice ?
Reeder MM. Reeder and Felson’s Gamuts in Radiology. 4th ed. 2003.
6
David M. DudzinskiGillian Lieberman, MD
Painless JaundiceSign classically associated with malignant etiologies of extrahepatic or obstructive jaundice• Carcinoma of ampulla of Vater• Extrahepatic cholangiocarcinoma (“CCA”)• Ductal adenocarcinoma of the pancreatic head (“ACA”)
Diagnostic caveat• Painless jaundice in some cases of cholecystitis• Advanced malignancies may often present with pain
Painless jaundice is the most common presentation associated with a resectable and curable malignancy. • Thus, the radiologist can facilitate rapid, lifesaving
diagnosis and surgical intervention.
Kalser MH, et al. Cancer. 1985; 56:397-402.Molodell I, et al. Annals Oncol. 1999; 10:S82-S84.
7
David M. DudzinskiGillian Lieberman, MD
Menu of Radiologic ExamsUS: dilated ducts, r/o cholelithiasis / cholecystitis; not as likely to show tumorCT: masses, local anatomy, metastasesMRI/MRCP: biliary tree anatomyERCP: giving way to MRCP, therapeutic roleFuture Modalities (?)• EUS: (irregularly hypoechoic mass, pancreatic
duct dilatation)• Functional: (PET protocols to detect metastases)
Talamonti MS, Denham W. Radiol. Clin. N. Am. 2002; 40: 1397-410.
8
David M. DudzinskiGillian Lieberman, MD
CT ImagingHelical CT = primary imaging study in suspected periampullary malignancy• Detection: more sensitive than US ≈
90% vs. 75%
CT Findings• Focal mass, mass effects, distort gland contour• Hypoattenuation with IV contrast (hypovascularity)
– “Negative oral contrast”: duodenal-pancreatic interfaces• Smoothly dilated pancreatic duct, abrupt cut-off
– Double duct sign (CBD involvement)• Enlarged gallbladder
No masses, but dilatation ? MRI/MRCPFaria SC, et al. Semin. Roentgenol. 2004; 39: 397-411.
Horton KM, Fishman EK. Radiol. Clin. N. Am. 2002; 40: 1263-72.Nino-Murcia M, et al. Abd. Imaging. 2003; 28: 366-77.
Smith SL, Rajan PS. Clin. Radiol. 2004; 59: 26-38.
9
David M. DudzinskiGillian Lieberman, MD
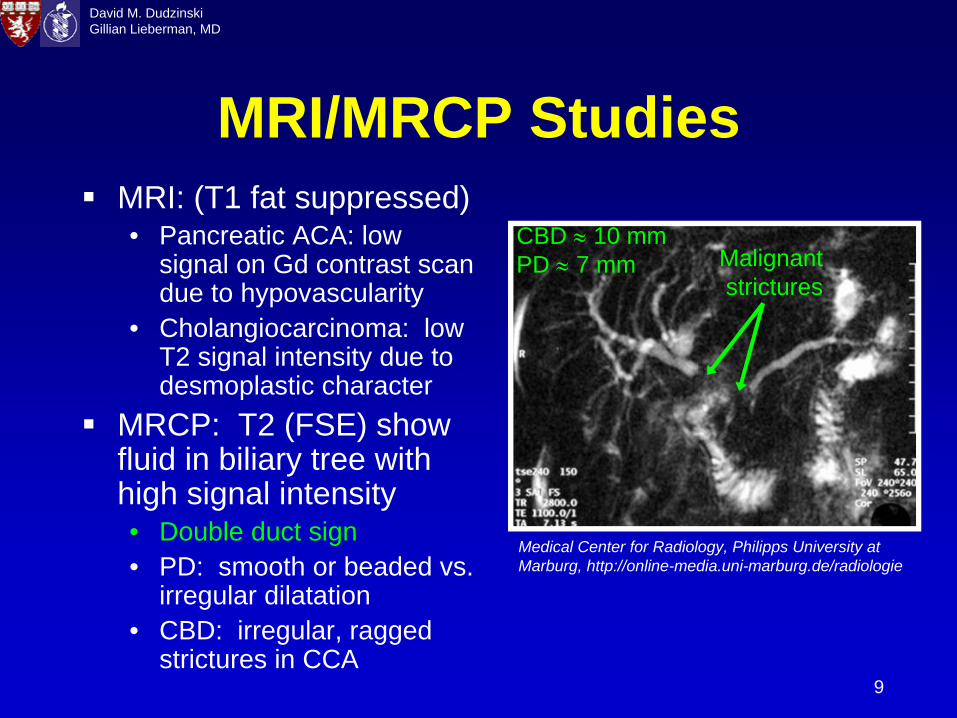
MRI/MRCP StudiesMRI: (T1 fat suppressed) • Pancreatic ACA: low
signal on Gd contrast scan due to hypovascularity
• Cholangiocarcinoma: low T2 signal intensity due to desmoplastic character
MRCP: T2 (FSE) show fluid in biliary tree with high signal intensity• Double duct sign• PD: smooth or beaded vs.
irregular dilatation• CBD: irregular, ragged
strictures in CCA
Medical Center for Radiology, Philipps University at Marburg, http://online-media.uni-marburg.de/radiologie
CBD ≈
10 mm PD ≈
7 mm Malignant strictures
10
David M. DudzinskiGillian Lieberman, MD
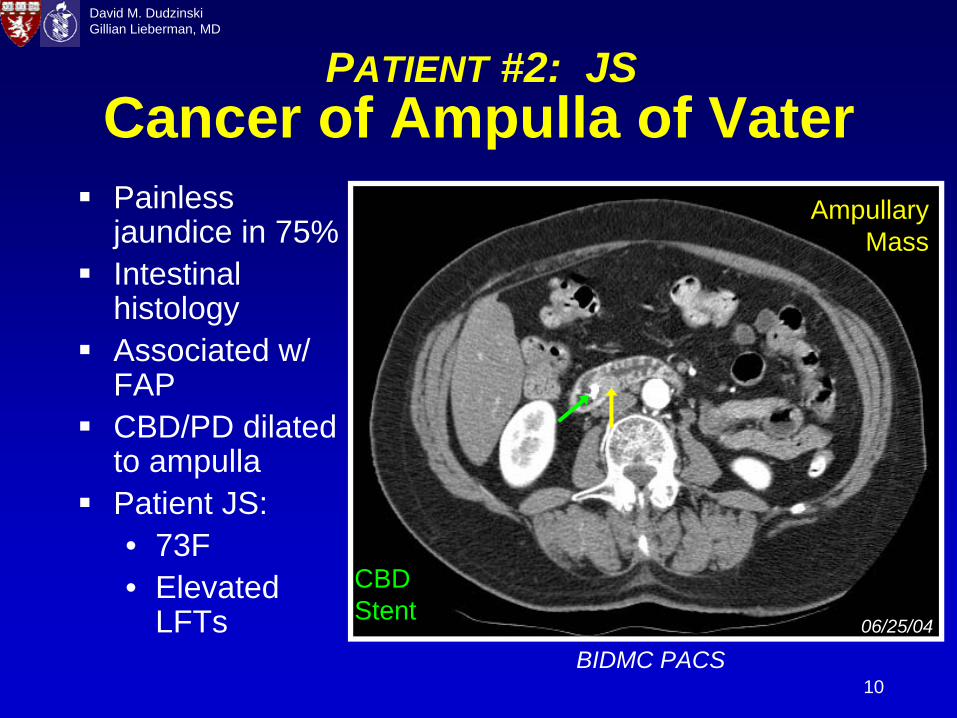
Cancer of Ampulla of VaterPainless jaundice in 75%Intestinal histologyAssociated w/ FAPCBD/PD dilated to ampullaPatient JS:• 73F• Elevated
LFTs
Ampullary Mass
CBD Stent
BIDMC PACS06/25/04
PATIENT #2: JS
11
David M. DudzinskiGillian Lieberman, MD
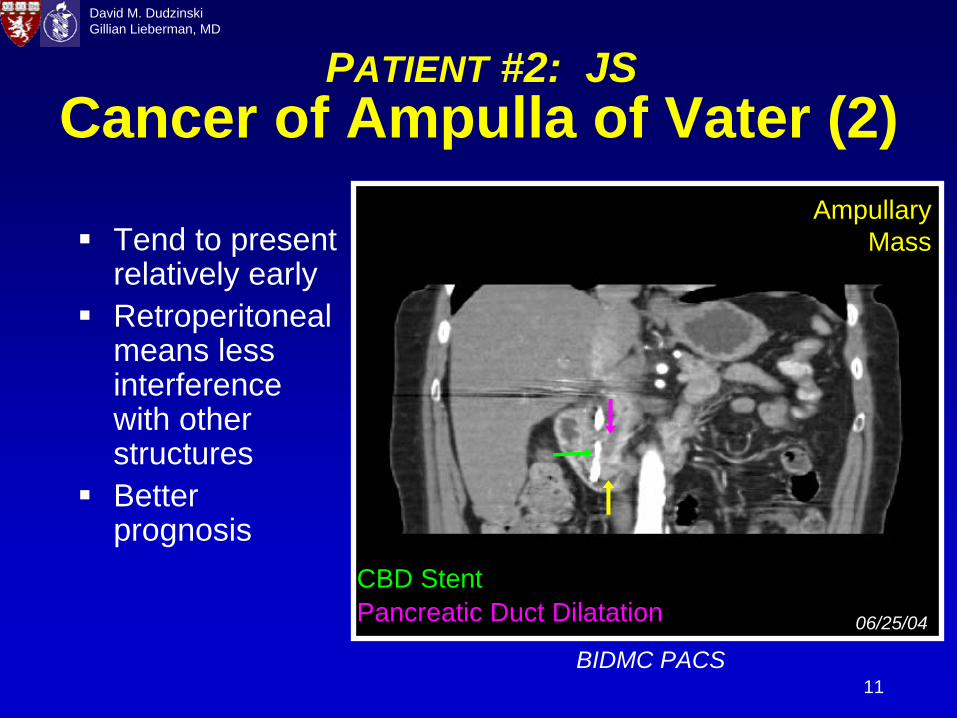
Cancer of Ampulla of Vater (2)
Tend to present relatively earlyRetroperitoneal means less interference with other structuresBetter prognosis
BIDMC PACS
Ampullary Mass
CBD StentPancreatic Duct Dilatation 06/25/04
PATIENT #2: JS
12
David M. DudzinskiGillian Lieberman, MD
Extrahepatic Cholangiocarcinoma
Location in Biliary Tree• Perihilar (Klatskin tumor): 60-70%• Distal CBD: 20-30% • [Intrahepatic ducts 10%]
5 year survival ≈ 5-15%Semin. Liver Dis., July 2004: Clinical picture is “complex”, “not straightforward”, and “continues to defy diagnosis”.• Imaging complements clinical observations
to reach the diagnosis.
13
David M. DudzinskiGillian Lieberman, MD
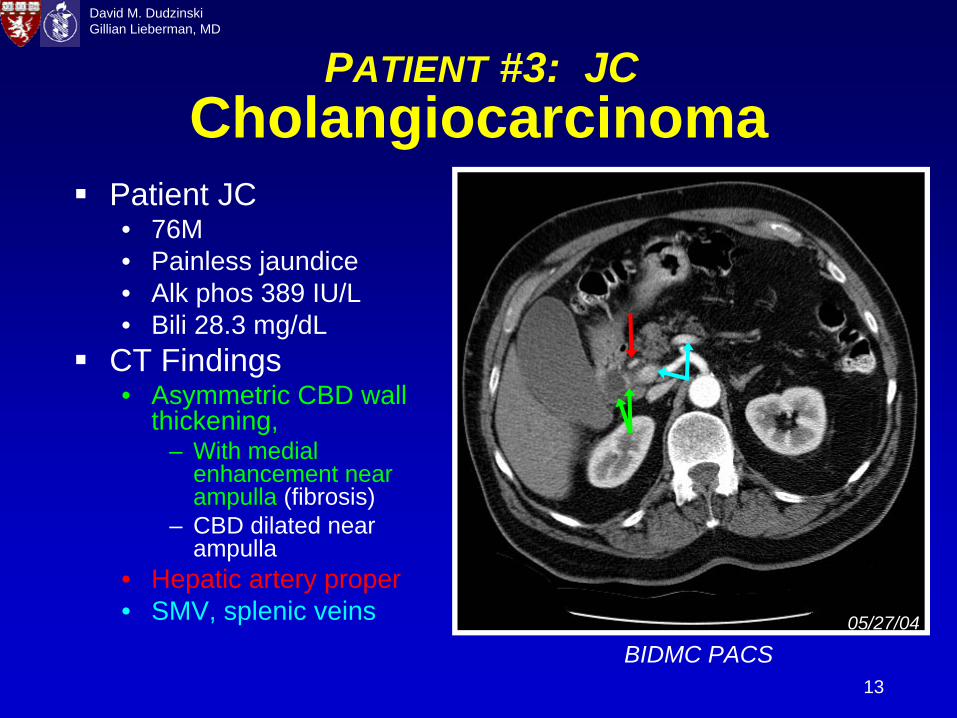
CholangiocarcinomaPatient JC• 76M• Painless jaundice• Alk phos 389 IU/L• Bili 28.3 mg/dL
CT Findings• Asymmetric CBD wall
thickening, – With medial
enhancement near ampulla (fibrosis)
– CBD dilated near ampulla
• Hepatic artery proper• SMV, splenic veins
BIDMC PACS05/27/04
PATIENT #3: JC
14
David M. DudzinskiGillian Lieberman, MD
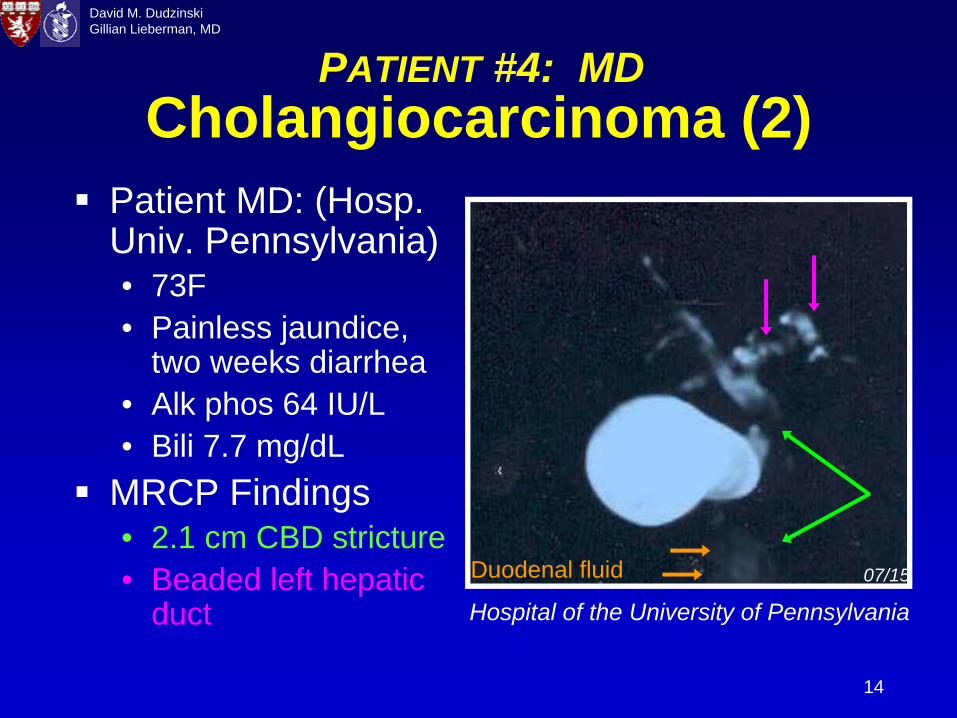
Cholangiocarcinoma (2)Patient MD: (Hosp. Univ. Pennsylvania)• 73F• Painless jaundice,
two weeks diarrhea• Alk phos 64 IU/L • Bili 7.7 mg/dL
MRCP Findings• 2.1 cm CBD stricture• Beaded left hepatic
duct Hospital of the University of Pennsylvania
06/02/0407/15Duodenal fluid
PATIENT #4: MD
15
David M. DudzinskiGillian Lieberman, MD
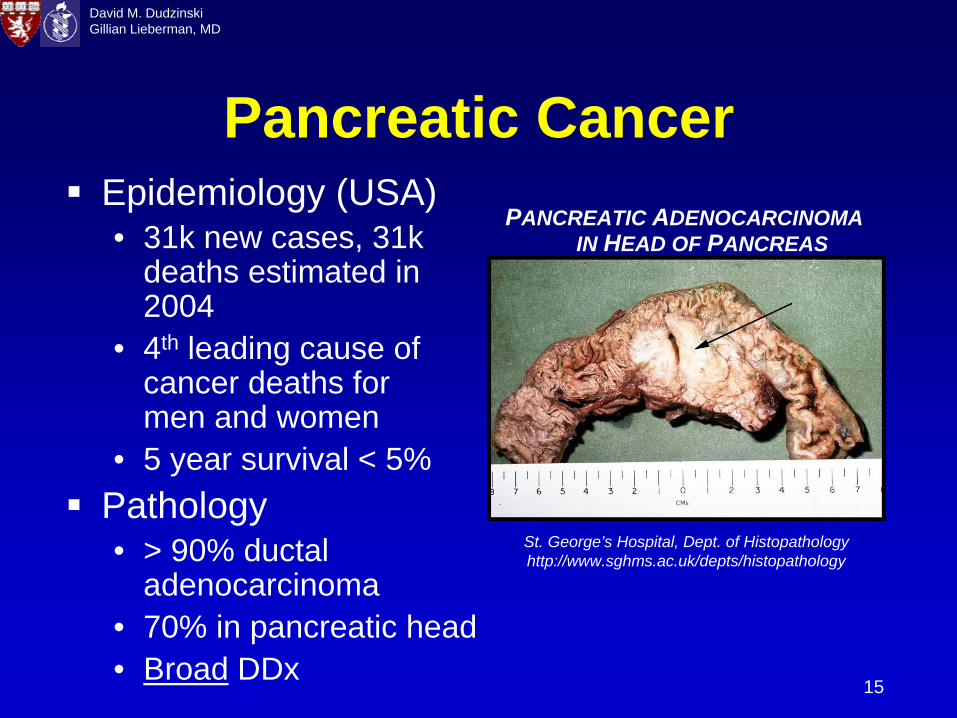
Pancreatic CancerEpidemiology (USA)• 31k new cases, 31k
deaths estimated in 2004
• 4th leading cause of cancer deaths for men and women
• 5 year survival < 5%Pathology• > 90% ductal
adenocarcinoma• 70% in pancreatic head • Broad DDx
St. George’s Hospital, Dept. of Histopathology http://www.sghms.ac.uk/depts/histopathology
PANCREATIC ADENOCARCINOMA IN HEAD OF PANCREAS
16
David M. DudzinskiGillian Lieberman, MD
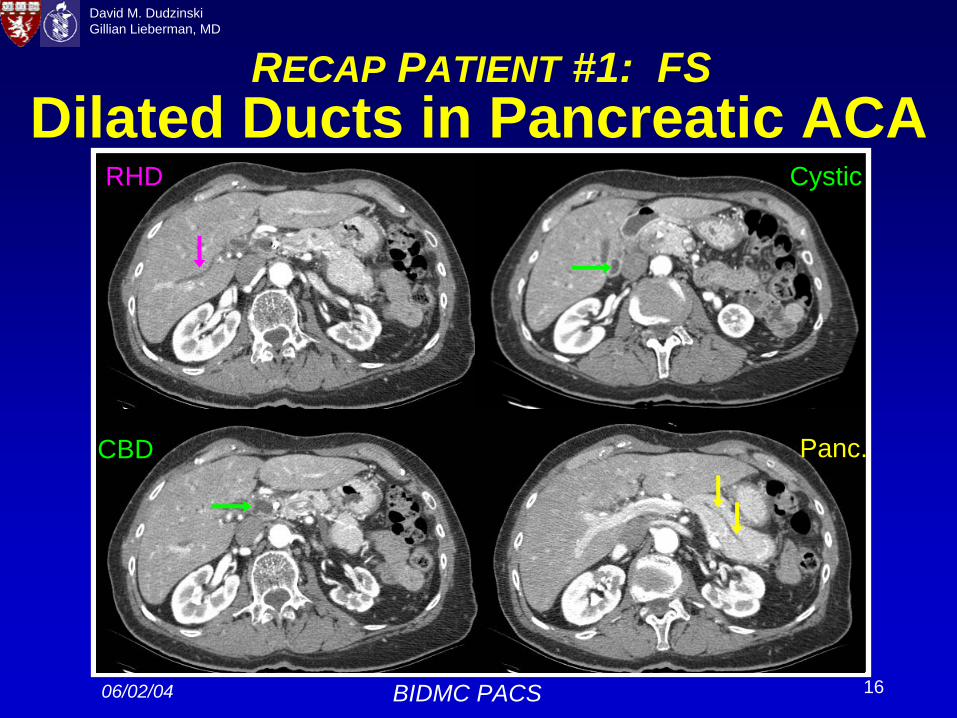
Dilated Ducts in Pancreatic ACA
06/02/04 BIDMC PACS
RHD
CBD Panc.
Cystic
RECAP PATIENT #1: FS
17
David M. DudzinskiGillian Lieberman, MD
Role of Radiology in Treatment“Imaging studies play a critical role in evaluating patients with biliary obstruction, and because resection is the only effective treatment, such studies should be directed at fully assessing the extent of disease.”
Jarnagin WR, Shoup M. Semin. Liver Dis. 2004; 24: 189-99.
18
David M. DudzinskiGillian Lieberman, MD
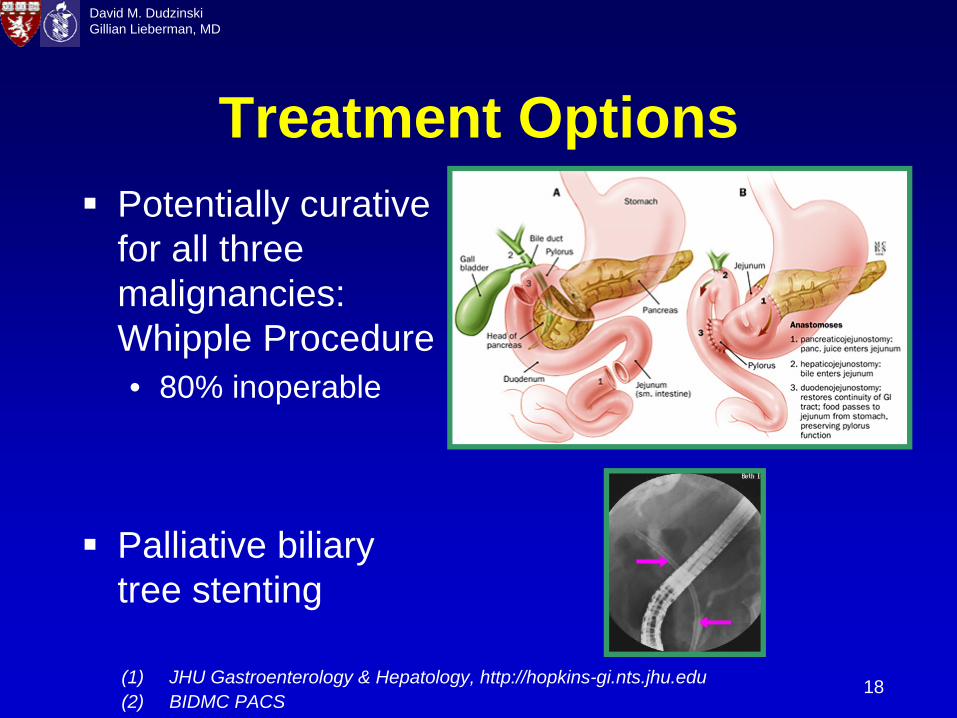
Treatment OptionsPotentially curative for all three malignancies: Whipple Procedure• 80% inoperable
Palliative biliarytree stenting
(1) JHU Gastroenterology & Hepatology, http://hopkins-gi.nts.jhu.edu(2) BIDMC PACS
19
David M. DudzinskiGillian Lieberman, MD
CT Evaluation of ResectabilityPost processing methodologies / CT angio• Multiplanar 3D reconstruction• Curved planar reformation• 3D volume rendering• Maximum intensity projection (MIP)
Evaluate by CT:• Adjacent invasion of tumor• Vascular: hepatic phase acquisition
– Tumor encasement: vessel narrowing, deformation, obliteration, and collaterals
• Neurovascular plexus: check fat planes• Metastases and nodal Involvement
Nino-Murcia M, et al. Abd. Imaging. 2003; 28: 366-77.Prokesch RW, et al. Eur. Radiol. 2003; 13: 2147-54.
20
David M. DudzinskiGillian Lieberman, MD
Staging Pancreatic Cancer for Determining ResectabilityOncologic Staging: TMN• Size (< 2cm), extension, metastases, nodes
CTA Surgical Staging (Raptopoulos, 1997):• 0. Normal• 1. Smooth displacement of vessel, resectable• 2. Flattening or deforming a vessel, ? resectable• 3. Narrowed vein, unresectable (unclear margin)• 4. Occluded vessel, unresectable• (5. Distant Metastases, unresectable)
Identical concept for cholangiocarcinomaRaptopoulos V, et al. AJR 1997; 168:971-977.
Prokesch RW, et al. Eur. Radiol. 2003; 13: 2147-54.
21
David M. DudzinskiGillian Lieberman, MD
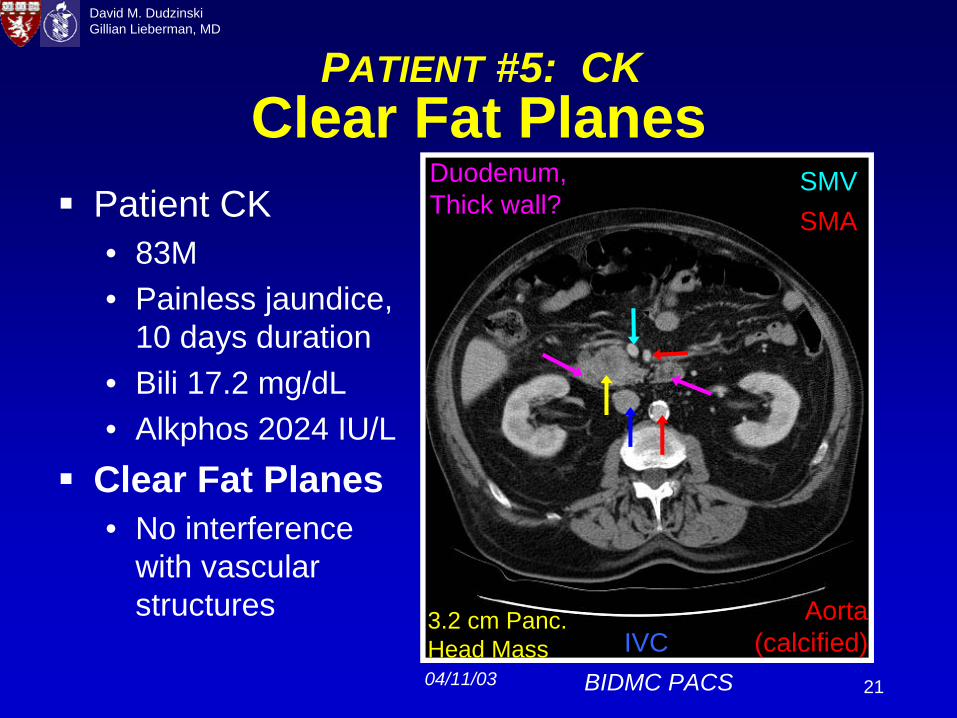
Clear Fat Planes
BIDMC PACS
Patient CK• 83M• Painless jaundice,
10 days duration• Bili 17.2 mg/dL• Alkphos 2024 IU/L
Clear Fat Planes• No interference
with vascular structures Aorta
(calcified)
SMVSMA
04/11/03
IVC3.2 cm Panc. Head Mass
Duodenum, Thick wall?
PATIENT #5: CK
22
David M. DudzinskiGillian Lieberman, MD
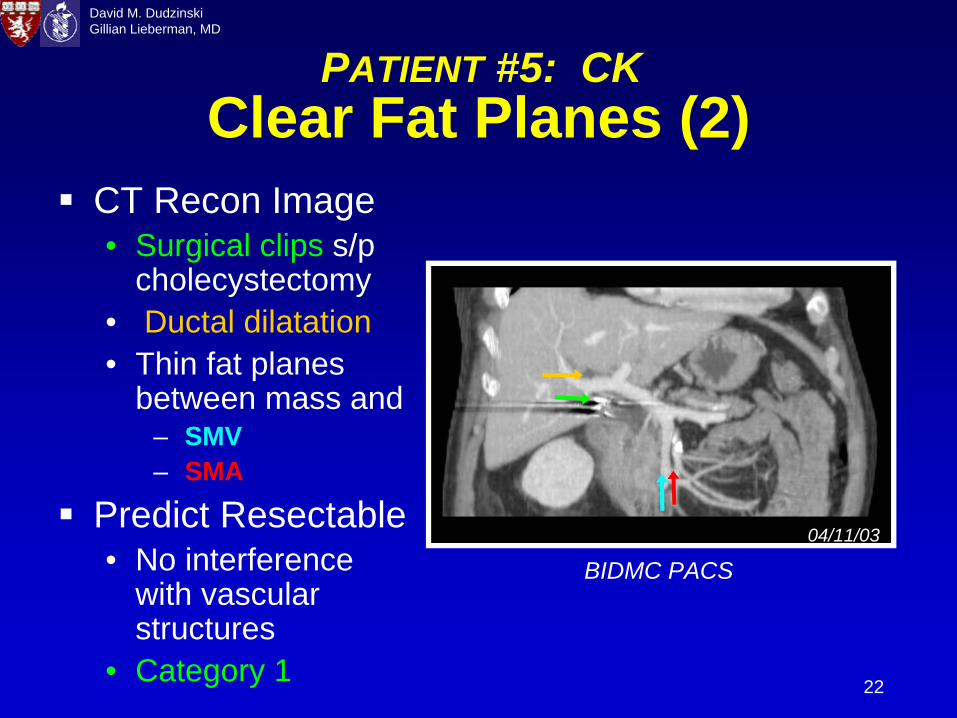
Clear Fat Planes (2)
BIDMC PACS
CT Recon Image• Surgical clips s/p
cholecystectomy• Ductal dilatation• Thin fat planes
between mass and– SMV– SMA
Predict Resectable• No interference
with vascular structures
• Category 1
04/11/03
PATIENT #5: CK
23
David M. DudzinskiGillian Lieberman, MD
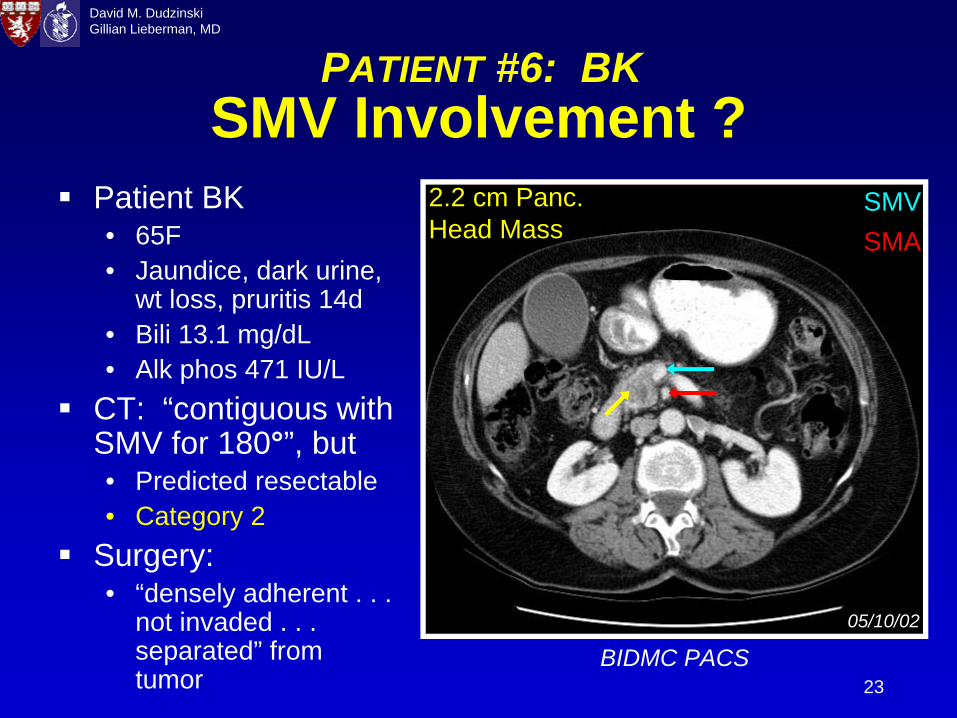
SMV Involvement ?Patient BK• 65F• Jaundice, dark urine,
wt loss, pruritis 14d• Bili 13.1 mg/dL• Alk phos 471 IU/L
CT: “contiguous with SMV for 180°”, but• Predicted resectable• Category 2
Surgery:• “densely adherent . . .
not invaded . . . separated” from tumor
BIDMC PACS
SMVSMA
05/10/02
2.2 cm Panc. Head Mass
PATIENT #6: BK
24
David M. DudzinskiGillian Lieberman, MD
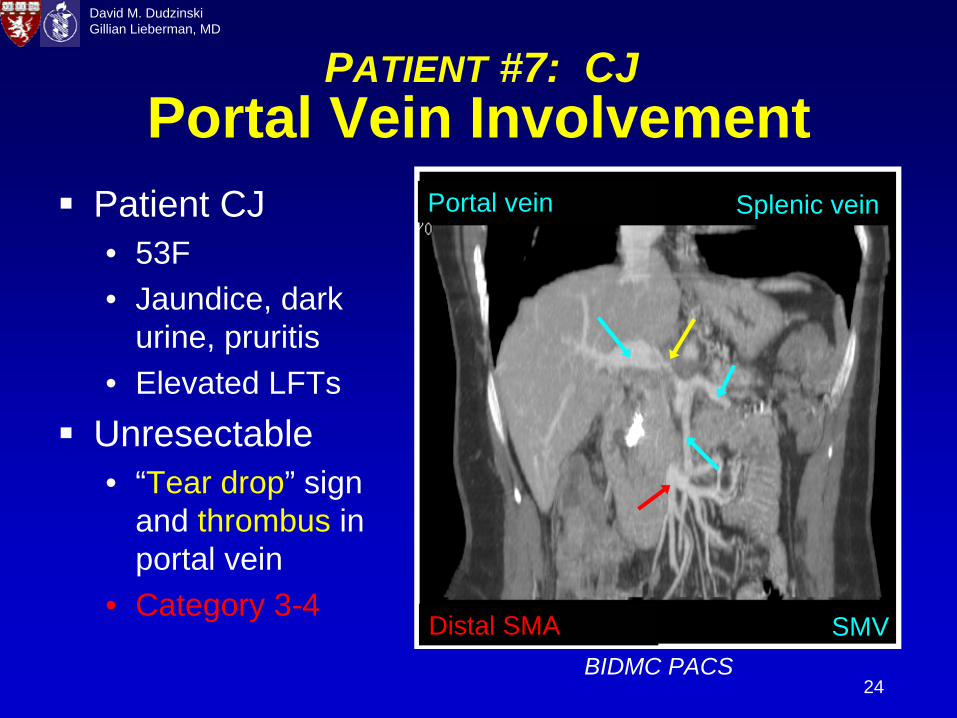
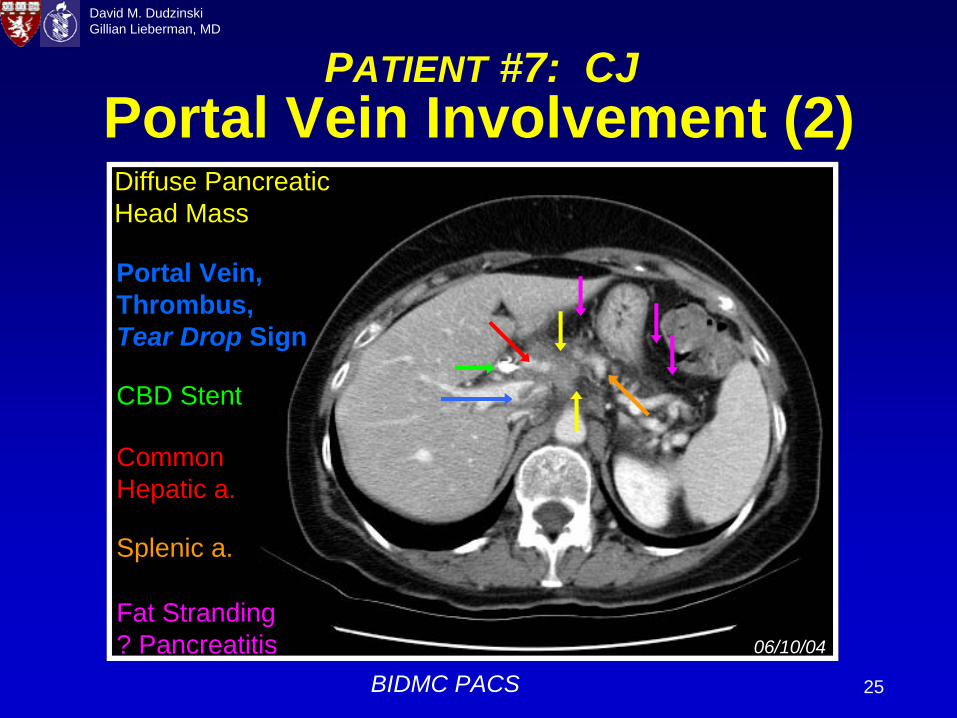
Portal Vein InvolvementPatient CJ• 53F• Jaundice, dark
urine, pruritis• Elevated LFTs
Unresectable• “Tear drop” sign
and thrombus in portal vein
• Category 3-4
BIDMC PACS
Distal SMA SMV
Splenic veinPortal vein
PATIENT #7: CJ
25
David M. DudzinskiGillian Lieberman, MD
Portal Vein Involvement (2)
06/10/04
BIDMC PACS
Common Hepatic a.
Diffuse Pancreatic Head Mass
Portal Vein, Thrombus, Tear Drop Sign
Fat Stranding ? Pancreatitis
Splenic a.
CBD Stent
PATIENT #7: CJ
26
David M. DudzinskiGillian Lieberman, MD
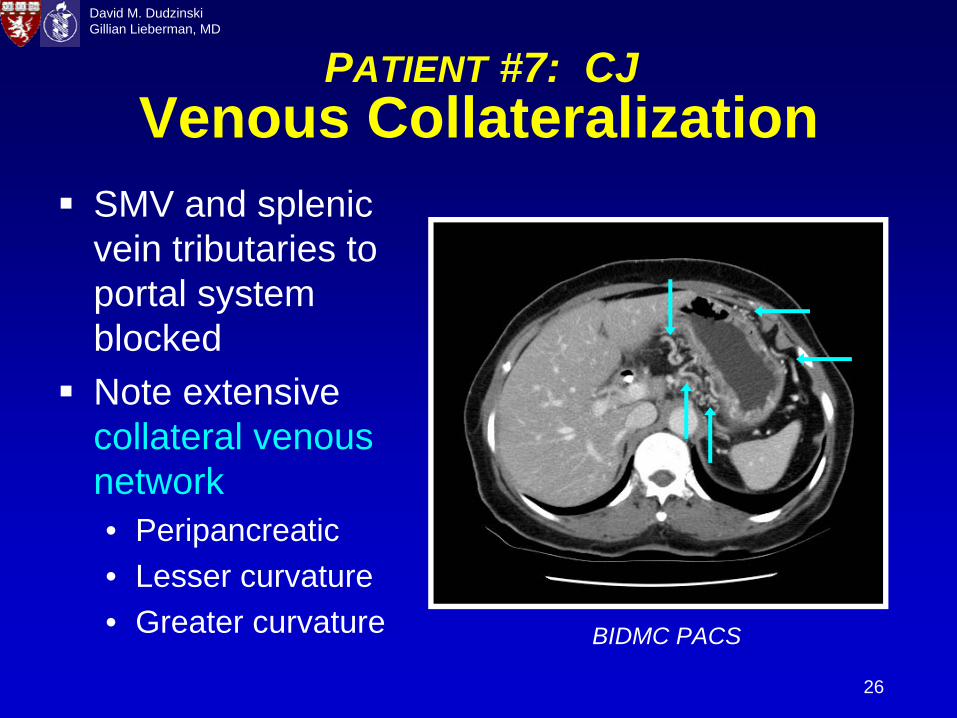
Venous Collateralization
BIDMC PACS
SMV and splenicvein tributaries to portal system blockedNote extensive collateral venous network • Peripancreatic• Lesser curvature• Greater curvature
PATIENT #7: CJ
27
David M. DudzinskiGillian Lieberman, MD
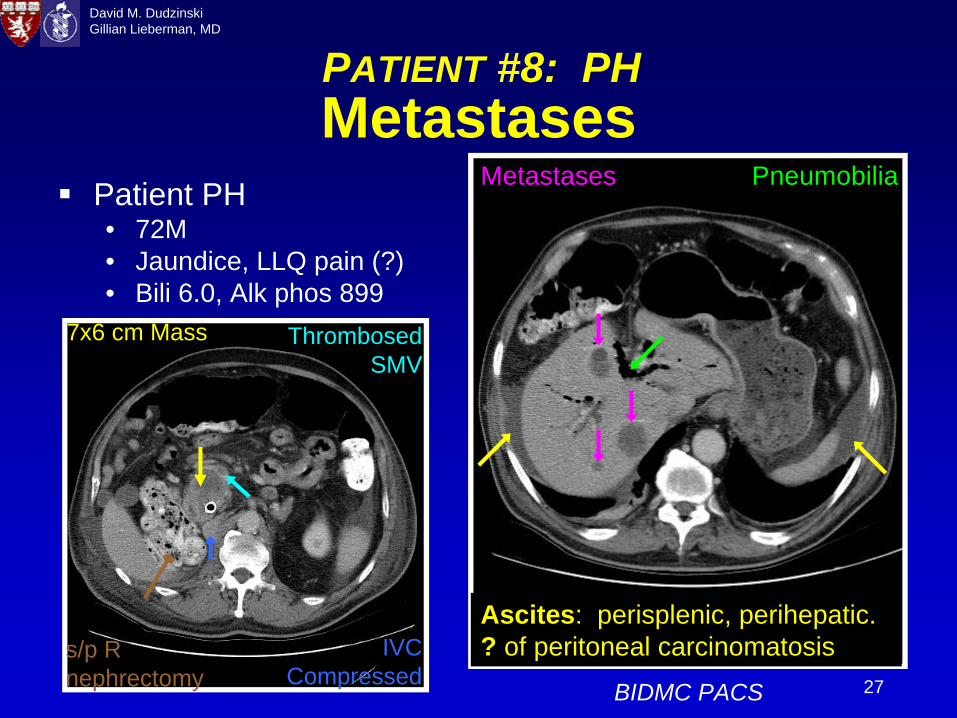
Metastases
BIDMC PACS
Patient PH• 72M• Jaundice, LLQ pain (?)• Bili 6.0, Alk phos 899
Thrombosed SMV
7x6 cm Mass
s/p R nephrectomy
IVC Compressed
Ascites: perisplenic, perihepatic. ? of peritoneal carcinomatosis
Metastases Pneumobilia
PATIENT #8: PH
28
David M. DudzinskiGillian Lieberman, MD
Patients’ ResultsPatient #1, FS: CT resectable, liver metastases at WhipplePatient #2, JS: CT resectable, s/p successful WhipplePatient #3, JC: CT resectable, awaiting Whipple, stent
placed by ERCPPatient #4, MD: MRI/MRCP resectable, s/p successful
WhipplePatient #5, CK: CT resectable, awaiting WhipplePatient #6, BK: CT resectable, s/p Whipple, but XRT/chemo for positive nodes diagnosed post surgeryPatient #7, CJ: CT non-resectable, chemotherapy/XRTPatient #8, PH: CT non-resectable, chemotherapy/stent
29
David M. DudzinskiGillian Lieberman, MD
Limitations: CT ResectabilityNPV of CT non-resectability approximately 100%In contrast, PPV of CT resectability lacking• 53% - 79% CT, 85+% with MDCT, CT angio
Causes of Lower PPV (false positives)• small (< 10mm) liver metastases (Patient #1, FS)• small peritoneal metastases• unknown nodal metastases (Patient #6, BK)• unappreciated portal vein or SMV involvement • unappreciated hepatic artery encasement • tumor spread: porta hepatis or root of mesentery• lack of CT angiography study
Lepanto L, et al. Radiology. 2002; 222:347-52.Raptopoulos V, et al. AJR 1997; 168:971-977.
Vargas R, et al. AJR 2004; 182:419-425.Valls C, et al. AJR 2002; 178: 821-826.
30
David M. DudzinskiGillian Lieberman, MD
SummaryPainless jaundice associated with curable periampullary malignancyRole of radiology in diagnosis• CT, MRI/MRCP methods distinguish
malignancies from other possible etiologiesRole of radiology in surgical planning• Involvement of adjacent vessels, tissues• Future improvements in CT detection and
staging of metastases, nodes
31
David M. DudzinskiGillian Lieberman, MD
ReferencesCay O, Raptopoulos V. Spiral CT for the Diagnosis and staging of pancreatic adenocarcinoma, in Spiral CT of the Abdomen (Terre F, Grossholz M, Becker CD, eds., 2002).Faria SC, Tamm EP, Loyer EM, Szklaruk J, Choi H, Charnsangavej C. Diagnosis and staging of pancreatic tumors. Semin. Roentgenol. 2004; 39: 397-411.Fletcher JG, Wiersema MJ, Farrell MA, et al. Pancreatic malignancy: value of arterial, pancreatic, and hepatic phase imaging with multi-detector row CT. Radiology 2003; 229: 81-90.Fujita N, Noda Y, Kobayashi G, Kimura K, Ito K. Endoscopic approach to early diagnosis of pancreatic cancer. Pancreas. 2004; 28: 279-81Horton KM, Fishman EK. Adenocarcinoma of the pancreas: CT imaging. Radiol. Clin. N. Am. 2002; 40: 1263-72.Kalra MK, Maher MM, Mueller PR, Saini S. State-of-the-art imaging of pancreatic neoplasms. Br. J. Radiol. 2003; 76: 857-65.Kalser MH, Barkin J, MacIntyre JM. Pancreatic cancer. Assessment of prognosis by clinical presentation. Cancer. 1985; 56:397-402.Lowenfels AB, Maisonneuve P. Epidemiology and prevention of pancreatic cancer. Jpn. J. Clin. Oncol. 2004; 34: 238-44.Nino-Murcia M, Jeffrey RB. Multidetector-row CT and volumetric imaging of pancreatic neoplasms. Gastroenterol. Clin. N. Am. 2002; 31: 881-96.Nino-Murcia M, Tamm EP, Charnsangavej C, Jeffrey RB. Multidetector-row helical CT and advanced postprocessing techniques for evaluation of pancreatic neoplasms. Abd. Imaging. 2003; 28: 366-77.Pafioleas MC, Moulakakis KG. Pancreatic cancer today. Hepato-gastroenterology. 2004; 51: 862-8.Prokesch RW, Schima W, Chow LC, Jeffrey RB. Multidetector CT of pancreatic adenocarcinoma: diagnostic advances and therapeutic relevance. Eur. Radiol. 2003; 13: 2147-54.
PANCREATIC CANCER
32
David M. DudzinskiGillian Lieberman, MD
Raptopoulos V, Steer ML, Sheiman RG, et al. The use of helical CT and CT angiography to predict vascular involvement from pancreatic cancer: correlation with findings at surgery. Am. J. Roentgenol. 1997; 168: 971-977. Smith SL, Rajan PS. Imaging of pancreatic adenocarcinoma with emphasis on multidetector CT. Clin. Radiol. 2004; 59: 26-38.Talamonti MS, Denham W. Staging and surgical management of pancreatic and biliary cancer and inflammation. Radiol. Clin. N. Am. 2002; 40: 1397-410.Valls C, Andia E, Sanchez A, et al. Dual-phase helical CT of pancreatic adenocarcinoma: assessment of resectability before surgery. Am. J. Roentgenol. 2002; 178: 821-826.Vargas R, Nino-Murcia M, Trueblood W, Jeffrey RB Jr. MDCT in Pancreatic adenocarcinoma: prediction of vascular invasion and resectability using a multiphasic technique with curved planar reformations. Am. J. Roentgenol. 2004; 182: 419-425.
References (cont.)
Abu-Hamda EM, Baron TH. Endoscopic management of cholangiocarcinoma. Semin. Liver Dis.2004; 24: 165-75.Chari RS, Love RC, Afdhal NH, Anderson C. Clinical manifestation and diagnosis of cholangiocarcinoma. UpToDate. 2004.Jarnagin WR, Shoup M. Surgical management of cholangiocarcinoma. Semin. Liver Dis. 2004; 24: 189-99. Lim JH. Cholangiocarcinoma: recent advances in imaging and intervention. Abd. Imaging. 2004; 29:538-9.Manfredi R, Barbaro B, Masselli G, Vecchioli A, Marano P. Magnetic resonance imaging of cholangiocarcinoma. Semin. Liver Dis. 2004; 24: 155-64.Olnes MJ, Erlich R. A review and update on cholangiocarcinoma. Oncology. 2004; 66: 167-79.
CHOLANGIOCARCINOMA
PANCREATIC CANCER
33
David M. DudzinskiGillian Lieberman, MD
References (cont.)AGA, AGA technical review: Epidemiology, diagnosis, and treatment of pancreatic ductaladenocarcinoma: Parts 1 and 2. UpToDate. 2004.BIDMC PACSChoi H, Loyer EM, Charnsangavej C. Neoplasms of the liver and bile ducts. Semin. Roentgenol.2004; 39: 312-427.Fayad LM, Kowalski T, Mitchell DG. MR cholangiopancreatography: evaluation of common pancreatic diseases. Radiol. Clin. N. Am. 2003; 41: 97-114.Fletcher ND, Wise PE, Sharp KW. Common bile duct papillary adenoma causing obstructive jaundice: case report and review of the literature. Am. Surg. 2004; 70: 448-52.Karnam US, Kruskal JB, Reddy KR. CT of the hepatobiliary tract. UpToDate. 2004.Lepanto L, Arzoumanian Y, Gianfelice D, et al. Helical CT with CT angiography in assessing periampullary neoplasms: identification of vascular invasion. Radiology. 2002; 222:347-52. Memon MA, Shiwani MH, Anwer S. Carcinoma of the ampulla of Vater: results of surgical treatment of a single center. Hepato-gastroenterology. 2004; 51:1275-7.Molodell I, Guarner L, Malageldala JR. Vagaries of clinical presentation of pancreatic and biliarytract cancer. Annals Oncol. 1999; 10:S82-S84.Motohara T, Semelka RC, Bader TR. MR cholangiopancreatography. Radiol. Clin. N. Am. 2003; 41: 89-96.National Cancer Institute. Pancreatic Cancer. http://www.nci.nih.gov/cancertopics/ Netter FH. Atlas of Human Anatomy. 2d ed. 1997.Parmar, MS. Courvoisier’s Law. Can. Med. Assoc. J. 2003; 168: 876.Reeder MM. Reeder and Felson’s Gamuts in Radiology. 4th ed. 2003.Rutstein L, Martin JA, Moser JA. Ampullary Carcinoma. UpToDate. 2004.
GENERAL
34
David M. DudzinskiGillian Lieberman, MD
Acknowledgements
Nicole Nelson, MD Jesse Wei, MDJason Handwerker, MDMichael Goldfinger, MDGillian Lieberman, MDPamela LepkowskiLarry Barbaras, our Webmaster