pain management pharmacology
TRANSCRIPT

Pain Management Pharmacology
Linda Vanni, MSN, RN-BC, ACNS-BC, NP, AP-PMN
Nurse Practitioner, Pain Management
Professional Pain Education & Consulting, LLC
Objectives•Discuss the pharmacologic shift taking place in pain management.
•Describe the pharmacologic agents used in pain management.
•Identify safe/monitoring issued related to pain management therapies.
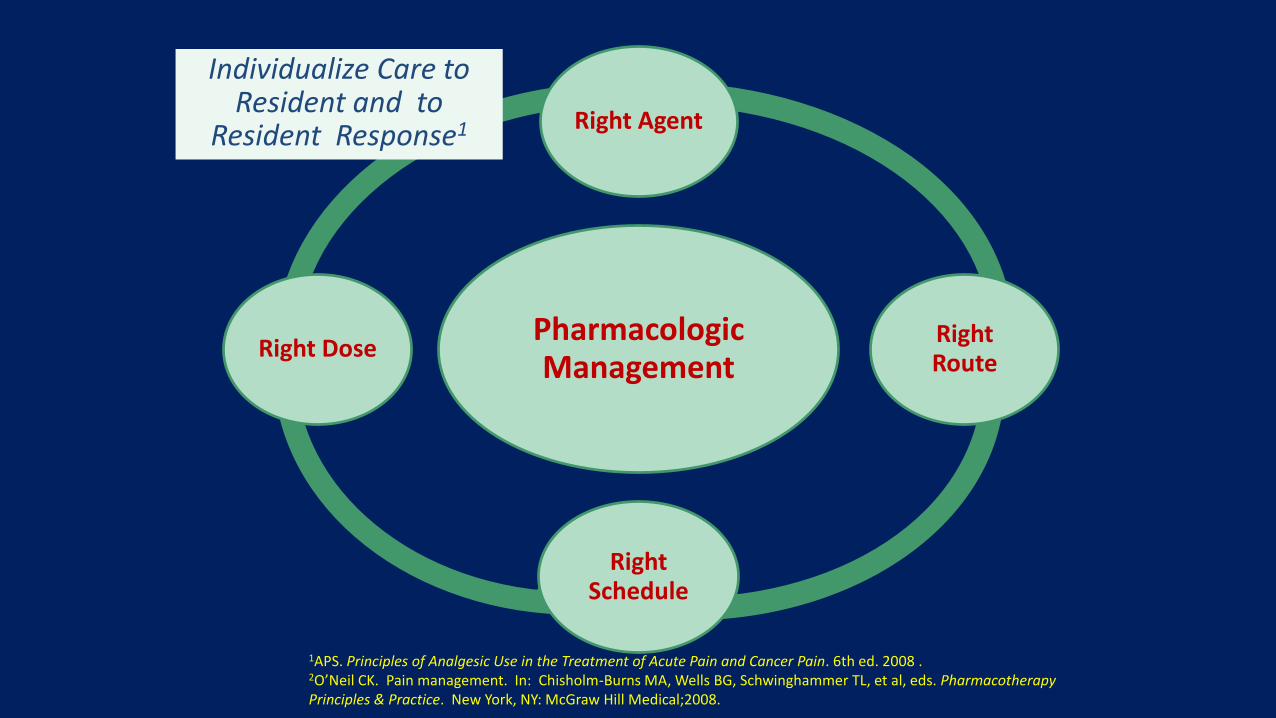
1APS. Principles of Analgesic Use in the Treatment of Acute Pain and Cancer Pain. 6th ed. 2008 .2O’Neil CK. Pain management. In: Chisholm-Burns MA, Wells BG, Schwinghammer TL, et al, eds. Pharmacotherapy Principles & Practice. New York, NY: McGraw Hill Medical;2008.
Pharmacologic Management
Right Agent
Right Route
Right Schedule
Right Dose
Individualize Care to Resident and to
Resident Response1

DistributionTransport of drug from the blood into body
fluids & tissues to sites of action.
Affected by:• Cardiac Output
• Regional permeability of the capillaries
Lipid solubility
• Blood-brain barrier
• CSF distribution, e.g. drug distribution
• Plasma protein binding
• Diffusion through Mater, e.g. Dura, subarachnoid, and Pia.
(Czarnecki & Turner, 2018)
Drug-drug interactions (Core Curriculum)
• Types of interactions– Additive effect- 2 drugs w/ similar action produce summed effect
– Synergistic effect- 2 drugs w/ combined effect greater than either alone
– Potentiation- 1 drug increases the effect of a second drug
– Liver enzyme effect- Cytochrome (CYP)P450 is a family of enzymes that transform drugs into metabolites
• Subject to competition and changes in metabolic speed of action

Pain Process• Definition of pain process:
-The neural mechanisms by which pain is perceived involves a process that has four major steps:
- Transduction
- Transmission
- Perception
- Modulation

Peripheral Excitatory Mediators (Pain)Substance Receptor Mechanism
Substance P
(SP)
NK1 neuronal excitability, edema
Prostaglandin
(PG)
? Sensitize nociceptors, inflammation, edema
Bradykinin B2 (normal)
B1 (inflammation)
Sensitize nociceptors
PG production
Histamine H1 C-fiber activation, edema,
vasodilatation
Serotonin 5-HT3 C-fiber activation, release SP
Norepinephrine
(NE)
1 Sensitize nociceptors
Activate nociceptors

The Shifting Paradigm All about multi-modal
Scheduled acetaminophen
Pain Management always linked to function
Bar coded, smart pumps for PCA and epidural
Opioid-sparing
The future of topicals
Integrative therapies
Always keeping it safe
Anti-abuse opioids being approved by FDA


Multimodal Therapy:
Clinical Advantages
Multimodal therapy
provides a way to achieve
balanced, safer pain
therapy1
➢ Improved quality of
analgesia2,3
➢ Fewer side effects2,3
➢ Better functional status4
Central• Anticonvulsants
• Opioids•2-agonist
(clonidine) • Acetaminophen
Peripheral• Local anesthetics
• Opioids
• Anti-inflammatory agents
• Capsaicin
Ascending
•Local anesthetics
•Anticonvulsants
•Opioids
•NMDA antagonists (ketamine)
•2-agonist (clonidine)
1. Gottschalk A, Smith DS. Am Fam Physician. 2001;63:1979-1984, 1985-1986.
2. Tiippana EM, et al. Anesth Analg. 2007;104:1545-1556.
34. Basse L, et al. Brit J Surg. 2002;89:446-453.
10
Descending• SNRIs, TCAs
• Endogenous systems
American Pain Society, multi-societies input, 2016
Evidence based
107 systematic & 858 primary studies reviews
Grading of evidence & recommendations
32 recommendations
Only 4 supported by high quality evidence, 11 recommendations by low-quality evidence
Panel came to near-unanimous consensus on almost all of its recommendations

Different Types of Pain
Somatic – localized pain in skin, muscle, bone described as aching, stabbing, throbbing
Therapies for somatic pain include NSAIDs (prostaglandin inhibitors), acetaminophen (works centrally), muscle relaxants, ice, and heat
Visceral – non-localized pain in organs or viscera described as gnawing, camping, aching or sharp
Therapies for visceral pain include opioids (occupies opioid receptors), and interventional therapies
Neuropathic – pain caused by nerve damage described as sharp, numbness, burning or shooting
Therapies for neuropathic pain include antidepressants (inhibits norepinephrine and serotonin re-uptake), anticonvulsants (blocks voltage-dependent calcium channels), local anesthetics, and interventional therapies caution: anticonvulsants can cause dizziness, potential for falls. Start low and go slow!
Opioids are not the medication of choice for neuropathic pain
These types of pain can occur individually or in combination
Adjuvants Tricyclic antidepressants
Anticonvulsants
Muscle relaxants
NSAIDs
Local Anesthetics
Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
• Inhibit both COX 1 & 2
• Analgesic, antipyretic, anti-inflammatory
• Initial analgesic effect - 1 hour
• Maximum anti-inflammatory effect - 2 wks
• Uses - rheumatoid arthritis, OA, pain, fever, bursitis, tendonitis
• Adverse Drug Reactions (ADRs) - GI upset, ulceration, bleeding, renal failure, anaphylaxis
• Often individualized responses
Important Facts NSAIDs
NSAIDs
NSAIDs bind to the platelets for the life of the
NSAIDs, i.e. 4-6 hours
ASA
ASA binds to the platelets for
the life of the platelet, i.e. 2 weeks
Black Box Warning
NSAIDs and CV RiskPaauw, D.S., 6/23/2017
US Food and Drug Adm., 7/2015
Longer acting NSAID, bigger risk for HF
Decrease renal excretion of Na+ and water
Short term use risk: increased risk of death and recurrent MI in patients with prior MI
No hx MI: Wen,YC, et al (2017), increased risk for MI-three fold when tx resp. infection, parenteral NSAIDs, seven fold
Risk benefit ratio
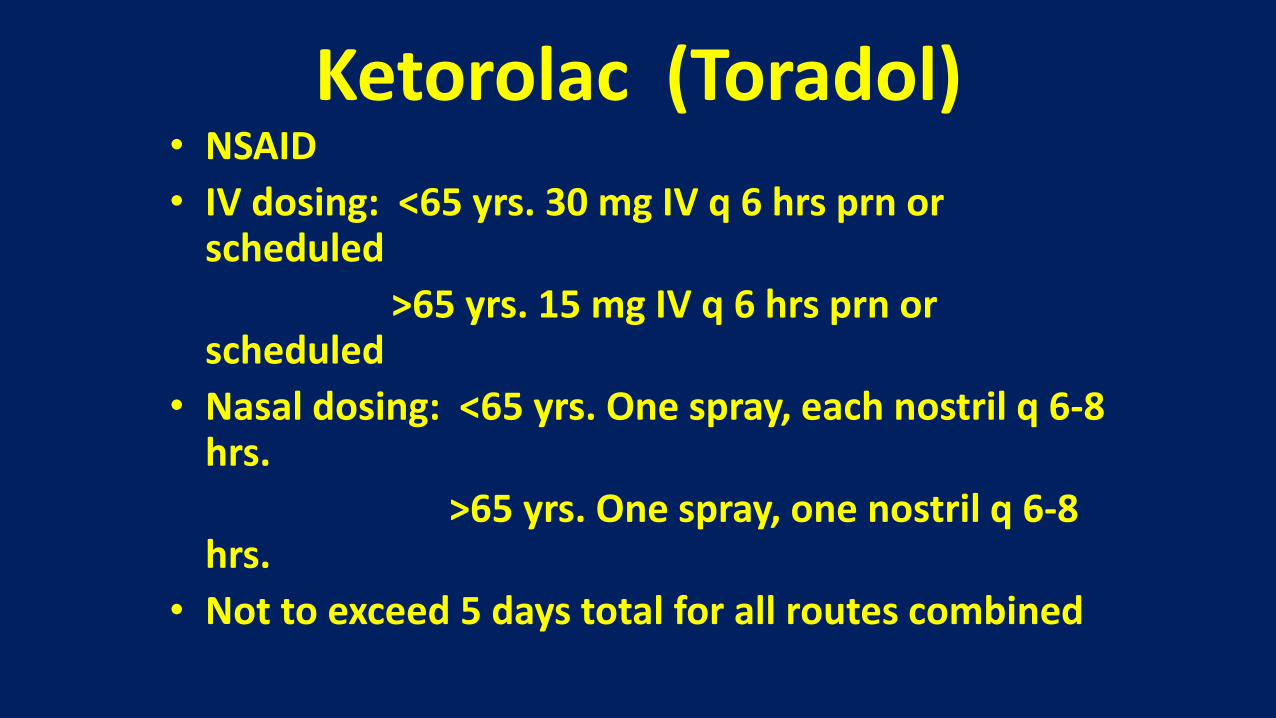
Ketorolac (Toradol)• NSAID
• IV dosing: <65 yrs. 30 mg IV q 6 hrs prn or scheduled
>65 yrs. 15 mg IV q 6 hrs prn or scheduled
• Nasal dosing: <65 yrs. One spray, each nostril q 6-8 hrs.
>65 yrs. One spray, one nostril q 6-8 hrs.
• Not to exceed 5 days total for all routes combined

**Perioperative: ► Induction: per anesthesia protocol ► Ketamine infusion 10µg/kg/min: initiated at induction, discontinued during closing ► Fentanyl intravenous as needed (amount recorded) ► 20mL 1% lidocaine/0.25% bupivacaine with epinephrine injected locally
**Postoperative (PO)—Post Anesthesia Care Unit (PACU) Intervention group: ► Ketorolac 15mg (15mg/mL) intravenous Q6H ► Dilaudid intravenous 0.5–2mg, 10min in between doses. Not to exceed 2mg Control group: ► Saline 1mL intravenous Q6H ► Dilaudid intravenous 0.5– 2mg, 10min in between doses. Not to exceed 2mg PO—floor
Intervention group: On arrival, ketorolac 15mg intravenous every 6 hours from the PACU dose for 48 hours ► Total ketorolac will be <110mg/day for 48 hours► Dilaudid intravenous 0.5–2mg, Q3H PRN—severe pain► Oxycodone/acetaminophen PO 5/325 two tab, Q4H as needed—moderate pain► Robaxin 750mg PO, Q6H as needed► Return to home non-opioid medicationsControl group: On arrival, normal saline 1 mL intravenous every 6 hours from the PACU dose for 48 hours ► Dilaudid intravenous 0.5–2mg push, Q3H PRN—severe pain ► Oxycodone/acetaminophen PO 5/325 2 tab, Q4H asneeded—moderate pain ► Robaxin 750 mg PO, Q6H as needed ► Convert all opioid doses to morphine equivalence ► Return to home non-opioid medications

diclofenac Patch

Local Anesthetics
Blocks conduction of nerve impulses by decreasing or preventing an increase in the permeability of excitable membranes to Na+.
(Catterall & Mackie, 1996)
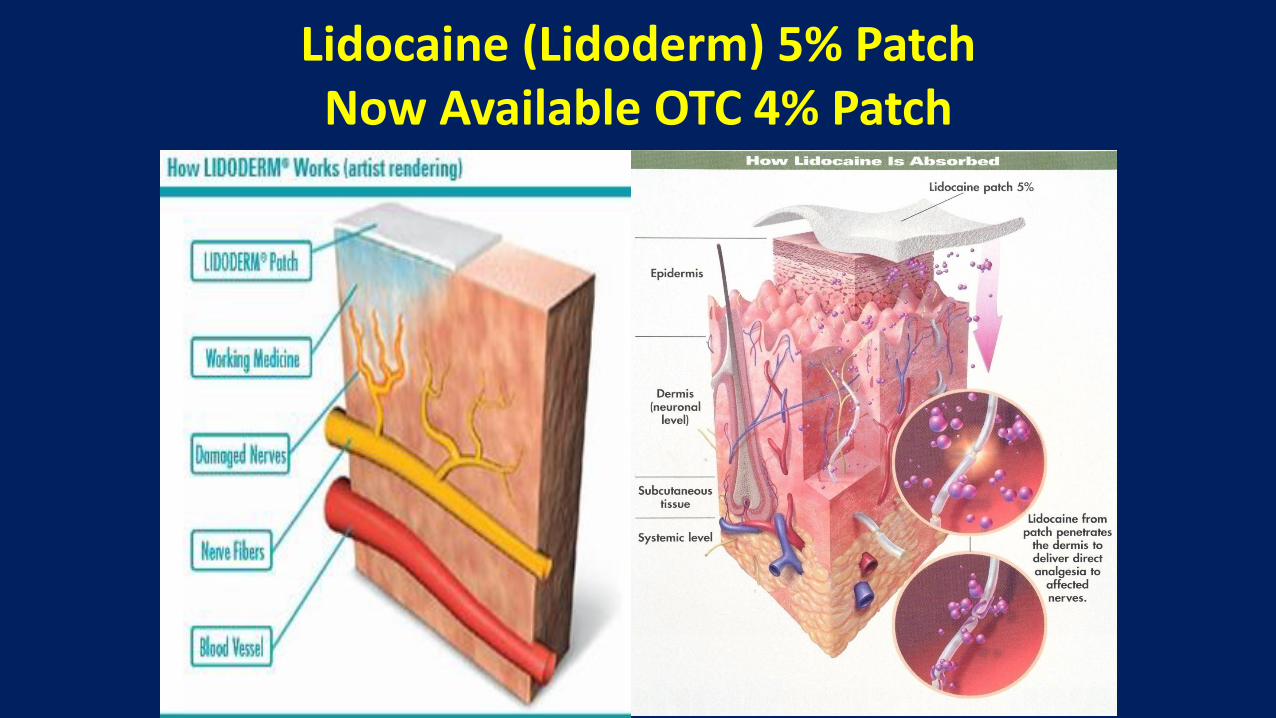
Lidocaine (Lidoderm) 5% PatchNow Available OTC 4% Patch

lidocaine 4% (LMX 4)

Breakdown of cartilage at delivery catheter site
Variability of dose infusion
AcetaminophenReinforces the descending inhibitory serotonergic pain pathways (proposed)
Acts centrally
Pickering, G., et al (2006). Analgesic effect of acetaminophen in humans: First evidence of a central serotonergic mechanism. Clinical Pharmacologic and Therapeutics, 79, 371-378.

Acetaminophen• Analgesic, antipyretic
• Well tolerated
• Used to treat osteoarthritis
• Maximum dose 4000 mg/day, except w/ ETOH
• Inhibits prostaglandin synthetase in the CNS, weak peripheral anti-inflammatory activity, centrally acting
• Risk of hepatotoxicity with higher doses
• Renal failure dosing based on creatinine clearance
• Moderately dialyzable
• Antidote – acetylcysteine (Mucomyst, Acetadote)
• IV acetaminophen – Ofirmev – non-formulary Ascension

Ketamine Use• Ketamine has traditionally been used only as a
dissociative anesthetic for moderate sedation and as part of general anesthesia for surgical procedures
• More recently, a number of studies have detailed the success of ketamine in lower doses as an analgesic given either intravenously or orally
Ketamine Action• Ketamine is an N-methyl-D-aspartate (NMDA)
antagonist that can inhibit induction and maintenance of central sensitization (“wind up”) after painful stimuli– Inhibits binding of glutamate to the NMDA receptor– Mediated via binding to the phencyclidine (PCP) site on
the NMDA receptor– Results in decreased intracellular proexcitatory
transmission of calcium (Ca2+), protein kinase C (PKC) and nitrous oxide (NO)
• Active at norepinephrine, serotonin and muscarinic cholinergic receptors in the descending facilitation of pain
Reference: Pain Physician, 10:493-500, 2007

Summary of ASRA/AAPM Recommendations for Subanesthetic Ketamine in Acute PainSourceConsensus Guidelines on the Use of Intravenous Ketamine Infusions for Acute Pain Management From the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain...Regional Anesthesia and Pain Medicine43(5):456-466, July 2018.

Ketamine administrationNurse administered starting doses for adults:
– Acute pain: 5-10 mg IV push over 3 minutes every 2 hours prn
– Refractory pain: 2.5-5 mg/hr IV infusion
– Wound care: 5-10 mg IV push over 3 minutes, 15 minutes prior to dressing change; or 25-50 mg PO 30 minutes prior to dressing change
– CRPS
Reference: Pain, 82:111-125, 1999
Centrally Acting Muscle Relaxantsbaclofen: activates GABA receptors to reduce the release of
neurotransmitters and amino acids. Acts specifically at the spinal end of the upper motor neurons to cause muscle relaxation.
carisoprodol (Soma, Soma Compound)
chlorzoxazone (Parafon Forte)
cyclobenzaprine (Flexeril)
methocarbamol (Robaxin)
tizanidine (Zanaflex)
metaxalone (Skelaxin) mechanism of action unknown.
orphenadrine (Norflex, Norgesic) reduces skeletal muscle spasms possibly through an atropine-like central action on cerebral motor centers in the medulla.

Tricyclic Antidepressants TCA amitriptyline (Elavil), 10 – 25 mg po hs, usual
effective dose 50-150 mg po hs., metabolized CYP450: 1A2, 2D6 (primary), 3A4 substrate, active metabolites incl. nortriptyline.
nortriptyline (Pamelor, Aventyl HCL),
10 – 25 mg po hs, usual effective dose 50 – 150 mg po hs, metabolized CYP450: 2D6 substrate, active metabolite.
desipramine (Norpramin), 10 – 25 mg po hs, usual effective dose 50 – 150 mg po hs, metabolized CYP450: 2C19, 2D6 (primary) substrate; active metabolite. (McDonald & Portenoy, 2006)

Serotonin Norepinephrine reuptake inhibitors-SNRIs
• Venlafaxine (Effexor), 75 – 225 mg. po daily, no anticholinergic, sedative, or orthostatic hypotension effects, metabolized by CYP2D6 isoenzyme. Blocks both norepinephrine and serotonin reuptake at higher doses ( 100-400 mgs/d)
(Esper & Kuebler, 2008)
• Duloxetine (Cymbalta), 60 mg po, q 12 hrs or daily, metabolized by CYP1A2 and CYP2D6 isoenzymes. (McDonald & Portenoy, 2006)
Second-Generation Anticonvulsants as Adjuvant Analgesics
gabapentin (Neurontin), starting 100 – 300 mg q hs, usual effective 900 – 3600 mg daily, divided, q 8 – 12 hrs.
pregabalin (Lyrica), starting 150 mg daily, usually effective, 150 – 300 mg q 12 hrs.
lamotrigine (Lamictal), starting 25 – 50 mg daily, usually effective, 200 – 400 mg daily.
topiramate (Topamax), starting 25 mg daily, usually effective 100 – 200 mg q 12 hrs., start at hs.
Benzodiazepines alprazolam (Xanax)
0.25-.05 mg po q 6 – 12 hrs., short half life (<12 hrs), multiple drug interactions
lorazepam (Ativan)
0.5 mg po q 6 – 8 hrs.; max 3 mg/day in older adults; medium half life (10-20 hrs), preferred benzo with liver impairment
diazepam (Valium) 2-10 mg po q 6 – 12 hrs., long half life (20-120 hrs), active metabolites
clonazepam (Klonopin) start 0.25 -0.5 mg po q 8 – 12 hrs., half life (18-50 hrs), rapid relief, monitor closely when discontinuing.
(Esper & Kuebler, 2008)
Federal and State Prescribing Requirements for Controlled Substances
• To comply with federal and state laws, a prescription for a controlled substance must be issued:
– For a legitimate medical purpose
– By an individual practitioner
– Acting in the usual course of professional practice (source: Controlled Substances Act 21 USC 829;21 C.F.R. 1306.04a)

Schedule of Controlled Substances
• Established by the DEA
• Based on abuse and dependence liability
• States may have stricter regulations
• Schedule I (C-I) – potential for abuse so high as to be unacceptable
– LSD, heroin
– marijuana, acceptable?
Cannabinoid & Opioid Synergism
• Combination cannabinoid-opioid therapy maybe effective for neuropathic pain
• The two systems may work synergistically in converging brain pathways.
• The cannabinoids have a distinct mechanism of action, targeting ubiquitous cannabinoid (CB) receptors in the central nervous system and periphery
• Opioid analgesics less effective for neuropathic pain

Changing Winds• Are long term opioids safe to use?
• How long is too long?
• CDC, national health risk, prescription abuse
• Are all of years of work to control pain utilizing opioids coming to an end?
• Will there be limits on how much can be prescribed?
• Who can have it?
• What else can we use to control the pain?

Schedule II (C-II) High potential for abuse & dependence
Outpatient Rx must be in writing
Emergency orders may be phoned in; written provided within 72 hours, No refills allowed
codeine (single) dextroamphetamine Fentanyl hydromorphone
meperidine methadone
methylphenidate morphine cocaine
oxycodone pentobarbital
tapentadol hydrocodone comb & ER **Oxymorphone (Opana ER, 6/8/17, request by FDA to manufacturer to withdraw due to abuse potential. 7/7/17 Endo Pharm release stating Opana ER to be taken off market.

Equianalgesic Opioid Conversion (Mg)*
Oral Parenteral Epidural Intrathecal
Morphine 300 100 10 1Hydromorphone
(Dilaudid) 60 20 2 0.2Meperidine
(Demerol) 3,000 1,000 100 10Fentanyl --- 1 0.1 0.01Sufentanil ---- 0.1 0.01 0.001
*Wallace, Mark MD., Yaksh, Tony, L. Ph.D., Long-term Spinal Analgesic Delivery: A Review of the Preclinical and Clinical Literature, Regional Anesthesia and Pain Medicine, Vol 25, No 2 (March-April): pp 120.
Methadone (Dolophine)• Synthetic opioid agonist
• Has been available since 1940s; synthesized during WWII when MSO4 was in short supply
• Structurally unique- unlike morphine and meperidine
• Metabolized in liver; CYP450; 2B6, 2C19, 3A4 (primary), 2C9, 2D6 (minor
substrate)
• May interact differently with mu opioid receptors

Methadone
• Inexpensive
• Accumulates with repeated dosing
– 85% protein bound, caution cachectic patient
– Slowly released up to 10 days after dose increase
– Rule of Thumb, Methadone takes 3-5 days to reach study state at steady dosing. Titrate slowly
• Available in 10 mg tablet or oral solution, use of 40 mg diskette no longer available for pain mgt use
• Patient may be subjected to scrutiny, stigma & misconceptions
• Can be prescribed for pain
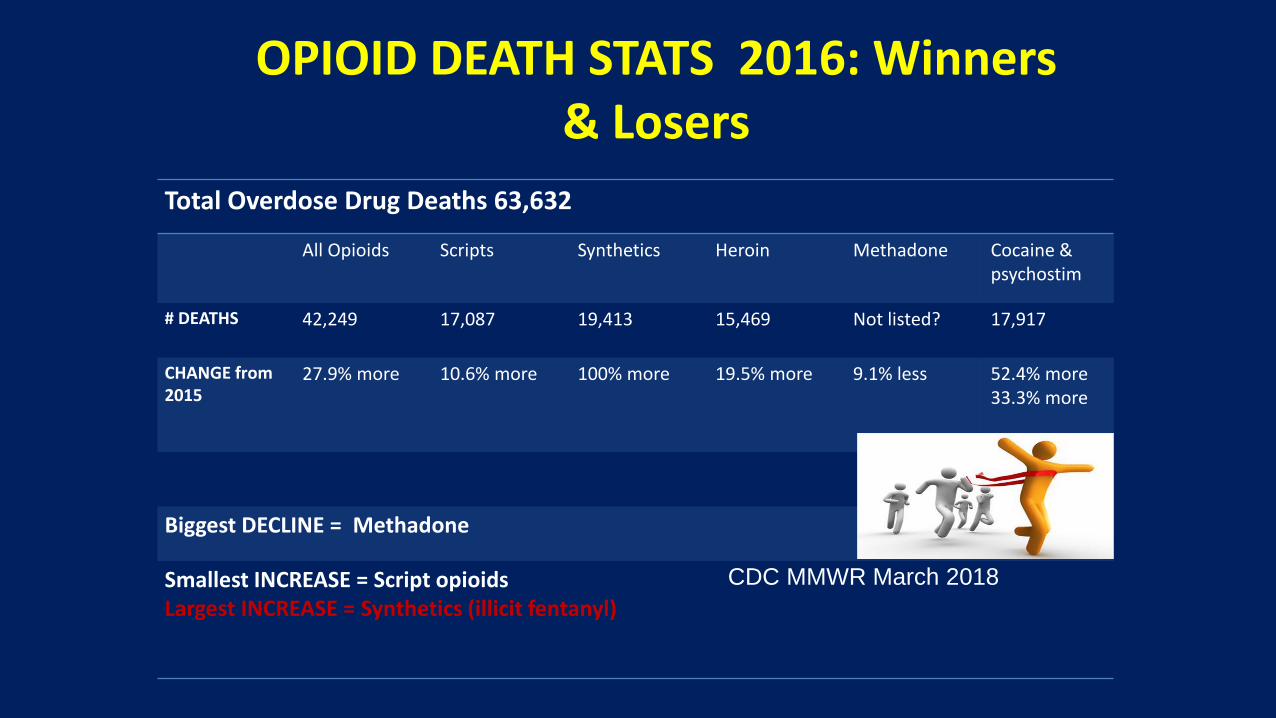
OPIOID DEATH STATS 2016: Winners & Losers
Total Overdose Drug Deaths 63,632
All Opioids Scripts Synthetics Heroin Methadone Cocaine & psychostim
# DEATHS 42,249 17,087 19,413 15,469 Not listed? 17,917
CHANGE from 2015
27.9% more 10.6% more 100% more 19.5% more 9.1% less 52.4% more33.3% more
Biggest DECLINE = Methadone
Smallest INCREASE = Script opioidsLargest INCREASE = Synthetics (illicit fentanyl)
CDC MMWR March 2018

Short Acting Opioids
• morphine – (MSIR, Roxanol)
• hydromorphone – (Dilaudid)
• oxycodone-(OxyIR, Roxicodone, Oxyfast)
Rapid Release Opioid
• fentanyl – (Abstral, Actiq, Fentora, Subsys, Lazanda-nasal) REMS

In 2019, significant issues over chronic opioid use remain
• Stigma
• Using opioids for chronic pain, these medications are not benign, ER
• Multiple guidelines, i.e. CDC
• Impotence
• Expense
• Addiction
• Diversion

Buprenorphine• When patients immediately come into your
service on buprenorphine and have pain– Inadequate analgesia by blocking effect of Mu
opioids
– Opioid overdose: Watch as buprenorphine plasma level declines in presence of concurrent Mu opioids.
– Acute opioid withdrawal syndrome when plasma level declines and there is inadequate dosing of Mu opioids

Buprenorphine• When patients are anticipated to enter your
services on buprenorphine and will have pain, i.e. surgery
– Discontinue buprenorphine 48 hours before painful elective procedures???
– Then administer usual Mu opioids and nonopioids as indicated for pain relief ???

Buprenorphine• Pain Medicine 2018; 0: 1–4 doi: 10.1093/pm/pny019
• Patients Maintained on Buprenorphine for Opioid Use Disorder Should Continue Buprenorphine Through the Perioperative Period
• Anna LEMBKE, MD,*,† Einar OTTESTAD, MD† AND Cliff SCHMIESING, MD† Departments of *Psychiatry and Behavioral Sciences and †Anesthesiology, Perioperative and Pain Medicine, Stanford University School of Medicine, Stanford, California, USA


Buprenorphine• For elective procedures with anticipated mild
to moderate pain
– Use low dose buprenorphine oral tablets or transdermal patches, titrated upward for increased analgesia
– Continue low doses without interference with additional Mu opioid analgesia.
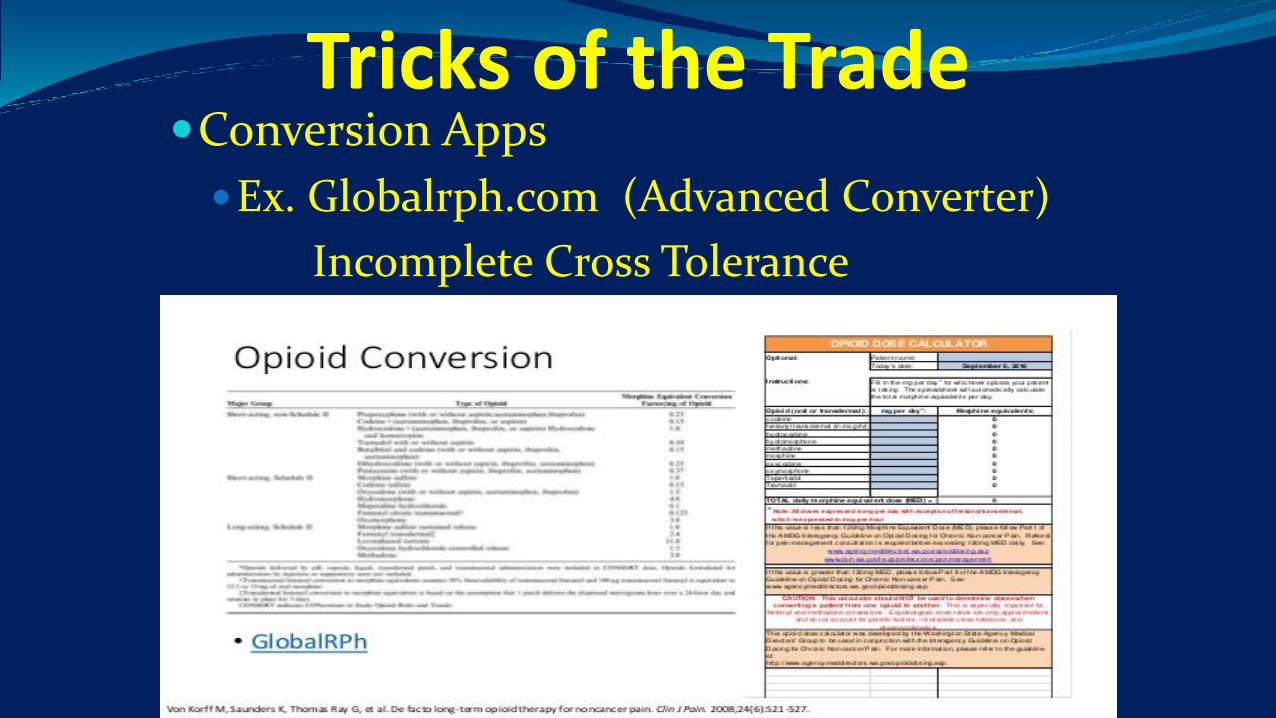
Tricks of the TradeConversion Apps
Ex. Globalrph.com (Advanced Converter)
Incomplete Cross Tolerance

Tricks of the Trade, continued Make your multi-modal medications scheduled
Helps with TJC, better pain relief, more tolerable
Always link pain management to function
Make sure you are using the correct medication for the correct type of pain
Don’t forget those topicals
Use integrative therapies, especially ice in the post-op populations
Keep expectations realistic
Is pre-emptive analgesia ?????
Little things help a lot, i.e. caffeine, blankets
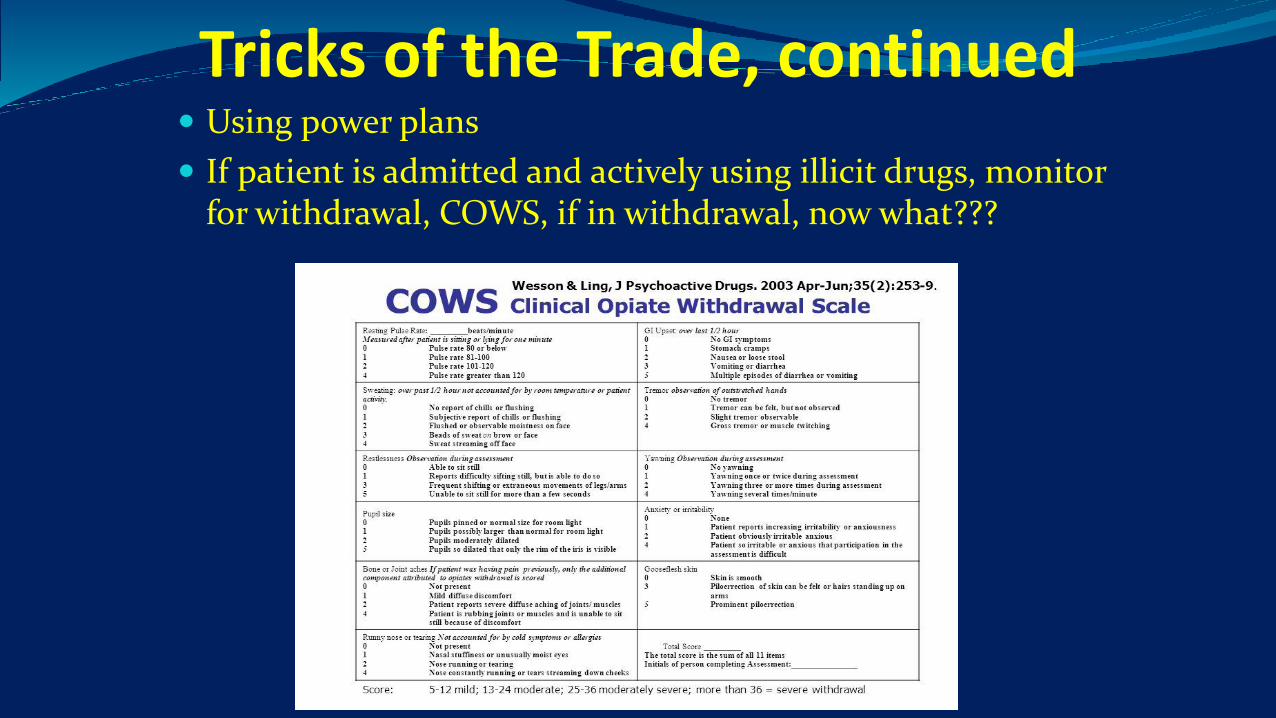
Tricks of the Trade, continued Using power plans
If patient is admitted and actively using illicit drugs, monitor for withdrawal, COWS, if in withdrawal, now what???

Tricks of the Trade, continued Make sure the chronic pain medications that the patient was
taking at home are restarted on admission Suboxone issue Methadone issue, ekg Watch those labs
What about the patient with acute pain arriving in the ED and “demanding” IVP whatever? Now what??
How about the patient wanting IVP Benadryl, at the closest port and pushed as fast as possible???? Oh my! (Remember the routes)
All medications brought in from home should be taken back home immediately
If applicable, discuss medical marijuana when admitted i.e. cannabis oil
Tricks of the Trade, continued Who is going to write the controlled substances on
discharge?
Exit strategy
Scripts for 3 days or 7 days? Check that PDMP
What about the period between medication running out and first post-op visit? PCP? All about communication! Is this our concern, once the patient leaves the hospital????? Absolutely-----30 day readmit.
How long before dependence occurs?
Patient’s/families view of tolerance vs. addiction

Let’s talk Sedation RASS – scale created, reliable and valid for
measurement of purposeful induced sedation.
Aldrete (I & II) – utilized in recovery room areas for measurement of recovering from anesthesia.
CPOT – utilized for patient unable to give self report of pain.
Pasero Opioid Sedation Scale (POSS) – reliable and valid for use in patients receiving opioid therapy for pain.
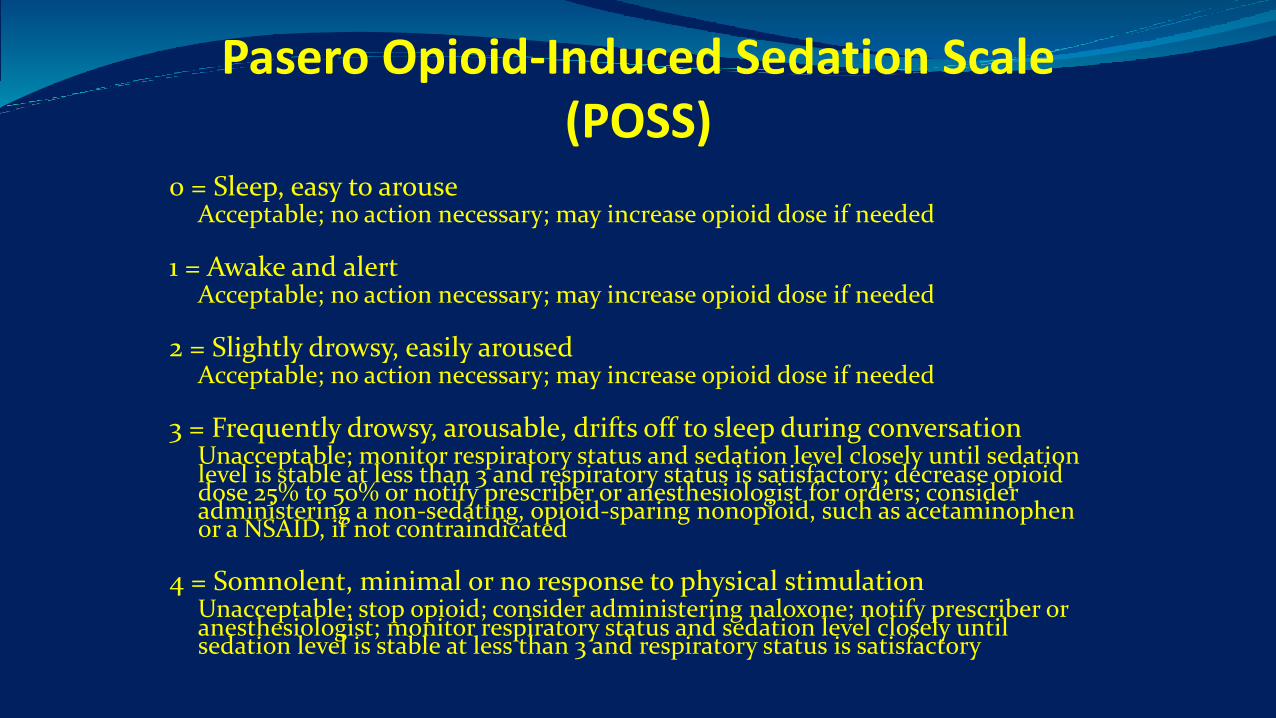
Pasero Opioid-Induced Sedation Scale (POSS)
0 = Sleep, easy to arouseAcceptable; no action necessary; may increase opioid dose if needed
1 = Awake and alertAcceptable; no action necessary; may increase opioid dose if needed
2 = Slightly drowsy, easily arousedAcceptable; no action necessary; may increase opioid dose if needed
3 = Frequently drowsy, arousable, drifts off to sleep during conversationUnacceptable; monitor respiratory status and sedation level closely until sedation level is stable at less than 3 and respiratory status is satisfactory; decrease opioid dose 25% to 50% or notify prescriber or anesthesiologist for orders; consider administering a non-sedating, opioid-sparing nonopioid, such as acetaminophen or a NSAID, if not contraindicated
4 = Somnolent, minimal or no response to physical stimulationUnacceptable; stop opioid; consider administering naloxone; notify prescriber or anesthesiologist; monitor respiratory status and sedation level closely until sedation level is stable at less than 3 and respiratory status is satisfactory

Reversal Agents
Naloxone (pure opioid antagonist)
Extremely short half life, 1.07-1.53h, normally longer than opioid being reversed. In the inpatient hospital
setting (excludes ER), intravenous route, an ampule of naloxone (0.4mg/ml is diluted with 9 mls of saline
for a final concentration of 0.04mg/ml). Initial dose of 2-3 mls administered and then titrated for effect to
reverse opioid sedation. Caution: Because of short life of naloxone, opioid half life is longer and
additional doses of naloxone maybe required. Patient must be continually monitored.
Flumazenil (benzodiazepine receptor antagonist)
Reversal agent for benzodiazepines, binds to benzodiazepine receptors, enhances GABA effects.
Intravenous route, 1 mg. q 2-3 minutes < 60 yo, max 2.5 mg/dose. >60 yo max dose 1.5 mg/dose.
epocrates, athenahealth service (2018)

50% of Beta Blockers work the first time 2
Current Practice is Trial and Error
2 http://publications.nigms.nih.gov/findings/mar10/rightfit.asp, 3 Science Daily; Dec 15, 2011. 4 AAPM 25th Annual Meeting – Methadone. 5 Personalized Medicine (2005) 2(4), 325-337
60% of Depressed patients do not respond fully to the first prescribed Medication 3
There is a 20 fold difference in the dosages of warfarin required to achieve therapeutic effect while the plasma concentrations vary 30-50
fold among individuals receiving the same dose. 5
Genomic testing can help identify people with genetic variations so that doctors can make more informed prescribing decisions, reducing the risk of adverse events
and increasing the likelihood of treatment success.

Genetic PolymorphismUGT 1A1; involved in the glucuronidation of morphine, buprenorphine, and
nalorphine.UGT 1A3/1A4; glucuronidation of TCA.UGT 2B7; glucuronidation of benzodiazepines.• Genetic polymorphism: population distribution for inheriting liver enzyme
activity controlled by a single gene locus. CYP 2C19 approx. 18% Japanese and African Americans, 3-5% of whites, poor
metabolizers with higher plasma conc. of drug substrates. Ex. Diazepam, imipramine, and phenytoin.
CYP2D6 7-10% whites, 1-4% African Americans inherit autosomal recessive allele on chromosome 22 results in poor metabolism with higher plasma conc., prolonged half lives. Ex. Codeine-cannot convert codeine to morphine, paroxetine, venlafaxine, fluoxetine, desipramine, imipramine, nortriptyline and oxycodone.
(Core, 2002), (Cleary & Hogan, 2007)***FDA Drug Safety Communications8/2012 Reviewing the safety of codeine administered post-
tonsillectomy/adenoidectomy. 2/20/13 Black box warningIssued. Deaths occurred in children ultra-rapid metabolizers with sleep apnea.
Avoidance of Codeine & tramadol inspecific populations
FDA Drug Safety Communication, Med Watch Alert, 4/20/17
Risk of subset of individuals that could be “ultra- rapid metabolizers” resulting in increased maternal serum levels and transferred to infant via breast milk (CYP2D6)
Preferred agents for breast feeding mothers, morphine, hydromorphone, & butorphanol
New contraindication against use in pts < 18 yo post-tonsillectomy or adenoidectomy will be added to tramadol labels, already present on Codeine

Patient Education Set pre-operative realistic expectations regarding pain by using scripting:
“Your pain control is very important to us. However, we also need to keep you safe.”
“It is normal to have pain after surgery.”
“It is our responsibility to keep your pain under control to allow you to do the things you need to do to get better and go home.”
“It is your responsibility to keep us informed about your pain, any side effects you experience, and if you are able to do the things you need to do to get better.”
Communicate with patients about a realistic pain management goal for elective procedures
Pain control is important, set goals, inform patients about risk benefit ratio and side effects when dosing medications
Be a patient advocate, the safety of the patient is the first priority
Restart patient’s pain medications from home on admission
Education of patients is an important part of pain control



Subcutaneous Methylnaltrexone
New Drug Application filed 5/30/07, approved in 2008
For treatment of opioid-induced constipation in patients receiving palliative care
Peripherally acting mu-opioid receptor antagonist
Without interfering with pain relief
Single use, pre-filled syringes introduced 2010
Phase III, oral formulation development for chronic, non-cancer pain patients
Patents and applications expirations ranging from 2017-2031