pain and addiction - secured.societyhq.com
TRANSCRIPT
Pain and Addiction
09/03/2021
CSAM Review Course in Addiction Medicine
Julio Meza, MD
Assistant Clinical Health Sciences Professor
Addiction Medicine Fellowship Program Director
Department of Family Medicine
UCLA David Geffen School of Medicine

CONFLICT OF INTEREST DISCLOSURE
I Julio Meza, MD have nothing to disclose, and I will not be discussing “off label” use of drugs or devices in this presentation.

Objectives
■ Discuss chronic pain, opioid prescribing and risk mitigation for opioid use disorder
■ Learn how to identify and manage the chronic pain patient with opioid use disorder
■ Identify pharmacological and non-pharmacological methods of treating chronic pain
■ Discuss special topics in pain and addiction
■ Review pain and addiction in special populations
Chronic Pain
• >116 million Americans have chronic pain (30-40%)
• Total costs $560-635 billion/year
• Higher than costs combined of cancer, CV disease, and diabetes
• About 21-29% of persons receiving chronic opioids show signs of misuse
• Between 8-12% develop OUD
• About 4-6% of people abusing prescription opioids transition to heroin
• 80% of heroin users started out with Rx opioids

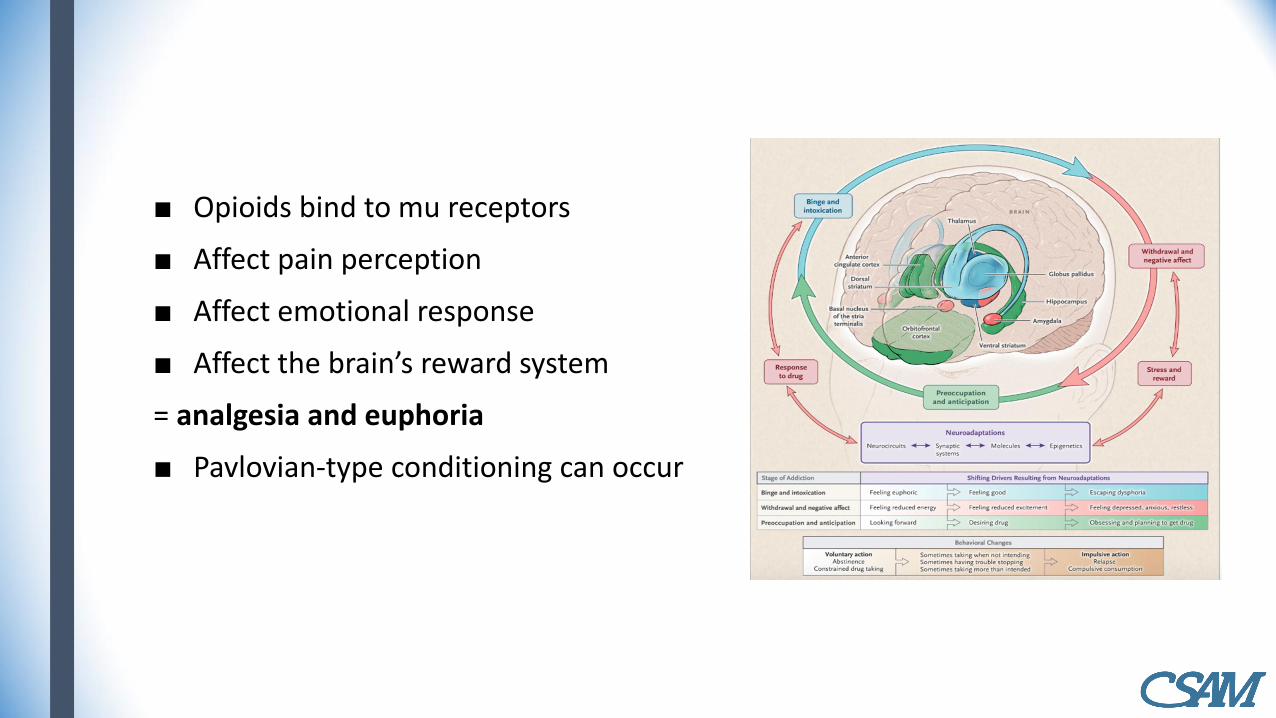
■ Opioids bind to mu receptors
■ Affect pain perception
■ Affect emotional response
■ Affect the brain’s reward system
= analgesia and euphoria
■ Pavlovian-type conditioning can occur
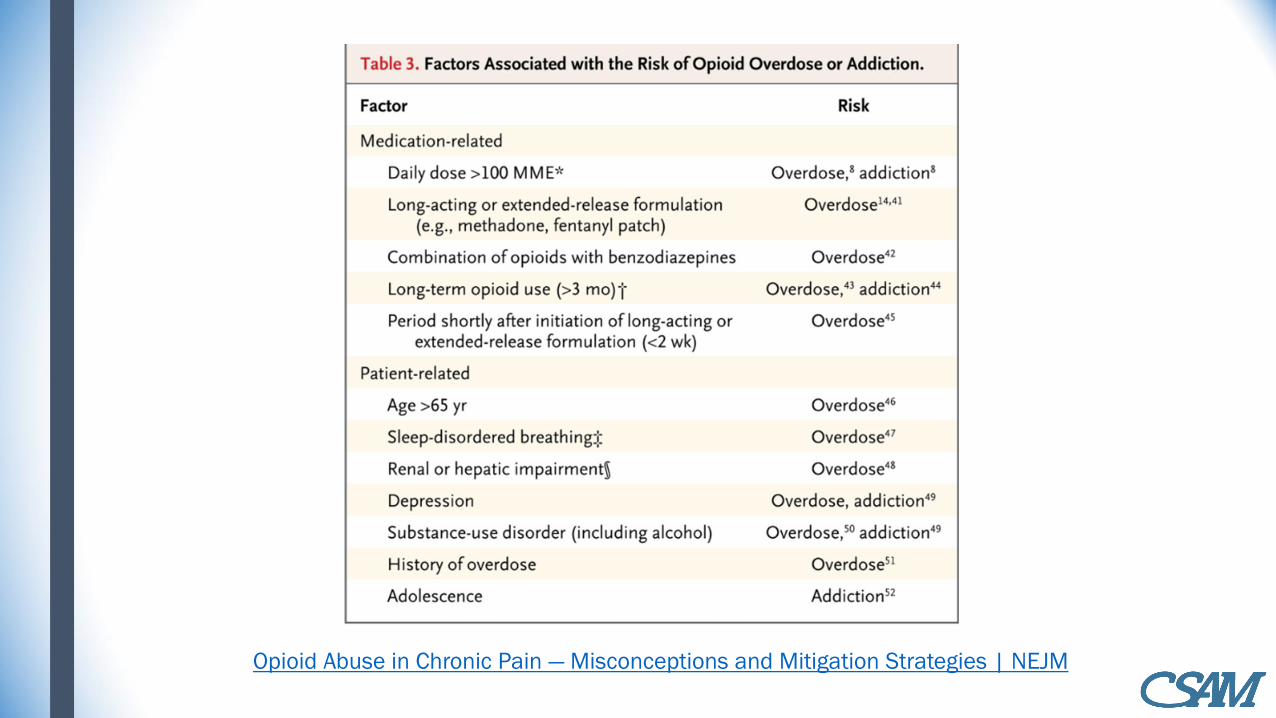
Opioid Abuse in Chronic Pain — Misconceptions and Mitigation Strategies | NEJM

Chronic pain dilemma
■ The “Opioid epidemic” is a big concern right now
■ Many patients have chronic pain but not addiction
■ Chronic opioids may be appropriate for patients with NCP but still have risks– Guidelines exist to help with utilization
■ Patients with both pain and addiction need aggressive treatment of both
■ Addiction, opioids, trauma (emotional pain) and mental illness can complicate chronic pain

Non-Opioid Recommended medications for Chronic Pain Indication Practice Guidelines
Chronic Pain Anticonvulsants (specially sodium channel blockers, membrane stabilizing agents and
ad2 calcium channel antagonists) are recommended for chronic pain.
SNRI and TCA’s
There is lack of evidence on Muscle relaxants but ASA and ASRA agree that might be
used.
Capsaicin and Lidocaine can be used for neuropathic pain
Intrathecal Ziconotide might be recommended
Low back Pain Tizanidine has the best evidence of the muscle relaxants
TCA’s are the only antidepressants with evidence
Gabapentin can provide short term improvement of radiculopathy
Fibromyalgia Amitriptyline, Fluoxetine, Duloxetine and Milnacipram are recommended
Gabapentin and Pramipexole are also recommended
Cyclobenzaprine can be used at night to sleep
Diabetic
Neuropathy
Pregabalin has the most consistent efficiency data
Other anticonvulsants recommended are gabapentin and Valproic acid
Antidepressants recommended include Fluoxetine, amitriptyline, and duloxetine.
Neuropathic pain TCA’s, SNRI’s, gabapentin, pregabalin and topical lidocaine.
Gabapentin and Valproic acid

Muscle relaxants
CDC Guideline for Prescribing Opioids for Chronic Pain
■ Effectiveness of nonpharmacologic and nonopioid pharmacologic treatments, including studies of any duration.
■ Benefits and harms of opioid.
■ Clinician and patient values and preferences related to opioids and medication risks, benefits, and use.
■ Resource allocation including costs and economic efficiency of opioid therapy and risk mitigation strategies.

Recommendations
The recommendations are grouped into three areas for consideration:
■ Determining when to initiate or continue opioids for chronic pain.
■ Opioid selection, dosage, duration, follow-up, and discontinuation.
■ Assessing risk and addressing harms of opioid use.

Tools available to assess risk

Other tools available STORM

Urine drug screen
Informed Consent and Pain Contracts
■ Opioid contracts, or patient-provider agreements (PPAs)
■ The Federation of State Medical Boards and several state departments of health have recommended the use of PPAs as part of their model policies.
■ The drawbacks of opioid PPAs include a lack consistency and clarity in their use of terms, including abuse, misuse, and addiction.
■ In addition, limited evidence is available to support the efficacy of PPAs in preventing opioid misuse, abuse, or diversion.
■ Furthermore, there is concern that PPAs may undermine the prescriber-patient relationship and create an atmosphere of mistrust. When PPAs first became commonly used in clinical practice, most were written in ways that protected prescribers more than patients

Informed Consent
■ Informed consent is a patient-centered approach to educating patients, which promotes the safe prescribing and use of opioids. During the informed consent process, patients should be briefed on the anticipated benefits and risks of using opioids to treat pain, as well as precautions that will be implemented to keep patients safe. The US Department of Veterans Affairs implemented this approach in 2014.
■ When bringing up the topic of PPAs, it is helpful to present this information in an open and honest way. For example, a prescriber might say, “Here are some things that I need you to do to keep you as safe as possible when taking these medications. In exchange for your agreement to do these things, I’m also going to agree to do some things.”

Methadone for chronic pain
■ Patients prescribed methadone for opioid use disorder should receive pain management in the same way as other patients.
■ Splitting the daily methadone dose across 3–4 doses per day can maximize the analgesic properties of this medication
■ Analgesic effects typically last for 6–8 hours.
■ The dose of additional full agonist opioid analgesic prescribed is anticipated to be higher than the typical dose necessary to achieve adequate analgesia in opioid-naive individuals

Buprenorphine for pain
■ The analgesic effects of buprenorphine last for approximately 6–8 hours
■ Increasing the daily dose of buprenorphine by 20–25% and splitting it into 3–4 doses can often adequately address acute pain
■ Patients receiving buprenorphine for opioid use disorder who have acute pain refractory to other treatments and require additional opioid-based analgesia may also benefit from the addition of as-needed doses of buprenorphine.
■ Adding a short acting full agonist opioid to the patient’s regular dose of buprenorphine can also be effective for managing severe acute pain.
■ In situations when a full opioid agonist is needed for pain management, discontinuation of buprenorphine is not required.

Perioperative management Methadone and Buprenorphine
■ Discontinuation of methadone or buprenorphine before surgery is not required
■ If it is decided that buprenorphine or methadone should be discontinued before a planned surgery, this may occur the day before or the day of surgery
■ Methadone or buprenorphine can be resumed postoperatively when the need for intravenous analgesia has resolved
■ The pre-surgery daily doses of these medications can be resumed if they are withheld for a short period of time (up to 2–3 days)
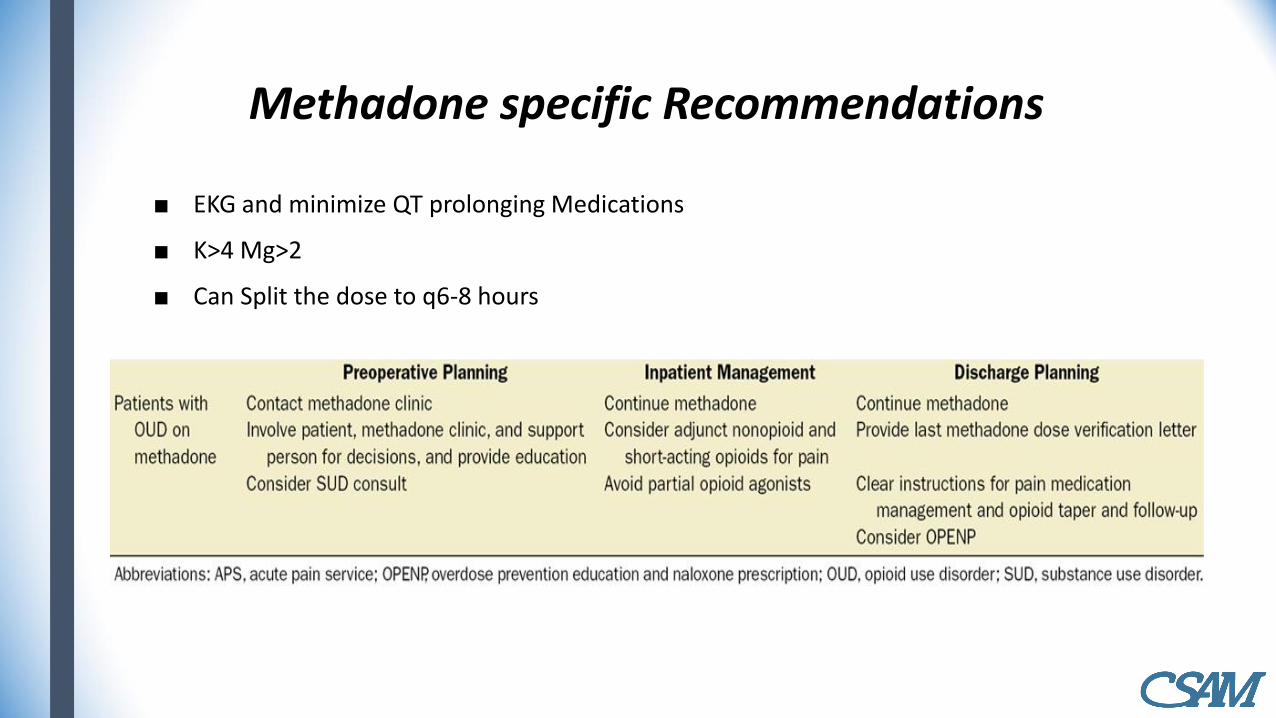
Methadone specific Recommendations
■ EKG and minimize QT prolonging Medications
■ K>4 Mg>2
■ Can Split the dose to q6-8 hours

Buprenorphine ASA Guidelines Elective Surgery
Anesthesiology June 2017, Vol. 126, 1180–1186.

Perioperative management of Naltrexone
■ Oral naltrexone should be discontinued at least 72 hours before elective surgery if pain management with opioids is anticipated.
■ Extended-release naltrexone should be stopped at least 30 days before surgery, and oral naltrexone may be used temporarily (until 72 hours prior to the planned surgery).
■ The surgical team should be aware of the use of naltrexone.
■ Patients should be off opioids for 3–7 days before resuming naltrexone (oral or extended-release formulations)

Overdose treatment: Naloxone Laws
Permission for “third-party prescriptions” that allow doctors
and pharmacists to prescribe and dispense naloxone to
someone who is not directly at risk for an overdose
Permission for pharmacists to dispense naloxone to individuals
without a prescription
States can also remove criminal or civil penalties for individuals
who possess naloxone without a prescription
“Good Samaritan” provisions, which encourage bystanders to
administer naloxone and to summon emergency responders in a timely manner, without fear of arrest or other negative legal
consequences
Removal of lay administrators’ civil, criminal, or professional
(such as Unauthorized Practice of Medicine penalties) liability
for administering naloxone

California Medical Board Recommendations
■ AB 2760 (Wood, Chapter 324) was signed into law in 2018 and becomes effective on January 1, 2019. This bill requires prescribers to offer a prescription for naloxone hydrochloride or another drug approved by the United States Food and Drug Administration for the complete or partial reversal of opioid depression to a patient when certain conditions
■ Mandate to consult CURES prior to prescribing, ordering, administering, or furnishing a Schedule II–IV controlled substance became effective October 2, 2018
• The first time a patient is prescribed, ordered, administered, or furnished a controlled substance, unless one of the exemptions below apply.
• Before subsequently prescribing a controlled substance, if previously exempt.
• At least once every six months if the controlled substance remains a part of the patient’s treatment plan.

References
■ Mee-Lee D, Shulman GD, Fishman MJ. The ASAM Criteria: Treatment Criteria for Addictive, Substance-Related, and Co-Occuring Conditions (3rd Ed.). The Change Companies; 2013
■ Sigmon SC, Bisaga A, Nunes EV, O’Connor PG, Kosten T, Woody G. Opioid detoxification and naltrexone induction strategies: recommendations for clinical practice. Am J Drug Alcohol Abuse. 2012;38(3):187–199. doi:10.3109/00952990.2011.653426.
■ Compton WM, Dawson DA, Goldstein RB, Grant BF. Crosswalk between DSM-IV dependence and DSM-5 substance use disorders for opioids, cannabis, cocaine and alcohol. Drug Alcohol Depend. 2013;132(1–2):387–390. doi:10.1016/j.drugalcdep.2013.02.036.
■ American Society on Addiction Medicine. The ASAM standards of care for the addiction specialist physician. http://www.asam.org/docs/ default-source/practice-support/quality-improvement/asam-standardsof-care.pdf?sfvrsn=10. Published 2019

References
■ Ling W, Charuvastra C, Collins JF, et al. Buprenorphine maintenance treatment of opiate dependence: a multicenter, randomized clinical trial. Addiction. 1998;93(4):475–486. doi:10.1046/j.1360-0443.1998.9344753.x
■ Larochelle MR, Bernson D, Land T, et al. Medication for opioid use disorder after nonfatal opioid overdose and association with mortality: A cohort study. Ann Intern Med. 2018;169(3):137–145. doi:10.7326/M17- 3107
■ National Institute on Drug Abuse. Principles of Drug Addiction Treatment: A Research-Based Guide 3rd Edition. Bethesda, MD: National Institute on Drug Abuse; National Institutes of Health; U.S. Department of Health and Human Services; 2018. https://www.drugabuse.gov/node/pdf/675/principles-of-drug-addiction-treatment-a-research-based-guide-third-edition

Thank You !