pafp pshpm interim guidance on family focused telehome
TRANSCRIPT
PAFP – PSHPM Interim Guidance on Family
Focused Telehome Care for Confirmed COVID-19
Patients with Mild or No Symptoms
Part 1
June 2021
Lead: Rojim J. Sorrosa, MD
Co-leads: Karin-Estepa Garcia, MD Mari Joanne G. Joson, MD Djhoanna Aguirre Pedro, MD Barbara Amity Flores, MD Arabelle Coleen P. Ofina, MD Rowena Marie T. Samares, MD Mae Alparaque-Corvera, MD
Technical Advisers: Leilanie Apostol-Nicodemus, MD
Aileen Riel-Espina, MD Rachel Rosario, MD
Technical Reviewers: Nenacia Ranali Nirena P. Mendoza, MD Jardine S. Sta. Ana, MD Technical Writer: Anna Charina R. Cabatuando, MD
Developed by: Philippine Academy of Family Physicians, Inc. Philippine Society of Hospice and Palliative Medicine
Table of Contents Background .................................................................................................................................................... 4
Objective: ...................................................................................................................................................... 5
Scope ........................................................................................................................................................... 5
Intended Target Users................................................................................................................................... 5
Limitations ..................................................................................................................................................... 5
I. Etiquette in Teleconsultation ........................................................................................................... 6
II. Confidentiality ................................................................................................................................... 7
III. Informed Consent ............................................................................................................................. 7
IV. Triaging .............................................................................................................................................. 8
V. Clinical Evaluation and Management ............................................................................................... 9
VI. Family-focused Care ........................................................................................................................ 14
VII. Community Involvement and Collaboration (PAFP, 2020)............................................................ 16
Decision Algorithms for the Telehome Care Management of Asymptomatic or Mildly Symptomatic
COVID – 19 Patients .................................................................................................................................... 18
Annex 1 ........................................................................................................................................................ 21
Annex 2 ........................................................................................................................................................ 23
Annex 3 ........................................................................................................................................................ 24
Annex 4 ........................................................................................................................................................ 27
References ................................................................................................................................................... 29
Background
COVID-19 infection was first documented in the last quarter of 2019 when China reported a cluster of pneumonia cases in Wuhan, Hubei province. A novel corona virus was identified. It was January of 2020 when the World Health Organization (WHO) declared an outbreak. Consequently, WHO has strategized to limit the impact the effect of COVID-19 by releasing the Strategic Preparedness and Response Plan in order to protect states and countries with weak health systems. It was in March 11 when the WHO declared COVID-19 as a pandemic when it spread rapidly to countries outside of China. By April of 2020, the cases reached up to 1 million worldwide (WHO, 2020). To date, multiple COVID variants have emerged. The B.1.1.7, B.1.351, P.1, B.1.427, and B.1.429 variants circulating in the United States have been classified as variants of concern according to the Centers for Disease Control and Prevention (CDC) (Centers for Disease Control and Prevention, 2021). Vaccines were developed to control the pandemic. These types of vaccines include Messenger RNA (mRNA) vaccines, vector vaccines and protein subunit vaccines (Mayo Clinic, 2021).
The Philippines was not spared from this unprecedented global health crisis. As of May 14, 2021, the Department of Health (DOH) has recorded 1,131,467 cases with the highest number of cases originating from the National Capital Region (NCR). In the NCR alone, almost 90% and more than 50% of the ICU and isolation beds are occupied, respectively (Department of Health, 2021). Furthermore, the occupancy rate reached a critical level, prompting the government to re-establish another Enhanced Community Quarantine for NCR last March 21, 2021. The Inter-agency Task Force (IATF) for the Management of Emerging Infectious Diseases proposed a resolution to curb the surge of COVID-19 cases in Bulacan, Cavite, Laguna, Rizal and the NCR. The resolution proposed that only less than 10% of confirmed cases and close contacts be kept monitored at home, and that the mandated 14-day quarantine and 10-day isolation are strictly observed. In addition, referral mechanisms of different treatment facilities should be ensured so that there would be a reduction in the occupancy rate by asymptomatic and mild cases to less than 10% of COVID-19 dedicated beds, improve health human resources, and facilitate effective coordination for the triaging and referral in the Local Government Unit (LGU), isolation, quarantine and health facilities (National Power Corporation, 2021).
In response to the persistent high tally of new cases daily, different hospitals started to create home care services to cater to COVID-19 confirmed patients in the mild to moderate category. The WHO and CDC also formulated recommendations on how to care for COVID-19 patients at home. These guidance documents were updated based on available latest evidences in the clinical management, implementation of self-care at home, and access to health facilities.
The Philippine Academy of Family Physicians (PAFP) in coordination with Philippine Society of Hospice and Palliative Medicine (PSHPM) developed this local guideline on how to care for asymptomatic to mildly symptomatic patients at home using the telemedicine platform. Currently existing guidelines mostly highlight hospital-based management and guidance on face-to-face consultations. Private stand-alone clinics, multispecialty clinics and hospitals have created different strategies to provide telehealth services, but these mostly cater to non-COVID patients. There are currently no guidance documents on how to provide telehome care for COVID-19 confirmed patients that is unique to our practice setting here in the Philippines. Furthermore, this telehome care guidance document will also provide steps to other primary care physicians, community practitioners, and health care workers on how to care for COVID-19 patients with mild symptoms in the home setting using a telehealth platform. It is recommended that these guidance documents be disseminated to all health care workers involved in telehome care for implementation, and evaluation of its effectiveness and acceptability.
Objective:
This telehome care guidance document was developed to guide health care workers who are involved in the management of asymptomatic or mild symptomatic COVID-19 at home through teleconsultation. It provides recommendations to the following clinical decisions: 1) Etiquette 2) Confidentiality; 3) Informed Consent; 3) Clinical Evaluation and management; 4) Family-focused Care; 5) Community Involvement and Collaboration. The recommendations shall not apply to patients with special needs (patients with medical, physical, cognitive, or developmental conditions who require special consideration when receiving care) and to COVID-19 patients with moderate and severe symptoms.
Scope
The use of this guidance document is limited to the provision of telehome care services to confirmed COVID-19 patients who are asymptomatic or with mild symptoms. These patients are confined at home in their respective communities or LGU’s with mandates or ordinances that allow home-based care.
Intended Target Users
The intended users are healthcare workers involved in the provision of telehome care services for confirmed COVID-19 patients who are confined at home.
Limitations
Applications for the provision of telehome care services may be insufficient for communities or LGU’s with limited infrastructural capacity to accommodate human resources persons operating the telehealth portal. Work from home provisions can possibly mitigate this problem, but several issues would still need to be addressed including: access to enough power supply, widespread unavailability of internet connectivity, limited bandwidth, weather instability, and insufficient computer specifications for operability of a centralized telehealth system. These can inevitably lead to poor image resolution and limited real-time video-conferencing thereby affecting the patient and family’s over-all care. City ordinances, executive orders from the local government unit, board resolutions, organizational or institutional policies, local skills, resources and knowledge which hinders proper infrastructure setup, process implementation, and referral systems may also limit the application of telehome care services.
I. Etiquette in Teleconsultation
In order to ensure that the professional standards of in-person care are maintained in a
virtual environment, the following recommendations are suggested for doctors and other
members of the care team who will be hosting the telehome care consultation. Here are the
key considerations to make when preparing to conduct telehealth visits (American Medical
Association, 2020; Department of Health, 2020; and Philippine Medical Association, 2020):
A. Environment
i. Choose a location that ensures privacy.
ii. Avoid background noise.
iii. Adequate lighting for clinical assessment
B. Equipment
i. Desktop computer/tablet/phone
ii. Adequate internet connection
iii. Web camera
iv. Headphone or earphone with a microphone (noise-cancelling if possible)
C. Attire and Decorum
i. The same level of professional attire as in-person care
ii. Be aware of one’s actions since these will be magnified on camera. Sit fully
upright.
iii. Avoid excessive hand movements or gestures. Do not fidget, scratch, play with
your hair, or touch your face.
iv. Disable picture-in-picture function.
v. Look directly at the camera or position video window of patient’s image at the
top of your screen below the webcam. This can be perceived by the patient as
making eye contact.
vi. Explain and narrate all your actions.
D. Communication
i. Speak slowly and clearly. Pause longer between statements to allow for
transmission delay.
ii. Type into the chat window to reiterate instructions or next steps.
iii. Check in frequently to elicit reactions and confirm understanding.
iv. Use non-verbal cues even on virtual visits: smile often, and use a warm tone of
voice.
v. Increase the frequency of empathetic statements to show that you are listening.
vi. Inform the patient when occupied such as when writing notes or looking at
radiologic images or laboratory results.
vii. Summarize and clarify questions in case of delay or signal interference.
viii. In case of disconnection during video consultations, inform the patient how to
continue the consultation.
E. Other Matters
i. Duration of teleconsultation – Length of teleconsult depends on the case of the
patient. It is important to manage your time wisely while ensuring that quality of
care is maintained, and proper patient counselling and education is done during
the encounter.
ii. Professional Fees – Charging of professional fee in any stage of telehome care is
left in the discretion of the practitioner.
II. Confidentiality
Telehome care offers a promising solution to many of the challenges facing health care
delivery in this time of the COVID19 pandemic. It is important to be vigilant with the
significant privacy and security risks in the telehealth system that can affect patients’ and
doctors’ level of trust and willingness to adopt and use the system. Both parties should be
aware that the use of telehealth might bring unique and unexpected risks for loss of
confidentiality. The following strategies are employed to minimize risks prior to commencing
a telehealth service:
• Inform the patient about the use of telehealth for the provision of care services.
• Obtain from the patient verbal or written consent for the use of telehealth as an
acceptable mode of delivering health services.
• Document the consent obtained from the patient in the treatment record. Verbal
consent can be documented in the form of a voice or video recording.
• Provide the patient with physician’s license or registration number and the type of
license or registration (written or verbal).
• Inform the patient of the potential risks and limitations of receiving treatment via
telehealth.
• Provide the patient with necessary health care advise and instructions either written or
verbal and ensure that it is well documented in the patient’s treatment record.
• Document reasonable efforts to ascertain the contact information of relevant resources,
including emergency services in the patient’s geographic area.
The following best practices can aid in ensuring that the security of the communication
medium and patient confidentiality are maintained:
• Researched and verified telehealth medium used is secured (e.g., transmission of voice
and video is encrypted).
• Ensure that the storage of all recordings and patient data is secured using the chosen
telehealth medium.
• If a personal computer is used, ensure antivirus software and/or firewalls are up to date.
• If a personal device is used (e.g., mobile phone), the most recent security update for the
device was installed.
III. Informed Consent
An informed consent shall be secured before triaging begins. This process ensures security,
privacy and confidentiality of information. Most importantly, communicating the informed
consent allows the patient to fully understand what accessing telehealth encompasses, what
its benefits are, and what possible risks it may pose to the patient. The purpose of the consent
form is to document that a discussion took place and that the patient was informed and was
able to understand the information provided. Once the patient has decided to use the
telehealth platform, it is important to follow these steps:
• Obtain the informed consent from the patient before the start of the consultation. This may be accomplished prior to the consultation where the consent form is sent to the patient beforehand. The physician may also opt to read the consent form to the patient before the consultation commences. The patient or the legally acceptable representative must express their voluntary consent during the teleconsultation.
• Give an explanation on what the patient can expect from the telehealth visit and what their rights are.
• Check with the patient about their responsibilities during the telehealth consultation. This may include specific steps like wearing headphones, finding a place to be alone during the visit to ensure privacy on their end, and staying in a location with secure signal or internet connection.
• If there’s anyone observing the visit, the patient should give their consent at the start.
IV. Triaging
The purpose of teletriaging is to identify patients who need urgent care. Although
originally, the triaging process is an element of care in the emergency department, this
process can also be applied during teleconsultation. It is imperative for physicians to assess
and triage patients encountered in telehealth. It is recommended to do this in a video-based
interaction in order to obtain adequate observational assessment, and complete history
taking and identification of exposure risk (Portnoy J et al, 2020).
Immediate classification of disease severity and categorization of mild, moderate,
severe, and critical conditions based on clinical evidence can help in identifying patients who
can proceed with in-home care with constant telehealth monitoring, and those who need to
be redirected to emergency facilities for urgent in-person care and referral (Reiss A et al,
2020). COVID-19 patients in the mild category commonly present with the following
symptoms namely: fever, cough, colds, nasal congestion, sore throat, headache, malaise,
some gastrointestinal symptoms such as diarrhea and abdominal pain, loss of taste and smell
(Cruz M et al, 2020).
Here are the recommended steps for the telephysician in doing the triaging process:
A. Establish rapport and introduce himself/herself to the index patient and his/her
family.
B. Assess the over-all clinical status of the patient and check for signs of severe COVID
infection and unstable medical comorbidity. The following questions should be taken
into consideration (Gilboy N, 2011):
i. Does this patient require immediate life-saving intervention?
ii. Is this a patient who shouldn't wait?
iii. How much resources will this patient need?
iv. What are the patient's vital signs?
C. Identify signs of severe COVID-19 infection (Philippine Society of Microbiology and
Infectious Diseases, 2020).
i. For adults and adolescents, watch out for ANY of the following signs and
symptoms:
1. Altered mental status
2. Severe respiratory distress
3. Respiratory rate of more than 30 cycles per minute
4. If with available portable or handheld pulse oximeter, oxygen
saturation below 93%
5. If with either digital or aneroidal sphygmomanometer, blood
pressure below 90/60mmHg
6. Other signs of shock or complications
ii. For children, watch out for presence of cough or difficulty of breathing plus at
least one of the following:
1. Central cyanosis
2. If with available portable or handheld pulse oximeter, oxygen
saturation below 90%
3. Severe respiratory distress (e.g. grunting, chest indrawing)
4. Signs of pneumonia with general danger signs: inability to
breastfeed or drink, lethargy unconsciousness, or convulsions
5. Other signs of pneumonia may be present such as fast breathing
• More than 60 breaths/min for less than 2 months
• More than 50 breaths/minute for 2 – 11 months
More than 40 breaths/min for 1 to 5 years old
D. Patients who are asymptomatic or have mild symptoms may be managed via
telehome care if they fulfill the following criteria (Philippine Society of Microbiology
and Infectious Diseases, 2020):
i. With available separate room in the household
ii. Able to adequately monitor and treat patient’s clinical evolution at home
iii. Prefers to stay at home instead of a quarantine facility
E. Patients exhibiting severe COVID – 19 infection or an unstable clinical status should
be advised to seek immediate physical face to face consultation and should
immediately be referred to the nearest emergency facility.
i. In the event that the patient refuses admission or emergency referral, the
primary care physician should identify and understand the reasons behind a
patient or a family’s hesitation. It is the role of the telehome care physician to
clarify any misperceptions and provide information that may aid in the
patient’s decision making.
ii. Document refusal of referral and admission through a digital waiver, or through
verbal audio recording.
V. Clinical Evaluation and Management
Clinical evaluation is indeed still possible in the telehealth setting despite the ongoing
unprecedented public health crisis. Based on the PAFP COVID-19 Task Force, adjustments
should pave the way for continuing the delivery or essential health care services (PAFP,
2020). The goal is to effectively and efficiently manage patients at home without
compromising quality of care. Clinicians should establish rapport, and trust should be
established through good eye contact by looking directly at the camera. During the
encounter, a designated space should be chosen to ensure privacy and professionalism.
While asking for subjective and objective findings, physicians are invited to look for new
opportunities to gather information from patients by using technology creatively to elicit
signs and symptoms for accurate assessment and management (Calton B et al, 2020).
These are the recommendations during the clinical evaluation and management:
A. Perform a complete and thorough history taking
i. Identify the patient’s reason for consultation and gather a reliable clinical
history.
ii. Find ways to elicit elements of the personal and social history such as
diet, physical activity, stress level, mood, mental health screening,
housing, transportation, safety, emergency contact details, housing
issues which may contribute to the success or failure of treatment
outcomes.
iii. Elicit the following information: number of people in the household,
number of rooms, number of bathrooms, ventilation, etc. which are
crucial in quarantine arrangements and instructions
B. Perform a general evaluation focusing on the patient’s general appearance, level
of alertness, level of distress, cognition, health literacy, and communication and
decision-making preferences.
C. Whenever applicable, use the 10-step method in doing patient assisted virtual
physical examination (Benziger CP, 2021).
i. Vital signs (weight, blood pressure, pulse, oxygen saturation,
temperature, respiratory rate)
ii. Skin assessment (new bruises, rash, swelling or edema, signs of
inflammation)
iii. Heads, Eyes, Ears, Nose and Throat (vision, hearing, sense of smell,
observe throat and swallowing)
iv. Neck (assess pain with rotation, neck vein engorgement, neck masses)
v. Lungs (observe for retractions, tachypnea, respiratory rate and pattern of
breathing)
vi. Heart (assess pulse, use available data from wearable items like a digital
watch with heart rate monitor, portable or handheld pulse oximeter)
vii. Abdomen (inspect if abdomen is distended, check for abdominal
breathing, allow the patient to palpate and observe for areas of
tenderness, may instruct the family member to do the abdominal
examination while the patient is lying on bed with the knees flexed)
viii. Extremities (press thumb in the pretibial area, assess edema)
ix. Neurological (mental status, gait and station, motor movements, sitting
to standing position)
x. Social Determinants of health (observe the patient’s facial expressions
and mood, and assess his/her surroundings and interactions with
caregivers and other members of the household),
D. Management of asymptomatic or mildly symptomatic patients is purely
supportive.
i. Pharmacologic treatment involves the use of antipyretics, analgesics,
decongestants, mucolytics, cough suppressants, and expectorants, which
are enumerated in Table 1 below.
ii. Patients with comorbidities should still be monitored and managed for
their existing medical conditions and should be advised on the
continuation of their maintenance medications
iii. Non-pharmacologic management should center on health education and
psychosocial support (PAFP, 2020).
1. Information about the virus and it’s pathophysiology
2. Prevention and control measures in order to limit transmission to
the other household members
3. Supportive management like nutrition and proper hydration
4. Mental health, psychosocial and practical support
5. Stress management, relaxation training, cognitive behavioral
therapy
6. Education and correction of emotionally critical misconceptions
E. Follow-up consultations may be done by the telephysician for monitoring of
improvement or progression of health outcomes. The frequency and duration of
follow-ups is on a case – to – case basis depending on the current scenario and
needs of the patient and his/her family.
F. Upon recovery of the patient, reintegration and clearance protocols found in the
most recently published HPAAC Unified COVID 19 Algorithms shall be followed.
Issuance of an online medical certificate and fit to work is under the discretion of
the attending telehealth physician.
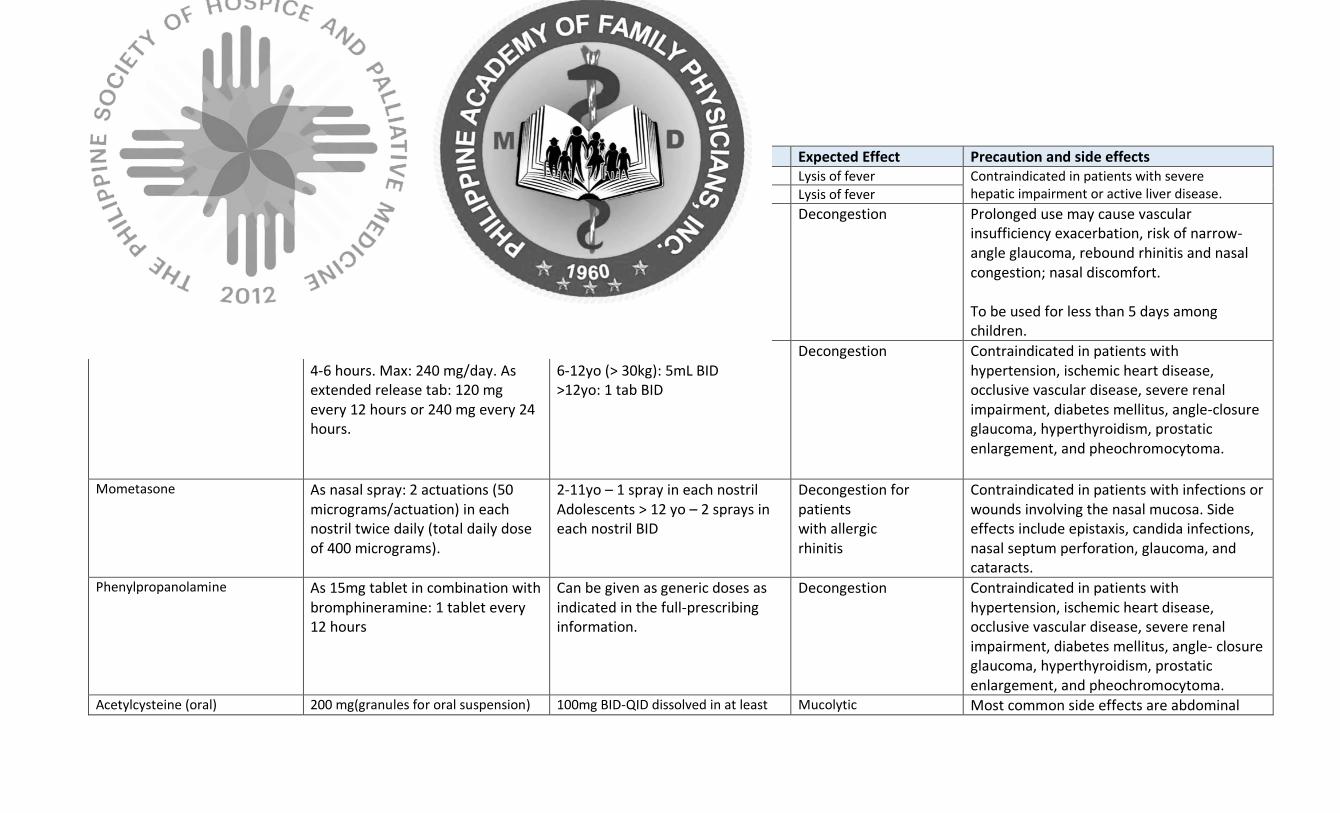
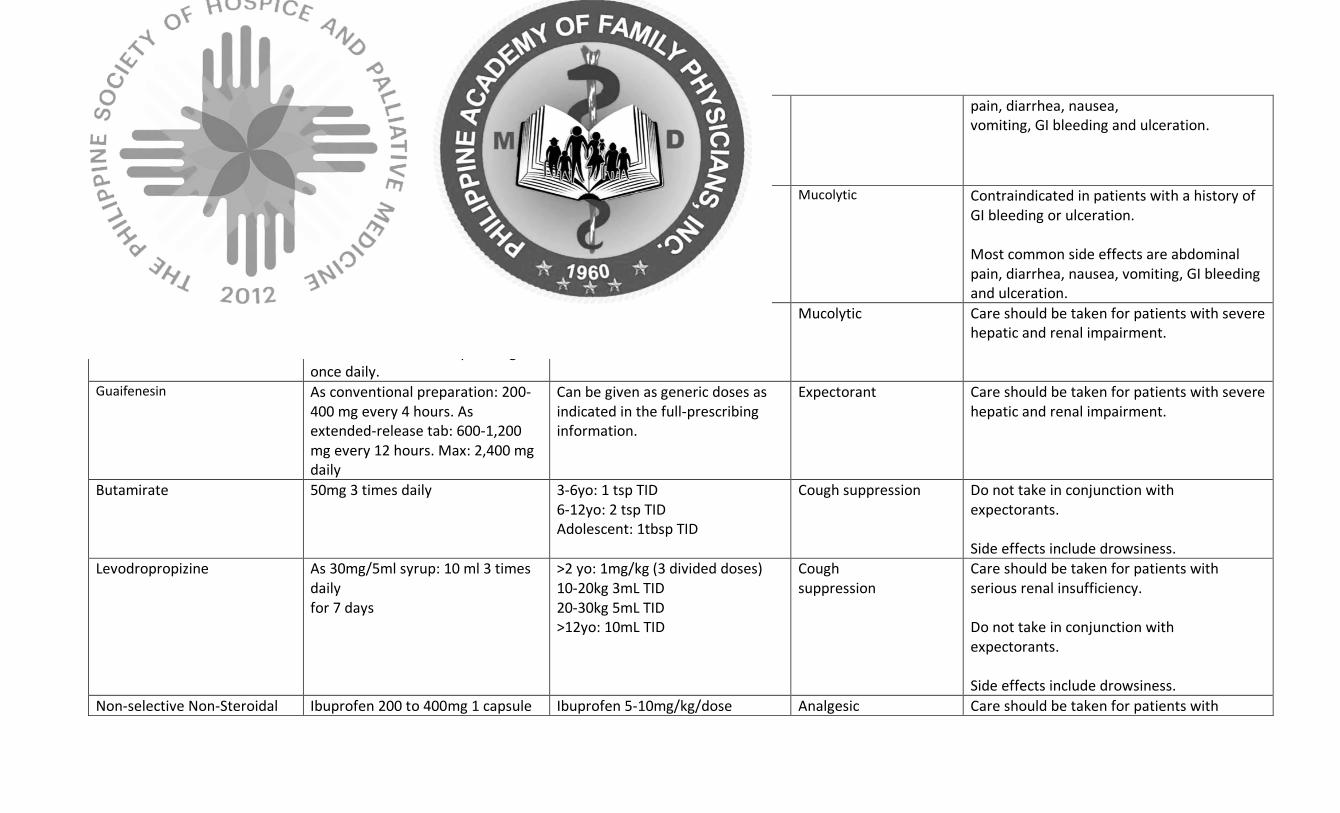
Table 1. Pharmacologic Options for COVID – 19 Patients with Mild Symptoms (PAFP, 2020).
Drug Dose Pediatric Dosages Expected Effect Precaution and side effects Paracetamol 500mg q4 PRN, 10-15mg/kg/dose Lysis of fever Contraindicated in patients with severe
hepatic impairment or active liver disease. Ibuprofen max 3g daily 5-10mg/kg/dose Lysis of fever
Oxymetazoline As 0.05% spray: 1-2 sprays twice daily into each nostril asneeded. Max duration of therapy: 3 days.
1mo-1yo (0.01%) – 1 drop TID 1-6yo (0.025%) – 1 drop TID >6yo (0.05%)- 1 drop TID
6yo
Decongestion Prolonged use may cause vascular insufficiency exacerbation, risk of narrow-angle glaucoma, rebound rhinitis and nasal congestion; nasal discomfort. To be used for less than 5 days among children.
Pseudoephedrine As conventional tab: 60 mg every 4-6 hours. Max: 240 mg/day. As extended release tab: 120 mg every 12 hours or 240 mg every 24 hours.
6-12yo (< 30kg): 2.5mL BID 6-12yo (> 30kg): 5mL BID >12yo: 1 tab BID
12 y
Decongestion Contraindicated in patients with hypertension, ischemic heart disease, occlusive vascular disease, severe renal impairment, diabetes mellitus, angle-closure glaucoma, hyperthyroidism, prostatic enlargement, and pheochromocytoma.
Mometasone As nasal spray: 2 actuations (50 micrograms/actuation) in each nostril twice daily (total daily dose of 400 micrograms).
2-11yo – 1 spray in each nostril Adolescents > 12 yo – 2 sprays in each nostril BID
Decongestion for patients with allergic rhinitis
Contraindicated in patients with infections or wounds involving the nasal mucosa. Side effects include epistaxis, candida infections, nasal septum perforation, glaucoma, and cataracts.
Phenylpropanolamine As 15mg tablet in combination with bromphineramine: 1 tablet every 12 hours
Can be given as generic doses as indicated in the full-prescribing information.
Decongestion Contraindicated in patients with hypertension, ischemic heart disease, occlusive vascular disease, severe renal impairment, diabetes mellitus, angle- closure glaucoma, hyperthyroidism, prostatic enlargement, and pheochromocytoma.
Acetylcysteine (oral) 200 mg(granules for oral suspension) 100mg BID-QID dissolved in at least Mucolytic Most common side effects are abdominal
2-3 times daily 600 mg (effervescent tablet) once daily to be dissolved in at least 75 mL of water
75 mL of water pain, diarrhea, nausea, vomiting, GI bleeding and ulceration.
Carbocisteine 500mg 3 times daily Can be given as generic doses as indicated in the full-prescribing information.
Mucolytic Contraindicated in patients with a history of GI bleeding or ulceration. Most common side effects are abdominal pain, diarrhea, nausea, vomiting, GI bleeding and ulceration.
Ambroxol As conventional preparation: 30 mg 3 times daily. As extended-release cap: 75 mg once daily.
Can be given as generic doses as indicated in the full-prescribing information.
Mucolytic Care should be taken for patients with severe hepatic and renal impairment.
Guaifenesin As conventional preparation: 200- 400 mg every 4 hours. As extended-release tab: 600-1,200 mg every 12 hours. Max: 2,400 mg daily
Can be given as generic doses as indicated in the full-prescribing information.
Expectorant Care should be taken for patients with severe hepatic and renal impairment.
Butamirate 50mg 3 times daily 3-6yo: 1 tsp TID 6-12yo: 2 tsp TID Adolescent: 1tbsp TID
Cough suppression Do not take in conjunction with expectorants. Side effects include drowsiness.
Levodropropizine As 30mg/5ml syrup: 10 ml 3 times daily for 7 days
>2 yo: 1mg/kg (3 divided doses) 10-20kg 3mL TID 20-30kg 5mL TID >12yo: 10mL TID
Cough suppression
Care should be taken for patients with serious renal insufficiency. Do not take in conjunction with expectorants. Side effects include drowsiness.
Non-selective Non-Steroidal Ibuprofen 200 to 400mg 1 capsule Ibuprofen 5-10mg/kg/dose Analgesic Care should be taken for patients with
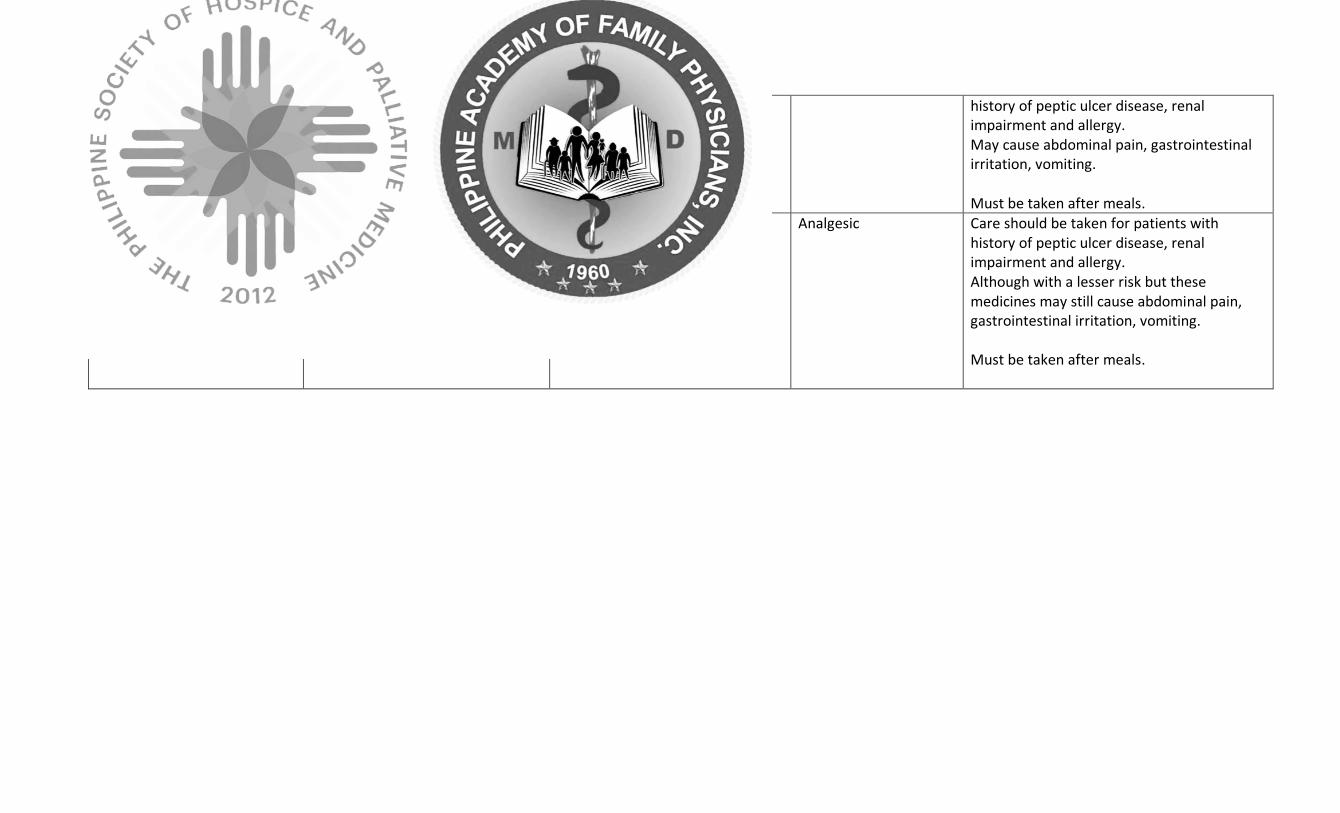
Anti-Inflammatory Drugs such as ibuprofen, mefenamic acid
every 6 hours Mefenamic acid 500mg 1 cap every 6 to 8 hours
history of peptic ulcer disease, renal impairment and allergy. May cause abdominal pain, gastrointestinal irritation, vomiting. Must be taken after meals.
Selective Cyclooxygenase- 2 inhibitors
Celecoxib 200mg BID Celecoxib 400mg OD
Celecoxib for adolescents only Analgesic Care should be taken for patients with history of peptic ulcer disease, renal impairment and allergy. Although with a lesser risk but these medicines may still cause abdominal pain, gastrointestinal irritation, vomiting. Must be taken after meals.
VI. Family-focused Care
Family-focused care is an approach that aims to address the needs of each of the
members of the family. Closely knit families are particularly at high risk of contracting the
COVID-19 infection. Preventive and control measures need to be in place. Psychosocial and
practical support is aimed at improving the family’s quality of life. Interventions in health
care with strong family involvement are known to be effective in addressing complex health
problems and conditions. These family mediations can be done both in the outpatient face-
face clinic or even in the virtual setting (Prado G et al, 2019). Creating a family-focused care
plan which outlines the activities applicable to the family’s home conditions, roles,
structures, and habits can allay the destructive effects of the current pandemic. The health
care plan includes the treatment goals and the roles that each family member assumes in
order to successfully conquer the disease as a unit. Designated family caregivers have a
crucial role as the one who continuously encourage collaboration among family members.
Proper setting up of the environment at home also plays a vital part in infection control and
in preventing sickness of other family members (PAFP, 2020).
These are the recommendations on how to provide a family-focused care at home:
A. Initiate family, psychosocial and spiritual support
i. The physician elicits the family genogram from the patient or other members
of the household. The physician should be able to identify the next of kin,
and other high-risk members.
ii. There should be focused assessment and discussion on the problematic areas
of the social determinants of health. Spiritual assessment and care should be
included.
iii. Identify a family caregiver who will remind the family to follow and
implement the plan. Make sure this person is supported by all family
members.
B. Assess the family’s performance of routine tasks for the prevention and safety of
other household family members (PAFP, 2020).
i. Practice personal hygiene that includes regular and appropriate hand
washing, daily bath, cough and sneezing etiquette, minimal hand contact
with eyes, nose and mouth, and strict personal use of eating utensils, bath
towels, etc.
ii. Daily cleaning of frequently touched surface like doorknobs, light and
appliance control switches, gadgets, armchairs and tabletops. Cleaning
agents can be ordinary detergents and water or 70% alcohol.
iii. Appropriate use and disposal of personal protective equipment like gloves,
face mask.
C. Implement home-based interventions and goals of care
i. Give medical advice and manage the identified medical problems of the
patient with mild COVID-19 infection (World Health Organization , 2021).
1. The patient should be placed on home isolation, and whenever
possible, transferred to a designated isolation facility if there are
available beds or units
2. The patient should be given supportive treatment and prescription
such as antipyretics for fever, analgesics for pain, adequate nutrition,
adequate hydration (World Health Organization , 2021; PAFP, 2020).
3. Counsel patients with mild COVID-19 about signs and symptoms of
complications that should prompt urgent care especially for persons
with risk factors for severe illness.
1
2
3
4
5
6
7
8
9
N
N
Y
Y
Y
ii. Advice an exposed family member to stay home and in the room or area
allocated for quarantine, wear mask and maintain at least 2 meters physical
distance from the other family members. Make sure their clothing, personal
belongings and other things that they usually hold is cleaned regularly and
not touched by other members.
iii. For exposed family members, advice on the monitoring for the appearance
of symptoms like fever, colds, cough, and difficulty of breathing or worsening
of symptoms.
1. If the symptoms are mild, continue home quarantine, take over-the-
counter medications like paracetamol for fever, increase water
intake and ensure adequate nutrition, sleep and rest.
2. Other family members are encouraged to provide psychological and
social support to an exposed and isolated member.
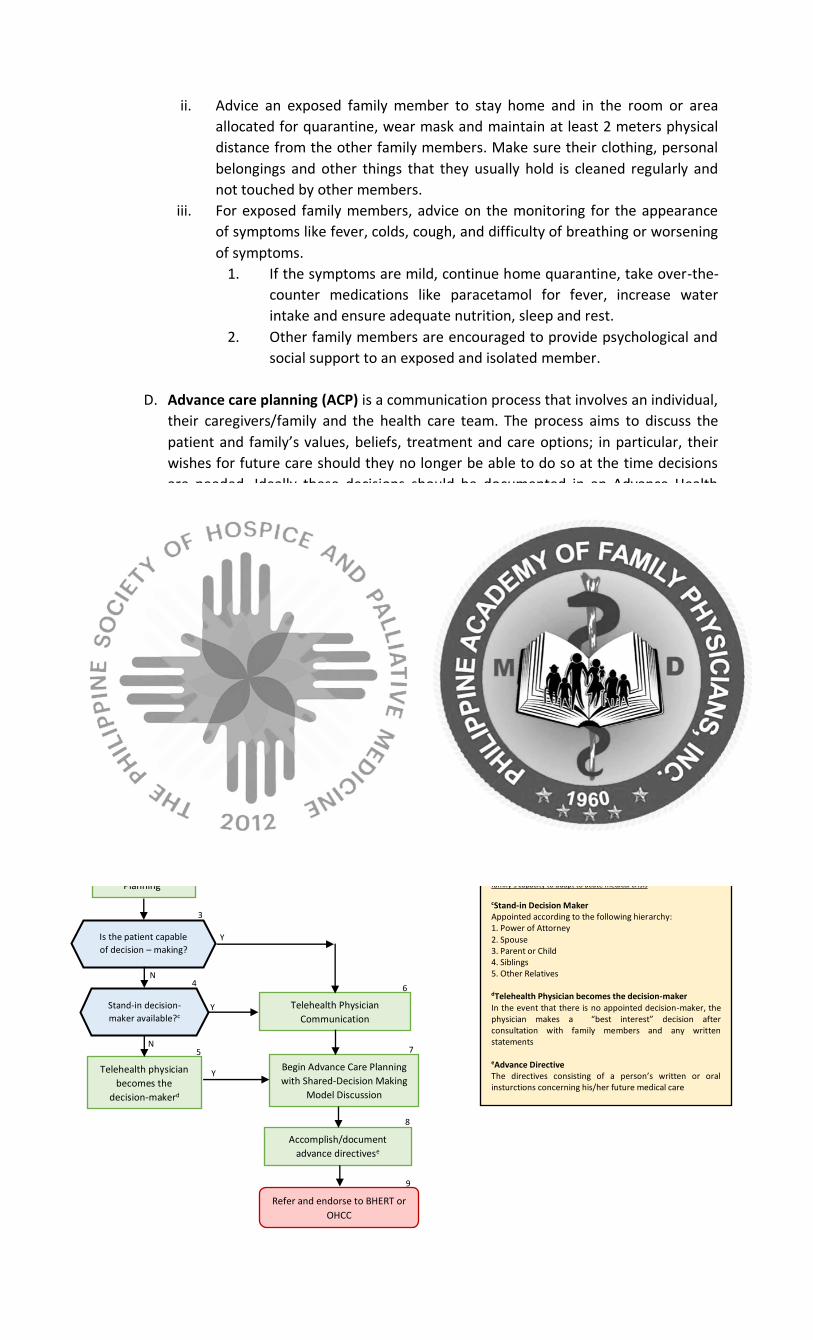
D. Advance care planning (ACP) is a communication process that involves an individual,
their caregivers/family and the health care team. The process aims to discuss the
patient and family’s values, beliefs, treatment and care options; in particular, their
wishes for future care should they no longer be able to do so at the time decisions
are needed. Ideally these decisions should be documented in an Advance Health
Directive. Shared decision making is a process in which clinicians and patients work
together to make decisions and select tests, treatments and care plans based on
clinical evidence that balances risks and expected outcomes with patient
preferences and values. These are the steps of the Advance Care Planning process
using the Shared Decision-Making Model (Office of the National Coordinator for
Health Information Technology, 2013):
i. Invite the patient to participate
ii. Present options
iii. Provide information on benefits and risks
iv. Assist patients in evaluating options based on their goals and concerns
v. Facilitate deliberation and decision making
vi. Assist patients to follow through on the decision
COVID-19 confirmed patient
consulting for telehome care using
mobile health applicationsa
Decision to discuss
Advance Care
Planningb
Is the patient capable
of decision – making?
Stand-in decision-
maker available?c
Telehealth physician
becomes the
decision-makerd
Telehealth Physician
Communication
Begin Advance Care Planning
with Shared-Decision Making
Model Discussion
Accomplish/document
advance directivese
FOOTNOTES aConfirmed COVID - 19 Patient Person who tested positive for SARS-CoV-2 RT PCR Test bTiming of ACP Discussion Timing should consider patient’s overall clinical status, patient’s/family’s values and preferences, and telephysician’s capabilities. Too early discussion may cause distress, whereas too late initiation may cause inconsistencies in patient care and may set back family’s capacity to adapt to acute medical crisis
cStand-in Decision Maker Appointed according to the following hierarchy: 1. Power of Attorney
2. Spouse 3. Parent or Child 4. Siblings 5. Other Relatives dTelehealth Physician becomes the decision-maker In the event that there is no appointed decision-maker, the physician makes a “best interest” decision after consultation with family members and any written statements eAdvance Directive The directives consisting of a person’s written or oral insturctions concerning his/her future medical care
Refer and endorse to BHERT or
OHCC
Figure 1. Decision Algorithm for Advance Care Planning in Telehome Care (adapted with modifications
from Philippine Society of Microbiology and Infectious Diseases Unified COVID 19 Algorithms (Section 4:
Special Considerations) Nov 7, 2020)
VII. Community Involvement and Collaboration (PAFP, 2020)
The COVID-19 pandemic calls for a more collaborative and community-oriented
preparedness and response for more effective achievement of health objectives. Family
physicians must provide patients and families access to community health resources by
conducting a quick community health resource mapping. Community-integrated response to
control wide-spread disease has been used historically. From previous experience, successful
infection and pandemic control necessitates coordination among health care workers,
government units, and the community (Stein-Zamir et al, 2019). Policies and approaches
include infection control and avoidance, immediate diagnosis, and sanitation control
measures synergized among all stakeholders (Takahashi et al, 2017). Collaborative pandemic
response requires providing access to health resources available at the community level
through facilitated coordination and referral systems with the Barangay Health Emergency
Response Team (BHERTs), community – established isolation facilities, and the different
private and government clinics and hospitals (PAFP, 2020). The One Hospital Command
Center (OHCC) is an initiative launched by the Department of Health and the Inter-agency
Task Force on Emerging Infectious Diseases (IATF EID) in coordination with different
government agencies. The OHCC aims to mitigate the gaps in the effectiveness and efficiency
of health facility referral of COVID 19 cases in Metro Manila. The OHCC shall ensure and
coordinate the timely transport and pick-up of patients needing emergent care and transfer
to facilities that could best provide for the level of care they require. The Center also updates
the public of the health system capacity data and risk communications of the hospitals in the
area. It ensures that scarce critical health care services are optimally allocated. (DOH, 2020)
These are the considerations when involving the community through the Local
Government Unit (LGU), Barangay Health Emergency Response Team (BHERT), and the One Hospital Command Center (OHCC):
A. Identify and be familiar with local triaging and referral systems /networking with the LGU and BHERTS. The BHERTs are teams assigned to give urgent and appropriate medical and emergency help to patients in the community during the COVID 19 pandemic. They are also tasked to implement needed health programs, standards, protocol dissemination and updates. This initiative was formed as a way of collaboration between the local government units of the DILG and the DOH. (DOH, 2020)
i. The telehome care physician is encouraged to advise the patient to coordinate and communicate with their designated BHERT for quarantine monitoring, contact tracing, and eventual clearance. The physician may also opt to coordinate and report to the BHERT themselves. A Case Investigation Form (CIF) may be submitted to the designated BHERT email or contact information for monitoring and proper contact tracing.
ii. In the event that the patient comes from a different municipality or city, coordination and reporting with the physician’s current BHERT or LGU can be done as mentioned above, and the receiving BHERT or LGU may aid in communicating and transferring information to the patient’s city/place of jurisdiction for further endorsement and management.
iii. While the patient is being monitored separately by BHERT, the telehome care physician may opt to do daily telemonitoring of patients who are on quarantine at home. This may be done through daily phone calls or video
consultations twice a day to check on the status of the patient and the family. The Patient-Centered and Family-focused Telehome Care Service Follow-up Record Form found in Annex 2 may be used for daily monitoring.
B. It is important for the telehealth physician to maintain contact details and information of various resources, as well as essential social and support services available in the community. The following details should be gathered and identified in order to maintain a proper referral network (PSHPM, 2020): Table 1. Sample table showing information needed to identify local networks for referral Category Institution Name of Contact Telephone/Mobile
Number
RHU, Distric Health Center or City Health Office
District Hospital
Provincial Hospital
Regional Hospital
Palliative and Hospice Care Specialist
Geriatric Specialist
Oncologist
Social Welfare
Religious Workers
Palliative Care Hotlines Pain Specialists
C. Facilitate appropriate coordination of care, including reporting, monitoring,
surveillance, outbreak investigations, isolation precautions, community health education and advocacy.
D. Once the telehealth physician triages/monitors and identifies a patient to be presenting with severe or critical COVID 19 signs and symptoms, the telephysician may:
i. Contact the designated BHERT where the patient belongs for coordinated referral and assistance for transfer of patient, and follow-up with the BHERT and patient as necessary to check on the status of transfer
ii. The patient may be advised to contact the BHERT directly and the One Hospital Command Center through the following ways (DOH, 2020):
i. Downloading the Pure Force Citizens Application at the Google Play Store or the Apple Store for free
ii. Call the dedicated hotlines: 02-886-505-00; 0915-777-7777 and 0919-977-3333
iii. Scan the Quick Response (QR) code iii. The telephysician may assist in coordinating transfer to the nearest ER facility
or through their affiliated hospital or network
2
3
4
7
8
9
10
5
6
11
12 13
14
Y
1
Decision Algorithms for the Telehome Care Management of Asymptomatic or Mildly Symptomatic COVID – 19 Patients
*Note: These forms may be modified and adapted based on your current practice setting and context. All changes and
adaptations should be communicated to the Philippine Academy of Family Physicians (PAFP) for consolidation of best practices
and documentation purposes through the PAFP secretariat using this email address: [email protected] or
\
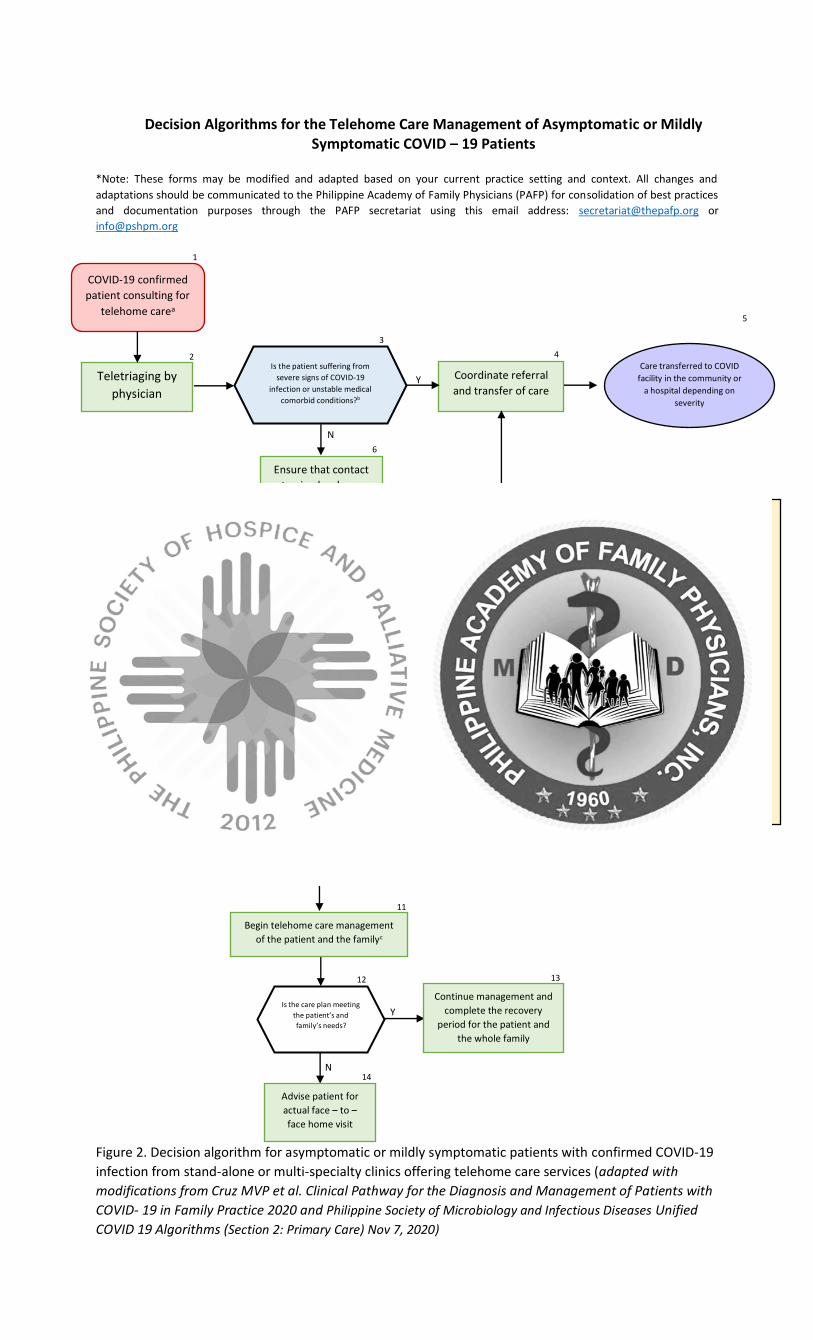
Figure 2. Decision algorithm for asymptomatic or mildly symptomatic patients with confirmed COVID-19
infection from stand-alone or multi-specialty clinics offering telehome care services (adapted with
modifications from Cruz MVP et al. Clinical Pathway for the Diagnosis and Management of Patients with
COVID- 19 in Family Practice 2020 and Philippine Society of Microbiology and Infectious Diseases Unified
COVID 19 Algorithms (Section 2: Primary Care) Nov 7, 2020)
Coordinate referral
and transfer of care
Ensure that contact
tracing has been
initiated thru
CESU/MESU
No available
separate room in
the household?
Y
N
Difficult to adequately
monitor and treat
patient’s clinical evolution
at home?
Y
N
Does the patient prefer
to stay in quarantine
facility?
Y
N
Isolate at home
FOOTNOTES aConfirmed COVID - 19 Patient Person who tested positive for SARS-CoV-2 RT PCR Test bSevere signs of COVID – 19 infection For adults and adolescents, watch out for ANY of the following signs and symptoms: Altered mental status, severe respiratory distress, RR ≥ 30/min, O2Sat < 93%, BP < 90/60 mmHg, signs of shock or complications For children, watch out for signs of DOB + 1 of the ff:
Central cyanosis, O2Sat < 90%, severe respiratory distress (e.g., retractions, grunting), signs of pneumonia with danger signs: inability to breastfeed or drink, lethargic, unconscious, with convulsions, RR > 60/min for < 2mos, RR>50/min for 2-11mos, RR > 40/min for 1-5y/o cTelehome care management Elicit patient’s complaint and do routine clinical
evaluation Symptomatic treatment Educate on COVID-19 Assess the family’s performance of routine tasks for
the prevention and safety of other household family members
Start patient-centered care Start family-focused health plan Start community-oriented plan Start telehealth home care set-up Establish telehome care set-up and continuity of care
Is the care plan meeting
the patient’s and
family’s needs?
Y
N
Advise patient for
actual face – to –
face home visit
Continue management and
complete the recovery
period for the patient and
the whole family
N
COVID-19 confirmed
patient consulting for
telehome carea
Teletriaging by
physician
Is the patient suffering from
severe signs of COVID-19
infection or unstable medical
comorbid conditions?b
Care transferred to COVID
facility in the community or
a hospital depending on
severity
Begin telehome care management
of the patient and the familyc
Y
2
3
4
7
8
9
10
5
6
11
12 13
14
\
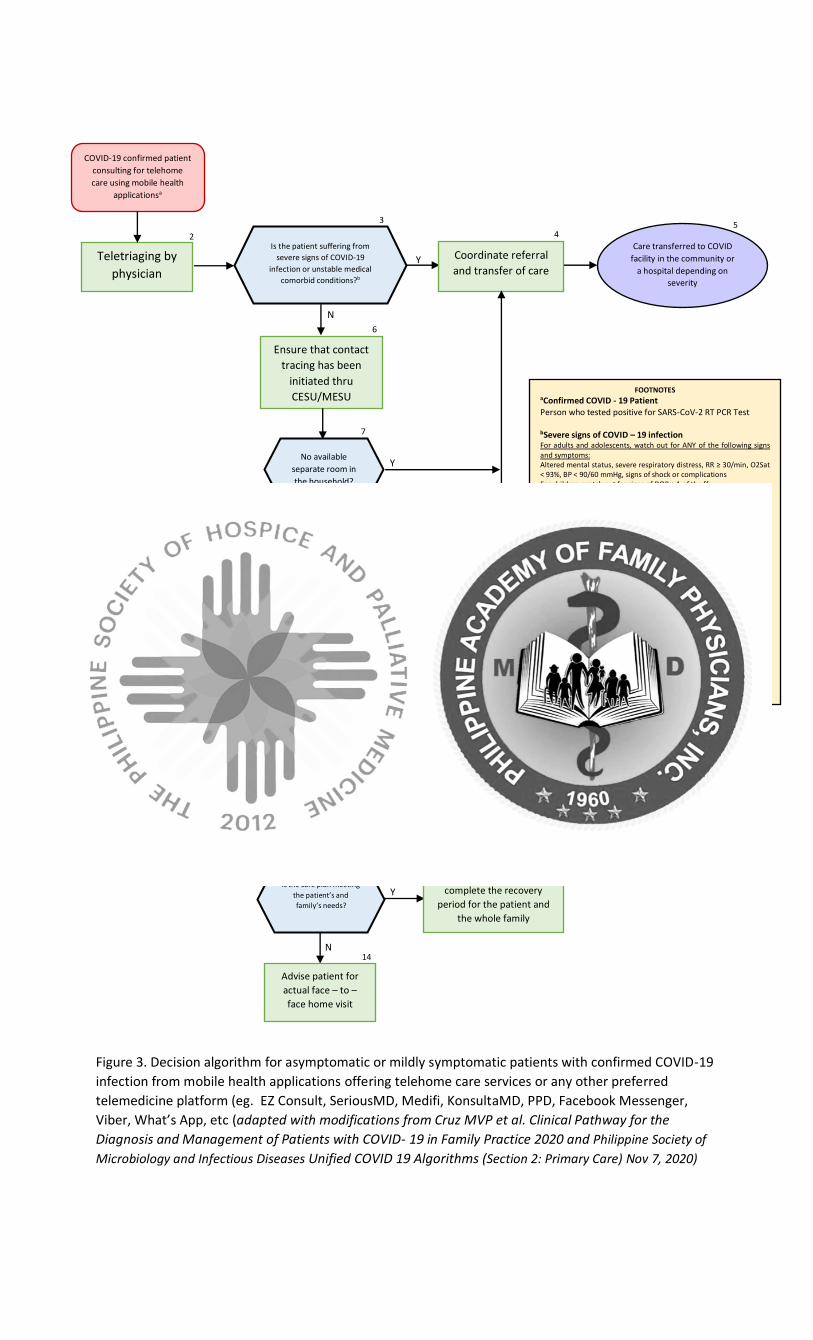
Figure 3. Decision algorithm for asymptomatic or mildly symptomatic patients with confirmed COVID-19
infection from mobile health applications offering telehome care services or any other preferred
telemedicine platform (eg. EZ Consult, SeriousMD, Medifi, KonsultaMD, PPD, Facebook Messenger,
Viber, What’s App, etc (adapted with modifications from Cruz MVP et al. Clinical Pathway for the
Diagnosis and Management of Patients with COVID- 19 in Family Practice 2020 and Philippine Society of
Microbiology and Infectious Diseases Unified COVID 19 Algorithms (Section 2: Primary Care) Nov 7, 2020)
N
COVID-19 confirmed patient
consulting for telehome
care using mobile health
applicationsa
Teletriaging by
physician
Is the patient suffering from
severe signs of COVID-19
infection or unstable medical
comorbid conditions?b
Coordinate referral
and transfer of care
Care transferred to COVID
facility in the community or
a hospital depending on
severity
Ensure that contact
tracing has been
initiated thru
CESU/MESU
No available
separate room in
the household?
Y
N
Difficult to adequately
monitor and treat
patient’s clinical evolution
at home?
Y
N
Does the patient prefer
to stay in quarantine
facility?
Y
N
Isolate at home
FOOTNOTES aConfirmed COVID - 19 Patient Person who tested positive for SARS-CoV-2 RT PCR Test bSevere signs of COVID – 19 infection For adults and adolescents, watch out for ANY of the following signs and symptoms: Altered mental status, severe respiratory distress, RR ≥ 30/min, O2Sat < 93%, BP < 90/60 mmHg, signs of shock or complications For children, watch out for signs of DOB + 1 of the ff: Central cyanosis, O2Sat < 90%, severe respiratory distress (e.g., retractions, grunting), signs of pneumonia with danger signs: inability to breastfeed or drink, lethargic, unconscious, with convulsions, RR > 60/min for < 2mos, RR>50/min for 2-11mos, RR > 40/min for 1-5y/o cTelehome care management Elicit patient’s complaint and do routine clinical
evaluation Symptomatic treatment Educate on COVID-19 Assess the family’s performance of routine tasks for
the prevention and safety of other household family members
Start patient-centered care Start family-focused health plan Start community-oriented plan Start telehealth home care set-up Establish telehome care set-up and continuity of care
Is the care plan meeting
the patient’s and
family’s needs?
Y
N
Advise patient for
actual face – to –
face home visit
Continue management and
complete the recovery
period for the patient and
the whole family
Begin telehome care management
of the patient and the familyc
Y
12 13
14
2
3
4
7
8
9
10
5
6
11
\
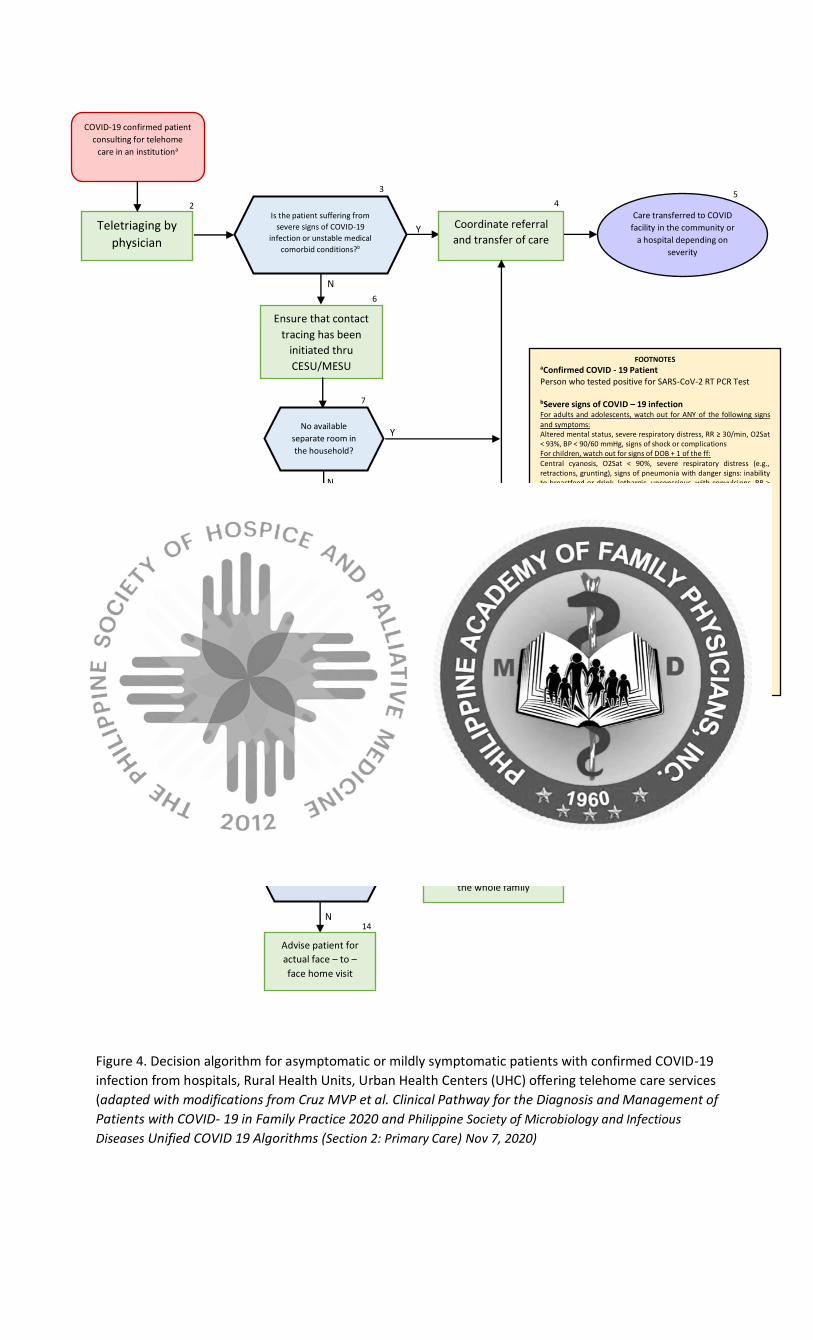
Figure 4. Decision algorithm for asymptomatic or mildly symptomatic patients with confirmed COVID-19
infection from hospitals, Rural Health Units, Urban Health Centers (UHC) offering telehome care services
(adapted with modifications from Cruz MVP et al. Clinical Pathway for the Diagnosis and Management of
Patients with COVID- 19 in Family Practice 2020 and Philippine Society of Microbiology and Infectious
Diseases Unified COVID 19 Algorithms (Section 2: Primary Care) Nov 7, 2020)
N
COVID-19 confirmed patient
consulting for telehome
care in an institutiona
Teletriaging by
physician
Is the patient suffering from
severe signs of COVID-19
infection or unstable medical
comorbid conditions?b
Coordinate referral
and transfer of care
Care transferred to COVID
facility in the community or
a hospital depending on
severity
Ensure that contact
tracing has been
initiated thru
CESU/MESU
No available
separate room in
the household?
Y
N
Difficult to adequately
monitor and treat
patient’s clinical evolution
at home?
Y
N
Does the patient prefer
to stay in quarantine
facility?
Y
N
Isolate at home
Begin telehome care management
of the patient and the familyc
FOOTNOTES aConfirmed COVID - 19 Patient Person who tested positive for SARS-CoV-2 RT PCR Test bSevere signs of COVID – 19 infection For adults and adolescents, watch out for ANY of the following signs
and symptoms: Altered mental status, severe respiratory distress, RR ≥ 30/min, O2Sat < 93%, BP < 90/60 mmHg, signs of shock or complications For children, watch out for signs of DOB + 1 of the ff:
Central cyanosis, O2Sat < 90%, severe respiratory distress (e.g., retractions, grunting), signs of pneumonia with danger signs: inability to breastfeed or drink, lethargic, unconscious, with convulsions, RR > 60/min for < 2mos, RR>50/min for 2-11mos, RR > 40/min for 1-5y/o cTelehome care management Elicit patient’s complaint and do routine clinical
evaluation Symptomatic treatment Educate on COVID-19 Assess the family’s performance of routine tasks for
the prevention and safety of other household family members
Start patient-centered care Start family-focused health plan Start community-oriented plan Start telehealth home care set-up Coordinate with affiliated institution for diagnostic
needs Establish telehome care set-up and continuity of care
Is the care plan meeting
the patient’s and
family’s needs?
Y
N
Advise patient for
actual face – to –
face home visit
Continue management and
complete the recovery
period for the patient and
the whole family
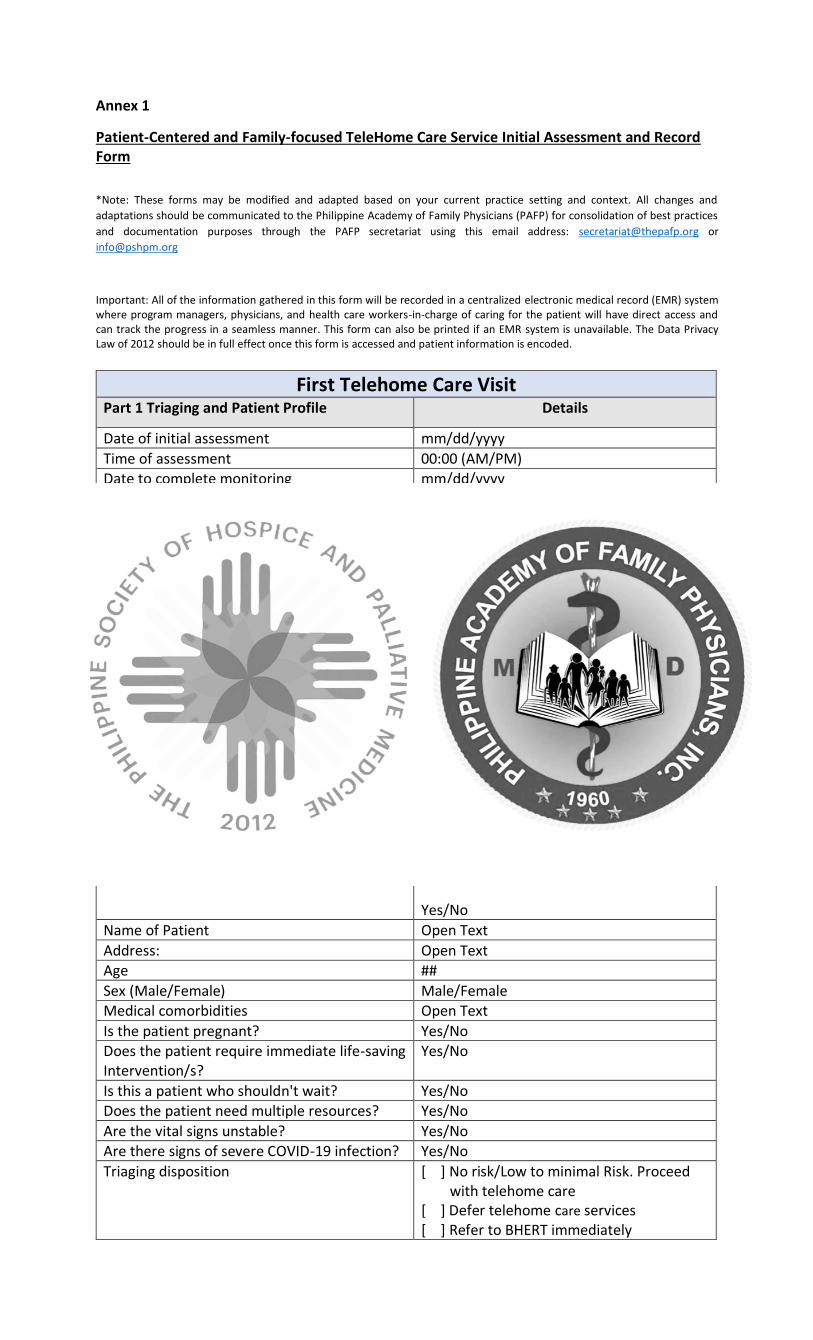
Annex 1
Patient-Centered and Family-focused TeleHome Care Service Initial Assessment and Record Form
*Note: These forms may be modified and adapted based on your current practice setting and context. All changes and
adaptations should be communicated to the Philippine Academy of Family Physicians (PAFP) for consolidation of best practices
and documentation purposes through the PAFP secretariat using this email address: [email protected] or
Important: All of the information gathered in this form will be recorded in a centralized electronic medical record (EMR) system where program managers, physicians, and health care workers-in-charge of caring for the patient will have direct access and can track the progress in a seamless manner. This form can also be printed if an EMR system is unavailable. The Data Privacy Law of 2012 should be in full effect once this form is accessed and patient information is encoded.
First Telehome Care Visit Part 1 Triaging and Patient Profile Details
Date of initial assessment mm/dd/yyyy
Time of assessment 00:00 (AM/PM)
Date to complete monitoring mm/dd/yyyy Date of last potential exposure to the virus (day 0): mm/dd/yyyy Date of confirmed to have a positive RT PCR test mm/dd/yyyy
Name of Telehome care physician Open Text
Obtain patient’s informed consent Good day, [insert name of patient]. I am [insert name of tele-triage officer], the telehome care physician/officer-in-charge for this call. I will be facilitating the discussion about telehome care which includes patient assessment, clinical evaluation, and family-focused advice. Please be informed that this conversation is recorded and we will collect sensitive data. Rest assured that all information will be treated with utmost confidentiality in accordance to the Data Privacy Law. Do you want to proceed with the telehome care for confirmed COVID-19 patients who are asymptomatic or with mild symptoms? Yes/No
Name of Patient Open Text
Address: Open Text
Age ##
Sex (Male/Female) Male/Female Medical comorbidities Open Text
Is the patient pregnant? Yes/No Does the patient require immediate life-saving Intervention/s?
Yes/No
Is this a patient who shouldn't wait? Yes/No Does the patient need multiple resources? Yes/No
Are the vital signs unstable? Yes/No
Are there signs of severe COVID-19 infection? Yes/No
Triaging disposition [ ] No risk/Low to minimal Risk. Proceed with telehome care
[ ] Defer telehome care services [ ] Refer to BHERT immediately
[ ] Refer to nearest hospital through one hospital command center
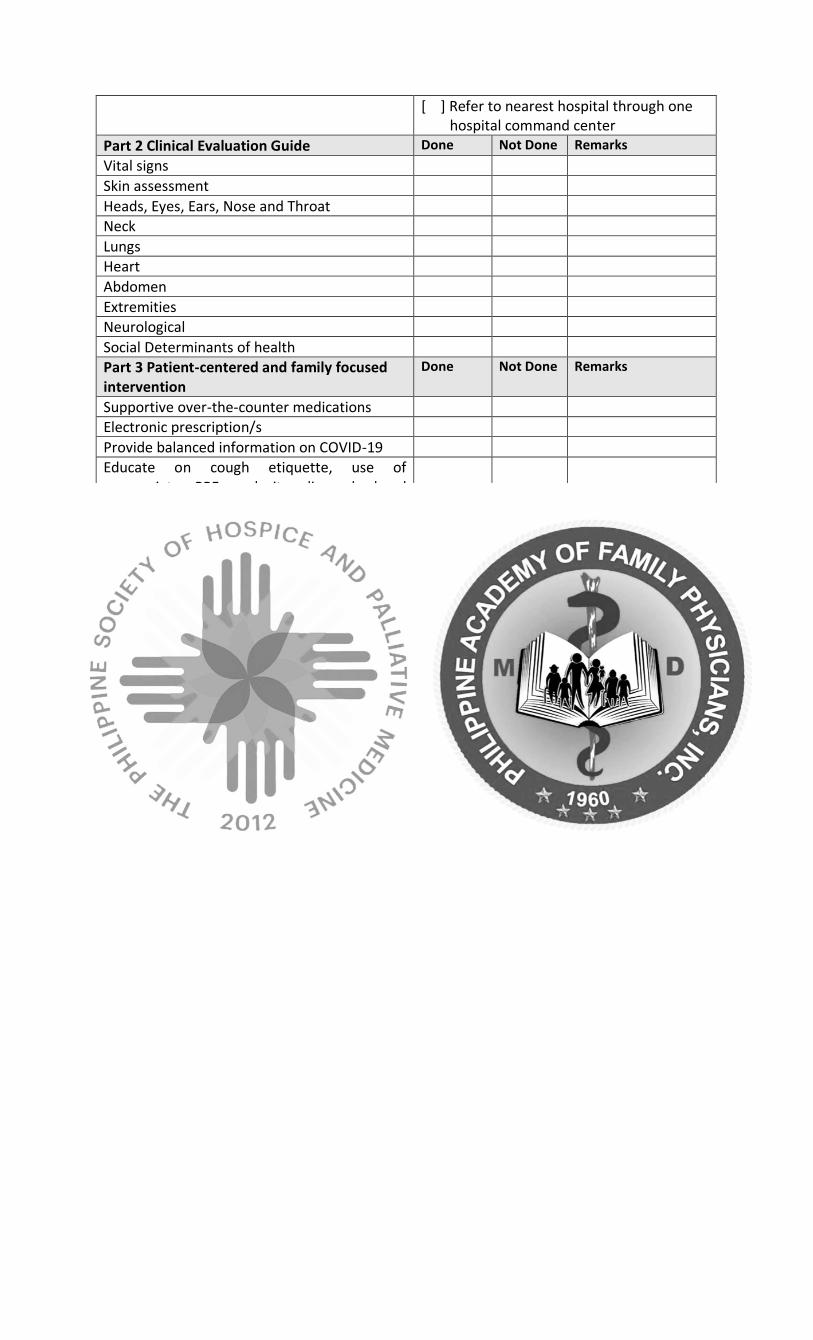
Part 2 Clinical Evaluation Guide Done Not Done Remarks Vital signs
Skin assessment
Heads, Eyes, Ears, Nose and Throat Neck
Lungs Heart
Abdomen
Extremities Neurological
Social Determinants of health Part 3 Patient-centered and family focused intervention
Done Not Done Remarks
Supportive over-the-counter medications Electronic prescription/s
Provide balanced information on COVID-19
Educate on cough etiquette, use of appropriate PPE and its disposal, hand hygiene, physical distancing and quarantine
Advice on adequate nutrition, hydration and rest
Offer psychological support, self-care advice and monitoring of symptoms
Assist to develop and implement a Family Health Plan
Refer for contact tracing and coordination of care with the municipal/city health office/BHERT/OHCC
Set-up telemedicine for monitoring and follow-up
Part 4 Patient Outcomes Yes No Remarks Does the patient have adequate knowledge about COVID-19?
Will the patient comply?
Are the family health care goals met?
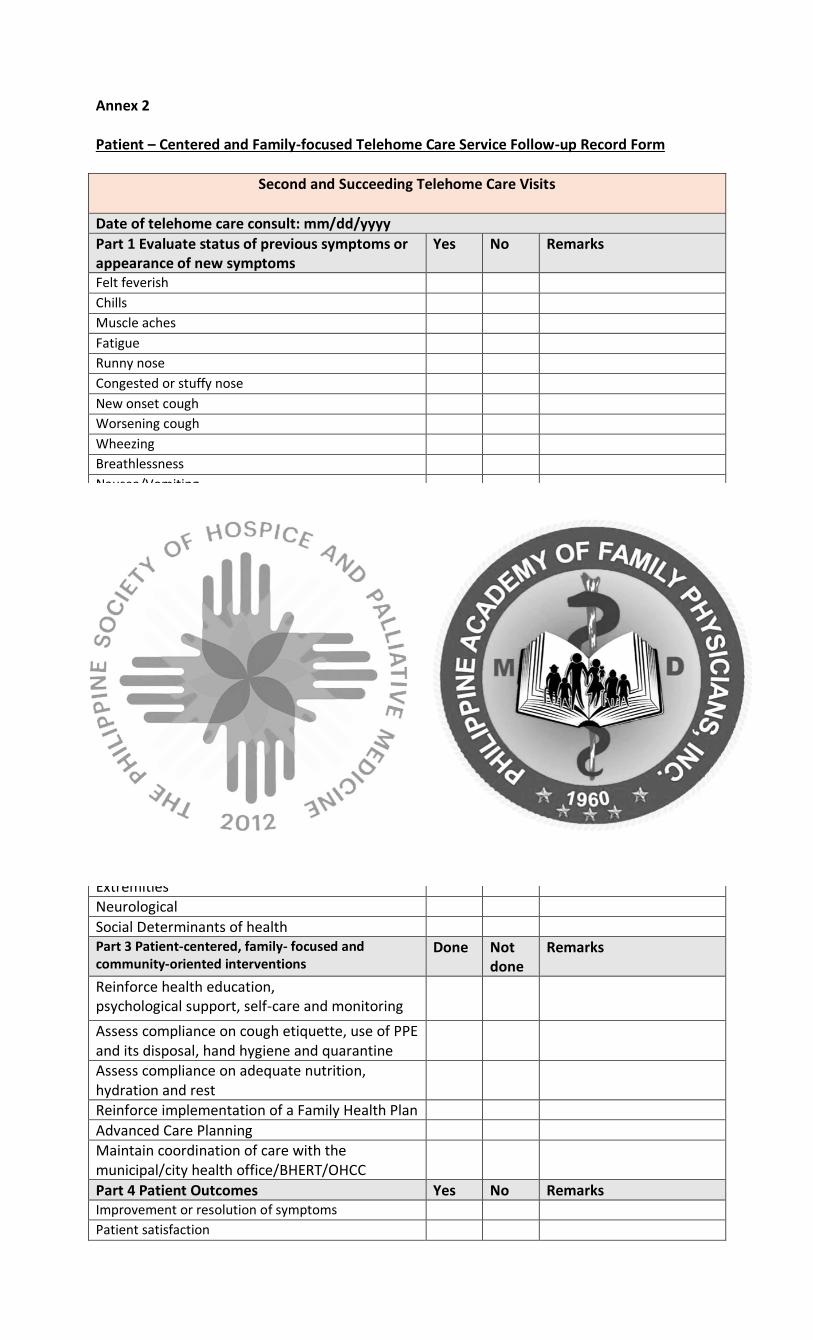
Annex 2 Patient – Centered and Family-focused Telehome Care Service Follow-up Record Form
Second and Succeeding Telehome Care Visits
Date of telehome care consult: mm/dd/yyyy
Part 1 Evaluate status of previous symptoms or appearance of new symptoms
Yes No Remarks
Felt feverish Chills Muscle aches Fatigue Runny nose Congested or stuffy nose New onset cough Worsening cough Wheezing Breathlessness Nausea/Vomiting Headache Abdominal Pain Chest pain Diarrhea Loss of appetite Loss of taste Loss of smell Others Are there family members experiencing the same symptoms?
Part 2 Clinical Evaluation Guide Done Not done
Remarks
Vital signs Skin assessment
Heads, Eyes, Ears, Nose and Throat Neck
Lungs
Heart Abdomen
Extremities Neurological
Social Determinants of health Part 3 Patient-centered, family- focused and community-oriented interventions
Done Not done
Remarks
Reinforce health education, psychological support, self-care and monitoring
Assess compliance on cough etiquette, use of PPE and its disposal, hand hygiene and quarantine
Assess compliance on adequate nutrition, hydration and rest
Reinforce implementation of a Family Health Plan
Advanced Care Planning
Maintain coordination of care with the municipal/city health office/BHERT/OHCC
Part 4 Patient Outcomes Yes No Remarks Improvement or resolution of symptoms Patient satisfaction
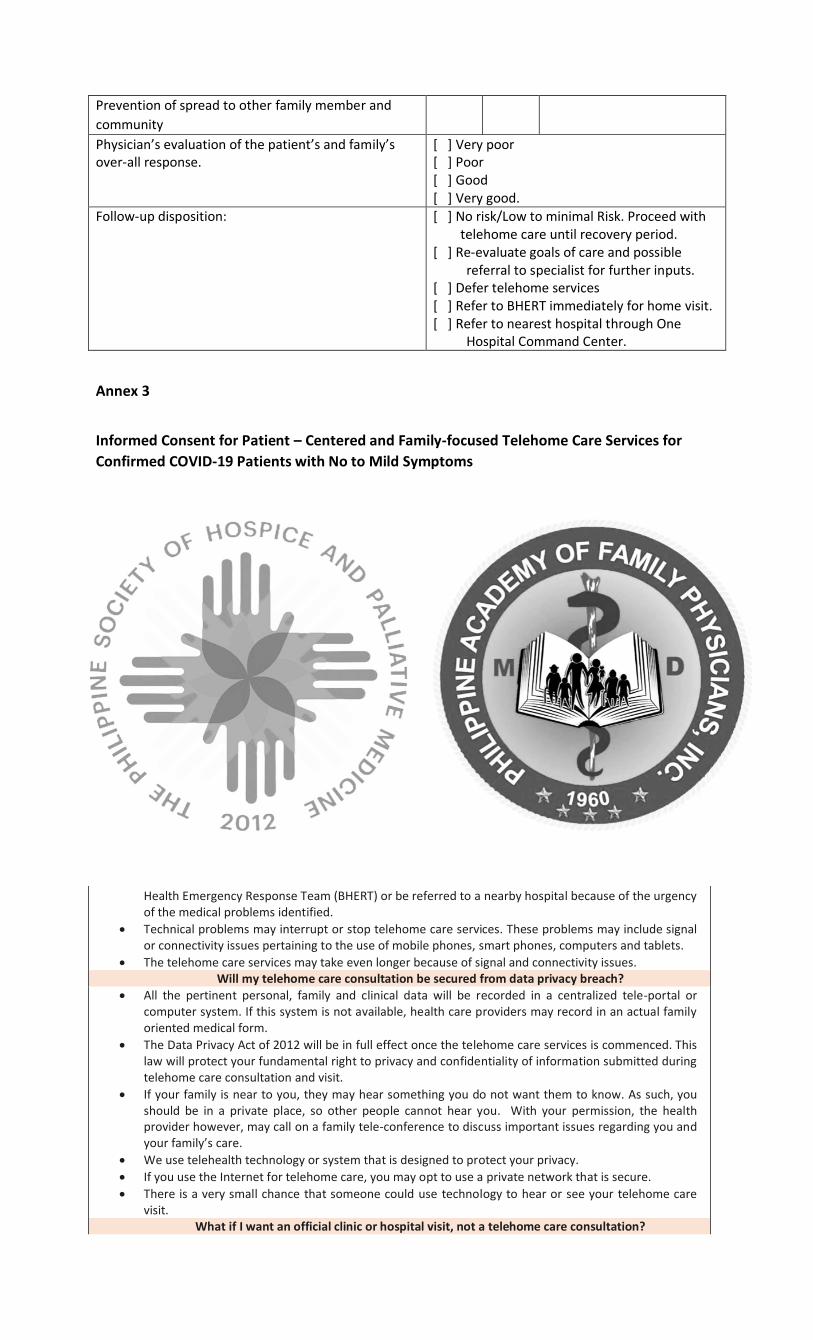
Prevention of spread to other family member and
community
Physician’s evaluation of the patient’s and family’s over-all response.
[ ] Very poor [ ] Poor [ ] Good [ ] Very good.
Follow-up disposition:
[ ] No risk/Low to minimal Risk. Proceed with telehome care until recovery period.
[ ] Re-evaluate goals of care and possible referral to specialist for further inputs.
[ ] Defer telehome services [ ] Refer to BHERT immediately for home visit. [ ] Refer to nearest hospital through One
Hospital Command Center.
Annex 3
Informed Consent for Patient – Centered and Family-focused Telehome Care Services for
Confirmed COVID-19 Patients with No to Mild Symptoms
*Note: Thes informed consent form may be modified and adapted based on your current practice setting and context. All
changes and adaptations should be communicated to the Philippine Academy of Family Physicians (PAFP) for consolidation of
best practices and documentation purposes through the PAFP secretariat using this email address: [email protected] or
Good day, [insert name of patient]. I am [insert name of physician], the physician in charge for this call. I will be facilitating the discussion about telehome care services. Please know that this conversation is recorded. Rest assured that all information will be treated in accordance to the Data Privacy Law.
What is telehome care?
• Telehome care is a way to provide services from healthcare providers, such as your doctor or nurse practitioner.
• You can talk to your doctor from home. You don’t go to a clinic or hospital unless if you have urgent medical reasons to do so.
How does telehome care help me?
• You don’t have to go to a clinic or hospital to see your doctor or any health provider.
• You won’t risk getting sick from other people especially during this pandemic. What are the disadvantages of telehomecare for me?
• You and your health care provider won’t be in the same room, so it may feel different than an actual clinic visit.
• Your health care provider may make a mistake because they cannot examine you closely compared to a clinic visit.
• We don’t know if mistakes are more common with telehome care.
• Your health care provider may decide if you still need an actual home care visit from the Barangay Health Emergency Response Team (BHERT) or be referred to a nearby hospital because of the urgency of the medical problems identified.
• Technical problems may interrupt or stop telehome care services. These problems may include signal or connectivity issues pertaining to the use of mobile phones, smart phones, computers and tablets.
• The telehome care services may take even longer because of signal and connectivity issues. Will my telehome care consultation be secured from data privacy breach?
• All the pertinent personal, family and clinical data will be recorded in a centralized tele-portal or computer system. If this system is not available, health care providers may record in an actual family oriented medical form.
• The Data Privacy Act of 2012 will be in full effect once the telehome care services is commenced. This law will protect your fundamental right to privacy and confidentiality of information submitted during telehome care consultation and visit.
• If your family is near to you, they may hear something you do not want them to know. As such, you should be in a private place, so other people cannot hear you. With your permission, the health provider however, may call on a family tele-conference to discuss important issues regarding you and your family’s care.
• We use telehealth technology or system that is designed to protect your privacy.
• If you use the Internet for telehome care, you may opt to use a private network that is secure.
• There is a very small chance that someone could use technology to hear or see your telehome care visit.
What if I want an official clinic or hospital visit, not a telehome care consultation?
• For now, almost all visits use the telehome care platform especially during the pandemic where people around you may need to be protected in order to limit or prevent transmission of the COVID-19 virus. You cannot schedule a hospital visit now, unless the following conditions are met:
o Urgent or emergent reasons o There are enough spaces for admission to a designated hospital or isolation facility. o You have completed the isolation period and have recovered from COVID-19 infection o Your family has completed the quarantine protocols.
What if I try the telehome care services and don’t like it?
• You can stop using telehealth at any time, even during a telehome care visit.
• You can still access or avail the telehome care services if you no longer want a telehealth visit.
• If you decide not to use telehome care services again, please contact the following numbers or access the following teleportal system:
o [insert contact numbers] o [insert tele-portal system]
How much does a telehealth visit cost?
• If the patient avails of the government services: o You need not pay anything since this is part of the services of your respective local
government unit represented by [insert name of institution/hospital/department/unit offering telehome care services].
o There is no payment should the doctor decide you need an actual home care visit in addition to telehome care consultation. In this situation, collaboration with the Barangay Health Emergency Response Team (BHERT) will be facilitated.
• If the patient avails of the private services o For private services, what you pay depends on the indicated professional fee or on the
insurance provided to you. You will be charged of [insert amount in Philippine Peso].You will need to coordinate with your insurance policy provider if telehome care services will be covered.
o You may be charged differently if the doctor decides you need an actual home care visit in addition to your telehome care consultation. You will be charged of [insert amount in Philippine Peso].
How do I proceed if I consent with the telehome care consultation?
• We need you to either sign this electronic document signifying consent to access telehome care services after all the details have been discussed to you.
• Do you want to proceed with the telehome care services? [Yes/No] What does it mean if I give my consent?
• If you signify your consent using the electronic record or verbally, you agree that: o We talked about the information in this document. o We answered all your questions. o You want telehome care services.
Do you have any questions or concerns?
• [Document questions or concerns]
We will give you a copy if you sign this document electronically using the portals biometrics and security features. You don’t need a witness to sign this electronic consent form.
________________________________________________________ ____________ Your name (electronic signature/biometrics and security recognition) Date

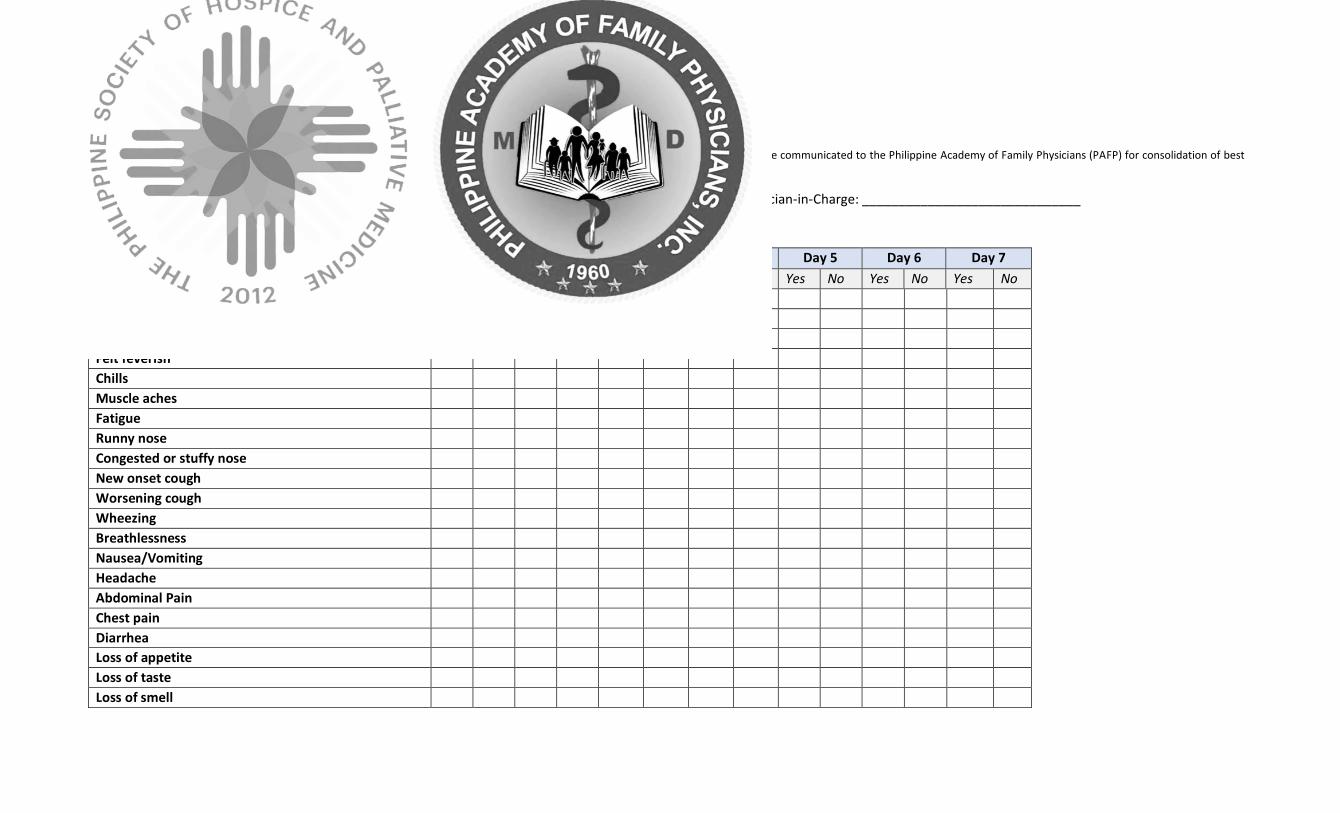
Annex 4
Daily monitoring of the index patient’s symptoms *Note: This form may be modified and adapted based on your current practice setting and context. All changes and adaptations should be communicated to the Philippine Academy of Family Physicians (PAFP) for consolidation of best
practices and documentation purposes through the PAFP secretariat using this email address: [email protected] or [email protected]
Name of Patient: ________________________________________________________ Tele-home Physician-in-Charge: ______________________________
Date of last potential exposure to the virus (day 0): ____________________________
Date to complete monitoring (14 days following last potential exposure): ___________
DATE (mm/dd/yy) Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7
Yes No Yes No Yes No Yes No Yes No Yes No Yes No
Medications taken today?
Temperature (morning) ⁰C
Temperature (evening) ⁰C
Felt feverish
Chills
Muscle aches
Fatigue
Runny nose
Congested or stuffy nose
New onset cough
Worsening cough
Wheezing
Breathlessness
Nausea/Vomiting
Headache
Abdominal Pain
Chest pain
Diarrhea
Loss of appetite
Loss of taste
Loss of smell
Others
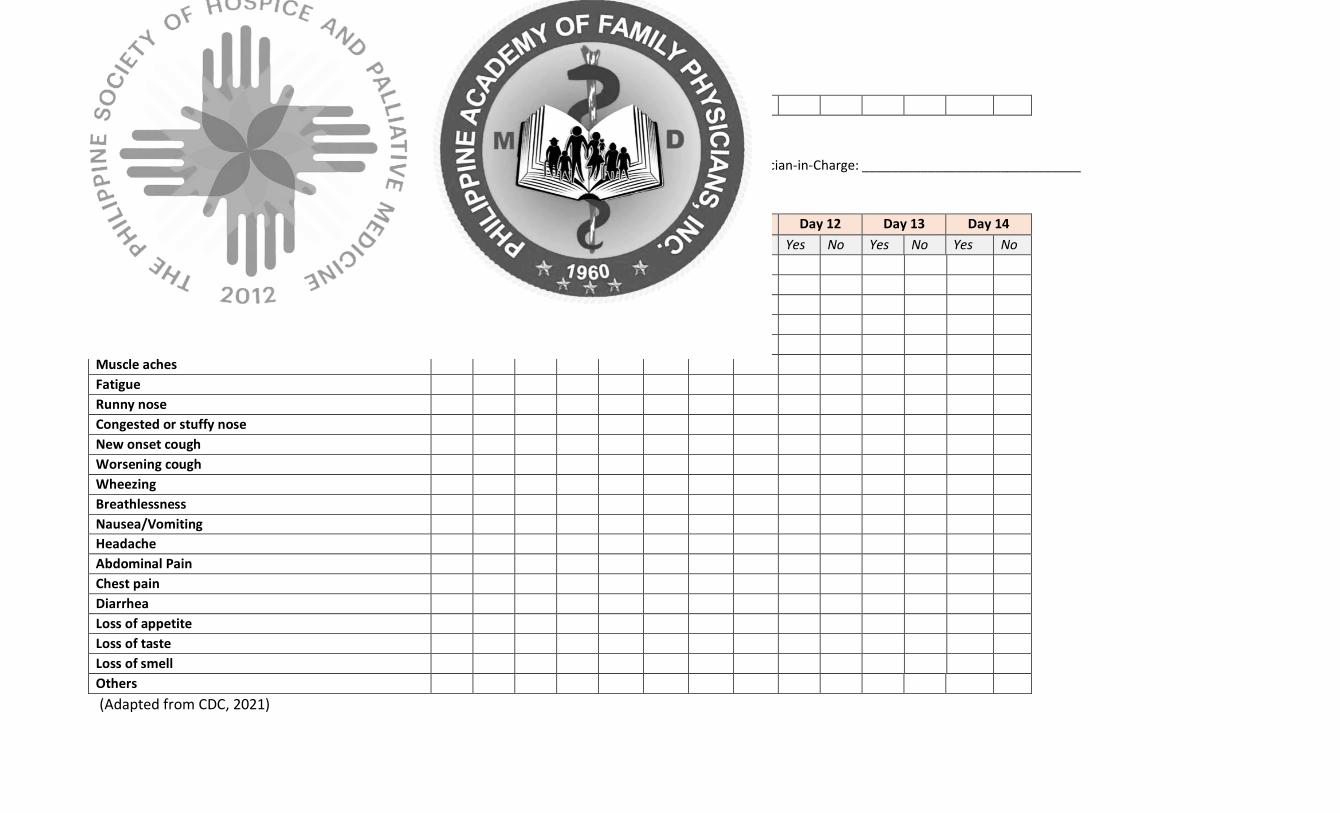
Daily monitoring of the index patient’s symptoms
Name of Patient: ________________________________________________________ Tele-home Physician-in-Charge: ______________________________
Date of last potential exposure to the virus (day 0): ____________________________
Date to complete monitoring (14 days following last potential exposure): ___________
DATE (mm/dd/yy) Day 8 Day 9 Day 10 Day 11 Day 12 Day 13 Day 14
Yes No Yes No Yes No Yes No Yes No Yes No Yes No
Medications taken today?
Temperature (morning) ⁰C
Temperature (evening) ⁰C
Felt feverish
Chills
Muscle aches
Fatigue
Runny nose
Congested or stuffy nose
New onset cough
Worsening cough
Wheezing
Breathlessness
Nausea/Vomiting
Headache
Abdominal Pain
Chest pain
Diarrhea
Loss of appetite
Loss of taste
Loss of smell
Others
(Adapted from CDC, 2021)
References
1. CDC. SARS-CoV-2 Variant Classifications and Definitions [Internet]. Cdc.gov. 2021 [cited 2021 May 01].
Available from: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/variant-surveillance/variant-
info.html
2. Different types of COVID-19 vaccines: How they work [Internet]. Mayoclinic.org. 2021 [cited 2021 May 15].
Available from: https://www.mayoclinic.org/diseases-conditions/coronavirus/in-depth/different-types-of-
covid-19-vaccines/art-20506465
3. Department of health [Internet]. Doh.gov.ph. 2021 [cited 2021 May 15]. Available from:
https://doh.gov.ph/2019-
nCoV?gclid=Cj0KCQjwgtWDBhDZARIsADEKwgNXTq9yMBFYQZMlkxhT2uTs5YIzTknfFjO51YL9Wi3nFi_y4ywvss8
aAl4iEALw_wcB
4. Republic of the Philippines Inter-agency Task Force For the Management of Emerging Infectious Diseases.
Resolution No. 106-A Series of 2021 [Internet]. 2021 Mar. Available from:
https://www.napocor.gov.ph/images/20210327-IATF-106-A-RRD.pdf
5. World Health Organization. Home care for patients with suspected or confirmed COVID-19 and
management of their contacts [Internet]. who.int. 2020 [cited 2021 May 15]. Available from:
https://www.who.int/publications/i/item/home-care-for-patients-with-suspected-novel-coronavirus-(ncov)-
infection-presenting-with-mild-symptoms-and-management-of-contacts
6. American Medical Association. Telehealth Visit Etiquette Checklist. In: Telehealth Implementation Playbook
[Internet]. 2020 Apr. Available from: https://www.ama-assn.org/system/files/2020-04/ama-telehealth-
playbook.pdf
7. Department of Health and University of the Philippines Manila. Telemedicine Practice Guidelines. Joint
Memorandum Circular, 2020;1:2-12.
8. Philippine Medical Association. Telemedicine for Health Professionals [Internet]. 2020 May. Available from:
https://www.philippinemedicalassociation.org/wp-content/uploads/2020/05/1-Telemedicine-for-Health-
Professionals.pdf
9. Hale TM and Kvedar JC. Privacy and Security Concerns in Telehealth. American Medical Association Journal
of Ethics, 2014; 16(12):981-985.
10. California Association of Marriage and Family Therapists. Checklist for Telehealth [Internet]. 2019 May.
Available from: https://www.camft.org/Portals/0/PDFs/articles/Checklist-for-Telehealth.pdf?ver=2019-05-
23-172903-570
11. Baumes A, Čolić M, and Araiba S. Comparison of Telehealth-Related Ethics and Guidelines and a Checklist
for Ethical Decision Making in the Midst of the COVID-19 Pandemic. Behavioral Analysis in Practice,
2020;13(4):736–747.
12. Chaet, D, Clearfield R, Sabin J, Skimming K, and Council on Ethical and Judicial Affairs American Medical
Association. Ethical practice in Telehealth and Telemedicine. Journal of General Internal Medicine,
2017;32(10):1136–1140.
13. Health Resources and Services Administration. Obtaining informed consent [Internet].
Telehealth.HHS.gov. 2021 [cited 2021 May 10]. Available from:
https://telehealth.hhs.gov/providers/preparing-patients-for-telehealth/obtaining-informed-consent/
14. Philippine Medical Association. Preparing for Teleconsultation: Guidance for Filipino Clinicians and Their
Patients [Internet]. 2020 May. Available from: https://www.philippinemedicalassociation.org/wp-
content/uploads/2020/05/3-Telemedicine-for-Patients.pdf
15. Telehealth policy 101 - CCHP [Internet]. Cchpca.org. 2021 [cited 2021 May 15]. Available from:
https://www.cchpca.org/policy-101/?category=informed-consent
16. Portnoy J, Waller M, and Elliott T. Telemedicine in the Era of COVID-19. The Journal of Allergy and Clinical
Immunology, 2020;8(5):1489–1491.
17. Reiss A, De Leon J, Dapkins I, Shahin G, Peltier M, and Goldberg E. Telemedicine in the Era of COVID-
19. Medicina, 2020;56(9):461.
18. Cruz MV, Policarpio Jr J, et al. Clinical Pathway for the Diagnosis and Management of Patients with COVID-
19 in Family Practice. 2020.
19. Gilboy N, Tanabe P, Travers D, and Rosenau A. Emergency Severity Index (ESI): Triage Tool For Emegerncy
Department Care Version 4 Implementation Handbook 2012 Edition. Agency for Healthcare Research and
Quality Publication, 2011;12(14):35-70.
20. Section 1: Patient navigation [Internet]. Psmid.org. Philippine Society of Microbiology and Infectious
Diseases; c2020 [cited 2021 Apr 29]. Available from: https://www.psmid.org/covid-algorithms-section-1-
patient-navigation/
21.PAFP Task Force on COVID. Community-Oriented Health Care During a COVID-19 Epidemic: A Consensus
Statement by the PAFP Task Force on COVID-19 [Internet]. 2020 Apr. Available from:
http://thepafp.org/website/wp-content/uploads/2018/09/PAFP-Consensus-Guidelines-on-Community-
oriented-Health-Care-In-COVID-19-1.pdf
22. Calton B, Abedini N, and Fratkin M. Telemedicine in the Time of Coronavirus. Journal of Pain and
Symptom Management, 2020;60(1):12–14.
23. Benziger CP, Huffman MD, Sweis RN, and Stone NJ. The Telehealth Ten: A Guide for a Patient-Assisted
Virtual Physical Examination. The American Journal of Medicine, 2021;134(1):48-51.
24. Prado G, Estrada Y, Rojas L, Bahamon M, Pantin H, Nagarsheth M, Gwynn L, Ofir A, Forster L, Torres N,
and Brown C. Rationale and design for eHealth Familias Unidas Primary Care: A drug use, sexual risk behavior,
and STI preventive intervention for hispanic youth in pediatric primary care clinics. Contemporary Clinical
Trials, 2019;76:64–71.
25. PAFP Task Force on COVID-19. Family-focused Home Care Plan During a COVID-19 Epidemic: A Consensus
Statement by the PAFP Task Force on COVID-19 [Internet]. 2020 Mar. Available from:
http://thepafp.org/website/wp-content/uploads/2018/09/PAFP-Consensus-Guidelines-on-Family-focused-
Care-In-CoViD-19-Epidemic_March-2020v.4-1.pdf
26. COVID-19 Clinical management: living guidance [Internet]. Who.int. World Health Organization; c2021
[cited 2021 May 15]. Available from: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-
2021-1
27. Office of the National Coordinator for Health Information Technology. Shared Decision Making Fact Sheet
[Internet]. healthit.gov. 2013 [cited 2021 May 1]. Available from:
https://www.healthit.gov/sites/default/files/nlc_shared_decision_making_fact_sheet.pdf
28. Section 4: Special Considerations [Internet]. Psmid.org. Philippine Society of Microbiology and Infectious
Diseases; c2020 [cited 2021 Jun 9]. Available from: https://www.psmid.org/covid-algorithms-section-2-
primary-care/
29. Stein-Zamir C, Abramson N, Edelstein N, Shoob H, Zentner G, and Zimmerman D. Community-Oriented
Epidemic Preparedness and Response to the Jerusalem 2018-2019 Measles Epidemic. American Journal of
Public Health, 2019;109(12):1714–1716.
30. Takahashi S, Sato K, Kusaka Y, and Hagihara A. Public preventive awareness and preventive behaviors
during a major influenza epidemic in Fukui, Japan. Journal of Infection and Public Health, 2017;10(5):637–
643.
31. DOH Launches One Hospital Command Center for Faster and More Efficient Covid-19 Case Referral
[Internet]. Gov.ph. [cited 2021 May 10]. Available from: https://doh.gov.ph/press-release/DOH-LAUNCHES-
ONE-HOSPITAL-COMMAND-CENTER-FOR-FASTER-AND-MORE-EFFICIENT-COVID-19-CASE-REFERRAL
32. Philippine Society of Hospice and Palliative Medicine and Hospice Philippines. Care for Palliative and
Bedridden Patients in Communities on Enhanced Community Quarantine [Internet]. 2020 Jun. Available from:
http://psphp.org/wp-content/uploads/2020/05/Part-1-Care-for-Palliative-and-Bedridden-Patients-in-
Communities-on-ECQ-Updated.pdf
33. DILG partners with DOH to Strengthen BHERTS’ Role in Ensuring Access to Public Healthcare Services
[Internet]. Gov.ph. [cited 2021 May 15]. Available from: https://doh.gov.ph/press-
release/DILG%20PARTNERS-WITH-DOH-TO-STRENGTHEN-BHERTS-ROLE-IN-ENSURING-ACCESS-TO-PUBLIC-
HEALTHCARE-SERVICES
34. CDC. Using telehealth to expand access to essential health services during the COVID-19 pandemic
[Internet]. Cdc.gov. 2021 [cited 2021 May 01]. Available from: https://www.cdc.gov/coronavirus/2019-
ncov/hcp/telehealth.html

35. Republic of the Philippines Department of the Interior and Local Government. Amended Guide to Action
Against the 2019 Novel Coronavirus Acute Respiratory Disease [Internet]. 2020. Available from:
https://dilg.gov.ph/PDF_File/issuances/memo_circulars/dilg-memocircular-202026_9dec468b19.pdf
36. Section 2: Primary Care [Internet]. Psmid.org. Philippine Society of Microbiology and Infectious Diseases;
c2020 [cited 2021 May 17]. Available from: https://www.psmid.org/covid-algorithms-section-2-primary-care/
37. CDC. Appendix 2: Monitoring Form Templates [Internet]. Cdc.gov. 2021 [cited 2021 Jun 09]. Available
from: https://www.cdc.gov/coronavirus/2019-ncov/downloads/appendix-2-monitoring-form-templates.pdf