paediatric public assessment report - hma.eu
TRANSCRIPT
Paediatric Public Assessment Report EU Worksharing Project
Zomig/Zomig Rapimelt/Zomig Nasal
(zolmitriptan)
Marketing Autorisation Holder: AstraZeneca
Date of this report: 19 December 2006
Rapporteur Sweden
Co-Rapporteur Holland
Currently approved indication
Acute treatment of migraine headache with or without aura
Pharmaceutical form affected by this variation
Film-coated tablets; orodispersible tablets; nasal spray solution
Strength(s) affected by this procedure
Zomig: 2,5 mg and 5 mg film-coated tablets
Zomig Rapimelt: 5 mg orodispersible tablets
Zomig Nasal: 2,5 mg/dose, 5 mg/dose

I. ABBREVIATIONS AE Adverse Event AUC Area under the curve AUC(0-t) Area under the plasma concentration-time curve to the last detected value CL Clearance CLR Renal clearance Cmax Maximum plasma concentration CYP1A2 Cytochrome P1A2 EU European Union FDA Food and Drug aAdministration ITT Intention to treat MAH Market Authorisation Holder MAO-A Monoamine oxidase-A MPA Medical Products Agency (Sweden) MR Mutual Recognition PK/PD Pharmacokinetics/Pharmacodynamics PP Per protocol SD Standard deviation SE Standard error SmPC Summary of Product Characteristics t1/2 Half-life tmax Time to maximum plasma concentration

II. RECOMMENDATION As a part of the EU work sharing project assessment of paediatric data of existing products, the MAH has submitted all available data in children and adolescents for Zomig. The submitted data on efficacy and safety concern studies in adolescents (12-17 years of age) whereas there are no data in children (below 12 years of age). Based on the clinical results available for assessment, it was concluded that an indication in the paediatric population or in adolescents is at present not approvable. Based on the review, the paediatric data should lead to an amendment of the currently approved SmPC text. The finally agreed changes to the SmPC are shown in section IV at the end of this assessment report.
II.1 Scope of the assessment The evaluation of efficacy and safety was based on the clinical studies which are shown in table 1. Table 1. Clinical studies included in the evaluation of Zolmitriptan used in the adolescent population Study code Age inclusion
(years) Zomig Formulation
Outcome
311CGW/0015 (136-015)
18-651 Oral tablets Efficacy, safety
311CGW/0017 (136-017)
12-65 Oral tablets Efficacy, safety
311CGW/0018 (136-018)
18-651 Oral tablets Efficacy, safety
311CGW/0042 (136-042)
12-65 Oral tablets Efficacy, safety
311CIL/0043 (136-043)
12-70 Oral tablets
Efficay, safety
311CIL/0070
18-651 Oral tablets
Efficacy, safety
311CIL/0092
12-17 (for adolescents) 18-65 (for adults)
Oral tablets PK, tolerability
311CIL/0099
18-651 Oral tablets Efficacy, safety
311CUS/0005 12-17 Oral tablets Efficacy, safety
311CUS/0007 12-17 Oral tablets Safety D1221C00004 12-17 (for adolescents)
>18 (for adults) Nasal Spray PK
D1221C00005 This study is not included in the overall evaluation, since it was not finalised at the time of submission
12-17 Nasal Spray Efficacy, safety
1 Subjects <18 years were excluded from the study therefore the appearance of adolescents within this trial represented a protocol violation.

III. SCIENTIFIC DISCUSSION
III.1 Quality aspects Not applicable
III.2 Non-clinical aspects Not applicable III.3 Clinical aspects
III.3.1 Clinical pharmacology
Background information Zolmitriptan is an intermediate clearance drug (CL = 12 ml/min/kg), of which 75 % is eliminated by metabolism and 25% by renal excretion of unchanged drug (CLR = 200 ml/min). The inter-individual variability of AUC after oral administration is approximately 50% (CV). The absolute bioavailability is approximately 40%. Zolmitriptan is metabolised by CYP1A2, forming an active metabolite, N-desmethylzolmitriptan (183C91). The active metabolite is then further metabolised through MAO-A. The active metabolite, which is 2-6 times as active as the parent drug reaches approximately 50% of the zolmitriptan AUC. The zolmitriptan plasma protein binding is 27%. The plasma protein binding of the active metabolite N-desmethyl-zolmitriptan is approximately the same, 20-25%. The elimination half-life for both zolmitriptan and N-desmethyl-zolmitriptan was approximately 2.5 hours, indicating that elimination of N-desmethyl-zolmitriptan is formation rate limited. AUCs for zolmitriptan and N-desmethyl-zolmitriptan are decreased in patients during a migraine attack by approximately 40%. There is an effect of gender, in that men have a 40-50% lower zolmitriptan AUC when compared with women, but this is not accompanied by a difference in efficacy. Submitted studies The MAH has performed two studies comparing the pharmacokinetics of zolmitriptan and its active metabolite in adults and adolescents. One study was performed using the film-coated tablet (oral) formulation (311CIL/0092) and one study used the nasal spray formulation (D1221C00004). Zolmitriptan film-coated tablets (Study 311CIL/0092) The pharmacokinetic profile was compared after a 5 mg single dose (two 2.5 mg tablets) in 18 adult (18-65 yrs, mean 39.1±12.9 ) and 21 pubertal adolescent (12-17 yrs, mean 14.5±1.5) healthy volunteers. The adolescent and adults groups contained 62 and 67% females, respectively. Plasma samples for assay of zolmitriptan and its metabolite, 183C91, were obtained at predetermined intervals for 15 hours post-dose. The results are presented in tables 2-5. Table 2 Plasma pharmacokinetic parameters for zolmitriptan after a single dose
Subject group Cmax (ng/ml) tmax (h) AUC
(ng.h/ml) AUC(0-t) (ng.h/ml) t½ (h)
n Mean SE Median (range) Mean SE Mean SE Mean SE Adolescents 21 9.66 0.87 1.5 (0.5-4.0) 51.4 4.0 49.7 3.8 3.01 0.16

Female 13 11.11 0.95 1.0 (0.5-4.0) 60.3 3.4 58.1 3.3 2.98 0.16 Male 8 7.31 1.36 2.3 (0.5-3.0) 37.0 6.1 35.9 6.1 3.05 0.35 Adults 18 8.58 0.60 1.0 (0.5-4.0) 46.3 4.1 43.7 3.8 3.75 0.22 Female 12 9.08 0.69 1.3 (0.5-4.0) 48.6 4.4 45.7 4.1 3.97 0.27 Male 6 7.57 1.12 1.0 (1.0-2.0) 41.9 9.0 39.6 8.5 3.29 0.33 Table 3 Pharmacokinetic parameters of zolmitriptan: geometric mean ratio of value for adolescents to value for adults
Parameter Adolescents Adults Ratio of geometric 90%CI for ratio (geometric mean) (geometric mean) means
Cmax(ng/ml) 8.9 8.2 1.09 0.89 to 1.33 AUC (ng.h/ml) 47.8 42.7 1.12 0.89 to 1.40 AUC(0-t) (ng.h/ml) 46.1 40.3 1.15 0.91 to 1.43 Table 4 Plasma pharmacokinetic parameters for 183C91 after a single dose of
zolmitriptan
Subject group
Cmax (ng/ml) tmax (h) AUC
(ng.h/ml) AUC(0-t) (ng.h/ml) t½ (h)
n Mean SE Median (range) Mean SE Mean SE Mean SE
Adolescents 21 5.32 0.50 3.0 (1.0-5.0) 29.6 1.9 28.3 1.9 3.01 0.17 Female 13 5.51 0.62 2.5 (1.0-4.0) 30.9 2.0 29.7 2.0 2.95 0.20 Male 8 4.99 0.90 3.0 (2.0-5.0) 27.4 4.0 26.1 4.0 3.11 0.33 Adults 18 3.59 0.15 2.5 (1.0-4.0) 21.5 1.4 19.6 1.2 3.05 0.27 Female 12 3.75 0.16 2.5 (1.0-4.0) 22.0 1.6 19.9 1.3 3.18 0.37 Male 6 3.26 0.26 2.5 (2.0-4.0) 20.8 2.6 19.0 2.4 2.83 0.41 Table 5 Pharmacokinetic parameters of 183C91: geometric mean ratio of value for adolescents to value for adults
Parameter Adolescents Adults Ratio of geometric 90%CI for ratio (geometric mean) (geometric mean) means Cmax(ng/ml) 4.9 3.5 1.39 1.17 to 1.65 AUC (ng.h/ml) 28.2 20.8 1.36 1.15 to 1.60 AUC (0-t) (ng.h/ml) 26.9 19.0 1.42 1.20 to 1.67

Assessors comment: Mean values for Cmax, AUC, and AUC(0-t) of the active metabolite (183C91) were 40% to 50% greater for adolescents than for adults. However, these differences were not judged to be clinically significant. The AUC and Cmax of the parent drug (zolmitriptan), was similar in adolescents and in adults. Zolmitriptan nasal spray (Study D1221C00004) The pharmacokinetic profile of 5 mg zolmitriptan as nasal spray was investigated in 15 adult (>18 yrs, mean 39.1±13.6yrs) and 15 adolescent (12-17 yrs, mean 14.4±1.6yrs) subjects with a history of migraine. Of the patients, there were 53 and 47% females in the adult and adolescent group, respectively. The patients were excluded if they had an attack of migraine on the dosing days. The results of the studies are presented in tables 6 and 7 below.
Table 6 Selected pharmacokinetic parameters of zolmitriptan in evaluable subjects following a single intranasal dose of 5.0-mg zolmitriptan, in adolescents and adults
Adolescent Adult Ratio (Adolescent/Adult)
95% CI 95% CI 90% CI
Parameter Gender N
Geometric Means Ratio
(Lower, upper limit)
N
Geometric Means Ratio
(Lower, upper limit)
Geometric Mean (Lower, upper limit)
AUC(hr*ng/mL) All 15 40.9 (30.6, 55.6) 15 46.9 (34.5,
63.9) 0.87 (0.61, 1.25)
Female 7 48.2 (29.9, 77.9) 8 49.5 (31.6,
77.4) 0.98 (0.57, 1.67)
Male 8 34.9 (22.2, 54.9) 7 44.9 (27.6,
72.9) 0.78 (0.45, 1.34)
Cmax(ng/mL) All 15 6.2 (4.7, 8.2) 15 6.4 (4.9, 8.5) 0.97 (0.70, 1.34) Female 7 7.7 (5.2, 11.5) 8 7.1 (4.9,
10.3) 1.09 (0.69, 1.71)
Male 8 5.0 (3.3, 7.7) 7 5.9 (3.7, 9.3) 0.86 (0.51, 1.43)
Gender N
Arithmetic Mean or median
(minimum and maximum)
N
Arithmetic Mean or median
(minimum and
maximum)
tmax (h) All 15 2.0 (0.3, 4.0) 15 2.0 (1.0, 4.0) Female 7 4.0 (0.50, 4.0) 8 2.0 (1.0, 4.0) Male 8 2.0 (0.3, 4.0) 7 2.0 (1.0, 4.0) t1/2(h) All 15 3.0 (1.0, 4.8) 15 3.8 (2.2, 5.5) Female 7 3.0 (2.2, 3.8) 8 3.6 (2.2, 5.2) Male 8 3.0 (1.0, 4.8) 7 4.1 (2.7, 5.5)
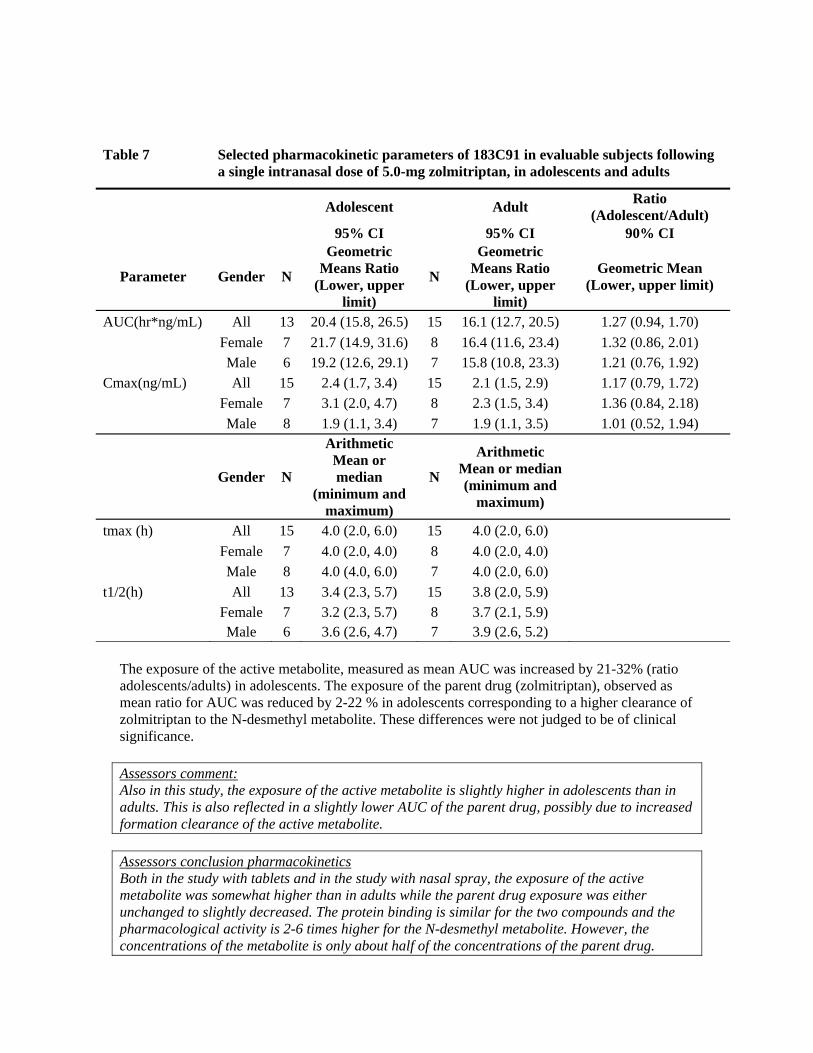
Table 7 Selected pharmacokinetic parameters of 183C91 in evaluable subjects following a single intranasal dose of 5.0-mg zolmitriptan, in adolescents and adults
Adolescent Adult Ratio (Adolescent/Adult)
95% CI 95% CI 90% CI
Parameter Gender N
Geometric Means Ratio
(Lower, upper limit)
N
Geometric Means Ratio
(Lower, upper limit)
Geometric Mean (Lower, upper limit)
AUC(hr*ng/mL) All 13 20.4 (15.8, 26.5) 15 16.1 (12.7, 20.5) 1.27 (0.94, 1.70) Female 7 21.7 (14.9, 31.6) 8 16.4 (11.6, 23.4) 1.32 (0.86, 2.01) Male 6 19.2 (12.6, 29.1) 7 15.8 (10.8, 23.3) 1.21 (0.76, 1.92) Cmax(ng/mL) All 15 2.4 (1.7, 3.4) 15 2.1 (1.5, 2.9) 1.17 (0.79, 1.72) Female 7 3.1 (2.0, 4.7) 8 2.3 (1.5, 3.4) 1.36 (0.84, 2.18) Male 8 1.9 (1.1, 3.4) 7 1.9 (1.1, 3.5) 1.01 (0.52, 1.94)
Gender N
Arithmetic Mean or median
(minimum and maximum)
N
Arithmetic Mean or median (minimum and
maximum)
tmax (h) All 15 4.0 (2.0, 6.0) 15 4.0 (2.0, 6.0) Female 7 4.0 (2.0, 4.0) 8 4.0 (2.0, 4.0) Male 8 4.0 (4.0, 6.0) 7 4.0 (2.0, 6.0) t1/2(h) All 13 3.4 (2.3, 5.7) 15 3.8 (2.0, 5.9) Female 7 3.2 (2.3, 5.7) 8 3.7 (2.1, 5.9) Male 6 3.6 (2.6, 4.7) 7 3.9 (2.6, 5.2)
The exposure of the active metabolite, measured as mean AUC was increased by 21-32% (ratio adolescents/adults) in adolescents. The exposure of the parent drug (zolmitriptan), observed as mean ratio for AUC was reduced by 2-22 % in adolescents corresponding to a higher clearance of zolmitriptan to the N-desmethyl metabolite. These differences were not judged to be of clinical significance. Assessors comment: Also in this study, the exposure of the active metabolite is slightly higher in adolescents than in adults. This is also reflected in a slightly lower AUC of the parent drug, possibly due to increased formation clearance of the active metabolite. Assessors conclusion pharmacokinetics Both in the study with tablets and in the study with nasal spray, the exposure of the active metabolite was somewhat higher than in adults while the parent drug exposure was either unchanged to slightly decreased. The protein binding is similar for the two compounds and the pharmacological activity is 2-6 times higher for the N-desmethyl metabolite. However, the concentrations of the metabolite is only about half of the concentrations of the parent drug.

For comparison, in the original assessment for Zomig 2.5 and 5 mg tablets, submitted studies showed that the exposure of zolmitriptan was almost doubled in women as compared to men and that the N-desmethyl metabolite to drug AUC0-∞ ratio was statistically significantly 70 and 30% higher in men after the 10 and 15 mg dose, respectively (09/IF/1023461), The differences in exposures were judged to lack clinical relevance. Hence, if the PK-PD relationship would be similar in adults and adolescents, we would expect the clinical efficacy to be similar in adults and adolescents Request for supplementary information
No further information requested from the MAH.
III.3.2 Clinical efficacy
Submitted studies
The MAH has performed one randomised, placebo-controlled clinical efficacy study (Trial 311CUS/0005) using Zomig tablets in adolescents with migraine. In addition, the MAH has submitted preliminary results for a randomised, controlled crossover study (D1221C00005) comparing Zomig Nasal Spray to placebo in adolescents.
Zolmitriptan film-coated tablets (Study 311CUS/0005) A phase II multi-centre outpatient study designed to evaluate safety and efficacy of oral administration of zolmitriptan in the acute treatment of migraine headache in adolescent patients. In phase I of the study, patients were randomised to treat a single migraine headache with 2.5 mg, 5 mg or 10 mg zolmitriptan or placebo. In the Phase II, open-label portion of the study, patients treated multiple migraine headaches over a 12-month period with 5.0 mg zolmitriptan (tablet form). A second 5.0 mg tablet was allowed in Phase II, if necessary, between 2 hours and 24 hours after the 1st dose of study treatment. Male and female patients aged between 12 and 17 years (inclusive), with a minimum of 2 migraines per month (according to International Headache Society [IHS]-defined criteria) and a maximum of 10 migraine headaches or nonmigraine headaches each month were eligible for inclusion in Phase I. Patients who completed Phase I of the study were eligible for inclusion in Phase II of the study. After the completion of Phase I and an analysis of Phase I data, a decision was made by the company to discontinue Phase II of the study. This decision was based on the fact that Phase I treatment of adolescents migraineurs with zolmitriptan failed to differentiate from placebo treatment for the primary efficacy variable and also because considerable safety data had already been collected on Phase II patients. In discussion with the FDA (teleconference on 15 August 2002) the agency supported the decision to stop the study. Efficacy variables Phase I • Primary variable: 4-point scale headache response at 2 hours • Secondary variables: Secondary variables included measurement of 4-point scale headache
response at 30 minutes and 1 hour; visual analog scale (VAS) headache response; 4-point scale painfree migraine headache relief; VAS change from baseline in headache intensity and proportion of patients with migraine-associated symptoms at 30 minutes, 1 hour and 2 hours;

use of escape medication and time to first use; migraine recurrence and time to migraine recurrence; and number and percent of patients who slept including time and duration.
Phase II Efficacy was not a primary objective of Phase II; however, data was collected and summarized for the majority of the primary and secondary efficacy variables listed above for Phase I. Demographics The 850 patients who entered Phase I were equally distributed among treatment groups with evenly matched demographic (Table 8) and baseline migraine-related characteristics. Across all treatment groups there was a higher percentage of patients aged 12 to 14 years and of female adolescents. The majority of patients were White. The percentage of patients completing the study and who were withdrawn due to adverse events (less than 1.0% for all zolmitriptan groups and none for placebo) was similar. 696 patients were evaluated for efficacy (whereas 699 were evaluable for safety). Concomitant medication (Phase II) During Phase II, 555 (92.0%) of patients in the safety population took a wide variety of concomitant medications. The most common concomitant medications were ibuprofen (38.0%), paracetamol (30.3%), sumatriptan (14.6%), and aspirin plus caffeine plus paracetamol (14.1%). Table 8. Demographic characteristics Study 311CUS/0005

Efficacy results Primary variable: For the primary efficacy variable (headache response at 2 hours) no statistically significant differences between 10.0 mg zolmitriptan and placebo were achieved at the alpha=0.05 level for the ITT population. The 2-hour headache response for the 10.0 mg zolmitriptan treatment group was 54.3% compared with 57.5% for placebo. Because a step down approach was taken to control the overall Type I error rate at 5.0 %, no analyses for statistical significance were done on the 5.0 mg and 2.5 mg zolmitriptan treatment groups for comparison with placebo. Results from the PP analysis on the primary variable were similar to those from the ITT analysis. Interactions for treatment by baseline intensity, and treatment by region interactions were assessed; however, these were not statistically or qualitatively significant and thus not considered for the final model. Secondary efficacy variables (phase I): No statistically significant improvement in efficacy for 10.0 mg zolmitriptan over placebo was demonstrated for any secondary efficacy variable analyzed in Phase I of the study. Table 9 provides results for 3 secondary efficacy variables at the 10.0 mg zolmitriptan dose compared with placebo. Table 9. Results for secondary efficacy variables in study 311CUS/0005
Z Tc
Assessor’s comment: There was no statistically significant difference in favour of oral zolmitriptan for the primary or any of the secondary efficacy variables. For headache response at 30 minutes and 1 hour, there was even a trend for better result with placebo.
olmitriptan nasal spray (Study D1221C00005)
he MAH has just completed a randomised, controlled, crossover study (D1221C00005) omparing Zomig Nasal Spray to placebo in adolescents. As a result of the findings from the

tablet study, the new study had an earlier time point as the primary endpoint (1 hour Headache Response), plus a second co-primary endpoint of 2 hour sustained response. In an attempt to reduce the placebo response in this study, this study used a single (patient) blind placebo challenge technique for each attack, where patients who responded to the placebo challenge at 15 minutes post dose received no further (randomised) treatment. Analysis of the results of study D1221C00005 is currently ongoing. The preliminary results indicate that zolmitriptan nasal spray has significantly higher headache response than placebo after one hour (58.1% vs. 43.3%; p<0.02) and that a significant treatment effect was seen as early as 15 minutes after administration (37.2% vs. 22.8%; p<0.02). Results also show that the sustained headache response at two hours was significantly higher with zolmitriptan nasal spray than with placebo (51.4% vs. 33.1%; p<0.01). The MAH states that following completion of the D1221C00005 clinical study report, the MAH will update the SmPC wording for Zomig. Assessor´s comment: Analysis of the results of this study is currently ongoing. The results for the completed study should be awaited.
Request for supplementary information and assessment of information provided
1. No statistically significant differences between the treatment arms were observed for the primary endpoint or any secondary efficacy variable analysed in study 311CUS/0005. However the placebo response after 30 minutes and after 1 hour is much better than the response in the active treatment arms. An explanation for these unexpected results is lacking. The company should comment.
Assessment of the MAH’s response The failure of the study to show efficacy is not unexpected given the experience of previous migraine studies with triptans, performed in adolescents. Also the high placebo response was not unexpected. What was unexpected, however, was that the response was highly in favour of placebo as compared to the active compound. This was not commented upon. The explanation put forward for the high placebo response rate is rather speculative. The reasons mentioned hold for both the placebo and active treatment group. As study 311CUS/0005 I is a randomised placebo-controlled trial and these factors are ’randomised’ response in both study arms is equally influenced by these psychological factors. Therefore, it is questioned whether the high placebo response should be considered responsible for study failure. In fact, the high placebo response is indicative for a deeper underlying explanation e.g. migraine is different in adolescents as compared to adults, the study design/conduct may have included a too heterogeneous patient population etc. Of note the remark that adolescents tend to have shorter duration migraine headaches than adults recently has been challenged by the new studies of migraine in adolescents. Considering the points above this poses the question whether zolmitriptan tablets should be prescribed to adolescents at all.

III.3.3 Clinical safety
Background In 2004, the company performed an extensive review concerning the use of Zomig in children and adolescents. The review included adverse event data from 11 clinical studies (see Table 1), and case reports from Clintrace, the global drug safety database of AstraZeneca. In this review, a total of 1172 subjects below 18 years of age had been treated with oral zolmitriptan (1 mg (n=3), 2.5 mg (n=253), 5.0 mg (n=713) , 10 mg (n=203)) and 15 subjects below 18 years of age had been treated with a single dose of nasal zolmitriptan 5.0 mg. The most commonly reported adverse events (>1%) in patients below 18 years of age were consistent with the current label for zolmitriptan in adults except for the adverse event with the preferred terms Abdominal pain, Headache, Vasodilation, Tremor, Pharyngitis and Sinusitis. The following differences were observed between the frequency seen in adolescents and adults. ‘Abdominal pain’ was reported in 1.2%, 1.1% and 3.0% of subjects treated with zolmitriptan 2.5 mg, 5.0 mg and 10 mg respectively. ‘Abdominal pain’ is a known adverse reaction seen in zolmitriptan use in adults, however labelled as ‘Very rare’ (<0.01%). ‘Headache’ was reported in 4.3%, 4.9% and 3.5% of subjects treated with zolmitriptan.5 mg, 5.0 mg and 10 mg respectively. ‘Headache’ is also a known adverse reaction seen in zolmitriptan use in adults, but is labelled as ‘Rare’ (<0.01-<0.1%). ‘Vasodilatation’, ‘Tremor’, ‘Pharyngitis’, and ‘Sinusitis’ are not listed adverse events for zolmitritpan use in adults. However, all 4 of these events have been reported following the use of zolmitriptan in clinical trials in adults. Submitted studies The applicant has included data from 11 clinical trials. Of these, four were studies where subjects aged less than 18 were specifically excluded (311CGW/0015, 311CGW/0018, 311CIL/0070, 311CIL0099), and the participating adolescents thus represent protocol violations. Two studies were pharmacokinetic studies (311CIL/0092, D1221C00004). The most important studies where safety was evaluated were studies 311CUS/0007 and 311CUS/0005. In addition, the preliminary safety data from study D1221C00005 have been evaluated, although the final report of this study was not available at the time of submission. The data from these 3 studies are presented in more detail below. Zolmitriptan film-coated tablets (Study 311CUS/0007) This trial was a double-blind, randomised, placebo-controlled 4 parallel group trial in healthy adolescent subjects with or without history of migraine headache. The primary measures were the incidence and severity of treatment-emergent adverse events that occurred with in 24 hours after administration of trial treatment. Demography A total of 84 subjects from 6 centres were randomized to receive a single oral dose of placebo or 2.5-mg, 5-mg, or 10-mg zolmitriptan (21 subjects per group). All subjects completed the trial. The mean age of subjects was 14.8 years (range 12 to 17 years); 64% (54 of 84) of subjects were male and 66% (55 of 84) were white. Demographic characteristics were similar for the 4 treatment groups.

Dosage and administration of trial treatment Each subject was randomized to 1 of the following 4 treatments:
• Placebo: 1 x 2.5-mg placebo tablet and 2 x 5-mg placebo tablets • 2.5-mg zolmitriptan: 1 x 2.5-mg zolmitriptan tablet and 2 x 5-mg placebo tablets • 5-mg zolmitriptan: 1 x 2.5-mg placebo tablet, 1 x 5-mg placebo tablet, and 1 x 5-mg
zolmitriptan tablet • 10-mg zolmitriptan: 1 x 2.5-mg placebo tablet and 2 x 5-mg zolmitriptan tablets
Each subject received a single dose of trial medication, consisting of 3 tablets as described above. Safety results Safety evaluations included adverse events, clinical laboratory tests, electrocardiographic (Holter monitoring), and physical examination and vital signs assessments. All subjects who received trial medication were evaluated for safety. Table 10 presents an overview of adverse events that occurred during the trial. Table 10. Overview of adverse events in Study 311CUS/0007
The incidence of subjects who had 1 or more adverse event was higher in the 5-mg and 10-mg zolmitriptan groups (71.4% and 66.7%, respectively) than in either the placebo group (28.6%) or the 2.5-mg zolmitriptan group (38.1%). There were no serious adverse events, withdrawals due to adverse events, or deaths during the trial. Across all treatment groups, the most common adverse event was headache, reported by 2 (9.5%) subjects in the placebo group, 6 (28.6%) in the 2.5-mg zolmitriptan group, 4 (19.0%) in the 5-mg zolmitriptan group, and 5 (23.8%) in the 10-mg zolmitriptan group (Table 11). Other commonly reported adverse events were nausea, a sensation of tightness (in the head, neck, jaw, throat, or shoulder), somnolence, and dizziness. Dizziness occurred only in the 5- and 10-mg zolmitriptan groups. The incidence of nausea and somnolence were higher in the 10-mg zolmitriptan group compared to the placebo group as well as the lower dose groups. The incidence of tightness was higher in the 5-mg zolmitriptan group than in all other groups. Table 11. Adverse events reported by more than 1 subject in any treatment group, by body system

Five (5%) adverse events were recorded to have an intensity of severe: thirst (placebo), tightness (2.5-mg zolmitriptan), somnolence (2.5-mg zolmitriptan), and headache (2.5-mg and 10-mg zolmitriptan). No deaths occurred during the trial or within 7 days after administration of trial medication. No subject was withdrawn from the trial because of an adverse event. No serious adverse events occurred during the trial or within 7 days after administration of trial medication. Electrocardiographic data All subjects had 12-lead ECGs performed at screening. All screening ECGs were considered normal by the investigator or, if abnormal, to be not clinically significant. Three ECGs were considered unevaluable by a central cardiologist because the length of the recording was insufficient. All subjects had ambulatory ECG monitoring (Holter monitoring) performed from approximately 30 minutes before to 24 hours after trial treatment administration. Holter monitoring data from 1 subject in the placebo group were lost; all other Holter monitoring data were read by a central cardiologist. A total of 13 subjects had potential events of ST segment depression recorded during Holter monitoring: 4 in the placebo group, 1 given 2.5-mg zolmitriptan, 2 given 5-mg zolmitriptan and 6 given 10-mg zolmitriptan. The central cardiologist considered the findings to be compatible with tachycardia in 11 of the 13 subjects; the remaining 2 subjects (Subject 0002/0025, 5-mg zolmitriptan and Subject 0002/0083, 10-mg zolmitriptan) were considered to have ST segment changes of undetermined significance. Further evaluation of Holter monitor recordings from all 13 subjects by an independent paediatric cardiologist determined that the findings in the latter 2 subjects were of undetermined significance, not ischemic in nature, and probably related to early repolarization. The paediatric cardiologist’s reading of the recordings from the 11 other subjects agreed with the earlier interpretation that the recordings were compatible with tachycardia. None of the 13 subjects had symptoms suggestive of an ischemic heart event. No clinically significant changes in chemistry, hematology, urinalysis, or vital signs were reported.
Assessors comment: The number of subjects in each dose group was low. The incidence of headache was considerably higher in this study than has been reported in previous studies in adults. A total of 13 subjects had potential events of ST segment depression, but further evaluation did not indicate that the cause of any of these events was ischemic in nature.

Zolmitriptan film-coated tablets (Study 311CUS/0005) The design of this study was discussed in the efficacy section of this assessment report. The study was divided in Phase I and Phase II. In Phase I of the study, patients were randomised to treat a single migraine headache with 2.5 mg, 5 mg or 10 mg zolmitriptan or placebo. In the Phase II, open-label portion of the study, patients treated multiple migraine headaches over a 12-month period with 5.0 mg zolmitriptan (tablet form). A second 5.0 mg tablet was allowed in Phase II, if necessary, between 2 hours and 24 hours after the 1st dose of study treatment. Male and female patients aged between 12 and 17 years (inclusive), with a minimum of 2 migraines per month (according to International Headache Society-defined criteria) and a maximum of 10 migraine headaches or non-migraine headaches each month were eligible for inclusion in Phase I. Patients who completed Phase I of the study were eligible for inclusion in Phase II of the study. After the completion of Phase I and an analysis of Phase I data, a decision was made by the company to discontinue Phase II of the study. This decision was based on the fact that Phase I treatment of adolescents migrant with zolmitriptan failed to differentiate from placebo treatment for the primary efficacy variable and also because considerable safety data had already been collected on Phase II patients. In discussion with the FDA (teleconference on 15 August 2002) the agency supported the decision to stop the study. Phase I of the study In Phase I, zolmitriptan tablets were taken at a dose of 10 mg, 5 mg or 2.5 mg. In Phase I of the study, 77.7% to 86.0% of patients in the ITT population took 3 study medication tablets. The highest rate of treatment compliance (86.0%) for patients taking 3 tablets was recorded for the 5.0 mg zolmitriptan treatment group. Less than 0.6% of patients in all treatment groups took 1 tablet of study medication and data was missing for the remaining participating patients in all groups. The percentage of patients with at least 1 adverse event over the course of the study was higher in all zolmitriptan groups (173 patients, 33.1 %) compared with placebo (22 patients, 12.5 %). The incidence of adverse events was higher in the 10 mg group (44.4 %) than for the 5 mg (25.9 %) or 2.5 mg (28.7 %) doses. The most frequent adverse events by COSTART term were tightness, dizziness, nausea, paresthesia, asthenia and pain. All of these events occurred in a higher percentage of zolmitriptan patients, regardless of dose, when compared with placebo. The most frequent adverse events are shown in Table 12. Table 12. Adverse events by COSTART term occurring in at least 5 % of patients in any treatment group, sorted by decreasing order of frequency – safety population (Phase I)
Treatment group number (%) of patients
Zolmitriptan 10.0 mg N=178
Zolmitriptan 5.0 mg N=174
Zolmi- triptan All zolmitriptan 2.5 mg N=523 N=171
Placebo N=176
All treatments
N=699
COSTART term
n (%) n (%) n (%) n (%) n (%) n (%)

All patients with adverse events (AEs)
79 (44.4) 45 (25.9) 49 (28.7) 173 (33.1) 22 (12.5) 195 (27.9)
Tightness 20 (11.2) 10 (5.8) 5 (2.9) 35 (6.7) 2 (1.1) 37 (5.3) Dizziness 16 (9.0) 8 (4.6) 8 (4.7) 32 (6.1) 4 (2.3) 36 (5.2)
Nausea 14 (7.9) 5 (2.9) 10 (5.9) 29 (5.5) 2 (1.1) 31 (4.4)
Paresthesia 11 (6.2) 8 (4.6) 3 (1.8) 22 (4.2) 0 22 (3.2) Asthenia 9 (5.1) 2 (1.2) 3 (1.8) 14 (2.7) 2 (1.1) 16 (2.3) Pain 9 (5.1) 3 (1.7) 3 (1.8) 15 (2.9) 0 15 (2.2) This table includes the number of patients reporting an adverse event at least once; patients reporting nonserious adverse events outside of the 24-hour time window are not included in the table. The decreasing order of frequency is based on the 10.0 mg zolmitriptan group. N Number of patients; n number of patients with adverse events.
During Phase I of the trial, serious adverse events, considered by the investigator as not related to treatment, occurred in 1 (0.2%) five mg zolmitriptan patient. Five zolmitriptan patients (4 [2.3%] in the 10.0 mg zolmitriptan group and 1 [0.6%] in the 2.5 mg zolmitriptan group) were withdrawn because of adverse events compared with none for the placebo group; 4 of the 5 patients had events that were considered by the investigators to be possibly drug related. Phase II of the study In Phase II, 319 patients who had exposures between up to 180 days treated a total of 1555 attacks, 239 patients who had exposures between 181 to 360 days treated a total of 4690 attacks up through 360 days, and 42 patients who had exposure times greater than 1 year (360 days) treated a total of 989 attacks over their total exposure time. In phase II, zolmitriptan tablets were taken at a 5 mg dosing. The mean number of zolmitriptan 5.0 mg tablets taken was 16.9 (SD 14.7, range: 1 to 77 tablets). In Phase II, 68.4% of patients took 0 to 20 zolmitriptan tablets and 22.7% of patients took 21 to 40 zolmitriptan tablets. For the most common adverse events, potentially treatment-related adverse events occurred in the following frequencies: dizziness 12.5 %, nausea 11.0 %, tightness 11.8 %, and paresthesia 8.5 %. For all of the most common adverse events, females had a higher reporting percentage than males. Ten (1.7 %) patients had serious adverse events (3 of which led to withdrawal). None o these events was assessed by the investigator as treatment related. Fifty patients in Phase II were withdrawn due to adverse events (3 patients for serious adverse events and 47 patients for non-serious adverse events). Assessors comment: The spectrum of adverse events in this trial was similar to that reported in adults. The incidence of side effects was dose-related. Zolmitriptan nasal spray (Study D1221C00005) The clinical study report is not yet available, but in response to a question from the Rapporteur, MPA, the applicant has prepared a preliminary safety summary. The primary objective of this study was to evaluate the efficacy of zolmitriptan 5 mg nasal spray, as compared to placebo for the acute treatment of migraine headache in adolescent subjects (aged 12 to 17 years). A total of 248 subjects were enrolled and randomised to either zolmitriptan/placebo (n=128) or placebo/zolmitriptan (n=120) at 18 centres in the US. 103 and 96

subjects in the zolmitriptan/placebo and placebo/zolmitriptan groups, respectively, completed the study. The study population (ITT) was primarily female (57.3%) and Caucasian (80.1%), with a mean age of 14.2 years. The most common AEs by treatment, as summarised by preferred term, are shown in Table 13. Table 13. Study Number (%) of subjects with the most commonly reported adverse events, sorted by decreasing order of frequency, by treatment, safety population
No deaths occurred during the study, and there were no SAEs and no withdrawals due to AEs. The most commonly reported adverse events were dysgeusia, nasal discomfort, dizziness, nasal congestion, and pharyngolaryngeal pain. All of these adverse events occurred in a greater proportion of patients in the zolmitriptan than the placebo group, except for pharyngolaryngeal pain. Females were more likely than males to report AEs. Most AEs were transient and mild or moderate in intensity. No evidence for treatment-related adverse changes in clinical laboratory results, ECG findings, vital signs, or physical examination was observed.
Laboratory findings There were no clinically significant changes in clinical laboratory parameters in adolescents exposed to zolmitriptan.
Assessors comment: The most common adverse events were of local character (dysgeusia, nasal discomfort etc.) and similar to those reported for nasal spray in adults. The safety results are preliminary and a final report should be awaited.
Request for supplementary information and assessment of information provided
1. The results of the Holter-monitoring in study 311/CUS/0007 raised serious concern. In 13 subjects a ST segment depression was observed. These have been interpreted as non-ischemic i.e. compatible with tachycardia in 11 of the 13 subjects and early repolarization in the other 2 subjects. There is however suggestion of a dose related conduction abnormality i.e. ST segment depression was observed in 4 subjects in the placebo group (19%), 1 subject receiving 2.5-mg zolmitriptan (4.8%), 2 subjects receiving 5-mg (9.5%) and 6 subjects receiving 10 mg

zolmitriptan (29%). A detailed report dealing with this potential serious safety concern is expected and labelling consequences should be discussed.
On the basis of the results of the Holter-monitoring in study 311/CUS/0007 an in-depth analysis of cardiac effects of zolmitriptan is mandatory. The details of serious adverse events should be provided. Assessment of the MAH’s response The argumentation of the MAH is accepted i.e. no serious adverse events of cardiovascular origin were reported from any of the clinical trials of zolmitriptan including studies in adolescents. Details of the serious adverse events observed were made available for verification. The events concerned prolong or intractable migraine (n=5), abdominal or epigastric pain (n=2), juvenile diabetes mellitus (n=1), ulcerative colitis (n=1), infection (n=1) and multiple fractures (n=1). It is emphasised by the MAH that none of these 11 serious adverse events were treatment related and only 2 occurred within the 24 hour of dosing with study medication. Issue resolved.
2. There is a relative high incidence of headache reported in single dose study with healthy volunteers (study 311/CUS/0007, 311CIL/0092, D1221C00004). Although the estimates may be unreliable due to small overall numbers of overall subject the difference with placebo in study 311/CUS/0007 is substantial. This poses the question whether zolmitriptan made induced headache and consequently supports it own use. The company should comment and discuss the consequences or for labelling. Assessment of the MAH’s response The difference in incidence of headache in study 311CUS/0007 i.e. 23.5%, 19% and 28.6% for zolmitriptan 10 mg, 5 mg and 2.5 mg versus 9.5% for placebo remains unexplained. As long as zolmitriptan is not recommended for adolescents there are no labelling consequences. 3. In study 311CIL/0092 an asymptomatic but clinical significant decrease in blood pressure as defined by the MAH was observed shortly (about 1 hour) after dosing with zolmitriptan 5.0 mg in 5 out of the 21 adolescents. Pulse frequency did not change. The consequences for labelling should be discussed. Assessment of the MAH’s response A decrease of more than 20 mm Hg in diastolic or systolic blood pressure is substantial and may be mentioned in the SmPC. However, as long as zolmitriptan is not recommended for adolescents there are no löabelling consequences. 4. From the repeated dose study (311/CUS/0005 part II) it was unclear whether the adverse event profile and frequency of adverse events differ after the first and second gift of zolmitriptan within a single migraine attack. The MAH should comment.

Assessment of the MAH’s response It is agreed that a formal evaluation can not be made. There are no positive arguments that the adverse event profile of the second gift is different from that of the first gift. Point resolved.
IV. OVERALL CONCLUSION AND BENEFIT-RISK ASSESSMENT
Zomig film-coated tablets, Zomig Rapimelt orodispersible tablets, and Zomig Nasal nasal spray are currently approved for the acute treatment of migraine headache with or without aura in adults. As a part of the EU work sharing project assessment of paediatric data of existing products, the MAH has submitted all available paediatric data for Zomig. The submitted data on efficacy and safety concern studies in adolescents (12-17 years of age) whereas there are no data in children (below 12 years of age). In one placebo-controlled study where a total of 696 adolescents were randomised to treat a single migraine headache with 2.5 mg, 5 mg or 10 mg zolmitriptan tablets or placebo, efficacy was not demonstrated for zolmitriptan. One randomised, controlled cross-over study comparing Zomig Nasal spray to placebo in adolescents has just been completed, but the final results are not yet available. After the primary assessment, an RSI was sent to the applicant. The questions in the RSI concerned the reason for lack of efficacy in Study 311 CUS/0005, and safety aspects on the use of zolmitriptan in adolescents (cardiovascular safety, effect of zolmitriptan on blood pressure, and the incidence of headache in one study in healthy volunteers). The MAH responded and after assessment of the responses the procedure was completed with the following agreement: An indication in the paediatric population or in adolescents is not approvable at present. Section 4.2 of the currently approved SmPC for zolmitriptan should be amended. In addition, the results of the negative study with Zomig tablets in adolescents should be described shortly in section 5.1 for all formulations of zolmitriptan. Final agreed changes to the zolmitriptan SPC 1. Zomig film-coated tablets and Zomig Rapimelt orodispersible tablets: Section 4.2 “Use in Children (under 12 years of age): Safety and efficacy of zolmitriptan tablets in paediatric patients have not been evaluated. Use of Zomig/Zomig Rapimelt in children is therefore not recommended.” “Adolescents (12 - 17 years of age) The efficacy of Zomig tablets was not demonstrated in a placebo controlled clinical trial for patients aged 12 to 17 years. Use of Zomig/Zomig Rapimelt tablets in adolescents is therefore not recommended. “ 2. Zomig Nasal Section 4.2

“Use in children (under 12 years of age) Safety and efficacy of Zomig Nasal in paediatric patients have not been evaluated. Use of Zomig Nasal in children is therefore not recommended.” “Adolescents (12-17 years of age) Safety and efficacy of Zomig Nasal in adolescents have not been evaluated. Use of Zomig Nasal in adolescents is therefore not recommended.” 3. For all formulations of Zomig: Section 5.1 “One controlled clinical trial in 696 adolescents with migraine failed to demonstrate superiority of zolmitriptan tablets at doses of 2.5 mg, 5 mg and 10 mg over placebo. Efficacy was not demonstrated.”