oxygen assessment and provision anne mcgown consultant royal berkshire hospital mar 2008
TRANSCRIPT
Oxygen assessment and provision
Anne McGown
Consultant
Royal Berkshire Hospital
Mar 2008
Old system
• Oxygen concentrators for long term oxygen therapy– some assessment done by chest clinics, but
prescription done by GPs
• Cylinders for prn use
• No provision of ambulatory oxygen
New system
• Divided according to oxygen requirement, and then company decide most economical system
• Long term oxygen therapy
• Ambulatory
• Short burst
• Emergency - indications yet to be defined
Therapeutic role of oxygen
• Only one of a number of effective treatments for chronic lung disease
• Need to have the right diagnosis
• Need to optimise other treatments
• Has defined indications and is not a universal panacea.
Oxygen for breathlessness
• No evidence that oxygen treats breathlessness in patients who are not hypoxic either at rest or on exercise.
• Why should it?
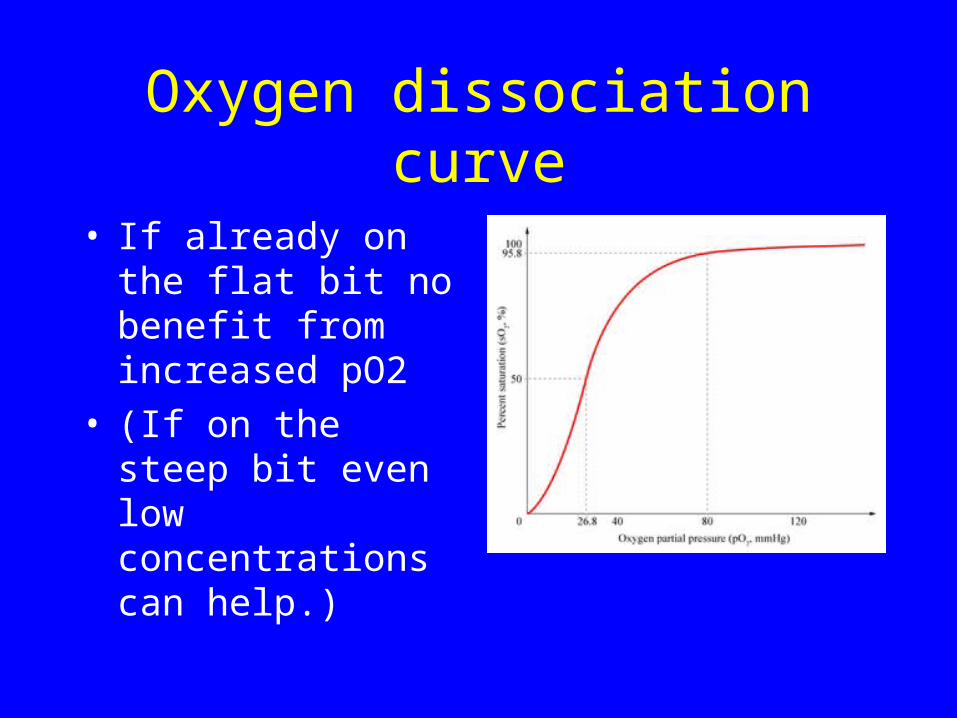
Oxygen dissociation curve
• If already on the flat bit no benefit from increased pO2
• (If on the steep bit even low concentrations can help.)
Long term oxygen therapy
• Continuous oxygen for at least 15hours a day
• Survival benefit in persistently hypoxaemic patient
• Mainly patients with COPD, other chronic lung disease with hypoxia.
• Criteria for prescription based only on blood gas measurements, not symptoms.
Who should be assessed? (COPD)
• All patients with severe airflow obstruction (FEV1 < 30% predicted)
• patients with cyanosis
• patients with polycythaemia
• patients with peripheral oedema
• patients with a raised JVP
Pulse oximetry• Can be used to screen who to refer for LTOT
assessment
• Non-invasive way to monitor percentage of haemoglobin that is saturated with oxygen.
• Works because oxygenated haemoglobin is a different colour from deoxygenated haemoglobin.
• Selects out pulsatile flow.
• Accurate above a saturation of 70%.
Pulse oximetry - practical points
• Not accurate if signal poor - always need to check signal– probe position– hypovolaemia/shock– peripheral vasoconstriction - cold– shivering– nail varnish
Checking the signal
Assessment for LTOT
• Pulse oximetry saturation <92%
• Arterial blood gases on 2 occasions 3 weeks apart when stable (ie not during exacerbation)
• Arterial puncture, traditionally performed by doctors in hospitals; we have a hospital protocol for nurse training and 4 nurses currently trained in clinic.
• Capillary sampling, easier, less reliable, tends to underestimate oxygen values
LTOT prescription• Strict criteria for prescription - pO2 of <7.3
or 7.3 to 8 with signs of cor pulmonale.• Do HOOF if fit the criteria.• Oxygen concentrator 15hours a day, 2l/min• Warn re smoking• Monitor compliance, sats, peripheral oedema• Evidence that it doesn’t help if not that bad.
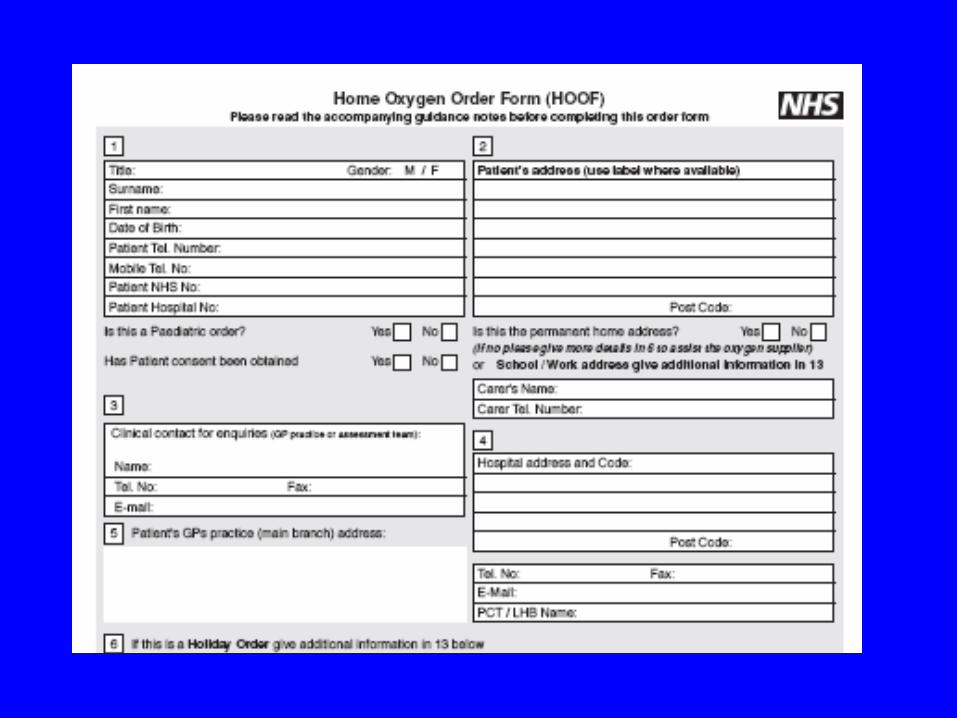
The HOOF and the HOCF
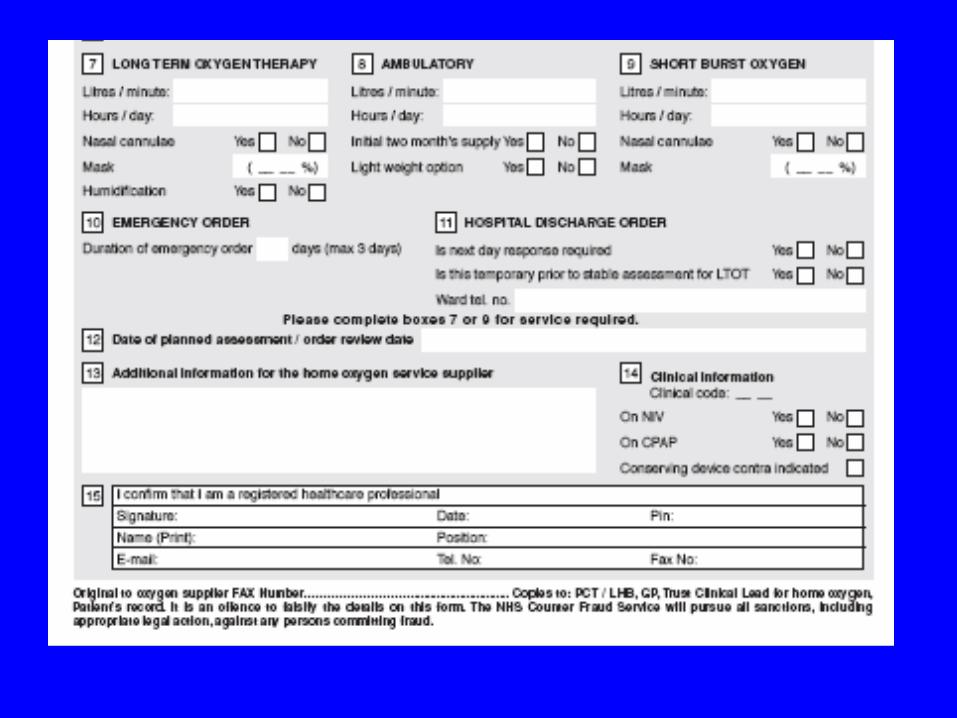
Small print
• Copies to– PCT– Trust clinical lead for oxygen– GP– patients notes– oxygen company
Oxygen concentrators
• Concentrate oxygen out of the air (by absorbing other gases)
• Plug into the wall, with tubing wired round the house.
• Need a cylinder for power cuts etc.
Ambulatory oxygen
• Provision of oxygen during exercise and activities of daily living.
• Shown to be effective in increasing exercise capacity and reducing breathlessness in patients with exercise arterial oxygen desaturation (fall of more than 4% or to below 90%).
Ambulatory assessment• New assessment procedure
• 6 minute walk, check desaturation
• 6 minute walk on oxygen, measure distance, desaturation correction and breathlessness on visual analogue scale.
• Time consuming, but less technically demanding than blood gases
• Only do assessment if reasonably mobile and motivated to carry the oxygen.
Ambulatory assessment
• Grade 1 oxygen requirements – on LTOT, walk nowhere, may want portable
cylinder for their wheelchair but don’t need assessment
• Grade 2 oxygen requirements – active LTOT - need assessment to see what flow
rate corrects desaturation
• Grade 3 oxygen requirements – exertional desaturation no LTOT
Ambulatory referrals
• Probably should offer assessment to all severe COPD patients if active enough.
• ? Also some moderate COPD patients who are SOBOE
• interstitial lung disease + SOBOE• new service so we don’t really know
nationally who will end up using it• compliance issues.
Short burst oxygen
• Prn cylinder patients
• no assessment necessary to prescribe short burst (no clear evidence of benefit)
• All new patients being considered for short burst oxygen should be referred for ambulatory assessment if mobile and LTOT assessment if hypoxic.
Compliance
• New system should allow better compliance/usage monitoring and removal of equipment if not used.
• Inappropriate short burst prescription should be reduced.
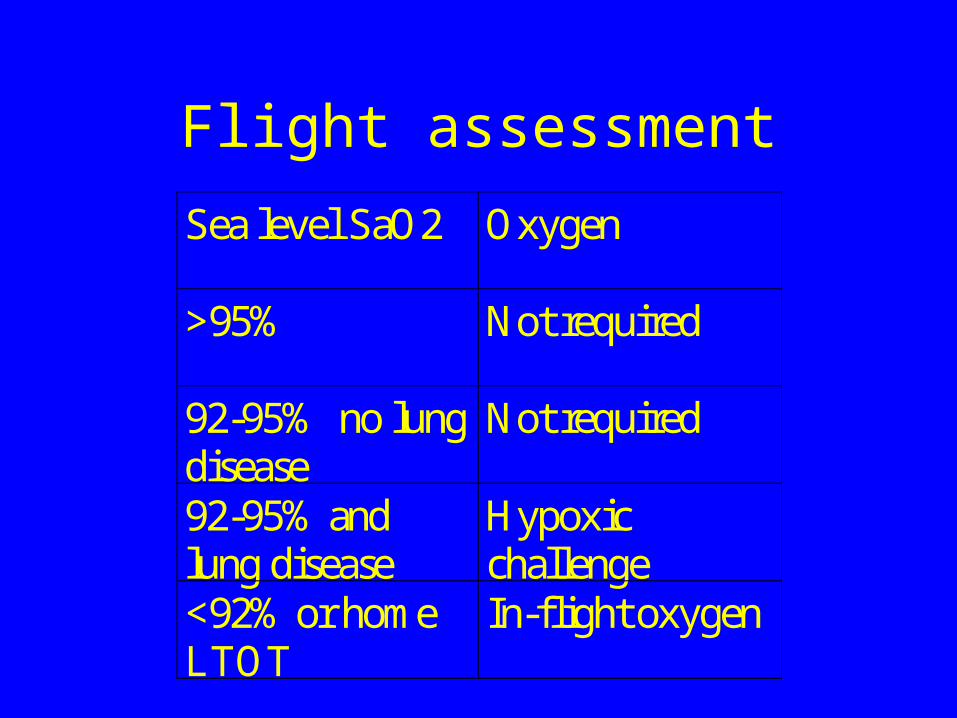
Flight assessment
Sea level SaO2 Oxygen
>95% Not required
92-95% no lungdisease
Not required
92-95% andlung disease
Hypoxicchallenge
<92% or homeLTOT
In-flight oxygen