outpatient dvt treatment protocol - enp-network.s3...
TRANSCRIPT

Outpatient DVT Treatment Protocol Adam Porath, PharmD, BCPS AQ-Cardiology, BCACP

Objectives
• Be able to identify medications that can facilitate outpatient DVT treatment
• Know which patients are not appropriate for outpatient DVT management
• Describe a patient care flow treatment model that facilitates outpatient DVT treatment

• Conflicts of Interest: None
• Will be discussing off-label use of FDA approved products
Patient Case
• MM is a 48 yo female who presents to Urgent Care with complains of LLE pain and swelling
• Ultrasound confirms extensive thombus in the common femoral, proximal femoral and proximal greater saphenous veins.
• Hx of recent travel to the Phillipines. No other risk factors for VTE
• No current medications or significant PMH • Renal function is unknown
Deep Vein Thrombosis (DVT)
• Venous thromboembolism (VTE) includes both DVT and pulmonary embolism (PE) ü Accounts for 1% of hospital admissions in the US ü 900,000 cases per year ü 60,000-300,000 deaths/year (mostly from
untreated/undiagnosed PE)

Deep Vein Thrombosis
• Often leads to unnecessary emergency department visits and admissions to initiate traditional anticoagulation (i.e. enoxaparin + warfarin)
• Uncomplicated disease can be managed on an outpatient basis ü Facilitated by the advent of direct acting oral
anticoagulants (DOACs)
DOACs for acute DVT
• Apixaban (Eliquis®) ü Approved for VTE treatment ü Dosed 10 mg PO BID x 7 days, then 5 mg PO BID
thereafter ü No parenteral anticoagulant required
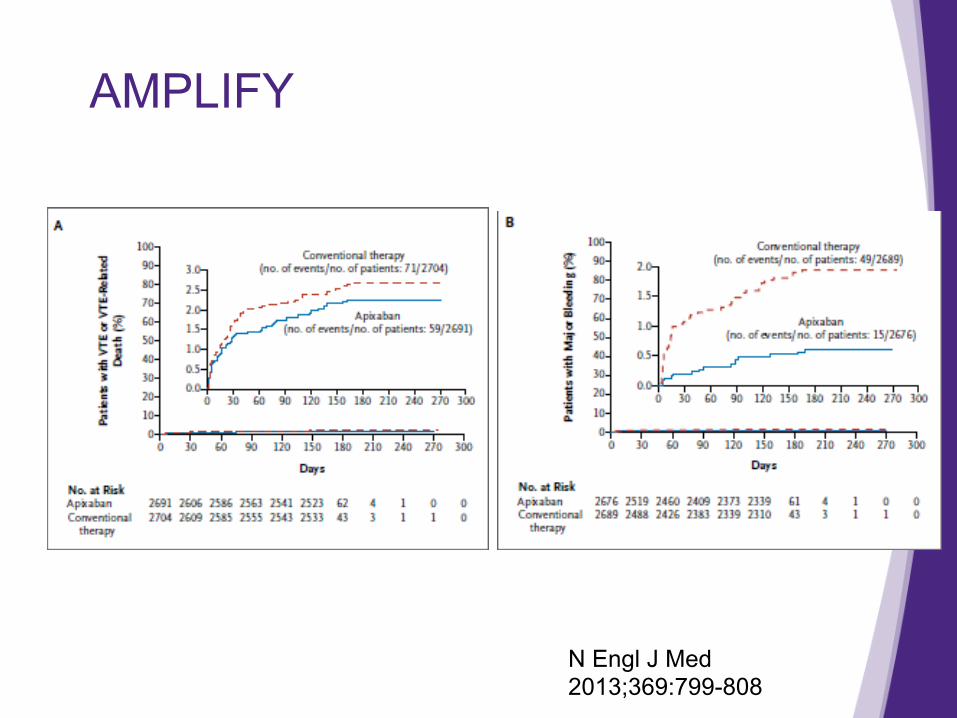
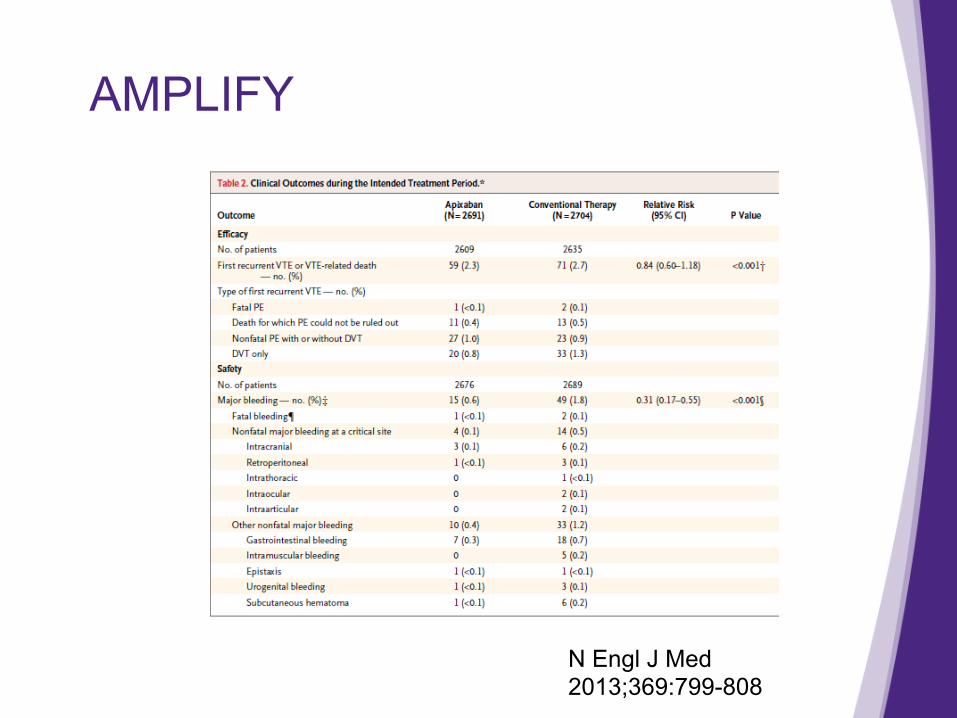
AMPLIFY
• Multi-national, double blind, non-inferiority study of 5395 patients randomized to apixaban 10 mg BID for 7 days followed by 5 mg BID for 6 months or SubQ enoxaparin followed by adjusted dose warfarin
• Primary outcome: recurrent symptomatic VTE or VTE related death
N Engl J Med 2013;369:799-808
AMPLIFY
N Engl J Med 2013;369:799-808
AMPLIFY
N Engl J Med 2013;369:799-808

AMPLIFY
N Engl J Med 2013;369:799-808
DOACs for acute DVT
• Rivaroxaban (Xarelto®) • Approved for the treatment of VTE • Dosed 15 mg PO BID x 3 weeks, then 20 mg PO
daily thereafter • No parenteral anticoagulant required
EINSTEIN DVT Trial
• Open label, randomized, non-inferiority study of 3449 patients randomized to rivaroxaban 15 mg BID for 21 days followed by 20 mg daily for 3,6, or 12 months or SubQ enoxaparin followed by adjusted dose warfarin
• Primary outcome: recurrent VTE
N Engl J Med 2010;363:2499-510.

EINSTEIN DVT Trial
N Engl J Med 2010;363:2499-510.

N Engl J Med 2010;363:2499-510.
When are DOACs inappropriate
• Pregnancy/Lactation ü No human data
• Impaired renal function ü Patients with a CrCl less than 30 mL/min were not
included in any of the DOAC trials for VTE treatment
• Financial considerations ü Medicare patients
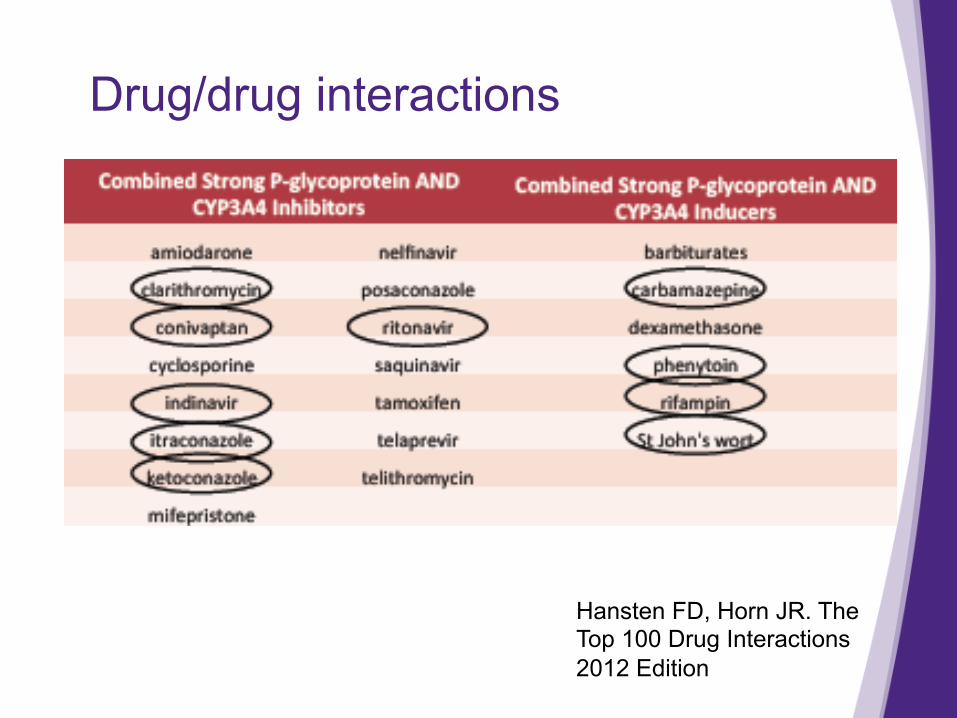
Drug/drug interactions
Hansten FD, Horn JR. The Top 100 Drug Interactions 2012 Edition

Other DOACs
• Dabigatran (Pradaxa®) ü Approved for the treatment of VTE after 5-10 days
of a parenteral anticoagulant ü Dose: 150 mg PO BID
• Edoxaban (Savaysa®) ü Approved for the treatment of VTE after 5-10 day of
a parenteral anticoagulant ü Dose: 60 mg PO once daily
– 30 mg PO once daily if CrCl 15-50 ml/min, body weight less than 60 Kg, or on concomitant P-gp inhibitors

Renown DVT Protocol
• Started in 2013 • Rivaroxaban was the only DOAC approved for
DVT treatment • Nearly 200 patients treated to date

DVT Protocol Patient Flow
Outpatient DVT Treatment
• Ambulatory, in stable condition, normal vitals • Low bleeding risk • System in place for appropriate follow up • No known contraindication to anticoagulation

Complicated DVT
• Known contraindication to anticoagulation/DOAC • Concern for PE • DVT in pregnancy • Potential candidate for thrombolysis • Psychosocial concerns for outpatient follow up
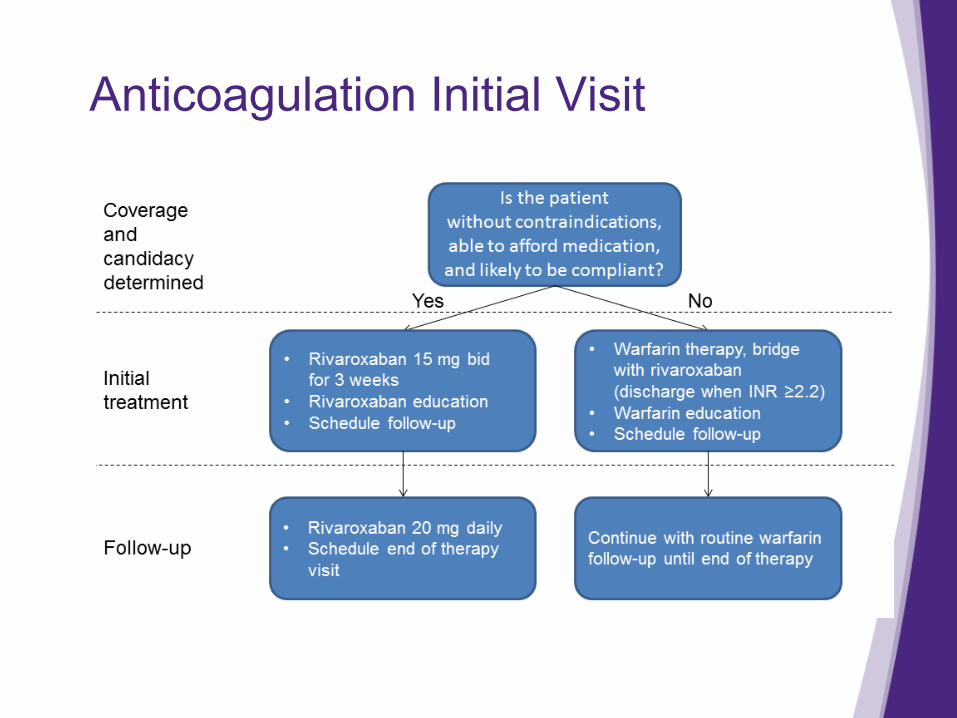
Anticoagulation Initial Visit

DOAC follow up
• ABCDEF ü Adherence
– Any missed doses of DOAC? ü Bleeding Risk Assessment
– Epistaxis, GIB, Hematuria, abnormal vaginal bleeding, significant headache/visual changes, anemia, EtOH, fall risk, uncontrolled hypertension
ü Creatinine clearance/renal function – Is CrCl greater than 30 mL/min? – Any recent dehydration, diuretic use
Gladstone DJ et al. Annals of Internal Medicine 2015
DOAC follow up
• Drug Interactions ü ASA/Antiplatelet medications ü NSAID use
• Exam ü Resolution of pain/swelling ü SOB ü Blood pressure ü Fall risk assessment ü Point of care INR
– No therapeutic range for DOACs – High INRs can indicate inappropriate therapy

DOAC follow up
• Final Assessment/Recommendations ü Benefit risk of continuation of DOAC ü Alternative anticoagulation
Renown DVT Protocol Results
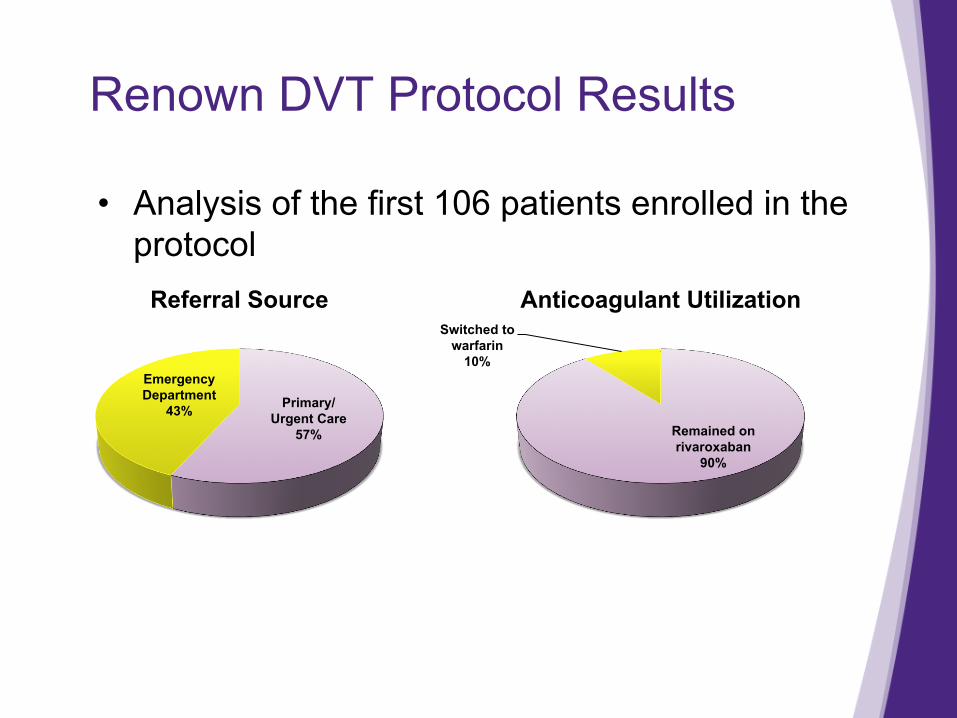
• Analysis of the first 106 patients enrolled in the protocol
Primary/ Urgent Care
57%
Emergency Department
43%
Referral Source
Remained on rivaroxaban
90%
Switched to warfarin
10%
Anticoagulant Utilization
Renown DVT Protocol Results
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
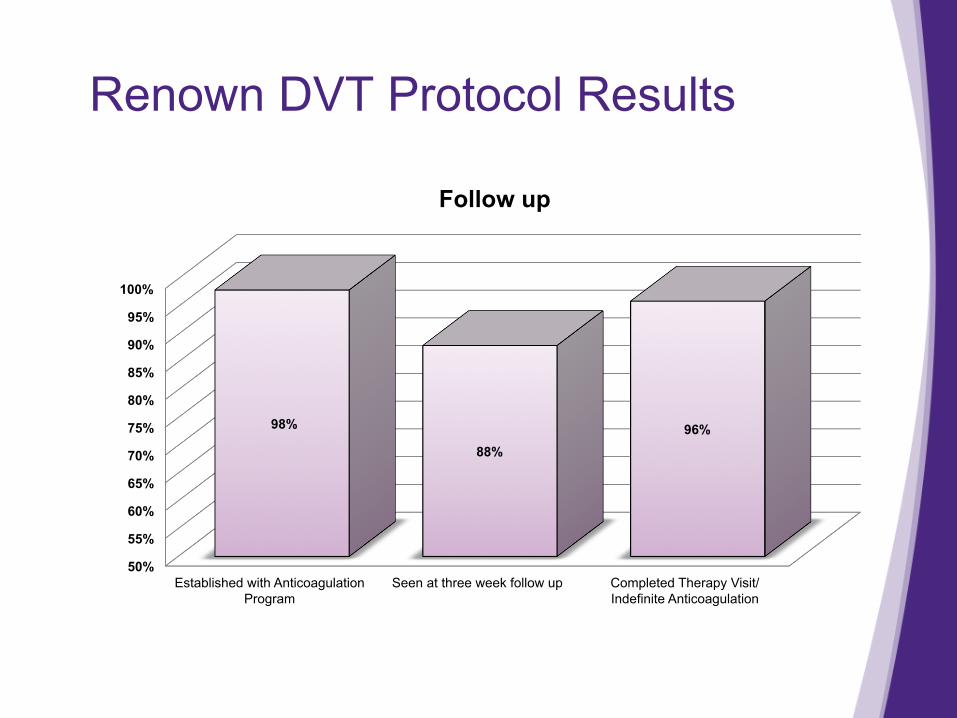
Established with Anticoagulation Program
Seen at three week follow up Completed Therapy Visit/Indefinite Anticoagulation
98%
88% 96%
Follow up

Renown DVT Protocol Results
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Admitted for any cause ≤ 6 month after diagnosis
Admitted for bleeding complications
Admitted for thrombotic complication
Visit to ED for any reason ≤ 6 months after
diagnosis
12%
3% 0.90%
15%
Health Care Utilization

Renown DVT Protocol
• Other lessons learned: ü 24 hour on-call resource is a key
– Nurse Navigator ü Medical assistant role important
– Determining co-pays – PA requests

Patient Case
• MM was started on rivaroxaban 15 mg BID and referred to Anticoagulation Program
• Initial Anticoagulation Visit: ü Renal function WNL ü Able to afford rivaroxaban
– PA needed on insurance ü Fitted for compression stocking

Patient Case
• 3 week follow up: ü Not tolerating rivaroxaban
– GI upset, excessive vaginal bleeding ü Switched to apixaban
– PA again required by insurance • Treated for 3 months
ü Switched to ASA 81 mg daily
Conclusions
• Patients with uncomplicated DVT can be successfully managed as outpatients
• DOAC medications can help simplify outpatient DVT management
• Potential for decreased healthcare utilization and expense
• Further study is needed and ongoing

Questions? [email protected]