outlines - clinical.pharmacy.psu.ac.thclinical.pharmacy.psu.ac.th/content/documents/inhalers.pdf ·...
TRANSCRIPT
Aerosolized antimicrobial agentsAerosolized antimicrobial agents
Buddharat Khan-asaPharmacy Residency Program
Buddharat Khan-asaPharmacy Residency Program
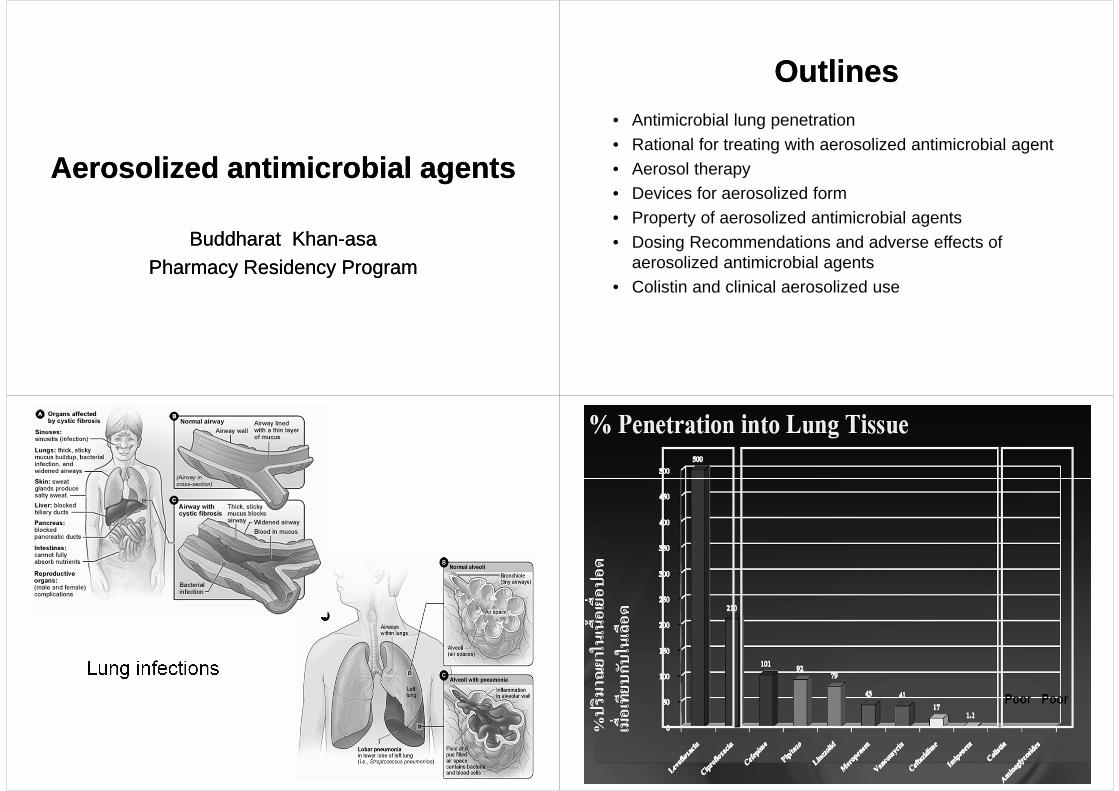
OutlinesOutlines• Antimicrobial lung penetration
• Rational for treating with aerosolized antimicrobial agent• Aerosol therapy• Devices for aerosolized form• Property of aerosolized antimicrobial agents
• Dosing Recommendations and adverse effects of aerosolized antimicrobial agents
• Colistin and clinical aerosolized use
Lung infections

Possible mechanisms of antibiotic penetration into the lung
Model of how VAP (A). treated with systemic antibiotics, may not treat VAT in proximal airway effectively(B). Aerosolized antibiotics with primarily central deposition eliminate VAT effectively (C). VAT could be targeted alone before VAP and/or as an adjuvant with systemic antibiotics in VAP( Modified from Current Opinion in Critical Care 2009;15:414)
Clin Chest Med 2011;32:559–74.
Clin Chest Med 2011;32:559–74.
Advantages and Disadvantages of Aerosolized therapy
Advantages and Disadvantages of Aerosolized therapy
Chest. 2001;120(suppl):S94-S98.

Aerosol therapyAerosol therapy• Aerosolized - in the form of
ultramicroscopic solid or liquid particles dispersed or suspended in air or gas
Tabel 1 Size of aerosol and lung target depositMass median aerodynamic diameter Lung target zone
< 0.5 µm0.5-2 µm2-5 µm
5-100 µm>100 µm
Stable and tent not to become depositAlveoliBronchi and bronchiolesMouth, nose, and upper airwaysDo not enter respiratory tract
Device of aerosolized formDevice of aerosolized formJet nebulizers• Small volume nebulizer (<10 ml)• Large volume nebulizer (up to 200 ml)
Jet nebulizers• Small volume nebulizer (<10 ml)• Large volume nebulizer (up to 200 ml)
Pharmacotherapy 2010;30(6):562–84.Respiratory Care. 2007;52(7):866-84. http;//www.medicalbuyer.co.th.in/index.php?option=com_content&task =view&id= 813&Itemid=48
Jet NebulizersJet Nebulizers

Respir Care. 2004 Jun;49(6):635-9.

Special considerationsSpecial considerationsThere are certain variables that allow optimization of antibiotic administration.
– Humidifying the air decreases the amount of drug delivered to the patient secondary to water in the air causing the droplets to clump together and more readily attach to the wall of the tubing
– Breath-actuated nebulization was found to administer a higher dose of antibiotic to the lung than did continuous nebulization
Factors affecting nebulizer performance include nebu lizer
Respiratory Care. 2007;52(7):866-84. http;//www.medicalbuyer.co.th.in/index.php?option=com_content&task =view&id= 813&Itemid=48
Breath-enhanced jet nebulizer
(Pari LC Plus®)
Breath-enhanced jet nebulizer
(Pari LC Plus®)
PARI LC Plus®

1. Review order, identify patient, and assess need for bronchodilator 2. Suction endotracheal and airway secretions3. Place drug in nebulizer to fill volume of 4–6 mL4. Place nebulizer in the inspiratory line 46 cm from the patient Y connector5. Turn off flow-by or continuous flow during nebulizer operation 6. Remove HME from circuit (do not disconnect humidifier)
Optimal Technique for Drug Delivery via Jet Nebulizer in Ventilated Patients Optimal Technique for Drug Delivery
via Jet Nebulizer in Ventilated Patients
Respiratory Care. 2007;52(7):866-84.
HME: heat-and-moisture exchanger
Optimal Technique for Drug Delivery via Jet Nebulizer in Ventilated Patients Optimal Technique for Drug Delivery
via Jet Nebulizer in Ventilated Patients 7. Set gas flow to nebulizer at 6–8 L/min.
a. Use a ventilator if it meets the nebulizer flow requirements and cycles on inspiration, or
b. Use continuous flow from external source8. Adjust ventilator volume or pressure limit to compensate for added flow9. Tap nebulizer periodically, until nebulizer begins to sputter10. Remove nebulizer from circuit, rinse with sterile water and dry, store in safe place11. Reconnect humidifier or HME, return ventilator settings and alarms to previous values 12. Monitor patient for adverse response13. Assess outcome and document findings.
Respiratory Care. 2007;52(7):866-84.
HME: heat-and-moisture exchanger
Ultrasonic nebulizerUltrasonic nebulizer
Pharmacotherapy 2010;30(6):562–84.Respiratory Care. 2007;52(7):866-84. http;//www.medicalbuyer.co.th.in/index.php?option=com_content&task =view&id= 813&Itemid=48
Ultrasonic nebulizersUltrasonic nebulizers
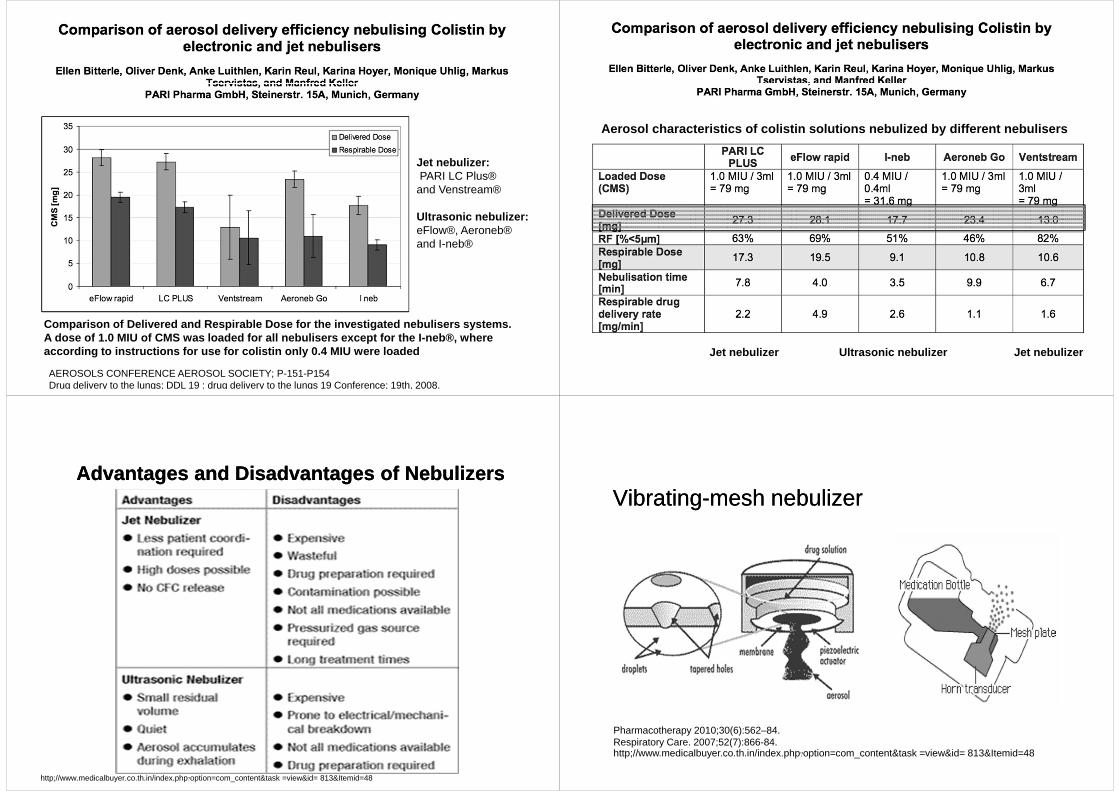
Comparison of Delivered and Respirable Dose for the investigated nebulisers systems. A dose of 1.0 MIU of CMS was loaded for all nebulis ers except for the I-neb®, where according to instructions for use for colistin only 0.4 MIU were loaded
Jet nebulizer:PARI LC Plus®
and Venstream®
Ultrasonic nebulizer:eFlow®, Aeroneb® and I-neb®
AEROSOLS CONFERENCE AEROSOL SOCIETY; P-151-P154Drug delivery to the lungs; DDL 19 : drug delivery to the lungs 19 Conference; 19th, 2008.
Aerosol characteristics of colistin solutions nebul ized by different nebulisers
Jet nebulizer Ultrasonic nebulize r Jet nebulizer
Advantages and Disadvantages of NebulizersAdvantages and Disadvantages of Nebulizers
http;//www.medicalbuyer.co.th.in/index.php?option=com_content&task =view&id= 813&Itemid=48
Vibrating-mesh nebulizerVibrating-mesh nebulizer
Pharmacotherapy 2010;30(6):562–84.Respiratory Care. 2007;52(7):866-84. http;//www.medicalbuyer.co.th.in/index.php?option=com_content&task =view&id= 813&Itemid=48

Ideal property of aerosolized antimicrobial agents
Ideal property of aerosolized antimicrobial agents
• Isotonic• Sterile or pyrogen-free• Unit of use• Tasteless or pleasant tasting• No preservatives or toxic materials• Solution that can be easily nebulized• Good chemical stability
• Isotonic• Sterile or pyrogen-free• Unit of use• Tasteless or pleasant tasting• No preservatives or toxic materials• Solution that can be easily nebulized• Good chemical stability
Chest. 2001;120(suppl):S94-S98.
Effect of Preservatives in Aerosol Delivery
Chest. 2001;120(suppl):S94-S98.
Amikacin(Siam Bheasach):Sodium metabisulfites
Gentamicin (GPOs): Methylparaben, Propylparaben
Product information: Siamik®, amikacin sulfate, Siam Bheasach, Bangkok, Thailand.Product information: Gentamicin sulfate®, gentamicin sulfate, The Government Pharmaceutical Organization, Bangkok,Thailand.
Preservatives in amikacin and gentamicinPreservatives in amikacin and gentamicin
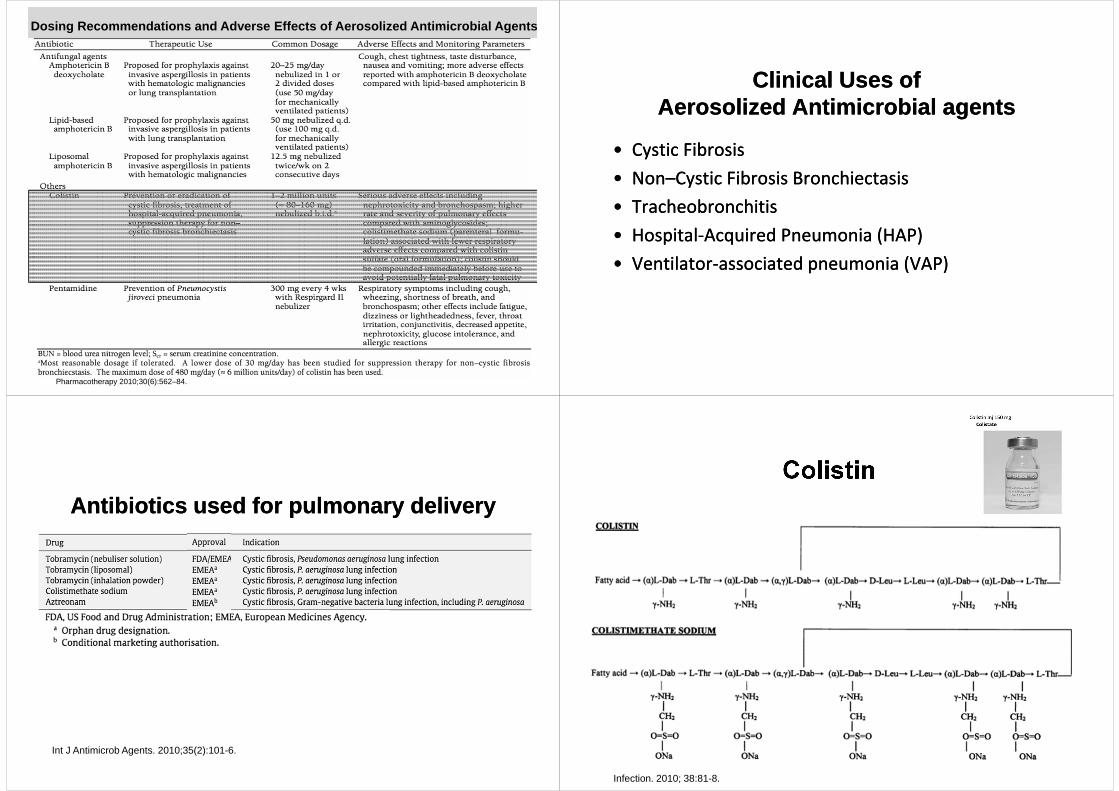
Dosing Recommendations and Adverse Effects of Aerosolized Antimicrobial Agents
Pharmacotherapy 2010;30(6):562–84.
Dosing Recommendations and Adverse Effects of Aeros olized Antimicrobial Agents
Pharmacotherapy 2010;30(6):562–84.
Clinical Uses of Aerosolized Antimicrobial agents
Clinical Uses of Aerosolized Antimicrobial agents
• Cystic Fibrosis
• Non–Cystic Fibrosis Bronchiectasis
• Tracheobronchitis
• Hospital-Acquired Pneumonia (HAP)
• Ventilator-associated pneumonia (VAP)
• Cystic Fibrosis
• Non–Cystic Fibrosis Bronchiectasis
• Tracheobronchitis
• Hospital-Acquired Pneumonia (HAP)
• Ventilator-associated pneumonia (VAP)
Antibiotics used for pulmonary delivery Antibiotics used for pulmonary delivery
Int J Antimicrob Agents. 2010;35(2):101-6.
ColistinColistin
Infection. 2010; 38:81-8.

Intensive Care Med. 2010;36(7):1147-55. Intensive Care Med. 2010;36(7):1147-55.
Intensive Care Med. 2010;36(7):1147-55.
Clinical and microbiological outcomes of the study patients
J Antimicrob Chemother. 2010;65(12):2645-9

Previous Studies on Colistin Inhalation Therapy for Pneumonia
Yonsei Med J. 2014;55(1):118-25.
Previous Studies on Colistin Inhalation Therapy for Pneumonia
Choi, et al. 120 COS INH/INH+other 75 mg q12h 19.5(12-29) 17(5-31) Microbiologic 50, 0
2014 A.baumannii antibiotics clinical 83
Yonsei Med J. 2014;55(1):118-25.
The recommended dose of colistin The recommended dose of colistin
• 40 mg (0.5 MIU) q 12 h for body weight ≤ 40 kg
• 80 mg (1 MIU) q 12 h for body weigh > 40 kg• For recurrent or severe pulmonary infections:
160 mg (2 MIU) q 8 h
• 40 mg (0.5 MIU) q 12 h for body weight ≤ 40 kg
• 80 mg (1 MIU) q 12 h for body weigh > 40 kg• For recurrent or severe pulmonary infections:
160 mg (2 MIU) q 8 h
Infection. 2010; 38:81-8.http://www.mhra.gov.uk/home/groups/par/documents/websiteresources/con125942.pdf
• The recommended dose for spontaneously breathing patients is 80 mg (1 MIU),the colistin is added to 4 ml of normal saline or sterile water
• The solution is nebulized with 8 L/min oxygen flow and inhaled via a face mask
• The exact optimal dosing remains unclear, as the precise pharmacokinetics and pharmacodynamics of the drug have not yet been clarified
• Colistin is not approved by the USA FDA to be inhaled via a nebulizer
The recommended administration of colistin The recommended administration of colistin
Infection. 2010; 38:81-8.http://www.mhra.gov.uk/home/groups/par/documents/websiteresources/con125942.pdf

Adverse effectsAdverse effects• Bronchoconstriction (decrease in FEV1 >10%)
– aerosolization of colistin occurring in ≈ 18-34%– polymyxin E1, the primary active component of
colistin has been shown to cause local airway
inflammation– The reaction seems to be caused by mast cell
degranulation induced in a dose dependent manner by polymyxin E1
• Nephrotoxicity - acute tubular necrosis• Neurotoxicity - dizziness, parasthesias, muscle
weakness, ataxia, or peripheral neuropath
Curr Opin Pulm Med. 2001 Nov;7(6):434-40.
Colistin-associated BronchoconstrictionColistin-associated Bronchoconstriction
• Suggest that solutions of CMS should be prepared freshly and administer solution promptly following preparation
• Use CMS within 24 hr after mixing NSS or SWI
• Premedication with bronchodilators can be used to reduce the potential for development in many individuals
• Pre- and post- treatment pulmonary function tests should be performed at initiation of therapy to identify patients who are predisposed to this reaction
Curr Opin Pulm Med. 2001 Nov;7(6):434-40.
Limitation of Aerosolized CMS therapyLimitation of Aerosolized CMS therapy
• Monotherapy with nebulized CMS is probably devoice of serious systemic adverse events, but drug lung deposition decreases with loss of aeration and colistin may not reach lung segments with pneumonia
• Monotherapy with nebulized CMS is inappropriate when pneumonia is associated with bacteremia
Annual updates in intensive care and emergency medicine. Brussels: Springer; 2013. p.99-110. 48
Thank You for Your Attention