outcomes, service models and integrated service delivery paul flatau the university of western...
TRANSCRIPT

OUTCOMES, SERVICE MODELS AND INTEGRATED SERVICE DELIVERY
Paul Flatau
The University of Western Australia Centre for Social Impact
1

THE FUNDING CONTEXT
2

Three Steps to Contract
• What would success look like for our clients
Client Outcomes

Three Steps to Contract
Step 1: Define Your Intended Client Outcomes
Step 2 Develop Your Service Delivery Model
Step 3 Establish Your Value Proposition

Step 1: Outcomes
Inputs
Activities
Outputs
Outcomes
Impacts
The focus of the WA Government’s procurement reform
Your Planned Work Your Intended Results
1 2 3 4 5
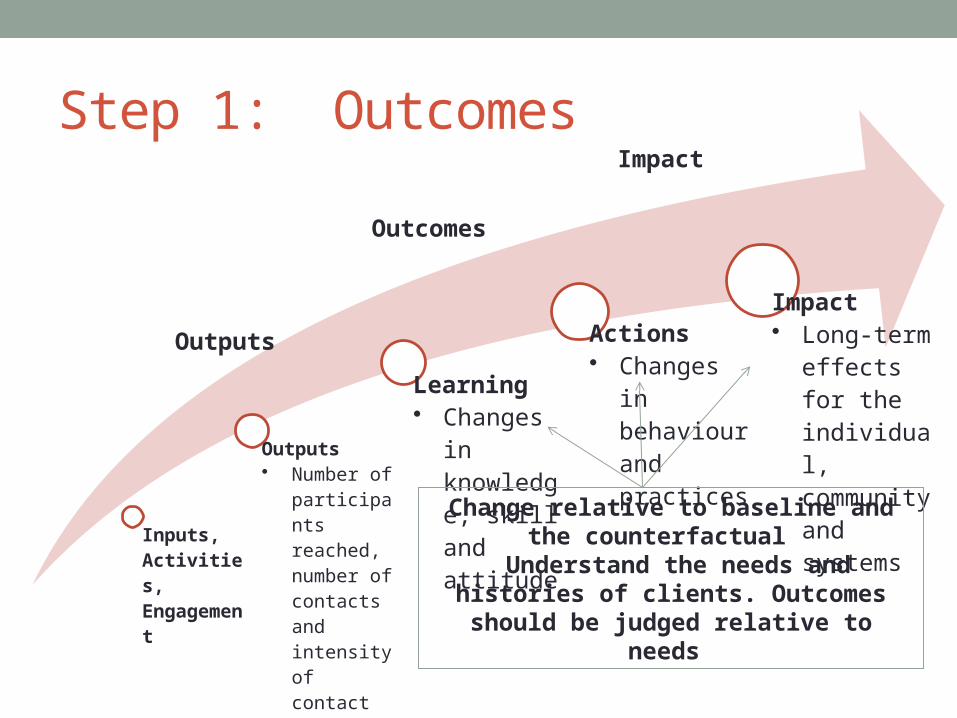
Step 1: Outcomes
Inputs, Activities, Engagement
Outputs • Number of
participants reached, number of contacts and intensity of contact
Learning• Changes in
knowledge, skill and attitude
Actions• Changes in
behaviour and practices
Impact• Long-term
effects for the individual, community and systems
Change relative to baseline and the counterfactual
Understand the needs and histories of clients. Outcomes should be judged
relative to needs
Outputs
Outcomes
Impact

DAO Residential Rehab Service Outocmes
• Improvement in clients wellbeing (physical, mental, emotional, social, standard definition) in the:• Short term(3-6 months post treatment)• Long term (+6 months post treatment)
• Greater awareness/understanding of own drug use and factors impacting upon
• Improvement in the clients capacity to relate to family and function in the community• Short term(3-6 months post treatment)• Long term (+6 months post treatment)
7

Step 2: The Service Delivery Model
• Establish HOW and WHY your service will achieve intended outcomes and impacts
• What links the activities you are undertaking to the intended short-term and medium-term outcomes and final impacts for clients and communities?
• How will your service model achieve the ends you are after?
• The THEORY OF CHANGE logic model

Step 3: The Value Proposition• Why your service represents value for money ……
Because you can demonstrate that your service delivery model produces (or has the capacity to produce) positive benefits for your clients and long-term positive impacts for the community … and you can do this at the right price

THE ROLE OF SERVICE INTEGRATION
10

Focus • Findings from ongoing studies IN HOMELESSNESS on
comorbidity and homelessness and social exclusion• Comorbidity: coexisting substance use and (other) mental health
disorders• Homelessness: primary homelessness; supported
accommodation and temporary accommodation (couch surfing family or friends; hotel/motel as have nowhere else to go; boarding/rooming houses)
• Social exclusion: Income, wealth, resources, friendships, family
11

MP Baseline: Mental Health• Mental Health
• Around half of all respondents indicated they had been diagnosed with a mental health disorder (excluding substance use disorders)
• Prevalence of mental health disorders • 33% with mood disorders• 34% anxiety disorders• 17% psychotic disorders• 12% personality disorders• 51% substance use disorder• Others less than 10%
• 34% Comorbidity (diagnosed substance use disorder and diagnosed other mental health disorder)
• 36% currently taking medication for a mental health condition
12

MP Baseline: AOD
13
Outreach and Emergency Short and Medium Term Accommodation
Ever tried Past month
Dependence
Ever tried
Past month
Dependence
n % n % n % % % n % n %Heroin 56 59.6 20 21.3 10 50.0 78 51.7 16 10.6 13 81.3
Opioids other than heroin 38 40.4 12 12.8 7 58.3 64 42.4 15 9.9 10 76.9
Alcohol 86 91.5 58 61.7 31 55.4 140 92.7 78 51.7 41 53.9
Cannabis 74 78.7 47 50.0 25 54.3 124 82.7 32 21.4 23 74.2
Amphetamines 57 60.6 20 21.3 13 65.0 89 59.3 14 9.4 7 53.8
Cocaine 48 51.1 12 12.8 9 75.0 79 52.7 6 4.0 2 40.0
Tranquillisers 39 41.5 15 16.0 8 53.3 64 42.4 10 6.6 3 30.0
Hallucinogens 44 46.8 3 3.2 0 0.0 80 53.0 3 2.0 2 100.0
Inhalants 24 25.5 2 2.1 0 0.0 41 27.2 3 3.0 1 50.0
Average 52 55.1 21 22.4 12 53.1 83 55.7 19 12.5 11 62.2

MP Baseline: Mental Health
14
Combat experience
Life threatening accident
Natural disaster
Witness someone being badly injured/killed
Raped
Sexually molested
Seriously physically assaulted
Threatened with weapon or held captive
Terrorist victim
Any other stressful event
Vicarious stressful event
0 20 40 60 80100
8.1
55.7
26.8
69.8
10.1
22.1
65.8
60.4
8.8
48.3
45
Pe
r ce
nt
Lifetime exposure to different traumatic events

MP Baseline: Mental Health• High to very high levels of psychological distress & very high rates
of PTSD & psychosis • 95% had experienced one or more traumatic events eg witness
someone being badly injured/killed; serious physical assault; life threatening accident etc
• Typically early adolescence when 1st traumatic event occurred with worst exposure in early adulthood
trauma history well established by adulthood• 20% of MP clients screened with post-traumatic stress disorder
(PTSD) compared with 1% of adult male pop
15

MP Baseline: Quality of Life16
Figures exclude participants who did not respond to the relevant questions.Findings on the 2000 Victorian Validation Study are reported in Australian WHOQOL Field Study Centre (2000 p.26).
Physical Psychological Social relationships Environment0
10
20
30
40
50
60
70
80
90
100
56.653.5
43.345.8
64.1
56.7
47.2
59.5
80.0
72.6 72.274.8
Outreach & emergency accommodation Short & medium term accommodationVVS Community sample
Me
an
Sco
res

MP Baseline: Deprivation & Social Exclusion
• 78% couldn’t afford dental treatment if needed; 80% unable to afford prescribed medicines
• Causes of social isolation (short & medium term accommodation respondents)
• Lack of money: 81%• Lack of own transport: 71%• Absence of supportive family: 70%• Family related problems: 66%• Lack of friends to provide support: 60%• Lack of involvement in community/sport: 49%• Mental health: 37%• Physical health: 31%
17

Intergenerational Homelessness Survey (HIS)
18

Prevalence of Intergenerational Homelessness, by Sex

Parental Experiences of Jail, Stays in Hospital and Problematic Drug and Alcohol Use While Growing Up

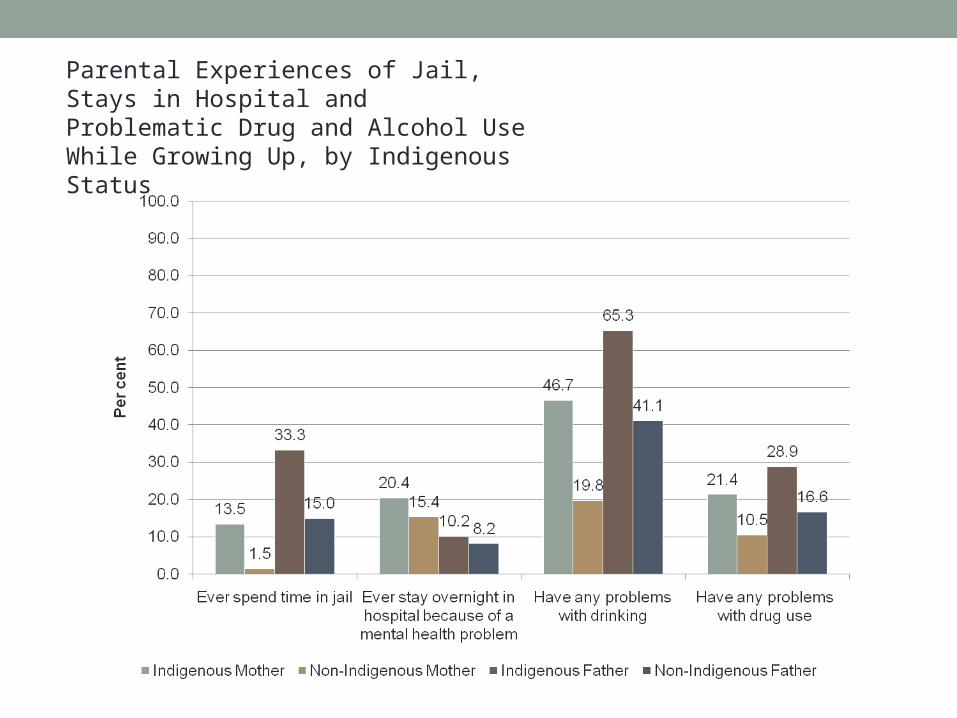
Parental Experiences of Jail, Stays in Hospital and Problematic Drug and Alcohol Use While Growing Up, by Indigenous Status

IHS – Respondent Problems
23
Not at all Slight Moderate Serious TotalN % N % N % N % N %
Being bored 99 18.3 140 25.9 165 30.5 137 25.3 541 100.0Being lonely 115 21.4 133 24.8 155 28.9 134 25.0 537 100.0Drinking too much 220 40.7 86 15.9 104 19.2 131 24.2 541 100.0Taking drugs 221 40.9 97 17.9 92 17.0 131 24.2 541 100.0Feeling depressed, anxious or stressed
65 11.9 130 23.9 143 26.3 206 37.9 544 100.0
Losing temper 132 24.4 159 29.4 137 25.4 112 20.7 540 100.0Getting along with family
131 24.3 159 29.5 125 23.2 124 23.0 539 100.0
Lifetime experiences of problems among respondents (select indicators only). Feeling depressed, anxious or stressed highest rating in terms of seriousness of lifetime problems.
Proxy of Comorbidity: 20 per cent of respondents cited a serious alcohol or other drug problem (at some point in their lives) and a serious problem of feeling depressed, anxious or stressed (at some point in their lives)

IHS – Respondent A&OD and Depressed, Anxious or Stressed
24

Comorbidity and Other Associations• Those respondents with (proxy of) comorbidity are much
more likely (than those without comorbidity) to • …have experienced homelessness first prior to the age of 12• …have experienced primary homelessness at some point in their
lives• …have experienced their parents argue with each other all the time• …have seen or heard their parents physically harm each other or
threaten each other with a weapon all the time• …left home more often because of violence between parents (with
a slightly greater chance of being residential and foster care)• …have run away from home more and done so more often
25

Comorbidity and Other Associations• …consider they have had at some point in their lives a serious
problem with • Gambling• Keeping bad company• Being bored• Being lonely • Repeating the same mistakes • Losing their temper• Managing their money/debt• Getting on with their family• Dealing with the authorities
26

What is integration?
Figure 2 : Ahgren and Axelsson’s integration continuum
Full segregation Full integration
Linkage Coordination Cooperation
in networks
Linkage: independent organisational units. Referral of patients to the right unit at the right time and good
communication between the professionals involved in order to promote continuity of care.
Coordination in networks: operates largely through existing organisational units.
Coordination of different
health services, sharing clinical information, and the management of the transition of patients
between different units.
Full integration: the resources of different organisational units are pooled in order to create a new
organisation.
Source: Ahgren and Axelsson (2005)

Motivation• Effectiveness of Service Delivery
• A fragmented human services system may:• Result in gaps in service delivery;• Pull clients in different directions;• Provide clients with conflicting advice and support and treatment
options; • Produce ineffective referral pathways; and,• Impose unnecessary transaction costs on clients as they navigate the
human services system

Motivation Cont…• Effectiveness of Service Delivery
• but potential issues …• Service integration may be costly (high setup costs and high transaction
costs for agencies), unwieldy and time-consuming• Possible loss of control/autonomy among agencies• Differing values of organisations• Difficulties in transmitting specific knowledge among partnership
members• Free rider problems• Requires leadership and good management particularly when
partnerships is ‘forced’ on to a set of agencies with different cultures and practices
• Loss of the benefits of specialisation in service delivery.

Ends and meansService Integration
Client Integration
Client Outcomes
Other factors
Other factors
Other factors
DAO Residential Outocmes• Improvement in clients wellbeing (physical, mental,
emotional, social, standard definition) in the:• Short term(3-6 months post treatment)• Long term (+6 months post treatment)
• Greater awareness/understanding of own drug use and factors impacting upon
• Improvement in the clients capacity to relate to family and function in the community• Short term(3-6 months post treatment)• Long term (+6 months post treatment)
31