outcomes of management of acute coronary syndrome in patients with congenital bleeding disorders: a...
TRANSCRIPT

Thrombosis Research 130 (2012) 316–322
Contents lists available at SciVerse ScienceDirect
Thrombosis Research
j ourna l homepage: www.e lsev ie r .com/ locate / thromres
Regular Article
Outcomes of management of acute coronary syndrome in patients with congenitalbleeding disorders: A single center experience and review of the literature
Ming Y. Lim a, Rajiv K. Pruthi b,⁎a Department of Internal Medicine, Mayo Clinic, Rochester, MN 55905, USAb Mayo Comprehensive Hemophilia Center, Rochester, MN 55905, USA
Abbreviations: CAD, coronary artery disease; ACS, apercutaneous coronary intervention; HA, hemophilia AWillebrand disease; UA, unstable angina; NSTEMI, non-Stion; STEMI, ST-elevation myocardial infarction; ECG, elangiography; ASA, aspirin; PCC, prothrombin complexnant factor VIIa; ER, emergency room; UFH, unfractiovenous malformation; GI, gastrointestinal; BMS, bareartery bypass grafting; EUHASS, European Haemophright femoral artery; LFA, left femoral artery; DES, drugIU, international unit.⁎ Corresponding author at: Hilton 200 SCL, 200 Fi
55905. Tel.: +1 507 284 2677; fax: +1 507 284 8286.E-mail address: [email protected] (R.K. Pruthi)
0049-3848/$ – see front matter © 2012 Elsevier Ltd. Alldoi:10.1016/j.thromres.2012.02.050
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 14 December 2011Received in revised form 15 February 2012Accepted 28 February 2012Available online 23 March 2012Keywords:Acute coronary syndromeHemophiliaVon WillebrandAntiplatelet therapy
Introduction: Evidence-based guidelines for the management of acute coronary syndrome (ACS) in patientswith congenital bleeding disorders are lacking and largely confined to case reports.Methods: Outcomes of acute and long-term management of ACS in patients with mild hemophilia and vonWillebrand disease managed at our institution from 2000-2011 were reviewed.Results: Between 2000-2011, 8 patients (median age 74 years) experienced 10 ACS events. In the emergencyroom, 3 of 4 patients received aspirin 325 mg and intravenous unfractionated heparin therapy, with no acutebleeding complications. The 8 patients underwent 10 coronary angiography procedures. Prophylactic factorconcentrates were not administered for 6/10 (60%) of the procedures; bleeding complications (groinhematoma) occurred in 1/6 (17%). Two patients receiving bare metal stents and glycoprotein IIb/IIIa inhibitorinfusion with factor concentrates experienced no acute hemorrhagic complications. On discharge, aspirin
was initiated/continued in 6/10 events; the 2 patients receiving dual anti-platelet therapy for 1 month didnot receive factor concentrates and experienced no bleeding complications. During a median follow-up of8.5 years (1 – 11.5 years), 2 of 5 patients developed minor bleeding complications while on aspirin.Conclusion: Our data demonstrate that in patients with mild congenital bleeding disorders, despite notreceiving factor concentrates prior to coronary angiography, the acute management of ACS did not resultin severe hemorrhagic complications. Short-term dual anti-platelet therapy seemed to be well tolerated. Inpatients receiving long-term aspirin for secondary prevention for ACS, bleeding complications were mild,however such patients warrant close follow-up.© 2012 Elsevier Ltd. All rights reserved.
Introduction
The increasing longevity of patients with congenital bleedingdisorders parallels the prevalence of coronary artery disease (CAD)in this population of patients [1] and is reflected in the increasingnumber of case reports describing management of acute coronarysyndrome (ACS). Given the potential need for percutaneous coronary
cute coronary syndrome; PCI,; HB, hemophilia B; VWD, vonT-elevation myocardial infarc-ectrocardiogram; CA, coronaryconcentrates; rFVIIa, recombi-nated heparin; AVM, arterio-metal stent; CABG, coronaryilia Safety Surveillance; RFA,eluting stent; UNK, unknown;
rst Street SW, Rochester, MN
.
rights reserved.
intervention (PCI), anti-coagulant and anti-platelet medications,management of ACS, in this population of patients, poses a majorchallenge to both hematologist and cardiologist.
Lack of clinical trials precludes development of evidence basedguidelines, however, such efforts, based on expert opinion havebeen published [2]. Herein, we summarize our experience withoutcomes in managing ACS in patients with hemophilia A (HA),hemophilia B (HB) and von Willebrand disease (VWD).
Methods
After IRB approval, the medical records of all patients with HA, HBor VWD who presented with ACS or suspected ACS to our institutionbetween January 2000 and June 2011 were retrospectively identifiedusing the Mayo Clinic, Rochester Comprehensive Hemophilia Centerdatabase. The medical notes were reviewed, focusing on clinicaloutcomes (bleeding complications and transfusion requirements)and long-term follow-up. Individual patients were assigned a letter(e.g. D) and those who experienced more than one event wereassigned a letter and a number for each event (e.g. D1 and D2).

317M.Y. Lim, R.K. Pruthi / Thrombosis Research 130 (2012) 316–322
Inclusion Criteria
Patients were considered to have had ACS if they had the follow-ing diagnosis documented: unstable angina (UA), non-ST-elevationmyocardial infarction (NSTEMI) or ST-elevation myocardial infarction(STEMI). Patients were considered to have had suspected ACS if theypresented with chest pain with a non-diagnostic electrocardiogram(ECG) and normal serial cardiac biomarkers, but had a high pre-testprobability for CAD, warranting further diagnostic evaluation withcoronary angiography (CA).
Exclusion Criteria
Patients who had suspected ACS and proceeded to havenon-invasive diagnostic testing (ie exercise treadmill testing, exerciseimaging testing) with negative results were excluded. Patients whodevelop ACS during or within a week of administration of clottingfactor concentrates [FVIII, FIX, prothrombin complex concentrates(PCCs), recombinant factor VIIa (rFVIIa)] or desmopressin were alsoexcluded.
Results
Over the 11.5 year study period, 8 patients meeting our inclusioncriteria (mild HA, n=2; VWD type 1, n=4; type 2B, n=1; type2M, n=1) experienced 10 ACS or suspected ACS events. We excludedone in-patient who developed ACS post-factor concentrate infusionwhile undergoing orthopedic surgery. In addition, we had no patientswith severe bleeding disorder presenting with ACS. Themedian age atthe time of event was 74 years (range: 55 – 80) and 5 were male. Thepatient characteristics and details of their presentation and manage-ment of ACS are summarized in Table 1. Location of initial presenta-tion included emergency room (ER) (n=4 events), outpatient clinic(n=4 events) and in-hospital (n=1 event) where as one patientpresented to a non-Mayo Clinic outpatient facility and was subse-quently transferred to our facility.
Initial Management of ACS
Patients presenting to the ER were managed with anti-platelet(aspirin 325 mg, HD-ASA) and anti-coagulant (intravenous unfractio-nated heparin, UFH) therapy according to established guidelines[3–6]. One patient (patient C, type 2B VWD) did not receive eitherASA or UFH due to an arterio-venous malformation (AVM)-relatedgastrointestinal (GI) bleed with a presenting hemoglobin of 6 g/dL.Of the 5 patients that presented to the outpatient clinic, only 2patients (patient G and H) were started or continued on ASA; nonereceived UFH. Patient D2 developed in-hospital ACS and was contin-ued on ASA. Overall, there were no immediate bleeding complicationsfrom ASA or UFH use in the initial management of ACS.
Management of Coronary Angiography
Of the eight patients, 6 underwent one and 2 underwent two cor-onary angiography (CA) procedures. All procedures were performedvia a femoral arterial puncture. Prior to CA, prophylactic clotting factorconcentrates were not administered for 6/10 (60%) of the procedures.For the remaining 4 procedures, appropriate prophylactic factorconcentrates were provided pre-CA with the dosages calculated toachieve approximately 100% of their respective clotting factor levels.
Characteristics and Hemostatic History of Patients that did not ReceiveProphylactic Concentrates Pre-procedure
Patient B (baseline FVIII:C:68%; VWF:Ag:37%; VWF:RCo: 26%)was diagnosed with type 2M VWD at 57 years of age when he
underwent hemostatic testing after his son was diagnosed withVWD. He had undergone a prior hemostatically uneventful open re-duction and internal fixation of an ankle fracture about 10 yearsprior to the VWD diagnosis and had been on 81 mg ASA (LD-ASA)for CAD primary prophylaxis with no hemorrhagic complications.Based on this unremarkable hemostatic history, the treating hematol-ogist elected not to provide prophylactic VWF concentrates. Thispatient experienced a post-CA groin hematoma (detailed in Postangiography bleeding complications section below).
Patient D (mild HA, baseline FVIII:C 10%) underwent 2 CA (D1 &D2). For his first CA (D1), he was evaluated in the ER and diagnosedwith a STEMI. As he had ongoing chest pain, he proceeded emergentlyto the cardiac catheterization laboratory. He received factor concen-trate post-procedure. One month later, while hospitalized for conges-tive heart failure, he experienced recurrent chest pain and underwenta second CA (D2), for which he did not receive any prophylactic FVIIIconcentrate; the hemophilia center was not informed about thedecision to proceed with CA.
Patient F (type 1 VWD; baseline FVIII:C:88%; VWF:Ag:33%; VWF:RCo: 38%) underwent an outpatient CA, although his VWD was notedin the record, the hemophilia center was not notified of theprocedure.
Patient G (type 1 VWD; baseline FVIII:C: 64%; VWF:Ag:40%; VWF:RCo: 49%) had experienced ease of bruising, post-tonsillectomy andpost dental extraction hemorrhage and menorrhagia. Her pre-CAVWF levels were in the 80s (thought to be secondary to the use ofestrogen replacement therapy), thus, she received no prophylacticVWF concentrate and underwent an outpatient CA.
Patient H (mild HA, FVIII:C 23%) underwent an outpatient CAwith no prophylactic FVIII, although the patient's HA was noted onthe patients procedure record, the hemophilia center was notcontacted.
Post Coronary Angiography Bleeding Complications
Overall, post-CA bleeding complication occurred in 1/10 (10%) ofthe procedures or in 1/6 (17%) of the patients not receiving prophy-lactic concentrate infusion. The one bleeding complication occurredin patient B (type 2M VWD, hemostatic history outlined above)who did not receiving prophylactic concentrate. He developed a‘golf ball’ sized groin hematoma at the arterial puncture site24 hours after coronary angiography; despite manual pressure andintranasal desmopressin, the hematoma progressed requiring admin-istration of VWF concentrate. At 48 hours post-CA, the hematomaremained stable and he was discharged with the advice to use intra-nasal desmopressin as needed, however, there was no worsening ofthe hematoma and no neurovascular compromise. He received noVWF or desmopressin post-hospital discharge and he experiencedno further bleeding.
Post Coronary Angiography Outcomes
Initial management of the 8 patients undergoing CA, consisted ofbare metal stent (BMS) placement (n=2), coronary artery bypassgrafting (CABG) (n=4) and medical management (n=2). Of these,2 patients presented with recurrent ACS for which a second CA wasperformed (A1 and D2); both were medically managed.
Management of Patients that Underwent BMS Placement
During CA, 2 patients (D1 & E) received BMS placement withglycoprotein IIb/IIIa inhibitor infusion. Patient D1 (mild HA) received2 boluses of eptifibatide with no continuous infusion. Although he re-ceived no pre-CA FVIII concentrate, approximately 3 hours post-CAand BMS placement, VWF concentrate was erroneously administered.His post VWF concentrate infusion FVIII:C remained approximately
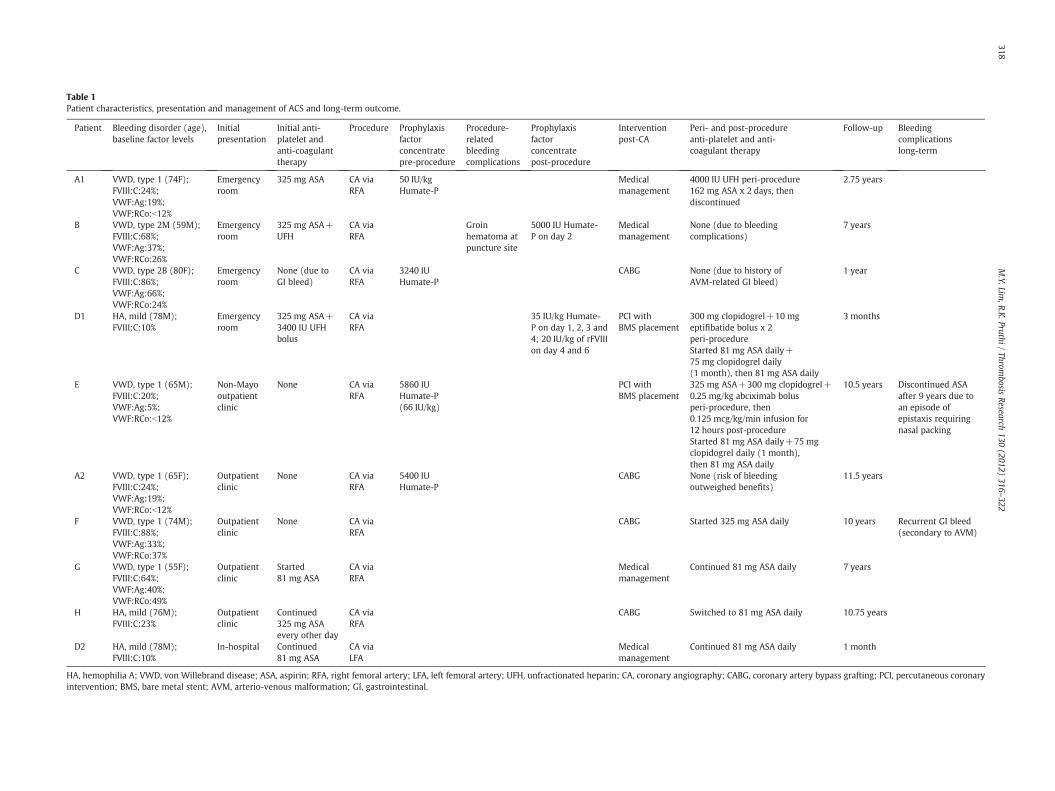
Table 1Patient characteristics, presentation and management of ACS and long-term outcome.
Patient Bleeding disorder (age),baseline factor levels
Initialpresentation
Initial anti-platelet andanti-coagulanttherapy
Procedure Prophylaxisfactorconcentratepre-procedure
Procedure-relatedbleedingcomplications
Prophylaxisfactorconcentratepost-procedure
Interventionpost-CA
Peri- and post-procedureanti-platelet and anti-coagulant therapy
Follow-up Bleedingcomplicationslong-term
A1 VWD, type 1 (74F);FVIII:C:24%;VWF:Ag:19%;VWF:RCo:b12%
Emergencyroom
325 mg ASA CA viaRFA
50 IU/kgHumate-P
Medicalmanagement
4000 IU UFH peri-procedure162 mg ASA x 2 days, thendiscontinued
2.75 years
B VWD, type 2M (59M);FVIII:C:68%;VWF:Ag:37%;VWF:RCo:26%
Emergencyroom
325 mg ASA+UFH
CA viaRFA
Groinhematoma atpuncture site
5000 IU Humate-P on day 2
Medicalmanagement
None (due to bleedingcomplications)
7 years
C VWD, type 2B (80F);FVIII:C:86%;VWF:Ag:66%;VWF:RCo:24%
Emergencyroom
None (due toGI bleed)
CA viaRFA
3240 IUHumate-P
CABG None (due to history ofAVM-related GI bleed)
1 year
D1 HA, mild (78M);FVIII:C:10%
Emergencyroom
325 mg ASA+3400 IU UFHbolus
CA viaRFA
35 IU/kg Humate-P on day 1, 2, 3 and4; 20 IU/kg of rFVIIIon day 4 and 6
PCI withBMS placement
300 mg clopidogrel+10 mgeptifibatide bolus x 2peri-procedureStarted 81 mg ASA daily+75 mg clopidogrel daily(1 month), then 81 mg ASA daily
3 months
E VWD, type 1 (65M);FVIII:C:20%;VWF:Ag:5%;VWF:RCo:b12%
Non-Mayooutpatientclinic
None CA viaRFA
5860 IUHumate-P(66 IU/kg)
PCI withBMS placement
325 mg ASA+300 mg clopidogrel+0.25 mg/kg abciximab bolusperi-procedure, then0.125 mcg/kg/min infusion for12 hours post-procedureStarted 81 mg ASA daily+75 mgclopidogrel daily (1 month),then 81 mg ASA daily
10.5 years Discontinued ASAafter 9 years due toan episode ofepistaxis requiringnasal packing
A2 VWD, type 1 (65F);FVIII:C:24%;VWF:Ag:19%;VWF:RCo:b12%
Outpatientclinic
None CA viaRFA
5400 IUHumate-P
CABG None (risk of bleedingoutweighed benefits)
11.5 years
F VWD, type 1 (74M);FVIII:C:88%;VWF:Ag:33%;VWF:RCo:37%
Outpatientclinic
None CA viaRFA
CABG Started 325 mg ASA daily 10 years Recurrent GI bleed(secondary to AVM)
G VWD, type 1 (55F);FVIII:C:64%;VWF:Ag:40%;VWF:RCo:49%
Outpatientclinic
Started81 mg ASA
CA viaRFA
Medicalmanagement
Continued 81 mg ASA daily 7 years
H HA, mild (76M);FVIII:C:23%
Outpatientclinic
Continued325 mg ASAevery other day
CA viaRFA
CABG Switched to 81 mg ASA daily 10.75 years
D2 HA, mild (78M);FVIII:C:10%
In-hospital Continued81 mg ASA
CA viaLFA
Medicalmanagement
Continued 81 mg ASA daily 1 month
HA, hemophilia A; VWD, von Willebrand disease; ASA, aspirin; RFA, right femoral artery; LFA, left femoral artery; UFH, unfractionated heparin; CA, coronary angiography; CABG, coronary artery bypass grafting; PCI, percutaneous coronaryintervention; BMS, bare metal stent; AVM, arterio-venous malformation; GI, gastrointestinal.
318M.Y.Lim
,R.K.Pruthi/
Thrombosis
Research130
(2012)316
–322

319M.Y. Lim, R.K. Pruthi / Thrombosis Research 130 (2012) 316–322
30 to 35% and eventually increased to 80% on day 4 post-CA; on thatday, his therapy was changed to recombinant factor VIII, which he re-ceived for two days. He did not experience any hemorrhagic compli-cations post-procedure.
Patient E (VWD type 1; baseline FVIII:C:20%; VWF:Ag: 5%; VWF:RCo: b12%) received 5860 IU Humate-P (66 IU/kg) pre-CA. DuringCA, he received a bolus of glycoprotein IIb/IIIa inhibitor (abciximab)which was continued post-CA for 12 hours. He did not experienceany post-procedure hemorrhagic complications.
Long-term Management of ACS
On discharge, ASA was started or continued in 6 events. PatientsD1 (mild HA) and E (type I VWD) received dual antiplatelet therapy(clopidogrel and LD-ASA) for one month post-BMS placement, andthen continued on LD-ASA. Both patients did not receive any prophy-lactic factor concentrates for the duration of dual anti-platelet agenttherapy; there were no minor or major bleeding complications. Inthe remaining 4 events, patients were dismissed without ASA, dueto bleeding complications (groin hematoma and AVM-related GIbleed) or based on the increased risk of bleeding which wereperceived to outweigh the benefit.
Long-term Follow-up
All patients were followed-up after discharge until death or theend date of the study. The mean duration of follow-up was 8.5 years(range 1 year – 11.5 years). Two patients (E and F) developedbleeding complications while on ASA. Patient E (type I VWD) stoppedLD-ASA after 9 years due to an episode of epistaxis requiring nasalpacking in the emergency department. Patient F (type 1 VWD) wasasked to stop HD-ASA after 2 years due to recurrent GI bleed ofuncertain etiology. HD-ASA was restarted 6 years later for secondaryprophylaxis for CAD. Unfortunately, a year later, he was hospitalizedfor another GI bleed, requiring blood transfusion and was subsequentfound to have a 1-cm colonic AV-malformation, which was treatedwith argon laser. The patient was discharged on LD-ASA and has notexperienced further hemorrhagic complications.
Discussion
Patients with bleeding disorders are experiencing similar age-related co-morbidity as the general population, of which obesityand CAD with attendant risk for ACS are common. The prevalence ofrisk factors for CAD have been documented in well designed epidemi-ological [1,7,8] studies, however, data on acute and chronic manage-ment of ACS remains confined to case reports and small series.
The use of factor concentrates has been associated with thrombot-ic events, including acute coronary syndromes [9,10]. The pathogene-sis of ACS associated with the use of factor concentrates appears to bedifferent from ACS de novo as it predominantly affects youngerpatients who often have no history or risk factors for cardiovasculardiseases [11]. To avoid potential bias in outcomes, we excluded pa-tients who develop ACS during or within a week of administrationof clotting factor concentrates [FVIII, FIX, prothrombin complex con-centrates (PCCs), recombinant factor VIIa (rFVIIa)] or desmopressinin our study.
We also performed a Medline search to identify case reports pub-lished in the English literature between January 2000 and December2010 that described the management of acute coronary syndromein patients with hemophilia A, hemophilia B or von Willebranddisease. Case reports were also obtained from cross-references. Casereports that reported the management of acute coronary syndromeoccurring after or during administration of clotting factor concen-trates [FVIII, FIX, prothrombin complex concentrates (PCCs), recombi-nant factor VIIa (rFVIIa)] or desmopressin were excluded.
Twelve reports were found in the literature, comprising 8 patientswith HA/HB [12–19] and 4 patients with VWD [20–23]. Initial andlong-term management of ACS, and short-term and long-term out-comes are summarized in Tables 2 and 3. In only 3/7 (43%) severeHA/HB reports did patients receive initial anti-platelet and/oranti-coagulant therapy. This heterogeneity in whether initial anti-platelet and/or anti-coagulant therapy was given, and in the dose ofanti-platelet and anti-coagulant therapy (if given), reflects the uncer-tainty involved in management despite clear guidelines from theACC/AHA taskforce for the general population [3–6]. 6/7 receivedclotting factor replacement therapy with no CA-related hemorrhagiccomplications. The one patient with moderate HA received LD-ASAand clotting factor replacement with no CA-related hemorrhage. Ofthe 4 VWD case reports, 3/4 received anti-platelet agents and 2/4 re-ceived VWF concentrate prior to CA, with no bleeding complications.
The traditional approach to managing invasive procedures in pa-tients with bleeding disorders has been to provide the appropriateclotting factor concentrate and to proceed with the appropriate inter-ventions as one would in patients without bleeding disorders. A newdimension in managing patients with bleeding disorders is theadditional consideration for use of anti-coagulant agents for variousindications such as ACS, atrial fibrillation and thromboprophylaxisin high risk situations such as orthopedic surgery.
Based on the data from the literature review, in the managementof ACS, coronary angiography and administration of appropriateanti-coagulant therapy appears to be safe, once the appropriateclotting factor concentrate has been provided, even in patients withsevere bleeding disorders. Yet a number of patients in our series didnot receive appropriate clotting factor concentrates. Prior to theintroduction of the electronic medical record, we relied on severalapproaches to ensure that patients with bleeding disorders weremanaged appropriately. These approaches included education andadvocacy on the part of the patient and/or family members, relyingon the patient carrying their bleeding disorders management guide-line or wearing their medical identifier on their person, having aprinted version of the treatment guideline on file in the emergencyroom and in the patient's paper medical record and finally, havingthe patient inform us directly anytime they were going to have aprocedure or were presenting themselves to the emergency roomand finally, anytime clotting factor was dispensed anywhere in the in-stitution, the hemophilia center would receive an email notification.These multiple ‘safety nets’, as our data demonstrate, were not infal-lible. Since the advent of the electronic medical record, our institutionhas been able to create a clinical alert ‘banner’ that is visible across thetop of the patients’ medical record once activated. The clinical alertbanner and easier access to the patient specific treatment guidelinehas led to elimination in the aforementioned error rates, thus demon-strating a meaningful use of the electronic medical record.
During coronary angiography, the choice of arterial access was thefemoral artery in all our patients. One patient who did not receiveclotting factor developed a groin hematoma, which reflects the in-creased risk of bleeding complications with femoral artery approach[24]. Radial artery approach is increasingly being used and likelysafer [2,25]. Dual antiplatelet therapy for 30 days is the standard ap-proach after PCI and placement of a BMS. For patients with bleedingdisorders, the use of prophylactic factor concentrate during thisperiod of time has been recommended [2,26]. Of the case reports of9 patients receiving stent placement, of whom 7 received dual anti-platelet therapy for at least a month, 2 patients received concomitantprophylactic factor concentrate while on dual anti-platelet therapy[12,17]. An additional 2 patients not receiving any prophylaxisexperienced increased minor bleeding frequency that resolved oncessation of clopidogrel [15,16]. They did not require factor replace-ment therapy or blood transfusion. In our series, the two patients(D1, mild HA and E, type 1 VWD) receiving a BMS did not receiveany prophylactic factor concentrate during that month and did not

Table 2Management of ACS and long-term outcome in hemophilia patients.
Report Type,severity(age)
Initial anti-plateletand anti-coagulanttherapy
Pre-procedureprophylaxis factorconcentrate
Procedure-relatedhemorrhagiccomplications
Typeof stent
Post-procedureprophylaxis factorconcentrate
Peri- and post-procedure anti-platelet andanti-coagulant therapy
Follow up Bleeding complications,type, date, interventions
Kim et al.(2010)
HA,severe(52)
None 2500 IU monoclonal FVIII None. Had 30 minutesof manual compressionat puncture site toprevent bleeding
BMS 1500 IUmonoclonal FVIIIat 12, 24 and 48 hrpost-procedure
300 mg clopidogrel+70 IU/kg UFH peri-procedure100 mg ASA daily+75 mg clopidogrel daily(1 month), then 100 mg ASA daily thereafter+regular FVIII supplements
10 months None
Coppolaet al.(2010)
HA,severe(63)
75 mg clopidogrel+2500 IU UFH bolus,then ~600 IU/hrUFH infusion
30 IU/kg rFVIII bolus, then1 IU/kg/hr rFVIII infusion
None None 1 IU/kg/hr rFVIIIinfusion continued
UFH continued 4 days Died, while awaitingcoronary artery bypassgrafting intervention
Ergelenet al.(2009)
HA,severe(60)
None None None None None None 5 days, thentransferred toanother hospitalfor surgicalintervention
None
Quineteroet al.(2008)
HA,severe(44)
325 mg ASA+600 mgclopidogrel+one doseof bivalirudin(0.7 mg/kg)
2500 IU rFVIII (unsure ifgiven pre- or peri-procedure)
None BMS Continued rFVIIIinfusion on day2 and 3
325 mg ASA daily+75 mg clopidogrel daily 2 years Clopidogrel discontinuedafter 4 months due togingival bleeding andecchymoses. Aspirincontinued
Ferrarioet al.(2007)
HA,severe(57)
100 mg ASA+300 mgclopidogrel+UFHinfusion
50 IU/kg rFVIII bolus, then25 IU/kg bolus 4 hr later,then 3 IU/kg/hr infusion
None BMS Continued rFVIIIinfusion peri- andpost-procedure
100 mg ASA daily+75 mg clopidogrel daily(1 month), then 100 mg ASA daily thereafter.Received prophylaxis rFVIII for 4 months
4 months None
Smolkaet al.(2007)
HA,moderate(62)
75 mg ASA 2500 IU monoclonal FVIII(35 IU/kg)
None BMS 1500 IUmonoclonal FVIIIat 12, 24 and48 hr post-procedure
70 IU/kg UFH peri-procedure+300 mg clopidogrel75 mg ASA daily+75 mg clopidogrel daily(1 month), then 75 mg ASA daily thereafter
5 months Frequent bleeding (jointhemorrhage, subcutaneousbleeding) and petechiaeduring dual anti-platelettherapy. No FVIIIadministered
Bovenziet al.(2003)
HB,severe(73)
None 30 IU/kg factor IX infusion None BMS None 5000 IU heparin+0.25 mg/kg abciximab bolusperi-procedure, then 2000 IU heparin+0.125 ug/kg/min abciximab infusion for 12 hrpost-procedureClopidogrel (1 month)
6 months None
Au et al.(2002)
HB,severe(31)
None Full factor replacement None UNK None Heparinization peri-procedure100 mg ASA daily+100 mg ticlopidine twicedaily (1 month)
6 months None
HA, hemophilia A; HB, hemophilia B; ASA, aspirin; UFH, unfractionated heparin; IU, international unit; BMS, bare metal stent; DES, drug eluting stent; UNK, unknown.
320M.Y.Lim
,R.K.Pruthi/
Thrombosis
Research130
(2012)316
–322

Table3
Man
agem
entof
ACS
andlong
-term
outcom
ein
vonW
illeb
rand
diseasepa
tien
ts.
Repo
rtTy
pe,
seve
rity
(age
)
Initiala
nti-platelet
andan
ti-coa
gulant
therap
y
Pre-proc
edure
prop
hylaxis
factor
conc
entrate
Proc
edure-relatedhe
morrh
agic
complications
Type
ofsten
tPo
st-procedu
reprop
hylaxisfactor
conc
entrate
Peri-an
dpo
st-procedu
rean
ti-plateletan
dan
ti-coa
gulant
therap
yFo
llow-up
Blee
ding
complications
,typ
e,da
ta,interve
ntions
Macdo
nald
etal.
(200
6)VW
D,typ
e1(5
6M)
ASA
3500
IUHem
ate-P,
then
1500
IUtw
iceda
ilyfor
48hr
pre-proc
edure
Non
e.Pa
ssivehe
mostaticde
vice
position
edov
erradial
artery
(pun
cturesite)ov
ernigh
trather
than
theus
ualfew
hoursforprecau
tion
DES
Continue
dHem
ate-P
Clop
idog
relloa
dan
dUFH
peri-procedu
rePo
st-procedu
remed
ications
notstated
1da
yEp
istaxison
day2,
requ
iring
cauterization
Fran
chinie
tal.
(200
4)VW
D,typ
e1(5
3M)
Non
e30
IU/kgHem
ate-P
Non
eUNK
Non
e40
00IU
hepa
rinbo
lustw
iceda
ily,the
n10
0mgASA
daily
+50
0mgticlop
idin
daily
UNK
Non
e
Arjom
andet
al.
(200
2)VW
D(4
5F)
ASA
Non
eNon
eBM
SNon
eIV
hepa
rinbo
lus+
tirofiba
nbo
lus
peri-procedu
re,the
nhe
parin+
tirofiba
ninfusion
for24
hrpo
st-procedu
reASA
+clop
idog
rel
3wee
ksNon
e
James
etal.(20
02)
VW
D,typ
e1(7
0F)
300mgASA
Non
eNon
eNon
eNon
eNon
e2mon
ths
Non
e
VW
D,v
onW
illeb
rand
disease;
ASA
,asp
irin;UFH
,unfractiona
tedhe
parin;
IU,interna
tion
alun
it;BM
S,ba
remetal
sten
t;DES
,drugelutingsten
t;UNK,u
nkno
wn.
321M.Y. Lim, R.K. Pruthi / Thrombosis Research 130 (2012) 316–322
report any minor or major bleeding complications. This suggests thatdual anti-platelet therapy is safe in patients withmild congenital bleed-ing disorders without prophylactic factor concentrate administration,however such patients should be closely monitored with appropriateintervention (initiation of prophylaxis ormodification of dual antiplate-let therapy) as indicated. An individualized discussion with the patientwould need to take place with a detailed review of the risks, benefitsand costs associated with management. For those with moderate andsevere bleeding disorders, data from the literature indicates that thereis an increased bleeding risk, thus prophylactic concentrates duringthis period of time should be considered.
Long-term treatment with low-dose aspirin is recommended forall patients with CAD, and this should be applicable to patients withcongenital bleeding disorders. None of the patients reported in theliterature who were on long term ASA appeared to have experiencedbleeding complications, although this could be due to the lack oflong-term follow-up, as the mean duration of follow-up was about6 months (range: 1 day - 2 years).
In our series, during long-term follow-up, 2/5 patients developedbleeding complications; one was secondary to an underlyingAV-malformation and the other occurred 9 years after initiation ofLD-ASA. Although somewhat reassuring, further observationalstudies are required to evaluate the long-term safety of anti-platelettherapy.
Given that patients with congenital bleeding disorders are a rarityin itself, it would be a challenge for a single institution alone to gathersufficient data to determine the optimal management. A multi-centerapproach is needed, similar to the European Haemophilia Safety Sur-veillance (EUHASS), where there is currently an ongoing prospectivesystem of collecting data on new cardiovascular events, its manage-ment and outcome. One approach is to expand the Centers for DiseaseControl and Surveillance Universal Data Collection tool to includesuch information to document outcomes; this will enable a moreevidence-based approach in determining the management of acutecoronary syndrome.
In conclusion, data from our small series of patients demonstratethat standard ACS management guidelines can be safely applied topatients with mild congenital bleeding disorders. When aggregatedwith data from the literature review, the same guidelines can beapplied to patients with moderate and severe congenital bleedingdisorders once appropriate clotting factor concentrates have beenadministered. However, optimal outcomes are predicated upongood communication between the health care team members,particularly, involvement of the Hemophilia Center at every step ofthe patient's management. In addition, long-term treatment withanti-platelet agents appears to be relatively safe and should beconsidered for all patients with coronary artery disease. Even thoughoptimal outcomes can be achieved in this population of patient, it isstill critical to emphasize the preventative aspects of CAD [27].
Conflict of Interest Statement
None.
References
[1] Kulkarni R, Soucie JM, Evatt BL. Prevalence and risk factors for heart disease amongmales with hemophilia. Am J Hematol 2005;79:36–42, doi:10.1002/ajh.20339.
[2] Schutgens RE, Tuinenburg A, Roosendaal G, Guyomi SH, Mauser-Bunschoten EP.Treatment of ischaemic heart disease in haemophilia patients: an institutionalguideline. Haemophilia 2009;15:952–8, doi:10.1111/j.1365-2516.2009.02020.xHAE2020 [pii].
[3] Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey Jr DE, et al.ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College ofCardiology/American Heart Association Task Force on Practice Guidelines(Writing Committee to Revise the 2002 Guidelines for the Management of Pa-tients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developedin collaboration with the American College of Emergency Physicians, the Society

322 M.Y. Lim, R.K. Pruthi / Thrombosis Research 130 (2012) 316–322
for Cardiovascular Angiography and Interventions, and the Society of ThoracicSurgeons endorsed by the American Association of Cardiovascular and Pulmonary Re-habilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol2007;50:e1–157, doi:10.1016/j.jacc.2007.02.013 S0735-1097(07)00511-6 [pii].
[4] Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, et al. ACC/AHAguidelines for the management of patients with ST-elevation myocardial infarc-tion: a report of the American College of Cardiology/American Heart AssociationTask Force on Practice Guidelines (Committee to Revise the 1999 Guidelines forthe Management of Patients with Acute Myocardial Infarction). Circulation2004;110:e82–292 110/9/e82 [pii].
[5] Antman EM, Hand M, Armstrong PW, Bates ER, Green LA, Halasyamani LK, et al.2007 Focused Update of the ACC/AHA 2004 Guidelines for the Management ofPatients With ST-Elevation Myocardial Infarction: a report of the American Col-lege of Cardiology/American Heart Association Task Force on Practice Guidelines:developed in collaboration With the Canadian Cardiovascular Society endorsed bythe American Academy of Family Physicians: 2007 Writing Group to Review NewEvidence and Update the ACC/AHA 2004 Guidelines for the Management ofPatients With ST-Elevation Myocardial Infarction, Writing on Behalf of the 2004Writing Committee. Circulation 2008;117:296–329, doi:10.1161/CIRCULATIO-NAHA.107.188209 CIRCULATIONAHA.107.188209 [pii].
[6] Harrington RA, Becker RC, Cannon CP, Gutterman D, Lincoff AM, Popma JJ, et al. Antith-rombotic therapy for non-ST-segment elevation acute coronary syndromes: AmericanCollege of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition).Chest 2008;133:670S–707S, doi:10.1378/chest.08-0691 133/6_suppl/670S [pii].
[7] Lim MY, Pruthi RK. Cardiovascular disease risk factors: prevalence and manage-ment in adult hemophilia patients. Blood Coagul Fibrinolysis 2011;22:402–6,doi:10.1097/MBC.0b013e328345f582.
[8] Ragni MV, Moore CG. Atherosclerotic heart disease: prevalence and risk factors inhospitalized men with haemophilia A. Haemophilia 2011, doi:10.1111/j.1365-2516.2011.02501.x.
[9] Girolami A, Randi ML, Ruzzon E, Zanon E, Girolami B. Myocardial infarction, other arte-rial thrombosis and invasive coronary procedures, in hemaophilia B: a critical evalua-tion of reported cases. J Thromb Thrombolysis 2005;20:43–6, doi:10.1007/s11239-005-2227-3.
[10] Girolami A, Ruzzon E, Fabris F, Varvarikis C, Sartori R, Girolami B. Myocardialinfarction and other arterial occlusions in hemophilia a patients. A cardiologicalevaluation of all 42 cases reported in the literature. Acta Haematol 2006;116:120–5, doi:10.1159/000093642 AHA2006116002120 [pii].
[11] Hough RE, Hampton KK, Preston FE, Channer KS, West J, Makris M. RecombinantVIIa concentrate in the management of bleeding following prothrombin complexconcentrate-related myocardial infarction in patients with haemophilia andinhibitors. Br J Haematol 2000;111:974–9 bjh2463 [pii].
[12] Kim DK, Kim DI, Kim MS, Lee EJ, Kim YB, Cho HJ, et al. Successful percutaneouscoronary intervention for acute coronary syndrome in a patient with severehemophilia a. Korean Circ J 2010;40:527–9, doi:10.4070/kcj.2010.40.10.527.
[13] Coppola A, De Simone C, Di CapuaM, Tufano A, Cimino E, Conca P, et al. Acute coronarysyndrome and severe haemophilia: an unusual associationwith challenging treatment.Thromb Haemost 2010;103:1270–2, doi:10.1160/TH09-11-0766 09-11-0766 [pii].
[14] Ergelen M, Osmonov D, Gunaydin ZY, Sahin O, Isik T, Uyarel H. Acute inferiormyocardial infarction in a patient with severe haemophilia A disease. Ann Hema-tol 2009;88:711–2, doi:10.1007/s00277-008-0663-9.
[15] Quintero D, Biria M, Meyers DG. Percutaneous coronary intervention in a patientwith acute ST-elevation myocardial infarction and hemophilia A. J InvasiveCardiol 2008;20:240–1.
[16] Smolka G, Kulach A, Dabek J, Szulc A, Gasior Z. Percutaneous coronary interven-tion with stent implantation in haemophilic A patient with unstable angina. Hae-mophilia 2007;13:428–31, doi:10.1111/j.1365-2516.2007.01436.x HAE1436 [pii].
[17] Ferrario C, Renders F, Cairoli A, Vuffray A, Spertini O, Angelillo-Scherrer A. Man-agement of an acute coronary syndrome in a patient with severe haemophilia A.Haemophilia 2007;13:763–5, doi:10.1111/j.1365-2516.2007.01530.x HAE1530[pii].
[18] Bovenzi F, De Luca L, Signore N, Fusco F, de Luca I. Abciximab for the treatment ofan acute thrombotic coronary occlusion during stent implantation in a patientwith severe hemophilia B. Ital Heart J 2003;4:728–30.
[19] Au WY, Jim MH, Lam CC. Unusual case of coronary artery disease in a patient withsevere hemophilia B. Am J Hematol 2002;69:152–3, doi:10.1002/ajh.10035 [pii].
[20] Macdonald J, Srinivasan M, More R. Percutaneous coronary intervention in apatient with von Willebrand's disease presenting with an acute coronary syn-drome. J Invasive Cardiol 2006;18:174–7.
[21] Franchini M, Veneri D. Are only haemophiliacs protected against ischemic heart dis-ease? Thromb Haemost 2004;92:1455, doi:10.1267/THRO04061455 04121455 [pii].
[22] Arjomand H, Aquilina P, McCormick D. Acute myocardial infarction in a patientwith von Willebrand disease: pathogenetic dilemmas and therapeutic challenges.J Invasive Cardiol 2002;14:615–8.
[23] James PR, de Belder AJ, Kenny MW. Successful percutaneous transluminalcoronary angioplasty for acute myocardial infarction in von Willebrand's disease.Haemophilia 2002;8:826–7 681 [pii].
[24] Kinnaird T, Anderson R, Hill J, Thomas M. Bleeding during percutaneous interven-tion: tailoring the approach to minimise risk. Heart 2009;95:15–9, doi:10.1136/hrt.2007.131284 hrt.2007.131284 [pii].
[25] Kiemeneij F, Laarman GJ, Odekerken D, Slagboom T, van der Wieken R. A random-ized comparison of percutaneous transluminal coronary angioplasty by the radial,brachial and femoral approaches: the access study. J Am Coll Cardiol 1997;29:1269–75 S0735109797000648 [pii].
[26] Mannucci PM, Schutgens RE, Santagostino E, Mauser-Bunschoten EP. How I treatage-related morbidities in elderly persons with hemophilia. Blood 2009;114:5256–63, doi:10.1182/blood-2009-07-215665 blood-2009-07-215665 [pii].
[27] Lim MY, Pruthi RK. Impact of lifestyle modification on symptomatic coronaryartery disease in a haemophilia patient with inhibitors. Haemophilia 2011, doi:10.1111/j.1365-2516.2011.02543.x.