outcomes in asperger syndrome wrexham, march 15, 2005
TRANSCRIPT
Outcomes in Asperger syndrome
Wrexham, March 15, 2005

• 1. General outcome
• 2. Deterioration in adulthood?
• 3. Psychiatric problems?
• 4. Forensic problems?
• 5. How can we improve outcome?

1. What do we know about outcome?
• Sources of data
• Personal accounts– Lawson, Holliday Willey, Grandin,
Gerland, Williams
• Clinical descriptions
• Systematic follow-up studies

Follow-up studies from child-adulthood (age 16-30+)
• 1950-1960’s: Anecdotal reports (Kanner; Eisenberg, Creak)
• 1969-1990’s: More systematic studies (Rutter, Lotter; Gillberg, Kobayashi; Ballabin-Gill)
• 1980’s on: Focus on more able individuals (Rumsey, Szatmari, Lord &Venter , Larsen, Mawhood, Tantam, Ballabin Gill, Howlin et al.)
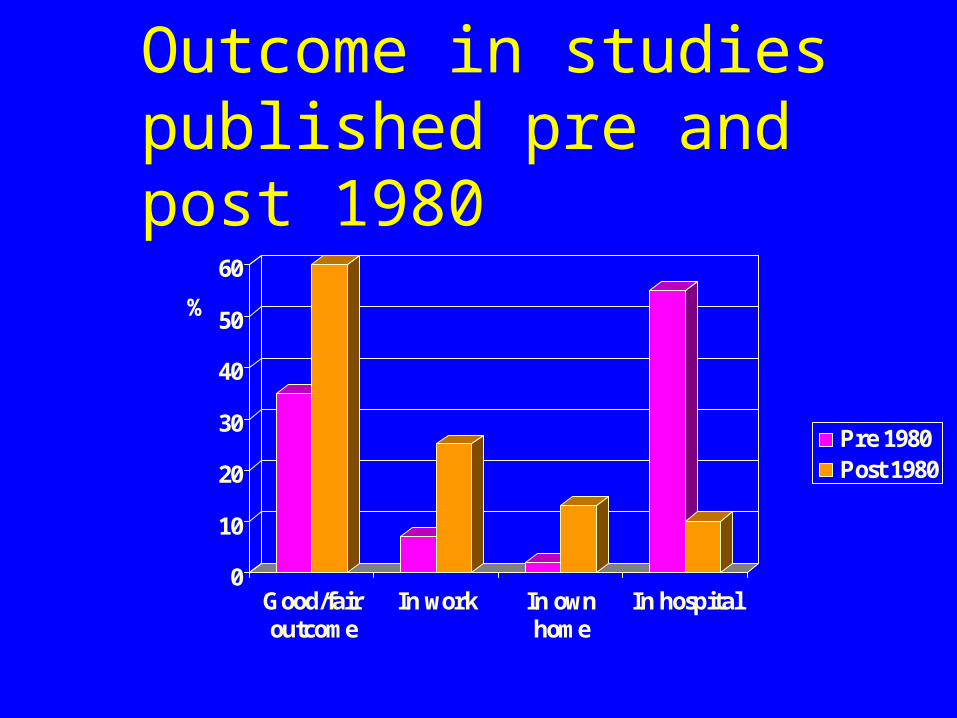
Outcome in studies published pre and post 1980
0
10
20
30
40
50
60
%
Good/fairoutcome
In work In ownhome
In hospital
Pre 1980Post 1980

Maudsley study- (Howlin, Goode, Hutton & Rutter, 2004)
• Group characteristics – N=68 (61 male, 7 female)– Age first seen 7 years – Age now 29 yrs – Diagnosis confirmed by ADI
– Initial PIQ 80 (51-137)

Principal school placement
0
5
10
15
20
25
30
35
40
45
Type of school
Mainstream
LD
Autistic
Other (EBD, Steiner etc)
%

Academic qualifications
0
10
20
30
40
50
60
70
80
College/universityGCE's+Diploma/GCSE'sNone
%

Residential status
0
5
10
15
20
25
30
35
Type of placement
IndependentShelteredWith parentsAutistic residOther residHosp. Care
%
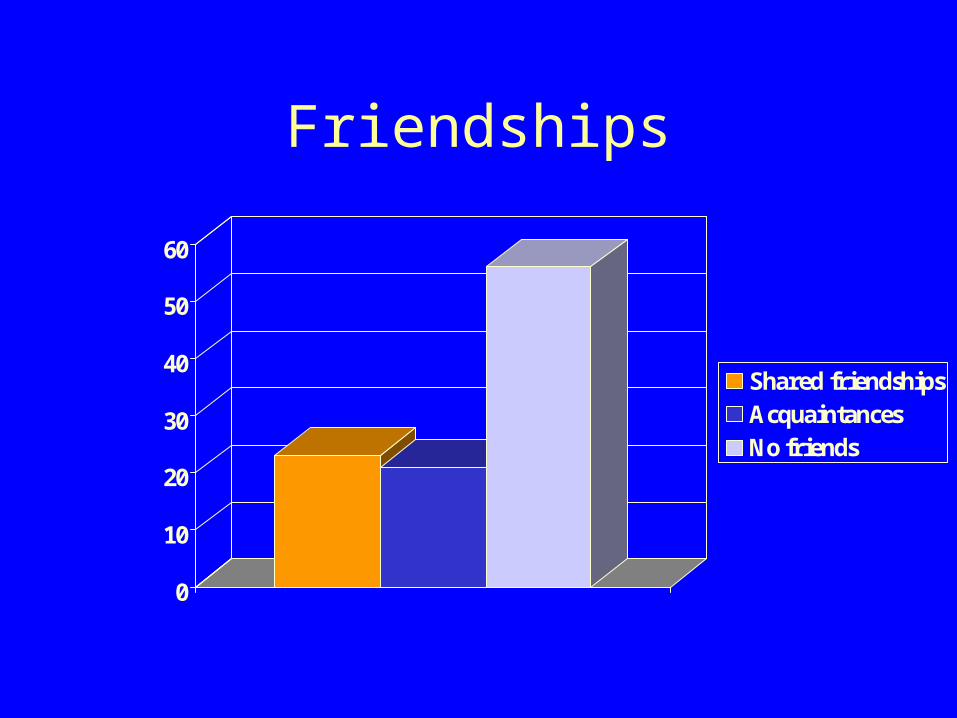
Friendships
0
10
20
30
40
50
60
Shared friendshipsAcquaintancesNo friends
%

Employment status
0
10
20
30
40
50
60
70
Type of job
IndependentVoluntaryShelteredNone
%
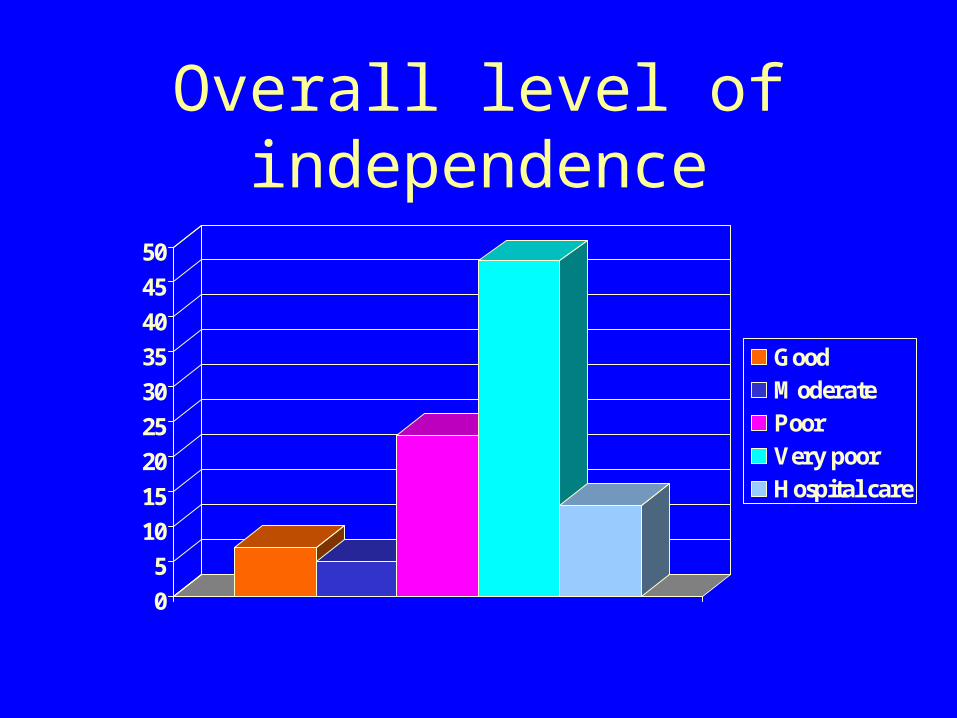
Overall level of independence
0
5
10
15
20
25
30
35
40
45
50
GoodModeratePoorVery poorHospital care
%

Predictors of outcome?

• High stability of IQ over time
• High correlations between child IQ and social/language abilities in adulthood
0
10
20
30
40
50
60
70
80
Non-verbal Verbal
Child IQAdult IQ
010
2030
405060
70
%Good/fair outcome
100+ 70-99 50-69
Initial PIQ level
Language
Social
However:
• IQ & Language not only predictive factors:
• Some adults with initial IQ>100 functioning much less well than those of IQ of 70
• Rituals/stereotyped behaviours & anxiety problems major impact on outcome for some

Relationship between IQ & ritualistic/stereotyped behaviours
0
10
20
30
40
50
60
% severe rituals
100+ 70-99 50-69
Initial IQ level

2. Do people with Asperger syndrome deteriorate in
adulthood?
Evidence of deterioration in adulthood
• Some follow-up studies indicate increases in problems over time – hyperactivity, aggression, destructiveness,
rituals, inertia, loss of language and “slow intellectual decline
• However, most report that 30- >40% of participants show marked improvements in late adolescence/early adulthood

Many follow-up studies report:
• Increases in verbal IQ
• Improvements in self awareness and self control
• Decreases in autistic symptomatology- social, communication and rituals/obsessions

• Kanner’s own (1973) follow-up of 96 adults found– Significant improvement often occurred in
mid/late teens as individuals became more aware of their problems and endeavoured to improve themselves
– Special interests often important in finding work and developing crucial contacts
3. Is there evidence of increased psychiatric disturbance in
adulthood?

• Systematic follow-ups do not report increased rates of schizophrenia using DSM criteria – Asperger, only 1 in 200 cases; Volkmar & Cohen,
1/163
• General conclusion is that rate is around 0.6%…no higher than in general population
• Wing = suggestions of increased risk “distressing without being constructive”

Psychiatric diagnoses in case studies of individuals with autism (N=200)
0
20
40
60
80
100
120
TOTAL DEPRESSIVE TYPE
Depression
Anxiety
Affective
Bipolar
Mania
Psychotic disorder, NOS
Schizophrenia
Catatonia
Other
N cases

Affective psychosis
• Most common type of psychotic disorder
• Often become worse in late adolescence/early adulthood
• May have delusional content associated with autistic obsessions
• Non-psychotic anxiety,depressive disorders, and attempted suicide also common
Incorrect diagnoses occur because:
• Many adult psychiatrists know little about developmental disorders (or mental retardation)
• Misinterpret symptoms due to patients’– inappropriate emotional responses
– inappropriate verbal responses
– unusual ways of describing symptoms
• Leading to incorrect conclusions and treatment

4. How common are forensic problems?

Examples of behaviours leading to problems with police
• Fascination with – poisons & chemicals guns; certain types of clothing;
washing machines; trains; cars
• Fire setting (or fire engines)• Particular dislikes (babies; noise) • “Sexual offences” - tend to be associated with
obsessions or lack of social understanding. • Very occasionally, cases of apparently
unexplained violence
Is there an increased rate of crime among people with autism/Asperger syndrome?
• Incorrect to base conclusions about incidence either on– Single cases – Atypical samples (e.g. Special hospital
population) – Anecdotal accounts/newspaper reports with no
confirmed diagnosis

Ghaziuddin et al., 1991
• Reviewed 132 reports of people with Asperger syndrome
• Only 3 had clear history of violent behaviour
• Conclude this much lower than the figure of 7% who commit violent crimes in the 20-24 year age group in the US.

However
• If problems do occur can be very difficult to resolve because of
• Lack of awareness of – social impact– implications for self– potential for harm
• Rigidity of beliefs• Obsessionality

Crucial to understand
• Factors leading to psychiatric and forensic problems in adults
• Desire for contact, without understanding the rules leads to:
• Misunderstanding of social cues• Misunderstanding by others
– Actions viewed as aggressive/psychotic
• Vulnerability– Teasing, bullying and misuse
• Lack of remorse & resistance to changing behaviour

• Often related to obsessional interests/preoccupations

5. How can the situation be improved?

Reduce factors likely to cause problems in adulthood
• Indications from some research (eg Lord & Venter, 1992) that extrinsic factors - ie support networks- may be just as important as individual variables
Improve education
• Increase understanding of educators
• Support necessary– to enhance positive social interactions – & to avoid negative ones
• Improve curriculum and aids for learning– structure, visual cues (TEACCH),
Address factors leading to psychiatric and forensic problems• Lack of structure & predictability
• Boredom ( >routines & rituals)
• Low self esteem
• Isolation from peer group
• Continuation of childhood behaviours that become unacceptable with age

Establish rules from early on
• Remember:
– What is clever, cute, charming at 3 (Mannerisms,attachments,obsessions/routines, inappropriate topics of conversation, social disinhibition) can be a disaster at 30!

Make use of existing skills to
• Encourage social contacts
• Increase social status
• Enhance self esteem
• Oddness may be tolerated/forgiven if compensated for by other skills

Creating an autism friendly environment
• Autism aware: – necessity of visual cues– disparity between verbal expression and
comprehension – importance of routines – limitations of choice; decision making

Creating an autism friendly environment
• Unconventional
• Controllable
• Predictable
• Consistent

• Improve opportunities for social inclusion
• Especially for work!

Supported employment for people with AS. Jobs found from 1995-2003
(Total =203)
0
10
20
30
40
50
60
1996 1997 1998 1999 2000 2001 2002 2003
Jobs found per year
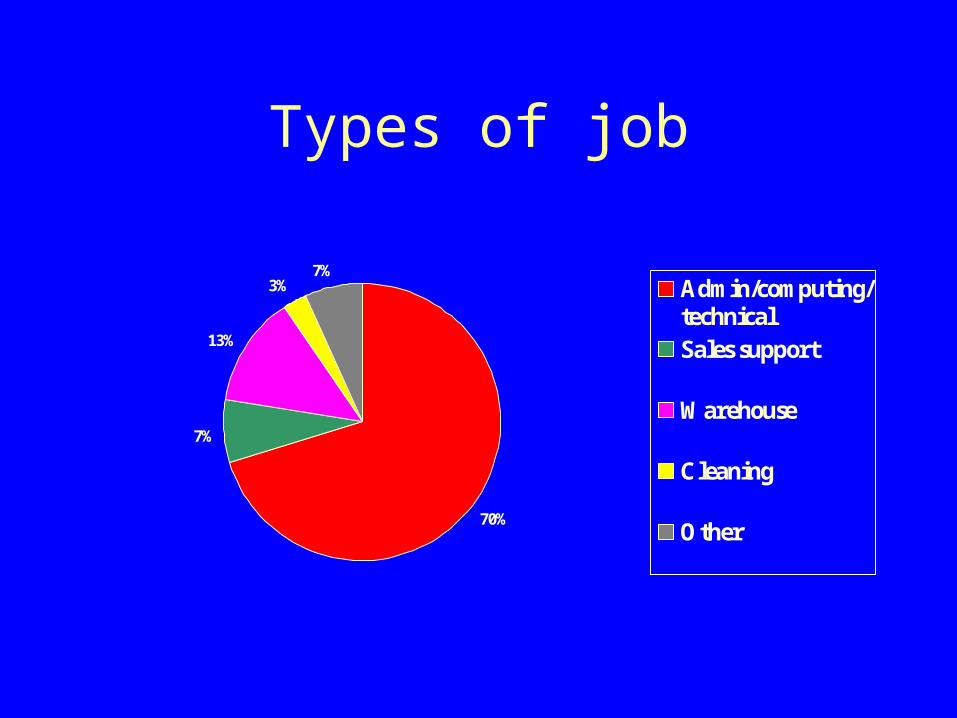
Types of job
70%
7%
13%
3%7%
Admin/computing/technicalSales support
Warehouse
Cleaning
Other

6. Future needs

Essential needs (1):
• Early diagnosis
• Management advice for parents (to avoid later problems; reduce rituals; establish acceptable social behaviours)
• Modification of special skills to promote social interactions/interests

Essential needs (2):
• Appropriate education
• Recognition by social, health and employment services of needs of adults with autism (especially those who are more able)
• Variety of options for supported and semi/independent living

Essential needs (3):
• Ways of improving social interactions (social skills groups; befriending schemes)
• Help for (more able) individuals to understand and cope with the “enigma” that is autism