otite media acuta con perforazione timpanica · acute otitis media rapid onset of signs and...
TRANSCRIPT

Otite media acuta con
perforazione timpanica
Paola MarchisioUOSD Pediatria ad Alta Intensità di Cura
Università degli Studi di Milano
Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico
Milano

Di chi parliamo?

Infezione prime vie respiratorie
Congestione mucosa vie respiratorie
Disfuzionetuba Eustachio
Accumulo secrezioni nell’orecchio medio
Risalitapatogeni dal nasofaringe
Perforazione spontanea della MT
NORMALITA’
OMAOME
PERFORAZIONE
Complicanza più frequente
10%>90%
GUARIGIONE PERFORAZIONE CRONICA

Incidenza

2,1 2,24,8
6,8
17,2
0
5
10
15
20
Italy UK Spain Germany Sweden
%
LIESE JG et al
Spontaneous tympanic membrane perforation Europe = 7%


OTITE MEDIA ACUTA vera o falsa o immaginata?
ACUTE OTITIS MEDIA
rapid onset of signs and symptoms of acute infection within
the middle ear, with evidence of effusion

IF each and every AOM diagnosisis not accurate
AOM count is wrong
ACUTE OTITIS MEDIA
rapid onset of signs and symptoms of acute infection within
the middle ear, with evidence of effusion

Valutare la potenziale associazione tra i polimorfismi a singolo nucleotide (SNPs) in geni selezionati e l‘otite media acuta ricorrente
Analizzare se le varianti genetiche possano predisporre, o meno, allo sviluppo di casi ricorrenti e complicati, come quelli con perforazione della membrana timpanica (PMT)

Analisi genetica
Per ogni bambino sono stati prelevati 3 ml di sangue intero
Sono stati selezionati 33 geni e 47 loro SNPs (polimorfismi a singolo nucleotide) da ricercare nei campioni ottenuti
Alcuni geni studiati
Gene dbSNP Descrizione HGVS Conseguenze funzionali Posizione (bp) Cr Locus genetico
IFNʏ rs12369470 NC_000012.12:g.68151116T>C Variante downstream 68151116 12 Intergenico
IL10 rs1800896 NG_012088.1:g.3943A>G Variante upstream 2KB 206773552 1 Intergenico
IL1α rs6746923 NC_000002.12:g.112795849A>G Variante upstream 112795849 2 Intergenico
IL1β rs1143627 NG_008851.1:g.4970C>T Variante upstream 2KB 112836810 2 Intergenico
IL8 rs2227306 NG_029889.1:g.5833C>T Variante intronica 73741338 4 Introne
TLR4 rs2737191 NC_000009.12:g.117700437A>G Variante upstream 117700437 9 Intergenico
Sono geni coinvolti nella regolazione del sistema immunitario, nella patogenesi dell'infiammazione e nella regolazione del metabolismo cellulare

Risultati
C/C C/T T/T
14,3%
61,9%
23,8%
16,4%
44,0%39,7%
SNP IL-10 rs1800896
Bambini con solo OMAR
Frequenze genotipiche
OR: 2,33 (95% IC: 1,17-4,77)
A/A A/G G/G
15,5%
41,7% 42,9%
20,7%
54,3%
25,0%
SNP IL-1α rs6746923
Bambini con OMAR e PMT
p=0,02 *
**OR: 0,44 (95% IC: 0,17-1,08)
* OR: 0,45 (95% IC: 0,22-0,89)
p=0,06 **
p=0,01

Conclusioni
Per quanto concerne l’OMAR con perforazione della MT
• Il SNP IL-10 rs1800896CT sembra ridurre il rischio di perforazione della MT
• Il SNP di IL-1α rs6746923AG sembra aumentare il rischio di OMA complicata
• Il SNP di IL-1α rs6746923A potrebbe avere un ruolo nel favorire la perforazione della MT

8,1 8,8
6,7
9,5
0
5
10
15
20
Total uncomplicated AOM only otorrhea mixed
%Spontaneous tympanic membraneperforation and immune deficiency
personal data - 2017

Eziologia
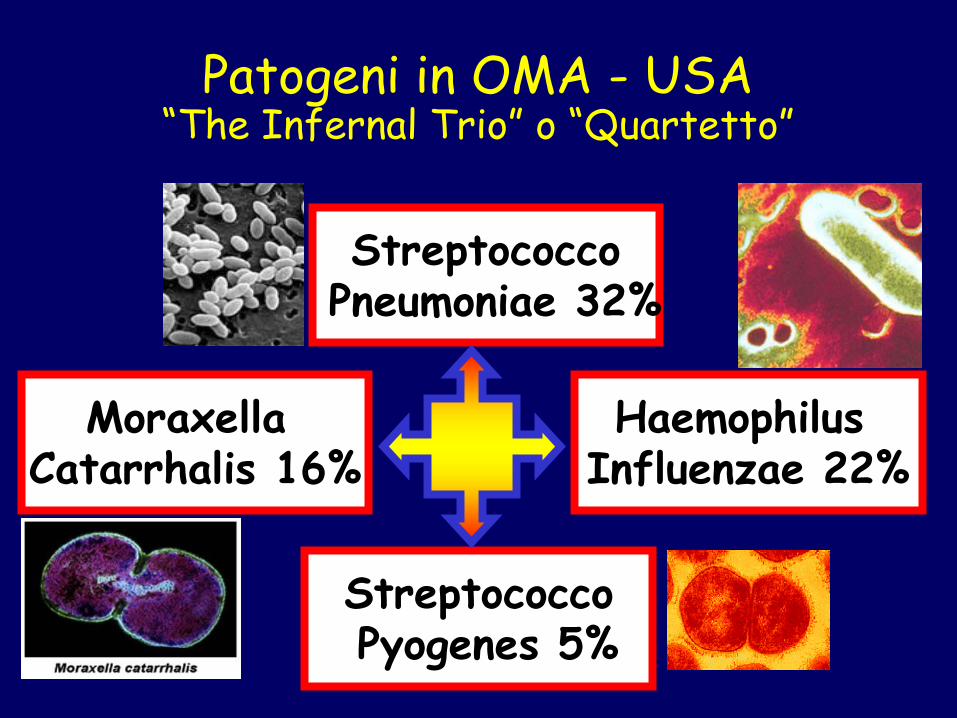
Patogeni in OMA - USA“The Infernal Trio” o “Quartetto”
StreptococcoPneumoniae 32%
StreptococcoPyogenes 5%
Haemophilus Influenzae 22%
Moraxella Catarrhalis 16%

No growth
Haemophilus influenzae
Staphylococcus aureus
Streptococcus pneumoniae
Streptococcus pyogenes
others
Moraxella catarrhalis
Isolates in 475 Italin children with acute otitis media [6 m - 12 a]Marchisio P et al. 8th International Symposium on Recent Advances in Otitis Media.
Fort Lauderdale; June 3–7, 2003
timpanocentesi[n: 145]
otorrea[n: 330]
28.3 %
22.8 %
14.5 %
2.7 %
2.7 %
3.4 %
25.6 %
13.6 %
32.7 %
20.9 %
3.3 %
1.2 %
5.1 %
23.0 %

Infection 2013; 41: 629

• prospective, single-center study, Italy
• enrollment for 12 months: May 1, 2015 to April 30,2016
• 177 previously healthy children (6 m – 7 yrs, mean age 3.5)
• 91% vaccinated with conjugate pneumococcal vaccine
• diagnosis of AOM with spontaneous otorrhea:
(a) middle ear effusion + signs of acute inflammation of the
tympanic membrane + acute symptoms and (b) otorrhea
(within 12 hours of spontaneous rupture of TM)

• excluded: tubes, midfacial abnormalities, chronic middle ear conditions, includingchronic perforation, immunodeficiency, antibiotics in the previous 2 weeks, topicaltreatment
• purulent fluid removed and MEE collected close to the perforation using an extra-thin flexible wire swab (Copan eNAT transport and preservation medium, Brescia, Italy).
• bacterial genomic DNA was extracted by clinical specimens by semi-automatic DNA extraction system. The presence of Streptococcus pneumoniae (S.pn) (and itsserotypes) , Haemophilus influenzae (Hi), Moraxella catarrhalis (M.cat), group A beta hemolyticus Streptocccus (GABHS) and Staphylococcus aureus was evaluatedby means of real-time PCR using specific oligos-probe sets. S.pn. cases were serotyped using primers and probes designed on the basis of the GenBankdatabase sequences (www.ncbi.nlm.nih.gov)


0,0% 10,0% 20,0% 30,0% 40,0% 50,0% 60,0%
S. aureus
S. pyogenes
S. pneumoniae
M. Catarrhalis
H. influenzae
11,3%
26,0%
27,1%
35,0%
50,8%
Culture – Italian data 2001 to 2011 Marchisio P et al., Infection, 2013
0,0% 10,0% 20,0% 30,0% 40,0% 50,0% 60,0%
10,7%
17,4%
19,4%
1,1%
51,0%
PCR – Italian data 2015 to 2016 Marchisio P et al., CMI, epub 2017
COMPARISON BETWEEN TIME AND DETECTION METHODS

In half of the cases 2 or more pathogens were identified.Non typeable H.Influenzae was the most frequent pathogen
(70%) in co-infections (M.catarrhalis GAS S.pneumoniae)

27,1
36,9
20,0 23,8
0
20
40
60
80
100
%
all
children
< 24
months
24-59
months
> 60
months
Streptococcus pneumoniae positive cases: age distribution
S. pneumoniae is still one of the main pathogens despite full immunization with
PCV13

0
20
40
60
80
100
all children < 24 m 24-59 m > 60 m
28 3329 30
77
6771 70
%
PCV13 ST non PCV 13 ST Streptococcuspneumoniae
positive cases: PCV13 versus non-
PCV13 serotypes
0
2
4
6
8
10
% p
os
itiv
e c
as
es
4
6B 9V 14
18
C
19
F
23
F 1 3 5
6A
7F
19
A
6C
/D 811
A/D
12
A/B
/F15
A/F
16
F
21
22
A/F
23
A
23
B24
A/B
/F33
F/3
7
35
B
35
F
38
no
nty
p
PCV7 PCV13 non PCV13
A significant
replacement
phenomenon has
developed,
reducing the
potential effect of
PCV13 on AOM
incidence

Terapia

OTITE MEDIA ACUTA - TERAPIA
Non antibiotico ?
Antibiotico subito?
Attesa vigile?

DIAGNOSI CERTA
LATERALITA’ bilaterale monolaterale
SEVERITA’ SINTOMI
grave lieve grave lieve
Età < 6 m. AB AB AB AB
Età 6 – 24 m. AB AB AB AV
Età > 24 m. AB AV AV AV
2010 – LG italiana –
OMA non complicata *
* NO OTORREA, NO RICORRENZA RECENTE, NO COMPLICANZE
AB = antibiotico immediato AV= possibile attesa vigile

2013 – AAP updated guidelines

OTITE MEDIA ACUTA - TERAPIA
Quale molecola?

• Non typeable H.influenzae , which is the most frequently pathogen
associated with biofilm formation, is predominant in spontaneous
otorrhea
• Group A Strep is confirmed to be a main cause of otorrhea, especially
in older children
• M. catharralis seems to be a relevant pathogen
• Co-infections are common , especially in children with recurrent AOM
and especially for NTHi
• The therapeutic approach should be different from that which is
usually reported for uncomplicated AOM, taking into account the
possible formation of biolfim and the presence of betalactamase
producers

Prevenzione

Occurrence of AOM (≥1 episodes) during the 6-months study
period: all children
54,4
82,2
0
20
40
60
80
100
%
influenza vaccine controls
p = 0.004
EFFICACY 33,8%
Marchisio P et al, PIDJ 2009

41,7
79,669,1
85,4
0
20
40
60
80
100
%
non complicated AOM complicated AOM
influenza vaccine controls
p = 0.002
p = NS
EFFICACY 47,6% EFFICACY 19,0%
Marchisio P et al, PIDJ 2009

• The study involved a total of 116 children aged 1 to 5 years witha history of rAOM
• Children were randomized to receive 1.000 IU/day by mouth for4 months or placebo
• The study was conducted double-blind
• Two extra months of follow-up were planned, for a total of 6months
• All the children had to return to the center for a control visit(anamnesis, complete physical examination, pneumaticotoscopy, tympanometry) every month
• A blood sample was obtained from each enrolled child atenrolment and within 2 days after the end of supplementation inorder to determine the serum vitamin D concentration

0.0
00.2
50.5
00.7
51.0
0
0 30 60 90 120 150 180
Time (days after randomisation)
ControlsTreated with vitamin D
complicatedwith othorrea AOM episodes
0.0
00.2
50.5
00.7
51.0
0
0 30 60 90 120 150 180Time (days after randomisation)
Controls
Treated with vitamin D
0.0
00.2
50.5
00.7
51.0
0
0 30 60 90 120 150 180Time (days after randomisation)
Controls
Treated with vitamin D
uncomplicatedAOM episodes
Efficacy of vitamin D3 1000 U/day (Nov through March) in children 1 – 5 yrs old with a history of rAOM
ALL episodes
Marchisio P et al. PIDJ 2013
Reduction
32% (p=0.03)

Is CAM effective in the treatment or
prevention of perforated
acute otitis media?
NO
a) Homepathy NO
b) Echinacea NO
c) Osteopathy NO
d) Propolis YES (29%) in uncomplicated AOM
e) Xylitol YES (9%) (in uncomplicated AOM)


16 studies of long-term antibiotic use (review
published in 2006, updated in 2010)
prevention of 1.5 episodes of AOM per year,
reducing in half the number of AOM episodes
during the period of treatment
PROFILASSI ANTIBIOTICA

Futuro

• periodical monitoring of pneumococcal ST circulation
after introduction of PCV with a defined number of ST is
needed in order to evaluate replacement phenomenon
and the need for new vaccines with greater protective
activity
• evaluation of new systemic treatments (broader
antibiotics to cover H.influenzae)
• assessment of nasopharyngeal microbiota
• easier (and early) identification of children prone to
perforation


Grazie per
l’attenzione! Never look for the
extraordinary, but, on the
contrary, concentrate on the
more prevalent and common
diseases, and try to cure them
These are the diseases you
will most frequently encounter
in your practice”
Emile Ménière
Deuxième Congrés
Otologique Internationale
Milan 1880