other changes related to pps and conclusions. carl suetens (ecdc)
TRANSCRIPT

ECDC PPS 2016-2017 protocol: other changes
Carl Suetens
Surveillance section, surveillance and response support unit European Centre for Disease Prevention and Control (ECDC)

Antimicrobial stewardship & antimicrobial use (1/4)
FTE dedicated antimicrobial stewardship consultancy “Antimicrobial stewardship refers to a coordinated programme that implements interventions to ensure appropriate antimicrobial prescribing in order to improve clinical efficacy of antimicrobial treatment, to limit AMR and to prevent Clostridium difficile infections. Antimicrobial stewardship contributes to high quality and effective healthcare through decreasing unnecessary antimicrobial-related morbidity and mortality and limiting selective pressure to minimize development of resistance to currently effective antibiotics.”
– Full-time equivalent (FTE) is the proportion of a full time position/job. 0.10 FTE is 10% of a full time position.
– dedicated time of an (‘external’) consultant - NOT the time spent by clinicians as part of daily practice.
– Salary support: (at least part of) job description
– deduct % ASt time from FTE IPC doctor if appropriate, and report separately

Antimicrobial Stewardship indicators
Antimicrobial stewardship & antimicrobial use (2/4)
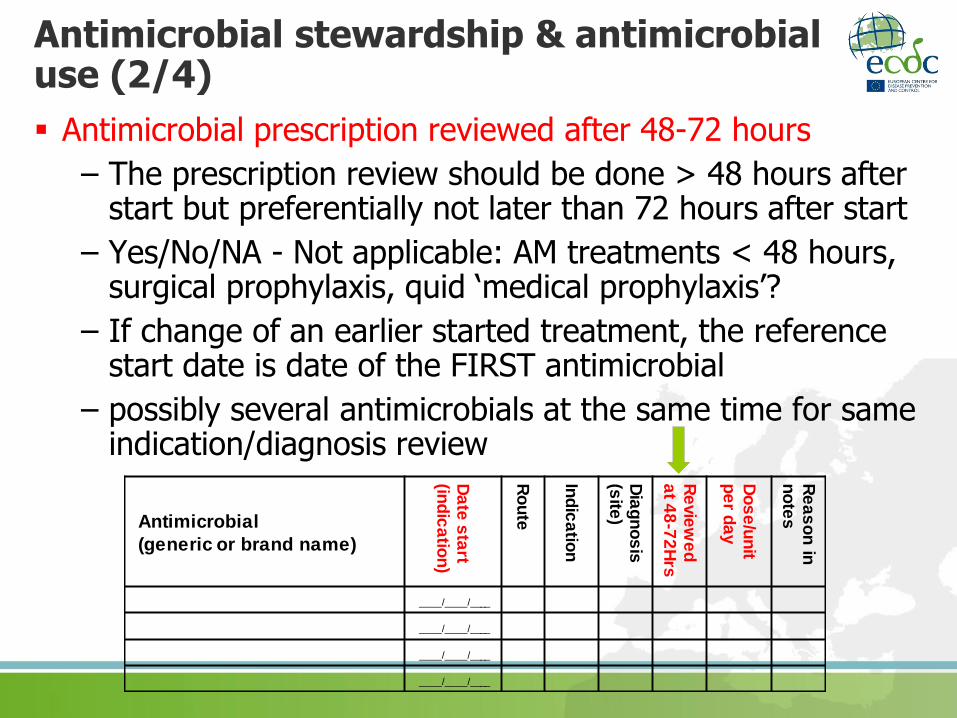
Antimicrobial prescription reviewed after 48-72 hours
– The prescription review should be done > 48 hours after start but preferentially not later than 72 hours after start
– Yes/No/NA - Not applicable: AM treatments < 48 hours, surgical prophylaxis, quid ‘medical prophylaxis’?
– If change of an earlier started treatment, the reference start date is date of the FIRST antimicrobial
– possibly several antimicrobials at the same time for same indication/diagnosis review
Antimicrobial
(generic or brand name)
Da
te s
tart
(ind
ica
tion
)
Ro
ute
Ind
ica
tion
Dia
gn
os
is
(site
)
Re
vie
we
d
at 4
8-7
2H
rs
Do
se
/un
it p
er d
ay
Re
as
on
in
no
tes
____/____/____
____/____/____
____/____/____
____/____/____

Antimicrobial stewardship & antimicrobial use (3/4)
Date start antimicrobial (indication)
Objectives: • Burden estimates antimicrobial use
• Reference date post-prescription review
• Proportion CI treatment with AM onset on Day 3 or later (validation parameter)
• Antimicrobials started in-hospital, check SP3 indication
If change of earlier started AM, record date of FIRST AM
Antimicrobial
(generic or brand name)
Da
te s
tart
(ind
ica
tion
)
Ro
ute
Ind
ica
tion
Dia
gn
os
is
(site
)
Re
vie
we
d
at 4
8-7
2H
rs
Do
se
/un
it p
er d
ay
Re
as
on
in
no
tes
____/____/____
____/____/____
____/____/____
____/____/____

Antimicrobial stewardship & antimicrobial use (4/4)
Dosage/unit per day
– Strong request ESAC-Net
– TATFAR Rec #2: EU=DDD, US=Days of Treatment (DOT): How to compare antimicrobial use between US and EU???
– Valuable information at ecological level
– Needed for DDD definition update in EU
– OPTIONAL
Antimicrobial
(generic or brand name)
Da
te s
tart
(ind
ica
tion
)
Ro
ute
Ind
ica
tion
Dia
gn
os
is
(site
)
Re
vie
we
d
at 4
8-7
2H
rs
Do
se
/un
it p
er d
ay
Re
as
on
in
no
tes
____/____/____
____/____/____
____/____/____
____/____/____

Other PPS II changes 1/4
Hospital ownership private/public
Hospital merger approach similar to ESAC-Net
=> how to record hospital specialty (primary/secondary/tertiary/specialised)?
Ward specialty:
– only main categories + neonatal
– If PED or NEO: combine with patient specialty
Hospital is part of merger: No Yes
Data apply to: Hospital site Merger
N of beds merger: Total Acute care
Other PPS II changes 2/4
Patient-based data:
– Birthweight for neonates (grams) – or gestational age (weeks)?
– Deletion ward specialty (ward data also in standard)
HAI data: HAI associated to current ward
– Yes = Onset > Day 2 in current ward
– No = Present on admission, onset on D1 or D2
– Unknown (optional variable)
– Objective: increase value PPS for ICU, haemato, other specialties

Include chronic/long-term care wards in acute care hospital
Add new specialty for healthy babies: PEDBAB: healthy baby on paediatric ward, GOBAB: healthy baby on obstetric ward
Adapt case definition pneumonia if underlying pulmonary/cardiac disease (2 X-rays rarely available): also consider previous X-rays
AMR definition: adapt to EARS-Net: report R only, not I+R
Other PPS II changes 3/4

September 2013 meeting: “More discussion needed”
– Surgery since admission: keep current categories? (NHSN/non-NHSN)?
– Change AM diagnosis list?
– Add LTCF to HAI origin?
– Body mass index ? (CDC)
(Almost) all new variables are OPTIONAL
Other PPS II changes 4/4

Conclusions of discussions 1/3
Structure and process indicators:
– Hospital level:
• Staff ratio: inclusion of interim/bank nurses, not students
• Multimodal strategies table: ICU/non-ICU, education/checklist/audit
• Participation to surveillance networks: add ‘other’
• Microlab results during weekends: separate clinical/screening tests
• Drop percentage of absenteeism
• Add number of airborne infection isolation rooms at hospital level
• OK for other indicators, move of single rooms to ward level
– Ward level:
• Add post-prescription review yes/no (moved from antimicrobial use)
• Percentage HCW with AHR in pocket: numerator and denominator (small numbers) – consider counting ‘non-empty’ bottles only?
• OK for other indicators
Conclusions of discussions 2/3
Patient risk factors:
– birth weight for neonates: agreed
– BMI: no
Antimicrobial use:
– Drop post-prescription review at antimicrobial level, move to ward level
– Date start antimicrobial/indication and dosage: agreed
HAI data:
– Association to current ward: agreed
– AMR markers: change from non-susceptible (I/R) to resistant (as in EARS-Net)?: needs more discussion
• Not possible or very difficult for several countries
• ‘R only’ is not in agreement with ECDC/CDC definition of ‘MDR’, ‘XDR’ and ‘PDR’ as in Magiorakos et al. , Clin Microbiol Infect 2012; 18: 268–281
Conclusions of discussions 3/3
Hospital data:
– OK to add hospital ownership & change merger approach
Ward data: OK to simplify ward specialty (and drop ward specialty from patient data)
Other: YES:
– inclusion of long term wards, add ‘LTC’ to ward specialty
– add PEDBAB/GOBAB (depending on country) for healthy babies
– Change PNEU definition as agreed in Sep 2013
– Drop categories NSHN/non-NSHN surgery (but: significant risk difference!)
Other: NO: inclusion of HAIs on admission associated with LTCF stay (add LTCF to HAI origin)