otc exam 2 study guide
TRANSCRIPT

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 1/32
OTC Exam 2 Study Guide
1 | P a g e
Nutrition/Vitamins: Klucken
Understand importance of nutrition and reasons for
supplementation
• What is the preferred source of nutrients?
• Food
• Why?
• Better absorption
• What are the risks of nutritional deficiencies?
• Compromised growth and development
• Contribute to chronic diseases
• Exacerbate aging process
• What are some of the dangers of supplementation?
• Delay medical care
• Risk of ADRs with exceeding recommended intake• Drug-nutrient interactions
• List various etiologies of nutritional deficiency
• What is the stages that causes of nutritional deficiencies?
• Inadequate intake
• Decreased absorption
• Increased metabolic requirements
• Medications
• Lack of knowledge
Appreciate diverse clinical presentation of various deficiencies
• What are the difficulties identifying nutritional deficiencies?
• symptoms not present until deficiency occurs
• symptoms overlap with other deficiencies
• What are the stages of evolution of nutritional deficiency?
• Inadequate synthesis or absorption
• Depletion of nutrient stores
• Biochemical changes• Physical manifestations of deficiency
• Morbidity and mortality
Be familiar with supplement dosing and labeling
• What is the intent of supplementation?
• Maintain present status
• Prevent deficiencies
• Replenish compromised stores
• Treat medical conditions
• What are the four DRI categories?• EAR: Estimated ave (half) requirements
• RDA: reference daily intake
• AI: adequate intake (lacks data)
• UL: tolerable upper intake
• What is the importance of supplement labeling?
• Indicates %DV
• List three problems that result because supplements are not
regulated by the FDA.
• Potential disparity of contents vs. label
• Do not require proof of safety or efficacy
• Do not require inspection of production• What does USP labeling indicate has been verified?
• Ingredients and amounts
• Effective disintegration and dissolution for absorption
• Absence of harmful contaminants
• Safe, sanitary, well-controlled manufacturing

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 2/32
OTC Exam 2 Study Guide
2 | P a g e
VITAMIN DEFICIENCIESCondition Symptoms Cause Non-Pharm Treatment Pharmacological
Vitamin A Deficiency Night Blindness
(usually first
symptom)
Dry/hardening of the
skin
Infections
Excess excretion of Vit A
Fat Malabsorption (little
absorption of fat due to
drugs or condition)
Natural Sources of
Vitamin A Vitamin A Supplement
(Must be medically
diagnosed)
Refer for any vitamin A
deficiency because OTC
supplement without
diagnosis is only intended
to:
Maintain present status
Prevent deficiency
Replenish compromised
stores (not intended
for self-treatment of vitamin deficiencies_
Vitamin D Deficiency Rickets
Osteoporosis
Muscle Weakness
Increased Risk of Falls
Colon, prostate, breast
cancer
Inadequate intake
GI Disease
Chronic Renal Failure
Inadequate sunlight
Long-term Phenytoin
Therapy
Liver/Kidney
Dysfunction
Natural Sources of
Vitamin D
Vitamin D Supplement
(Must be medically
diagnosed)
Refer for any vitamin D
deficiency because OTC
supplement without
diagnosis is only intended
to:
Maintain present status
Prevent deficiency Replenish compromised
stores (not intended
for self-treatment of
vitamin deficiencies)

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 3/32
OTC Exam 2 Study Guide
3 | P a g e
Vitamin E Deficiency Neurological
Abnormalities
Muscle pain, ache,
cramp, numbness or
sense of fatigue
(intermittent
claudication) Muscle weakness
Hemolytic anemia
Premature, low birth
weight
Fat Malabsorption
Natural Sources of
Vitamin E *DO NOT TAKE
WITHOUT PHYSICIAN
DIAGNOSIS*
Vitamin E Supplement
(Must be medically
diagnosed)
Refer for any vitamin Edeficiency because OTC
supplement without
diagnosis is only intended
to:
Maintain present status
Prevent deficiency
Replenish compromised
stores (not intended
for self-treatment of
vitamin deficiencies)
Vitamin K Deficiency Unusual Bleeding
Prolonged PT (time it
takes for blood clot to
form)
Osteoporotic Fractures
Reduction in gut flora
that produces Vit K
Malabsorption
syndromes
Bowel resections
Liver Disease
Antibiotic therapy
Natural Sources of
Vitamin K
Vitamin k Supplement
(Must be medically
diagnosed)
Refer for any vitamin k
deficiency because OTC
supplement without
diagnosis is only intended
to:
Maintain present status
Prevent deficiency
Replenish compromised
stores (not intended
for self-treatment of
vitamin deficiencies)

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 4/32

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 5/32
OTC Exam 2 Study Guide
5 | P a g e
Iron Deficiency Iron Deficiency Anemia
(IDA)
Pallor(pale appearance)
Fatigue
Blood Loss
Malabsorption
Inadequate diet
Erythropoietin (EPO)
w/o iron
supplementation
Natural Source of
Calcium
Iron Supplement
Magnesium Deficiency Neuromusculaririitability
Increase CNS
stimulation: Delirum
and convulsions
Hypocalcemia and
Hypokalemia (low
potassium) cannot be
corrected unless
Magnesium is within
normal levels
GI losses Renal losses
Natural Sources of Magnesium
Magnesium Supplement
OTC SUPPLEMENTSDrug Indication Dosing Interactions Exclusion
Vitamin A
Retinoids: retinol
Carotenoids: alpha-
carotene, beta-carotene)
Natural Sources
Dark green vegetables Red, Orange, or deep
yellow vegetables and
fruits
Liver, Liver fat, egg yolk
Normal Growth and
Development
Bone development
Proper organ function
Eye health
Epithelial cell mucoussecretions
Not Important for this
exam Warfarin: increase in
anticoagulation
Cholestyramine,
colestipol, mineral oil:
decrease absorption of
Vitamin A
Anyone who is on blood
thinners
Smokers have an
increased risk of
cancer,CVD, and death
w/ Beta-Carotene People at risk for bone
fractures
Pregnancy: increase risk
of birth defect/liver
abnormalities

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 6/32
OTC Exam 2 Study Guide
6 | P a g e
Vitamin D
Cholecalciferol (D3) –
naturally occurring
Ergocalciferol (D2) –
food additive
Calcitriol – Active form
of Vit D that aids inabsorption of calcium
Natural Sources
UV Light
Milk, egg yolk, liver,
salmon, tuna, sardines,
milk fat
Proper bone/mineral
formation
Increase calcium and
phosphate absorption
Improves renal
reabsorption of
calcium Maintains serum
calcium and
phosphorous levels
600-800 IU/day
Max Dose: 4000 IU /day
(100mcg/day)
(1mcg = 40 IU Vitamin
D)
Phenytoin,
carbamazepine,
barbituates: increase
metabolism of Vit D
Cholestyramine,
colestipol, mineral oil:
decrease absorption of Vit D
Patients at risk of
hypercalcemia
Patient at risk of kidney
stones
Patient at risk of renal
failure
Patients with cancer
Vitamin E
Tocopherols
Tocotrienols
Natural Sources
Wheat germ Vegetable Oils
Margarine
Green Leafy Vegetables
Milk Fat
Egg Yolk
Nuts
Antioxidant
Hemebiosynthesis
(Creates heme groups
which carry oxygen)
Steroid metabolism Collagen formation
Prevents stretch
marks
15mg/day
Max Dose: 1000mg/day
**@ 400 IU/day can
cause death in some
patients**
Warfarin: Increase
coagulation
Cholestyramine,
colestipol, mineral oil :
decrease absorption of Vit E
Do not take without
medical referral
Patients @ risk of
Chronic Heart Failure
(CHF) Patients @ risk of
hemorrhagic stroke
May cause fetal loss

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 7/32
OTC Exam 2 Study Guide
7 | P a g e
Vitamin K
Phytonadione (K1) –
vegetables
Menaquinone (K2) –
Product of bacterial
metabolism (produced
in the gut) Menadione (K3) –
synthetic (3x potency)
Natural Sources
Liver
Vegetable Oil
Spinach
Kale
Cabbage
cauliflower
Promotes the
synthesis of clotting
factors
Activates clotting factors
Activate coagulation
protein C & S
Activation of osteocalcin- bone mineralization
Not needed for this
exam Warfarin: Decreased
anticoagulation
Broad Spectrum
Antibiotics reduce
vitamin K via gut Flora
Vit A & E: reduce vit Kactivity
Cholestyramine,
colestipol, mineral
oil :Decreased
absorption of Vit K
Do not take if you are on
blood thinners
**NEED DOCTOR
EVALUATION IF YOU
ARE AT RISK FOR
STROKE OR CHF**
Vitamin C
Ascorbic AcidNatural Sources
Green & Red Peppers
Broccoli
Spinach
Tomatoes
Potatoes
Strawberries
Citrus Fruits
Kiwi
Reducing agent
Help absorption of non-
heme iron (ferric ->
ferrous)
Claims to prevent and
treat common cold
(unsupported)
Not important for this
exam
Cholestyramine,
colestipol, mineral oil :Decreased
absorption of Vit C
Rare side effects:
Nausea, stomachcramps, diarrhea,
nephrolithiasis
Creates acidic urine

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 8/32

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 9/32

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 10/32

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 11/32

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 12/32
7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 13/32

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 14/32
OTC Exam 2 Study Guide
14 | P a g e
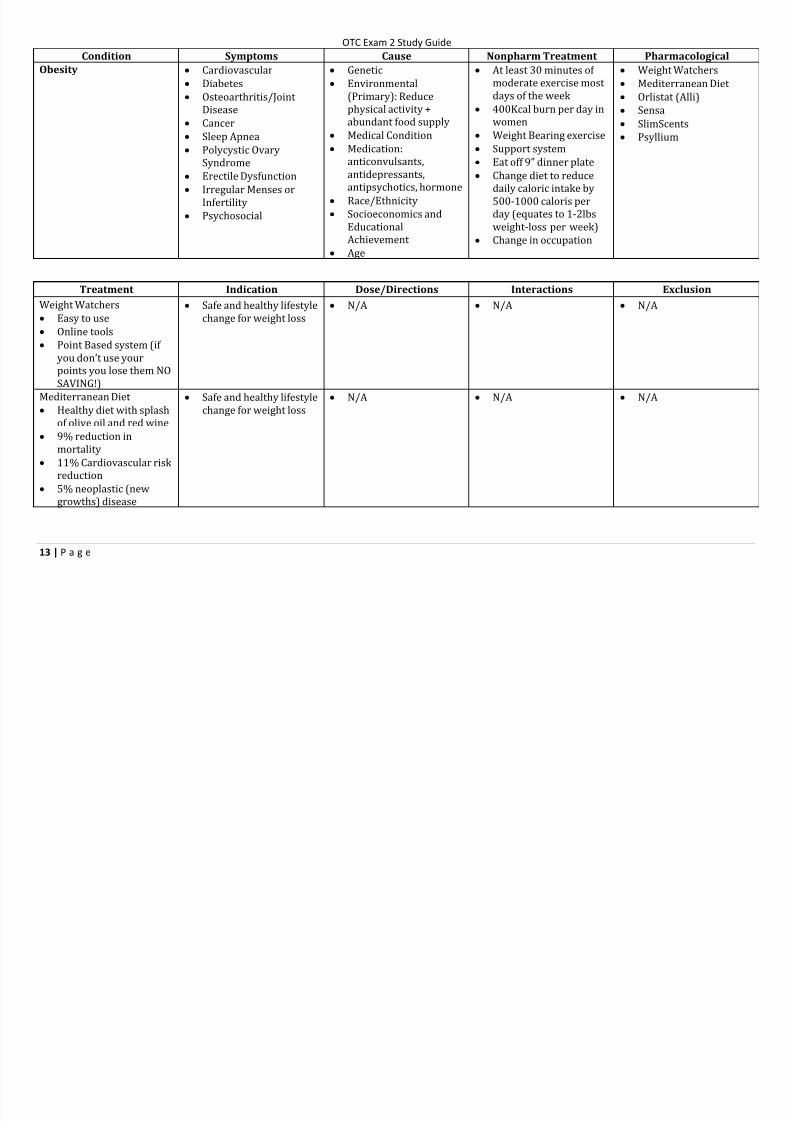
Orlistat
Lipase inhibitor
Inhibits the absorption
of dietary fats
Long-term weight loss
management aid
Need to accompany a
change to healthier diet
(low in fat) and exercise
Expected weight-loss of
5-10 lbs within 6months
May also lower LDL
cholesterol and blood
pressure
60mg TID
Take within 1 hour of
eating a meal (if meal
does not contain fat the
omit dose)
MVI to be taken 4-6
hours after or 2-4 hrsprior to taking orlistat
Vit ADEK: decrease
absorption of Vit ADEK
Lipophillic Drugs
(amiodarone,valproic
acids): may affect
efficacy of lipophilic
drugs
Patient taking warfarin
due to decrease in
vitamin K absorption
Patients with
osteoporosis due to
decrease in vitamin D
absorption Patients with
gallbladder problems
Chronic malabsorption
syndrome
May cause GI upset if
fatty foods are ingested
Sensa
Tastants that trick your
brain and stomach into
thinking you are full
through sense of smell
6 month weight loss
system
Does not need to change
diet or starve
themselves Two monthly containers
shipped to patients and
new blend of tastants
per month
Sprinkle on any food you
eat N/A Expensive – patients
may not be able to afford
SlimScents
Dietary pens that are
inhaled through nose
before meals
Three pens that are
rotated constantly
Does not require
patients to eat special
meals or starve
themselves
Inhale gently three times
in EACH nostril 5-6
minutes before you eat
and 5-10 minutes after
you eat OR everytime
you feel the least bit
hungry
Sniff at least 10 times in
each nostril per day
N/A Expensive – patients
may not be able to afford
A little bit more
expensive than sense
Psyllium **FIBER**
Non-digestible carb and
lignin (fiber)
Favorable effects on
obesity, and improved
lipid and hypertension
control
20-38 gram per day Hypoglycemic agents:
may affect efficacy of
hypoglycemic agents
N/A
7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 15/32
OTC Exam 2 Study Guide
15 | P a g e
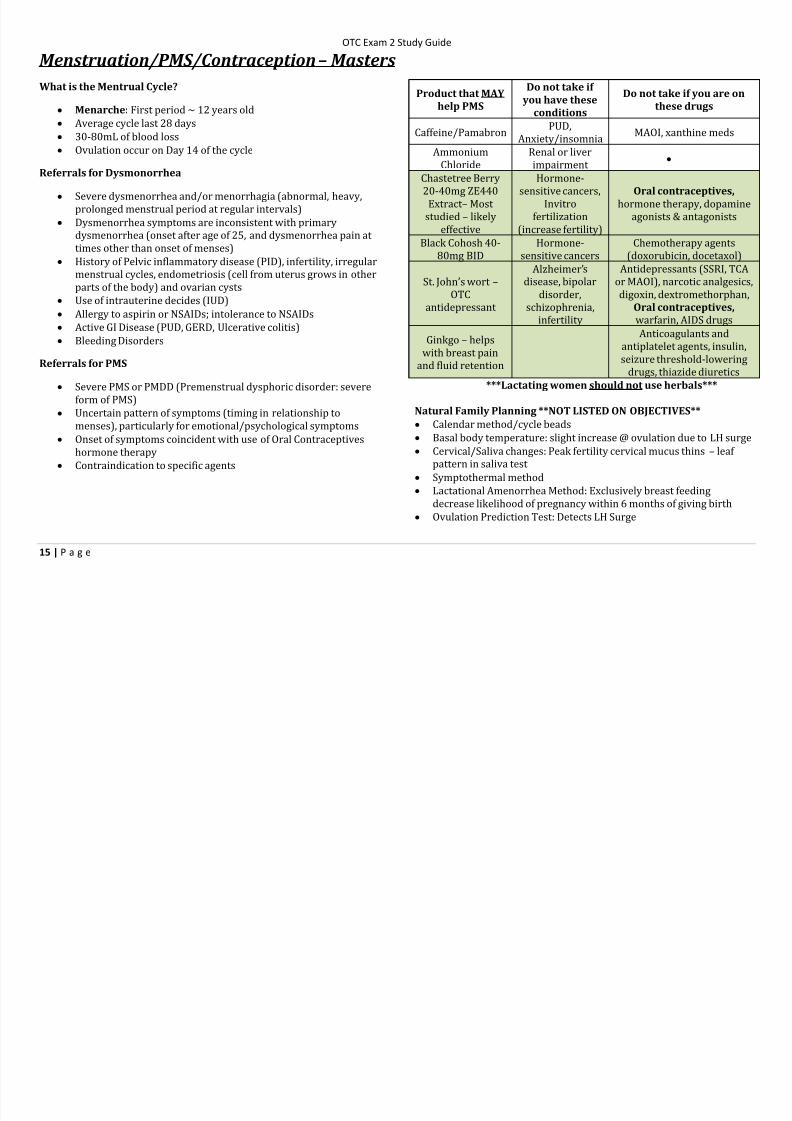
Menstruation/PMS/Contraception– Masters
What is the Mentrual Cycle?
Menarche: First period ~ 12 years old
Average cycle last 28 days
30-80mL of blood loss Ovulation occur on Day 14 of the cycle
Referrals for Dysmonorrhea
Severe dysmenorrhea and/or menorrhagia (abnormal, heavy,
prolonged menstrual period at regular intervals)
Dysmenorrhea symptoms are inconsistent with primary
dysmenorrhea (onset after age of 25, and dysmenorrhea pain at
times other than onset of menses)
History of Pelvic inflammatory disease (PID), infertility, irregular
menstrual cycles, endometriosis (cell from uterus grows in otherparts of the body) and ovarian cysts
Use of intrauterine decides (IUD)
Allergy to aspirin or NSAIDs; intolerance to NSAIDs
Active GI Disease (PUD, GERD, Ulcerative colitis)
Bleeding Disorders
Referrals for PMS
Severe PMS or PMDD (Premenstrual dysphoric disorder: severe
form of PMS)
Uncertain pattern of symptoms (timing in relationship tomenses), particularly for emotional/psychological symptoms
Onset of symptoms coincident with use of Oral Contraceptives
hormone therapy
Contraindication to specific agents
Product that MAY
help PMS
Do not take if
you have these
conditions
Do not take if you are on
these drugs
Caffeine/PamabronPUD,
Anxiety/insomniaMAOI, xanthine meds
Ammonium
Chloride
Renal or liver
impairment
Chastetree Berry
20-40mg ZE440
Extract – Most
studied – likely
effective
Hormone-
sensitive cancers,
Invitro
fertilization
(increase fertility)
Oral contraceptives,
hormone therapy, dopamine
agonists & antagonists
Black Cohosh 40-
80mg BID
Hormone-
sensitive cancers
Chemotherapy agents
(doxorubicin, docetaxol)
St. John’s wort – OTC
antidepressant
Alzheimer’s
disease, bipolardisorder,
schizophrenia,
infertility
Antidepressants (SSRI, TCA
or MAOI), narcotic analgesics,digoxin, dextromethorphan,
Oral contraceptives,
warfarin, AIDS drugs
Ginkgo – helps
with breast pain
and fluid retention
Anticoagulants and
antiplatelet agents, insulin,
seizure threshold-lowering
drugs, thiazide diuretics
***Lactating women should not use herbals***
Natural Family Planning **NOT LISTED ON OBJECTIVES** Calendar method/cycle beads
Basal body temperature: slight increase @ ovulation due to LH surge
Cervical/Saliva changes: Peak fertility cervical mucus thins – leaf
pattern in saliva test
Symptothermal method
Lactational Amenorrhea Method: Exclusively breast feeding
decrease likelihood of pregnancy within 6 months of giving birth
Ovulation Prediction Test: Detects LH Surge

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 16/32
7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 17/32
OTC Exam 2 Study Guide
17 | P a g e
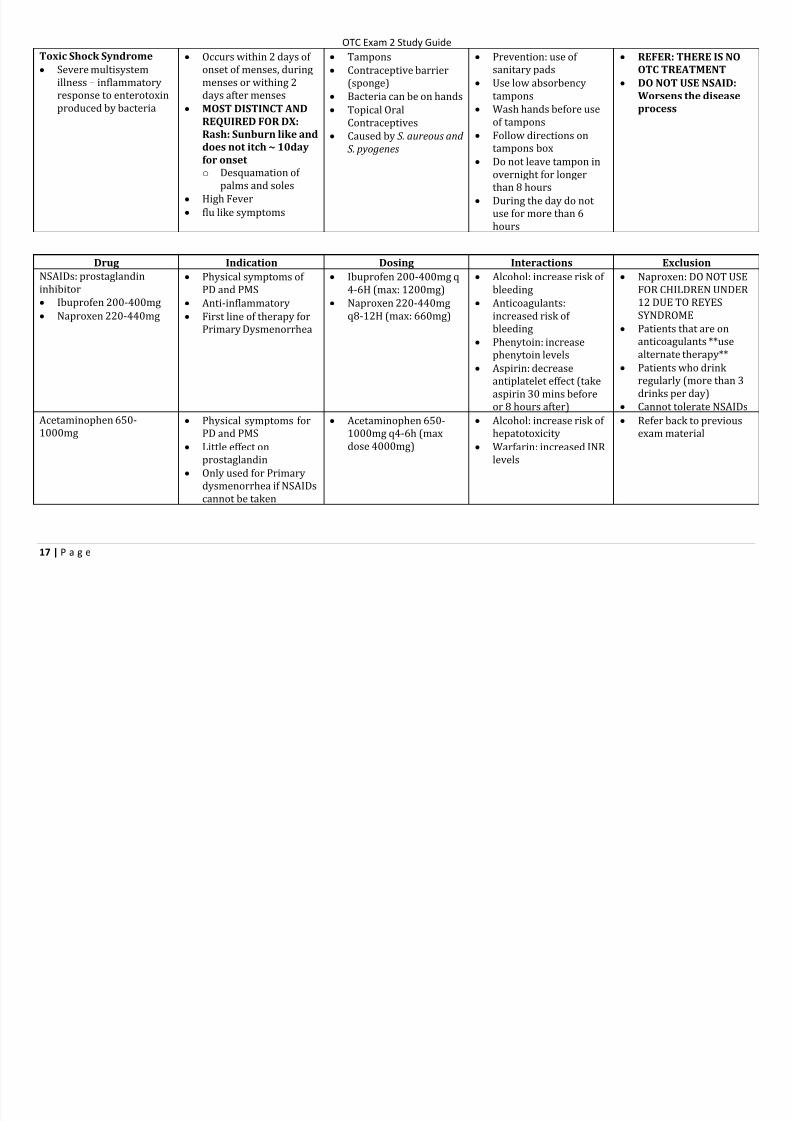
Toxic Shock Syndrome
Severe multisystem
illness – inflammatory
response to enterotoxin
produced by bacteria
Occurs within 2 days of
onset of menses, during
menses or withing 2
days after menses
MOST DISTINCT AND
REQUIRED FOR DX:
Rash: Sunburn like and
does not itch ~ 10day
for onset
o Desquamation of
palms and soles
High Fever
flu like symptoms
Tampons
Contraceptive barrier
(sponge)
Bacteria can be on hands
Topical Oral
Contraceptives
Caused by S. aureous and S. pyogenes
Prevention: use of
sanitary pads
Use low absorbency
tampons
Wash hands before use
of tampons
Follow directions ontampons box
Do not leave tampon in
overnight for longer
than 8 hours
During the day do not
use for more than 6
hours
REFER: THERE IS NO
OTC TREATMENT
DO NOT USE NSAID:
Worsens the disease
process
Drug Indication Dosing Interactions Exclusion
NSAIDs: prostaglandininhibitor
Ibuprofen 200-400mg
Naproxen 220-440mg
Physical symptoms of PD and PMS
Anti-inflammatory
First line of therapy for
Primary Dysmenorrhea
Ibuprofen 200-400mg q4-6H (max: 1200mg)
Naproxen 220-440mg
q8-12H (max: 660mg)
Alcohol: increase risk of bleeding
Anticoagulants:
increased risk of
bleeding
Phenytoin: increase
phenytoin levels
Aspirin: decrease
antiplatelet effect (take
aspirin 30 mins before
or 8 hours after)
Naproxen: DO NOT USEFOR CHILDREN UNDER
12 DUE TO REYES
SYNDROME
Patients that are on
anticoagulants **use
alternate therapy**
Patients who drink
regularly (more than 3
drinks per day)
Cannot tolerate NSAIDs
Acetaminophen 650-1000mg
Physical symptoms forPD and PMS
Little effect on
prostaglandin
Only used for Primary
dysmenorrhea if NSAIDs
cannot be taken
Acetaminophen 650-1000mg q4-6h (max
dose 4000mg)
Alcohol: increase risk of hepatotoxicity
Warfarin: increased INR
levels
Refer back to previousexam material

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 18/32
OTC Exam 2 Study Guide
18 | P a g e
Aspirin Little effect on PG Not important n/A Last line – do not use
cause of increase in
menstrual flow
DO NOT USE IN
PATIENTS UNDER 15
DUE TO REYES
SYNDROME
Ammonium Chloride Treatment of PMS
Diuretic
TID (max: 3g – no more
than 6 days) N/A Renal or liver
impairment
Caffeine Inhibits renal tubular
reabsorption of sodium
and water
Diuretic: Treatment for
fluid retention
100-200mg q3-4H MAOI (depression meds)
Xanthine (Gout Meds)
Theophylline (treats
asthma)
PUD
Anxiety
Insomnia
Pamabrom
Derivative of
theophylline
Treatment of PMS
Diuretic
50mg QID
In combination products
MAOI (depression meds)
Xanthine (Gout Meds)
PUD
Anxiety
Insomnia
Midol and Pamprin Acetaminophen
Pamabrom
Pyrilamine
(antihistamine)
Combination of painreliever, diuretic and
antihistamine
N/A N/A N/A
Condoms
Latex
Polyurethane
Lamb skin
Female Condoms (DO
NOT RECOMMENDWITH MALE CONDOM)
Contraception N/A N/A Latex allergies -> use
polyurethane or natural
skin
Lamb skin DOES NOT
prevent STD prevention
DO NOT USE OIL BASEDLUBRICANTS – Degrades
LATEX condoms
DO NOT WEAR Female
condom for more than 8
hours

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 19/32
OTC Exam 2 Study Guide
19 | P a g e
Vaginal Spermicides
Films
Foams
Gels
Suppositories
Contraception Films: Need 10-15 min –
3 hours to dissolve N/A Does not protect against
STI
Increase risk of
contracting HIV/AIDS
due to irritability of
vaginal canal
Today’s Sponge
Contraceptive Barrior
Spermicide
Semen absorbant
contraception
Moisten with tap water
Effective IMMEDIATELY
Must remain in place 6
hours AFTER
intercourse
Effective for 24 hours –
REMOVE BY 24 HOURS
N/A
More effective in womenwho have not given birth
Increased risk of HIV
and cervical infections
Increase risk in TSS
Plan B One Step
Levonorgestrel 1.5mg
Approved for women of
all ages
DOES NOT ENDPREGNANCY
Emergency
contraception
ONLY FDA approved to
work if taken within 72
hours ~ if within 120hours would be
appropriate to sell but
counsel!
Take 1 pill as soon as
possible after
unprotected intercourse
or contraception failure
Most effective if takenwithin 3 days
Should start menstrual
cycle within 1 week (3
weeks if irregular)
Refer if menses does not
occur
N/A Does not protect against
HIV/AIDS
Most Common AE:
o Nausea
o Abdominal Paino Fatigue
o Headache
DO NOT TAKE IF YOU
HAVE UNDIAGNOSED
VAGINAL BLEEDING
Plan B Generic
Levonorgestrel 0.75mg
TWO PILLS
Available for women
17+ OTC
Under 17 = RX only
DOES NOT END
PREGNANCY
Emergency
Contraceptive
ONLY FDA approved to
work if taken within 72
hours ~ if within 120
hours would be
appropriate to sell but
counsel!
Take 1 tablet ASAP after
unprotected intercourse
or contraceptive failure
Take Second dose 12
hours later
Will still be effective is
2nd dose is forgotten
Should start menstrual
cycle within 1 week (3
weeks if irregular)
Refer if menses does not
occur
N/A Does not protect against
HIV and AIDS
Most Common AE:
o Nausea
o Abdominal Pain
o Fatigue
o Headache
DO NOT TAKE IF YOU
HAVE UNDIAGNOSED
VAGINAL BLEEDING

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 20/32
OTC Exam 2 Study Guide
20 | P a g e
Vaginal Infections and Atrophic Vaginitis – Adams
Referral for Vaginal Infection
Pregnancy
Girls less than 12 years old
Fever or pain is present in the lower abdomen, back, or shoulder
Medications that predispose (lead) to Vaginal Candidiasis
o Corticosteroids
o Antineoplastics
Medical disorders that can predispose to Vaginal Candidiasis
o HIB
o Diabetes
Recurrent Vaginal Candidiasis
o More than 3 vaginal infection per year or vaginal infection in the past 2 months
ODOROUS DISCHARGE IS AUTOMATIC REFERRAL TO DOCTOR
What is a pH testing device and what are its limits
Press application for women with normal periods
DO NOT USE WHEN MENSTRUATING
DO NOT URINATE OR TOUCH THE APPLICATOR
Intercourse = Wait 2 days before using, Spermicide/Lubricant? = wait 3 days before using
Will only tell you if you have vaginal candidiasis – high pH must refer to doctor
Referral for Atrophic Vaginitis
Symptoms of severe vaginal dryness or dyspareunia
Symptoms that are not localized (widespread)
Vaginal Dryness or dyspareunia not relieved by use of personal lubricants after 7 days

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 21/32

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 22/32

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 23/32

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 24/32
OTC Exam 2 Study Guide
24 | P a g e
Alopecia – Adams
Referral for Alopecia
Less than 18 years old
Pregnancy or breast feeding
Recent discontinuation of oral contraceptives
Hair loss in patient with no family history of hair loss
Hair loss in patient with positive hair-pull test
Hair loss related to history of endocrine dysfunction
(chemotherapy, medication use) and dietary deficiencies
Sudden or patchy hair loss
Evidence of fever or inflammation (occurring 3-6 months before
hair loss begins)
Skin lesion that indicate autoimmune disease or infection
Scaling, sunburn, or other damage to scalp
Broken-off hair shafts that resemble those caused by fungal
infection or trichotillomania Loss of eyebrows or eyelashes
Changes in nails
Women with sudden or severe hair loss
o Due to hyperandrogenism
Postpartum women with hair loss
Positive Hair Pull Test
10% = excellent
25% = average person
35% = Concern
**SHOULD NOT SEE ANY ROOTS***
Minoxidil Patient Counseling Points **was not on objectives**
Initial Effect
o Might see minor hair loss
Effectiveness
o Works best when you FIRST notice hair loss
Hair Stimulation
o Turns Vellus (Thin) -> Terminal (thick) Hair
o Using 2% form: see improvement @ 4 months
o Using 5% Form: see improvement @ 2 months
Therapeutic Endpoint – Hair
o 2%: Must use for one full year to see full effect
o 5%: must use for 4 months to see full effect
Discontinuation
o Hair density returns to pretreatment

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 25/32

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 26/32

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 27/32
OTC Exam 2 Study Guide
27 | P a g e
Equipment Indication Directions Interactions Exclusion
Forearm Crutches Long term patients that
need support for a long
period of time
Requires good grip
Requires good wrist
Bad wrist
Bad grip
Platform Crutches People without inadequate grip
People who cannot deal
with wrist compression
People who cannot deal
with axillary pressure
Axillary Crutches
Most common Requires good grip
Requires arm strength
Bad axillary
Bad grip
Bad arm
Canes Need safety blanket
Four point or quad is
most stable People w/ good grips,
arm strength, leg
strength
Use on good side Patients that need actual
support
Bad arms Bad wrist
Bad legs
Hose
Usually need to be
referred to get correct
sizing
OTC = lower grade
support hose Moderate (mild
tiredness)
o 10-20mm Hg
Firm (begin to feel
pain)
o 20-30mm Hg
Heavy (Severe)
o 30-40 mm Hg & 40-
50mm Hg
Assist blood flow
Reduce swelling in feet
and ankles
Help relieve pain and
fatigue in legs
40+ circulatoryinsufficiency
Women of child bearing
age
Workers who do
prolonged sitting or
standing
Patients who need 50
mmHg – Should get RX
Does not have usual leg
size

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 28/32
7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 29/32

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 30/32

7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 31/32
7/27/2019 OTC Exam 2 Study Guide
http://slidepdf.com/reader/full/otc-exam-2-study-guide 32/32
OTC Exam 2 Study Guide
32 | P a g e
Otic Disorders – Falter
When do you refer?
Signs of infection; Pain due to ear discharge
Ear surgery in past 6 weeks Bleeding, trauma, or ruptured tympanic membrane
Children under the age of 12
presence of tympanostomy tubes
Hypersensitivity to ingredients
Unable to follow administration directions
Presence of boil(s) anywhere other than auricle or multiple boils
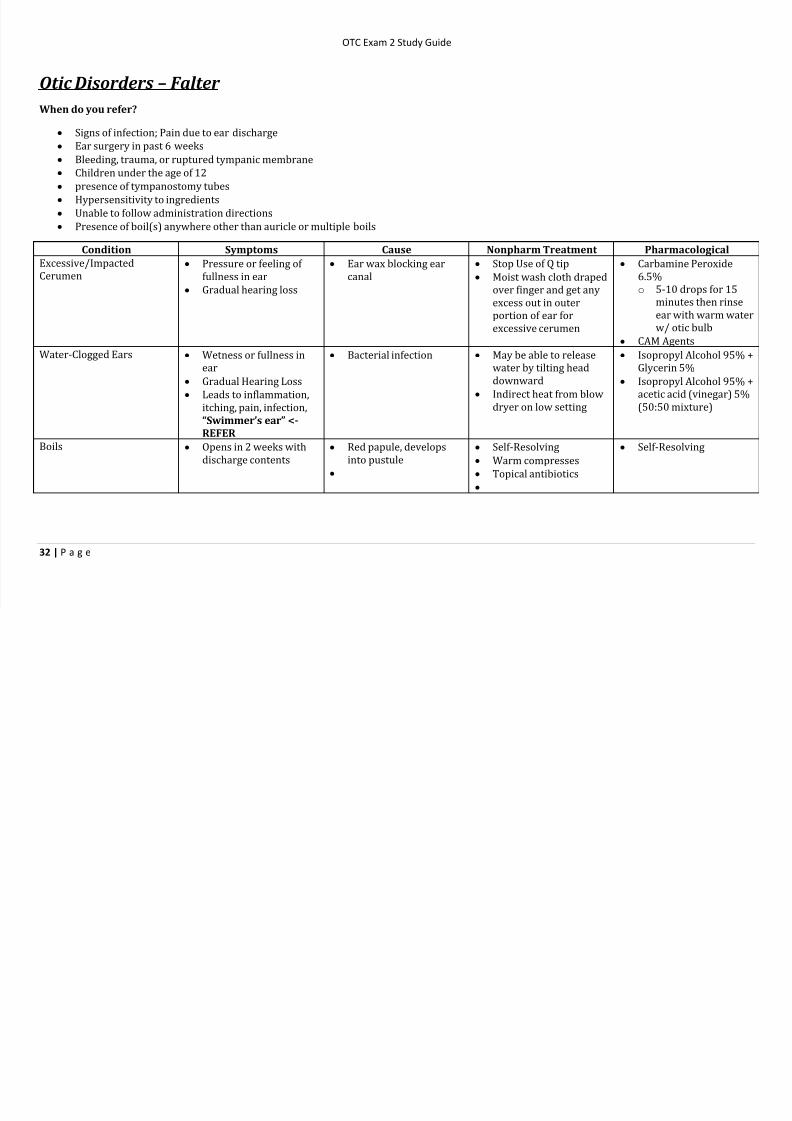
Condition Symptoms Cause Nonpharm Treatment Pharmacological
Excessive/Impacted
Cerumen
Pressure or feeling of
fullness in ear Gradual hearing loss
Ear wax blocking ear
canal
Stop Use of Q tip
Moist wash cloth drapedover finger and get any
excess out in outer
portion of ear for
excessive cerumen
Carbamine Peroxide
6.5%o 5-10 drops for 15
minutes then rinse
ear with warm water
w/ otic bulb
CAM Agents
Water-Clogged Ears Wetness or fullness in
ear
Gradual Hearing Loss
Leads to inflammation,
itching, pain, infection,
“Swimmer’s ear” <-REFER
Bacterial infection May be able to release
water by tilting head
downward
Indirect heat from blow
dryer on low setting
Isopropyl Alcohol 95% +
Glycerin 5%
Isopropyl Alcohol 95% +
acetic acid (vinegar) 5%
(50:50 mixture)
Boils Opens in 2 weeks with
discharge contents Red papule, develops
into pustule
Self-Resolving
Warm compresses
Topical antibiotics
Self-Resolving