osteoarthrosis - prof. chit soe (maulamyaing)
TRANSCRIPT

Osteoarthrosis Update
Dr. Chit SoeMBBS,MMed.Sc,MRCP,FRCP,Dr.Med.ScSr. Consultant/Associate ProfessorEast Yangon General Hospital University of Medicine I

18.2.06 OA-CS 2
Definition of the Problem Osteoarthritis of the knee is an
increasingly common problem due to a more active society, often leading to
prior knee injuries; an increasingly elderly population; and a growing percentage of the population
that is overweight.

18.2.06 OA-CS 3
FAQ-Question • Nowadays there are so many
NSAIDs available in the market and many medical representatives make promotion for their products.
• General practitioner may confuse how to prescribe the drugs. Please could you explain the rationale about the use of NSAIDs?

18.2.06 OA-CS 4
Strength of Recommendation
A. Type I evidence or consistent findings from multiple studies of types II, III, or IV
B. Types II, III, or IV evidence and findings are generally consistent
C. Types II, III, or IV evidence, but findings are inconsistent
D. Little or no systematic empirical evidence
18.2.06 OA-CS 5
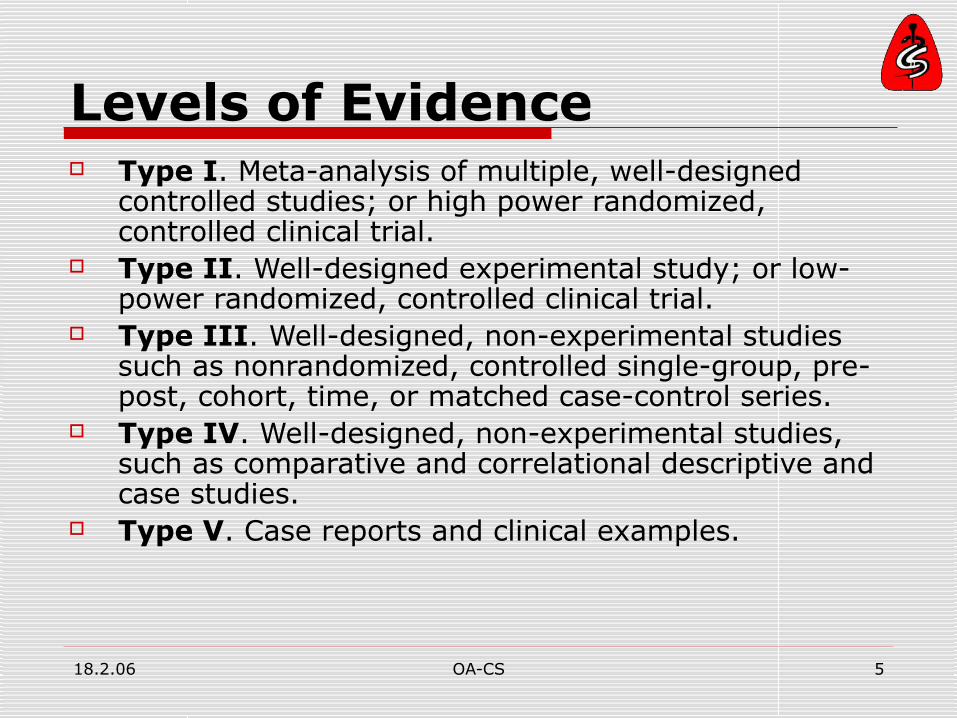
Levels of Evidence Type I. Meta-analysis of multiple, well-designed
controlled studies; or high power randomized, controlled clinical trial.
Type II. Well-designed experimental study; or low-power randomized, controlled clinical trial.
Type III. Well-designed, non-experimental studies such as nonrandomized, controlled single-group, pre-post, cohort, time, or matched case-control series.
Type IV. Well-designed, non-experimental studies, such as comparative and correlational descriptive and case studies.
Type V. Case reports and clinical examples.

18.2.06 OA-CS 6

18.2.06 OA-CS 7
NSAID in OA

18.2.06 OA-CS 8
NSAIDs
WILLOW BARK AS HERBAL MEDICINE
1899 ASPIRIN
1960 INDOMETHACIN
DICLOFENAC, OXICAMS, MEFENAMATES
“PROBLEM OF GI & RENAL TOXICITY”

18.2.06 OA-CS 9
In rank order: GI Toxicity index 1. Salsalate 0.871 2. Aspirin 1.063. Ibuprofen 1.16 4. Sulindac 1.635. Naproxen 1.786. Piroxicam 2.07 7. Tolmetin 2.16 8. Diclofenac 2.17 9. Indomethacin 2.4010. Fenoprofen 2.48 11. Ketoprofen 3.0912. Meclofenamate 4.03
NSAIDSCURRENT ADVERSE GI EFFECTS
NSAIDSCURRENT ADVERSE GI EFFECTS

18.2.06 OA-CS 10
18.2.06 OA-CS 11
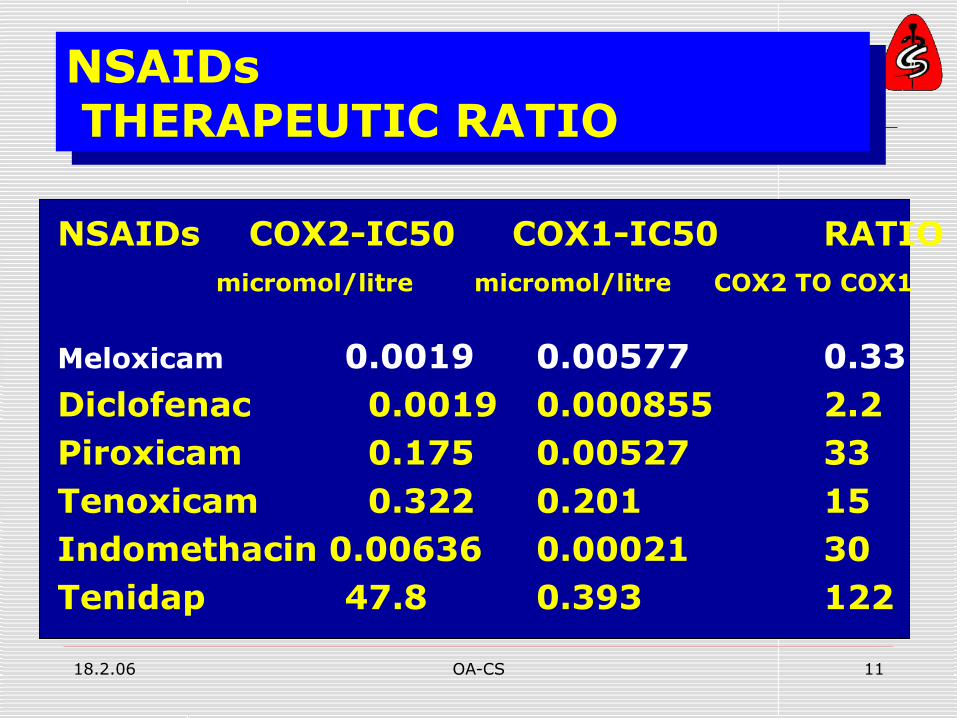
NSAIDs COX2-IC50 COX1-IC50 RATIO micromol/litre micromol/litre COX2 TO COX1
Meloxicam 0.0019 0.00577 0.33 Diclofenac 0.0019 0.000855 2.2 Piroxicam 0.175 0.00527 33 Tenoxicam 0.322 0.201 15 Indomethacin 0.00636 0.00021 30 Tenidap 47.8 0.393 122
NSAIDs THERAPEUTIC RATIO
NSAIDs THERAPEUTIC RATIO

18.2.06 OA-CS 12

18.2.06 OA-CS 13
What are the indications and uses for these at present?
Celecoxib (Celebrex) Rofecoxib (Vioxx,
Rofedole) and Valdecoxib are
all available for treatment of acute pain, Dysmenorrhea, OA and RA.

18.2.06 OA-CS 14
For OA, celecoxib can be given as 200 mg once a day or 100 mg twice daily. Adherence is usually better with once-a-day doses, but for pain, sometimes it's good to give a twice-daily dose
valdecoxib is 10 mg/day.
Because of the prize, they can not be the first choice for all, but be the choice for those with high risk for GI bleeding.

18.2.06 OA-CS 15

18.2.06 OA-CS 16
Recommendation Different NSAIDs has different
severity of effect on GIT Ibuprofen and naproxan are the
safest Response to NSAID also differ with
different individual. If not satisfactory response to one drug in one month, can try another compound which may show response
Should not combine two NSAIDs

18.2.06 OA-CS 17

18.2.06 OA-CS 18
Question
• What is rofecoxib scandal?
• What should we learn?

18.2.06 OA-CS 19

18.2.06 OA-CS 20

18.2.06 OA-CS 21

18.2.06 OA-CS 22

18.2.06 OA-CS 23
Celecoxib Fear Based on this evaluation, the National Cancer
Institute (NCI) today stopped drug administration in a three year celecoxib (Celebrex) study [Adenoma
Prevention with Celecoxib (APC)] because an interim analysis by the study's Data Monitoring
Committee showed a statistically significant increase in the risk of CV events (composite endpoint
of cardiovacular death, acute myocardial infarction and stroke) in patients randomized to
celecoxib. The study, a three-year evaluation of The interim analysis revealed: • placebo - 6 CV events • celecoxib 200 mg bid - 15 CV events (2.5 fold
increase over placebo) • celecoxib 400 mg bid - 20 CV events (3.4 fold
increase over placebo)

18.2.06 OA-CS 24

18.2.06 OA-CS 25

18.2.06 OA-CS 26

18.2.06 OA-CS 27
Lessons There is no drug safe 100% Use at required time with limited
duration (Educate the patients about possible
side effects to prevent self use and self prescription to others)
Observational studies are also useful as RCT especially for drug side effects and yellow cards should be used by practioners to report the adversed events
18.2.06 OA-CS 28
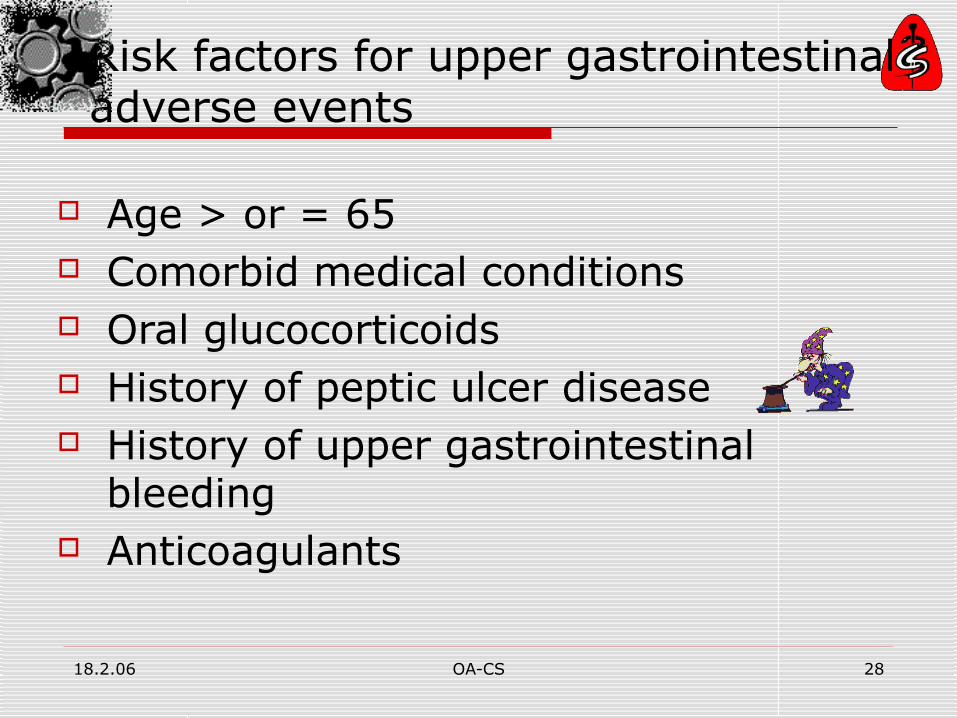
Risk factors for upper gastrointestinal adverse events
Age > or = 65 Comorbid medical conditions Oral glucocorticoids History of peptic ulcer disease History of upper gastrointestinal
bleeding Anticoagulants

18.2.06 OA-CS 29
Latest News FDA Advisory Committee Reaffirms
Continued use of Cox-2 (17 Feb 2005)
Contra-indication: pts with IHD or stroke, HT whose BP is not under control.
There are risks but benefits outweigh them

18.2.06 OA-CS 30
NSAIDS & Para The magnitude of pain relief afforded by
NSAIDs, and their superiority to placebo, is only modest. Improvement averages only about 20% relative to baseline
Similarly, in a recent double blind, crossover trial, some 45% of subjects preferred Paracetamol even when an NSAID was significantly better than para in improving pain, function, and quality of life.
Thus, statistically significant differences between treatments do not necessarily translate into clinically significant differences.

18.2.06 OA-CS 31
Question
One of the degenerative disorders, OA is frequently seen in clinical practice. Some have been receiving NSAIDs for long period with or without improvement.
Could you give the guide lines for the effective management of OA? How long can they take NSAIDs safely? What about the role of newer drugs like “Disease Modifying”in OA?

18.2.06 OA-CS 32

18.2.06 OA-CS 33

18.2.06 OA-CS 34
In the very earliest stage of OA there is fibrillation of the articular surface & disruption of the extracellular matrix.
At the same time, the cells are stimulated to increase synthesis.Very early in the process, there is thickening of the subchondral bone.
Grossly, roughening of the articular surface, narrowing of the joint space, and some increased subchondral bone density.
18.2.06 OA-CS 35
As the disease progresses, pieces of the articular cartilage are lost into the joint (tufts and irregular areas of the surface, fragments in the joint, some microscopic, some grossly visible are released into the joint)
It occurs because of the release of enzymes that break down the matrix and cause the actual loss of most of the articular cartilage.

18.2.06 OA-CS 36
Grossly, loss of the joint space, formation of osteophytes, and thickening of the synovial membrane.
This is the end stage of the disease that we recognize in most of the patients that we're treating with total joint replacement.

18.2.06 OA-CS 37

18.2.06 OA-CS 38

18.2.06 OA-CS 39

18.2.06 OA-CS 40

18.2.06 OA-CS 41
18.2.06 OA-CS 42
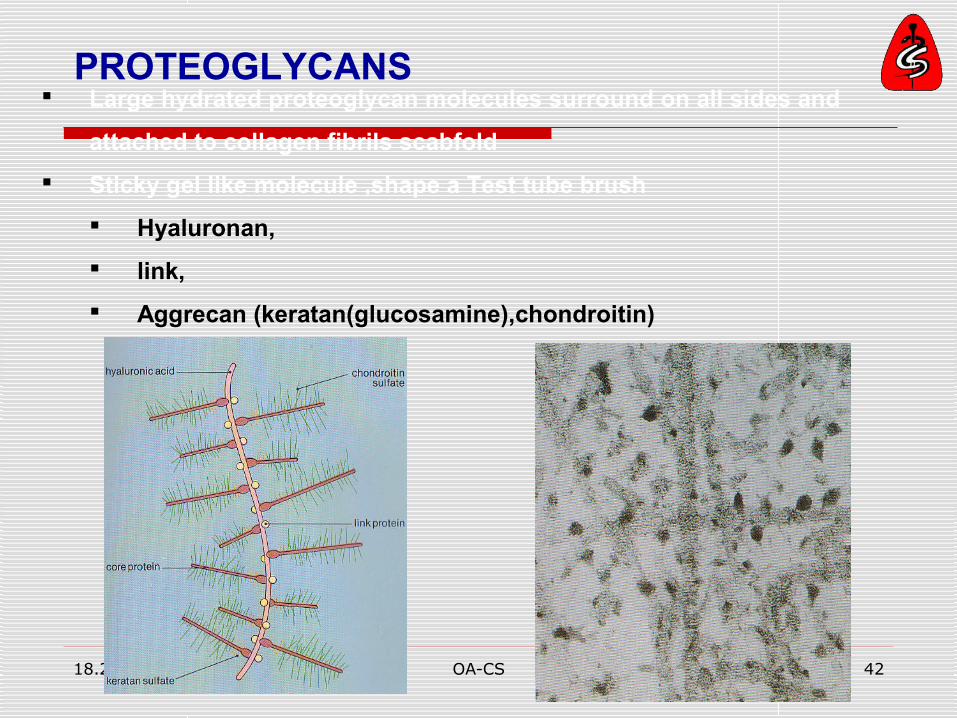
Large hydrated proteoglycan molecules surround on all sides and
attached to collagen fibrils scabfold
Sticky gel like molecule ,shape a Test tube brush
Hyaluronan,
link,
Aggrecan (keratan(glucosamine),chondroitin)
PROTEOGLYCANS

18.2.06 OA-CS 43

18.2.06 OA-CS 44
Cell Senescence When the cell duplicate for certain
limit their rate of replication become slow and then stop.
After certain number of duplication, their differentiated phenotype is lost.
The aging clock in all the tissues of our body is the chromosome, and the end of the chromosome or the telomere is what allows the chromosome to be replicated.
if telomere is shortening, there is a decrease in the ability of the cells to respond to anabolic factors, decreasing the ability of the cells to maintain the extracellular matrix.

18.2.06 OA-CS 45
after a certain number of cell divisions, these cells just quit functioning as articular cartilage chondrocytes and are no longer able to maintain the extracellular matrix.
people vary considerably in the onset of chondrocyte senescence.
Trauma and excessive joint loading accelerate the senescence by releasing free radicals that stimulate the degradation of not only the nuclear (DNA), but also the mitochondrial DNA.
to attack this disease, we have to find treatments that prevent or delay the development of chondrocyte senescence and decrease the intensity of articular cartilage contact stress.

18.2.06 OA-CS 46
AGE Chondroitin-
increased Keratin- increased Reduction in water Impair shock-
absorption

18.2.06 OA-CS 47
Not merelyAge

18.2.06 OA-CS 48
SusceptibilityHeredity
Gender/Hormonal statusObesity
(Osteoporosis-negative)(Smoking-negative)
Aging
TraumaJoint shape
Usage-occupational-recreationalMechanical

18.2.06 OA-CS 49

18.2.06 OA-CS 50
Genetic susceptibility T869C polymorphism in TGFβ-1 gene Frequencies of Genotypes and Allelic
Variants SubpopulationsCC CT TT C AlleleT Allele OA, total 0.47 0.3 0.23 0.62 0.38 Hand OA 0.5 0.25 0.25 0.625 0.375 Knee OA 0.44 0.32 0.24 0.6 0.4 Control 0.2 0.42 0.38 0.41 0.59

18.2.06 OA-CS 51
Diagnosis is purely clinical. A plain radiograph is the only
useful, but non-essential investigation.
Insidious onset of pain and functional restriction at a joint without significant inflammation is the main feature.
E.g. Do you have pain in knees disturbing walking in most of the days up to one month during last year which is not part of the generalized pain? Is a good screening question for detecting Knee OA.

18.2.06 OA-CS 52
Diagnosis Osteoarthritis of the knee should be
suspected when a patient presents with knee pain that has been longstanding, increases with activity, particularly weight bearing and stairs, and improves with rest.

18.2.06 OA-CS 53
The correlation between the presence of structural OA (clinical signs, radiographic changes) and pain and disability varies according to site and patient.

18.2.06 OA-CS 54

18.2.06 OA-CS 55
Cartilage loss andJoint space narrowing

18.2.06 OA-CS 56
Subchondral bone sclerosis

18.2.06 OA-CS 57
Osteophytes

18.2.06 OA-CS 58
Treatment (OA) of the knee of 10 or more years
duration, about 10% stabilize or improve spontaneously, presumably because the balance shifts towards synthesis. The others go on to progressive disease.
At the end stage of the disease, there's a failure of the cellular response. So if we're going to intervene, ideally, we want to target the disease in the earlier stage.

18.2.06 OA-CS 59
Modifying activity, decreasing torsional and impact loading, can make a significant difference in the progression of OA.
There are good data to show that muscle strengthening across joints decreases the rate of progression and symptoms, and that weak muscles increase the risk of OA and its rate of progression.

18.2.06 OA-CS 60
Pharmacological (non-steroidal anti-inflammatory drugs, analgesics, intra-articular injections of corticosteroids or hyaluronic acid)
Surgical (osteotomy, arthroplasty, graft).
Non-pharmacological (patient education, physical therapy, use of cane, weight management programme in overweight patient, etc),

18.2.06 OA-CS 61

18.2.06 OA-CS 62

18.2.06 OA-CS 63
Nonpharmacologic therapy for patients with osteoarthritis (9.10)
Patient education Self-management programs (e.g., Arthritis Foundation
Self-Management Program) Personalized social support through telephone contact Weight loss (if overweight) Aerobic exercise programs Physical therapy Range-of-motion exercises Muscle-strengthening exercises Assistive devices for ambulation Patellar taping Appropriate footwear Lateral-wedged insoles (for genu varum) Bracing Occupational therapy Joint protection and energy cosservation Assistive devices for activities of daily living

18.2.06 OA-CS 64
EULAR 2005 and ARA recommendation "Optimal management of knee
osteoarthritis requires a combination of pharmacological and non-pharmacological treatment modalities. Non-pharmacological treatment of knee osteoarthritis should include regular education, exercise, appliances (sticks, insoles), and weight reduction."

Pharmacological Treatment

18.2.06 OA-CS 66
Paracetamol treatment for OA
One study compared acetaminophen to placebo, and five compared acetaminophen to NSAIDs.
In the placebo-controlled RCT, acetaminophen clearly superior to placebo
In the comparator-controlled RCTs, acetaminophen was less effective overall than NSAIDs
Reviewers' conclusions: The evidence to date suggests that NSAIDs are superior to acetaminophen for improving knee and hip pain in people with OA but have not been shown to be superior in improving function.

18.2.06 OA-CS 67

18.2.06 OA-CS 68
EULAR 2003 recommendation "Paracetamol (acetaminophen) is the
oral analgesic to try first and, if successful, is the preferred long term analgesic.
Non-steroidal anti-inflammatory drugs (NSAIDs) should be considered in patients (with effusion) unresponsive to paracetamol."

18.2.06 OA-CS 69

18.2.06 OA-CS 70
Studies reviewed 23 trials including 10 845 patients, median age of 62.5 years. 7807 patients received adequate doses of NSAIDs and 3038 received placebo. The mean weighted baseline pain score was 64.2 mm on 100 mm visual analogue scale (VAS), and average duration of symptoms was 8.2 years.
Main outcome measure Change in overall intensity of pain.

18.2.06 OA-CS 71
Conclusion NSAIDs can reduce short term pain in osteoarthritis of the knee slightly better than placebo, but the current analysis does not support long term use of NSAIDs for this condition.
As serious adverse effects are associated with oral NSAIDs, only limited use (3 months) can be recommended.

18.2.06 OA-CS 72
Herbal intervention in OA
Five studies (four different herbal interventions) met the review criteria
not possible to draw firm conclusions from the single studies
but the two combined studies of avocado/soybean unsaponifiables showed beneficial effects on functional index, pain, intake of non-steroidal anti-inflammatory drugs (NSAIDs) and global evaluation.
No serious side effects

18.2.06 OA-CS 73
Reviewers' conclusions: The evidence for avocado-soybean unsaponifiables in the treatment of osteoarthritis is convincing but evidence for the other herbal interventions is insufficient to either recommend or discourage their use.14

18.2.06 OA-CS 74
High vit-C associated with 3 fold reduction in progression
C Soe

18.2.06 OA-CS 75

18.2.06 OA-CS 76
The disease-modifying agent for osteoarthritis treatment
Glucosamine (2-amino-2-deoxy-
alpha-D-glucose) sulfate is the salt of the natural amino-monosaccharide , included in keratan.
Chondrotin 4 sulphate & 6 sulphate and keratan are included in Aggrecan

18.2.06 OA-CS 77
The Cochrane Library, Issue 2 2003. Oxford: In Cochrane review (2003), Collectively, the
16 identified RCTs provided evidence that glucosamine is both effective and safe in OA.
In the 13 RCTs in which glucosamine was compared to placebo, glucosamine was found to be superior in all RCTs, except one.
In the four RCTs in which glucosamine was compared to an NSAID, glucosamine was superior in two, and equivalent in two.

18.2.06 OA-CS 78
Combination (Lippiello) Glucosamine- more anabolic Chondroitin- more anticatabolic There is a synergistic effect with
complete preservation of the femoral condyle (Structure)
(rabbit)

18.2.06 OA-CS 79
Chondroitin sulfate (Navy Seal Study) 800mg to 1200mg/d for 3 months to
see the response Treatment given during rigorous
training Relieved symptoms of knee OA No effect on back pain (Symptom)
Osteomin = Glucosamine + Chondroitin

18.2.06 OA-CS 80

18.2.06 OA-CS 81
Human Study (Switzerland, 1998) Measuring the progression of joint
space minimum width by automatic image analysis of digitised X-rays.
(weightbearing view with the knees flexed to 20o)
Randomised double-blind, two year trial of 300 patients showed significant effect

18.2.06 OA-CS 82
GLUCOSAMINE, CHONDROITIN SULPHATE Several studies have shown that the
efficacy of glucosamine is greater than that of placebo and comparable to that of NSAIDs in patients with knee OA, with a better safety profile than NSAIDs

18.2.06 OA-CS 83
Is glucosamine "chondroprotective"? Mazzuca SA, Brandt KD, Lane KA, Katz BP. Knee pain reduces joint space width in conventional standing anteroposterior radiographs of
osteoarthritic knees. Arthritis Rheum 2002;46:1223–7 Results of two recent virtually
identical randomised clinical trials,both of which were supported by the manufacturer, have led to the suggestion that glucosamine not only improves joint pain in patients with knee OA but protects against articular cartilage damage, based upon analyses of changes in joint space width in the standing anteroposterior (AP) knee radiograph.

18.2.06 OA-CS 84
Chondroitin A similar analysis of eight randomised
clinical trials of chondroitin showed a pooled effect size of 0.78—that is, much greater than that for glucosamine.
This corresponded with a difference in pain reduction between chondroitin and placebo of about 20 mm on a 100 mm VAS.

18.2.06 OA-CS 85
Reginster JY, Deroisy R, Rovati LC, Lee RL, Lejeune E, Bruyere O, et al. Long-term effects of glucosamine sulphate on osteoarthritis progression: a randomized, placebo-controlled clinical trial. Lancet 2001;357:251–6
An NIH supported multicentre study, the Glucosamine Chondroitin Arthritis Intervention Trial (GAIT), currently in progress, is comparing glucosamine, chondroitin sulphate, the combination, and celecoxib to placebo in patients with knee OA.
Although the primary outcome measure will be joint pain after 6 months of treatment, approximately 50% of the subjects will be maintained on treatment for 2 years and radiographs obtained at baseline will be compared with those obtained after 1 and 2 years of treatment.

18.2.06 OA-CS 86
The final EULAR 2003 recommendations for treating knee OA are:
Knee OA treatment should be tailored according to: Knee risk factors (obesity, adverse
mechanical factors, physical activity) General risk factors (age, comorbidity,
polypharmacy) Level of pain intensity and disability Sign of inflammation eg, effusion Location and degree of structural
damage

18.2.06 OA-CS 87
Recommendations activity modification and trial of an analgesic or non-
steroidal anti-inflammatory medication (NSAID) ("A" recommendation).
Acetaminophen has been shown to be as effective a pain reliever as NSAIDs in patients with osteoarthritis (OA) of the knee ("A" recommendation).
Selective cyclooxygenase II (COX-II) inhibitors should only be used in those patients with renal or GI risk factors ("B" recommendation).
Patients that respond well to initial treatment should be monitored. Those that use NSAIDs for 6 months should have a complete blood count (CBC), renal and liver function tests and a stool guaiac every 6 months ("D" recommendation).

18.2.06 OA-CS 88
X’ray after 1 month For patients that fail to respond to the
initial treatment, or for whom pain returns, radiographs should be obtained ("D" recommendation).
A standing anteroposterior (AP) and a lateral view should be taken initially

18.2.06 OA-CS 89
patient education ("D" recommendation), physical therapy ("A" recommendation) Patient education includes counseling about
weight loss, avoidance of aggravating activities, and support groups such as the Arthritis Foundation.
Durable medical equipment that can reduce pain includes: assistive devices for ambulation such as a cane, appropriate and occasionally modified footwear, and bracing.

18.2.06 OA-CS 90
Steroid after 1 month. The final treatment intervention involves
consideration of aspiration and cortisone injection ("D" recommendation).
If the patient has an effusion and the physician is technically proficient at aspiration, the knee joint should be aspirated in a sterile manner, and the fluid sent for appropriate studies.
If the synovial fluid does not show signs of hemarthrosis or infection, the knee joint should be injected with corticosteroid.

18.2.06 OA-CS 91
Indication for steroid injection In patients without an effusion, a
cortisone injection may be indicated if there are signs of inflammation such as: synovial thickening, pain that is diffuse or felt at night or
rest, or improved with NSAIDs. (Localized knee pain that is felt only with
weight bearing is less likely to respond to cortisone injection.)

18.2.06 OA-CS 92
NON-PHARMACOLOGICAL MEASURES instruction in principles of
joint protection, weight loss, exercise to improve fitness and strengthen periarticular muscles, orthotics, thermal modalities: that are
now recognised as the keystone of OA treatment.

18.2.06 OA-CS 93
Opioid analgesics, with or without paracetamol, are useful alternatives in patients in whom NSAIDs, including COX-2 specific inhibitors are contraindicated, ineffective and/or poorly tolerated
DMOAD (glucosamine sulphate, chondroitin sulphate, avocado and soya unsaponifiables, diaceirin, hyaluronic acid) have symptomatic effects and may modify structure

18.2.06 OA-CS 94
Joint replacement must be considered in patients with radiographical evidence of knee OA who have refractory pain and disability.

18.2.06 OA-CS 95
Summary OA
OA is not an in-evitable event of aging, but interaction of susceptibility, aging and mechanical factors.
It can be preventable Early treatment with understanding of
patho-physiology is essential Diagnosis is mainly clinical Use safer drugs like Paracetamol,
glucosamine and chondroitin Together with physical aids

18.2.06 OA-CS 96