organisational development plan 20120621 final
TRANSCRIPT

1 | P a g e
Organisational Development Plan
2012/13-2014/15
Final Version: June 2012

2 | P a g e
Table of Contents Organisational Development Plan
1. Executive Summary .............................................................................................. 3
2. Background ............................................................................................................ 3
3. Organisational Design Process ............................................................................. 6
4. Organisational Structure ........................................................................................ 7
5. Running Costs ....................................................................................................... 9
6. Organisational Values ........................................................................................... 10
7. Capacity and Capability ......................................................................................... 11
8. Diagnostic Self Assessment ................................................................................. 12
9. Organisation Development Aims ........................................................................... 14
10. Roles and Responsibilities .................................................................................. 20
11. Implementing and Monitoring the Plan ............................................................... 20
Appendices
1. Do, Buy, Share Model .......................................................................................... 21
2. CCG Organisational Structure ............................................................................... 22
3. CCG Board Structure ............................................................................................ 23
4. CCG Committee Structure .................................................................................... 24
5. Locality Map ........................................................................................................... 25
6. Action Plan ............................................................................................................. 26

3 | P a g e
1 Executive Summary This Organisational Development Plan has been developed to ensure that North Staffordshire Clinical Commissioning Group (the CCG) has the skills and capacity to commission high quality, safe services for our population of 213,000 and to support the delivery of our Integrated Strategy and Operating Plan 2012/13-2014/15. All organisations require a plan to guide and support their development. With the radical changes to the NHS set out in the Health and Social Care Act and the creation of a new commissioning landscape, this is particularly important. CCGs will need to be authorised by April 2013 and will need to demonstrate their competence to exercise the functions and responsibilities that will transfer to them from PCTs to be authorised. CCGs are membership organisations and will need to develop structures and processes that effectively engage member practices and GPs in shaping the CCGs priorities and day to day commissioning activities. Furthermore, CCGs must effectively involve service users and their wider populations in setting priorities and designing services, ensuring that improving quality and patient experience drive their commissioning activities. This Plan articulates the organisation development aims of the CCG, which are:
We will commission safe, effective and high quality sustainable services
We will deliver better patient outcomes through effective, federated and collaborative arrangements with key partners
We will improve patient engagement, feedback and involvement in decisions throughout the whole
commissioning cycle
We will reduce health inequalities and inappropriate clinical variation
We will achieve all the above while remaining within financial balance and achieving best value This Plan sets out the development plans for the CCG towards authorisation and beyond. It:
Describes the progress the CCG has made since its establishment in April 2011
Sets out the action we need to take this year to be successfully authorised as a statutory organisation from April 2013
Articulates the further development needed in our first two years as a public body
2 Background Once established in April 2011, with an organisational structure, staff assigned to populate that structure and a Shadow Board of clinical leads, senior managers and an Executive Chair, the CCG prepared and successfully implemented a Transition Plan for 2011/12.

4 | P a g e
This had two elements; transitioning to a new organisation and transitioning the business. The Transition Plan focussed on:
Governance
Board Development
Business as usual
Organisational Development The Transition Plan acted as our OD plan for 2011/12, and as key actions and outcomes were achieved, has since been reviewed, revised and refreshed for 2012/13 as we progress towards authorisation. The CCG’s organisational development (OD) priorities are focused on the overall organisational capacity and capability required to deliver its Strategy and Delivery Plan and to become a highly competent clinical commissioning organisation. Our OD Plan has four OD priorities that support us in achieving our vision, strategic goals and outcomes and strengthening our commissioning competencies:
Working in Partnership
Leadership Development
Quality and Innovation
Capacity and Capabilities
Our OD Action Plan has been informed by the self assessment carried out against the six competency domains we have used to prepare for authorisation:
Clinical Focus
Organisational Capacity and Capability
Clear and Credible Plan
Engagement with Patients and Communities
Leadership Capability and Capacity
Collaborative Arrangements Each of these domains has a set of criteria from which actions have been developed that will help us to secure the capacity and capabilities required to develop into an effective commissioning organisation. As part of the review of our OD Plan, we repeated our initial self assessment against the six domains, which demonstrates that we have made good progress in the three areas in which we identified the greatest room for improvement. These were ‘Engagement with Patients and Communities’, ‘Clear and Credible Plan’ and ‘Collaborative Arrangements’. As a result, we:
Have strengthened our patient and public involvement structures and process

5 | P a g e
Developed patient participation groups attached to 33 of our 35 practices
Run locality public engagement sessions in each of our five localities that will be repeated at regular intervals
Have a patient representative nominated by our patient membership on our Board
Hold our Board meetings in public
Developed our Integrated Strategy and Operating Plan 2012/13-2014/15
Our OD Plan for 2012/13 sets out the way in which we intend to further develop our organisation, our members and relationships with key strategic partners. Our plan is intended to develop the commissioning functions of the CCG and its member practices. OD is a positive change management process through which an organisation develops its internal capacity to deliver its core purpose efficiently and effectively to sustain itself long term. OD is an ongoing process and the content of our Plan sets out the progress we have already achieved during the transition year 2011/12 and the continuation of this development as we aspire to become a fully authorised CCG from April 2013. Our Plan recognises that we will require transformation change as an organisation as well as improved technical ability as commissioners, and there are three specific areas of OD that will need to be addressed to successfully achieve this:
Our organisational structure should provide the right people, with the right skills in the right roles
Our governance assurance is robust in order to ensure the management processes are in place to deliver our organisational objectives and statutory requirements
We have systems for capturing the progress of projects and programmes which enable the delivery
of improved health outcomes In order to successfully implement our OD Plan, we have ensured that it links closely with and is mutually supportive of other key organisational policies, plans and strategies:
Delivery Plan
Equality and Diversity Strategy
Communication and Engagement Plan
Financial Plan
Prime Financial Policies and Scheme of Delegation
Governance Framework
Human Resources Policy
Risk Register

6 | P a g e
3 Organisational Design Process
OD Process to Date The development of the CCG started in October 2010. The Board of North Staffordshire PCT asked the PCT’s three clinical constituencies, the Clinical Commissioning Committee, the Practice Based Commissioning Consortium and the QIPP clinical leads to lead the design and OD process.
The OD process has four stages, which are shown in figure below:
.
The forming stage took place from October 2010 to April 2011 and using the form follows function principle, was the initial design stage leading to the formation of the CCG. The aim of the forming stage was to design the organisational structure of the CCG, establish and appoint to the Board and assign PCT staff to the CCG.
The transition stage took place from April 2011 until October 2011 and was the period during which the PCT concluded transitioned its business to the CCG. The aim of the transition stage was to transition and embed the delegated responsibilities and business of the PCT to the new organisation
The developing stage took place between April 2011 and March 2012 and involved analysing the progress made by the CCG, understanding where development was required and moving towards a position where the CCG was ready for authorisation. The aim of the developing stage was to develop the CCG to a position where it was ready for authorisation.
The planning stage was initiated in March 2012 and involves assessing progress during the first shadow year, understanding where further development is needed and setting new aims for the further development of the CCG. The aim of the planning stage is to plan the further develop the CCG following its first year in shadow form.

7 | P a g e
The organisational design process set out in our Transition Plan for 2011/12 had a number of milestones that have been achieved. These are set out in the figure below:
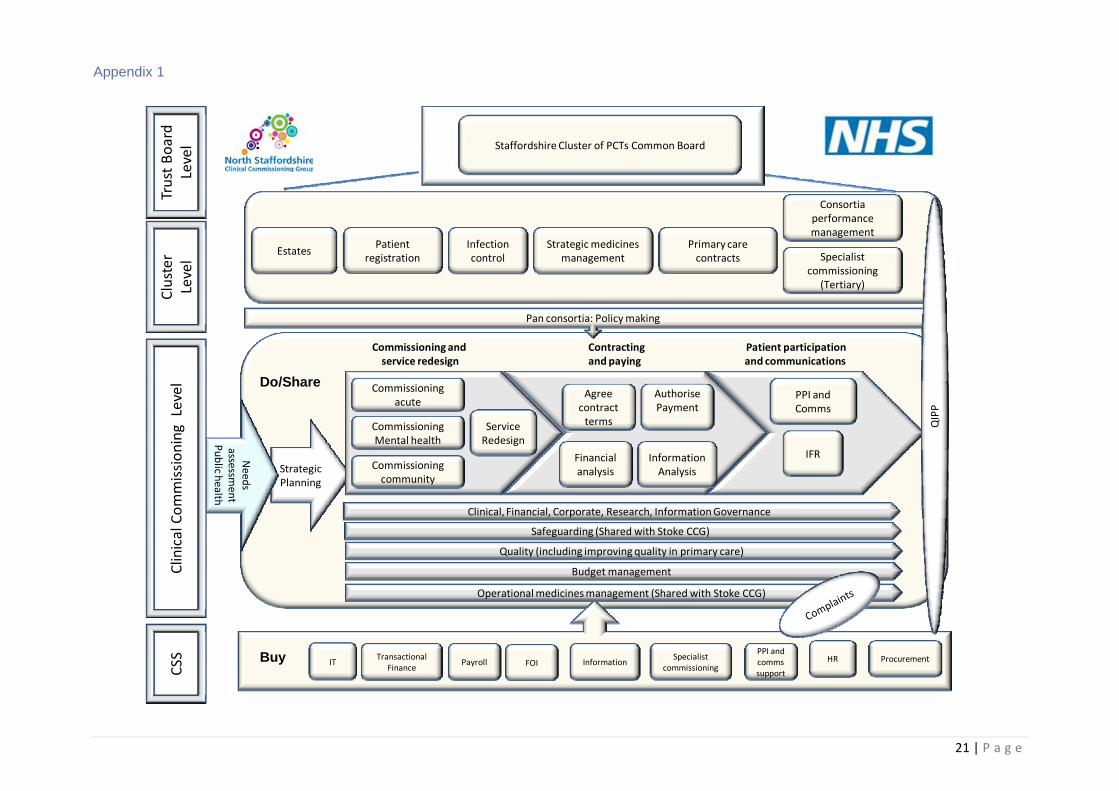
4 Organisational Structure As a result of the organisational design process, the CCG worked with the PCT during 2010/11 to decide on the functions it would directly manage, those that it would share with Stoke and other CCGs and those that it buy in from the Commissioning Support Service. The ‘Do, Buy, Share’ model is shown as Appendix 1. The CCG’s organisational structure is shown at Appendix 2 and reflects ‘Do, Buy, Share’, the CCG has a:
Governing Board
Committee structure
Clinical Associates
Assigned management team
Aligned Commissioning Support Service team
Strategic programmes
Locality structure
Governing Board The Board was established in April 2011. The Board structure is shown on the CCG organisational diagram shown in Appendix 3. All clinical Board members and lay members have been selected through an interview process and assessed against a job description and person specification to ensure they can demonstrate the leadership competencies and skills required to lead the CCG. Posts were advertised to all

8 | P a g e
GPs from the CCG’s 35 practices in January and February 2011. Clinical directors have a maximum tenure of four years and the full terms and conditions of the appointments are set out in the CCG’s Constitution. The vacant Board positions are being recruited to during June 2012.
Committee Structure The CCG’s committee structure is shown in Appendix 4. The current committee structure was agreed in November 2011 and ensures that the CCG has robust governance arrangements in place to enable it to expedite its responsibilities in an open and transparent manner.
Clinical Associates In addition to the clinical directors, the CCG employs clinical associates to work on time limited pieces of work to support the clinical directors and strategic programmes in designing and commissioning services. The clinical associates are GPs and along with the locality leads are the basis for succession planning. Some clinical associates will be developed into the next generation of clinical directors.
Assigned Management Team All CCG management and administration staff were assigned by the PCT to the CCG in March 2011 and were in post from 1 April 2011. Some minor changes have been made to the structure and vacancies are being recruited to in June. The employment of assigned staff will transfer to the CCG once authorised.
Aligned Commissioning Support Service (CSS) Team The Staffordshire CSS provides the CCG’s commissioning support services and staff have been aligned to and based with the CCG accordingly. Where functions are shared with neighbouring CCGs, equitable hosting arrangements have been agreed. The CSS is the CCG’s preferred supplier and the CCG has worked closely with the CSS to agree its product listing; the services it will be buying. The CCG’s Chief Financial Officer (CFO) and Chief Operating Officer (COO) have led the procurement of services from the CSS and the CFO leads on the contract with and the performance management of the CSS. The CSS supported the CCG during 2011/12 and is at an advanced stage of development having successful passed through Checkpoint 2 in the CSS authorisation process. A Heads of Agreement was signed by the CCG and CSS in May 2012. Strategic Initiative Programmes The CCG’s five programmes are:
Transforming Community Services
Planned Care
Unplanned Care
Mental Health
Practice Development, Performance and Education

9 | P a g e
In addition, we have a sixth programme, Health Improvement that now sits with Staffordshire County Council following Public Health’s move to the local authority. The Public Health team will continue to work closely with the CCG to deliver the range of health improvement initiatives that are critical to the successful achievement of our goals and outcomes. Each programme leads on the design and commissioning of services and initiatives to deliver the CCG’s goals and improve its outcomes. Each programme is:
The responsibility of a Clinical Director as sponsor and clinical lead (shared leadership model)
Managed by a designated Head of Commissioning
Supported by a multi-disciplinary team of commissioning managers and commissioning support staff
working in a matrix way
Shaped by stakeholder engagement
monitored by the CSS performance team under the lead of the COO and CFO and reported to the
Executive Committee monthly
Reported to the Board bi-monthly
Monitored using a standardised RAG rated highlight report and exception report where performance
is less than expected
Each programme has an outline three-year plan with milestones and an annual delivery plan, which specifies key activities, success metrics, monitoring metrics, milestones and major interdependencies. The plans for each programme form the Delivery Plan, which is updated annually. Internal accountability structures have been established. All of the Clinical Directors are members of the Executive Committee, which receives monthly monitoring reports. Reports are also routinely included on the Quality and Performance Committee.
Locality Structure Our five localities are the main mechanisms for engaging with our practice membership to prioritise, design and commission services for our population as well as tackling inequalities in health, variations in primary care and improving outcomes and quality in primary care. A locality map is attached as Appendix 5. Each locality has a GP Locality Lead and a Practice Manager Lead. The GP Locality Leads sit on the Executive Committee and ensure that the practices within their localities are able to shape and influence the CCG’s service design and commissioning processes. Each locality has a Patient Participation Group (PPG), which enables service users and local people to engage with the locality and shape its priorities and commissioning activities.
5 Running Costs The CCG’s organisational structure and staffing, both directly managed or shared with Stoke CCG and bought in from the CSS have to be affordable within the £25 per head of population running cost allocation. The CCG has a registered population of c213,000 so this equates to c£5.32m. The CCG has assessed its running costs (see below), and is confident that it will be within the target of £25 per head of population before April 2013 with some headroom.

10 | P a g e
The Staffordshire CSS has confirmed that it expects its cost per head of population from April 2013 to be no more than £11.00, and to be somewhere between £10.50 and £11.00. The CCG running cost of £13.52 assumes the full year effect of a full complement of staff. We have some in year appointments so this year’s running costs will be below the £13.52.
6 Organisational Values The CCG is committed to ensuring that quality and patient experience are at the very centre of its culture and commissioning activities. We intend to commission services that deliver the best possible outcomes for patients within the financial resources available to us. Our organisational values are encapsulated in our delivery priorities, which are:
We will commission safe, effective and high quality sustainable services
We will deliver better patient outcomes through effective, federated and collaborative arrangements with key partners
We will improve patient engagement, feedback and involvement in decisions throughout the whole
commissioning cycle
We will reduce health inequalities and inappropriate clinical variation
We will achieve all the above while remaining within financial balance and achieving best value
The way in which we communicate and engage with our practice members, service users, partners and providers is set out in our Communication and Engagement Strategy. Our plans to tackle discrimination and promote diversity, equality and inclusion are set out in our Equality and Diversity Strategy. The way in which we work with neighbouring CCGs is set out in our Federation Agreement.
Population = 212,959
Total Cost/
Cost Head
£ £
Running Cost Allowance 5,323,975 25.00
Corporate Base Costs 2,143,666 10.07
Clinical Leadership Costs 366,323 1.72
Minimum Costs of In-House Service 2,509,989 11.79
Estimated Staff Costs for Other CCG Functions 368,498 1.73
Total Estimated In-House Costs 2,878,487 13.52
Balance of Running Costs Available for CSS 2,445,488 11.48
CCG RUNNING COSTSAMOUNT FOR CSS

11 | P a g e
7 Capacity and Capability The CCG is a new organisation that aspires to be clinically led and professionally managed. We recognise that to become a world class commissioning organisation we need a staffing establishment which has the skills and is highly competent in commissioning, service redesign, strategic and financial planning, patient engagement and partnership working. During 2011/12, we focused on the delivery of more effective staff appraisal, personal development and support for and engagement with clinical, management and administration staff. Skills audits have been undertaken and are linked to personal develop plans and ongoing training needs analysis. An assessment of capacity and capability was undertaken by the PCT in 2009/10 and was repeated prior to the CCG being established in 2011 as part of the forming stage. It identified a number of strengths with areas for further improvement, including the following priorities to strengthen:
Contracting and provider management capacity, competency and capability
Knowledge management and fact-based prioritisation
Financial modelling and planning, including improved benchmarking/analysis
Public engagement capability
Communications capacity and capability
Programme and project management approach
Planning capacity and capability
Health market analysis and procurement skills/approaches
Organisation development capacity and capability From April 2011, a number of the functions that the PCT provided in house moved to the CSS along with the workforce that delivered them. However, the CCG retains responsibility for these areas even when bought in and has developed strategies and plans to guide the delivery of these functions by the CSS. For instance, a communications function is bought from the CSS, but is delivered in line with the CCG’s Communication and Engagement Strategy and the SLA with the CSS, which sets out the CCG’s specific communication requirements. Building on the work started by the PCT we developed a plan last year for internal development, securing specific external expertise in key areas where skills transference was essential. This has been particularly important for clinical leads that are now leading on critical commissioning functions with limited previous experience of doing so. Areas covered by our education and skills development programmes to date include:
Commissioning Cycle
Strategy development
Financial strategy/planning

12 | P a g e
Fact-based analysis and prioritisation
OD specialist skills and OD planning
Health market analysis
Programme management and project management
Staff development, improving effective appraisal and personal development plan
Executive coaching for clinical directors This has resulted in accelerated programmes of development for clinicians and managers. The work to develop the CCG’s commissioning capacity and capability is embedded in our Organisation Development Plan and based on our diagnostic self assessment.
8 Diagnostic Self Assessment As mentioned in section 2, the CCG carried out an initial self assessment in November 2011 using the DH’s, “GP Commissioning Emerging Consortia Self Assessment Diagnostic Tool”. The assessment was carried out against the following six domains:
Clinical focus and added value
Engagement with patients/communities
Clear and credible plan
Capacity and credibility
Collaborative arrangements
Leadership capacity and capability The results of the initial self assessment are shown below:
13 | P a g e
Whilst there was potential for development in all six domains, the Board prioritised three areas in particular for action:
Clear and Credible Plan
Engagement with Patients and Communities
Collaborative Arrangements In addition, a comprehensive domain review against all six domains was undertaken to highlight all gaps and areas of development. Each of the six domains was assigned a lead responsible for leading the domain review and implementing actions to address gaps and develop the CCG’s capacity and capability in these areas:
Domain Lead Clinical Focus and added value Executive Chair (Accountable Officer)
Engagement with patients /communities Executive Chair (Accountable Officer)
Clear and Credible Plan Chief Operating Officer
Capacity and Capability Chief Financial Officer
Collaborative Arrangements Chief Operating Officer
Leadership, capacity and capability Executive Chair , Chief Operating Officer, Chief Financial Officer
Some key actions undertaken included:
Preparing the Integrated Strategy and Operating Plan 2012/13-2013/14 (ISOP) to deliver our vision, strategic goals and outcomes and set out our strategy to 2015
Preparing supporting plans and strategies and refreshing the Delivery Plan for 2012/13 so that it was aligned to the ISOP goals and outcomes
Strengthening our locality patient involvement arrangements and preparing a Communication and Engagement Strategy to shape how we systematically and meaningfully engage service users and the public in our commissioning activities
Working with the local authority to review and revise existing joint commissioning arrangements and to develop a Memorandum of Understanding to cover how Public Health Directorate and the CCG will work together during 2012/13 as they transfer to the County Council
Following the actions undertaken by the domain leads between November 2011 and May 2012, the self assessment was repeated in May 2012 to inform a refresh of the OD Plan and to enable the CCG to progress through the planning stage of its development.

14 | P a g e
Improvements have been made across all domains and areas where further development is required have been identified. The self assessment has also been used to inform the OD aims that the CCG has used to frame its OD action plan for 2012/13.
9 Organisation Development Aims The CCG has used the OD diagnostic/self assessment tool to assess our current development against the six domains, to shape our five OD aims and to identify a number of key actions that we need to take to make further progress towards our goal of being authorised by April 2013. Our OD aims have been informed by our four OD priorities and are:
Develop the CCG as an effective commissioning organisation
Improve engagement with and the involvement of our members, staff, service users, partners and providers to shape our priorities and inform our commissioning activities
Develop the leadership competence and potential of CCG clinicians and managers
Improve the quality and safety of services commissioned by the CCG through fostering and developing a culture of innovation
Embed a culture of learning at every level in the organisation to develop our commissioning capacity and capability
For each of the five aims, we have summarised progress to date and identified what we need to do next with specific actions that will form our OD action plan (Appendix 6).
Aim 1 – Develop the CCG as an effective commissioning organisation

15 | P a g e
How are we doing? The CCG’s organisational structure has been based on the principle of form follows function. The structure reflects the functions that the CCG decided to do itself and share with Stoke CCG and enables the CCG to embed and manage functions it buys from the CSS. The CCG organisational structure and components along with the bought functions from the CSS are affordable within the £25 per head of population running costs limit. In developing its structure, the CCG made reference to wider health economy arrangements, particularly the Fit for the Future Programme, QIPP arrangements, the PCT’s strategic programmes and Stoke CCG’s emerging structure. We have ensured that the CCG’s strategic programmes provide an effective commissioning architecture to facilitate our commissioning activities, but also link with and deliver Fit for the Future and QIPP commitments and our federated agreements with Stoke CCG. Each strategic programme, which provide the focus for our annual Delivery Plan is led by a Clinical Director and Head of Commissioning, supported by clinical associates, commissioning managers and aligned CSS staff. This is in line with our key principle of being a clinically led, professionally managed organisation. The CCG has embedded the commissioning cycle in our everyday business, with Board level leadership of each stage of the cycle. We have adopted a programme and project management approach to implement the commissioning cycle, with clear plans, milestones and targets for each stage. We have led the redesign of various care pathways and services during our first year, using effective outcome focussed business processes to commission new services in line with our commissioning intentions, goals and outcomes. We have used the Joint Strategic Needs Assessment (JSNA) to determine our priorities and to ensure that tackling the health inequalities that exist across the CCG is a primary objective of each commissioned service or intervention. We have a clinically led prioritisation process coordinated by our Commissioning Priorities Advisory Group that helps to determine our investment and disinvestment and commissioning and decommissioning decisions. We have robust contracting and procurement arrangements in place with aligned CSS contract management teams for our acute, community, mental health and third sector contracts, and specialist procurement advice and a procurement policy that complies with EU rules for when we tender services. We have Quality Strategy that ensures that quality and patient experience are at the heart of all our commissioning processes and activities. With Stoke CCG a number of our clinical directors chair the contract Clinical Quality Review Meetings (CQRMs) for each of our main contracts. We routinely carry out health market analysis as part of our day to day commissioning activity and develop market management plans in areas where identify opportunities to develop the market for healthcare services, most recently for spinal surgery services. What do we need to do next? Whilst we have made good progress in our first year in shadow form, due in no small part to work initiated by the PCT over the past few years, we need to further develop our organisational effectiveness as a clinical commissioner in a number of areas. Service user involvement at the beginning of all service design and redesign is critical. We have developed an effective model in the recent redesign of orthotics and phlebotomy services and these needs to be rolled out and embedded across all commission functions and programme areas.

16 | P a g e
We aspire to matrix work across our strategic programme areas and whilst good in parts, more work needs to be done to avoid silo working and to better integrate joint working on cross cutting issues such as elderly care and long term conditions. Our focus needs to be on priority areas that in many cases cut across programme areas and not on the programmes themselves. We will implement additional training for clinicians and managers to facilitate matrix working and will review our structures to break down silos where they exist. Health market analysis needs to be carried out more widely and should inform service redesign and potential market testing, not be a result of a decision to test the market. Training in how to conduct health market analysis will be provided for all commissioners and an updated plan for further health market analysis put in place to inform commissioning intentions for 2013/14. Whilst the CCG has a systematic process for identifying health needs, for prioritisation and the commissioning of services, we need to get better at generating an evidence base to inform our commissioning decisions. We will work with the Public Health Intelligence and CSS Health Intelligence teams to develop a comprehensive evidence base to ensure we better understand what interventions do and do not work so we can target our resources more effectively to deliver our outcomes.
Action: Work with our PPI teams to build in service user involvement at the start of all service design and commissioning activities.
Action: Review structures and provide training to fully embed matrix working across the organisation.
Action: Provide training in health market analysis to all commissioning managers.
Action: Develop a comprehensive evidence base to inform all our commissioning activities.
Aim 2 – Improve engagement with and the involvement of our members, staff, service users, partners and providers to shape our priorities and inform our commissioning activities
How are we doing? Involving our service users and wider public is important to us and is one of our five delivery priorities. We have a Communication and Engagement Strategy that sets out our approach to patient and public involvement (PPI). We have worked closely with our localities and through the PPI team in the CSS, with our membership of over 2000 members, existing patient participation groups (PPGs) and other patient and public stakeholder groups to further develop our model of PPI. We have built PPI into every stage of the commissioning cycle and are working to ensure that this is firmly embedded in our day to day business. We have established a PPI structure that enables patient and public engagement at every level, from practices to the Board and beyond, and is based upon our patient membership scheme, patient participation groups attached to 33 of our 35 practices, a patient reference group, five patient locality groups and a Patient Congress, which is in development. In addition, there are three patient representatives on the Commissioning Priorities Advisory Group (CPAG), which as part of the CCG’s prioritisation process makes recommendations to the Executive Committee and Board on priorities for investment and disinvestment and commissioning and decommissioning decisions.

17 | P a g e
A patient rep sits on the Individual Funding Request (IFR) Review Group, which oversees the IFR process and work of the IFR panels in considering requests for treatments not routinely commissioned. The PPI team has built a model of engagement called ‘Customer Insight’, which ensures that a range of methods and mechanisms are used to engage patients and the public, to seek their views and input and for consultation purposes. Our practice membership is engaged through our five localities, through individual practice PDPE team listening visits, an education programme, the incentive scheme, QOF XL and the Quality and Productivity programme. The CCG is an active participant in the Staffordshire Health and Wellbeing Board. What do we need to do next? Our patient and public involvement mechanisms are developing well, but further development is needed to ensure that service users and the public can routinely inform and influence the CCG’s commissioning activity. We need to do more to engage communities to identify their health needs and aspirations and in decisions about priorities and strategies. Service user engagement in service design and improvement is good in some areas but needs to be routinely built into all commissioning processes. We must establish the patient congress, developing the role of the PPI Steering Group to drive forward the Communication and Engagement Strategy. We will build on the engagement event for the wider clinical community on 13 June 2012 to establish positive and effective links with non-GP clinicians and developing our engagement with the voluntary sector in terms of understanding their contribution and involving this sector in the patient congress. The CCG has inherited joint commissioning arrangements with the County Council from the PCT. The Joint Commissioning Unit (JCU), which is hosted by the Council, commissions a range of services on our behalf. The agreement has been extended to March 2013 but the Council and Staffordshire CCGs are reviewing the purpose of the JCU with a view to put in place arrangements that fit with the new commissioning landscape.
Action: Further develop locality and practice patient participation groups.
Action: Further work to develop and widen stakeholder engagement in service design and commissioning processes.
Action: Establish and develop the Patient Congress.
Action: Review the JCU and design with the County Council and staffordshire CCGs integrated commission arrangements that fit with the new commissioning landscape.
Aim 3 – Develop the leadership competence and potential of CCG clinicians and managers and the CCG as a whole
How are we doing? Each Clinical Director, as well as the COO and CFO, have an Executive Coach and have done since shortly after they were appointed in March 2011. They have undergone 360 assessments and these have formed the basis of development plans and provided focus for the coaching sessions.

18 | P a g e
The CCG has regular development days involving the whole CCG as well as Board development days. Informal Board meetings/seminars held every two months also provide opportunities for the Board to undertake more in depth learning around key strategic and governance issues. The clinical associates and locality leads are supported to develop their leadership potential with a view to their becoming the next generation of clinical directors. All clinicians and managers have monthly one to ones and have personal development plans linked to their objectives, which provide opportunities to identify gaps in leadership skills and opportunities to develop them. Each of our strategic programmes is led by a Clinical Director, supported by an experienced head of commissioning and commissioning managers. This provides hands on opportunities and experience for clinicians to develop their clinical leadership skills on a day to day basis. What do we need to do next? We are exploring the potential to widen access to coaches to other senior managers as part of their personal development plans and to build on their leadership potential. We are exploring the potential to develop a Leadership Academy for clinicians and managers as part of wider succession planning. This will help to ensure that we have clinicians ready to take on leadership roles at Board level and that there is greater completion for clinical director roles as they become available. We are exploring leadership training, development and coaching for the localities.
Action: Widen access to coaching to senior managers.
Action: Develop Leadership Academy.
Aim 4 – Improve the quality and safety of services commissioned by the CCG through fostering and developing a culture of Innovation
How are we doing? We have well established Clinical Quality Review Meetings (CQRMs) for each of our main provider contracts, which enable quality and patient safety issues to be identified with providers and addressed early. Our Quality Strategy provides a clear framework with principles and outcomes for quality improvement. The Quality Strategy sets out our plan to embed quality into the commissioning cycle and for gaining assurance from provider organisations in the transition period to April 2013, whilst the CCG moves towards authorisation. The Quality and Performance Committee is a sub-committee of the CCG Board. The Committee provides a forum for robust debate around quality issues and enables the CCG to be proactive in monitoring and promoting quality outcomes. The Committee provides an interface between the CCG Board and the CSS contract management teams. The Committee reviews quality, performance and patient safety data with a view to understanding the impact of provider performance on outcomes for patients. The Committee provides an additional level of

19 | P a g e
governance around quality and its membership includes the Board’s appointed lay members and provides assurance to the CCG Board. The CCG has a range of mechanism for gauging patient experience and for using it to help redesign care pathways and services in innovative ways that improve patient experience and outcomes. Our PDPE team works with localities and practices through QOF XL and the Quality and Productivity indicators to identify, support and develop innovative approaches to service and care pathway design. A recent example is the redesign of the renal colic pathway, which was led by GPs in one locality, rolled out to the other localities and commissioned from the local acute trust. We encourage innovation from practices through our locally agreed incentive scheme to drive improvements in the quality of care. We have developed and promote clinical guidelines to ensure that referrals from GPs to secondary care are consistent with local protocols and of consistently high quality. We also support and fund a locality innovation scheme which is allowing a number of imaginative commissioning ideas to become a reality whilst robustly monitoring their outcomes and matching to CCG priorities. We have a commitment to looking outwards for examples of best practice and seek to learn from other organisations To maximise clinical quality in primary care we have developed a targeted practice education scheme which focuses on areas of clinical priority and need at individual, practice, locality, CCG membership level and across the wider LHE. What do we need to do next? Whilst the PCT has robust safeguarding arrangements in place, the responsibility for both adult and children’s safeguarding transfers to the CCG during 2012/13. A training programme led by the lead nurses for safeguarding, who will be transferring to the CCG this year will be in place from September 2012 to ensure that all CCG staff understand their safeguarding responsibilities and comply with them when commissioning services. We are in the process of recruiting a practice nurse facilitator to support practices and localities to improve their clinical quality, performance and education.
Action: Put in place safeguarding training plan from 1 September 2012 and implement safeguarding training for all CCG clinicians and staff.
Action: Recruit practice nurse facilitator to support practice quality, performance and education programmes.
Aim 5 – Embed a culture of learning at every level of the organisation to develop our commissioning capabilities and capacities.
How are we doing? Building on the work started by the PCT and informed by the OD diagnostic/self assessment we developed a plan last year for internal development, securing specific external expertise in key areas where there were knowledge and skills gaps. This was important for clinical leads leading on critical commissioning functions with limited previous experience of doing so. The education and skills development opportunities included

20 | P a g e
elements of the commissioning cycle, financial planning, governance, health market analysis and strategic planning. The Practice Development, Performance and Education Team coordinate the delivery of an education programme across the five localities, which is designed to develop the commissioning competence and capabilities of individual GPs and practices and enables the localities to become effective locality commissioners and to manage their delegated budgets. What do we need to do next? We need to build on the education and skills development programme, rolling it out across the localities and covering new areas identifies through one to ones and skills and knowledge audits. Training is planned to ensure that all clinicians and managers fully understand the public sector Equality Duty and further equality and diversity training in line with our Equality and diversity Strategy is planned. In particular training to carry out equality assessments where required to ensure that all policies, strategies and services build in and carry out their
Action: Expand and roll out education and skills development programme.
Action: Train all clinicians and managers to undertake equality assessments and to carry them out at the planning phase of all commissioning and policy/strategy development processes.
10 Roles and Responsibilities The roles and responsibilities for ensuring the OD Plan is successfully implemented and its aims achieved are as follows:
The Accountable Officer is responsible for the development of the organisation and its authorisation as a statutory body by April 2013
The Chief Operating Officer has delegated responsibility for delivery of the OD Plan
The Chief Financial Officer has delegated responsibility for ensuring that governance arrangements are reviewed and developed in line with the OD Plan and that the OD Plan aligns with the principles of good governance set out the the CCG’s governance framework
The CCG Development Manager has day to day responsibility for delivery of the OD Plan
11 Implementing and Monitoring the Plan The action plan is attached as Appendix 6 sets out lead responsibilities and timescales for the actions to be delivered. The Board will receive a report at each bi-monthly meeting on progress in implementing the Plan and any issues that arise on which it needs to be sighted. The Organisational Development and Transition Group, which is a sub-committee of the Board will lead on the implementation of the OD Plan and leads on OD issues for the CCG.
21 | P a g e
Appendix 1
Strategic Planning
Commissioning acute
Commissioning Mental health
Commissioning community
Service Redesign
Agree contract terms
Authorise Payment
Commissioning and service redesign
Contracting and paying
Patient participationand communications
PPI and Comms
Budget management
Need
s assessm
ent
Public h
ealth
IFRFinancial analysis
InformationAnalysis
Staffordshire Cluster of PCTs Common Board
Strategic medicines management
Consortia performance management
Primary care contracts
EstatesPatient
registration Specialist commissioning
(Tertiary)
Pan consortia: Policy making
ITTransactional
Finance
PPI and commssupport
InformationSpecialist
commissioningPayroll HR
Trust Board
Level
Cluster
Level
Clinical Commissioning Level
CSS
QIPP
Infection control
Operational medicines management (Shared with Stoke CCG)
Quality (including improving quality in primary care)
Clinical, Financial, Corporate, Research, Information Governance
Safeguarding (Shared with Stoke CCG)
Do/Share
Buy ProcurementFOI

22 | P a g e
Appendix 2
PA/Admin Support PA to COO PA to CFO
PA to Clinical Directors/PDPE Team
Administration Officer
Commissioning Support Manager
( Management and Practice Development Accountant
Head of Medicines
Management Shared 50:50 with Stoke
CCG Development Manager
Office
Manager/ Executive Assistant
Clinical Director Unplanned
Care
Clinical Director Planned Care
Clinical Director TCS
ChiefOperating Officer
Commissioning Managers x4
Locality Support Manager
Clinical Audit
Facilitator
Practice Support
Technician / NICE
Technician
Head of Commissioning x 3
Unplanned Care Planned Care
TCS
Head of Commissioning
Practice Development Performance &
Education
Senior Commissioning Manager x2
Senior Commissioning
Manager Locality & Practice
Engagement
Joint Commissioning
Unit
Adult Mental Health LTC’s
Learning Disabilities
Prevention and Independence
Lead Commissioning
Manager ‐ Children and Non‐acute
CSS
Project Support Manager
Locality Leads
Chair of Governing Board
Accountable Officer (GP)
Governing Board
Clinical Member Secondary
Care S i li t
Clinical Member Registered Nurse
Head of Governance
Prescribing Advisor Primary Care
Clinical Director Mental Health
Clinical Director PDPE
Clinical Director Quality &
Engagement
N GP
Lay Member Public &
Patient Lead
Senior Prescribing Advisor
Practice Support
Technician
Practice Support
Technician
Practice Support
Technician
Chief Finance Officer
Shared 50:50 with Stoke
Deputy Chief Finance Officer
Shared 50:50 with Stoke
Safeguarding Nurses x2
Shared 50:50 with Stoke
Head of Quality
Lay Member Governance
Lead
Clinical Associates

23 | P a g e
Appendix 3
North Staffordshire Clinical Commissioning Group Governing Board
Clinical Director
Unplanned Care
Dr Richard Page
Clinical Director Planned Care
Dr Sunil Angris
Dr Vamsi
Clinical Director TCS
Dr Alison Bradley
Dr Latif Hussain
Chief Operating Officer
Marcus Warnes
Chair of Governing Board
Accountable Officer(GP)
Dr David Hughes
Clinical Member – Secondary
Care Specialist Vacant
Clinical Member – Registered Nurse Vacant
Clinical Director Mental Health
Dr Paul Unyolo
Clinical DirectorPractice
Development Performance &
Education Dr Julie Oxtoby
Clinical Director Quality &
Engagement Non GP Clinician Sally Parkin
Lay Members
x2 (Vacant) Interviews 14th&19th June
ChiefFinancial Officer
Tony Matthews
Stoke CCG representativ
e
Andrew
Bartlam
Local Representative Committees
LMC Paul Scott LPC Tanya Cork
PCT Cluster representative
Brigid Stacey
Patient Representative Interim Joyce Tagell
Public Health Consultant or Senior Representative Dr Aliko Ahmed Jackie Small
LA Member – Vanessa Pugh Voting
Member Observers
Invited members
Other Members of the public Press

24 | P a g e
North Staffordshire Clinical Commissioning Group Governing Board
Links to other Local Committees/Boards
(External)
Contract & Quality Executive Committee
CSS Project Board
Fit for the Future
Steering Group
Health & Wellbeing Board
Health Economy NICE
Implementation Group
Emergency Care Network
Commissioning Boards
Operational Meetings
(Internal)
Heads of Service
and Clinical
Directors
CCG Executive
Committee
Commissioning
Team Meeting
Patient Congress
(to be
established)
Audit Committee
(To be established)
Remuneration Committee
(To be established)
Performance & Quality
Committee
Clinical Priorities Advisory Group
Organisational Development & Transition Group
CCG Primary Care Performance & Quality Sub Committee
Medicines Management Committee
Clinical Quality Review Meeting
UHNS/SSOTP/CHC
Localities Leads
meeting
Appendix 4

25 | P a g e
Appendix 5

26 | P a g e
Appendix 6 – Action Plan
Aim Action Outcomes Lead Timescale
Develop the CCG as an effective commissioning organisation
Work with our PPI teams to build in service user involvement at the start of all service design and commissioning activities
Evidence of service user involvement in commissioning activities
Clinical Director of Quality, Engagement and Partnerships
March 2013
Review structures and provide training to fully embed matrix working across the organisation
Evidence of matrix working across CCG Chief Operating Officer
March 2013
Provide training in health market analysis to all commissioning managers
HMA carried across all programme areas Chief Operating Officer
March 2013
Develop a comprehensive evidence base to inform all our commissioning activities
Evidence base developed and utilised Chief Operating Officer
March 2013 and ongoing
Improve engagement with and the involvement of our members, staff, service users, partners and providers to shape our priorities and inform our commissioning activities
Further develop locality and practice patient participation groups.
Evidence that PPGs embedded in commissioning cycle
Clinical Director of Quality, Engagement and Partnerships
October 2012
Further work to develop and widen stakeholder engagement in service design and commissioning processes.
Evidence of wider stakeholder involvement in commissioning activities
Clinical Director of Quality, Engagement and Partnerships
March 2013
Establish and develop the Patient Congress. Patient Congress established Clinical Director of Quality, Engagement and Partnerships
September 2012
Review the JCU and design with the County Council and Staffordshire CCGs integrated commission arrangements that fit with the new commissioning landscape.
Revised integrated commissioning arrangements in place
Chief Operating Officer
March 2013

27 | P a g e
Develop the leadership competence and potential of CCG clinicians and managers and the CCG as a whole
Widen access to coaching to senior managers. Coaching available to senior managers Chief Operating Officer
March 2013
Develop Leadership Academy. Leadership Academy established Chief Operating Officer
March 2013
Develop leadership training, development and coaching for the localities
Locality development programme in place Clinical Director for PDPE
March 2013
Improve the quality and safety of services commissioned by the CCG through fostering and developing a culture of innovation
Put in place safeguarding training plan from 1 September 2012 and implement safeguarding training for all CCG clinicians and staff.
All staff trained and operating in line with safeguarding duties
Clinical Director of Quality, Engagement and Partnerships
Chief Operating Officer
December 2012
Recruit practice nurse facilitator to support practice quality, performance and education programmes.
Facilitator recruited Clinical Director for PDPE
July 2012
Embed a culture of learning at every level in the organisation to develop our commissioning capacity and capability
Expand and roll out education and skills development programme.
Programme rolled out across CCG CCG Development Manager
October 2012
Train all clinicians and managers to undertake equality assessments and to carry them out at the planning phase of all commissioning and policy/strategy development processes.
All staff trained and carrying out EAs Head of Governance
October 2012