oregon board of pharmacy · karbowicz #c2 action necessary ... budget orbits financial adj budget...
TRANSCRIPT
Note: Thursday’s meeting will start at 9:30AM.
Agenda – February 7-8, 2018 NOTE: The Board may rearrange its agenda to accommodate the Board or members of the public.
Page 1 of 4
Oregon Board of Pharmacy
BOARD MEETING AGENDA Meeting Location:
Portland State Office Building 800 NE Oregon Street, Portland, OR 97232
February 7-8, 2018 Updated 2/6/18
The mission of the Oregon State Board of Pharmacy is to promote, preserve and protect the public health, safety and welfare by ensuring high standards in the practice of pharmacy and by
regulating the quality, manufacture, sale and distribution of drugs.
WEDNESDAY, FEBRUARY 7, 2018 I. 8:30AM OPEN SESSION, Penny Reher, R.Ph, Presiding
A. Roll Call B. Agenda Review and Approval Action Necessary
II. Contested Case Deliberation pursuant to ORS 192.690(1) - Not Open to the Public
III. EXECUTIVE SESSION – NOT OPEN TO THE PUBLIC, pursuant to ORS 676.175, ORS 192.660 (1) (2) (f) (k). A. Items for Consideration and Discussion: 1. Deliberation on Disciplinary Cases and Investigations 2. Personal Appearances 3. Deficiency Notifications 4. Case Review IV. OPEN SESSION - PUBLIC MAY ATTEND - At the conclusion of Executive Session, the Board may convene Open Session to begin some of the following scheduled agenda items - time permitting at approximately 3:30PM. V. Approve Consent Agenda* Action Necessary
*Items listed under the consent agenda are considered to be routine agency matters and will be approved by a single motion of the Board without separate discussion. If separate discussion is desired, that item will be removed from the consent agenda and placed on the regular business agenda.
1. NAPLEX Scores – none 2. MPJE Scores – none
Wednesday, February 7, 2018 @ 8:30AM – Conference Rm A Thursday, February 8, 2018 @ 9:30AM – Conference Room A
≈ If special accommodations are needed for you to attend or participate in this Board Meeting, please contact
Loretta Glenn at: (971) 673-0001. ≈

Note: Thursday’s meeting will start at 9:30AM.
Agenda – February 7-8, 2018 NOTE: The Board may rearrange its agenda to accommodate the Board or members of the public.
Page 2 of 4
3. License/Registration Ratification – November 29, 2017-February 2, 20184. Pharmacy Technician Extensions – none5. Board Minutes – November 7-8, 2017
VI. ISSUES/ACTIVITIES
A. Board Meeting Dates• April 4-5, 2018 Portland • June 6-7, 2018 Portland • August 8-10, 2018* Portland (*3 day meeting) • October 3-4, 2018 Portland • November 7-8, 2018 Portland (Strategic Planning) • December 12-13, 2018 Portland • February 6-8, 2019* Portland (*3 day meeting) • April 3-4, 2019 Portland updated • June 5-6, 2019 Portland • August 7-9, 2019* Portland (*3 day meeting) • October 2-3, 2019 Portland updated • November 6-7, 2019 Portland (Strategic Planning) • December 11-12, 2019 Portland
B. Rulemaking Hearing Dates(The following dates are reserved for potential rulemaking hearings and identified only for planning purposes and approved by theBoard. Actual Rulemaking Activities will be noticed as required by law and may deviate from this schedule as needed.)
• May 23, 2018• November 27, 2018• May 22, 2019• November 26, 2019
C. Committees/Meetings1. OSPA Lane County – 2/17-18/2018, Eugene – Watt/ DeBarmore/Frost/Baldwin2. OSHP Annual Meeting – 4/27-29/2018, Gleneden Beach3. NABP 114th Annual Meeting – 5/5-8/2018, Denver, CO Action Necessary4. NABP District VI-VIII, meeting Kansas City, MO 10/14-17/2018
D. Board Member/Staff Presentations – Reher• Pharmacy Coalition – 1/9/18, 2/13/18• Professional Practice Roundtable – 1/23/18• Naloxone Outreach – Roseburg/Eugene 2/12-13/2018 - Karbowicz
E. Financial/Budget Report – Watt/MacLean #A-A1
F. Legislative update – Watt• 2018 Session 2/5/18 – 3/10/18
o Opioid Task Force update

Note: Thursday’s meeting will start at 9:30AM.
Agenda – February 7-8, 2018 NOTE: The Board may rearrange its agenda to accommodate the Board or members of the public.
Page 3 of 4
G. Reports: 1. Board President/Members 2. Executive Director
3. Board Counsel 4. Compliance Director
5. Pharmacist Consultant 6. Administrative Director 7. Licensing Department Supervisor 8. Project Manager
Adjourn
THURSDAY, FEBRUARY 8, 2018 9:30AM VII. OPEN SESSION, Penny Reher, R.Ph, Presiding
A. Roll Call B. Motions for Contested Cases & Disciplinary Action Action Necessary
(Some or all of the items below may be re-arranged and occur before or after lunch depending on the length of the Board’s discussions.)
9:00 AM VIII. GENERAL ADMINISTRATION
A. Rules *First Look ** Second Look *** Third Look
1. Rules Process Changes - Watt 2. Review Rulemaking Hearing Report & Comments – none 3. Consider Adoption of Rules – none 4. Consider Adoption of Temporary Rules - none 5. Rules Review
• Div 045 – Compounding * #B and B1 • Div 019 - Naloxone Temp. Rule ** #B2
6. Consider Rules and send to Rulemaking Hearing - None 7. Policy Issues for Discussion – Karbowicz/Efremoff
• Div 019 & 041 – Community Pharmacy Personnel/PIC *** #B3 • 5-year Rule Review
B. Discussion Items
1. Waiver Requests - none 2. Providence 1-yr TCVP Report – Efremoff/Karbowicz #C Action Necessary 3. Providence 5-yr TCVP Request - Efremoff/Karbowicz #C1Action Necessary 4. OBOP Syringe Access Position Statement for review and possible approval –
Karbowicz #C2 Action Necessary 5. Pharmacy Technician Exam Updates #C3-C4
Note: Thursday’s meeting will start at 9:30AM.
Agenda – February 7-8, 2018 NOTE: The Board may rearrange its agenda to accommodate the Board or members of the public.
Page 4 of 4
6. Drug Shortages - Reher 7. Governor’s Advisory Committee on DUII - Watt 8. Recognition of outgoing Board Member Christine Chute - Reher
Noon – Lunch break
C. Public Health and Pharmacy Formulary Advisory Committee - Watt/Frost
1. 1.24.18 Committee meeting update 2. Advisory Committee/Board Flowchart #D 3. Draft Concept Intake Form 4. Committee Recommendations - none 5. Tentative Committee meeting dates: 2/16/18, 4/13/18, 7/13/18, 10/26/18
D. Strategic Planning – Watt/MacLean
• Prioritize Topics from 2017 meeting
IX. OPEN FORUM – At the completion of regular Board business, the Board provides an opportunity to make comments or present issues of general interest. The Board will not deliberate any issues or requests during Open Forum. Therefore, Open Forum should not be used to make formal requests to the Board, nor to address issues currently under investigation or requests pending before the Board. If you wish to be called upon, please sign up on the sheet at the podium in advance for inclusion. Adjourn

BOARD OF PHARMACYAY19 CASH FLOW - November 2017OF Appn 30235
LAB Rstars EBoard or AdjustedBudget ORBITS Financial Adj Budget or Financial ACTUALS UnobligatedObjects REVENUE & EXPENDITURES BUDGET Plan Salary Pot Plan To Date BalanceREVENUE
0205 Other Business Licenses 4,431,667 4,431,667 4,431,667 1,107,878 3,323,790 25%0210 Other NonBusiness Licenses and Fee 505,552 505,552 505,552 41,634 463,918 8%0505 Fines and Forfeits 420,000 420,000 420,000 75,929 344,071 18%0605 Interest and Investments 48,000 48,000 48,000 31,200 16,800 65%0975 Other Revenue 39,700 39,700 39,700 22,148 17,552 56%
SubTotal Revenue 5,444,919 5,444,919 0 5,444,919 1,278,788 4,166,131 23%TRANSFERS
2443 Transfer out to OHA--Workforce Dat (409,357) (409,357) (409,357) 0 (409,357) 0%2443 Transfer out to OHA--PDMP program 0 0 0 - 0 0%
SubTotal Transfers (409,357) (409,357) 0 (409,357) 0 (409,357) 0%TOTAL REVENUE & TRANSFERS 5,035,562 5,035,562 0 5,035,562 1,278,788 4,575,488 25%
PERSONAL SERVICES3110 Regular Employees 3,191,268 3,270,388 3,270,388 656,404 2,654,973.43 20%
Board Member Stipends 40,990 40,990 - 3160 Temporary Appointments 25,222 - 0 - - 0%3170 Overtime Payments - 0 - - 0%3190 All Other Differential O/Class Lead W 183,457 208,454 208,454 40,482 167,972 19%3210 Employment Relations Board Assess 1,083 1,100 1,100 210 890 19%3220 Public Employees Retirement Contri 504,012 342,953 342,953 94,071 248,882 27%3221 Pension Bond Contribution 195,224 180,023 180,023 38,924 141,099 22%3230 Social Security Taxes 256,020 261,922 261,922 48,695 213,227 19%3240 Unemployment Assessment 0 - - 0%3250 Workers' Compensation Assessment 1,380 1,127 1,127 203 924 18%3260 Mass Transit Tax 20,334 20,873 20,873 4,168 16,705 20%3270 Flexible Benefits 666,720 688,091 688,091 127,940 560,150 19%3455 Vacancy Savings-ORBITS only (169,448) 0 - - 0%3465 Reconciliation Adjustment-ORBITS only 0 - - 0%3470 Undistributed Personal Services-ORBITS 0 - - 0%3991 PERS Policy Adjustment-ORBITS 0 - - 0%
SubTotal Personal Services 4,875,272 5,015,919 - 5,015,919 1,011,097 4,004,823 20%SERVICES AND SUPPLIES Proj all
4100 InState Travel 102,270 102,270 102,270 16,717 85,553 16%4125 Out of State Travel 15,724 15,724 15,724 1,131 14,593 7%4150 Employee Training 52,335 52,335 52,335 5,220 47,115 10%4175 Office Expenses 123,883 123,883 123,883 14,371 109,512 12%4200 Telecommunications 43,879 43,879 43,879 6,709 37,170 15%4225 State Govt. Service Chgs. 119,969 119,969 119,969 20,206 99,763 17%4250 Data Processing 73,694 73,694 73,694 15,507 58,187 21%4275 Publicity & Publications 37,712 37,712 37,712 2,987 34,725 8%4300 Professional Services 402,408 402,408 402,408 64,495 337,913 16%4315 IT Professional Services 353,340 353,340 353,340 10,500 342,840 3%4325 Attorney General 326,595 326,595 326,595 102,841 223,754 31%4375 Employee Recruitment & Develop 207 207 207 - 207 0%4400 Dues & Subscriptions 4,583 4,583 4,583 310 4,273 7%4425 Facilities Rent & Taxes 219,519 219,519 219,519 39,578 179,941 18%4475 Facilities Maintenance 51 51 51 - 51 0%4525 Medical Supplies and Services 1,110 1,110 1,110 1,697 (587) 153%4575 Agency Program Related S&S 229,434 229,434 229,434 35,913 193,521 16%4650 Other Services & Supplies 278,652 278,652 278,652 144,089 134,563 52%4700 Expendable Property 10,499 10,499 10,499 15 10,484 0%4715 IT Expendable Property 43,976 43,976 43,976 1,053 42,923 2%5550 Data Processing Software - 0 - - 0%5600 Data Processing Hardware 8,296 8,296 8,296 - 8,296 0%
0 - SubTotal Services and Supplies 2,448,136 2,448,136 - 2,448,136 483,339 1,964,797 20%
SPECIAL PAYMENTS6085 Other Special Payments 11,991 11,563 11,563 - 11,563 0%6443 Special Payments to OHA-HPSP 176,899 176,899 - 176,899 0%
SubTotal Transfers 11,991 188,462 0 188,462 0 188,462 0%
Total Expenditures Budget 7,335,399 7,652,517 - 7,652,517 1,494,435 6,158,082 20%7,057,070
LAB % PS 66% 66% Target 100%LAB % S&S 33% 32%LAB % SP 0% 2%
CashAY17 Ending Cash Balance 4,794,930Revenue less Expenditures ActualsTotal Revenue & Transfers 1,278,788Total Expenditures (1,494,435)Total Revenues & Transfers less Expenditures (215,647) (215,647)AY19 Cash Balance after the Fiscal Month Closed 4,579,283
Budgeted Revenues not yet received (zero) less Estimated Transfers to OHA-PMP & Workforce Data program to be mad 0Budgeted Expenditures not yet spent (6,158,082) AY19 Estimated Cash Balance (1,578,799)Cash Balance Contingency (Months) (5.17) months
% Expended
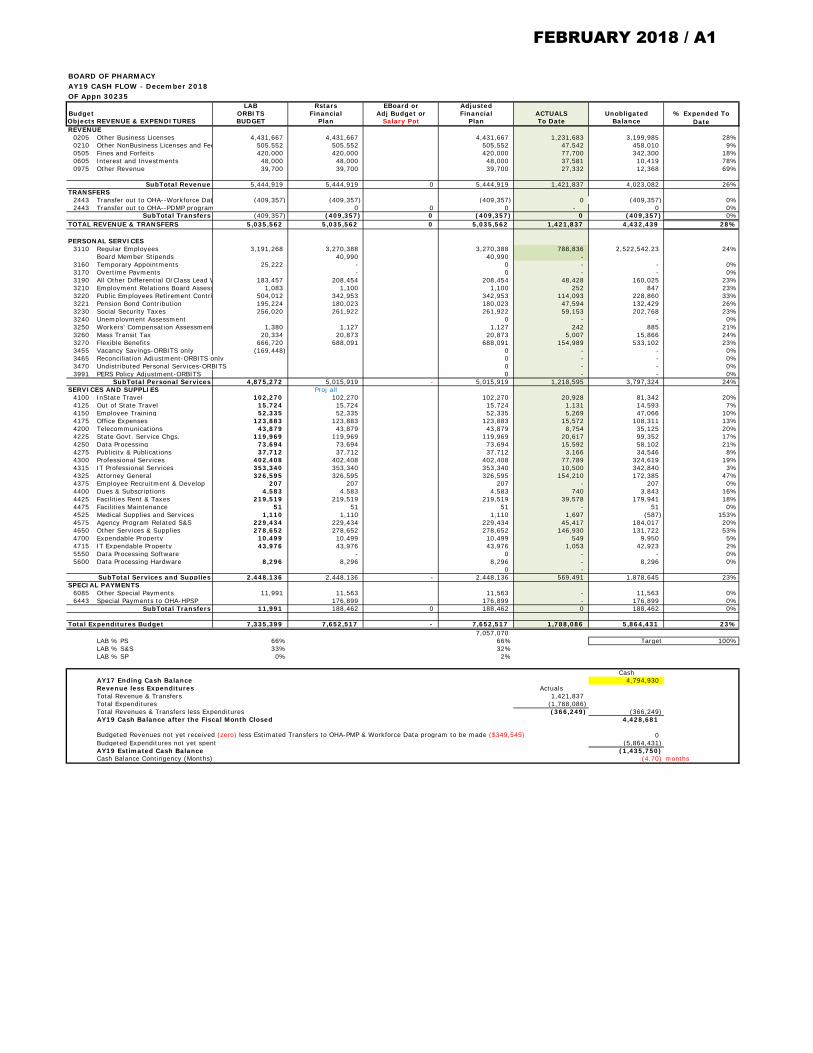
BOARD OF PHARMACYAY19 CASH FLOW - December 2018OF Appn 30235
LAB Rstars EBoard or AdjustedBudget ORBITS Financial Adj Budget or Financial ACTUALS UnobligatedObjects REVENUE & EXPENDITURES BUDGET Plan Salary Pot Plan To Date BalanceREVENUE
0205 Other Business Licenses 4,431,667 4,431,667 4,431,667 1,231,683 3,199,985 28%0210 Other NonBusiness Licenses and Fee 505,552 505,552 505,552 47,542 458,010 9%0505 Fines and Forfeits 420,000 420,000 420,000 77,700 342,300 18%0605 Interest and Investments 48,000 48,000 48,000 37,581 10,419 78%0975 Other Revenue 39,700 39,700 39,700 27,332 12,368 69%
SubTotal Revenue 5,444,919 5,444,919 0 5,444,919 1,421,837 4,023,082 26%TRANSFERS
2443 Transfer out to OHA--Workforce Dat (409,357) (409,357) (409,357) 0 (409,357) 0%2443 Transfer out to OHA--PDMP program 0 0 0 - 0 0%
SubTotal Transfers (409,357) (409,357) 0 (409,357) 0 (409,357) 0%TOTAL REVENUE & TRANSFERS 5,035,562 5,035,562 0 5,035,562 1,421,837 4,432,439 28%
PERSONAL SERVICES3110 Regular Employees 3,191,268 3,270,388 3,270,388 788,836 2,522,542.23 24%
Board Member Stipends 40,990 40,990 - 3160 Temporary Appointments 25,222 - 0 - - 0%3170 Overtime Payments - 0 - - 0%3190 All Other Differential O/Class Lead W 183,457 208,454 208,454 48,428 160,025 23%3210 Employment Relations Board Assess 1,083 1,100 1,100 252 847 23%3220 Public Employees Retirement Contri 504,012 342,953 342,953 114,093 228,860 33%3221 Pension Bond Contribution 195,224 180,023 180,023 47,594 132,429 26%3230 Social Security Taxes 256,020 261,922 261,922 59,153 202,768 23%3240 Unemployment Assessment 0 - - 0%3250 Workers' Compensation Assessment 1,380 1,127 1,127 242 885 21%3260 Mass Transit Tax 20,334 20,873 20,873 5,007 15,866 24%3270 Flexible Benefits 666,720 688,091 688,091 154,989 533,102 23%3455 Vacancy Savings-ORBITS only (169,448) 0 - - 0%3465 Reconciliation Adjustment-ORBITS only 0 - - 0%3470 Undistributed Personal Services-ORBITS 0 - - 0%3991 PERS Policy Adjustment-ORBITS 0 - - 0%
SubTotal Personal Services 4,875,272 5,015,919 - 5,015,919 1,218,595 3,797,324 24%SERVICES AND SUPPLIES Proj all
4100 InState Travel 102,270 102,270 102,270 20,928 81,342 20%4125 Out of State Travel 15,724 15,724 15,724 1,131 14,593 7%4150 Employee Training 52,335 52,335 52,335 5,269 47,066 10%4175 Office Expenses 123,883 123,883 123,883 15,572 108,311 13%4200 Telecommunications 43,879 43,879 43,879 8,754 35,125 20%4225 State Govt. Service Chgs. 119,969 119,969 119,969 20,617 99,352 17%4250 Data Processing 73,694 73,694 73,694 15,592 58,102 21%4275 Publicity & Publications 37,712 37,712 37,712 3,166 34,546 8%4300 Professional Services 402,408 402,408 402,408 77,789 324,619 19%4315 IT Professional Services 353,340 353,340 353,340 10,500 342,840 3%4325 Attorney General 326,595 326,595 326,595 154,210 172,385 47%4375 Employee Recruitment & Develop 207 207 207 - 207 0%4400 Dues & Subscriptions 4,583 4,583 4,583 740 3,843 16%4425 Facilities Rent & Taxes 219,519 219,519 219,519 39,578 179,941 18%4475 Facilities Maintenance 51 51 51 - 51 0%4525 Medical Supplies and Services 1,110 1,110 1,110 1,697 (587) 153%4575 Agency Program Related S&S 229,434 229,434 229,434 45,417 184,017 20%4650 Other Services & Supplies 278,652 278,652 278,652 146,930 131,722 53%4700 Expendable Property 10,499 10,499 10,499 549 9,950 5%4715 IT Expendable Property 43,976 43,976 43,976 1,053 42,923 2%5550 Data Processing Software - 0 - - 0%5600 Data Processing Hardware 8,296 8,296 8,296 - 8,296 0%
0 - SubTotal Services and Supplies 2,448,136 2,448,136 - 2,448,136 569,491 1,878,645 23%
SPECIAL PAYMENTS6085 Other Special Payments 11,991 11,563 11,563 - 11,563 0%6443 Special Payments to OHA-HPSP 176,899 176,899 - 176,899 0%
SubTotal Transfers 11,991 188,462 0 188,462 0 188,462 0%
Total Expenditures Budget 7,335,399 7,652,517 - 7,652,517 1,788,086 5,864,431 23%7,057,070
LAB % PS 66% 66% Target 100%LAB % S&S 33% 32%LAB % SP 0% 2%
CashAY17 Ending Cash Balance 4,794,930Revenue less Expenditures ActualsTotal Revenue & Transfers 1,421,837Total Expenditures (1,788,086)Total Revenues & Transfers less Expenditures (366,249) (366,249)AY19 Cash Balance after the Fiscal Month Closed 4,428,681
Budgeted Revenues not yet received (zero) less Estimated Transfers to OHA-PMP & Workforce Data program to be made ($349,545) 0Budgeted Expenditures not yet spent (5,864,431) AY19 Estimated Cash Balance (1,435,750)Cash Balance Contingency (Months) (4.70) months
% Expended To Date
FEBRUARY 2018 / A1
Compounding > 2018 Compounding Policy Priorities Plan
https://www.fda.gov/...g%20Policy%20Priorities%20Plan-%20Drug%20Information%20Update&utm_medium=email&utm_source=Eloqua[1/19/2018 12:31:35 PM]
Home Drugs Guidance, Compliance & Regulatory Information Compounding
2018 Compounding Policy Priorities Plan
I am pleased to share the FDA’s 2018 Compounding Policy Priorities Plan. This planprovides an overview of the key priorities our agency will pursue to implement thefederal law on compounding and to advance the FDA’s public health mission. As weundertake these steps, we must continue to recognize the importance ofcompounders’ role in providing quality drugs so that patients have access to themedicines they need. We will clarify and appropriately tailor the policies for traditionalcompounding pharmacies and the outsourcing facilities that may supply a broadermarket.
Most of these priorities are well underway. Several draft and final guidances outlinedin this plan were announced today. Others parts of this plan will be rolled out over thecourse of the coming year. We plan for all of the commitments made under this planto be completed in 2018.
BackgroundA key aspect of the FDA’s mission is to ensure that medicines for patients are madeaccording to appropriate quality standards. Five years ago, Congress, the FDA, stateregulators and health care practitioners across the country grappled with the largesthealth care-related outbreak in recent history.
The 2012 outbreak of fungal meningitis, resulting from a pharmacy that shippedcontaminated compounded drugs throughout the country, led to more than 750 casesof illness and 60 deaths in 20 states. The tragic proportions of this outbreak weremainly attributable to the company’s large-scale, multistate distribution of an injectabledrug intended to be sterile that had been prepared under inappropriate conditions.This outbreak, combined with the FDA’s continued concerns based on monitoringpharmacy compounding, underscored the need for improvement in compoundingpractices. It also highlighted the need for more robust oversight of compounders,close federal and state collaboration and a clear legal framework that would providefor compounding to meet patients’ medical needs, while also providing the FDA withtools to address unlawful practices that threaten public health.
Further, it became apparent that it was necessary to better define and separate the
SHARE TWEET LINKEDIN PIN IT EMAIL PRINT
FEBRUARY 2018 - B

Compounding > 2018 Compounding Policy Priorities Plan
https://www.fda.gov/...g%20Policy%20Priorities%20Plan-%20Drug%20Information%20Update&utm_medium=email&utm_source=Eloqua[1/19/2018 12:31:35 PM]
legitimate practice of pharmacy compounding from a growing number of enterprisesthat were acting as large-scale drug manufacturers seeking to operate outside of thepurview of FDA oversight by operating under the guise of a pharmacy license. Theseoutfits often created substantial risk in the process by manufacturing and shippinglarge quantities of purportedly sterile drugs and not adhering to good manufacturingpractices.
Congress addressed these challenges and affirmed the FDA’s role in applying itsmission to compounded drugs by passing the Drug Quality and Security Act (DQSA)in November 2013.
Of particular note, DQSA created a new category of compounders, called outsourcingfacilities, which may engage in larger-scale, nationwide distribution with associatedhigher risks. DQSA sets forth a framework for pharmacy compounders andoutsourcing facilities to compound drugs for patients when FDA-approved drugs arenot available to meet patients’ clinical needs. The law sought to balance the importantrole for the practice of pharmacy compounding with the need to promote the quality ofcompounded products, which pose greater risks to patients because they have notundergone premarket review for safety, efficacy and certain manufacturing controls.
Because of the profound public health implications, the FDA’s compounding programis a priority for the agency and the FDA is committed to implementing the DQSAframework. During the last four years, we have made great strides in DQSAimplementation through significant policy development, robust inspection andenforcement actions and strong collaboration with state regulators. We also havecommunicated actively with key stakeholders, allowing us to obtain important inputand advice on scientific, technical and medical issues concerning drug compoundingand related activities.
Our 2018 compounding policy priorities plan lays out how the agency will implementcertain key provisions of DQSA and other provisions of the law relevant tocompounders over the course of the coming year. Our policy will be part of a series ofdraft and final guidance documents, proposed and final rules and a revised draftmemorandum of understanding (MOU) between the FDA and the states.
Specifically, this plan lays out how we will address quality standards for outsourcingfacilities; regulate compounding from bulk drug substances; restrict compounding ofdrugs that are essentially copies of FDA-approved drugs; solidify the FDA’spartnership with state regulatory authorities; and provide guidance on other activitiesthat compounders undertake. We know that to fulfill our public health mission, weneed to keep in mind the critical role that compounding has played in meeting patientneeds and that we must work with the compounding community to continue todevelop an appropriately balanced approach to regulation. As part of our plan, we willcontinue to help protect patients from harm by taking a strong, proactive approachtoward enforcement and ensuring compliance with the law.
FEBRUARY 2018 - B

Compounding > 2018 Compounding Policy Priorities Plan
https://www.fda.gov/...g%20Policy%20Priorities%20Plan-%20Drug%20Information%20Update&utm_medium=email&utm_source=Eloqua[1/19/2018 12:31:35 PM]
2018 COMPOUNDING POLICY PRIORITIESAs we meet our obligations under DQSA, we will balance the need to preserve accessto appropriately compounded drugs for patients who have a medical need for theseproducts with the need to help protect patients from poor quality compounded drugsthat could cause harm. At the same time, we’ll continue to take steps to preserve thenew drug approval requirements that obligate sponsors to demonstrate that drugs aresafe and effective for their intended purpose before they can be lawfully marketed.
Risk-Based Approach to Manufacturing Standards forOutsourcing FacilitiesAs amended by DQSA, the Federal Food, Drug and Cosmetic Act (FD&C Act)provides two pathways for lawful compounding under the Act. Under one pathway, insection 503A, state-licensed pharmacies, among others, compound drugs pursuant topatient-specific prescriptions (referred to as “503A facilities” or as “traditionalcompounders”). Under the other pathway, in section 503B, drugs are compounded bya new category of compounders called outsourcing facilities (or “503B facilities”)according to heightened statutory requirements relative to the 503A facilities.
For example, drugs produced by outsourcing facilities must be compounded incompliance with current good manufacturing practice (CGMP) requirements and in anFDA-registered facility that is subject to regular, risk-based inspections. Informationon the products compounded at outsourcing facilities, including the source of theactive ingredients used, must be reported to the FDA.
Other conditions also must be met under section 503B, including reporting adverseevents and labeling products with certain information. Outsourcing facilities that meetthese conditions may compound drugs that are not necessarily in response to patient-specific prescriptions, whereas 503A facilities may not.
To further describe the operating parameters for outsourcing facilities, and promotethe ability of compounding pharmacies to efficiently meet the more stringentproduction standards, we plan to take several steps. Our policy goal is to make itmore efficient and lower cost for more compounding pharmacies to voluntarily meetthe higher production standards for 503B outsourcing facilities as a way to promotemore patient access to higher quality compounded medicines.
The FDA plans to issue proposed regulations on CGMP requirements that theseoutsourcing facilities must meet. In the interim, the agency is revising the draftguidance to describe a new flexible, risk-based approach to CGMP requirements foroutsourcing facilities. The policies described in the revised draft guidance will considerhow CGMP requirements should be applied in light of the size and scope of anoutsourcing facility’s operations. We anticipate that in response to these new, moreflexible policies, certain smaller compounders that compound limited volumes of
FEBRUARY 2018 - B
Compounding > 2018 Compounding Policy Priorities Plan
https://www.fda.gov/...g%20Policy%20Priorities%20Plan-%20Drug%20Information%20Update&utm_medium=email&utm_source=Eloqua[1/19/2018 12:31:35 PM]
drugs, and presumably present lower risks, may decide to register as outsourcingfacilities, which will allow them to compound drugs with or without patient-specificprescriptions under section 503B. Our goal is for more compounders to register asoutsourcing facilities with the understanding that they can still meet the FDA’s corerequirements for drug quality, based on the size and scope of their compoundingoperations.
Like the 2014 draft guidance, our revised draft guidance also will describe thecircumstances under which the FDA generally does not intend to enforce againstoutsourcing facilities certain CGMP requirements applicable to conventional drugmanufacturers. Based on the comments we received to the FDA’s 2014 draftguidance, the new draft revised guidance will address standards critical to producinga high-quality product, while balancing appropriate flexibility. We believe that theseadditional steps will make it more feasible for smaller compounders to register andcompound drugs as outsourcing facilities.
Ultimately, the goal is to increase patient access to medically necessary compoundeddrugs from outsourcing facilities, which are subject to higher quality standards andoversight than 503A facilities.
Restricting Compounding of Drugs that are EssentiallyCopies of FDA-Approved DrugsA critical component of the FD&C Act is its restrictions on compounding drugs that areessentially copies of FDA-approved or commercially available products. Today, theFDA has issued two final guidance documents regarding the copies provisions for503A and 503B facilities, respectively.
These provisions of the law are an important mechanism to protect both public healthand the premarket approval process. These restrictions are intended to ensure thatdrugs are not compounded for patients who could use an available, FDA-approvedproduct. Even when drugs are compounded in accordance with section 503A or 503Bof the FD&C Act, they have not undergone FDA premarket review for safety,effectiveness and quality. They also lack a premarket inspection and finding ofmanufacturing quality that is part of the drug approval process. Because they aresubject to a lower regulatory standard, compounded drugs should only be distributedto meet the needs of patients whose medical needs cannot be met by an FDA-approved drug. This principle was a key feature of the DQSA passed by Congress.
The restrictions on compounding drugs that are essentially copies of approved drugsalso protect the incentives for conventional drug manufacturers to pursue researchand to develop FDA-approved drugs. Sponsors would be less likely to invest in andseek approval of innovative, life-saving medications if compounders could, after adrug is approved, compound “substitutes” that may be less expensive because theyhave not gone through the premarket approval process. Sponsors also would be less
FEBRUARY 2018 - B

Compounding > 2018 Compounding Policy Priorities Plan
https://www.fda.gov/...g%20Policy%20Priorities%20Plan-%20Drug%20Information%20Update&utm_medium=email&utm_source=Eloqua[1/19/2018 12:31:35 PM]
likely to seek approval of an ANDA for a generic drug if outsourcing facilities werepermitted to compound drugs that were essentially copies of approved drugs withoutgoing through the ANDA process.
Our policies regarding these provisions carefully balance preserving access tocompounded drugs for patients who need them, while preventing compounders fromundermining the drug approval process or unnecessarily exposing patients to risksassociated with unapproved drugs. This is the careful balance that Congress soughtin enacting DQSA and first creating this modern framework. In implementing thesepolicies, we have taken into consideration the concerns from various stakeholders.
As we move toward implementation and enforcement, we intend to focus our initialefforts on education and outreach to practitioners, including prescribers ofcompounded drugs who can determine whether there is a change between thecompounded drug and the commercially available drug, or comparable approveddrug, that produces a significant or clinical difference for an individual patient.
We also intend to prioritize review of situations that could adversely impact the publichealth and premarket approval process, such as compounding using a bulk drugsubstance to produce a product that can otherwise be made by diluting an FDA-approved drug according to its labeled instructions.
Our goal will be to make sure that patients do not receive compounded drugsunnecessarily when an FDA-approved drug is appropriate to meet their medicalneeds.
Regulating Compounding from Bulk Drug Substances503A facilities may compound drugs in accordance with the FD&C Act using bulk drugsubstances that comply with existing United States Pharmacopeia (USP) or NationalFormulary monograph standards; are components of FDA-approved drugs; or appearon a list developed by the FDA through regulation, after consultation with USP andthe Pharmacy Compounding Advisory Committee (the 503A bulks list). 503Boutsourcing facilities may use a bulk drug substance to compound a drug thatcomplies with the FD&C Act if the FDA has determined there is clinical need tocompound with the substance and places it on the 503B bulks list, or if the drugcompounded appears on the FDA’s drug shortage list.
As an interim step, the agency issued interim policy guidances to addresscompounding from bulk drug substances by 503A and 503B facilities while we aredeveloping the bulks lists. These temporary policies were designed to address theuncertainty concerning compounding from bulk drug substances that may be used incompounding by 503A and 503B facilities during the interim period in which theagency evaluates bulk drug substances nominated for use in compounding.
The FDA believed this temporary approach was in the best interest of the public
FEBRUARY 2018 - B

Compounding > 2018 Compounding Policy Priorities Plan
https://www.fda.gov/...g%20Policy%20Priorities%20Plan-%20Drug%20Information%20Update&utm_medium=email&utm_source=Eloqua[1/19/2018 12:31:35 PM]
health, because it would not prevent outsourcing facilities from compounding with bulkdrug substances while the 503B bulks list was being developed. The FDA wasconcerned that an alternative, interim policy approach would have left allcompounding from bulk drug substances to facilities operating under section 503A,which, unlike outsourcing facilities, may compound drugs that are exempt from CGMPrequirements, generally do not report adverse events and generally are not subject torisk-based FDA inspection.
The FDA cautions, however, that the exercise of enforcement discretion during thistime period for a certain nominated substance consistent with the 503A or 503Binterim policies does not reflect a determination that the substance belongs on the503A or 503B bulks lists or that there is a clinical need under section 503B tocompound with the bulk drug substance.
Regarding development of the 503A bulks list, the agency solicited nominations forbulk drug substances to include on the 503A bulks list and presented 48 substancesthat were nominated to the Pharmacy Compounding Advisory Committee for its input.In December 2016, the agency issued proposed regulations to address 10 of thesesubstances and establish the criteria it will use to evaluate substances for inclusion onthe list. After considering public comments, we intend to issue a final regulation. Wealso will continue our process for evaluating additional bulk drug substances that havebeen nominated and addressing those substances in proposed regulations.
Regarding development of the 503B bulks list, the agency solicited nominations forbulk drug substances for inclusion on the 503B bulks list. The next step is for the FDAto issue, in March 2018, a draft guidance document that proposes criteria for makingclinical need determinations for purposes of establishing the 503B bulks list. Theagency has heard concerns about compounding from bulk drug substances when thedrug can be compounded from FDA-approved drugs. The FDA intends to addressthese concerns in its draft guidance document, and it will carefully consider anyadditional concerns that may be raised during the public comment period for the draftguidance. Health care clinicians and practitioners are especially encouraged to submitcomments on the draft clinical needs guidance, so that we receive their feedback onthe use of compounded drugs in clinical care and the potential impacts on patientsafety.
As the agency develops what we intend to be our policy going forward, we know thatmany competing concerns will be brought to our attention. The FDA’s decisions willbe guided by the conditions set forth in the statute, so that bulk drug substances areplaced on the 503B bulks list only when there is clinical need to compound drugsusing these substances. This protects patient health and the drug approval process,for example, by helping to ensure that outsourcing facilities do not compound using abulk drug substance when an FDA-approved drug can be used to meet patientmedical needs.
FEBRUARY 2018 - B

Compounding > 2018 Compounding Policy Priorities Plan
https://www.fda.gov/...g%20Policy%20Priorities%20Plan-%20Drug%20Information%20Update&utm_medium=email&utm_source=Eloqua[1/19/2018 12:31:35 PM]
Solidifying FDA’s Partnership with State RegulatoryAuthoritiesTo address risks presented by compounded drugs, the FDA is working closely withour state partners on oversight of compounding activities. Our objective is to focusFDA resources on outsourcing facilities and on 503A facilities that present thegreatest risks. At the same time, the FDA intends to clarify circumstances in which theagency will look primarily to state partners to oversee certain compounding operationsfor example because the compounded drugs are being distributed intrastate inresponse to prescriptions for named patients and fall within what’s commonly viewedas the practice of pharmacy.
Strong partnerships with our state and other public health partners are an essentialaspect of our efforts to implement DQSA. Last September, the FDA hosted an annualintergovernmental meeting with the state boards of pharmacy, and in the upcomingmonths we plan to issue a significantly revised draft MOU between the FDA and thestates regarding compounding under section 503A. We received more than 3,000comments as well as considerable congressional interest in response to the previousdraft MOU. The draft MOU will be substantially revised to address many of theconcerns we heard.
The draft MOU addresses the percentage of compounded drugs that could beshipped interstate by 503A compounders and state investigation of complaints. Underthe draft MOU, if a pharmacy distributes an “inordinate amount” of compounded drugproduct interstate, the state would agree to take action. FDA had defined “inordinateamount” for states that have entered into the MOU as “an amount of compoundeddrug product distributed interstate in a given month that is equal or greater to 30percent of all drug products dispensed or distributed by the pharmacist, pharmacy, orphysician.”
Among some of the provisions of the revised draft MOU, the FDA will clarify that acompounder has distributed an inordinate amount of drug interstate if the number ofprescriptions of compounded drugs distributed interstate during any calendar month isgreater than 50 percent. Instead of serving as a hard limit for state action, the 50percent would instead trigger certain reporting requirements. The new MOU alsowould make it more feasible for states to enter into the MOU by providing more timeto report to the FDA and greater flexibility in the mechanisms states use to identifyinordinate amounts instead of just relying upon inspection records. Under thisapproach, states will be able to further pursue a risk-based approach, and focus onnotifying the FDA of those compounders where the size or scope of the activitiesmerits greater oversight. Our aim is to leave the oversight of traditional pharmacy tostates.
The FDA appreciates the critical role that pharmacies play in the U.S. health caresystem, and we recognize the need to preserve access to compounded drugs for
FEBRUARY 2018 - B
Compounding > 2018 Compounding Policy Priorities Plan
https://www.fda.gov/...g%20Policy%20Priorities%20Plan-%20Drug%20Information%20Update&utm_medium=email&utm_source=Eloqua[1/19/2018 12:31:35 PM]
patients who have a medical need for them. We believe that the significantly revisedMOU will provide states with additional flexibilities without compromising our sharedpublic health goals.
Once revised and issued in final form, the MOU will serve as an important mechanismfor the FDA and the states to come to a mutual understanding about what types ofactivities are primarily overseen at the state versus federal level, and will help ensurerobust communication between the FDA and its state partners. Our underlying goal ofthe MOU is to make sure that, with respect to 503A facilities, we focus our inspectionand enforcement resources on activities that present the greatest risk to patientsacross many states, while primarily leaving to our state partners routine oversight ofthose activities that mainly affect patients within their own borders, as well asoversight of compounders that distribute a limited percentage of products interstate,pursuant to valid prescriptions for identified individual patients.
Finalization of Biological Products Guidance and ClarifyingOther Policies on Activities that Compounders UndertakeToday, the FDA finalized its guidance, Mixing, Diluting, or Repackaging BiologicalProducts Outside the Scope of an Approved Biologics License Application. This finalguidance is a good example of how the FDA is developing policies to reflect thefeedback we have received for balancing patient access and public health objectives.In this case, the final guidance describes a mechanism for outsourcing facilities toassign beyond use dates (BUDs) to repackaged biological products that exceed the“default” BUDs of 24 hours, based on data. We heard the concerns about theconsequences of adopting a policy with specific caps on BUDs for these productswithout a means to extend the BUDs.
To address these concerns, we are putting forward a more flexible, science and data-driven policy approach to support patients and their clinicians, while also protectingpublic health.
As part of our efforts, in the upcoming months, we will further clarify policiesapplicable to compounding by outsourcing facilities with a guidance on the “definitionof a facility” in section 503B. This guidance will address the question of whether anoutsourcing facility can be co-located with a 503A pharmacy, and whether anoutsourcing facility also can manufacture FDA-approved drugs within the samefacility. This guidance will address concerns raised by some stakeholders about whendifferently situated products were manufactured in the same or nearby facility, and willdefine more clearly when products intended to be produced under 503A would not bescoped into 503B and a more stringent framework just because they weremanufactured near an outsourcing facility. Similarly, the FDA soon will issue finalguidance on compounding and repackaging of radiopharmaceuticals by state-licensednuclear pharmacies, federal facilities and certain other entities, as well ascompounding and repackaging of radiopharmaceuticals by outsourcing facilities.
FEBRUARY 2018 - B

Compounding > 2018 Compounding Policy Priorities Plan
https://www.fda.gov/...g%20Policy%20Priorities%20Plan-%20Drug%20Information%20Update&utm_medium=email&utm_source=Eloqua[1/19/2018 12:31:35 PM]
These guidance documents will be followed by revised draft guidance describingexamples of conditions that the FDA considers to be insanitary and in violation of theFD&C Act. This guidance will address concerns raised by some providers whocompound small quantities of drugs in their offices for patient use, and as part of theirroutine clinical practice. This came up in the setting of certain dermatologicalprocedures, for example. The FDA plans to better define the circumstances underwhich we believe drugs are being mixed and applied in a manner that createsnegligible patient risk, and therefore wouldn’t be subject to the same compliancepolicy under the agency’s risk-based approach to implementing these requirements.
We also intend to issue a final rule regarding the additions and modifications to the listof drug products that cannot be compounded because the products or theircomponents have been withdrawn or removed from the market for reasons of safetyor effectiveness. The FDA previously issued a final rule with other additions andmodifications to that list in October 2016.
ComplianceMonitoring compliance with the law and taking enforcement action when needed willremain a cornerstone of the FDA’s oversight role because of the ongoing and seriousrisks poorly compounded drugs can pose. Examples of risks include contamination ofdrugs that need to be sterile because they are entering the bloodstream, as well asdrugs that are super-potent and therefore can cause harm. These risks are apparentand are underscored by recent compounding risk alerts that the FDA issued to informthe public of serious concerns with specific compounded products.
Since enactment of the DQSA, the FDA has conducted nearly 500 inspections, issuedmore than 180 warning letters advising compounders of significant violations offederal law, issued more than 70 letters referring inspectional findings to stateregulatory agencies, overseen more than 150 recalls involving compounded drugsand worked with the Department of Justice on multiple civil and criminal enforcementactions.
We recognize the public health imperative to quickly and fully implement federalcompounding law and to clearly and proactively communicate our progress inimplementing this critical public health law. Our policies will aim to foster thecontinued development of reliable compounding by traditional compoundingpharmacies and outsourcing facilities, so that patients have access to qualitycompounded drugs when they need them. I look forward to soon sharing moreregarding how we will continue to build on our efforts to fully implement the provisionsof DQSA and employ strong oversight of compounding as part of our public healthmission.
Scott Gottlieb, M.D.FDA Commissioner
FEBRUARY 2018 - B
DIVISION 045 COMPOUNDING
855-045-05001 COMPOUNDING 2
Purpose 3 4
(1) These rules apply to any person, including any business entity that engages in the5 practice of compounding drugs, or any person, including any business entity, located in any 6 other state that compounds drugs for the use of patients located in Oregon. Any person 7 located outside Oregon that compounds drugs for the use of patients located in Oregon is 8 expected to follow the compounding rules of their home state or these rules, whichever are 9 more stringent. 10
11 (2) These rules apply to sterile and non-sterile compounding of medications that are12 prepared for a specific patient or practitioner and that are prescribed or ordered subject to 13 a valid patient-practitioner relationship. 14
15 (3) All drug compounding must adhere to guidelines of the current edition of the United16 States Pharmacopeia Chapters 795 (USP <795>) and 797 (USP <797>), as well as all 17 applicable Chapters of USP and USP-NF related to the compounding practices at any 18 location. This includes but is not limited to Chapters 7, 71, 85, 151, 659, 731, 823, 1072, 19 1116, 1160, 1163, 1211, and 1229.5. 20
21 (4) Compounding pharmacies and personnel must follow applicable federal and state22 regulations regarding hazardous drug products. 23
24 Stat. Auth.: ORS 689.205 25 Stats Implemented: ORS 689.155 26
27 28
855-045-051029 30
General Definitions 31 32
REVIEW ONCE RULES ARE EDITED. THIS SECTION IS FOR GENERAL 33 COMPOUNDING TERMS THAT NEED TO BE DEFINED. 34
35 • APIs36 • Bulk37 • Aliquot38 • ???39
40 (1) “Batch” means any specific quantity greater than one of a drug or other material that is41 intended to have uniform character and quality, within specified limits, and is produced 42 during a single preparation cycle. 43
Commented [KF*B1]: Remove or restate?
FEBRUARY 2018 / B1

2
U Drive: Rules2018/Phase I/Division 45 Compounding January 2018
(2) “Batch preparation compounding” means compounding of batch preparation units, in a 44 single discrete process, by the same individual(s), carried out during one limited time 45 period. 46
(3) “Beyond-Use Date” and “BUD” means the date or time after which a compounded 47 product shall not be used (or stored or transported). The date is determined from the date 48 or time the preparation is compounded. 49
(4) “Hazardous Drug” means any drug identified as hazardous by the National Institute for 50 Occupational Safety and Health (NIOSH) at the Centers for Disease Control or any drug 51 that meets at least one of following six criteria. 52 (a) Carcinogenicity. 53 (b) Teratogenicity or developmental toxicity. 54 (c) Reproductive toxicity in humans. 55 (d) Organ toxicity at low doses in humans or animals. 56 (e) Genotoxicity. 57 (f) New drugs that mimic existing hazardous drugs in structure or toxicity. 58 59
Stat. Auth.: ORS 689.205 60 Stats Implemented: ORS 689.155 61 62 63 855-045-0520 64 65 Registration 66 67 (1) A compounding pharmacy dispensing patient specific drugs must register as an Oregon 68 Retail Pharmacy (RP) or Institutional Pharmacy (IP). This applies to resident and non-69 resident pharmacies. 70 71 (2) A non-resident facility distributing non-patient specific drugs into Oregon must be 72 registered with the Federal Drug Administration as a 503B Outsourcing Facility and 73 register as an Oregon Manufacturer, Category II. 74 75 (3) A resident facility distributing non-patient specific drugs outside of Oregon must 76 register with the Federal Drug Administration as a 503B Outsourcing Facility and register 77 as an Oregon Manufacturer, Category II. 78 79 (4) In addition to obtaining an Oregon pharmacy drug outlet license, all compounding 80 pharmacies shall either pass an inspection by a Board approved entity or shall receive 81 accreditation by a Board approved entity, every 3 years at a minimum, in order to 82 distribute or dispense compounded preparations into and within Oregon. 83 84
Commented [FK2]: See:
Compounding Certification Option
FEBRUARY 2018 / B1
3
U Drive: Rules2018/Phase I/Division 45 Compounding January 2018
Stat. Auth.: ORS 689.205 85 Stats Implemented: ORS 689.155 86 87 88 855-045-0530 89 90 General Requirements for Compounding 91 92 (1) All active pharmaceutical ingredients must be obtained from an FDA registered 93 manufacturer. 94
(2) Unless the active pharmaceutical ingredient complies with the standards of an 95 applicable USP-NF monograph, a Certificate of Analysis (COA) must be obtained for all 96 active pharmaceutical ingredients procured for compounding and retained for a period of 97 not less than three years from the date the container is emptied, expired, returned, or 98 disposed of. The following minimum information is required on the COA: 99
(a) Product name; 100
(b) Lot number; 101
(c) Expiration date; and 102
(d) Assay. 103
(3) The equipment, components, devices, and utensils used for compounding of a drug 104 preparation must be of appropriate design and capacity and shall also be designed to 105 protect the compounder from hazardous materials. Minimum standards for pharmacies 106 and equipment are dependent on the risk level of the products being prepared. A 107 pharmacy must comply with all applicable USP standards commensurate with level of 108 compounding being performed. 109 110 (a) Equipment must be of suitable composition that the surfaces which contact components 111 are neither reactive or alter the purity of the compounded preparations. 112 113 (b) Equipment must be stored to protect it from contamination and must be located to 114 facilitate its use, maintenance and cleaning. 115 116 (c) Automated, mechanical, electronic and other types of equipment must be routinely 117 inspected and calibrated as necessary, per manufacturer’s specifications. 118 119 ADD?? A general statement related to the safe environment for compounding. 120
(4) The accuracy of identities, concentrations, amounts, and purities of ingredients in 121 compounded products shall be confirmed by reviewing labels on packages, observing and 122 documenting correct measurements with approved and correctly standardized devices, and 123 reviewing information in labeling and certificates of analysis provided by suppliers. 124 125
Commented [FK3]: Use other words, such as drugs, components, raw materials, etc???
FEBRUARY 2018 / B1

4
U Drive: Rules2018/Phase I/Division 45 Compounding January 2018
(a) If the correct identity, purity, strength and sterility of ingredients and components of 126 compounded products cannot be confirmed, such ingredients and components shall be 127 discarded immediately. 128 129 (b) Individual ingredients such as bulk drug substances that are not labeled with expiration 130 dates shall require testing to determine the correct amount to weigh for accurate content of 131 active ingredients. Components that do not have expiration dates assigned by the 132 manufacturer or supplier, shall be labeled on the container with the date of receipt and 133 shall be assigned an expiration date not to exceed three years after receipt of the 134 component. 135 136
(5) Any compounding activity that is not pursuant to a valid prescription or an order to 137 prepare for administration and for a specific patient is considered to be manufacturing, 138 and any person engaged in manufacturing must be registered in accordance with OAR 139 855-060-0001, with the following exceptions: 140 141 (a) Compounding in anticipation of a prescription drug order or an order to prepare for 142 administration, based on a history of receiving valid prescription drug orders for the 143 compounded or sterile prepackaged drug product; or 144
(b) Compounding non-controlled substances by a pharmacy located in Oregon for a 145 practitioner or dispenser located in Oregon that is covered by an Oregon Board approved 146 Shared Pharmacy Services agreement as defined in Division 006. Doing business within 147 Oregon, documented by use of Shared Pharmacy Services agreements exempts an Oregon 148 compounding pharmacy from additionally registering as an Oregon Manufacturer. 149 150 (6) A drug product that is commercially available may only be compounded if not 151 compounded regularly or in inordinate amounts and if: 152
(a) It is medically warranted to provide an alternate ingredient, dosage form, or strength of 153 significance; or 154
(b) The commercial product is not reasonably available in the market in time to meet the 155 patient’s needs. 156
(c) Justification of compounding in this manner shall be documented and retained by the 157 pharmacy for a minimum of three years and be made available. 158
(7) Compounding any drug product for human use that the FDA has been identified as 159 presenting demonstrable difficulties in compounding or has withdrawn or removed from 160 the market for safety or efficacy reasons is prohibited. 161
162 Stat. Auth.: ORS 689.205 163 Stats Implemented: ORS 689.155 164 165 855-045-0540 166
Commented [FK4]: Current is 5?
Commented [KF*B5]: Remove or re-write?
FEBRUARY 2018 / B1
5
U Drive: Rules2018/Phase I/Division 45 Compounding January 2018
167 Compounding Personnel and Responsibilities 168 169 (1) All personnel who prepare compounded pharmaceuticals shall be provided with 170 appropriate training before they begin to prepare such products, including theoretical 171 principles and practical skills of manipulations. A person licensed to practice pharmacy by 172 the Oregon Board of Pharmacy who is working in a compounding pharmacy, including a 173 pharmacy that only prepares sterile parenteral products, has the duty to exercise that 174 degree of care, skill, diligence and professional judgment that is used by ordinarily 175 competent, careful pharmacists in the same or similar circumstances. 176 177 (2) All compounding personnel shall possess the education, training and competency 178 necessary to properly and safely perform compounding duties undertaken or supervised. 179 180 (3) The pharmacist in charge (PIC) shall establish pharmacy’s standard operating 181 procedures and processes in accordance with the guidelines of current USP Chapters, as 182 applicable, for all compounding related activities of the pharmacy. 183 184 (4) A pharmacist who engages in compounding shall: 185
(a) Follow all relevant laws and rules; 186
(b) Perform documented review and verification of each step of the compounding process; 187
(c) Provide written information about the compounded preparation’s active ingredient(s) 188 to the patient at the time of dispensing. If there is no written information available, the 189 patient shall be advised that the drug had been compounded and how to contact a 190 pharmacist, and if appropriate, the prescriber, concerning the medication; and 191
(d) Compound batch sizes that the pharmacist has determined are of an appropriate size to 192 maintain patient safety. 193
Stat. Auth.: ORS 689.205 194 Stats Implemented: ORS 689.155 195 196 OAR 855-045-0550 197 198 Labeling 199 200 (1) In addition to the labeling requirements as specified in Division 41, the label dispensed 201 or distributed pursuant to a compounded prescription drug or medication order shall 202 contain the following, at a minimum: 203 204 (a) The generic name(s) or the official name(s) of the active ingredient(s) of the product; 205 206 (A) The name of each drug included; 207
Commented [KF*B6]: Who is responsible for establishing P&P and assuring compliance …. Is it PIC, outlet, both? Once determined, be sure this is consistent throughout.
FEBRUARY 2018 / B1
6
U Drive: Rules2018/Phase I/Division 45 Compounding January 2018
(B) The strength or concentration of each drug included. 208
(C) The name and concentration of the base or diluents, if applicable. 209
(D) The dosage form or route of administration. 210
(E) The total quantity of the drug product. 211
(F) The expiration or beyond use date. 212
(G) Handling, storage or drug specific instructions, cautionary information, and warnings 213 as necessary or appropriate for proper use and patient safety. 214
(b) A statement that the product has been compounded by the pharmacy. (An auxiliary 215 label may be used on the container to meet this requirement); and 216 217 (c) An appropriate beyond-use-date (BUD). 218 219 Stat. Auth.: ORS 689.205 220 Stats Implemented: ORS 689.155 221 222 OAR 855-045-0560 223 Hazardous Drugs 224 225 Compounding pharmacies and personnel must follow all applicable federal and state 226 regulations regarding hazardous drugs. 227 228 Stat. Auth.: ORS 689.205 229 Stats Implemented: ORS 689.155 230 231 232 855-045-0570 233 Quality Controls for Compounding 234 235 (1) The pharmacist-in-charge shall develop and the pharmacy shall follow quality control 236 procedures to monitor the compounding environment and quality of compounded drug 237 preparations for conformity with the quality indicators established for the preparation. 238 239 (2) The pharmacist-in-charge shall consider the provisions of all applicable USP chapters 240 for development and ongoing adherence to quality control procedures. Such procedures 241 shall be documented and be available for inspection. 242 243 (3) The pharmacist-in-charge shall establish an adverse event reporting process. Any 244 adverse event shall be reported by the pharmacist-in-charge to MedWatch: The United 245 States Food and Drug Administration Safety Information and Adverse Event Reporting 246 Program within forty-eight (48) hours of becoming aware of the adverse event. A copy of 247 each reported adverse event shall be made available during an inspection. 248 249
Commented [FK7]: Include aqueous BUDs, etc here??
Commented [KF*B8]: Retain, remove or re-write?
Commented [FK9]: Or does the Board want all MedWatch reports submitted to also be proactively submitted to OBOP as well?
FEBRUARY 2018 / B1

7
U Drive: Rules2018/Phase I/Division 45 Compounding January 2018
Stat. Auth.: ORS 689.205 250 Stats Implemented: ORS 689.155 251 252 855-045-0580 253 254 Records 255 256 (1) All compounding records, including training documents, master formula worksheets, 257 individual batch worksheets and individual prescription records, shall be maintained 258 electronically or manually, stored in an organized manner, retained for a minimum of 259 three years and be made readily available for inspection by the Board. 260 261 (2) The pharmacy shall maintain a training record on each person, including temporary 262 personnel, who compound preparations. At a minimum, the record shall contain: 263 264 (a) Documentation of initial and continuing competency, training, and education; and 265 266 (b) Name and signature of the PIC or other pharmacist employed by the pharmacy who is 267 designated as responsible for validating the completion of all training. 268 269 (3) The pharmacy shall maintain an organized index of master formulas for all 270 compounded products. 271 272 (4) Records for compounding shall utilize a master formula worksheet. All master formula 273 worksheets shall be developed and approved by the PIC for preparations in each batch, 274 and shall contain, at a minimum: 275 276 (a) A complete formula, including methodology and necessary equipment; 277 278 (b) The name and strength/concentration of all drugs, components or raw materials, both 279 active and inactive; 280 281 (c) The quantities of all drugs, components or raw materials, both active and inactive; 282 283 (d) Specific, step-by-step compounding/mixing instructions and double check sign-off steps, 284 where appropriate; 285 286 (e) Beyond-use-dating; 287 288 (f) Device or equipment-specific instructions, where appropriate; 289 290 (g) Batch size; 291 292 (h) Containers and closures used; 293 294 (i) Evaluation and testing requirements; 295
Commented [KF*B10]: Maybe technician? If so, change to licensee, or add technician
Commented [FK11]: Are these the correct terms? Or use “ingredients”?
FEBRUARY 2018 / B1

8
U Drive: Rules2018/Phase I/Division 45 Compounding January 2018
296 (j) Appropriate ancillary instructions, such as storage instructions or cautionary 297 statements, including hazardous drug warning labels where appropriate; 298 299 (k) A reference to the location of related documentation, which may be maintained with 300 other records, including, but not limited to: 301 302 (A) The criteria used to determine the BUD; and 303 304 (B) The documentation of performance of quality control procedures. 305 306 (5) Records for the individual preparation batch worksheets for each batch, must include 307 but not be limited to the following: 308 309 (a) Identity of all drugs, components, or raw materials and their corresponding amounts, 310 concentrations or volumes; 311 312 (b) Lot number and expiration date for each component; 313 314 (c) Component manufacturer/distributor or suitable identifying number; 315 316 (d) Container specification (i.e. syringe, pump, cassette, etc); 317 318 (e) Unique pharmacy lot or control number assigned to batch; 319 320 (f) Beyond use date of batch-prepared preparations; 321 322 (g) Time and date of preparation 323 324 (h) The quantity, in units, of finished products prepared; 325 326 (i) Physical evidence of the proper weight of each drug, component, or raw material used; 327 328 (j) Signature or initials of the pharmacist responsible for supervising pharmacy technicians 329 and conducting in-process and final checks of compounded pharmaceuticals if pharmacy 330 technicians perform the compounding function; 331 332 (k) Names of all technicians involved in the process; 333 334 (l) Finished preparation evaluation and testing specifications, when applicable; and 335 336 (m) Comparison of actual yield to anticipated or theoretical yield, when appropriate. 337 338
Commented [KF*B12]: When applicable? (or is this needed?)
FEBRUARY 2018 / B1
9
U Drive: Rules2018/Phase I/Division 45 Compounding January 2018
STERILE COMPOUNDING 339 340 855-045-0600 341 342 Purpose – Sterile Compounding 343
The requirements of this chapter apply to any person or facility that compounds sterile 344 drug preparations (CSPs). These rules represent minimum sterile compounding practices 345 for the preparation of drug products for dispensing or administering and are intended to 346 help compounding personnel produce compounded sterile preparations of high quality and 347 reduce the potential for harm to patients. It is expected that a pharmacy compounding 348 CSPs will comply with all applicable rules in this division. The minimum standards of the 349 current edition of the United States Pharmacopeia Chapter <797> and all other applicable 350 USP Chapters regarding sterile compounded products shall be met unless requirements 351 listed are more stringent. 352
Stat. Auth.: ORS 689.205 353 Stats Implemented: ORS 689.155 354 355 OAR 855-045-0610 356
Personnel Compounding Sterile Preparations (CSPs) 357 358 (1) These rules are intended to apply to all persons who prepare compounded sterile 359 preparations (CSPs) and all places where CSPs are prepared. 360 361 (2) Compounding personnel are responsible for ensuring that CSPs are accurately 362 identified, measured, diluted, and mixed and are correctly purified, sterilized, packaged, 363 sealed, labeled, stored, administered, dispensed, and distributed. 364 365 (3) Documented training for each person, including temporary personnel shall be 366 performed and completed prior compounding sterile preparations, and must include, at a 367 minimum: 368 369 (a) Fundamentals of sterile compounding manipulations; 370 371 (b) Responsibilities of compounding personnel; 372 373 (c) Purpose and utilization of policies and procedures; 374 375 (d) Use of all applicable equipment and supplies, to include automated compounding 376 devices; 377 378 (e) Facility and personnel environmental sampling metrics, to include but not limited to: 379 380 (A) Garbing competency; 381
Commented [FK13]: Need to DETAIL each and every component of garbing???
FEBRUARY 2018 / B1

10
U Drive: Rules2018/Phase I/Division 45 Compounding January 2018
382 (B) Hand hygiene and proper work practices competency, via gloved fingertip sampling; 383 384 (C) Media-fill testing of aseptic manipulation competency, at least annually for low and 385 medium-risk level compounding and semi-annually for high-risk level compounding; and 386 387 (D) Cleaning and disinfecting competency, to include surface sample testing; 388 389 (f) Understanding of primary and secondary engineering controls, such as function, use, 390 testing, and certification; 391 392 (g) Assignment of BUDs; 393 394 (h) Quality assurance, quality releases and final checks of CSPs; 395 396 (i) Labeling and packaging controls; 397 398 (j) Batch documentation; 399 400 (k) Cleaning and disinfecting of controlled environments; 401 402 (l) Filtration and sterility processes, moist and dry-heat sterilization, bacterial endotoxin 403 (pyrogen) testing; and 404 405 (m) Hazardous drug material handling. 406 407 (4) Personnel who fail any element of subsection (3) must be reinstructed and re-evaluated 408 by trained sterile compounding personnel prior to performing compounding duties. 409 Certification of competencies outlined in subsection (3)(e) shall also be performed 410 whenever: 411 412 (a) Any increase in difficulty or production of a higher risk level CSP is performed; 413 414 (b) The quality assurance 415 416 (c) Unacceptable techniques are observed. 417 418 (5) The Pharmacist-In-Charge (PIC) shall possess the education, training and proficiency 419 necessary to properly and safely perform compounding duties undertaken or supervised. 420 421 (a) The PIC shall not be in charge of more than one licensed compounding pharmacy at a 422 time. The PIC shall be on site at that pharmacy for a minimum of twenty hours per week. 423 424 (b) The PIC is responsible for overall validation of the compounding competency of 425 pharmacists and technicians. The PIC may train and authorize, in writing, assistant 426 personnel who may validate compounding competencies. 427
Commented [FK14]: For discussion
Commented [KF*B15]: Necessary? And see OAR 855-045-0580 – make similar!
FEBRUARY 2018 / B1

11
U Drive: Rules2018/Phase I/Division 45 Compounding January 2018
428 (6) The PIC and pharmacy shall establish and enforce written policies and procedures 429 based on standards set forth in the current Chapters of USP and USP-NF, and are 430 designed to ensure accountability, accuracy, quality, safety and uniformity in the sterile 431 compounding process. They shall include but not be limited to: 432 433 (a) Education, training, and competency evaluation of all regular and temporary 434 personnel; 435 436 (b) Proper hand hygiene and garbing for all CSP compounding; 437 438 (c) Proper maintenance and calibration of primary and secondary engineering controls as 439 well as other areas and equipment used in the compounding process; 440 441 (d) Compounding procedures including but not limited to the use of automated 442 compounding devices and other specific procedures for CSPs; 443 444 (e) CSP compounding methodology and formula information, to include assignment of 445 appropriate risk levels for all CSPs; 446 447 (f) Determination of beyond-use-dates, assigned on the basis of direct testing or 448 extrapolated from reliable sources and other documentation; 449 450 (g) Appropriate sterilization and other preparation checks and release tests of CSPs; 451 452 (h) Verification of compounding accuracy and sterility for CSPs; 453 454 (i) Labeling, to include all names and amounts/concentrations of active ingredients; 455 456 (j) Proper maintenance of environmental quality and control, to include appropriate 457 environmental sampling testing; 458 459 (k) Finished preparation release checks and tests; 460 461 (l) Cleaning and disinfecting the direct and contiguous compounding areas; 462 463 (m) Recall procedures for CSPs; 464 465 (n) Drug disposal, including hazardous waste if applicable. Hazardous waste disposal must 466 comply with all federal and state regulations; 467 468 (o) Procurement, container selection, shipping, delivery and storage of pharmaceutical 469 materials including compounded drug preparations and components used in the 470 compounding of sterile preparations and drug delivery devices; 471 472 (p) Patient care and instructions; 473
Commented [KF*B16]: Responsibilities?
Commented [KF*B17]: Keep this as the consistent language?
Commented [FK18]: Correct words here? (See previous similar comments)
FEBRUARY 2018 / B1
12
U Drive: Rules2018/Phase I/Division 45 Compounding January 2018
474 (q) Bulk compounding, including the development of master formulas and individual batch 475 compounding worksheets; 476 477 (r) Quality assurance and control, to include adverse event reporting per OAR 855-045-478 0570. 479 480 (7) All pharmacists who compound sterile preparations shall: 481 482 (a) Possess the education, training and proficiency as required to properly and safely 483 perform compounding duties undertaken or supervised; 484 485 (b) Successfully complete the required competency training appropriate for the type of 486 compounding performed or supervised; 487 488 (c) Inspect and approve all components, drug preparation containers, closures, labeling, 489 and any other materials involved in the compounding process; 490 491 (d) Review all compounding records for accuracy and conduct in-process and final checks 492 to ensure that errors have not occurred in the compounding process; and 493 494 (e) Ensure proper maintenance, cleanliness, calibration, and use of all equipment used in 495 the compounding process. 496 497 (8) All pharmacy technicians who compound sterile preparations shall: 498 499 (a) Possess the education, training and proficiency as required to properly and safely 500 perform compounding duties undertaken; 501 502 (b) Successfully complete the required competency training appropriate for the type of 503 compounding performed by the pharmacy technician; 504 505 (c) Conduct in-process and completion checks, and maintains appropriate records; and 506 507 (d) Ensure proper maintenance, cleanliness, and use of all equipment used in the 508 compounding process. 509
510
Stat. Auth.: ORS 689.205 511 Stats Implemented: ORS 689.155 512 513 OAR 855-045-0620 514 515 Microbial Contamination Risk Levels and Beyond-Use-Dates 516 517 Risk levels of CSPs recognized by USP <797> are based on the probability of 518 contamination by microbial, chemical or physical agents. Low-Risk and Medium-Risk 519
FEBRUARY 2018 / B1
13
U Drive: Rules2018/Phase I/Division 45 Compounding January 2018
Level CSPs are determined by the potential for microbial contamination during 520 preparation, and High-Risk Level CSPs by the potential for not being properly sterilized 521 before administration to patients. These risk levels, including Immediate-use provisions, 522 are defined, and products must be prepared and managed per current USP standards. 523 524
Stat. Auth.: ORS 689.205 525 Stats Implemented: ORS 689.155 526 527 528
855-045-0630 529
Records 530
(1) In addition to the requirements set forth in 855-045-0580, batch records for all 531 compounded sterile products (CSPs) must include: 532 533 (a) Primary solution; 534 535 (b) Container specification (e.g., syringe, pump cassette); and 536 537 (c) Infusion rate. 538 539 (2) Sterile compounding training documentation shall include: 540 541 (a) Printed name and signature of the person receiving the training; 542 543 (b) Name and signature of the person providing the training or evaluating competencies; 544 and 545 546 (c) Dates and results of all elements found in OAR 955-045-0610(3). 547 548 (3) Records of maintenance and certifications for all equipment, including environmental 549 sampling shall be maintained electronically or manually, stored in an organized manner, 550 retained for a minimum of three years and be made readily available for inspection by the 551 Board. 552 553 (4) Records of cleaning and disinfecting of all compounding areas and equipment shall be 554 maintained electronically or manually, stored in an organized manner, retained for a 555 minimum of three years and be made readily available for inspection by the Board. 556 557 Stat. Auth.: ORS 689.205 558 Stats Implemented: ORS 689.155 559 560
Commented [FK19]: Do we need a Radiopharm statement here??
FEBRUARY 2018 / B1

Oregon Board of Pharmacy Temporary Rule adopted 2/29/2017 Proposed for permanent rulemaking 1.2018
The proposed amendments in OAR 855-019-0460 are provided for the Board’s review for a temp 1 rule. 2
ORS 689.681(4) states “Notwithstanding any other provision of law, a pharmacy, a health care 3 professional with prescription and dispensing privileges or any other person designated by the 4 State Board of Pharmacy by rule may distribute unit-of-use packages of naloxone, and the 5 necessary medical supplies to administer the naloxone. 6
Certain entities are in the position to provide naloxone distribution within their agency. In order 7 to allow this to occur, sub (8) is proposed. 8
Another question: Now that the mandate to provide training is removed, does the Board find it 9 necessary to mandate counseling on all naloxone prescriptions a pharmacist prescribes? See 10 proposed sub (6) edits. 11
12 855-019-046013
Delivery of Care 14
(1) A pharmacist can prescribe naloxone and the necessary medical supplies for opiate overdose15 training. 16
(2) A pharmacist can prescribe naloxone and the necessary medical supplies to an individual or17 entity seeking naloxone. 18
(3) The pharmacist shall determine that the individual (or the individual on behalf of an entity)19 seeking naloxone demonstrates understanding of educational materials related to opioid overdose 20 prevention, recognition, response, and the administration of naloxone. 21
(4) The pharmacist may prescribe naloxone in any FDA approved dosage form and the necessary22 medical supplies needed to administer naloxone. 23
(5) The pharmacist shall dispense the naloxone product in a properly labeled container.24
(5) (6) Naloxone may not be dispensed prescribed without offering to provideing oral25 counseling to the authorized recipient, to which may include dose, effectiveness, adverse effects, 26 storage conditions, and safety. 27
(7) The pharmacist must document the encounter and the prescription, and maintain records for28 three years. 29
(8) Any person, having once lawfully obtained naloxone may possess, distribute or30 administer it for the purpose of reversing opiate overdose. 31
Stat. Auth.: ORS 689.205 32 Stats. Implemented: ORS 689.305, 689.681 & 2016 OL Ch. 100 33
FEBRUARY 2018 /B2
1
Oregon Board of Pharmacy 1.26.18 revised
Edits to Div 041 and Div 019 are proposed to address Retail Drug Outlet (RP)/Community 1 Pharmacy personnel and compliance requirements. 2
These edits (1) Describe requirements for a resident community pharmacy outlet that employs a 3 person who directs the professional activities of PICs, as this is a part of the Practice of 4 Pharmacy (2) Update the PIC rules to clarify the role of a PIC; and (3) Incorporate 5 general/housekeeping edits for the PIC duties and responsibilities. 6
Per ORS 689.005(30)(k) The practice of pharmacy means the offering or performing of those 7 acts, services, operations, or transactions necessary in the conduct, operation, management and 8 control of pharmacy. The practice of pharmacy of Pharmacy in Oregon may only be performed 9 by an Oregon licensed pharmacist. 10
11
12
General Community Pharmacy 13
855-041-2105 Personnel14
(1) Each community pharmacy drug outlet (RP) must have an Oregon licensed pharmacist15 designated as Pharmacist-in-Charge (PIC) who is responsible for the daily operations of 16 the pharmacy. The PIC is responsible for exercising professional judgment and discretion 17 to ensure a pharmacy environment that is safe and effective, and fulfils the responsibilities 18 listed in Div 019. 19
(2) Each resident community pharmacy that employs a person who directs the professional20 activities of multiple PICs shall ensure that: 21
(a) The person is an Oregon licensed pharmacist; and22
(b) When a vacancy occurs, the pharmacy will notify the Board within ten business days,23 and will appoint an Oregon licensed person within 90 days. 24
25
26
Stat. Auth.: ORS 689.205 27 Stats. Implemented: ORS 689.155 28
FEBRUARY 2018 / B3

2
Oregon Board of Pharmacy 1.26.18 revised
Pharmacist-in-Charge 29
855-019-0300 30
Duties of a Pharmacist-in-Charge 31
(1) In accordance with Division 41 of this chapter of rules, a pharmacy must, at all times have 32 one Pharmacist-in-Charge (PIC) employed on a regular basis at that location who is 33 responsible for the daily operation of the pharmacy. 34
(2) In order to be a PIC, a pharmacist must have: 35
(a) Completed at least one year of pharmacy practice; or 36
(b) Completed a Board approved PIC training course either before the appointment or within 30 37 days after the appointment. With the approval of the Board, this course may be employer 38 provided and may qualify for continuing education credit. 39
(3) A pharmacist may not be designated PIC of more than two pharmacies without prior written 40 approval by the Board. If such approval is given, the pharmacist must comply with the 41 requirements in sub-section (4)(e) of this rule. A pharmacist may be designated as a PIC of up 42 to two Oregon licensed pharmacies only upon notification of the second site to the Board in 43 writing within 15 days. 44
(4) The PIC is responsible for must perform the following the duties and responsibilities: 45
exercising professional judgment and discretion to ensure a pharmacy environment that is 46 safe and effective, to include: 47
(a) Assessing pharmacy demand, and workload; 48
(b) Evaluating pharmacy staffing, inventory, resources, and capacity; 49
(c) Prioritizing pharmacy tasks, responsibilities, and assignments; and 50
(d) Modifying pharmacy workflow and services provided. 51
(5) The PIC must perform the following duties and responsibilities: 52
(a) When a change of PIC occurs, both outgoing and incoming PICs must report the change to 53 the Board within 15 days of the occurrence, on a form provided by the Board; 54
(b) The new PIC must complete an inspection on the PIC Annual Self-Inspection Form, within 55 15 days of becoming PIC; 56
(c) The PIC may not authorize non-pharmacist employees to have unsupervised access to the 57 pharmacy, except in the case of hospitals that do not have a 24-hour pharmacy where access may 58 be granted as specified in OAR 855-041-0120--6310; 59
FEBRUARY 2018 / B3

3
Oregon Board of Pharmacy 1.26.18 revised
(d) In a hospital only, the PIC is responsible for providing education and training to the nurse 60 supervisor who has been designated to have access to the pharmacy department in the absence of 61 a pharmacist; 62
(e) A pharmacist designated as PIC for more than one pharmacy shall personally conduct and 63 document a quarterly compliance audit at each location. This audit shall be on the Quarterly PIC 64 Compliance Audit Form provided by the Board; 65
(f) (e) If a discrepancy is noted on a Board inspection, the PIC must submit a plan of correction 66 within 15 days for a Non-Compliance Notification and 30 days of receiving a Deficiency 67 Notification. notice. 68
(g) (f) The records and forms required by this section must be filed in the pharmacy, made 69 available to the Board for inspection upon request, and must be retained for three years. 70
(5) (6) The PIC is responsible for ensuring that the following activities are correctly completed: 71
(a) An inventory of all controlled substances must be taken within 15 days before or after the 72 effective date of change of PIC, and must be dated and signed by the new PIC. This inventory 73 must be maintained in the pharmacy for three years and in accordance with all federal laws and 74 regulations; 75
(b) Verifying, on employment and as appropriate, but not less than annually, the licensure of all 76 pharmacy personnel who are required to be licensed by the Board; 77
(c) Conducting an annual inspection of the pharmacy using the PIC Annual Self-Inspection Form 78 provided by the Board, by February 1 each year. The completed self-inspection forms must be 79 signed and dated by the PIC and maintained for three years from the date of completion; 80
(d) Conducting an annual inventory of all controlled drugs as required by OAR 855-080; 81
(e) Performing a quarterly inventory reconciliation of all Schedule II controlled drugs.; 82
(f) Ensuring that all pharmacy staff have been trained appropriately for the practice site. Such 83 training should include an annual review of the PIC Self-Inspection Report; 84
(g) Implementing a Maintaining the continuous quality assurance plan program for the 85 pharmacy; 86
(h) The records and forms required by this section must be filed in the pharmacy, made available 87 to the Board for inspection upon request, and must be retained for three years. 88
(6) (7) The PIC, along with other licensed pharmacy personnel, must ensure that the pharmacy is 89 in compliance with all state and federal laws and rules governing the practice of pharmacy and 90 that all controlled substance records and inventories are maintained in accordance with all state 91 and federal laws and rules. 92
Stat. Auth.: ORS 689.205 93 Stats. Implemented: ORS 689.151, 689.155 94 95
FEBRUARY 2018 / B3

Subject: Providence Portland Medical Center (PPMC) Technician Checking Validation Program (TCVP) – Year 1 Review
Date: December 14, 2017
Request/Inquiry Type: Policy / Compliance
Background: Providence Portland Medical Center in Portland, Oregon (IP-0000374) implemented TCVP on February 10, 2017 and have submitted their Year 1 Follow-Up Report:
TCVP – Year One Questions 1. When was program implemented?Our first technician completed the program on 2/10/2017. We have a total of 3 technicians whohave completed the training.
2. General comments on the programProgram has allowed pharmacists to focus on medication order verification, clinical review ofappropriateness of medications and doses ordered, thereby enhancing patient safety.
3. Quality Assurance / Did you catch error?We have completed four random, unannounced quality assurance checks (at 1, 2, 3, and 6months) of 100 line items for technicians checking ADC and non-emergent trays and kits andhave found no errors.
4. Did training program and materials work?Yesa. Were any revisions needed for training program/materials?We updated the high risk medication list to include paralytics and anticoagulants. Attached isProvidence Portland list of items that are not eligible for technician checking.
5. Any problems with the rules and any recommended changes?Would recommend reducing the amount of unit dose checks that are required to complete theprogram. 1500 checks requires a lot of additional hours to complete the program. We feel thesame intent could be accomplished with 1000 checks.
6. Suggestions for others considering utilizing TCVP?We believe there is significant benefit in this program for large hospitals to allow pharmacistsmore time for clinical pharmacist activities that contribute to medication safety.
7. Questions to Board of Pharmacy?No questions at this time.
PICs Bali and Buxell also submitted an updated list of High Risk Medications not Eligible for TCVP (see Page 3 of this report).
FEBRUARY 2018 - C

Recommendations: Accept report & have Providence Portland Medical Center Pharmacy report back in February 2022 for 5-year renewal. Contact: Providence Portland Medical Center PIC Sanjeev Bali, PharmD, RPh & Shannon Buxell, PharmD, RPh 4805 NE Glisan St. Portland, OR 97213
FEBRUARY 2018 - C

High Risk Medication List (not eligbile for Tech Checking)Med Description**ONCOLOGY EMERGENCY MED** KIT**STEM CELL REINFUSION EMR MED KIT*ENDO/MPU KIT* KITACI KITADENOSINE 6 MG 2 ML SDVADENOSINE 90 MG 30 ML INJECTIONADRENALIN CHLORIDE-NS 1/100000 100 ML SOLUTIONALBUMIN (HUMAN) 5% 12.5 GM 250 ML INJECTIONALBUMIN 5% 2.5 GM 50 ML SOLUTIONALBUTEROL SULFATE DOSE PACK 8 GM INHALERALTEPLASE RECOMBINANT 100 MG 100 ML INJECTIONALTEPLASE RECOMBINANT 50 MG INJECTIONAMIODARONE 150 MG 3 ML INJECTIONAMIODARONE HCL IN D5W 150 MG 100 ML SOLUTIONAMOXICILLIN SUSP DOSE PACK 250 250 MG 5 ML SUSPENSIONANAGRELIDE HCL 0.5 MG CAPSULEAPIXABAN 2.5 MG TABLETAPIXABAN 5 MG TABLETATROPINE SULFATE 0.4 MG 1 ML INJECTIONATROPINE SULFATE 1 MG 10 ML INJECTIONAZITHROMYCIN IN NS 500 MG 250 ML PREMIX SOLBIVALIRUDIN 250 MG 5 ML INJECTIONCALCIUM CHLORIDE SYRINGE 10% 1 GM 10 ML INJECTIONCALCIUM GLUCONATE 4.65 MEQ 10 ML INJECTIONCALCIUM GLUCONATE IN NS 1 GM 50 ML SOLUTIONCLOPIDOGREL BISULFATE 300 MG TABLETCLOPIDOGREL BISULFATE 75 MG TABLETCycloSPORINE (NEORAL) 25 MG CAPSULE EMCycloSPORINE (SANDIMMUNE) 100 MG CAPSULE EMDABIGATRAN ETEXILATE 150 MG CAPSULEDARBEPOETIN ALFA 200 MCG 0.4 ML SYRINGEDARBEPOETIN ALFA 300 MCG 0.6 ML SYRINGEDARBEPOETIN ALFA 500 MCG 1 ML SYRINGEDENOSUMAB 120 MG 1.7 ML SDVDENOSUMAB 60 MG 1 ML INJECTIONDESFLURANE 240 ML LIQ INHALDEXMEDETOMIDINE HCL IN NACL 200 MCG 50 ML PREMIX SOLDEXTROSE 25% **INFANT** 2.5 GM 10 ML SYRINGEDEXTROSE 50% 25 GM 50 ML VIALDEXTROSE 50% SYRINGE 25 GM 50 ML INJECTIONDIGOXIN 0.5 MG 2 ML INJECTIONDIVALPROEX CAPSULE 125 MG SPRINKLESDIVALPROEX EC Delayed Release 125 MG TABLET DRDIVALPROEX EC Delayed Release 250 MG TABLET DRDIVALPROEX EC Delayed Release 500 MG TABLET DRDIVALPROEX ER 24HR 250 MG TABLET ERDIVALPROEX ER 24HR 500 MG TABLET ERDOBUTamine 250 MG 20 ML INJECTIONDOBUTamine-DEXTROSE 5% 500 MG 250 ML INJECTIONDOPamine IN D5W (1.6MG/ML) 400 MG 250 ML INJECTIONENOXAPARIN 100 MG 1 ML SYRINGEENOXAPARIN 120 MG 0.8 ML SYRINGEENOXAPARIN 30 MG 0.3 ML SYRINGEENOXAPARIN 40 MG 0.4 ML SYRINGEENOXAPARIN 60 MG 0.6 ML SYRINGEENOXAPARIN 80 MG 0.8 ML SYRINGEEPINEPHrine HCL 1 MG 10 ML SYRINGEEPINEPHrine IM/SQ 1 MG 1 ML INJECTIONEPINHEPHrine OCCULAR 1 MG 1 ML AMPULEETOMIDATE 20 MG 10 ML INJECTIONFILGRASTIM-SNDZ 300 MCG 0.5 ML SYRINGEFILGRASTIM-SNDZ 480 MCG 0.8 ML SYRINGEFULVESTRANT 500mg (2x250mg) SYRINGEGI COCKTAIL 60 ML LIQUIDGLUCAGON 1 MG 1 ML INJECTIONGLYCERIN 80% RECTAL NEONATE 0.2 ML ENEMAGOSERELIN 10.8 MG IMPLANTGOSERELIN 3.6 MG IMPLANTHEPARIN (PMX) 50UNITS/ML 500 ML SOLUTIONHEPARIN FLUSH 10 UNITS/ML 5 ML INJECTIONHEPARIN FLUSH 100 UNITS/ML 5 ML INJECTIONHEPARIN LOCK UVC/UAC/PICC 5 UNITS 5 ML SYRINGEHEPARIN SODIUM 10000 UNIT 10 ML MDVHEPARIN SODIUM 1000units/ml 30 ML MDVHEPARIN SODIUM SQ 5000 UNIT 1 ML INJECTIONINDOCYANINE GREEN 25 MG 10 ML INJECTIONINSULIN 70/30 REG-ISOPHANE 3 ML INJECTIONINSULIN LISPRO 100 UNITS/ML 3 ML INJECTIONINSULIN NPH 100UNITS/ML 3 ML INJECTIONINSULIN REGULAR 100UNITS/ML 3 ML INJECTIONISOFLURANE LIQ INHALLABETALOL HCL INJECTION 20 MG 4 ML INJECTIONLET SOLUTION 5 ML LIQUIDLEUPROLIDE 11.25 MG KITLEUPROLIDE 22.5 MG KITLEUPROLIDE 3.75 MG KITLEUPROLIDE 7.5 MG KITLEVONORGESTREL-DOSE PAK 1.5 MG TABLETLIDOCAINE 2% 100 MG 5 ML SYRINGELIDOCAINE IN D5W 2 GM 500 ML PREMIX SOLMAGNESIUM SULFATE 1 GM 2 ML INJECTIONMAGNESIUM SULFATE 2 GM 50 ML PREMIX SOLMAGNESIUM SULFATE 20 GM 500 ML PREMIX SOLMAGNESIUM SULFATE 4 GM 100 ML PREMIX SOLMULTIVITAMIN-(plain) 0.5 ML LIQUIDMULTIVITAMIN-IRON-DROPS (PFL) 0.5 ML SOLUTIONMYCOPHENOLATE MOFETIL 250 MG CAPSULEMYCOPHENOLATE MOFETIL 500 MG TABLETNEOSTIGMINE 5 MG 5 ML SYRINGENEOSTIGMINE METHYLSULFATE 10 MG 10 ML MDVniCARdipine IN SALINE 40 MG 200 ML SOLUTIONNITROGLYCERIN DOSE PACK 0.4 MG TABLETNITROGLYCERIN VIAL 50 MG 10 ML INJECTIONNITROGLYCERIN/DEXTROSE 25000 MCG 250 ML INFUSIONNOREPINEPHRINE BITARTRATE 8 MG 500 ML PREMIX SOLOCTREOTIDE ACETATE 20 MG KITOCTREOTIDE ACETATE 30 MG KITONDANSETRON ODT DOSEPAK 4 MG TABLET DISOXYTOCIN 10 UNITS 1 ML INJECTIONOXYTOCIN IN NS 30 UNIT 500 ML PREMIX SOLPACU DRUG KITPEGFILGRASTIM 6 MG 0.6 ML SYRINGEPHENYLEPHRINE 10 MG 1 ML INJECTIONPHENYLEPHRINE 100mcg/mL 10 ML SYRINGEPHENYLephrine 200mcg/ml 500 ML PREMIX SOLPHYTONADIONE **INFANT** 1 MG 0.5 ML SYRINGEPOTASSIUM CHLORIDE BAG 20 MEQ 50 ML PREMIX SOLPRASUGREL 10 MG TABLETPROMETHAZINE HCL DOSE PACK 25 MG SUPPOSITORPROPOFOL 1000 MG 100 ML INJECTIONPROPOFOL 200 MG 20 ML INJECTIONPROPOFOL 500 MG 50 ML INJECTIONRHOGAM PREFILL SYR (FULL DOSE) 300 MCG INJECTIONRIVAROXABAN 10 MG TABLETRIVAROXABAN 20 MG TABLETROCURONIUM 50 MG 5 ML SYRINGEROCURONIUM BROMIDE 10MG/ML 10 ML MDVRSI KITSODIUM BICARBONATE 4.2% INFANT 4.2 % 10 ML SYRINGESODIUM BICARBONATE 8.4% 50 MEQ 50 ML SDVSODIUM BICARBONATE 8.4% 50 MEQ 50 ML SYRINGESODIUM CHLORIDE 0.9% BACTEROST 30 ML INJECTIONSUCCINYLCHOLINE CHLORIDE 200 MG 10 ML MDVSUCCINYLCHOLINE CHLORIDE 200 MG 10 ML SYRINGESUGAMMADEX SODIUM 500 MG 5 ML SDVSULFACETAMIDE DOSE PACK 15 ML DROPSTBO-FILGRASTIM 300 MCG 0.5 ML SOLUTIONTBO-FILGRASTIM 480 MCG 0.8 ML SOLUTIONTHROMBIN 5000 UNITS POWDERTICAGRELOR 90 MG TABLETTRANEXAMIC ACID 1000 MG 10 ML INJECTIONVASOPRESSIN 20 UNIT 1 ML INJECTIONVECURONIUM 10 MG 10 ML SYRINGEVECURONIUM BROMIDE 10 MG 10 ML INJECTIONWARFARIN 1 MG TABLETWARFARIN 10 MG TABLETWARFARIN 2 MG TABLETWARFARIN 2.5 MG TABLETWARFARIN 3 MG TABLETWARFARIN 4 MG TABLETWARFARIN 5 MG TABLETWARFARIN 6 MG TABLETWARFARIN 7.5 MG TABLET
FEBRUARY 2018 - C

Subject: Providence St. Vincent Pharmacy Technician Checking Validation Program (TCVP) – Year 5 Review
Date: November 30, 2017
Request/Inquiry Type: Policy / Compliance
Background: Providence St. Vincent Pharmacy in Portland, Oregon (IP-0000362) received Board approval for its TCVP program in 2012 and has submitted the Year 5 Follow-Up Report:
TCVP – Year 5 • Who is the program’s primary contact? Randy Neukamm
Since the Year 1 report: • Have the P&P been edited? No. The policy and procedure remains as originally
submitted.
• Are the same personnel still involved? Why/why not?Over the course of theprogram we trained a total of 27 technicians. We currently have 17 active TCVPcertified technicians. The other 10 technicians no longer work at PSVMC. Wehave a need to certify approximately 5 more staff members but have not hadresources to establish dedicated time for the didactic program and initial validation.
• Have any failures/re-trainings/etc. occurred? Please describe. We did have onetechnician who did not catch errors introduced as part of the semi-annual testing. He was removed from TCVP checking duties. The PharmacyOperations Supervisor reviewed training materials and expectations. Hesubsequently was retested passed. He was then allowed to perform tech checktech duties and has not failed any routine tests in the interim.
• Have there been any additional improvements to patient safety and/or pharmacistresource utilization? What specific clinical responsibilities have your pharmacistsbeen freed up to do since your program began?The TCVP program has allowed us tofree up 56 hours of pharmacist time. This time was used to deploy a Transition ofCare Pharmacist shift. Literature demonstrates that many medication relatedproblems occur during hand offs of patient upon admission, transfer and discharge(e.g. transitions of care). The TOC pharmacist has allowed for increasedpharmacist education of high risk patients, allowed us to expand our patientrounding program and facilitate a smoother and safer discharge process for thepatients we serve.
FEBRUARY 2018 - C1
See pages 3-4 for a copy of their 1-year follow-up report, and pages 5-16 for essential components of their original 2012 request.
Recommendations: Accept report & have Providence Portland Medical Center Pharmacy report back in February 2022 for 5-year renewal.
Contact: Randy S. Neukamm R.Ph. Operations Manager Providence St. Vincent Pharmacy Phone: 503-216-2158
FEBRUARY 2018 - C1

OCTOBER 2014 / C
Providence St. Vincent Medical Center Pharmacy Portland, Oregon
Technician Checking Validation Program Report-- October 8, 2014
When implemented? • Didactic training of initial group of pharmacy technicians began 12/1/2012.• Practical session (observations) for ADC & Non-Emergent Kits/Trays began 12/3/2012.• First pharmacy technician to be validated was on 1/2/2013.• Five pharmacy technicians were validated at the start of our program on 1/13/2013.
How has it gone? • The implementation of the TCVP has provided us the opportunity to improve our patient’s healthand safety. We have adjusted our pharmacist staffing model to incorporate approximately fiveadditional hours a day (over 2900 hours since its inception) of pharmacist staffing time to be re-directed from distributive services to clinical services.• We have completed four didactic training classes.• We have validated 23 pharmacy technicians.• We currently have 20 pharmacy technicians working in the program. Three previously validatedpharmacy technicians have terminated their employment.
Did you catch errors? • Yes, five pharmacy technicians did not pass a random and unannounced quality assurance check.All five pharmacy technician did pass the retake quality assurance check.
TCVP Initial Validation and QA Check Accuracy (12/3/2013- 8/31/2014)
Total Items Checked 23,968 Accuracy rate 99.8665% Introduced Artificial Errors Missed
Drug 8 (0.0334 %) Dose 12 (0.0501 %) Form 0 Quantity 6 (0.0250 %) Expiration Date 6 (0.0250 %)
Total Errors Missed 32 Error Rate 0.1335 %
FEBRUARY 2018 - C1

OCTOBER 2014 / C
Did training program and materials work? • They worked very well. Positive feedback was received from the technicians that were trained. Any revisions needed? • No revisions of the training program or materials. Any problems with the rules and any recommended changes? • Oral Cart fill is approximately 27 doses a day. We have not implemented the Unit of Use Cart Fill
technician checking due to the 1500 doses (5 batches x 300 doses) that are needed to validate a technician and 300 doses per QA check. Pharmacists continue to provide the distributive service of checking the Unit of Use Cart Fill instead of providing clinical services.
o Recommend keeping separate training for Unit of Use Cart Fill Checking but decrease the quantity of doses needed for initial validation and for the QA check. • Consider incorporating the use of technology in checking process. Suggests for others considering TCVP. • Designate and train pharmacists from different shifts to be involved in the QA checks. Future implementation at other Providence hospitals. • Providence Medford Medical Center is not implementing due to current staffing restraints but
have it on list of future projects. • Providence Hood River Memorial Hospital Is evaluating the practice. • Providence Seaside Hospital – No plans to implement. • Providence Newberg Medical Center- No plans to implement. Current process is too laborious. • Providence Portland Medical Center Is considering but no timeline has been established. • Providence Milwaukie Hospital - No plans to implement (only one technician staffing at one
time). • Providence Willamette Falls Medical Center – No plans to implement. Current process is too
laborious.
FEBRUARY 2018 - C1

OCTOBER 2012 / #CFEBRUARY 2018 - C1

OCTOBER 2012 / #CFEBRUARY 2018 - C1
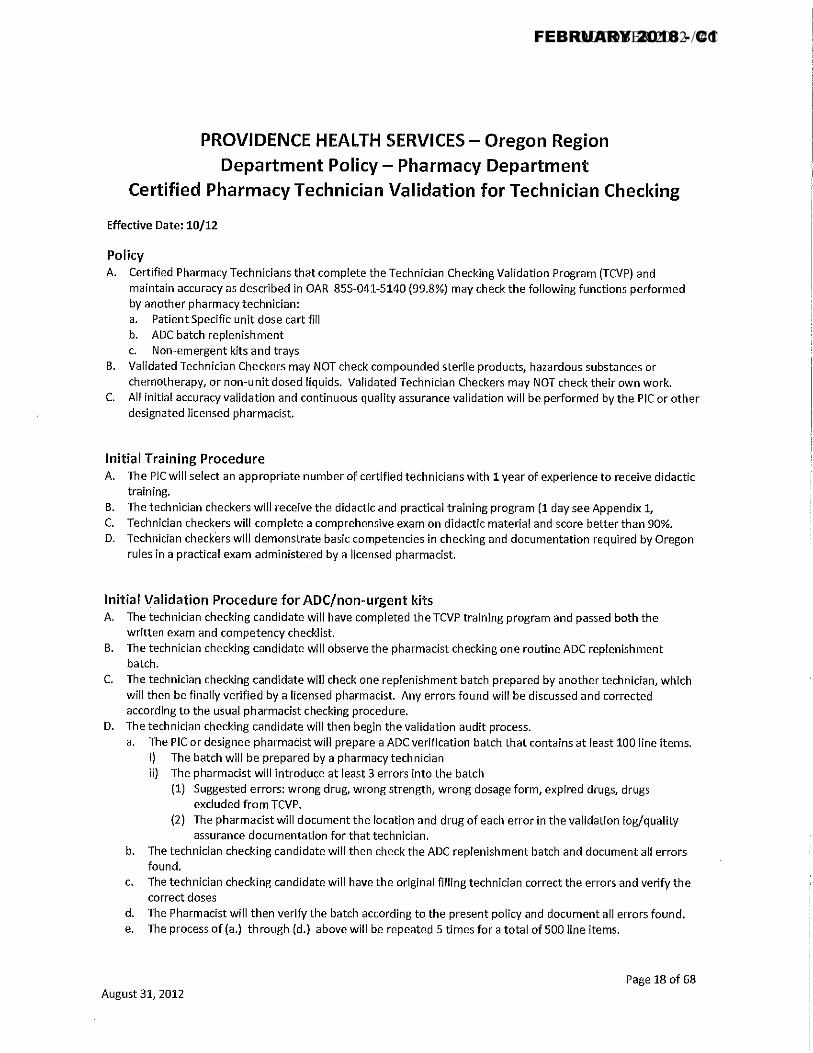
OCTOBER 2012 / #CFEBRUARY 2018 - C1
OCTOBER 2012 / #CFEBRUARY 2018 - C1

OCTOBER 2012 / #CFEBRUARY 2018 - C1

OCTOBER 2012 / #CFEBRUARY 2018 - C1

OCTOBER 2012 / #CFEBRUARY 2018 - C1

OCTOBER 2012 / #CFEBRUARY 2018 - C1
OCTOBER 2012 / #CFEBRUARY 2018 - C1

OCTOBER 2012 / #CFEBRUARY 2018 - C1

OCTOBER 2012 / #CFEBRUARY 2018 - C1

OCTOBER 2012 / #CFEBRUARY 2018 - C1

Oregon Board of Pharmacy – Position Statement February 2018
Sterile Syringe Access and Harm Prevention
There is an opioid, heroin and methamphetamine crisis occurring across Oregon and the US. Evidence shows that access to sterile syringes and naloxone are effective strategies to reduce negative health outcomes and the spread of disease related to injection drug use, including HIV, Hepatitis B and C and overdose. Reuse of syringes is common when new syringes are unavailable; this increases intravenous drug users (IDUs) risk of infections and communicable diseases.
Oregon was the first state to squarely face the question of syringe access as a public health measure. Prior to 1987, syringe sales were not regulated. In that year, the legislature passed a paraphernalia law based on the model statute but heeded the advice of state health officials to explicitly exclude syringes from the definition of paraphernalia (ORS 475.525(3)). In Oregon, it is therefore legal to sell syringes not only in pharmacies but also in other retail outlets, and to distribute them free through Syringe Exchange Programs (SEPs) or other mechanisms. Of note, the sale of syringes in Oregon does not require a prescription. However, a pharmacist must use good professional judgment when selling syringes to minors (individuals less than 18 years of age) see ORS 475.744. The Oregon approach has minimized the legal barriers to syringe access.
Public health studies have proven legal syringe access reduces syringe reuse and sharing, does not promote injection drug use, and does not increase criminal activity in surrounding areas. When pharmacies or pharmacists choose to directly or indirectly restrict syringe sales to IDUs, or to not carry naloxone, the opportunity to decrease or prevent individual and community harm from addiction and injection drug use are lost.
The Board recommends and encourages pharmacies and pharmacists to increase access of sterile syringes and naloxone to the public. Pharmacies are important public health partners for infectious disease and drug overdose prevention. Existing laws in Oregon have positioned pharmacies and pharmacists to support public health efforts to increase community member access to sterile syringes and naloxone, deliver health education, and refer IDUs to local health care and recovery services. Removing the stigma of selling sterile syringes and prescribing and dispensing naloxone will improve patient care in the short and long term.
FEBRUARY 2018 - C2

Documents associated with February 2018 / C3 can be obtained on the following links through the PTCB website:
Press Release:
http://www.ptcb.org/about-ptcb/news-room/news-landing/2018/01/11/ptcb-announces-new-pharmacy-technician-certification-examination-(ptce)-content-outline-and-updated-education-training-requirement-for-cpht-certification#.WnDB2eRy6Uk
Summary of PTCE program changes:
http://www.ptcb.org/about-ptcb/certification-program-changes#.WnDBM-Ry6Uk
CPhT Program Recognition Attestation Form:
https://www.ptcb.org/docs/default-source/about-ptcb/cpht-program-recognition-attestation-form-v-1---jan-2018.pdf?sfvrsn=2
CPhT Work Experience Attestation Form:
https://www.ptcb.org/docs/default-source/about-ptcb/cpht-work-experience-attestation-form-v-1---nov-2017.pdf?sfvrsn=2
PTCE Content Outline Effective 1/1/2020:
https://www.ptcb.org/docs/default-source/about-ptcb/ptce-content-outline-effective-january-1-2020.pdf?sfvrsn=2
PTCE 2.0 to 3.0 Crosswalk:
https://www.ptcb.org/docs/default-source/about-ptcb/ptce-2-0-to-3-0-crosswalk-v1---nov-2017.pdf?sfvrsn=2
FEBRUARY 2018 / C3 - LINKS

TO: EXECUTIVE OFFICERS – STATE BOARDS OF PHARMACY
FROM: Carmen A. Catizone, Executive Director/Secretary
DATE: January 12, 2018
RE: National Healthcareer Association ExCPT Program Before the end of 2017, NABP was asked by a number of member state boards of pharmacy to provide evaluative information on the National Healthcareer Association’s (NHA) ExCPT exam for pharmacy technicians. NHA agreed to cooperate with NABP and, with NABP, commissioned a panel of psychometricians to review components of the ExCPT exam in accordance with the attached criteria. The panel of psychometricians determined that the ExCPT exam met the criteria and NABP accepted that determination. For proprietary and confidentiality reasons, NABP did not have access to the materials reviewed by the panel. However, the panel indicated to NABP that all requests for information and follow-ups were provided by NHA. Attachment cc: NABP Executive Committee
FEBRUARY 2018 - C4

Overall Criteria
1. The intended interpretation and use of exam scores is clearly defined for the appropriate stakeholder audiences.
2. Subject matter experts who participate in exam development activities have the individual and collective expertise necessary to adequately inform the exam definition, the practice or curriculum analysis, the creation and defense of exam questions, the establishment and interpretation of the cut scores, and other aspects of exam development.
3. The exam’s domain of interest is based on a thorough practice or curriculum analysis using sound methodology.
4. The exam blueprint and other exam specifications represent a conversion of the domain of interest into a set of exam authoring and assembly rules based on defensible and explicit decision-making procedures.
5. The exam items are logically linked to the exam blueprint.
6. Safeguards are in place for ensuring that the questions developed and included on the examination are appropriate for Pharmacy Technicians who are practicing in any of the states.
7. The exam questions are clear, well-formed, unambiguous, inoffensive, and interpretable by all subgroups in the candidate population.
8. Algorithms responsible for scoring individual exam questions, and producing exam scores or any reported part scores are defensible, implemented correctly, and function dependably.
9. The contribution of individual exam questions to the measurement scale is empirically established based on response data from examinees who represent the candidate population of interest.
10. The exam forms are assembled in compliance with the exam blueprint and other exam specifications.
11. Steps are taken to minimize the risk of items appearing on the same exam form that either compromise one another (i.e., any part of the content of one item provides the answer to another item) or duplicate one another (i.e., two items make the same demand of the candidate).
12. Procedures are implemented on a routine basis to assess exam security and multiple equivalent forms of the exam are assembled as needed to protect exam security and the equivalence of alternate or successive exam forms is established empirically.
FEBRUARY 2018 - C4

13. If well-measured external variables exist that can be expected to relate to the exam scores in specific ways, these relationships are borne out in exam score correlations with these variables.
14. All reported scores and sub-scores have acceptable levels of reliability and their reliability is monitored and reported over time.
15. The procedures used to set the location of the cut score on the measurement scale are defensible.
16. The standard error of measurement near the cut score and pass-fail classification consistency are adequate.
17. The stability of the measurement scale is monitored and maintained over time.
18. Candidates have sufficient time to complete the exam.
19. Potential sources of construct-irrelevant variance in exam responding are evaluated and eliminated.
20. Candidate instructions are adequate to guide the candidate to interact with the exam in ways intended by the exam developer.
21. Candidates receive standardized and equitable treatment at the testing center, including justified accommodations to remove physical or emotional barriers to testing that are not relevant to the domain of interest.
22. The test environment affords reasonable comfort and minimal distractions.
23. Score reports and other reports delivered to stakeholders are timely and interpretable and steps are taken to prevent potential misinterpretations of exam scores and unintended negative consequences of exam use.
24. Exam technical reports are available to users that enable them to make judgments about exam quality and the validity of pass-fail decisions.
25. Examinee bulletins, user’s guides, tutorials, and other preparatory publications by the exam sponsor should be produced in a timely manner and should clarify the purposes of the exam to the user, inform the candidate about exam eligibility, exam registration procedures, the examination experience and score reporting policy, and answer frequently-asked questions, so that irrelevant sources of score variance are minimized and the interests of the candidate and the exam sponsor are protected.
FEBRUARY 2018 - C4

26. The exam sponsor takes reasonable steps to prevent exam content and metadata from being stolen and divulged outside of the controlled exam delivery environment.
27. The exam sponsor follows and communicates clear policies about the transmission and storage of personal and exam-related information and takes steps to secure this information against unauthorized access.
28. The exam delivery provider works with the exam sponsor to ensure that protocols are being followed at the test center to verify candidate identity and prevent cheating.
29. Irregular or anomalous exam sessions are flagged and evaluated using established protocols ensuring fair treatment of all candidates while upholding the validity of pass-fail decisions. Pass-fail judgments are not endorsed when available evidence calls into question their validity.
30. Candidates are given fair treatment and afforded a reasonable resolution process for charges of candidate misconduct or irregular behavior by the exam sponsor or challenges by the candidate to the accuracy of scoring or the correctness of the scoring key.
31. Quality assurance protocols are established and followed related to all exam development, delivery, and results processing activities. Efforts are made to proactively detect errors and to correct them quickly.
32. Revisions to the item pool content, item metadata, exam blueprint and specifications, exam measurement scale(s), cut score, and domain of interest are made in response to new evidence. This evidence is collected as part of an established exam development life cycle.
References
American Educational Research Association, American Psychological Association, National Council on Measurement in Education (2014). Standards for educational and psychological testing. Washington, D.C.: American Educational Research Association.
FEBRUARY 2018 - C4

Oregon Board of Pharmacy January 2018
1. RPh submits aconcept intake form
2. Board staff reviewsrequest; gathers additional
information if necessary
3. Board staff will summarizethe information and present
the concept to the committee
4. Committee reviewsand discusses concept
5. Committee makes arecommendation to the
Board (via a motion)
6. Board reviewsrecommendation;if approved, Boardstaff will draft rule
8. Board reviewscomments, decides to
approve (“adopt”) or not approve proposed rule (see Board’s Timeline)
9. Committee reviewsformulary and protocolson a regular basis Advisory Committee
Process
7. Board sendsproposed rule to a public rulemaking
hearing for comments
FEBRUARY 2018 / D