oral surgery in childrendental.subharti.org/pedodontics_lectures/oral_surgery.pdfprinciples of...
TRANSCRIPT

Oral surgery in children
Dr. Himanshu Kapoor
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

SURGERY: Branch of medical science which treats injuries , trauma , or diseases by
manipulation or operation
Differences
Small oral cavity
Lack of patient co-
operation
Jaws are in growing
phase
Abundant blood supply
Bone is porous , more
malleable
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

ORAL SURGICAL PROCEDURES IN CHILDREN
1. EXTRACTION
2. IMPACTION
3. FRENECTOMY
4. APICOECTOMY
5. CYST
6. FRACTURE
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

DEFINITION
” Extraction is defined as complete, painless removal of tooth or tooth root with minimal trauma to surrounding investing structures, so that the wound heals uneventfully and there will be no post operative prosthetic problems”.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

INDICATIONS FOR EXTRACTION
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

CONTRA INDICATIONS
FOR
EXTARACTION
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

ABSOLUTE
CONTRA INDICATIONS
1) LOCAL :-
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

2) SYSTEMIC
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

RELATIVE CONTRA INDICATIONS
1). LOCAL :-
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

SYSTEMIC CONTRA INDICATIONS
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

EVALUATION OF TEETH REMOVAL
• Access to Tooth
• Mobility of Tooth
• Condition of Crown
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

RADIOGRAPHIC EVALUATION
• Condition of the Tooth.
• Condition of the Bone.
• Relationship with associated Vital structures.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

RADIOGRAPHIC INDICATIONS
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

TYPES OF EXODONTIA
• Intra-alveolar extraction also called as Closed extraction. Where tooth is luxated and elevated out of socket with elevators and forceps.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

• Trans-alveolar extraction in this method an incision is placed and mucoperiosteal flap is reflected for proper accessibility, bone cutting is done either with a chisel and mallet or a bur. Sutures are placed to approximate wound margins.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

PRINCIPLES OF EXTRACTION
• Intra-alveolar or Closed method
1. Forcep blade should be placed below the C.E. junction on sound root portion with apical thrust.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

2. Mechanical principles:
1.) Expansion of bony socket
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

2) use of lever and fulcrum to elevate the tooth.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

3). Use of wedge or wedges within root or socket.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU
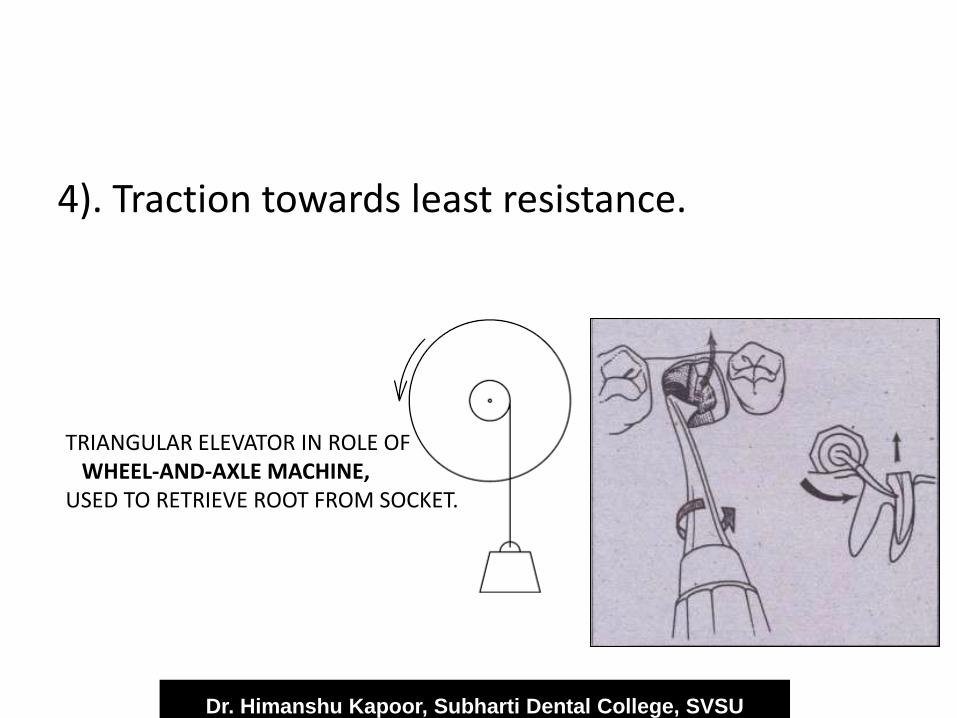
4). Traction towards least resistance.
TRIANGULAR ELEVATOR IN ROLE OF WHEEL-AND-AXLE MACHINE, USED TO RETRIEVE ROOT FROM SOCKET.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

PRINCIPLES FOR DECIDUOUS TEETH
EXTRACTION • Gentle and Judicious use of elevators
• Beak of the forceps should be carefully placed, so that it should not injure the hidden permanent tooth bud.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

ORDER OF EXTRACTION
• To prevent bleeding from socket of extracted teeth obscuring the field of operation distal most tooth is first extracted.
• Maxillary teeth should be extracted before mandibular to prevent falling of debris or totth material in to socket.
• Canine should not be left last as alveolus may get fractured due to its length.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

FORCES DURING EXTRACTION
• Apical force: to wedge the forceps firmly in the periodontal ligament space. this does not actually move the tooth but expands the bony socket
• Buccal force: Expands the buccal cortical plate. • Lingual force: Expands the lingual cortical plate. • Rotational force: Teeth with single conical roots
can be extracted by this method. it causes internal expansion of the bony socket.
• Tractional force: These are forces applied finally to remove the tooth completely out of socket.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

RULES FOR APPLICATION OF FORCEPS
• Correct forceps for particular tooth should be selected.
• Grasp the forceps at the far end of handles.
• Long axis of the beaks of the forceps should be parallel to the long axis of the tooth.
• Beaks should be firmly grasped on sound root structure, not on enamel of crown.
• Beaks should not impinge on adjacent teeth.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

FORCES APPLIED FOR DIFFERENT
TEETH • MAXILLARY:
• Incisors: labial-lingual-labial with mesial rotation.
• Cuspids: labial-lingual-labial with mesial rotation.
• First premolar: buccal-palatal-removal in buccal direction.
• Second premolar: buccal-palatal-removal in buccal or palatal direction.
• Molars: buccal-slight palatal and distal rotation.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

MANDIBULAR:
• Anteriors: labial-lingual-slight mesial to distal
force and removal in labial direction.
• Premolars: buccal with slight mesio-distal rotation.
• Molars: buccal-lingual and removal in buccal direction.
• Third molars: buccal pressure and removal in buccal or lingual direction.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

COMPLICATIONS OF EXODONTIA
• A complication is any deviation from normal expected pattern of events
• Fracture of:
• Crown of tooth.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

POST OPERATIVELY DAMAGE TO:-
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

POST OPERATIVE PAIN DUE TO:-
• Acute osteomyelitis
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

POST OPERATIVE SWELLING DUE TO
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

TECHNIQUE FOR TOOTH REMOVAL IN CHILDREN
Explain the child : sensations
Procedure
Use elevator to free the attached gingiva from the cervix of the tooth labilally and lingually. Luxate the tooth slightly.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

FOR PRIMARY ANTERIORS :
Beak of plier cervically……….slight rotation
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

FOR PRIMARY POSTERIORS
• Reflection of buccal and lingual gingiva ……beak at the furcation area……………give buccal movement ----normal----buccal ----normal ----then pull .
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Inaccessible Root Tips If root tip is hopelessly unattainable through normal
means & will not interfere with normal growth and eruption, leave the root to exfoliate on its own.
Or remove surgically.
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

• If permanent tooth bud is moved during extraction, reinsert it properly ( buccolingual position ), apply suture to close socket .
• Pulp tests
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

INDICATIONS FOR EXTRACTION OF PERMANENT FIRST MOLARS
• If first molar extracted before second molar eruption (in gingiva ) – 2nd molar will move mesially and occupy the space .
• If 2nd molar has erupted – mesial tilting ( periodontal disease and orthodontic problems )
• If three molars are diseased – extract all four
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

IMPACTIONS
• Tooth fails to erupt even after its normal force of eruption due to any physical barrier.
• Prevalence : Permanent maxillary canine
Mandibular II pre molar
Maxillary lateral incisor
Supernumerary tooth
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

CAUSES
Local • Arch length deficiency
• Thick fibrous gingiva
• Premature loss of primary tooth
• Any pathology
Systemic • Hypopituitarism
• Hypothyroidism
• Genetic
• Cleft palate
• Cleidocranial dystosis
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

MANAGEMENT
1. NO NEED TO EXTRACT
2. ORTHODONTIC MANAGEMENT
3. SURGICAL REMOVAL
Dr. Himanshu Kapoor, Subharti Dental College, SVSU
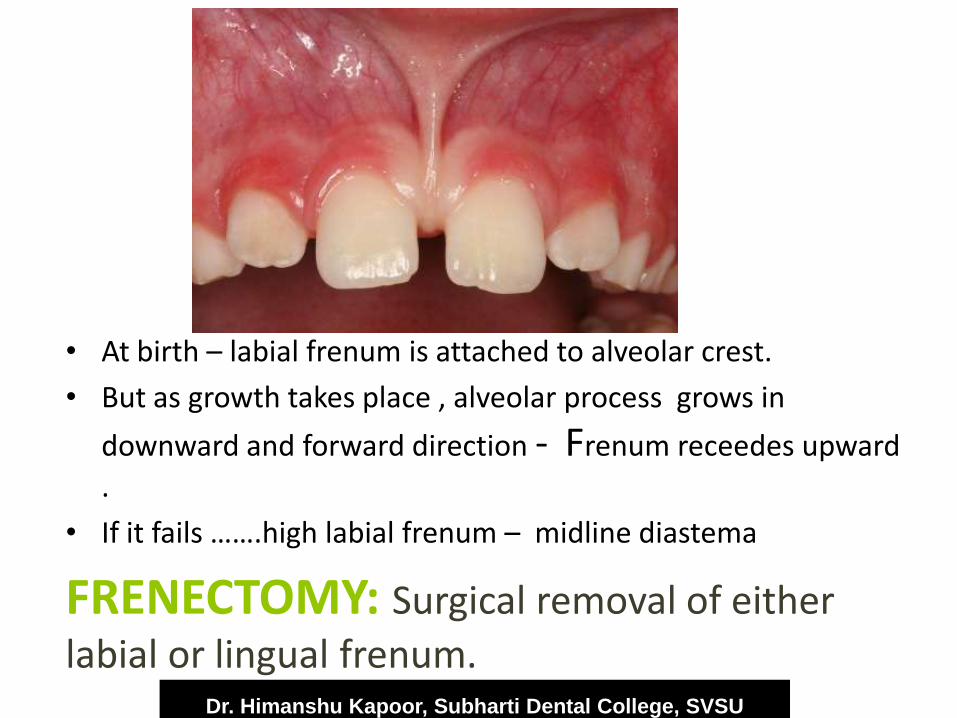
• At birth – labial frenum is attached to alveolar crest.
• But as growth takes place , alveolar process grows in
downward and forward direction - Frenum receedes upward
.
• If it fails …….high labial frenum – midline diastema
FRENECTOMY: Surgical removal of either
labial or lingual frenum. Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

APICOECTOMY
• Surgical removal of the apical end of periapically involved teeth /tooth in order to remove the pathology and to achieve a proper hermetic seal
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Indications
Tooth / teeth which cannot be obturated by conventional orthograde method .
Broken instrument
Periapically involved teeth involving more than 1/3rd of the total root.
Failure to heal even after endodontic procedure .
Horizontal root fracture ( apical 3rd )
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Contraindications
Medically compromised patients
Acute infections
Anatomical landmarks are close to root apex
Intentional Reimplantation
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

Dr. Himanshu Kapoor, Subharti Dental College, SVSU

CYSTS IN THE SOFT TISSUES OF THE ORAL CAVITY
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

MUCOUS CYSTS
Site : lips and cheeks
hard and soft palate.
Appearance: Bluish in color
Elastic consistency
Treatment : Excision .
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

RANULAS AND DERMOID CYSTS
RANULAS
Site: floor of the mouth
Thin walled , blue-red ,
vesicular prominence
Have viscous fluid
Treatment :
marsupialization
DERMOID CYSTS
Yellowish in color
rubber like consistency
Filled with cheesy yellow
material
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

FRACTURES IN CHILDREN
• Facial fractures : 5%
• In young children :
• 1. More retruded position relative to the “protective” skull
• 2. The high elasticity of young bones, a thick layer of the adipose tissue covering them contributing to the low incidence of facial fractures
Dr. Himanshu Kapoor, Subharti Dental College, SVSU

• Relatively larger amount of medullary bone held by a strong periosteal support
• Osteogenic potential of the periosteum leads to rapid and easier healing .
• In # without displacement : careful observation
• Minimally displaced #:crylic splints, circumferential wiring, arch bar or gunning splint
Dr. Himanshu Kapoor, Subharti Dental College, SVSU
