oral premalignant lesions and early detection - heshno.org lesions and early... · oral...
TRANSCRIPT
Oral Premalignant Lesions and Early Detection
Nikolaos G. Nikitakis, MD, DDS, PhDDiplomate, American Board of Oral and Maxillofacial PathologyFellow AAOMP – Fellow AAOM Associate Professor, Dept. of Oral Pathology and Medicine, University of Athens, GreeceSecretary General, European Association of Oral MedicinePresident, Hellenic Society of Oral Medicine and Oral Pathology
Lecture Outline
Epidemiologic aspects of oral cancer
Classification Clinicopathologic features Diagnosis Malignant transformation Management
EPIDEMIOLOGIC ASPECTS OF ORAL CANCER
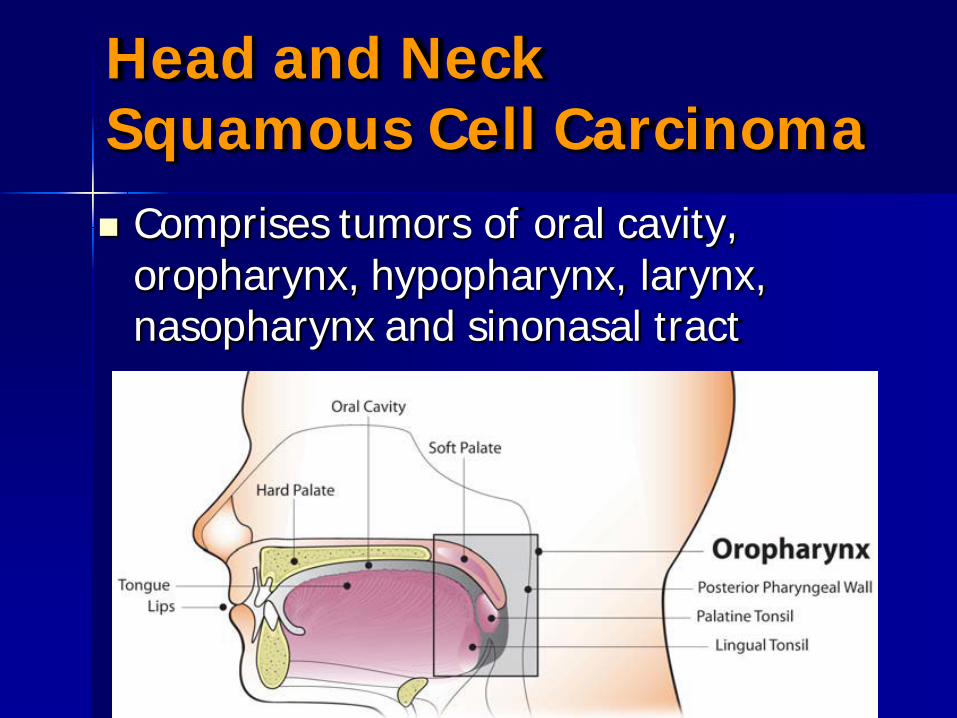
Head and Neck Squamous Cell Carcinoma Comprises tumors of oral cavity,
oropharynx, hypopharynx, larynx, nasopharynx and sinonasal tract
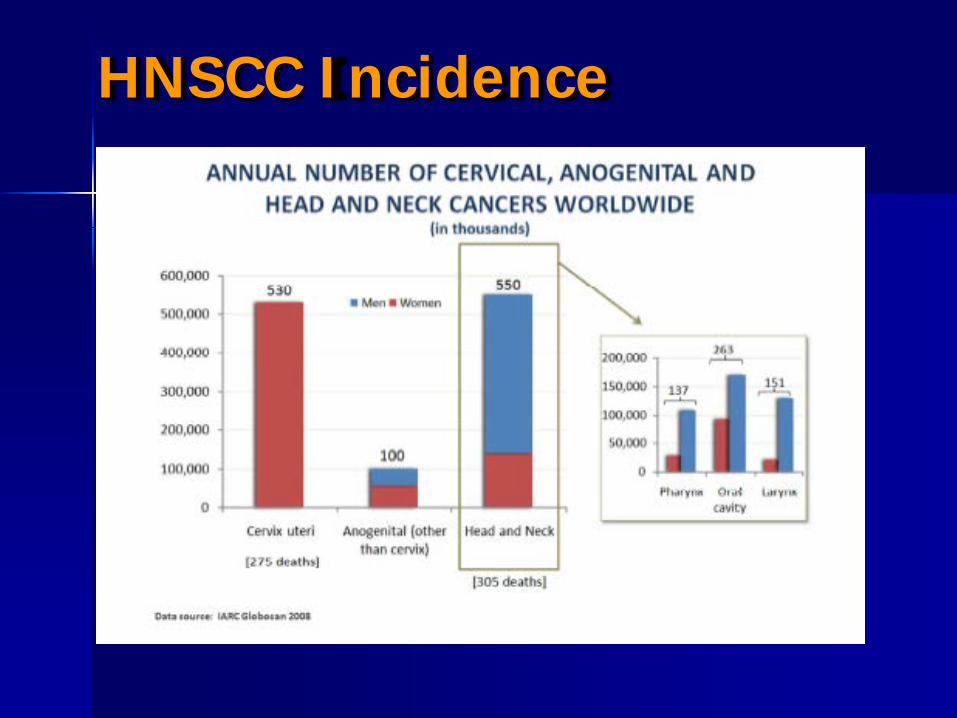
HNSCC Incidence
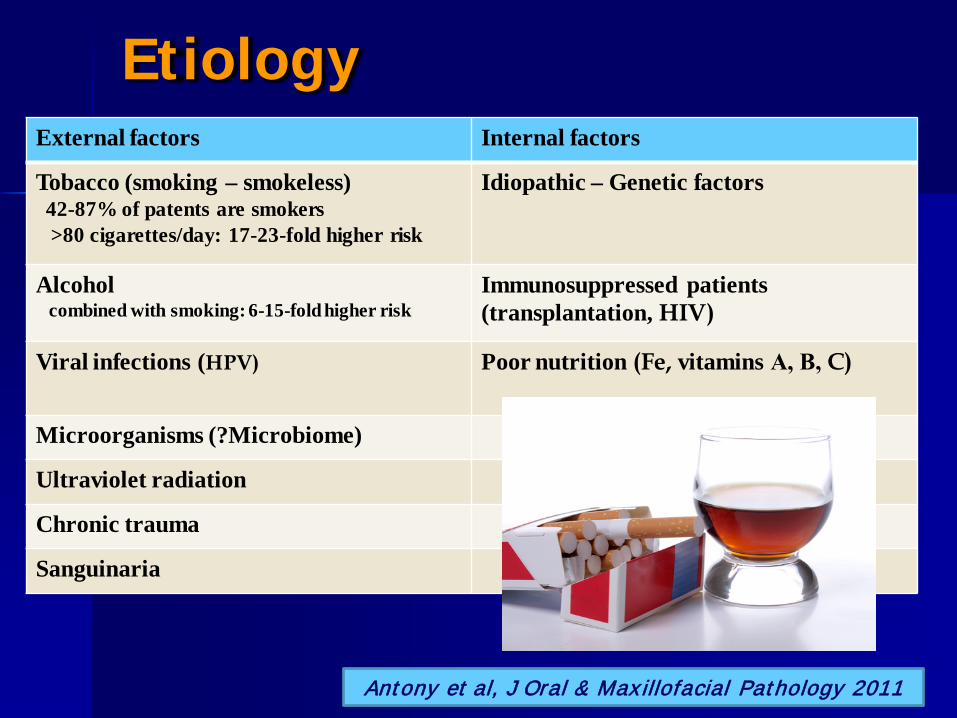
EtiologyExternal factors Internal factors
Tobacco (smoking – smokeless)42-87% of patents are smokers>80 cigarettes/day: 17-23-fold higher risk
Idiopathic – Genetic factors
Alcoholcombined with smoking: 6-15-fold higher risk
Immunosuppressed patients(transplantation, HIV)
Viral infections (HPV) Poor nutrition (Fe, vitamins Α, Β, C)
Microorganisms (?Microbiome)
Ultraviolet radiation
Chronic trauma
Sanguinaria
Antony et al, J Oral & Max illofacial Pathology 2011
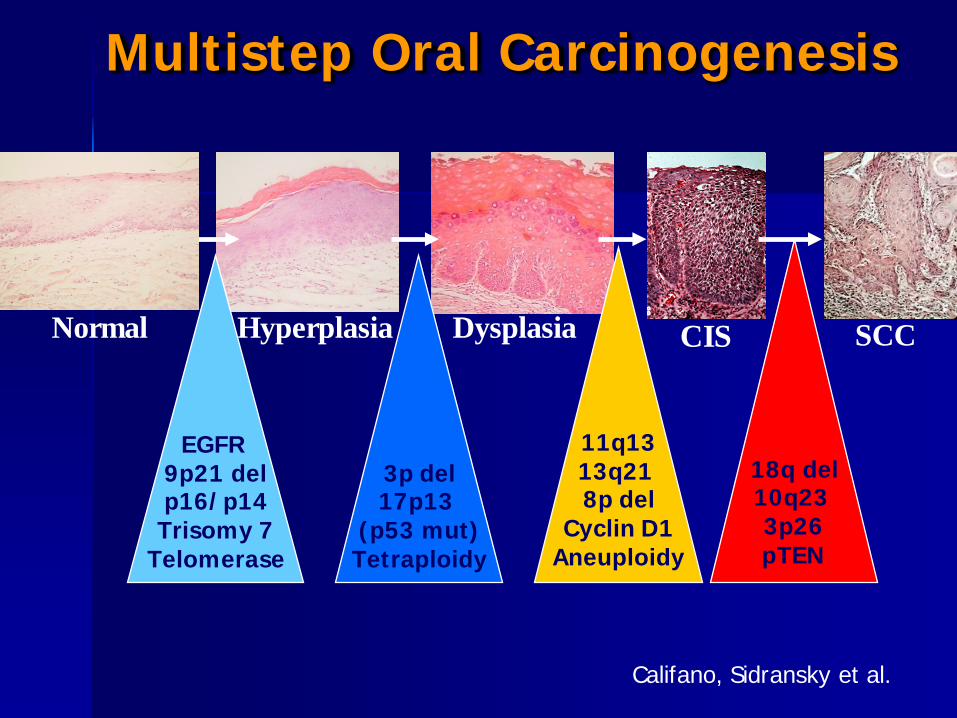
Multistep Oral Carcinogenesis
CISHyperplasia
EGFR 9p21 delp16/p14Trisomy 7
Telomerase
3p del17p13
(p53 mut)Tetraploidy
Dysplasia
11q1313q21 8p del
Cyclin D1Aneuploidy
18q del10q23 3p26pTEN
Normal SCC
Califano, Sidransky et al.
Epidemiology of Oral Cancer
Patients with HNSCC frequently present with advanced stage disease
Prognosis for oral cancer: relatively unchanged despite treatment advances
Many cases of oral cancer are preceded by premalignant lesions (most notably leukoplakia and erythroplakia), allowing their early detection and eradication
Epidemiology of Oral Precancer
Oral leukoplakia
Global Prevalence 2.6%
23 studies: 17 countries, 1986-2002
Petti S. Pooled estimate of world leukoplakia prevalence: a systematic review. Oral Oncol 2003; 39: 770–80.
CLASSIFICATION AND NOMENCLATURE OF ORAL PMDs
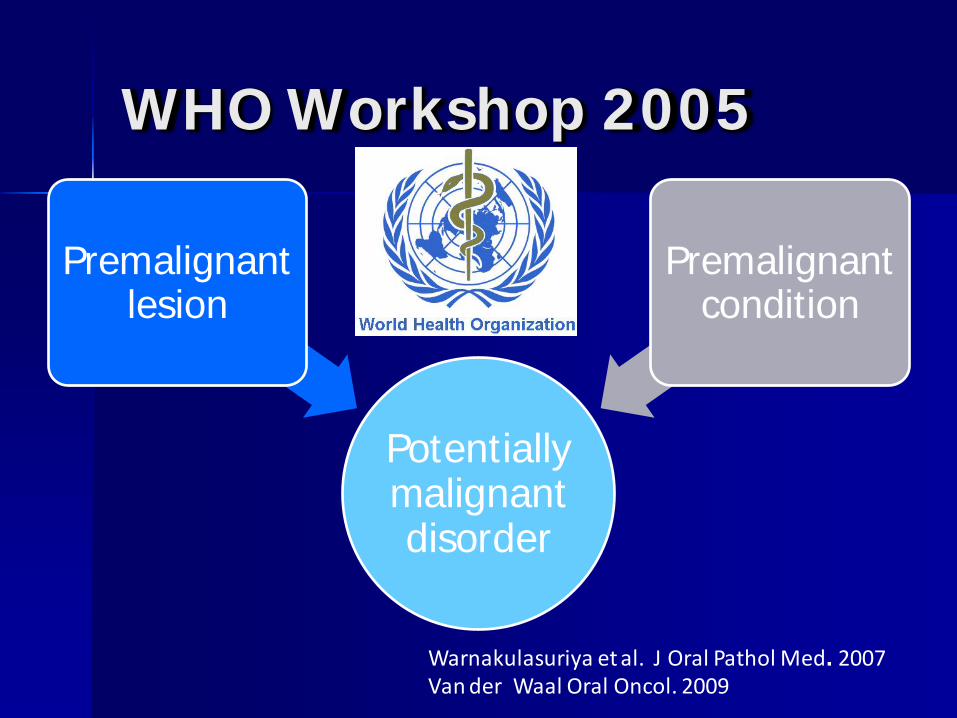
WHO Workshop 2005
Potentially malignant disorder
Premalignant lesion
Premalignant condition
Warnakulasuriya et al. J Oral Pathol Med. 2007Van der Waal Oral Oncol. 2009
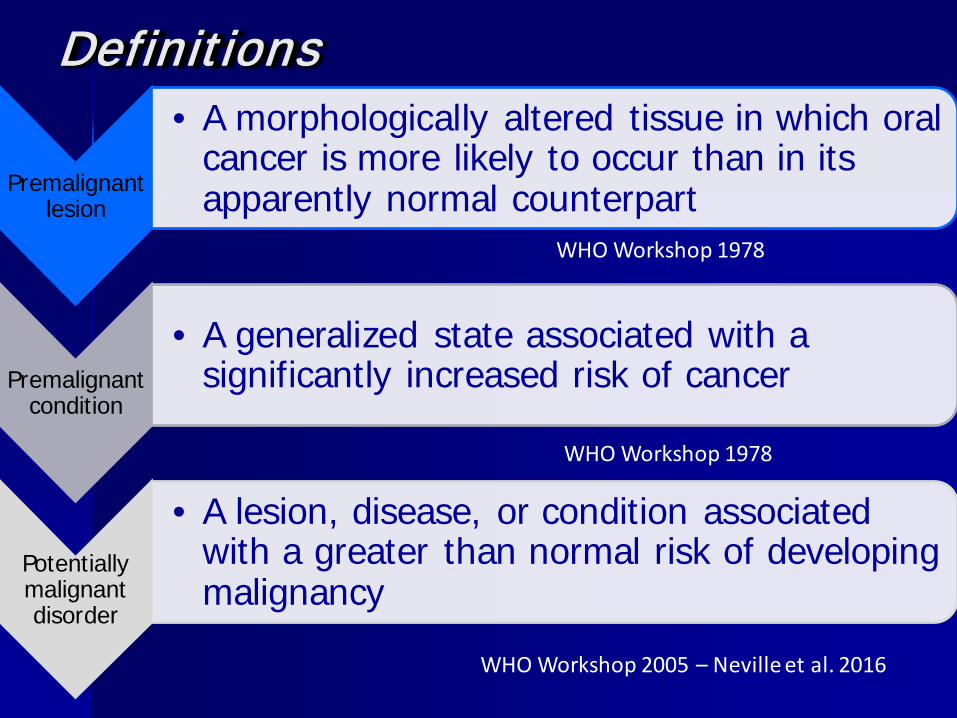
Definitions
Premalignant lesion
• A morphologically altered tissue in which oral cancer is more likely to occur than in its apparently normal counterpart
Premalignant condition
• A generalized state associated with a significantly increased risk of cancer
Potentially malignant disorder
• A lesion, disease, or condition associated with a greater than normal risk of developing malignancy
WHO Workshop 1978
WHO Workshop 1978
WHO Workshop 2005 – Neville et al. 2016
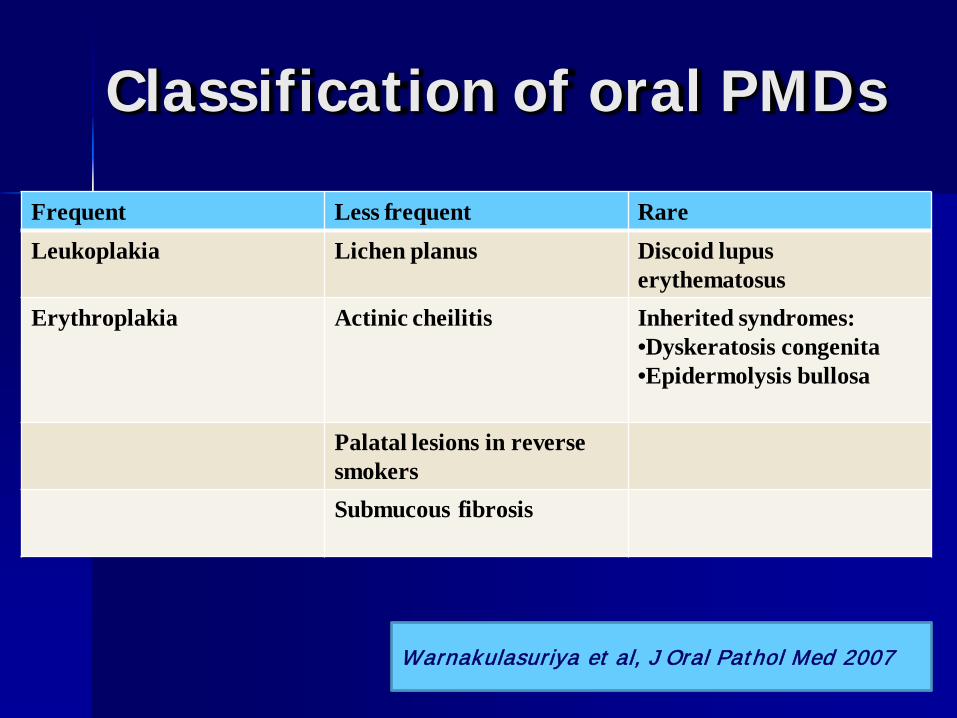
Frequent Less frequent RareLeukoplakia Lichen planus Discoid lupus
erythematosusErythroplakia Actinic cheilitis Inherited syndromes:
•Dyskeratosis congenita•Epidermolysis bullosa
Palatal lesions in reverse smokersSubmucous fibrosis
Warnakulasuriya et al, J Oral Pathol Med 2007
Classification of oral PMDs
A white plaque of questionable risk having excluded (other) known diseases or disorders that carry no increased risk for cancer
Diagnosis of exclusion Clinical term that does not indicate specific
histopathologic features Presence or absence of dysplasia
WHO 2005
Definition of Leukoplakia
CLINICOPATHOLOGIC FEATURES
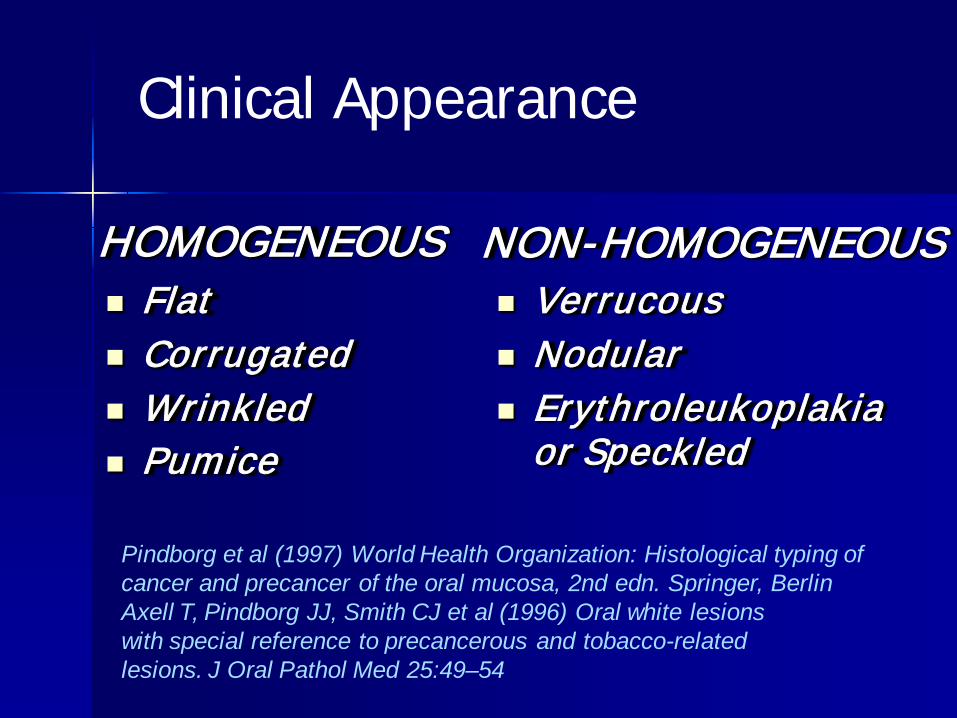
HOMOGENEOUS NON-HOMOGENEOUS Flat Corrugated Wrinkled Pumice
Verrucous Nodular Erythroleukoplakia
or Speckled
Pindborg et al (1997) World Health Organization: Histological typing of cancer and precancer of the oral mucosa, 2nd edn. Springer, BerlinAxell T, Pindborg JJ, Smith CJ et al (1996) Oral white lesionswith special reference to precancerous and tobacco-relatedlesions. J Oral Pathol Med 25:49–54
Clinical Appearance
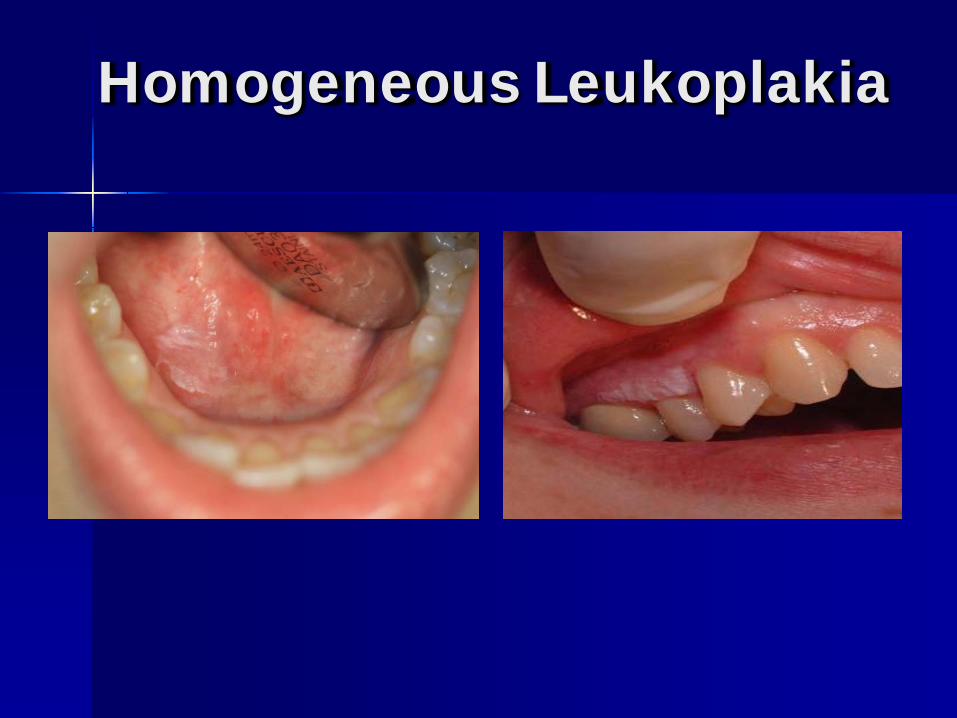
Homogeneous Leukoplakia
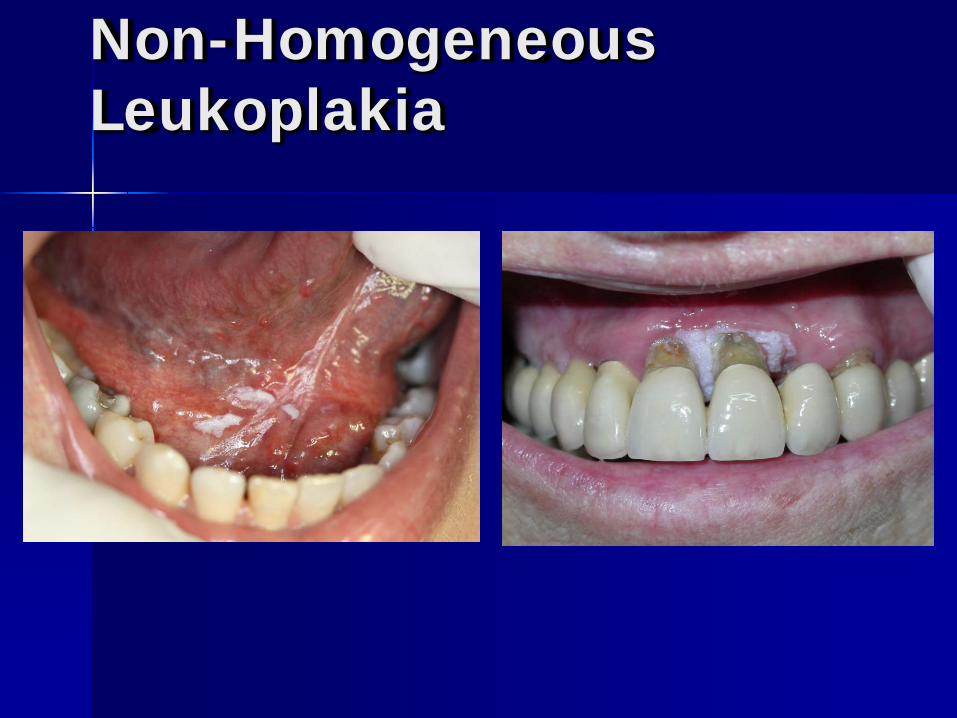
Non-Homogeneous Leukoplakia

Multifocal Leukoplakia
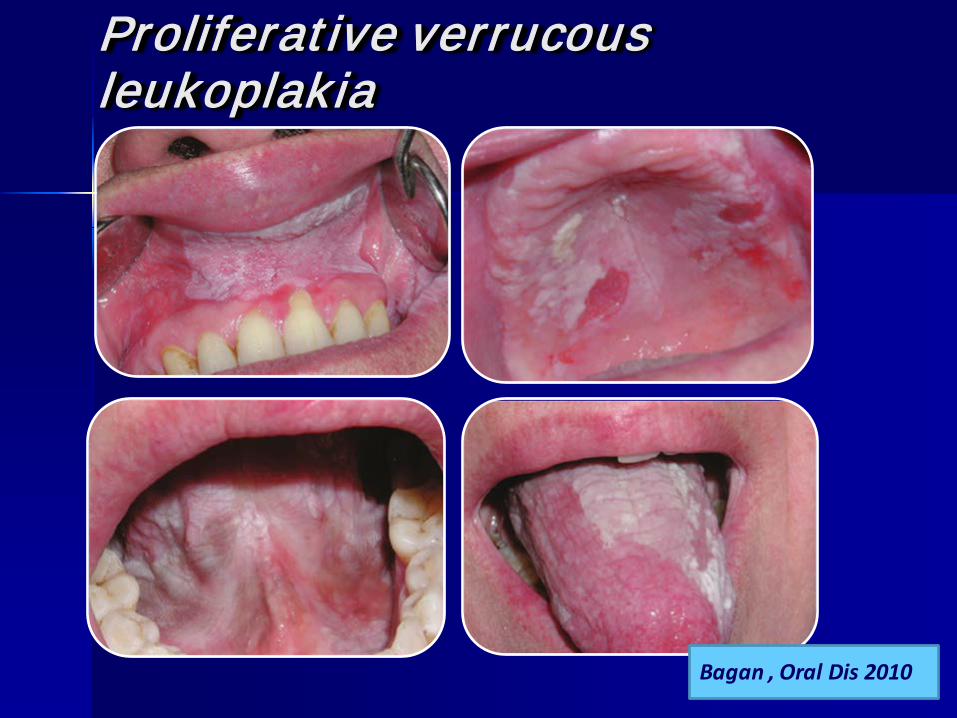
Βagan , Oral Dis 2010
Proliferative verrucousleukoplak ia
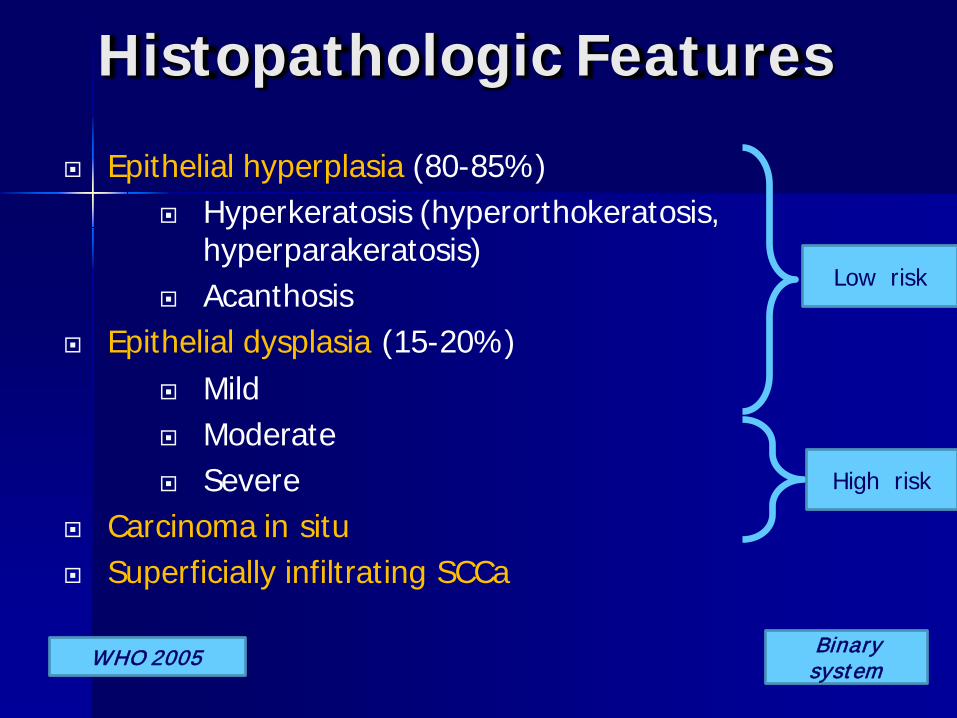
Histopathologic Features Epithelial hyperplasia (80-85%)
Hyperkeratosis (hyperorthokeratosis, hyperparakeratosis)
Acanthosis Epithelial dysplasia (15-20%)
Mild Moderate Severe
Carcinoma in situ Superficially infiltrating SCCa
WHO 2005
Low risk
High risk
Binary system
Erythroplakia Red patch or plaque that cannot be
characterized clinically as any other specific disease entity
Lack of keratinization and epithelial atrophy 90% of cases represent severe dysplasia, Ca in situ
or superficially invasive cancer Progression: 18-47%
Actinic Cheilitis
Premalignant lesion secondary to prolonged exposure to ultraviolet radiation
The lower lip is most often involved Slow to develop Pale blotchy appearance that gradually becomes
scaly Squamous carcinoma develops in 6-10% cases
DIAGNOSIS
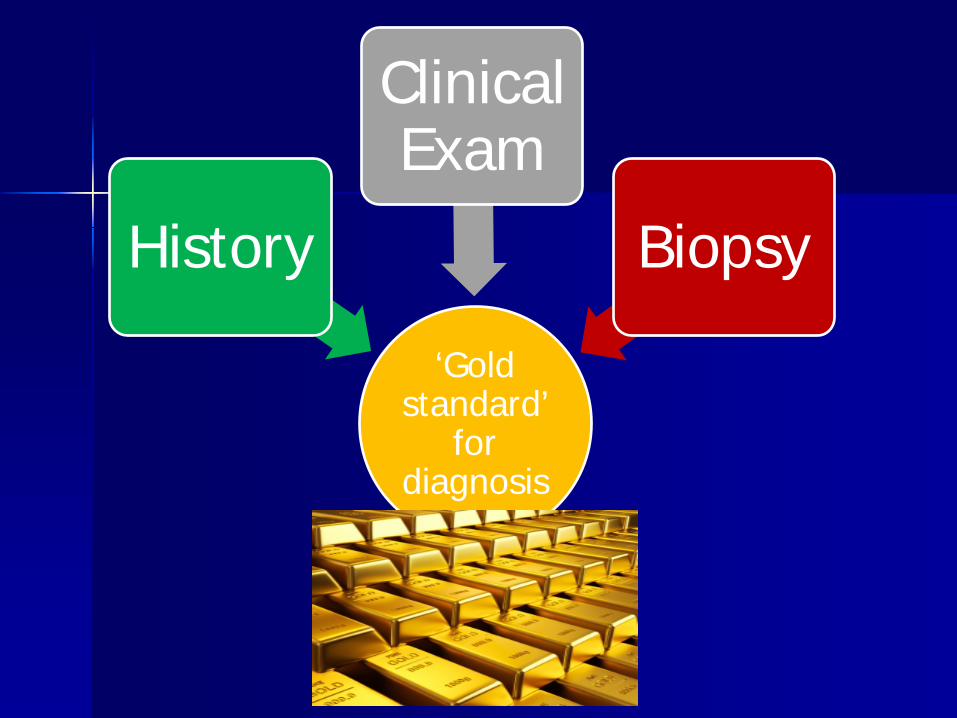
‘Gold standard’
for diagnosis
History
Clinical Exam
Biopsy
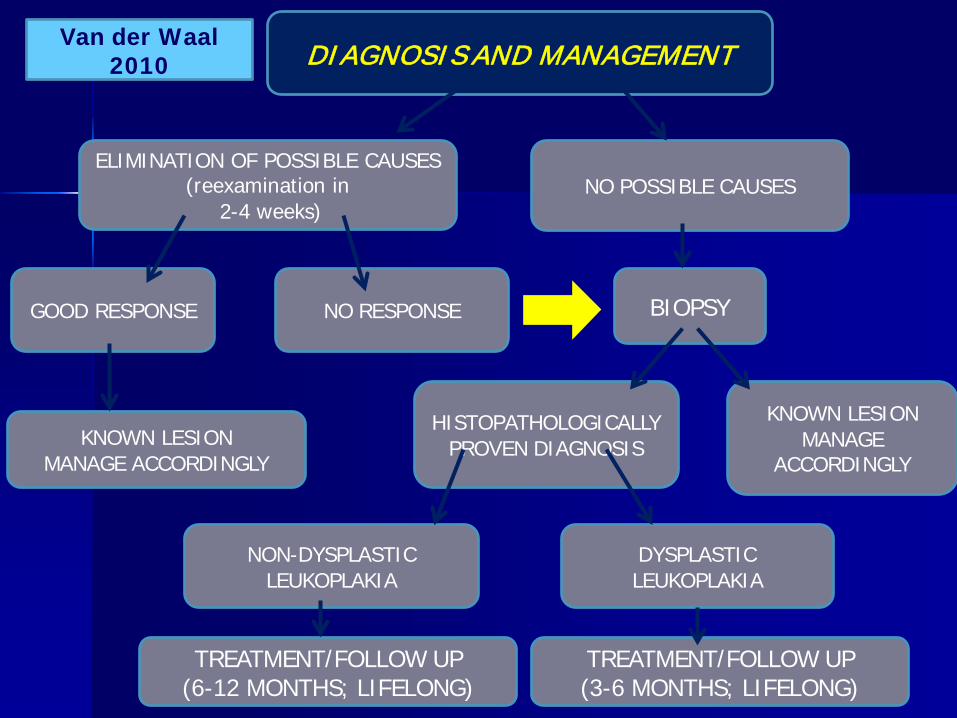
DIAGNOSIS AND MANAGEMENT
ELIMINATION OF POSSIBLE CAUSES (reexamination in
2-4 weeks)NO POSSIBLE CAUSES
BIOPSYNO RESPONSEGOOD RESPONSE
KNOWN LESIONMANAGE ACCORDINGLY
HISTOPATHOLOGICALLY PROVEN DIAGNOSIS
DYSPLASTIC LEUKOPLAKIA
NON-DYSPLASTIC LEUKOPLAKIA
TREATMENT/FOLLOW UP(6-12 MONTHS; LIFELONG)
TREATMENT/FOLLOW UP(3-6 MONTHS; LIFELONG)
KNOWN LESIONMANAGE
ACCORDINGLY
Van der Waal 2010
Scalpel or punch biopsy
Currently, the only definitive diagnostic method
Sample should be taken from the most suspicious areas
Multiple (geographic) biopsies
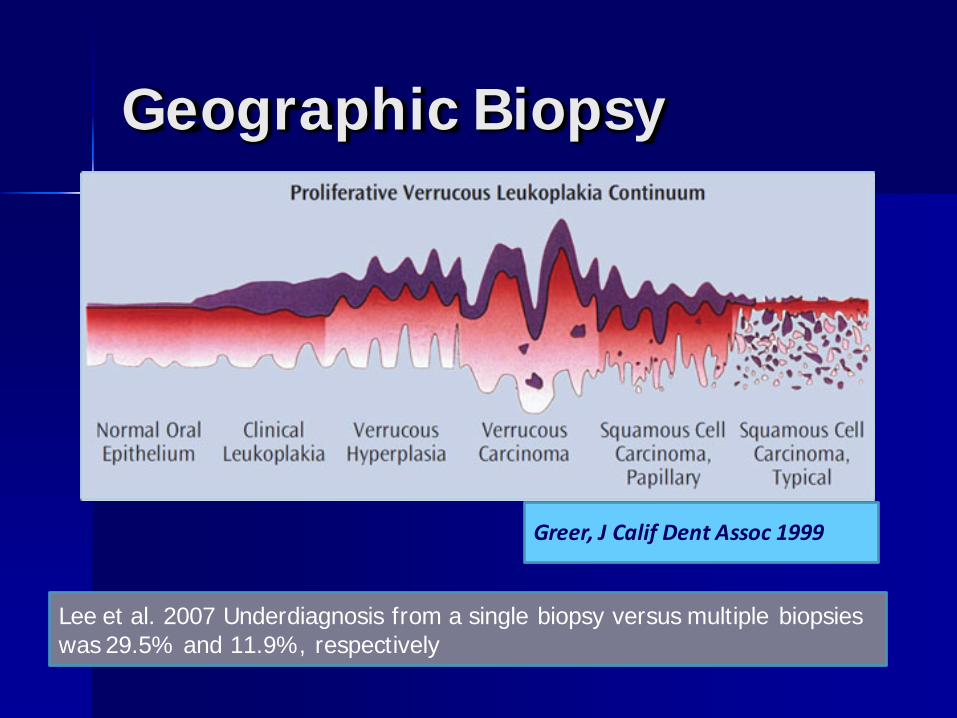
Geographic Biopsy
Greer, J Calif Dent Assoc 1999
Lee et al. 2007 Underdiagnosis from a single biopsy versus multiple biopsies was 29.5% and 11.9%, respectively

Proliferative verrucousleukoplakia

SCC

Proliferative verrucousleukoplakia

SCC (Second primary)


SCC (in multifocal leukoplakia)
Diagnostic Aids
Autofluorescence– VELscope– Identafi 3000
• Chemiluminence• Vizilite Plus with
Tοluidine blue• MicroLux DL
Toluidine blue
Oral cytology– Oral CDx brush Test
Saliva markers– microRNAs– mRNAs– Proteins
Diagnostic adjuncts to scalpel biopsy Useful if used by properly trained clinicians
in the proper setting In the hands of an inexperienced clinician,
these techniques may prove confusing, unnecessary and/or dangerous
They should not be used as a substitute of scalpel biopsy because of lack of confidence, lack of appropriate training in minor oral surgery, or ease of performance and reimbursement

MALIGNANT TRANSFORMATION
Malignant Transformation
Overall, 4-11% (3.6-17.5%) of oral leukoplakiasbecome squamous cell carcinoma
Annual MT rate: 1-3%– Average: 1.36% (Petti, Oral
Oncol 2003) Progression to invasive
carcinoma can range from a few weeks to 10 or more years, average 3 years
Malignant Transformation
Lesions of the floor of mouth and ventral tongue have a progression rate of 16% to 39% and, if female, 47%
Moderate dysplasia: 4-11%
Severe dysplasia: 20-35%
Factors associated with increased risk of malignant transformation
1. Female gender2. Long duration3. Non-smokers4. Location on the tongue and/or floor of mouth5. Size >200mm2 (5.4-fold higher risk)6. Non-homogeneous type 7. Presence of C. albicans8. Presence of epithelial dysplasia
Van der Waal, Oral Oncol. 2010
The use of molecular markers Advanced
knowledge of the molecular basis of cancer has prompted the investigation of a number of molecules as possible biomarkers
Investigated molecular predictors in oral PMDs
Cytogenetics– Loss of heterozygocity (LOH)–Aneuploidy
Cell cycle, proliferation and apoptosis
Cell signaling
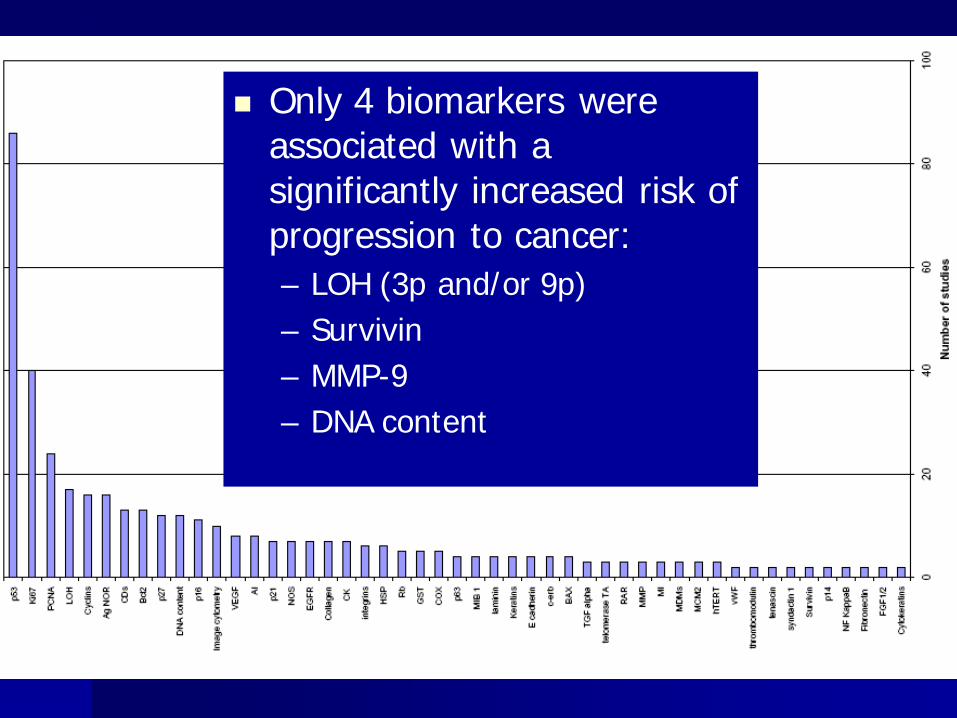
Only 4 biomarkers were associated with a significantly increased risk of progression to cancer:– LOH (3p and/or 9p)– Survivin– MMP-9– DNA content

MANAGEMENT
AIMS
Prevention of malignant transformation– Avoidance of progression – Elimination of lesion
Clinically Microscopically Molecularly
– Prevention of recurrence or new lesion development
Early detection of malignant transformation
Discontinuation/removal of etiologic factors Follow-up – Repeat biopsy Therapeutic intervention – Surgical removal
– Depends upon Histopathologic examination: presence and
degree of dysplasia Size and location of the lesions
Strategy
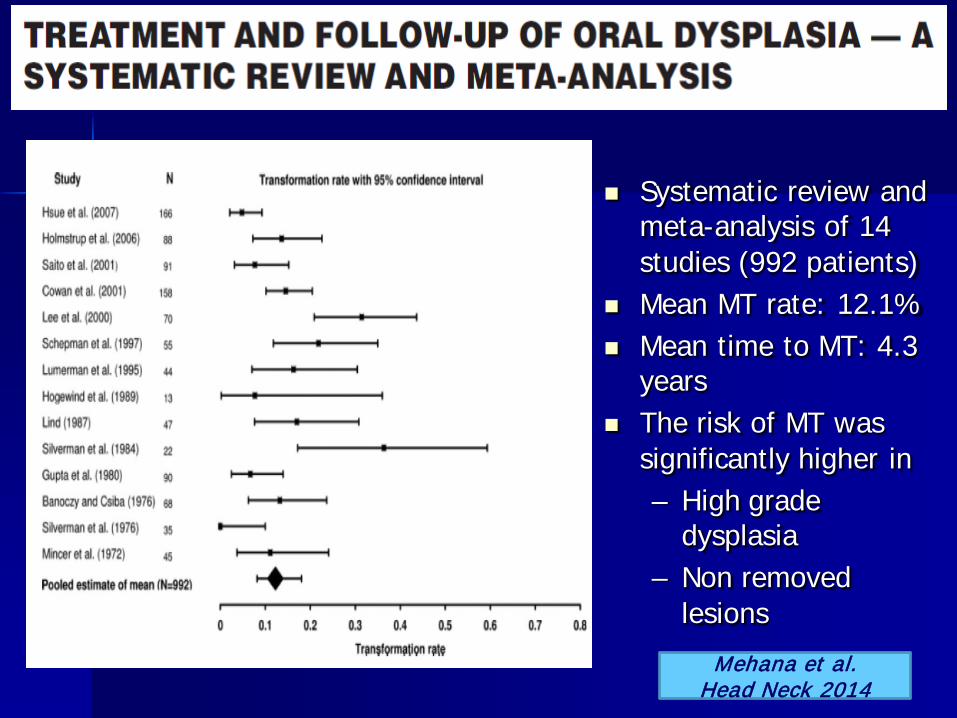
Systematic review and meta-analysis of 14 studies (992 patients)
Mean MT rate: 12.1% Mean time to MT: 4.3
years The risk of MT was
significantly higher in– High grade
dysplasia– Non removed
lesionsMehana et al.
Head Neck 2014
THERAPEUTIC APPROACHES Surgical
– Conventional (scalpel)– Laser– Cryosurgery– Electrosurgery
Conservative– Photodynamic therapy– Chemoprevention
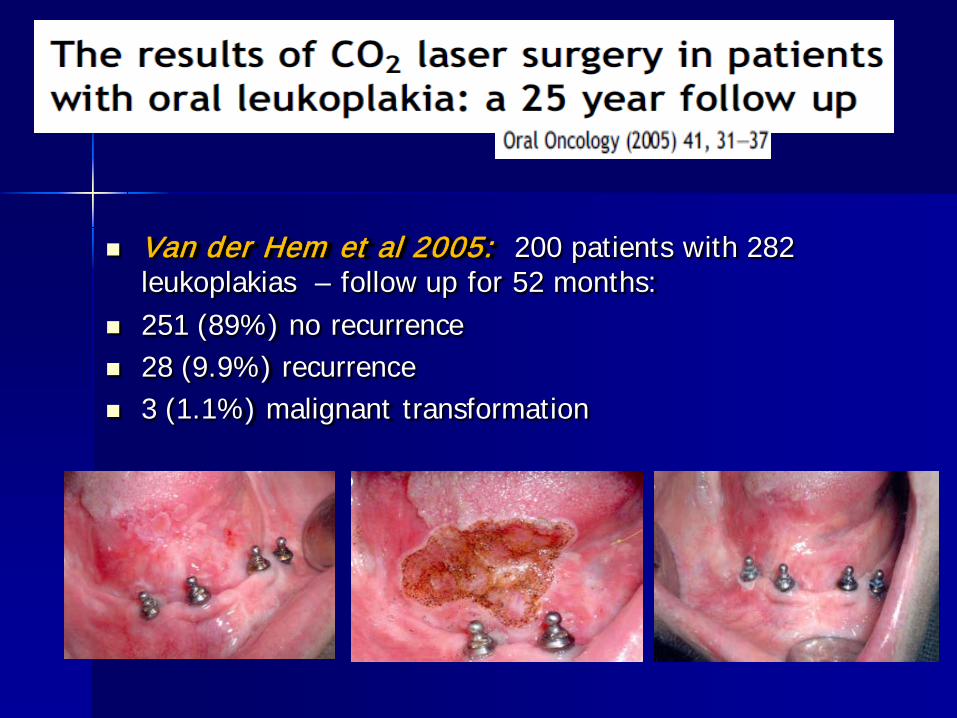
Van der Hem et al 2005: 200 patients with 282 leukoplakias – follow up for 52 months:
251 (89%) no recurrence 28 (9.9%) recurrence 3 (1.1%) malignant transformation
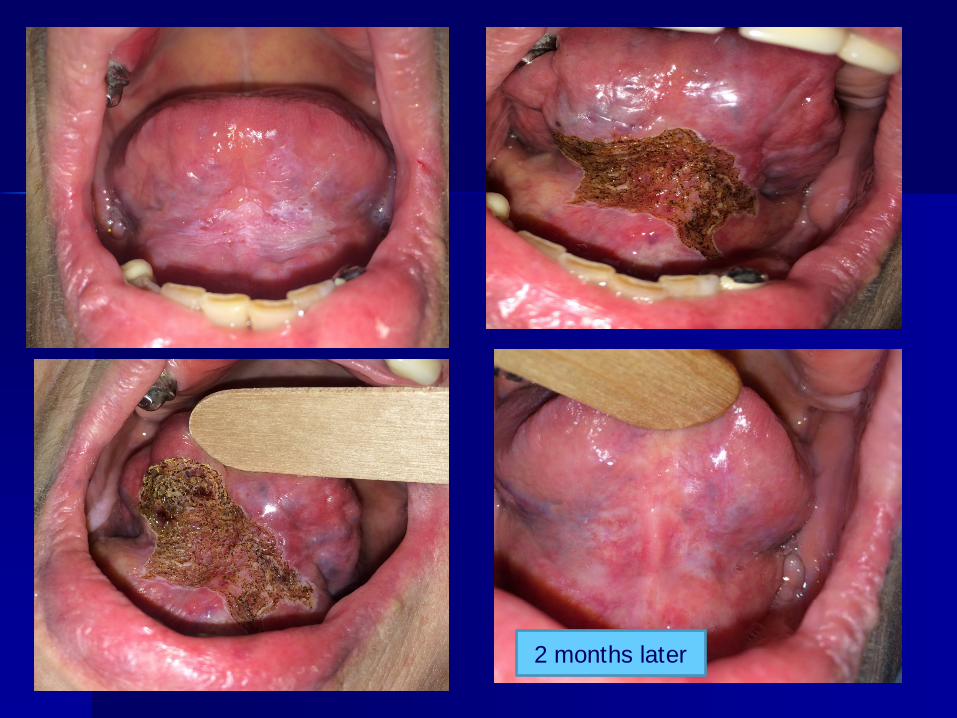
2 months later

The various therapeutic approaches frequently have only transient results
Despite clinical or microscopic remission, molecular alterations remain
Limitations
Lodi, Cochrane Database Syst Rev 2004
Field cancerization
Presence of one or more mucosal areas harboring cancer-associated genetic or epigenetic alterations
Provides an explanation for the high frequency of recurrences and second primary tumors in a large mucosal area
Has been associated with– Diffuse exposure to carcinogens– Lateral expansion and migration of a monoclone
of genetically altered cells
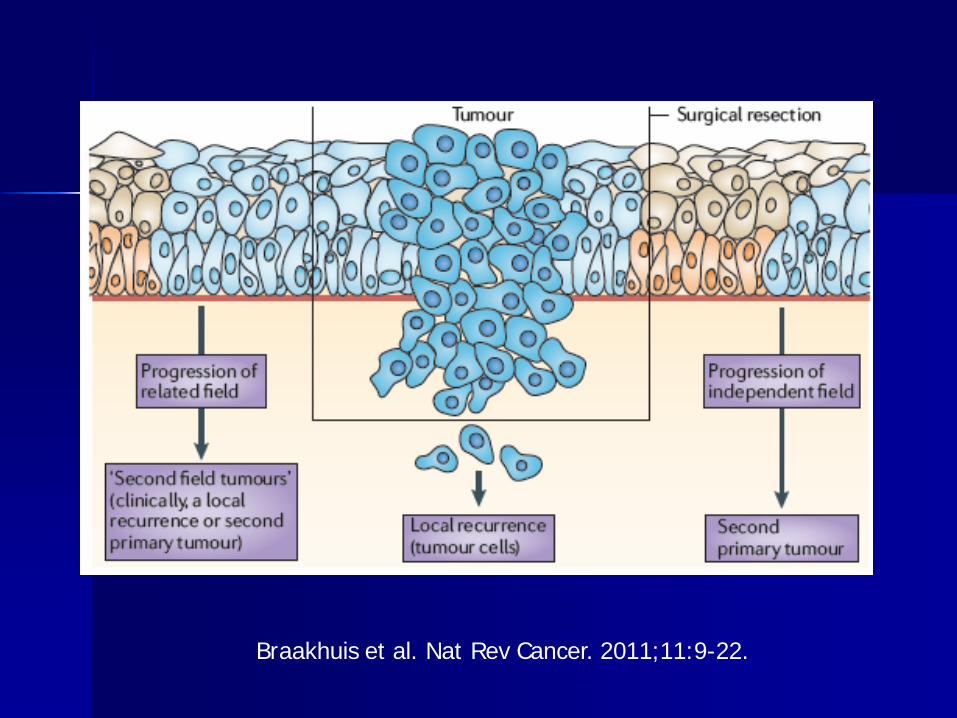
Braakhuis et al. Nat Rev Cancer. 2011;11:9-22.
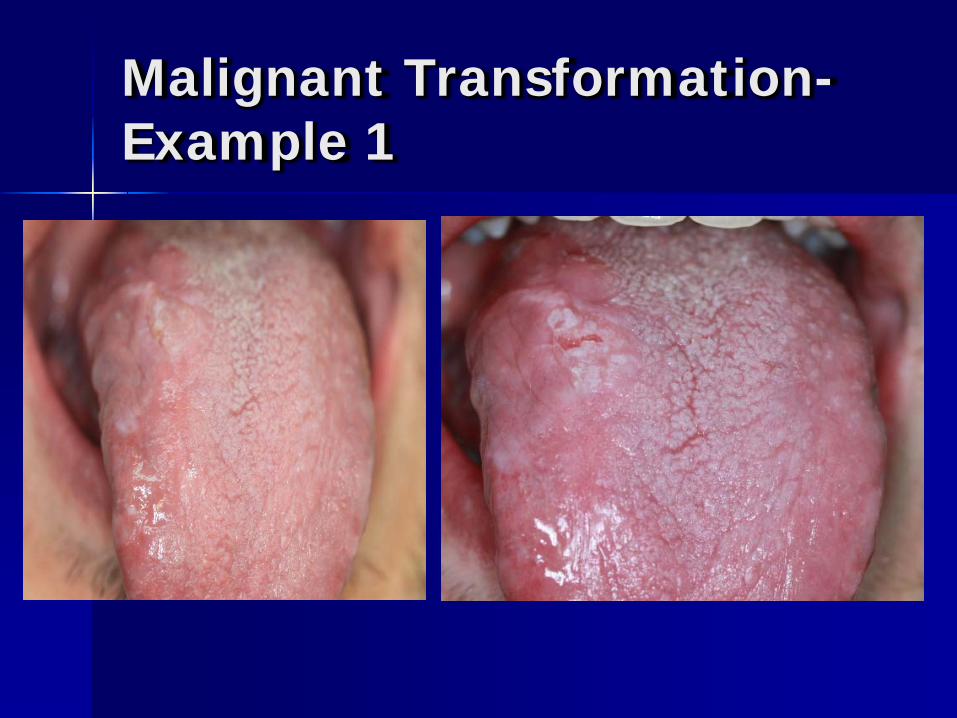
Malignant Transformation-Example 1

Malignant Transformation-Example 2
Chemoprevention
Carcinogenesis – multistep process Use of natural or synthetic substances
with the potential to prevent, stop, or reverse the process of carcinogenesis
Conclusion
At present, improvement in oral cancer survival lies in prevention– Primary: discontinuation of
predisposing factors– Secondary: regular and careful oral
examination of all dental patients for early detection of premalignant lesions

