oral pathology by: alex pagonis. nicotine stomatitis: palatal mucosa is white and criss-crossed with...
TRANSCRIPT

Oral Pathology
By: Alex Pagonis

Nicotine Stomatitis: palatal mucosa is white and criss-crossed with fissures, gingiva is a dried creekbed, lots of small red elevations
Etiology: smoking (usually of a pipe, possibly of the corn-cob fashion), may be caused by the heat rather than the tobacco, usually disappears after quitting smoking

Herpesvirus infections: 3 forms most comon is secondary herpes labialis, next is primary herpetic stomatitis (generalized oral infection) and least comon is small ulcers localized on palatal mucosa
Etiology: Herpesvirus hominis Most are Type 1 10% are Type II, can treat with acyclovir

Torus (mandibularis & palatinus): bony extoses in midline of hard palate or lingual aspect of mandible
Etiology: overgrowths of bone (possibly inherited) (found in freaks of nature… just kidding)
Ring torus (unrelated)

Traumatic ulcer: localize area of skin or mucosa where surface epithelium has been destroyed, usually painful and short duration
Etiology: common causes: dentures, biting injuries, hard foods, chemicals, dry cotton rolls
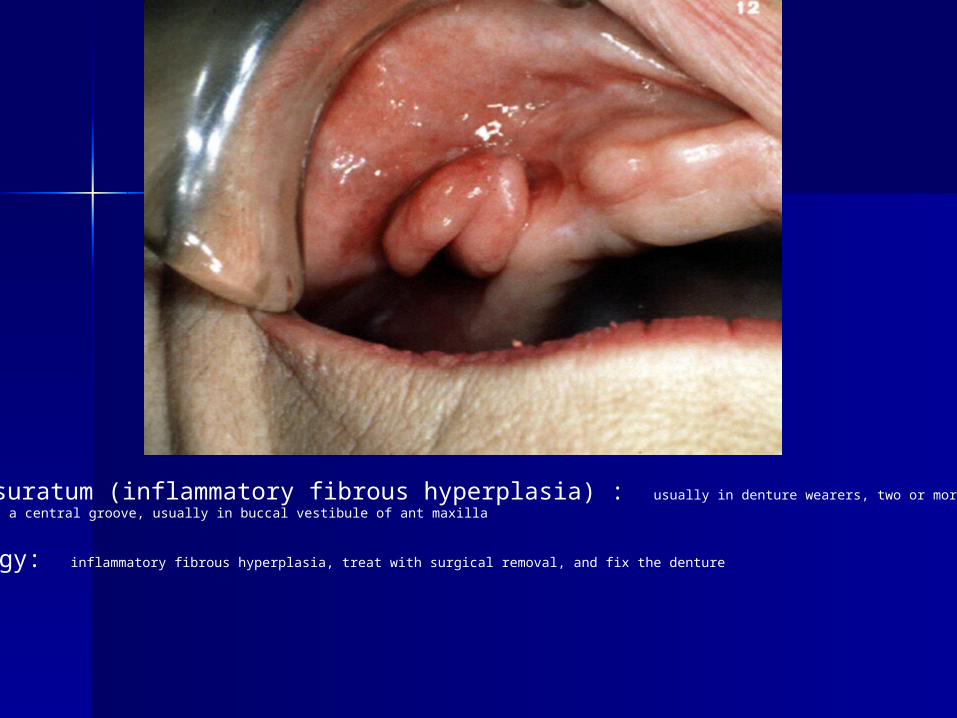
Epulis fissuratum (inflammatory fibrous hyperplasia) : usually in denture wearers, two or more folds of soft tissue separated by a central groove, usually in buccal vestibule of ant maxilla
Etiology: inflammatory fibrous hyperplasia, treat with surgical removal, and fix the denture

Idiopathic Osteosclerosis: osteosclerosis in an area of dense but normal bone in the jaws may or may not be attached to tooth, common in mand. molar-premolar area
Etiology: probably deveolpmental, maybe reactive in some cases, not treatment required, but periodic x-rays recommende

Denture sore mouth & Papillary hyperlasia: both are probably expressions of same disease, both related to wearing Dentures, red spots on posterior of palatal mucosa, can worsen to a red, pebbly appearance of papillary hyperplasia
Etiology: unkown, but candida albicans is probably contributory, often treated with antifungals good sterilization of dentures

Aphthous stomatitis (canker sore): 20-60% of population. Painful ulcers 1mm-2cm, single or multiple, begins as a red macule, then becomes ulcerated and covered by pyogenic membrane, found on freely movable mucosa NOT overlying bone
Etiology: unkown
Cure: pour salt on it, or use topical anaglegics/anti-inflammatories

Dilantin Gingival Hyperplasia: overgrowth of gingiva associated with dilantin (phyentoin therapy) medication for seizures
Etiology: stated above, may impair secretion of gingival fibroblasts permitting excessive gingival collagen can somewhat treat with good hygeine fibrous overgrowth requires surgical removal

Osteoporotic bone marrow defect: localized increase of marrow elements = radiographic defect. More common in womenUsually in molar region of mandible, especially extraction sites. Don’t have sharp borders like a cyst, and have scattered trabeculae.
Etiology: unkown, no treatment (book has a good pic)

Geographic tongue (benign migratory glossitis): maplike areas that are smooth and red with a whitish-yellow rim at the perimeter, parakaratin accumlates in rim, usually no sypmtoms or a slight burning.
Etiology: unkown, no treatment required

Leukoedema: filmy opaque gray discoloration of mucosa (usually buccal), wrinkeled appearance, may disappear on stretching seen in 90% of blacks, 40% of whites
Etiology: variation of normal, probably intracellular edema of superficial epithelial cells coupled w/ superficial parakeratin

Lichen Planus: 3 forms, erosive (white lacy lines and ulceration most common), reticular (white lacy lines), plaque (solid white). Most comonly on buccal mucosa
Etiology: unkown, but hypersensitivity reaction is supected

Irritation Fibroma: dome shaped soft tissue mass, on buccal surface along line of occlusion (sometimes lips and tongue) most common oral lesion
Etiology: trauma to affected mucosa (biting yourself)

Fordyce Granules: elevated yellow plaques or grains beneath mucosa, usually on buccal, 80% of population affected at some point
Etiology: ectopic sebaceous glands, presumably developmental anomaly

Mucocele: collection of saliva in the substance of the oral mucosa, soft elevations (light blue to white) lesion gets larger, then smaleer, then larger again. Most often on lower lip and buccal surface, but area which contains intraoral salivary glands is a potential site
Etiology: Traumatic severance of a salivary duct, treat by surgical excision

Peripheral firbroma: mass of tissue arising from gingiva near or between teeth, favors kids, may cause resorption of interdental bone
Etiology: unkown, should be removed surgically

Angular Cheilosis(cheilitis): fissuring at commissures of lips
Etiology: riboflavin deficiency, overclosure from loss of vertical dimension, oral skin bacteria and fungi (namely Candida)

Peripheral giant cell granuloma: nodular red soft mass arising from gingiva or alveolar mucosa, usually under 1 cm usually under 30 yrs and females, not painful, has lots of fibroblasts and mulitnucleated giant cells
Etiology: unkown, can be excised
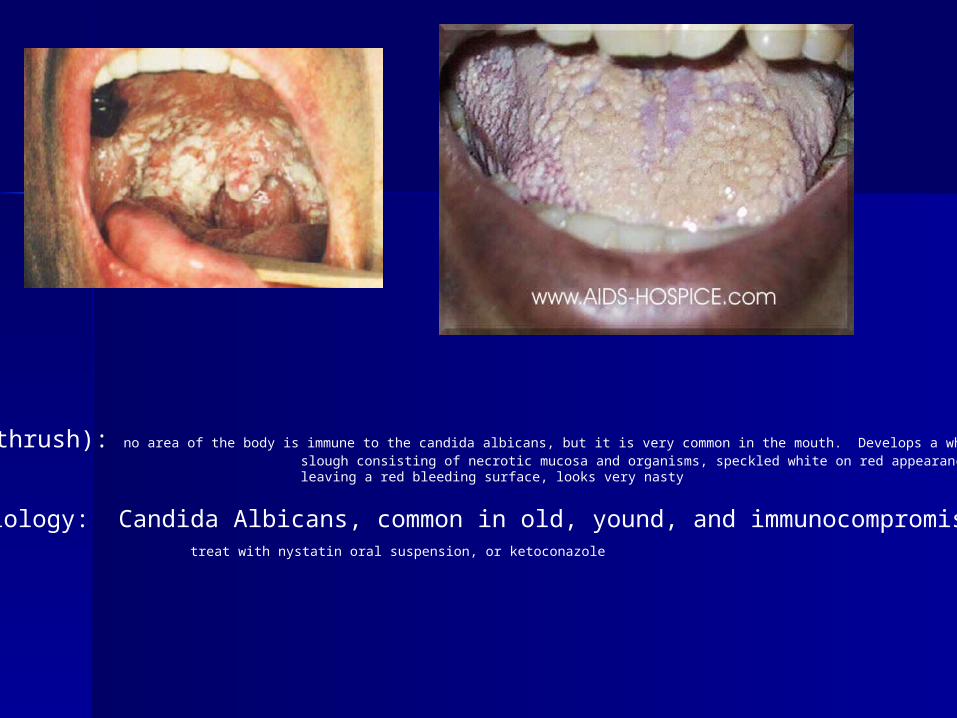
Candidosis (thrush): no area of the body is immune to the candida albicans, but it is very common in the mouth. Develops a white slough consisting of necrotic mucosa and organisms, speckled white on red appearance, white can be wiped off leaving a red bleeding surface, looks very nasty
Etiology: Candida Albicans, common in old, yound, and immunocompromised treat with nystatin oral suspension, or ketoconazole

Varix: red, blue, purple, elevations usually found on bucall mucosa, lip, tongue, floor of mouth if you have lot on your ventral tongue it is called caviar tongue.
Etiology: distended vein (possibly secondary to aging)


Pericapical cyst: cyst at the apex of a nonvital tooth from pulpitis, epithelium lined central cavity, sharply circumscriped radiolucent lesion

Pyogenic granuloma: red nodular overgrowth of granulation tissue arrising from mucosal or skin surface, bleed easily (vascular nature) very common with pregnancy
Etiology: unkown, maybe mild truama and infection (it looks the same as a periphereal fibroma to me, and im not too sure on how to differentiate b/n them so be careful)

Periapical Granuloma: also caused by pulpitis and looks like a periapical cyst to me… so refer to the book and see if you can tell what the difference is…. sorry
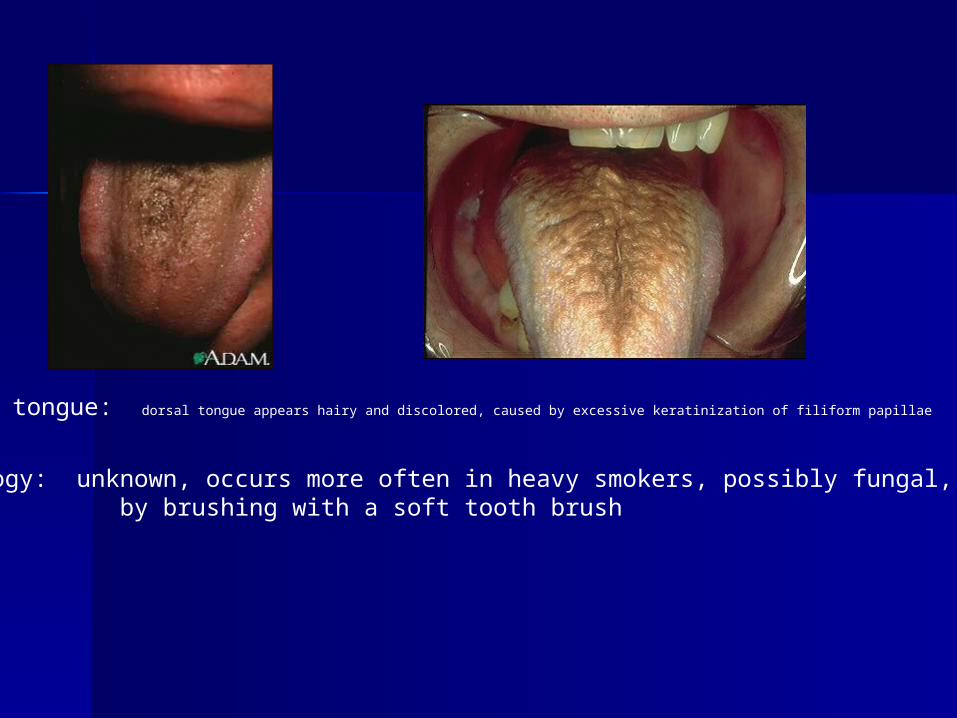
Hairy tongue: dorsal tongue appears hairy and discolored, caused by excessive keratinization of filiform papillae
Etiology: unknown, occurs more often in heavy smokers, possibly fungal, treat by brushing with a soft tooth brush

Periocronitis: inflammation around the gingival tissue around the crown of a partially erupted tooth, usually lower molars, becomes red swollen, and painful
Etiology: bacterial infection of gingiva, periocoronal dental follicle becomes a cul-de-sac extension of the mouth, excellent for bacteria, patient should rinse with water or saline, antibiotics indicated in severe cases, and extraction helps too

Amalgam tattoo: localized blue-gray pigment, usually inert and no tissue damage, but is permanent

Condensing osteitis: reaction to infection, unique in that it causes bone production instead of destruction, (looks like idiopathic osteosclerosis so be sure to read description)
Etiology: infection of pericapical tissue by organisms of low virulence, usually only treat symptomatic cases

Nasopalatine duct cyst: developmental cyst in nasopalatine duct, at apices of incisors, usually asymptomatic, rarely extends into mucosa, does not interefere with vitality often in edentulous
Etiology: developmental cyst arising from epithelial remnants of nasopalatine duct, can be surgically enucleated

Dentigerous cyst: cyst around crown of unerupted tooth, size is variable, usually 3rd molars
Etiology: accumulation of fluid between unerupted tooth and surrounding dental follicle, corrected by surgical enucleation, all should be submitted for pathological exam

Leukoplakia: white lesion of mucous membrane, hyperkeratosis, some will show dysplasia (a premaligant lesion), some will show carcinoma in-situ, or invasive carcinoma
Etiology: unkown, but trauma, smoking, alcohol, vitamin A insufficiency are suspect

Erythroplasia: red but not ulcerated area on mucous membrane, normal or roughened texture, variable size, often early carcinoma
Etiology: tobacco, alcohol, irritants … check out books pic
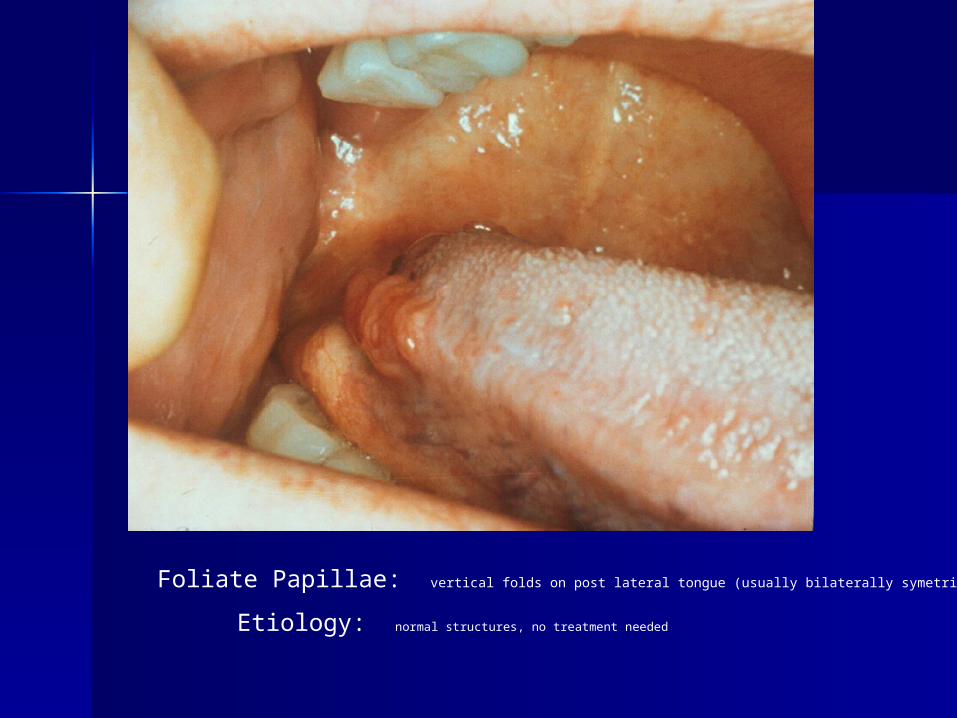
Foliate Papillae: vertical folds on post lateral tongue (usually bilaterally symetrical
Etiology: normal structures, no treatment needed

Squamous cell carcinoma: 90% of all oral cancers, may look like leukoplakia, or erythroplasia, also has chronic ulceration, more common on soft palate, lateral and ventral tongue, mucosa, and floor of mouth
Etiology: unkown, suspected smoking and alcohol

Snuff lesion: lesion develops on mucosa adjacent to smokeless tobacco, thick white corrugate, wrinkled mucosa, perio degeneration is also common.
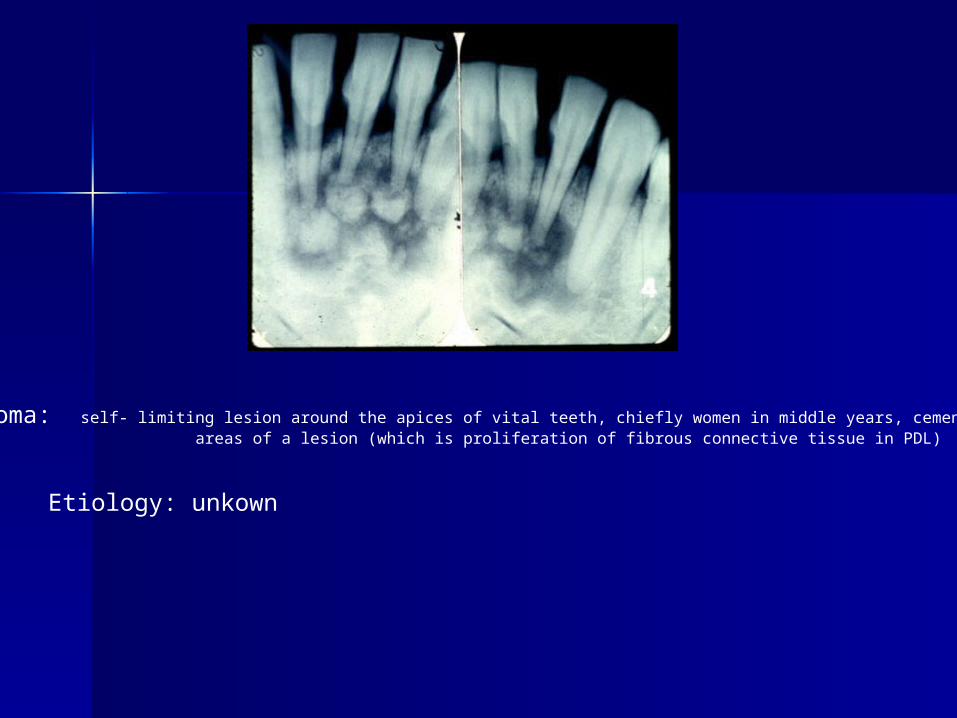
Cementoma: self- limiting lesion around the apices of vital teeth, chiefly women in middle years, cementum fills in areas of a lesion (which is proliferation of fibrous connective tissue in PDL)
Etiology: unkown